Indirect comparison of nivolumab ± ipilimumab (CheckMate 032) versus other treatments for recurrent small-cell lung cancer
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To estimate the comparative efficacy of nivolumab ± ipilimumab versus alternative treatments for small-cell lung cancer after at least one prior line of chemotherapy. Materials & m ethods: A systematic literature review identified six randomized controlled trials (RCTs) that could be connected in a network. The Kaplan–Meier survival curves from these RCTs were synthesized using network meta-analysis models. Aggregate-level matching was used to connect CheckMate 032 to the RCTs. Results: CheckMate 032 was connected to the network by Amrubicin Clinical Trial-1. Nivolumab ± ipilimumab had a more durable tumor response and more favorable long-term survival versus topotecan via intravenous and versus amrubicin. Conclusion: Compared with chemotherapies for recurrent small-cell lung cancer, nivolumab ± ipilimumab improves response duration, which may translate to long-term survival benefits.
Small-cell lung cancer (SCLC) is an aggressive malignancy that accounts for 10–15% of all lung cancers [1,2]. First-line (1L) treatment commonly includes platinum-based chemotherapy [3,4], which may be combined with radiotherapy [3–6]. Despite high initial response rates to 1L chemotherapy for select patients, median survival in 1L ranges from 15 to 20 months and from 8 to 13 months for patients with limited disease (LD), defined as stages I–III (T any, N any, M0) using American Joint Committee on Cancer Tumor, Node, Metastasis (TNM) classification, and extensive disease (ED), defined as stage IV (T any, N any, M 1a/b), respectively. Most patients (70%) fall into the latter group at diagnosis [5,7,8], for whom 5-year survival is only 1–2%. Five-year survival for LD patients is only marginally better at 10–20% [1,2,7,9]. ED patients who respond to 1L treatment may be considered for maintenance therapy, but this is not routinely offered because of minimal survival benefit (4% increase in 2-year survival rate) and potential for increased risk of cumulative toxicities [3,10].
For patients who fail to respond to 1L treatment or who subsequently progress, treatment options are limited. Topotecan, a topoisomerase I inhibitor, is currently the only drug approved by the US FDA for second-line (2L) treatment [3,4,9,11], which has been associated with median overall survival (OS) between 6.0 and 7.6 months for oral (p.o.) administration and between 5.8 and 8.0 months for intravenous (iv.) administration in 2L [3,4,9,11–17]. Furthermore, a recent study based on the US SEER database suggested median OS after initiating 2L treatment was less than 6 months for both platinum-refractory (3.7 months; 95% CI: 3.5–4.1) and platinum-sensitive patients (5.3 months; 95% CI: 4.9–5.8) in the Medicare population [18]. Given these suboptimal outcomes, the National Comprehensive Cancer Network (NCCN) still recommends that clinical trials be considered for 2L treatment, and if necessary third-line (3L) treatment, where available [10].
Nivolumab, a PD-1 checkpoint inhibitor, with or without the CTLA-4 inhibitor ipilimumab (nivolumab ± ipilimumab), has been recommended by the NCCN as an alternative to chemotherapy for 2L treatment of SCLC patients who have failed prior systemic therapy within 6 months in either the primary or adjuvant setting [10]. This recommendation was based on positive results from CheckMate 032 [19–23], a Phase I/II, open-label trial of nivolumab ± ipilimumab for SCLC patients who are platinum-sensitive (relapse ≥90 days) or platinum-resistant (relapse <90 days) after having received at least one platinum-based chemotherapy regimen (or during treatment for platinum-resistant patients). More recently, the FDA granted an accelerated approval for nivolumab as the first and only immuno-oncology treatment option for patients with metastatic SCLC whose cancer has progressed after platinum-based chemotherapy and at least one other line of therapy [24]. CheckMate 032 consisted of a nonrandomized cohort of patients treated with nivolumab alone or in combination with ipilimumab (nivolumab monotherapy 3 mg/kg iv. on day 1 of a 2-week cycle [Q2W]; nivolumab 1 mg/kg + ipilimumab 3 mg/kg iv. on day 1 of each 3-week cycle [Q3W] for a maximum of four cycles, followed by nivolumab 3 mg/kg iv. Q2W). A randomized cohort was added to the trial to evaluate nivolumab ± ipilimumab in this population. At the time of analysis, only the results of the nonrandomized cohort had been published, where the median OS for nivolumab + ipilimumab was 7.8 months (95% CI: 3.6–14.2) [22]. The aim of this study was to use data from the nonrandomized cohort in CheckMate 032 to estimate the comparative efficacy of nivolumab ± ipilimumab versus alternative treatments for SCLC after at least one prior line of chemotherapy.
Methods
Systematic literature review
A systematic literature review (SLR) was performed to identify randomized controlled trials (RCTs) featuring systemic therapies for the treatment of adults with refractory SCLC or disease progression after at least one prior line of chemotherapy or chemoradiotherapy. The RCTs were required to evaluate at least one of the following efficacy outcomes: OS, progression-free survival (PFS) and/or objective response rate (ORR). Relevant studies were identified based on predefined search strategies in line with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [25] from the following databases on 1 June 2018 using the Ovid platform: Medical Literature Analysis and Retrieval System Online, including In-Process/MEDLINE®, Daily/MEDLINE®, Excerpta Medica database and Cochrane Central Register of Controlled Trials (search strategies presented in Supplementary Tables 1–3). The proceedings of the following conferences from 2014 to 2016 were also searched: American Association for Cancer Research Annual Meeting, American Society of Clinical Oncology Annual Meeting, European Society for Median Oncology Congress and the International Association for the Study of Lung Cancer World Conference on Lung Cancer. Finally, manual searches were conducted of ClinicalTrials.gov and the WHO International Clinical Trials Registry Platform to identify eligible trials that had not yet been published but had results (Supplementary Tables 4 & 5). Two investigators participated in study selection and data extraction. A third investigator provided arbitration if there were any discrepancies in decisions. For all included trials, relevant patient and study characteristics and outcomes of interest were extracted.
Statistical analyses
In the absence of head-to-head clinical trial evidence for nivolumab ± ipilimumab and other chemotherapies including topotecan, an indirect treatment comparison by means of a network meta-analysis (NMA) of RCTs identified through an SLR provides a valid alternative [26–29]. In order to gauge the appropriateness of proceeding with an NMA [30], a feasibility assessment was first carried out to: determine whether the RCT evidence for the interventions formed one evidence network for the population and each outcome of interest; and assess the distribution of study characteristics, treatment characteristics, outcomes and patient characteristics that may have affected treatment effects across direct comparisons of the evidence networks. The most important potential treatment effect modifiers were identified as lines of previous treatments (1 vs >1), platinum sensitivity (sensitive vs resistant) and race (Asian vs non-Asian), which were included as subgroups of interest.
Given that the preexpansion cohort of CheckMate 032 was not randomized, it could not be connected to the wider network of RCTs. In the absence of a connected network of RCTs, a population-adjusted indirect treatment comparison can be performed using individual patient data (IPD) from an index trial, such as CheckMate 032, to create a connection with one of the trials in the network [31]. As IPD were not available for CheckMate 032 at the time of this analysis, we instead used matching based on aggregate study-level data from the nonrandomized cohort. By examining study design, inclusion and exclusion criteria and patient characteristics of all trials, the trial which was most similar to CheckMate 032 was selected and the CheckMate 032 arms were then treated as arms of this trial within the NMA. This relied on the same assumption as traditional NMA, as well as an additional assumption that the outcomes in the control arm from the external trial were applicable to CheckMate 032.
NMAs were performed for each outcome of interest where the RCTs identified in the SLR, including the matched trial featuring the previously disconnected arms of CheckMate 032, formed one evidence network and were deemed sufficiently similar for the population of interest. Under the assumption of consistency, the NMA model relates the data from the individual studies to basic parameters reflecting the (pooled) relative treatment effect of each intervention compared with the control (i.e., topotecan via iv.). Based on these basic parameters, the relative treatment effects between each of the contrasts in the network were obtained. All analyses were performed in a Bayesian framework involving a model with parameters, data and a likelihood function, and prior distributions. Only fixed-effect models were used as there was an insufficient number of trials per comparison to estimate between-study heterogeneity.
The NMA of OS and PFS was performed assuming nonproportional hazards. Fractional polynomial models were used to model the log hazard functions of the interventions in a trial. The difference in the parameters was considered the multidimensional treatment effect, which was pooled and indirectly compared across studies [27,32,33]. For the median duration of response (DOR) and number of patients at risk, a binomial likelihood and cloglog link (with offset for median) were used [34]. For ORRs, the NMA was performed based on the proportion of patients experiencing the event of interest using a regression model with a binomial likelihood and logit link [26]. Noninformative prior distributions were used for all models (assuming a normal distribution for the difference measures with a mean 0, variance 104).
The parameters of the different models were estimated using a Markov Chain Monte Carlo method implemented in the OpenBUGS software package [35,36]. A first series of iterations from the OpenBUGS sampler were discarded as ‘burn-in’, and the inferences were based on additional iterations using two chains. All analyses were performed using R version 3.0.3 (www.r-project.org/) and OpenBUGS version 3.2.3 (OpenBUGS Project Management Group).
The results of the NMA were presented with estimates for treatment effects of each intervention relative to the reference treatment. The posterior distributions of relative treatment effects were summarized by the median and 95% credible intervals (CrIs), which were constructed from the 2.5th and 97.5th percentiles of the posterior distributions. For OS, PFS and DOR, results were presented in terms of hazard ratios (HRs). Results for ORR were presented in terms of odds ratios (ORs).
Results
Systematic literature review
Based on the SLR, 18 RCTs [12–17,37–55] and one nonrandomized study [19–23] (CheckMate 032 was included as the reference population) evaluating 15 combination chemotherapies, 23 single-agent chemotherapies and best supportive care were identified (Figure 1 & Supplementary Table 6).

Figure 1. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses study selection flow diagram.
NMA: Network meta-analysis; RCT: Randomized controlled trial; SLR: Systematic literature review.
Feasibility assessment
Figure 2 presents the overall network of evidence, which included the disconnected nodes from the nonrandomized cohort of CheckMate 032 and all RCTs from the SLR that could be connected to each other. Three RCTs, which compared topotecan via iv. or p.o. administration to linsitinib, irinotecan to irinotecan + gemcitabine, and cisplatin + amrubicin to cisplatin + doxorubicin + etoposide + vincristine, were not included in the network given that they did not share an intervention in common with the other trials [40,49,51]. Four trials in the network were conducted exclusively in Asia [42–46,55]. Asian versus non-Asian race may be a treatment effect modifier based on evidence of significant OS improvement associated with amrubicin versus topotecan in Japan [44] that was not identified in a similar study conducted in Europe and North America [15]. Additional evidence from an RCT including both Asian and non-Asian patients is required to better understand whether these differences may be explained by distinctions in genetic background, medical care, study design and drug exposure. The Asian trials connected to a pooled node for platinum doublet, which included either cisplatin + etoposide [48,50] or a mix of carboplatin + etoposide (76.7%), carboplatin + irinotecan (13.3%) and cisplatin + irinotecan (10.0%) [46]. Finally, three trials in the network evaluated interventions that failed to demonstrate improved efficacy and therefore have not been recommended or licensed for SCLC [10] (cabazitaxel [37–39], lomustine + cyclophosphamide + etoposide [41], and topotecan via iv. + ziv-aflibercept [52,53]). These trials did not provide indirect evidence regarding other interventions of interest.

Figure 2. Network of trials included in the feasibility assessment.
Solid lines: randomized controlled trials; dotted line: nonrandomized controlled trial; red text: Asian studies; blue treatment nodes: approved or recommended for small-cell lung cancer; gray treatment nodes: not approved or recommended; light blue treatment node: only included in sensitivity analysis (excluded from base case).
†Platinum doublet included: cisplatin + etoposide ([50], [48]) or a mix of carboplatin + etoposide (76.7%), carboplatin + irinotecan (13.3%) and cisplatin + irinotecan (10.0%; Inoue et al.).
GFPC: Groupe Français de Pneumo-Cancérologie; iv.: Intravenous; JCOG: Japan Clinical Oncology Group; NJLCSGT: North Japan Lung Cancer Study Group Trial; p.o.: Oral; SWOG: Southwest Oncology Group.
Figure 3 shows the network that was analyzed after excluding the Asian studies (n = 4), trials no longer connected due to exclusion of Asian studies (n = 2) and nonrecommended/licensed treatments (n = 3). O’Brien et al. was the only trial in the network that included patients who were incompatible with standard iv. chemotherapy due to co-morbidities or refusal on account of the risk of toxicity [56]. In contrast, all other trials in the network, except for CheckMate 032, featured at least one arm with iv. chemotherapy. Therefore, O’Brien et al. was only included in a sensitivity analysis. As CheckMate 032 was not connected to the network and IPD were not available, aggregate-level matching was used to connect CheckMate 032 to the network of RCTs. To identify the most similar trial to CheckMate 032, the trials included in this network [12–17] were compared in terms of study, patient, outcome and treatment characteristics. Amrubicin Clinical Trial-1 (ACT-1) was the most similar trial to CheckMate 032; consequently, the nivolumab and the nivolumab + ipilimumab arms from the nonrandomized cohort of CheckMate 032 were included as additional arms in ACT-1.
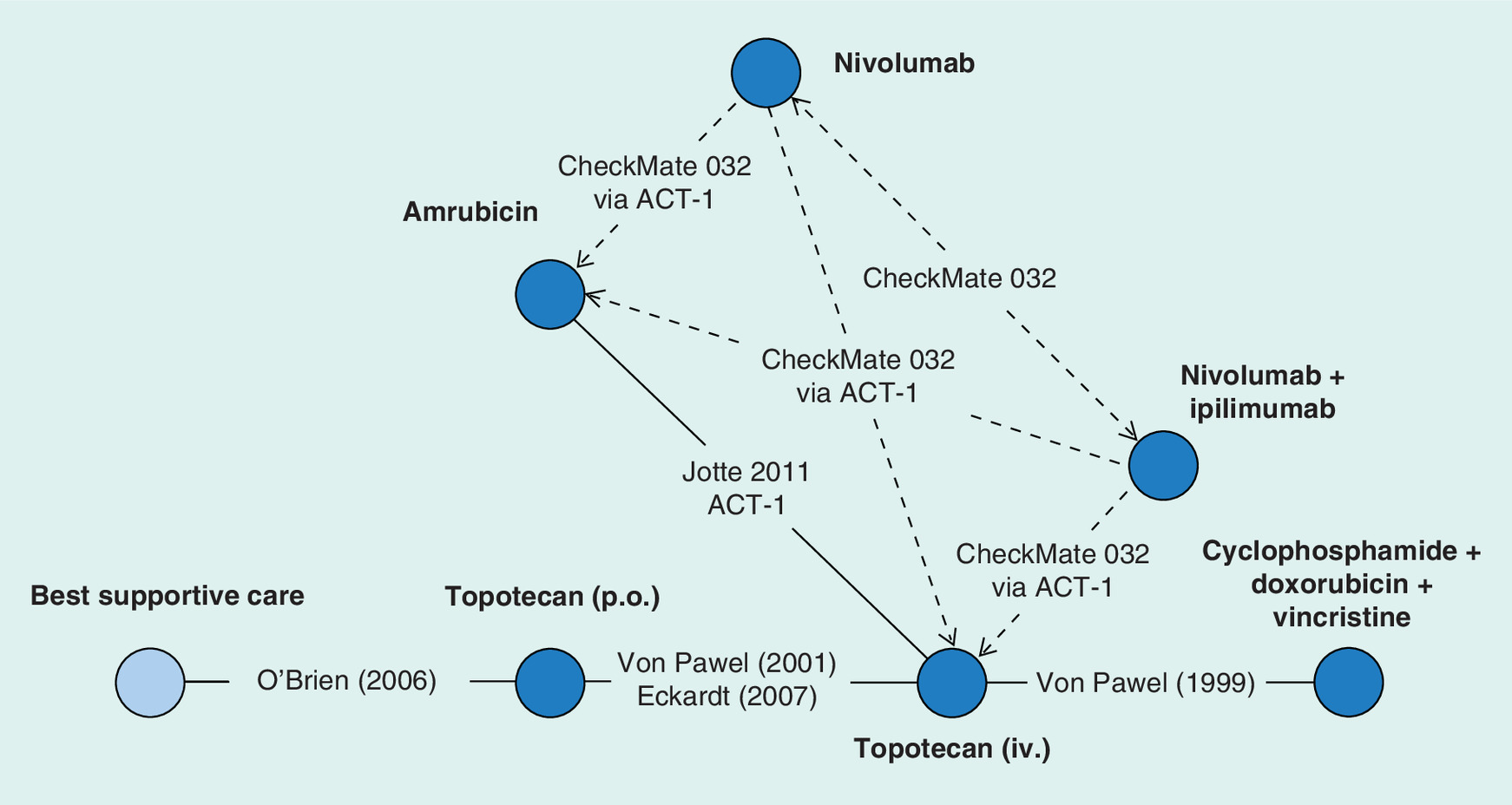
Figure 3. Network of non-Asian randomized controlled trials included in the network meta-analysis with CheckMate 032 connected through Amrubicin Clinical Trial-1.
Solid lines: randomized controlled trials; dotted lines: hypothetical nonrandomized controlled trial; blue treatment nodes: approved or recommended for small-cell lung cancer; light blue treatment node: only included in sensitivity analysis (excluded from base case).
ACT-1: Amrubicin Clinical Trial-1; iv.: Intravenous; p.o.: Oral.
All the trials included adults with either LD or ED SCLC, and had disease progression after at least one previous platinum-containing regimen. CheckMate 032, ACT-1 and O’Brien et al. included both platinum-sensitive and platinum-resistant or -refractory patients, whereas the other four trials included only patients who were platinum-sensitive [13,14,16,17], with definitions regarding platinum sensitivity ranging from recurrence or progression at least 60 or 90 days after completion of 1L chemotherapy. All trials were conducted entirely in 2L patients, except for CheckMate 032, which also included patients with up to five prior lines of therapy. CheckMate 032 allowed ECOG performance score of 0–1, which was consistent with ACT-1 (amended from 0 to 2), whereas other trials included patients with ECOG 0–2. All trials allowed patients with asymptomatic CNS metastases. Within interventions, dosing was consistent across the included trials, although ACT-1 was the only trial to place a limit on the maximum number of cycles (six) that could be received. Overall, the inclusion criteria in CheckMate 032 were most similar to ACT-1 in terms of platinum sensitivity and ECOG status.
CheckMate 032 is an ongoing Phase I/II multicenter trial conducted in Europe and North America. ACT-1 was a Phase III multicenter trial conducted in a similar region (also including sites in Australia) published in 2014. Other trials included a mix of older (1999–2011) Phase II or Phase III trials (or phase was not reported) that included centers from North America, except for Von Pawel 2001, which included only centers from Europe, South Africa and Australia. Beyond North America and Europe, other regions included southeast Asia and Australia [14], South Africa [17] and Russia [12]. With the exception of CheckMate 032, where the nonrandomized cohort was included, all trials were randomized and generally low risk of bias (or unclear), except in terms of performance bias, which was high risk given the open-label or single-blinded trial designs (Supplementary Figure 1). Patients characteristics from all the included studies can be found in Table 1.
| Trial | Treatment | N | ECOG 0 | ECOG 1 | ECOG 2 | LD | ED | Sensitive | Resistant | Patient trial inclusion | Ref. |
|---|---|---|---|---|---|---|---|---|---|---|---|
| ACT-1; Phase III | Topotecan, iv. | 213 | 72 (33.8%) | 137 (64.3%) | 4 (1.9%) | 26 (12.2%) | 187 (87.8%) | 117 (54.9%) | 96 (45.1%) | Progression after 1L platinum-based chemo (sensitive [≥90 days] and refractory) | [15] |
| Amrubicin | 424 | 126 (29.7%) | 289 (68.2%) | 9 (2.1%) | 53 (12.5%) | 371 (87.8%) | 225 (53.1%) | 199 (46.9%) | |||
| ARD12166; Phase II†, †† | Cabazitaxel | 90 | 31 (34.4%) | 59 (56.6%) | 0 (0%) | 0 (0%) | 90 (100%) | 45 (50.0%) | 45 (50.0%) | Progressed after 1L chemo (sensitive [≥90 days] and refractory [<90 days]) | [37–39] |
| Topotecan | 89 | 17 (19.1%) | 71 (79.8%) | 1 (1.1%) | 0 (0%) | 89 (100%) | 46 (51.7%) | 43 (48.3%) | |||
| CheckMate 032; Phase I/II | Nivolumab | 98 | 73/245 (39.8%)† | 171/245 (69.8%)† | 0 (0%) | (24.0%)‡ | (76.0%)‡ | 55 (56.1%) | 30 (30.6%) | Progression after ≥1L platinum-based therapy | [19–23] |
| Nivolumab + ipilimumab | 61 | 49/156 (31.4%)† | 106/156 (67.9%)† | 0 (0%) | 25 (41.0%) | 23 (37.7%) | |||||
| Chiappori et al. (2016); Phase II†, †† | Topotecan, iv. or p.o. | 15 | 12 (80.0%) | 3 (20.0%) | 0 (0%) | 15 (100%) | 7 (46.7%) | 8 (53.3%) | Progression after 1L platinum-based chemo (sensitive [<90 days] and resistant [>90 days]) | [40] | |
| Linsitinib | 29 | 24 (82.8%) | 5 (17.2%) | 0 (0%) | 29 (100%) | 13 (44.8%) | 16 (55.2%) | ||||
| Eckardt et al. (2007); Phase III | Topotecan, p.o. | 153 | 48 (31.4%) | 85 (55.6%) | 20 (13.1%) | 51 (33.3%) | 102 (67.7%) | 153 (100%) | 0 (0%) | Recurrence after ≥90 days after CR or PR to 1L therapy | [14] |
| Topotecan, iv. | 151 | 35 (23.2%) | 98 (64.9%) | 18 (11.9%) | 45 (29.8%) | 106 (70.2%) | 151 (100%) | 0 (0%) | |||
| GFPC 0501; Phase II†, †† | CEL | 65 | 22 (33.8%) | 34 (52.3%) | 9 (13.8%) | 34 (52.3%) | 31 (47.7%) | 65 (100%) | 0 (0%) | Progression after 1L chemo (<3 months) | [41] |
| CAV | 66 | 23 (24.8%) | 33 (50.0%) | 10 (15.2%) | 27 (40.9%) | 39 (59.1%) | 66 (100%) | 0 (0%) | |||
| JCOG0605; Phase III†, †† | CEI | 90 | 52 (57.8%) | 36 (40%) | 2 (2.2%) | 20 (22.2%) | 70 (77.8%) | 90 (100%) | 0 (0%) | Relapse or progression ≥90 days after 1L platinum-based chemo or CRT | [42,43] |
| Topotecan, iv. | 90 | 40 (44.4%) | 47 (52.2%) | 3 (3.3%) | 25 (27.8%) | 65 (72.2%) | 90 (100%) | 0 (0%) | |||
| Jotte et al. (2011); Phase II | Amrubicin | 50 | 20 (40.0%) | 24 (48.0%) | 6 (12.0%) | 0 (0%) | 50 (100%) | 50 (100%) | 0 (0%) | Recurrence/ progression ≥90 days after completion of 1L chemo | [16] |
| Topotecan, iv. | 26 | 10 (38.5%) | 14 (53.8%) | 2 (7.7%) | 0 (0%) | 26 (100%) | 26 (100%) | 0 (0%) | |||
| NJLCSGT 0402; Phase II†, †† | Amrubicin | 29 | 15 (55.6%) | 10 (37.0%) | 2 (7.4%) | 15 (55.6%) | 12 (44.4%) | 17 (58.6%) | 12 (41.4%) | Progression after 1L platinum-based chemo (sensitive [≥90 days] and refractory) | [44] |
| Topotecan, iv. | 30 | 17 (56.7%) | 11 (36.7%) | 2 (6.7%) | 18 (60.0%) | 12 (40.0%) | 19 (63.3%) | 11 (36.7%) | |||
| NJLCSGT 0702; Phase II†, †† | Amrubicin | 27 | 6 (8.6%) | 41 (58.6%) | 23 (32.9%) | 27 (38.6%) | 43 (61.4%) | 27 (100%) | 0 (0%) | Relapse or progression >90 days after 1L platinum-based chemo | [45,46] |
| Platinum doublet | 30 | 8 (11.3%) | 44 (62%) | 19 (26.8%) | 23 (32.4%) | 48 (67.6%) | 30 (100%) | 0 (0%) | |||
| O'Brien et al. (2006)§; Phase III | BSC | 70 | 6 (8.6%) | 41 (58.6%) | 23 (32.9%) | 27 (38.6%) | 43 (61.4%) | 35 (50.0%)¶ | 35 (50.0%)¶ | Following 1L chemo and unsuitable for chemo iv. | [12] |
| Topotecan, p.o. | 71 | 8 (11.3%) | 44 (62.0%) | 19 (26.8%) | 23 (32.4%) | 48 (67.6%) | 30 (42.3%)¶ | 41 (57.7%)¶ | |||
| O'Bryan et al. (1990); Phase NR†, †† | CTVC | 45 | 24 (53.3%)# | 21 (46.7%)§ | 38 (84.4%) | 7(15.6%) | – | – | Failed or relapse after 1L systemic therapy | [48] | |
| Cisplatin + etoposide | 84 | 33 (39.5%)# | 51 (60.7%)§ | 66 (78.6%) | 18 (21.4%) | – | – | ||||
| Pallis et al. (2009); Phase II†, †† | Gemcitabine + irinotecan | 38 | 12 (31.6%) | 20 (52.6%) | 6 (15.8%) | – | – | 20 (52.6%) | 18 (47.4%) | Following ≥1L chemo (ED patients), or CRT (LD patients) | [49] |
| Irinotecan | 31 | 10 (32.3%) | 19 (61.3%) | 2 (6.5%) | – | – | 10 (32.3%) | 18 (58.1%) | |||
| Sculier et al. (2002); Phase II†, †† | Cisplatin + etoposide | 31 | 14 (45.2%)‡‡ | 17 (54.8%)§§ | – | 2 (6.5%)¶¶ | 29 (93.5%)## | – | – | Failed during, or relapsed after 1L chemo | [50] |
| CCE | 34 | 11 (32.4%)‡‡ | 23 (67.6%)§§ | – | 2 (5.9%)¶¶ | 32 (94.1%)## | – | – | |||
| Sekine et al. (2015); Phase II††† | CODE | 39 | – | – | – | 39 (100%) | – | – | – | Responded (CR, PR or SD) to 1L CRT | [51] |
| Amrubicin + cisplatin | 36 | – | – | – | 36 (100%) | – | – | – | |||
| SWOG S0802; Phase II††† | Topotecan, iv. + Ziv-Aflibercept | 97 | 26 (26.8%) | 71 (73.2%) | 0 (0%) | 31 (32.0%) | 66 (68.0%) | 42 (43.3%) | 55 (56.7%) | Progression after 1L platinum-based chemo (sensitive [>90 days for ED or ≥180 days for LD] and refractory [≤90 days for ED or <180 days for LD]) | [52,53] |
| Topotecan, iv. | 92 | 36 (39.1%) | 56 (60.6%) | 0 (0%) | 27 (29.3%) | 65 (70.7%) | 41 (44.6%) | 51 (55.4%) | |||
| Von Pawel et al. (1999); Phase NR | Topotecan, iv. | 107 | 18 (16.8%) | 64 (59.8%) | 25 (23.4%) | 18 (16.8%) | 89 (83.2%) | 107 (100%) | 0 (0%) | Progression ≥60 days after completion of 1L chemo | [17] |
| CAV | 104 | 20 (19.2%) | 64 (61.5%) | 20 (19.2%) | 16 (15.4%) | 88 (84.6%) | 104 (100%) | 0 (0%) | |||
| Von Pawel et al. (2001); Phase II | Topotecan, p.o. | 52 | 10 (19.2%) | 34 (65.4%) | 8 (15.4%) | 14 (26.9%) | 37 (71.2%) | 52 (100%) | 0 (0%) | Recurrence after ≥90 days after CR or PR of 1L chemo | [13] |
| Topotecan, iv. | 54 | 18 (33.3%) | 21 (38.9%) | 15 (27.8%) | 14 (25.8%) | 39 (72.2%) | 54 (100%) | 0 (0%) | |||
| Yoon et al. (2015); Phase II††† | Belotecan | 61 | – | – | – | – | – | – | – | Progression <6 months after 1L platinum-based chemo or CRT | [55] |
| Topotecan, iv. | 55 | – | – | – | – | – | – | – |
†
Baseline characteristics for the randomized cohort and the nonrandomized cohort of CheckMate 032 were pooled.
‡
These estimates are derived from a clinical study report for CheckMate 032 on all cohorts;
§
O’Brien was only included in the sensitivity analysis;
¶
Patients reported to have a treatment-free interval of more than 90 days are considered platinum-sensitive while those with a treatment-free interval of ≤90 days are considered platinum-resistant.
#
Karnofsky performance status of 0–1.
††
Karnofsky performance status of 2–3.
‡‡
Karnofsky performance status of 60–70.
§§
Karnofsky performance status of 80–100.
¶¶
Stages I–III.
##
Stage IV.
†††
Studies not included in the network meta-analysis.
1L: First line; BSC: Best supportive care; CAV: Cyclophosphamide + doxorubicin + vincristine; CCE: Carboplatin + cisplatin + etoposide; CEI: Cisplatin, + etoposide + irinotecan; CEL: Cyclophosphamide + etoposide + lomustine; CODE: Cisplatin + doxorubicin + etoposide + vincristine; CR: Complete response; CRT: Chemoradiotherapy; CTVC: Carmustine + thiotepa + vincristine + cyclophosphamide; ECOG: Eastern Cooperative Oncology Group; ED: Extensive disease; iv.: Intravenous; LD: Limited disease; NR: Not reported; PR: Partial response; p.o.: Oral; SD: Stable disease.
OS and ORRs were reported in all of the trials. ORR (a complete response [CR] or partial response [PR]) was investigator-assessed using the Response Evaluation Criteria in Solid Tumors (RECIST) in CheckMate 032 (version 1.1) and ACT-1 (version 1.0), whereas three trials assessed ORR by blinded-independent review using the WHO criteria [13,14,17]. Jotte et al. did not provide a definition for OS or PFS but did report that RECIST (v1.0) was used to assess response. O’Brien et al. did not report how ORR was determined. All of the trials, except O’Brien et al., reported DOR, defined as time from first documented response to disease progression. However, CheckMate 032 defined DOR as time from a best overall response of PR or CR until the date of documented progressive disease or death due to any cause.
Three trials [15,16,19–22] reported PFS, whereas three trials [13,14,17] reported time to progression (TTP). TTP differs from PFS in that any deaths are considered censored values in the TTP analyses, while they are considered events in the PFS analyses. In the context of NMA, there are differences between treatment arms that are modeled. This means that if the mortality rates are equivalent across arms in a trial, then the bias arising from the use of TTP is not expected to be substantial. No significant differences in OS were observed in either of the two trials reporting TTP data, so they were included within the PFS analysis.
Network meta-analysis
Overall survival & progression-free survival
Digitized (DigitizeIt; www.digitizeit.de/) OS Kaplan–Meier curves from ACT-1 are presented in Figure 4, including CheckMate 032 nivolumab ± ipilimumab overlaid with ACT-1 as if patients were randomized to this trial. OS for nivolumab appears to plateau at 24 months (n = 14 patients at risk). Figure 5 presents the time-varying HRs for each intervention versus topotecan via iv. for OS and PFS, including the 95% CrI. The HRs for OS trended in favor of topotecan via iv. versus nivolumab ± ipilimumab in the early time periods (3–6 months), after which the direction of the effect switched in favor of the latter. This advantage steadily increased up to around 30 months at which time the differences between the treatments became relatively constant. Of the remaining chemotherapies, oral totopecan performed best relative to topotecan via iv., suggesting some potential benefit with the p.o. form, while amrubicin appeared to offer very similar efficacy. Including the O’Brien et al.’s study as part of the sensitivity analysis did not lead to any substantive changes in the direction or magnitude of the observed relative effects, and showed HRs that trended in favor of nivolumab ± ipilimumab versus best supportive care. For PFS, a similar trend to that seen for OS was observed but in this case the differences in favor of nivolumab ± ipilimumab versus topotecan via iv. became relatively constant at around 18 months.

Figure 4. Kaplan–Meier curve of overall survival for CheckMate 032 and Amrubicin Clinical Trial-1.
HR: Hazard ratio; iv.: Intravenous.
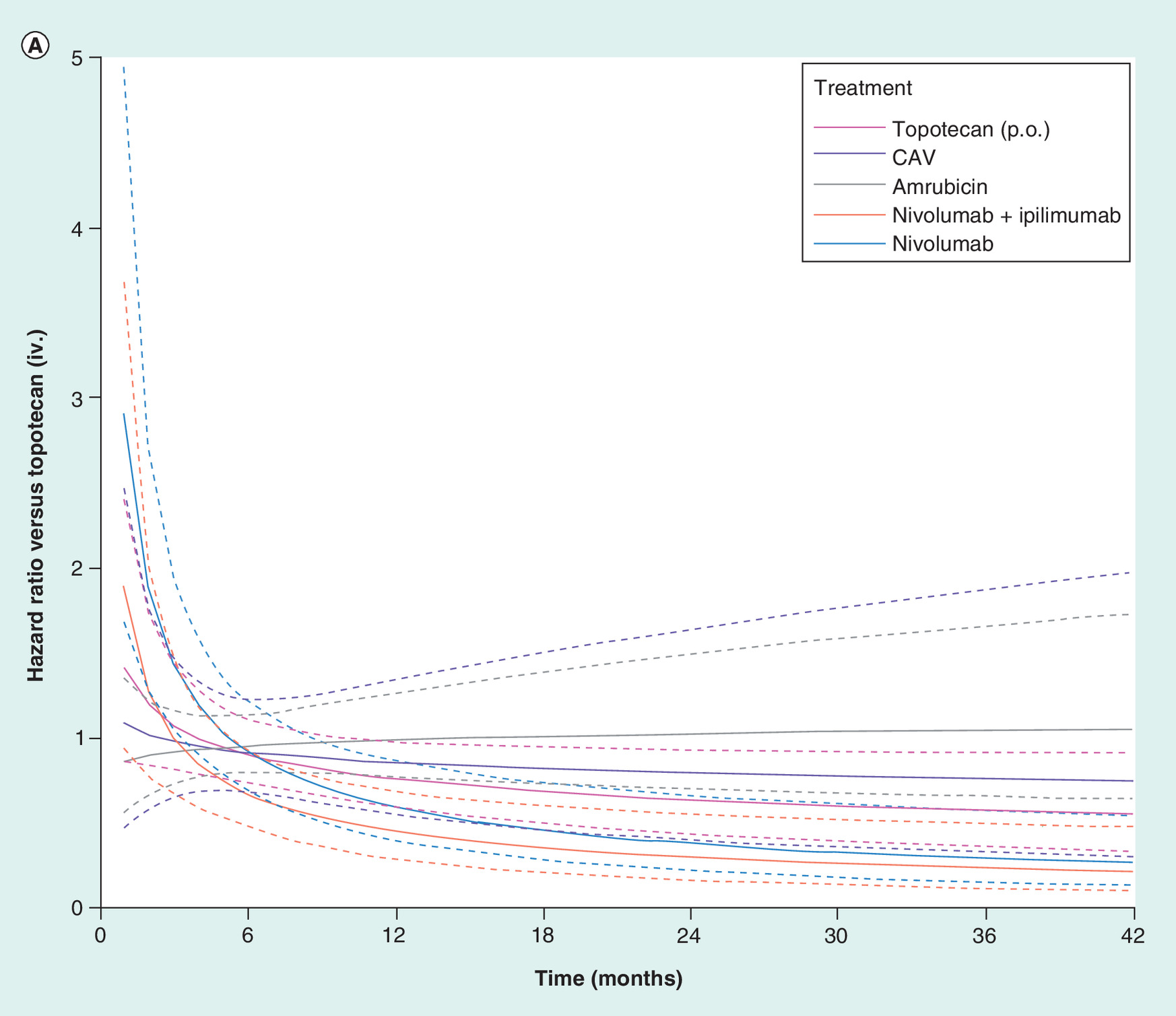
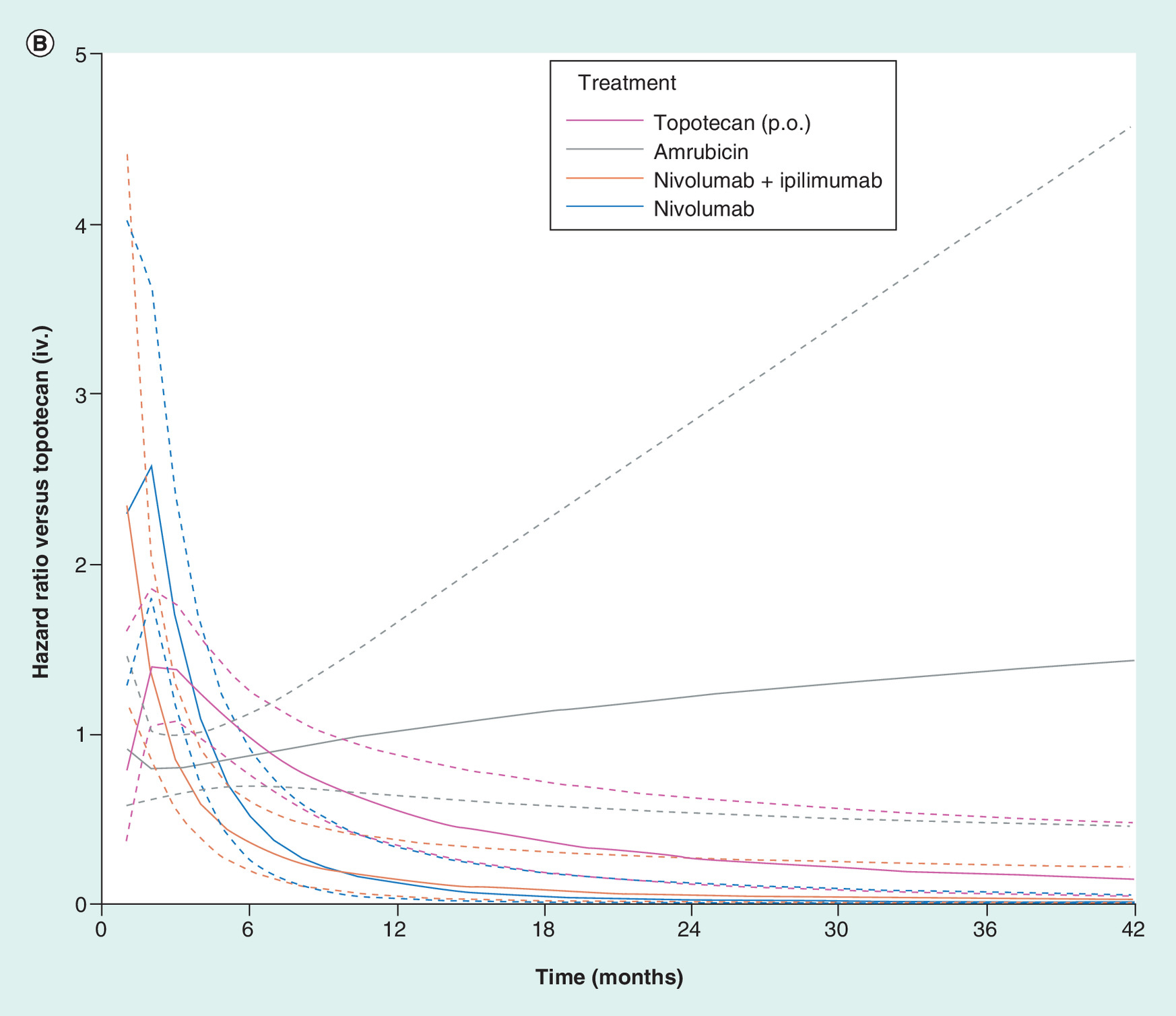
Figure 5. Results from network meta-analysis.
Estimated hazard ratios of each intervention versus intravenous topotecan for overall survival (A) and progression-free survival (B). Models according to second-order fractional polynomial model for overall survival (p1 = 0 and p2 = 1) and progression-free survival (p1 = 0 and p2 = -1).
CAV: Cyclophosphamide + doxorubicin + vincristine; iv.: Intravenous; p.o.: Oral
To facilitate the interpretation of the above results, estimates of the expected survival proportions over time assuming topotecan via iv. as the reference curve are presented in Figure 6, including the proportion of patients alive at 1 and 2 years. In terms of OS, relative to topotecan via iv. or amrubicin, the survival improvement was observed as early as month 6 for nivolumab + ipilimumab and at month 12 for nivolumab. Relative to the chemotherapies, long-term OS results were favorable for both the nivolumab regimens, and improvement in PFS for nivolumab was observed between months 12 and 36 and between 6 and 18 months for nivolumab + ipilimumab. Results were generally consistent when CheckMate 032 was connected to the network using different RCTs that included topotecan via iv. [13–16].
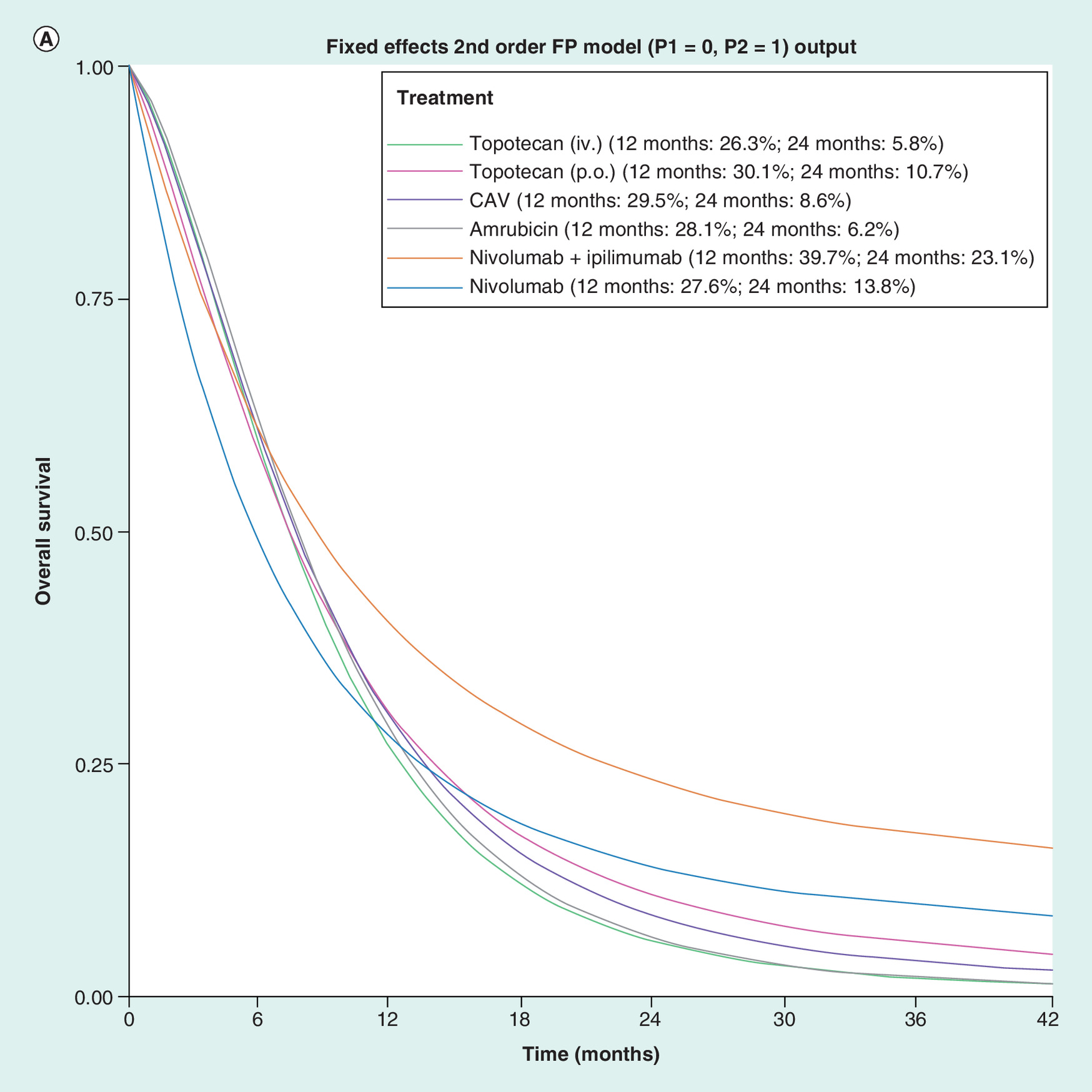
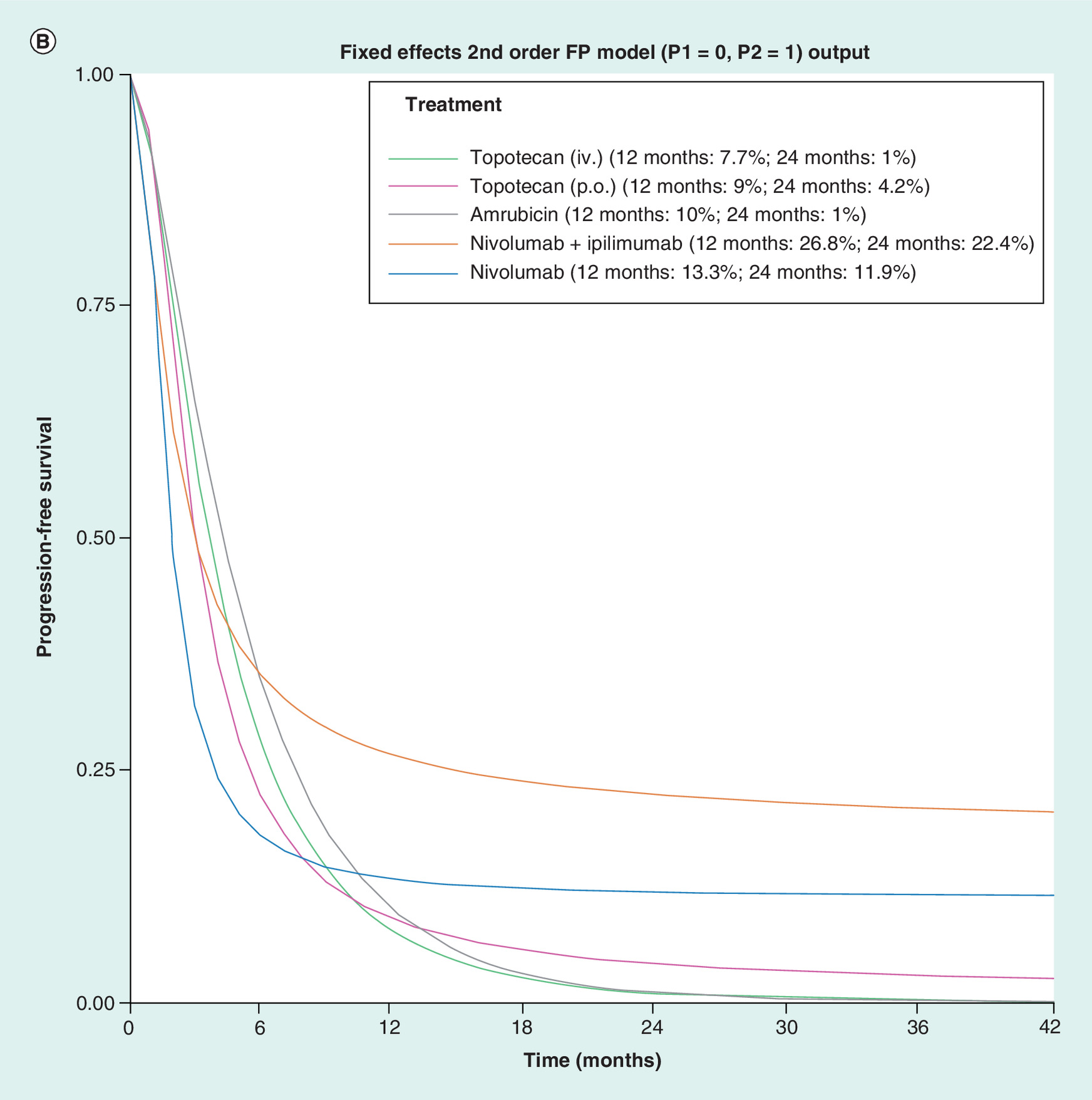
Figure 6. Results from network meta-analysis.
Estimated survival proportions over time for overall survival (A) and progression-free survival (B) assuming intravenous topotecan as the reference curve. Models according to second-order fractional polynomial model for overall survival (p1 = 0 and p2 = 1) and progression-free survival (p1 = 0 and p2 = -1).
CAV: Cyclophosphamide + doxorubicin + vincristine; iv.: Intravenous; p.o.: oral.
ORR & duration of response
Observed ORRs ranged from 10.2% for nivolumab [19–23] to 44.0% for amrubicin [16], whereas the median DOR ranged from 3.2 months for topotecan via iv. [13] to 17.9 months for nivolumab [19–23]. The estimated ORs resulting from the NMA suggest that nivolumab ± ipilimumab did not improve ORR versus any of the chemotherapies, though point estimates did trend in favor of nivolumab + ipilimumab in all comparisons with the exception of amrubicin. However, nivolumab monotherapy and nivolumab + ipilimumab significantly improved the DOR compared with all chemotherapies, except for nivolumab monotherapy versus CAV, which was not statistically significant. Of note, nivolumab ± ipilimumab significantly improved the DOR compared with the current standard of care topotecan via iv. (Figure 7).
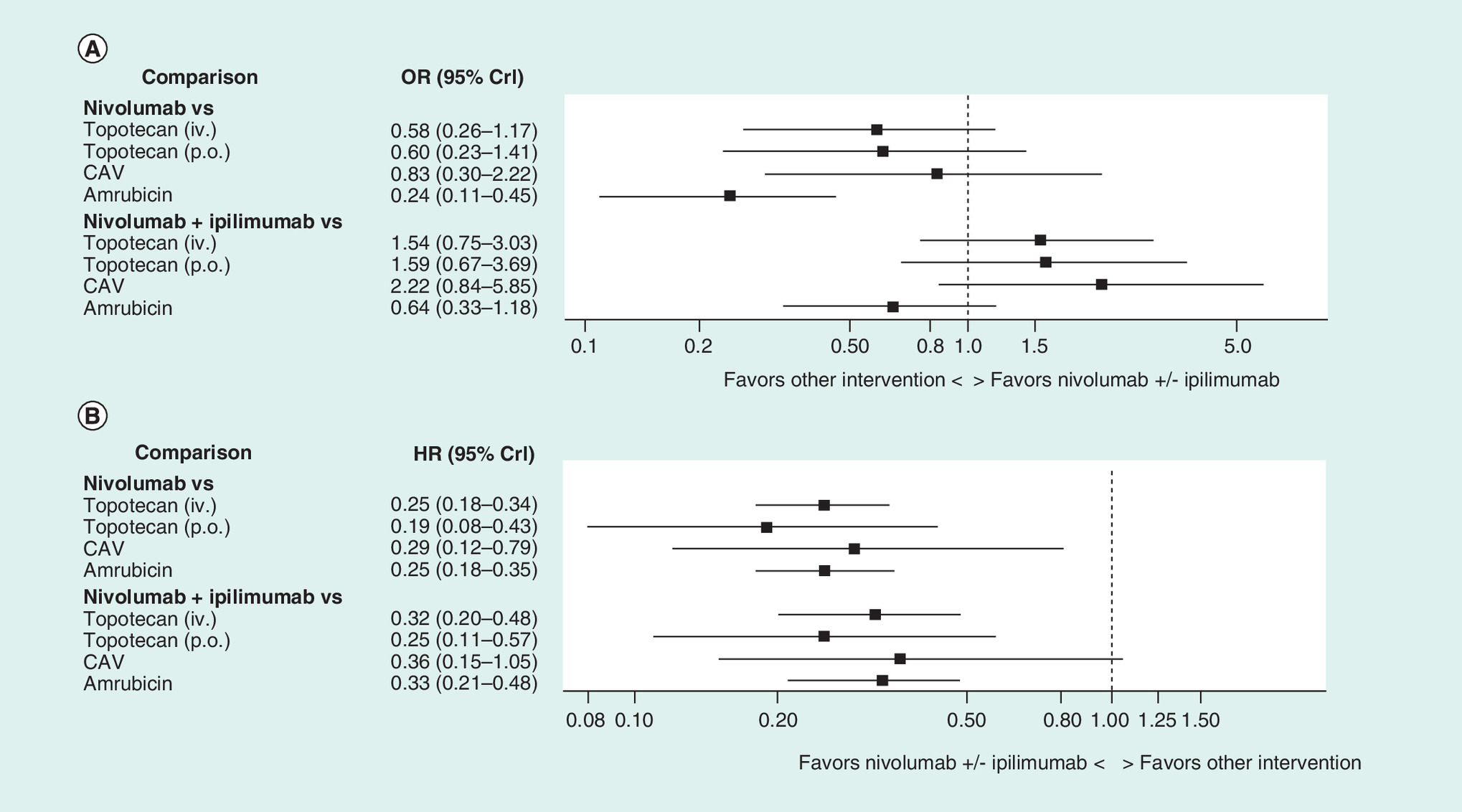
Figure 7. Results from network meta-analysis.
Forest plot of odds ratios of objective response (A) and hazard ratios of duration of response (B) for nivolumab ± ipilimumab versus other interventions.
CAV: Cyclophosphamide + doxorubicin + vincristine; HR: Hazard ratio; iv.: Intravenous; OR: Odds ratio; p.o.: Oral.
Discussion
The overall prognosis for patients with SCLC remains poor, with little improvement in OS since the late seventies, especially for patients with ED [57]. This is despite high initial response rates to 1L treatment with chemotherapy or chemoradiotherapy. The results of this SLR showed that a limited number of RCTs have been conducted in 2L patients, and just two of the identified trials (CheckMate 032 and Pallis et al.) included 3L+ patients. After excluding trials conducted in Asian populations, the network of RCTs comprised of evidence on amrubicin, CAV, oral topotecan and topotecan via iv. It is noteworthy that the network did not include a trial of rechallenge with a platinum-based regimen, as this has been identified as a key comparator of interest. The median OS among the trials in the network ranged from 5.7 to 9.2 months. The results of this analysis confirm that outcomes among this population are poor despite chemotherapy, and there are no differences between agents in terms of survival. This aligns with observational data from the USA, where median OS after 2L therapy, most often with topotecan, was less than 6 months for both platinum-refractory and sensitive patients [18].
The findings underscore the need for new treatments for this population and provide justification for the recent FDA accelerated approval of nivolumab for SCLC and the recommendation of nivolumab ± ipilimumab by the NCCN based on evidence from CheckMate 032. Despite the significant limitations regarding the methodology for aggregate-level matching, initial results suggest that nivolumab ± ipilimumab had a much longer DOR than existing therapies. These benefits may translate to improvements in longer-term OS and PFS, which will be important to evaluate based on longer follow-up. The analysis of survival outcomes further supports this hypothesis, given outcomes were more favorable for nivolumab at later time points. Note that time-varying HRs were used since nivolumab + ipilimumab curves crossed the observed chemotherapy survival curves in several cases, meaning that the proportional hazards assumption was not valid. These results align with expectations given the differences in the mechanism of action for nivolumab, a novel immunotherapy, compared with traditional chemotherapies.
It is important to emphasize that in the absence of randomization, it is not possible to disentangle the treatment effects from the study effects; therefore, relying on single-arm evidence may introduce a significant risk of bias when used as the foundation for estimating relative treatment effects. For example, ACT-1 included only 2L patients, whereas CheckMate 032 included patients with more than one prior line of therapy. Therefore, comparative efficacy estimates for nivolumab may be conservative given the more advanced population included in CheckMate 032. A population-adjusted indirect treatment comparison using IPD from CheckMate 032 would better account for between-study differences in patient characteristics. However, even with IPD, there is a risk of bias due to unmeasured or unknown study-level differences. Furthermore, some between-study differences within the connected network of RCTs may have introduced bias. For example, platinum sensitivity may act as a treatment effect modifier. However, given the limited number of studies it was not feasible to adjust for differences across studies.
Given the high-unmet need in SCLC, results from this study can help inform decision-makers of the potential benefit from nivolumab + ipilimumab until results from other trials become available. There are currently several ongoing trials investigating immunotherapies in SCLC. CheckMate 331 is a randomized, open-label, Phase III trial comparing nivolumab monotherapy versus topotecan/amrubicin in patients with progression during or after platinum-based 1L chemotherapy or chemoradiation. Although this trial failed to meet its primary end point of OS [58], an investigation of potential patient subgroups that may benefit from nivolumab, such as those with elevated PD-L1 expression or high tumor mutation burden (TMB), is ongoing.
A treatment approach using immunotherapy in the 1L and 1L maintenance settings, rather than only in the 2L setting, is a promising option to increase the proportion of patients showing a clinical response. In the 1L setting, IMpower133 is a randomized, double-blind, Phase III trial of carboplatin and etoposide with either atezolizumab or placebo in SCLC ED patients who had not previously received treatment [59]. Interim results show that the addition of atezolizumab to chemotherapy results in significantly longer OS and PFS compared with chemotherapy alone [59]. Other Phase III randomized trials in SCLC ED patients in the 1L setting that do not yet have results available include KEYNOTE-604, a double-blind trial of cisplatin/carboplatin and etoposide in combination with pembrolizumab or placebo, and CASPIAN, an open-label trial of cisplatin/carboplatin and etoposide in combination with durvalumab with or without tremelimumab. In the 1L maintenance setting, CheckMate 451 is a randomized, double-blind, Phase III trial of nivolumab ± ipilimumab versus placebo for ED patients who have either an ongoing CR, PR or SD after completion of four cycles of platinum-based 1L chemotherapy [60]. However, this trial failed to meet its primary end point, though as with CheckMate 331 subgroup analyses are ongoing.
Evidence from these ongoing trials may provide insight into the optimal approach to target therapies. Although PD-L1 expression is a useful biomarker in non-small-cell lung cancer, tumor PD-L1 expression is uncommon in SCLC and has not shown correlation with efficacy parameters [19], so an alternative biomarker may be required. The majority of SCLC patients are current or former smokers, and these patients tend to have a high TMB. An exploratory analysis of CheckMate 032, as well as other studies in non-small-cell lung cancer, urothelial carcinoma and melanoma, have shown an association between high TMB and improved clinical outcomes in patients receiving immunotherapies, suggesting that TMB may be a relevant biomarker in SCLC [23,61–64]. The addition of a CTLA-4 inhibitor, such as ipilimumab, to immunotherapy may further improve the response in SCLC patients with high TMB due to the synergistic effect of these treatments [23,65]. However, an exploratory analysis in IMpower133 of survival according to TMB, using a blood-based assay to measure TMB, did not identify an association [59]. Therefore, further research into the best biomarkers and treatment combinations is required to increase the proportion of SCLC patients who benefit from treatment.
Conclusion
In conclusion, based on data from the nonrandomized cohort in CheckMate 032 to estimate the comparative efficacy of nivolumab ± ipilimumab versus alternative treatments for SCLC after at least one prior line of chemotherapy, results of the indirect comparison suggest nivolumab ± ipilimumab improved response duration and was associated with favorable OS estimates compared with existing chemotherapies. Therefore, nivolumab ± ipilimumab may provide an immuno-oncology treatment option for SCLC patients who have received prior treatment.
Future perspective
It is anticipated that in 5–10 years the role of immuno-oncology for SCLC patients will be established, based on anticipated results from ongoing trials. Moreover, it is expected that additional data from these trials may help to identify additional biomarkers to select for SCLC patients who may benefit from targeted molecular therapies. These trials may also help to elucidate the role of TMB, which may help to better target the optimal treatments for this difficult to treat population. Ultimately, patients who respond to immuno-oncology treatments may experience sustained benefits in terms of improved survival compared with chemotherapy alone.
Background
•
The majority of patients with small-cell lung cancer (SCLC) are sensitive to first-line chemotherapy; however, for patients with disease progression/recurrence, topotecan is the only approved therapy in the second-line (2L) setting, with no approved third-line (3L) therapies.
•
National Comprehensive Cancer Network guidelines now recommend nivolumab ± ipilimumab for SCLC patients who have failed prior systemic therapy within 6 months in either the primary or adjuvant setting based on results from a nonrandomized cohort from CheckMate 032, Phase I/II trial. Pembrolizumab was recently added to the National Comprehensive Cancer Network guidelines following results of the KEYNOTE-158 trial and is also recommended for SCLC patients who relapse within 6 months.
•
More recently, the US FDA granted an accelerated approval for nivolumab as the first and only immuno-oncology treatment option for patients with metastatic SCLC whose cancer has progressed after platinum-based chemotherapy and at least one other line of therapy.
•
A standard approach to obtain relative treatment effects between the competing interventions not directly compared is based on a network meta-analysis (NMA) of randomized controlled trials (RCTs) as identified through a systematic literature review.
•
Given that the preexpansion cohort of CheckMate 032 was not randomized, we used matching based on aggregate study-level data to evaluate the comparative efficacy of nivolumab ± ipilimumab versus alternative treatments for SCLC after at least one prior line of chemotherapy (2L/3L).
Methods
Systematic literature review
•
A systematic literature review was performed (June 2018) including searches of EMBASE, MEDLINE and Cochrane Central Registry of Controlled Trials, published ≥1990, along with relevant conferences.
•
The quality of individual trials was assessed using the Risk of Bias instrument endorsed by the Cochrane Collaboration.
Network meta-analysis
•
Relative treatment effects regarding overall survival (OS), progression-free survival (PFS), objective response rate (ORR) and duration of response (DOR) were estimated for the alternative interventions in 2L/3L treatment of advanced SCLC based on the available RCTs using NMA models.
•
To facilitate a comparison of nivolumab ± ipilimumab based on study-level results from the nonrandomized cohort of CheckMate 032 with the other interventions, we linked CheckMate 032 to the RCT that best-matched in terms of study design, inclusion criteria and patient characteristics (‘aggregate-level matching’).
•
ACT-1 (amrubicin versus topotecan via intravenous [iv.] administration) was identified as the best matching trial. Therefore, in the base case, CheckMate 032 arms were treated as arms of ACT-1 within the analysis, which assumed that the outcomes in the control arm of ACT-1 were applicable to CheckMate 032.
•
For survival, fractional polynomial models were used to model the log hazard functions of the interventions in a trial. The differences in the parameters were considered the multidimensional treatment effect, which were pooled and indirectly compared across studies. For the median DOR and number of patients at risk, a binomial likelihood and cloglog link (with offset for median) were used. For ORRs, the NMA was performed based on the proportion of patients experiencing the event of interest using a regression model with a binomial likelihood and logit link.
Results
Systematic literature review
•
A total of 19 individual clinical trials were identified through the database, conference and hand searches for the NMA: 18 RCTs and one non-RCT (CheckMate 032 was included as the reference population) of 2L/3L treatments (from 35 citations).
Network meta-analysis
•
In terms of OS, relative to topotecan via iv. or amrubicin, the survival improvement was observed as early as month 6 for nivolumab ± ipilimumab and month 12 for nivolumab. Relative to other chemotherapies, long-term OS results favored nivolumab ± ipilimumab.
•
Relative to other chemotherapies, the improvement in PFS for nivolumab was observed between months 12 and 36 and for nivolumab + ipilimumab between 6 and 18 months.
•
Though no meaningful differences were observed between treatments in terms of ORR, nivolumab as monotherapy and nivolumab + ipilimumab significantly improved the duration of response compared with all chemotherapies, especially compared with the current standard of care, topotecan via iv.
Conclusion
•
SCLC patients who have received at least one prior line of chemotherapy have poor outcomes despite additional treatment with chemotherapy in the second-line context, and survival is similar with different agents. These results align with observational data from the USA, where median OS after 2L therapy, most often with topotecan, was less than 6 months for both platinum-refractory and sensitive patients.
•
Results suggest nivolumab ± ipilimumab responders had a much longer DOR compared with existing therapies. These benefits may translate to improvements in longer-term OS and PFS, which will be important to evaluate based on longer follow-up.
Supplementary data
To view the supplementary data that accompany this paper please visit the journal website at: Supplementary Material
Acknowledgments
The authors acknowledge the statistical analysis support by Melissa Barazandegan and Evan Popoff, as well as writing/editorial support from Florence R Wilson.
Financial & competing interests disclosure
This study was funded by Bristol-Myers Squibb. JR Penrod, B Korytowsky, A Juarez-Garcia, and Y Yuan are employees of Bristol-Myers Squibb. S Cope, S Keeping, D Ayers, and JP Jansen are employees of Precision Xtract. R Goldgrub was an employee of Precision Xtract at the time the manuscript was submitted. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing assistance was utilized in the production of this manuscript. Precision Xtract, funded by Bristol-Myers Squibb, provided professional editorial assistance.
Supplementary Material
File (supplementarymaterial.docx)
- Download
- 368.56 KB
References
1.
Byers LA, Rudin CM. Small cell lung cancer: where do we go from here? Cancer 121(5), 664–672 (2015).
2.
Van Meerbeeck JP, Fennell DA, De Ruysscher DK. Small-cell lung cancer. Lancet 378(9804), 1741–1755 (2011).
3.
Früh M, De Ruysscher D, Popat S, Crino L, Peters S, Felip E. Small-cell lung cancer (SCLC): ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 24(Suppl. 6), vi99–vi105 (2013).
4.
Rudin CM, Ismaila N, Hann CL et al. Treatment of small-cell lung cancer: American Society of Clinical Oncology endorsement of the American College of Chest Physicians Guideline. J. Clin. Oncol. 33(34), 4106–4111 (2015).
5.
Micke P, Faldum A, Metz T et al. Staging small cell lung cancer: Veterans Administration Lung Study Group versus International Association for the Study of Lung Cancer – what limits limited disease? Lung Cancer 37(3), 271–276 (2002).
6.
Turrisi AT 3rd, Kim K, Blum R et al. Twice-daily compared with once-daily thoracic radiotherapy in limited small-cell lung cancer treated concurrently with cisplatin and etoposide. N. Engl. J. Med. 340(4), 265–271 (1999).
7.
Chan BA, Coward JI. Chemotherapy advances in small-cell lung cancer. J. Thorac. Dis. 5(Suppl. 5), S565–S578 (2013).
8.
Simon GR, Turrisi A. Management of small cell lung cancer: ACCP evidence-based clinical practice guidelines (2nd edition). Chest 132(3 Suppl.), 324S–339S (2007).
9.
Hurwitz JL, McCoy F, Scullin P, Fennell DA. New advances in the second-line treatment of small cell lung cancer. Oncologist 14(10), 986–994 (2009).
10.
National Comprehensive Cancer Network. Small cell lung cancer (Version 1.2019) (2018). www.nccn.org/professionals/physician_gls/pdf/sclc_blocks.pdf
11.
Waqar SN, Morgensztern D. Treatment advances in small cell lung cancer (SCLC). Pharmacol. Ther. 180, 16–23 (2017).
12.
O'Brien ME, Ciuleanu TE, Tsekov H et al. Phase III trial comparing supportive care alone with supportive care with oral topotecan in patients with relapsed small-cell lung cancer. J. Clin. Oncol. 24(34), 5441–5447 (2006).
13.
Von Pawel J, Gatzemeier U, Pujol JL et al. Phase II comparator study of oral versus intravenous topotecan in patients with chemosensitive small-cell lung cancer. J. Clin. Oncol. 19(6), 1743–1749 (2001).
14.
Eckardt JR, Von Pawel J, Pujol JL et al. Phase III study of oral compared with intravenous topotecan as second-line therapy in small-cell lung cancer. J. Clin. Oncol. 25(15), 2086–2092 (2007).
15.
Von Pawel J, Jotte R, Spigel DR et al. Randomized Phase III trial of amrubicin versus topotecan as second-line treatment for patients with small-cell lung cancer. J. Clin. Oncol. 32(35), 4012–4019 (2014).
16.
Jotte R, Conkling P, Reynolds C et al. Randomized Phase II trial of single-agent amrubicin or topotecan as second-line treatment in patients with small-cell lung cancer sensitive to first-line platinum-based chemotherapy. J. Clin. Oncol. 29(3), 287–293 (2011).
17.
Von Pawel J, Schiller JH, Shepherd FA et al. Topotecan versus cyclophosphamide, doxorubicin, and vincristine for the treatment of recurrent small-cell lung cancer. J. Clin. Oncol. 17(2), 658–667 (1999).
18.
Danese M, Gleeson M, Lubeck D, Penrod J, Korytowsky B, Yuan Y. P1.15-003 Survival by response to first-line platinum-based therapy among patients with extensive disease small cell lung cancer. J. Thorac. Oncol. 12(11), S2044 (2017).
19.
Antonia SJ, Lopez-Martin JA, Bendell J et al. Nivolumab alone and nivolumab plus ipilimumab in recurrent small-cell lung cancer (CheckMate 032): a multicentre, open-label, Phase 1/2 trial. Lancet Oncol. 17(7), 883–895 (2016).
20.
Taylor M, Antonia S, Bendell J et al. Phase I/II study of nivolumab with or without ipilimumab for treatment of recurrent small cell lung cancer (SCLC): CA209–032. J. Immunother. Cancer 3(Suppl. 2), P376 (2015).
21.
Antonia SJ, Lopez-Martin JA, Bendell JC et al. Checkmate 032: Nivolumab (N) alone or in combination with ipilimumab (I) for the treatment of recurrent small cell lung cancer (SCLC). J. Clin. Oncol. 34(15 Suppl.), 100–100 (2016).
22.
Hellmann M, Ott PA, Zugazagoitia J et al. Nivolumab±ipilimumab in advanced small cell lung cancer: first report of a randomized cohort from CheckMate 032. Presented at: ASCO Annual Meeting. IL, USA, 2–6 June 2017.
23.
Hellmann MD, Callahan MK, Awad MM et al. Tumor mutational burden and efficacy of nivolumab monotherapy and in combination with ipilimumab in small-cell lung cancer. Cancer Cell 33(5), 853–861.e4 (2018).
24.
Opdivo Prescribing Information. Opdivo US Product Information. Bristol-Myers Squibb Company, NJ, USA (2018).
25.
Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. J. Clin. Epidemiol. 62(10), 1006–1012 (2009).
26.
Dias S, Welton NJ, Sutton AJ, Caldwell DM, Lu G, Ades AE. Evidence synthesis for decision making 4: inconsistency in networks of evidence based on randomized controlled trials. Med. Decis. Making 33(5), 641–656 (2013).
27.
Jansen JP. Network meta-analysis of survival data with fractional polynomials. BMC Med. Res. Methodol. 11, 61 (2011).
28.
Lu G, Ades AE. Combination of direct and indirect evidence in mixed treatment comparisons. Stat. Med. 23(20), 3105–3124 (2004).
29.
Mills EJ, Ioannidis JP, Thorlund K, Schunemann HJ, Puhan MA, Guyatt GH. How to use an article reporting a multiple treatment comparison meta-analysis. JAMA 308(12), 1246–1253 (2012).
30.
Jansen JP, Naci H. Is network meta-analysis as valid as standard pairwise meta-analysis? It all depends on the distribution of effect modifiers. BMC Med. 11, 159 (2013).
31.
Phillippo DM, Ades AE, Dias S, Palmer S, Abrams KR, Welton KJ. NICE DSU Technical support document 18: methods for population-adjusted indirect comparisons in submissions to NICE (2016). https://scharr.dept.shef.ac.uk/nicedsu/wp-content/uploads/sites/7/2017/05/Population-adjustment-TSD-FINAL.pdf
32.
Ouwens MJNM, Philips Z, Jansen JP. Network meta-analysis of parametric survival curves. Res. Synth. Methods 1(3–4), 258–271 (2011).
33.
Jansen JP, Cope S. Meta-regression models to address heterogeneity and inconsistency in network meta-analysis of survival outcomes. BMC Med. Res. Methodol. 12(1), 152–152 (2012).
34.
Woods BS, Hawkins N, Scott DA. Network meta-analysis on the log-hazard scale, combining count and hazard ratio statistics accounting for multi-arm trials: a tutorial. BMC Med. Res. Methodol. 10, 54 (2010).
35.
Spiegelhalter D, Thomas A, Best N, Lunn D. WinBUGS user manual version 1.4. (2003). www.mrc-bsu.cam.ac.uk/wp-content/uploads/manual14.pdf
36.
Lunn D, Spiegelhalter D, Thomas A, Best N. The BUGS project: evolution, critique and future directions. Statist. Med. 28, 3049–3067 (2009).
37.
Evans TL, Cho BC, Udud K et al. Cabazitaxel versus topotecan in patients with small-cell lung cancer with progressive disease during or after first-line platinum-based chemotherapy. J. Thorac. Oncol. 10(8), 1221–1228 (2015).
38.
Evans T, Cho BC, Udud K et al. Cabazitaxel (Cbz) Vs topotecan (Tpt) in patients (Pts) with small cell lung cancer (SCLC) with progressive disease during/after first-line (1l) treatment with platinum-based chemotherapy (Ctx). Presented at: European Lung Cancer Conference 2014. Geneva, Switzerland, 26–29 March 2014.
39.
Clinical Trials Database: NCT01500720. https://clinicaltrials.gov/ct2/show/NCT01500720?term=NCT01500720&rank=1
40.
Chiappori AA, Otterson GA, Dowlati A et al. A randomized Phase II study of linsitinib (OSI-906) versus topotecan in patients with relapsed small-cell lung cancer. Oncologist 21(10), 1163–1164 (2016).
41.
Gervais R, Le Caer H, Monnet I et al. Second-line oral chemotherapy (lomustine, cyclophosphamide, etoposide) versus intravenous therapy (cyclophosphamide, doxorubicin, and vincristine) in patients with relapsed small cell lung cancer: a randomized Phase II study of GFPC 0501. Clin. Lung Cancer 16(2), 100–105 (2015).
42.
Goto K, Ohe Y, Shibata T et al. Combined chemotherapy with cisplatin, etoposide, and irinotecan versus topotecan alone as second-line treatment for patients with sensitive relapsed small-cell lung cancer (JCOG0605): a multicentre, open-label, randomised Phase 3 trial. Lancet Oncol. 17(8), 1147–1157 (2016).
43.
Seto T, Goto K, Takahashi T et al. O1-21-6A Phase III study of CDDP, ETOP and irinotecan vs, topotecan as 2nd-line chemotherapy for sensitive relaspsed SCLC: JCOG0605. Ann. Oncol. 25(Suppl. 5), v56–v57 (2014).
44.
Inoue A, Sugawara S, Yamazaki K et al. Randomized Phase II trial comparing amrubicin with topotecan in patients with previously treated small-cell lung cancer: North Japan Lung Cancer Study Group Trial 0402. J. Clin. Oncol. 26(33), 5401–5406 (2008).
45.
Nakamura A, Inoue A, Maemondo M et al. Randomized Phase 2 trial comparing amrubicin (A) with re-challenge of platinum doublet (P) in patients (pts) with sensitive-relapsed small-cell lung cancer (SCLC). J. Clin. Oncol. 32(15 Suppl.), 7520–7520 (2014).
46.
Inoue A, Sugawara S, Maemondo M et al. Randomized Phase II trial comparing amrubicin with re-challenge of platinum doublet in patients with sensitive-relapsed small-cell lung cancer: North Japan Lung Cancer Study Group trial 0702. Lung Cancer 89(1), 61–65 (2015).
47.
Chen L, Antras L, Duh MS, Neary M, O'Brien MER. Symptom assessment in relapsed small cell lung cancer: cross-validation of the patient symptom assessment in lung cancer instrument. J. Thorac. Oncol. 3(10), 1137–1145 (2008).
48.
O'Bryan RM, Crowley JJ, Kim PN et al. Comparison of etoposide and cisplatin with bis-chloro-ethylnitrosourea, thiotepa, vincristine, and cyclophosphamide for salvage treatment in small cell lung cancer. A Southwest Oncology Group Study. Cancer 65(4), 856–860 (1990).
49.
Pallis AG, Agelidou A, Agelaki S et al. A multicenter randomized Phase II study of the irinotecan/gemcitabine doublet versus irinotecan monotherapy in previously treated patients with extensive stage small-cell lung cancer. Lung Cancer 65(2), 187–191 (2009).
50.
Sculier JP, Lafitte JJ, Lecomte J et al. A Phase II randomised trial comparing the cisplatin–etoposide combination chemotherapy with or without carboplatin as second-line therapy for small-cell lung cancer. Ann. Oncol. 13(9), 1454–1459 (2002).
51.
Sekine CI, Harada H, Yamamoto N et al. Randomized Phase II trial of code or amrubicin plus cisplatin chemotherapy after chemoradiotherapy for limited-disease small cell lung. J. Thorac. Dis. 2, S400 (2015).
52.
Allen JW, Moon J, Redman M et al. Southwest Oncology Group S0802: a randomized, Phase II trial of weekly topotecan with and without ziv-aflibercept in patients with platinum-treated small-cell lung cancer. J. Clin. Oncol. 32(23), 2463–2470 (2014).
53.
Clinical Trials Database: NCT00828139. https://clinicaltrials.gov/ct2/show/NCT00828139?term=NCT00828139&rank=1
54.
Chen L, Antras L, Mei SD et al. Psychometric validation of the patient symptom assessment in lung cancer instrument for small cell lung cancer. Curr. Med. Res. Opin. 23(11), 2741–2752 (2007).
55.
Yoon S, Lee DH, Choi CM, Lee JC, Lee JS, Kim SW. Randomized Phase II study of belotecan or topotecan as second-line chemotherapy after platinum based chemotherapy for small cell lung cancer. J. Thorac. Dis. 2, S787–S788 (2015).
56.
Loveman E, Jones J, Hartwell D et al. The clinical effectiveness and cost–effectiveness of topotecan for small cell lung cancer: a systematic review and economic evaluation. Health Technol. Assess. 14(19), 1–204 (2010).
57.
Navada S, Lai P, Schwartz AG, Kalemkerian GP. Temporal trends in small cell lung cancer: analysis of the national Surveillance, Epidemiology, and End-Results (SEER) database. J. Clin. Oncol. 24(18 Suppl.), 7082–7082 (2006).
58.
Source: Bristol-Myers Squibb. Bristol-Myers Squibb announces Phase 3 CheckMate -331 study does not meet primary endpoint of overall survival with Opdivo versus chemotherapy in patients with previously treated relapsed small cell lung cancer. Press release: https://news.bms.com/press-release/corporatefinancial-news/bristol-myers-squibb-announces-phase-3-checkmate-331-study-doe
59.
Horn L, Mansfield AS, Szczęsna A et al. First-line atezolizumab plus chemotherapy in extensive-stage small-cell lung cancer. N. Engl. J. Med. 379(23), 2220–2229 (2018).
60.
Clinical Trialss Database: NCT02538666. https://clinicaltrials.gov/ct2/show/NCT02538666
61.
Hellmann MD, Nathanson T, Rizvi H et al. Genomic features of response to combination immunotherapy in patients with advanced non-small-cell lung cancer. Cancer Cell 33(5), 843–852 e844 (2018).
62.
Carbone DP, Reck M, Paz-Ares L et al. First-line nivolumab in stage IV or recurrent non-small-cell lung cancer. N. Engl. J. Med. 376(25), 2415–2426 (2017).
63.
Galsky MD, Saci A, Szabo PM et al. Impact of tumor mutation burden on nivolumab efficacy in second-line urothelial carcinoma patients: exploratory analysis of the Phase II CheckMate 275 study, [abstract 848PD]. Ann. Oncol. 28(Suppl. 5), v295–v329 (2017).
64.
Snyder A, Makarov V, Merghoub T et al. Genetic basis for clinical response to CTLA-4 blockade in melanoma. N. Engl. J. Med. 371(23), 2189–2199 (2014).
65.
Boumber Y. Tumor mutational burden (TMB) as a biomarker of response to immunotherapy in small cell lung cancer. J. Thorac. Dis. 10(8), 4689–4693 (2018).
Information & Authors
Information
Published In
Pages: 733 - 751
PubMed: 31237143
Copyright
© 2019 Future Medicine Ltd.
History
Received: 3 December 2018
Accepted: 7 May 2019
Published online: 25 June 2019
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Indirect comparison of nivolumab ± ipilimumab (CheckMate 032) versus other treatments for recurrent small-cell lung cancer. (2019) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2018-0130
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Luis Guilherme de Oliveira Silva, Fabian Fellipe Bueno Lemos, Marcel Silva Luz, Samuel Luca Rocha Pinheiro, Mariana dos Santos Calmon, Gabriel Lima Correa Santos, Gabriel Reis Rocha, Fabrício Freire de Melo, New avenues for the treatment of immunotherapy-resistant pancreatic cancer, World Journal of Gastrointestinal Oncology, 10.4251/wjgo.v16.i4.1134, 16, 4, (1134-1153), (2024).
- Julie E. Park, Harlan Campbell, Kevin Towle, Yong Yuan, Jeroen P. Jansen, David Phillippo, Shannon Cope, Unanchored Population-Adjusted Indirect Comparison Methods for Time-to-Event Outcomes Using Inverse Odds Weighting, Regression Adjustment, and Doubly Robust Methods With Either Individual Patient or Aggregate Data, Value in Health, 10.1016/j.jval.2023.11.011, 27, 3, (278-286), (2024).
- Song Zhang, Small Cell Lung Carcinoma, Diagnostic Imaging of Lung Cancers, 10.1007/978-981-99-6815-2_3, (65-78), (2024).
- Cinzia Vetrei, Margherita Passariello, Guendalina Froechlich, Rosa Rapuano Lembo, Nicola Zambrano, Claudia De Lorenzo, Immunomodulatory mAbs as Tools to Investigate on Cis-Interaction of PD-1/PD-L1 on Tumor Cells and to Set Up Methods for Early Screening of Safe and Potent Combinatorial Treatments, Cancers, 10.3390/cancers13122858, 13, 12, (2858), (2021).
- Sam T Keeping, Shannon Cope, Keith Chan, Florence R Wilson, Jeroen P Jansen, John R Penrod, Pranav Abraham, D Ross Camidge, Beata Korytowsky, Tao Gu, Ariadna Juarez Garcia, Trong K Le, Yong Yuan, Comparative effectiveness of nivolumab versus standard of care for third-line patients with small-cell lung cancer, Journal of Comparative Effectiveness Research, 10.2217/cer-2020-0134, 9, 18, (1275-1284), (2020).
- Venu Madhav Konala, Bhaskar Reddy Madhira, Sara Ashraf, Stephen Graziano, Use of Immunotherapy in Extensive-Stage Small Cell Lung Cancer, Oncology, 10.1159/000508516, 98, 11, (749-754), (2020).
- Jingjie Chen, Shengnan Li, Qigu Yao, Nannan Du, Xiaojun Fu, Yuanmei Lou, Mengru Wang, Feiyan Mao, Danyi Mao, Parikshit Asutosh Khadaroo, Yingying Tang, The efficacy and safety of combined immune checkpoint inhibitors (nivolumab plus ipilimumab): a systematic review and meta-analysis, World Journal of Surgical Oncology, 10.1186/s12957-020-01933-5, 18, 1, (2020).