Evolution of functional class, biochemical and echocardiographic parameters and clinical outcomes after sacubitril/valsartan initiation in daily practice
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To analyze the impact of sacubitril/valsartan on functional class, surrogate parameters and clinical outcomes in clinical practice. Methods: Retrospective study of patients with heart failure and reduced ejection fraction that started treatment with sacubitril/valsartan. Results: 149 patients (70.7 ± 9.6 years) were included. At baseline, 83.9, 15.4 and 0.7% were taking sacubitril/valsartan 24/26, 49/51 and 97/103 mg, respectively. After 316.1 ± 155.9 days, these numbers moved to 38.9, 39.6, 12.8% (8.7% discontinued). Sacubitril/valsartan improved functional class (from 2.3 ± 0.6 to 1.8 ± 0.5; p < 0.001), increased ejection fraction (from 31.2 ± 7.0 to 37.3 ± 10.5%; p < 0.001) and reduced NT-proBNP (from 3884 ± 4871 to 1975.3 ± 3006.6 pg/ml; p = 0.0001). Rates of any event, cardiovascular death and heart failure hospitalization/decompensation were 13.2 events/100 patient-years. Conclusion: Sacubitril/valsartan is effective and safe in routine practice.
Heart failure (HF) is associated with significant morbidity and mortality [1,2]. Thus, after hospital admission for acute decompensated HF, rates of readmission are as high as 30% and 50% at 1 and 6 months, respectively, after the acute event, and, in this context, 1-year all-cause mortality reaches 30% [3,4]. In addition, healthcare costs associated with HF are very high, being HF hospitalizations the main responsible [5]. Despite the use of traditional guideline-directed medical therapies, including angiotensin-converting enzyme inhibitors (angiotensin receptor blockers if not tolerated), beta-adrenergic blockers and mineralocorticoid receptor antagonists, mortality rates for HF patients remain unacceptably high [6].
The PARADIGM-HF trial showed among 8442 patients with symptomatic HF and an ejection fraction ≤40% that compared with enalapril, sacubitril/valsartan significantly reduced the risk of the composite of death from cardiovascular causes or hospitalization for HF, death from any cause and significantly improved functional class [7]. Despite the information of the pivotal PARADIGM-HF trial translated into a modification of clinical guidelines [8], the fact is that patients included in this study were selected according to strict inclusion/exclusion criteria, limiting the generalization of the results to the overall HF population [9–11]. As a result, observational studies performed in clinical practice are mandatory to confirm whether the effectiveness and safety of sacubitril/valsartan in ‘real-life’ patients are consistent with those of the PARADIGM-HF trial [12–14].
In the last years, a number of small studies that have analyzed the clinical profile of patients using sacubitril/valsartan in routine practice have been published [15–22]. However, the information about the impact of sacubitril/valsartan on functional class, surrogate variables and cardiovascular outcomes in ‘real-life’ patients is very scarce [16,19,20,22] and more information is needed.
The aim of this study was to analyze the clinical profile, and the impact of the use of sacubitril/valsartan on functional class, biochemical and echocardiographic parameters, safety and clinical outcomes among patients with systolic HF attended in a provincial hospital in clinical practice.
Methods
This was a retrospective and unicenter real-life study that included all patients with HF and left ventricular ejection fraction less than 40% taking sacubitril/valsartan (at least one dose) in the hospital of Denia, Alicante, Spain. Patients without complete data, inappropriate indication of prescription (i.e., preserved left ventricular ejection fraction), or withdrawal of the drug during the first 2 months without a clear reason were excluded. This study was approved by the Clinical Research Ethics Committee of the hospital.
Clinical data were collected from the medical history of the patients and during the physician interview at baseline and during follow-up visits. There was not a specific protocol, and patients were managed according to the clinical situation of the patients and physicians’ judgment.
At baseline, biodemographic data (age and sex), physical examination (blood pressure, heart rate and bodyweight), cardiovascular risk factors (hypertension, diabetes, dyslipidemia, smoking and alcoholism), concomitant conditions (history of myocardial infarction, stroke, atrial fibrillation and new-onset atrial fibrillation during the follow-up), the cause of HF, NYHA functional class and hospitalization or admission to the emergency department for HF in the previous year were recorded. Treatment for HF was also documented. Data from blood analysis (closest to the moment of starting treatment with sacubitril/valsartan, and during the follow-up) were recorded. Blood analysis included serum creatinine, urea, sodium, potassium, transaminases, glucose, HbA1c, hemoglobin, platelets count, NT-proBNP, CA 125, ferritin, transferrin saturation, serum iron and uric acid. Data from the echocardiogram (closest to the moment of starting treatment with sacubitril/valsartan and during the follow-up) that included left ventricular end-diastolic diameter, left ventricular ejection fraction, systolic pulmonary artery pressure and the presence of mitral insufficiency and its severity were also determined. All these data were analyzed in the overall study population, and according to the physician that attended the patient (HF unit vs other clinical settings) and the initial dose prescribed of sacubitril/valsartan.
The initial and the final doses of sacubitril/valsartan were recorded in the overall study population and according to the physician that started treatment with this drug. The reasons for prescribing sacubitril/valsartan 24/26 mg at baseline were specifically analyzed.
The evolution of functional class, physical examination, treatment with diuretics, biochemical and echocardiographic parameters during the study according to the physician that started treatment with sacubitril/valsartan and the final dose prescribed of the drug was analyzed.
Due to the retrospective nature of the study, measurements were taken in different time points. However, in order to standardize as much as possible data collection, three different time points were considered: baseline: last measurement of every single variable collected in the six previous months before sacubitril/valsartan initiation, regardless of whether it was carried out during the hospitalization or in an outpatient basis, and regardless the clinical setting (general cardiology, HF unit, internal medicine, hospitalization, etc.) where the drug was initially prescribed; first visit: first measurement of every single variable after sacubitril/valsartan initiation, regardless the clinical setting or the time after drug prescription; study end: last measurement of every single variable before the study end, regardless the clinical setting or the time after drug prescription. Baseline values were compared with those at study end.
Any side effect and specific adverse events during treatment with sacubitril/valsartan in the overall study population and according to the physician that started treatment with this drug and according to the final dose prescribed were determined.
Events during treatment with sacubitril/valsartan in the overall study population and according to the physician that started treatment with this drug and according to the final dose prescribed were analyzed. Rates of outcomes (any event, death from any cause, cardiovascular death, sudden cardiac death, any hospitalization and hospitalization for HF) were independently analyzed, but also the variable composed of any event, cardiovascular death or hospitalization for HF and the variable composed of any event, cardiovascular death, hospitalization for HF or decompensated HF.
Statistical analysis
For the descriptive analysis, quantitative variables were described with measures of central tendency (mean) and dispersion (standard deviation) and qualitative variables as absolute frequency (n) and proportions (%). When two means at baseline and during follow-up were compared, paired sample t-test was used. Categorical variables were compared with the χ2 test or the Fisher exact test, according to the sample size. Outcomes during treatment with sacubitril/valsartan were calculated as events per 100 patient-years. Statistical significance was set at a p-value < 0.05. The statistical analysis was performed using SPSS 23.0 (SPSS, Inc., IL, USA).
Results
From June 2016 to June 2018, 167 patients started treatment with sacubitril/valsartan. Of these, 18 patients were excluded (3 for incomplete data, 2 for inappropriate indication and 13 for premature discontinuation). Finally, a total of 149 patients were included in the study (mean duration of treatment of 316.1 ± 155.9 days); 42 patients (28.2%) were attended in the HF unit and the remaining 107 patients (71.8%) in other clinical settings (97 patients [65.1%] in general cardiology, 6 patients [4.0%] in internal medicine, 3 patients [2.0%] in primary care and 1 patient [0.7%] in nephrology).
Overall, at baseline, mean age was 70.7 ± 9.6 years, 69.8% of patients were men, 73.8% of patients had hypertension, 49.0% previous myocardial infarction and 53.7% had no history of atrial fibrillation. Of these patients, 8.9% developed new-onset atrial fibrillation during the follow-up. Ischemic heart disease was the most common cause of HF, followed by idiopathic cardiomyopathy. Totally, 26.8% patients had been hospitalized for HF in the previous year. With regard to the treatment for HF at baseline, 89.9% of patients were taking angiotensin-converting enzyme inhibitors or angiotensin receptor blockers, 91.9% beta blockers, 79.9% aldosterone antagonists and 73.2% diuretics. Mean NT-proBNP was 3884 ± 4871 pg/ml and CA 125 25.6 ± 39.9 U/ml. Mean left ventricular ejection fraction was 31.2 ± 7.0% and 33.1% had moderate to severe mitral insufficiency (Table 1).
| Variable | Overall (n = 149) |
|---|---|
| Biodemographic data | |
| Age (years) | 70.7 ± 9.6 |
| Sex, male (%) | 69.8 |
| Physical examination | |
| Systolic blood pressure (mmHg) | 129.5 ± 16.3 |
| Diastolic blood pressure (mmHg) | 78.9 ± 13.7 |
| Heart rate (bpm) | 70.7 ± 12.4 |
| Bodyweight (kg) | 79.2 ± 15.9 |
| Cardiovascular risk factors | |
| Hypertension (%) | 73.8 |
| Diabetes (%) | 40.9 |
| Dyslipidemia (%) | 77.9 |
| Smoking (%) Never Current Former | 53.8 14.0 32.2 |
| Alcoholism (%) Never Current Former | 82.1 9.7 8.3 |
| Concomitant conditions | |
| Previous myocardial infarction (%) | 49.0 |
| Prior stroke (%) | 6.7 |
| Atrial fibrillation (%) No Paroxysmal Persistent Permanent | 53.7 12.2 4.8 29.3 |
| New-onset atrial fibrillation (%) | 8.9 |
| HF data | |
| Type of cardiac disease (%) Ischemic Idiopathic Alcoholic Tachycardiomyopathy Valvular Others | 57.0 18.8 5.4 6.7 6.7 5.4 |
| NYHA functional class | 2.3 ± 0.6 |
| Hospitalization for HF in the previous year (%) | 26.8 |
| Admission to the emergency department for HF in the previous year (%) | 23.5 |
| Treatment | |
| ACEI/ARB (%) Equivalent dose of enalapril (mg) | 89.9 11.3 ± 10.9 |
| Beta blockers (%) | 91.9 |
| Ivabradine (%) | 22.1 |
| Sodium–glucose cotransporter 2 inhibitors (%) | 23.5 |
| Aldosterone antagonists (%) | 79.9 |
| Diuretics (%) Equivalent dose of furosemide (mg) | 73.2 48.4 ± 31.8 |
| Implantable cardioverter–defibrillator, n (%) | 36.9 |
| Cardiac resynchronization therapy (%) | 24.2 |
| Biochemical data | |
| Serum creatinine (mg/dl) | 1.06 ± 0.3 |
| Urea (mg/dl) | 48.8 ± 17.5 |
| Sodium (mmol/l) | 140.6 ± 2.7 |
| Potassium (mmol/l) | 4.47 ± 0.5 |
| GPT (UI/l) | 30.0 ± 28.0 |
| Glucose (mg/dl) | 114.3 ± 54.3 |
| HbA1c (%) | 6.4 ± 2.8 |
| Hemoglobin (g/dl) | 13.6 ± 1.8 |
| Platelets (×103/μl) | 198.9 ± 59.8 |
| NT-proBNP (pg/ml) | 3884 ± 4871 |
| CA 125(U/ml) | 25.6 ± 39.9 |
| Ferritin (ng/ml) | 191.8 ± 221.7 |
| Transferrin saturation (%) | 22.4 ± 13.2 |
| Serum iron (μg/dl) | 67.8 ± 45.7 |
| Uric acid (mg/dl) | 7.5 ± 4.3 |
| Echocardiographic parameters | |
| LV end-diastolic diameter (mm) | 59.3 ± 9.3 |
| LV ejection fraction (%) | 31.2 ± 7.0 |
| Systolic pulmonary artery pressure (mmHg) | 39.8 ± 12.4 |
| Mitral insufficiency (%) No Mild Moderate Severe | 20.9 46.0 27.7 5.4 |
ACEI: Angiotensin-converting enzyme inhibitor; ARB: Angiotensin receptor blocker; bpm: beats per minute; CA 125: Cancer antigen 125; HF: Heart failure; LV: Left ventricular; NT-proBNP: N-terminal prohormone of BNP; NYHA: New York Heart Association Functional Classification.
Baseline clinical characteristics of the study population were compared according to the physician that started treatment with sacubitril/valsartan (HF unit vs no HF unit). Those patients attended in the HF unit were younger (65.9 ± 10.1 vs 72.6 ± 8.8; p < 0.001), more commonly men (83.3% vs 64.5%; p = 0.01) and ischemic heart disease was the most common cause of HF (61.9% vs 55.1%; p = 0.01). Angiotensin-converting enzyme inhibitors/angiotensin receptor blockers, ivabradine, diuretics and implantable cardioverter–defibrillators were more commonly prescribed among patients attended in the HF unit than in other clinical settings, whereas NT-proBNP levels (2566.0 ± 3208.2 vs 4544.2 ± 5417.8 pg/ml; p = 0.02) were lower in those patients attended in the HF unit, CA 125 levels were higher (37.4 ± 54.3 vs 18.2 ± 25.6 pg/ml; p = 0.003). No other significant differences were found between both groups.
At baseline, 83.9% of patients were taking sacubitril/valsartan at a dose of 24/26 mg, 15.4% at a dose of 49/51 mg and 0.7% at a dose of 97/103 mg. At the end of the follow-up, these numbers moved to 38.9, 39.6 and 12.8%, respectively. Totally, 8.7% patients discontinued treatment with sacubitril/valsartan during the follow-up. Among the 125 patients that started treatment with sacubitril/valsartan at a dose of 24/26 mg, 90.4% met at least one criterion recommended for beginning with this dose. These data did not significantly differ between patients attended in the HF unit or other clinical settings.
Overall, mean duration of treatment with sacubitril/valsartan was 316.1 ± 155.9 days. With regard to the evolution of different clinical, biochemical and echocardiographic parameters during the follow-up (Table 2 & Figure 1), systolic and diastolic blood pressure significantly decreased (from 129.5 ± 16.3/78.9 ± 13.7 to 117.8 ± 15.5/73.0 ± 9.8 mmHg, respectively; p < 0.001), as well as the use of diuretics (from 73.2% to 57.4%; p = 0.008); NYHA functional class (from 2.3 ± 0.6 to 1.8 ± 0.5; p < 0.001) significantly improved; potassium levels significantly increased (from 4.47 ± 0.5 to 4.73 ± 0.4; p < 0.001), NT-proBNP (from 3884 ± 4871 to 1975.3 ± 3006.6 pg/ml; p = 0.0001), and CA 125 levels (from 25.6 ± 39.9 to 11.3 ± 21.5 U/ml; p = 0.0001); left ventricular end-diastolic diameter (from 59.3 ± 9.3 to 57.1 ± 7.6 mm; p = 0.02) and systolic pulmonary artery pressure (from 39.8 ± 12.4 to 35.3 ± 7.4 mmHg; p = 0.0002) significantly decreased and left ventricular ejection fraction significantly increased (from 31.2 ± 7.0 to 37.3 ± 10.5%; p < 0.001). In general, the positive evolution of the majority of these parameters occurred in both, patients attended in HF unit and other clinical settings and with all doses of sacubitril/valsartan. The increase of left ventricular ejection fraction and the decrease of NT-proBNP levels were slightly higher in patients with nonischemic cardiomyopathy than in patients with ischemic heart disease (from 28.8 ± 7.5% to 38.4 ± 12.9%; p < 0.001 and from 32.9% ± 6.0% to 36.3 ± 7.5%; p = 0.001, respectively and from 4279.4 ± 5130.3 to 1912.8 ± 3696.5 pg/ml; p = 0.003 and from 3527.8 ± 4638.1 to 2043.2 ± 2064.8 pg/ml; p = 0.007, respectively). In those patients who discontinued treatment with sacubitril/valsartan, NT-proBNP levels and left ventricular ejection fraction did not significantly change during the follow-up.
| Variable | Overall (n = 149) | p-value |
|---|---|---|
| Physical examination | ||
| Systolic blood pressure (mmHg) baseline | 129.5 ± 16.3 | <0.001 |
| Study end | 117.8 ± 15.5 | |
| Diastolic blood pressure (mmHg) baseline | 78.9 ± 13.7 | <0.001 |
| Study end | 73.0 ± 9.8 | |
| Heart rate (bpm) baseline | 70.7 ± 12.4 | NS |
| Study end | 68.9 ± 10.7 | |
| Bodyweight (kg) baseline | 79.2 ± 15.9 | NS |
| Study end | 79.7 ± 15.9 | |
| HF data | ||
| NYHA functional class baseline | 2.3 ± 0.6 | <0.001 |
| Study end | 1.8 ± 0.5 | |
| Treatment | ||
| Diuretics (%) baseline | 73.2 | 0.008 |
| Study end | 57.4 | |
| Equivalent dose of furosemide (mg) baseline | 48.4 ± 31.8 | 0.007 |
| Study end | 38.3 ± 32.7 | |
| Biochemical data | ||
| Serum creatinine (mg/dl) baseline | 1.06 ± 0.3 | NS |
| Study end | 1.07 ± 0.4 | |
| Urea (mg/dl) baseline | 48.8 ± 17.5 | NS |
| Study end | 52.7 ± 25.3 | |
| Sodium (mmol/l) baseline | 140.6 ± 2.7 | NS |
| Study end | 139.9 ± 11.8 | |
| Potassium (mmol/l) baseline | 4.47 ± 0.5 | <0.001 |
| Study end | 4.73 ± 0.4 | |
| GPT (UI/l) baseline | 30.0 ± 28.0 | NS |
| Study end | 26.5 ± 18.0 | |
| Glucose (mg/dl) baseline | 114.3 ± 54.3 | NS |
| Study end | 107.6 ± 66.4 | |
| HbA1c (%) baseline | 6.4 ± 2.8 | NS |
| Study end | 6.0 ± 0.9 | |
| Hemoglobin (g/dl) baseline | 13.6 ± 1.8 | <0.001 |
| Study end | 14.6 ± 1.5 | |
| Plateletes (×103/μl) baseline | 198.9 ± 59.8 | 0.0005 |
| Study end | 176.7 ± 49.2 | |
| NT-proBNP (pg/ml) baseline | 3884 ± 4871 | 0.0001 |
| Study end | 1975.3 ± 3006.6 | |
| CA 125 (U/ml) baseline | 25.6 ± 39.9 | 0.0001 |
| Study end | 11.3 ± 21.5 | |
| Ferritin (ng/ml) baseline | 191.8 ± 221.7 | 0.007 |
| Study end | 252.9 ± 167.6 | |
| Transferrin saturation (%) baseline | 22.4 ± 13.2 | 0.0002 |
| Study end | 28.4 ± 14.3 | |
| Serum iron (μg/dl) baseline | 67.8 ± 45.7 | 0.01 |
| Study end | 81.0 ± 44.0 | |
| Uric acid (mg/dl) baseline | 7.5 ± 4.3 | 0.002 |
| Study end | 6.3 ± 1.9 | |
| Echocardiographic parameters | ||
| LV end-diastolic diameter (mm) baseline | 59.3 ± 9.3 | 0.02 |
| Study end | 57.1 ± 7.6 | |
| LV ejection fraction (%) baseline | 31.2 ± 7.0 | <0.001 |
| Study end | 37.3 ± 10.5 | |
| Systolic pulmonary artery pressure (mmHg) baseline | 39.8 ± 12.4 | 0.0002 |
| Study end | 35.3 ± 7.4 | |
bpm: Beats per minute; HF: Heart failure; LV: Left ventricular; NS: Nonsignificant; NYHA: New York Heart Association Functional Classification.
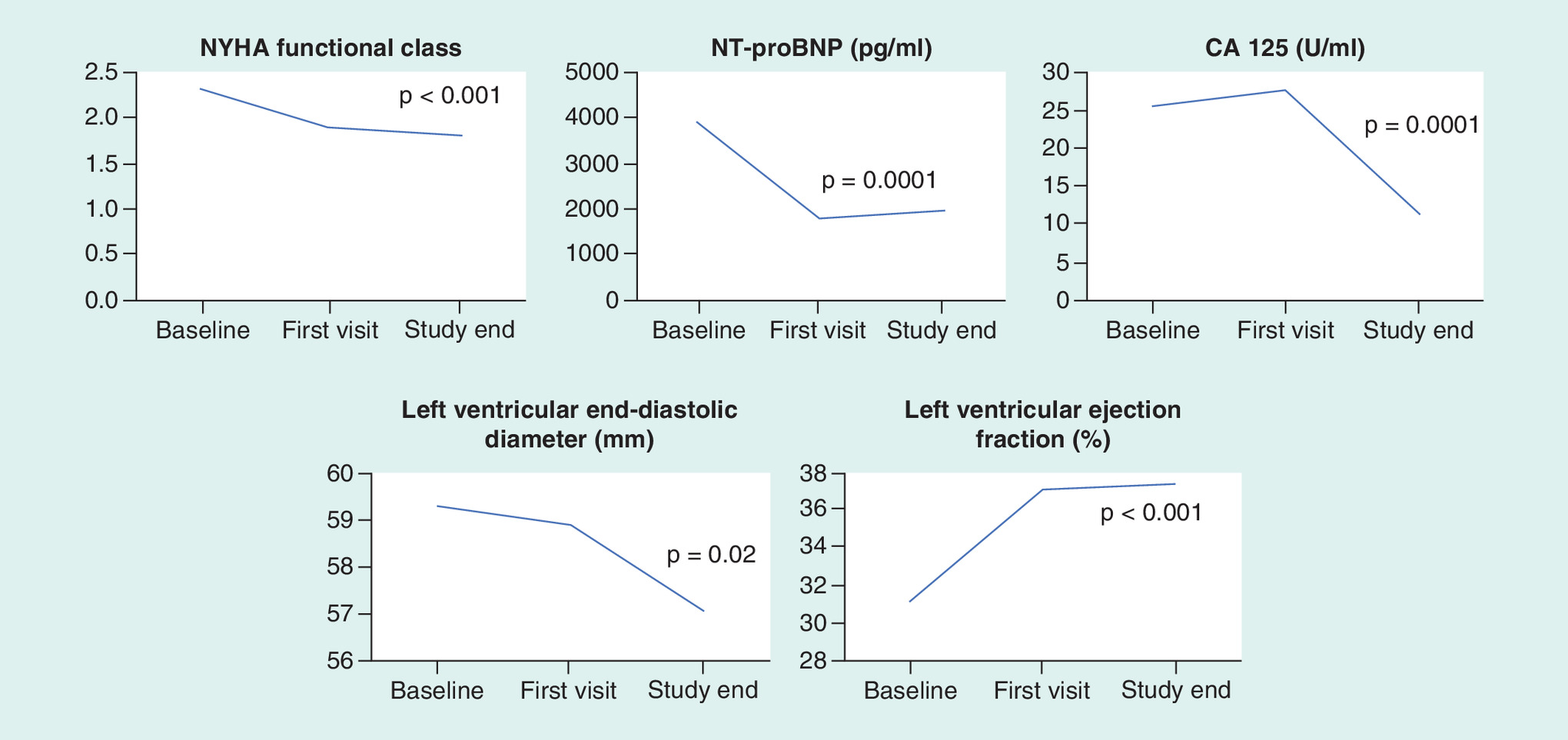
Figure 1. Evolution of functional class, NT-proBNP, CA 125, left ventricular end-diastolic diameter and left ventricular ejection fraction during the study in the overall study population.
CA 125: Cancer antigen 125; NYHA: New York Heart Association Functional Classification; NT-proBNP: N-terminal prohormone of BNP.
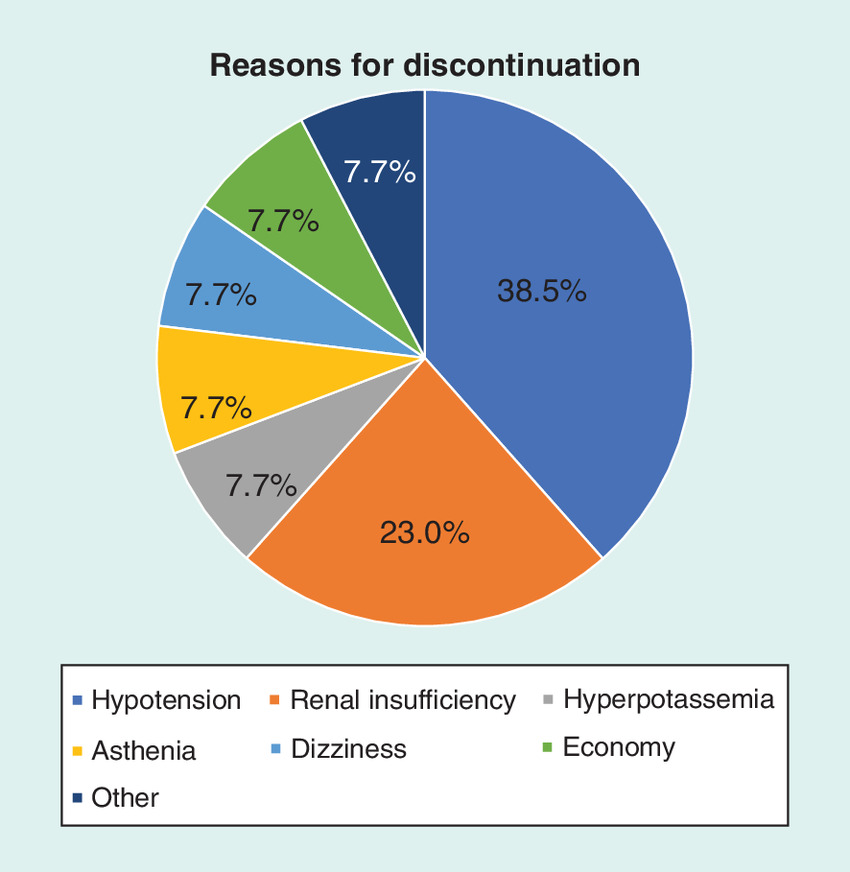
With regard to side effects associated with treatment with sacubitril/valsartan (Table 3), 21.5% of patients reported at least one adverse event, being hypotension (11.4%) and dizziness (4.0%) the most common ones. The proportion of patients with any side effect was independent of the clinical setting in which patients were attended. All patients that discontinued treatment with sacubitril/valsartan had at least one side effect, mainly hypotension, and renal insufficiency (Figure 2), and among patients who remained on sacubitril/valsartan, the frequency of any side effect was more common in those patients taking sacubitril/valsartan 24/26 mg (Table 3).
| Variable | Overall (n = 149) | 24/26 mg (n = 58) | 49/51 mg (n = 59) | 97/103 mg (n = 19) | Discontinuation (n = 13) | p-value |
|---|---|---|---|---|---|---|
| Any side effect (%) | 21.5 | 17.2 | 11.9 | 10.5 | 100 | <0.001 |
| Reduction of dose (%) | 4.7 | 5.2 | 1.7 | 5.3 | 15.4 | NS |
| Discontinuation of treatment (%) | 8.7 | 0 | 0 | 0 | 100 | <0.001 |
| Hypotension (%) | 11.4 | 13.8 | 5.1 | 5.3 | 38.5 | 0.005 |
| Hyperpotassemia (%) | 0.7 | 0 | 0 | 0 | 7.7 | NS |
| Renal insufficiency (%) | 2.0 | 0 | 0 | 0 | 23.1 | 0.003 |
| Headache (%) | 0.7 | 0 | 0 | 5.3 | 0 | NS |
| Asthenia (%) | 2.7 | 3.4 | 0 | 5.3 | 7.7 | NS |
| Dizziness (%) | 4.0 | 5.2 | 3.4 | 0 | 7.7 | NS |
| Cutaneous reaction (%) | 0.7 | 0 | 0 | 5.3 | 0 | NS |
| Cough (%) | 1.3 | 0 | 3.4 | 0 | 0 | NS |
| Angioedema (%) | 0.7 | 0 | 1.7 | 0 | 0 | NS |
| Others (%) | 2.7 | 1.7 | 5.1 | 0 | 0 | NS |
NS: Nonsignificant.
Events during treatment with sacubitril/valsartan were reported in Table 4. During the study period, the combined variable composed of any event, cardiovascular death, hospitalization for HF or decompensated HF occurred in 17 patients (11.4%; 13.2 events per 100 patient-years). No cardiovascular death, or sudden cardiac death occurred during the follow-up. There was a trend towards more events (the combined variable of any event, cardiovascular death, hospitalization for HF or decompensated HF) among patients taking sacubitril/valsartan 24/26 mg or those that discontinued treatment compared with patients taking sacubitril/valsartan 49/51 or 197/203 mg, that reached statistical significance when patients taking low doses of sacubitril/valsartan were combined with those patients that discontinued treatment compared with patients taking sacubitril/valsartan at moderate or high doses (16.9 vs 6.4%, p = 0.04). Rates of events were independent of the clinical setting in which patients were attended.
| Variable | Overall (n = 149) | 24/26 mg (n = 58) | 49/51 mg (n = 59) | 97/103 mg (n = 19) | Discontinuation (n = 13) | p-value | 24/26 + discontinuation (n = 71) | 49/51 + 97/103 mg (n = 78) | p-value |
|---|---|---|---|---|---|---|---|---|---|
| Mean duration of treatment (days) | 316.1 ± 155.9 | 275.4 ± 163.8 | 329.7 ± 145.5 | 387.8 ± 140.1 | 330.9 ± 152.3 | 0.03 | 285.6 ± 162.1 | 343.8 ± 145.5 | 0.02 |
| Any event, n (%) Events per 100 patient-years | 9 (6.0) 6.9 | 4 (6.9) 9.1 | 3 (5.1) 5.6 | 1 (5.3) 5.0 | 1 (7.7) 8.5 | NS | 5 (7.0) 8.9 | 4 (5.1) 5.4 | NS |
| Death from any cause, n (%) Events per 100 patient-years | 3 (2.0) 2.3 | 2 (3.4) 4.5 | 1 (1.7) 1.9 | 0 | 0 | NS | 2 (2.8) 3.6 | 1 (1.3) 1.4 | NS |
| CV death, n (%) Events per 100 patient-years | 0 | 0 | 0 | 0 | 0 | – | 0 | 0 | – |
| Sudden cardiac death, n (%) Events per 100 patient-years | 0 | 0 | 0 | 0 | 0 | – | 0 | 0 | – |
| Any hospitalization, n (%) Events per 100 patient-years | 13 (8.7) 10.0 | 5 (8.6) 11.4 | 2 (3.4) 3.8 | 3 (15.8) 14.9 | 3 (23.1) 25.5 | NS | 8 (11.3) 14.4 | 5 (6.4) 6.8 | NS |
| Hospitalization for HF, n (%) Events per 100 patient-years | 8 (5.4) 6.2 | 4 (6.9) 9.1 | 0 | 2 (10.5) 9.9 | 2 (15.4) 17.0 | NS | 6 (8.5) 10.9 | 2 (2.6) 2.8 | NS |
| Any event, CV death or hospitalization for HF, n (%) Events per 100 patient-years | 8 (5.4) 6.2 | 4 (6.9) 9.1 | 0 | 2 (10.5) 9.9 | 2 (15.4) 17.0 | NS | 6 (8.5) 10.9 | 2 (2.6) 2.8 | NS |
| Any event, CV death, hospitalization for HF or decompensated HF, n (%) Events per 100 patient-years | 17 (11.4) 13.2 | 9 (15.5) 20.5 | 2 (3.4) 3.8 | 3 (15.8) 14.9 | 3 (23.1) 25.5 | NS (0.08) | 12 (16.9) 21.6 | 5 (6.4) 6.8 | 0.04 |
CV: Cardiovascular; HF: Heart failure.
Discussion
In the PARADIGM-HF trial [7], to be included, patients were required to take a stable dose of renin angiotensin system inhibitors (equivalent to at least 10 mg of enalapril daily). In addition, patients were excluded if they had a systolic blood pressure <100 mmHg at screening or 95 mmHg at randomization, an estimated glomerular filtration rate below 30 ml/min/1.73 m2, a serum potassium level >5.2 mmol/l at screening (or >5.4 mmol/l at randomization) or unacceptable side effects during treatment with angiotensin-converting enzyme inhibitors or angiotensin receptor blockers. This means that in clinical practice, many patients with HF and reduced ejection fraction may not meet inclusion/exclusion criteria of the PARADIGM-HF trial. Thus, it has been reported that only 25% of real-world population with HF and reduced ejection fraction are eligible for sacubitril-valsartan according to the PARADIGM-HF criteria [13,23]. In addition, the adoption of sacubitril/valsartan in ‘real-life’ patients is slow [24], and this may limit the beneficial effects of sacubitril/valsartan in HF population in routine practice. This lack of data makes necessary the publication of observational studies that evaluate whether the results of the PARADIGM-HF trial may be extrapolated to the overall HF study population.
In our study, patients from different clinical settings (i.e., HF unit, general cardiology, internal medicine, primary care and nephrology) were included, and this makes our data more representative of the whole HF population. Our patients were old, 70% were men, the presence of cardiovascular risk factors and other comorbidities was common and ischemic heart disease was the main cause of HF. Compared with the PARADIGM-HF trial [7], our patients were older (71 vs 64 years), systolic blood pressure and NT-proBNP levels were higher (130 vs 122 mmHg and 3884 vs 1631 pg/ml, respectively). The majority of the studies that have analyzed the use of sacubitril/valsartan in clinical practice have included patients with a similar clinical profile than those included in the pivotal trial [17,20,22,25], and only a small number of studies have included patients with a worse clinical profile. Thus, in a prospective study in 10 hospitals with 427 patients, subjects had a higher risk profile than in the pivotal trial, poorer functional class, higher levels of natriuretic peptides and worse renal function [18]. In addition, in our study, the clinical profile of patients according to the clinical setting in which patients were attended was also analyzed. Patients attended in the HF unit were younger, more commonly men and the use of guideline-directed medical therapies was higher than in other clinical settings. As a result, our data may provide relevant information about the effectiveness and safety of sacubitril/valsartan in more complex patients attended by different specialties and clinical scenarios.
In our study, in the great majority of patients (84%), the initial dose of sacubitril/valsartan was 24/26 mg, and at the end of the follow-up, 39% remained on this dose. As our study showed, there were some relevant differences regarding the clinical profile of patients according to the initial dose prescribed of sacubitril/valsartan. Remarkably, this dose was not tested in the PARADIGM-HF trial [7]. Thus, in the PARADIGM-HF trial [7], during the run-in period, patients received enalapril (at a dose of 10 mg twice daily) for 2 weeks and if no unacceptable side effects occurred, this regimen was followed by treatment with sacubitril/valsartan for an additional 4–6 weeks (initially at a dose of 49/51 mg twice daily, which was increased to 97/103 mg twice daily). Since no specific Phase III clinical trial has been developed for the lowest dose of sacubitril/valsartan, the effectiveness and safety of this dose can only be analyzed in observational studies at this moment. According to the summary of product characteristics [26], those patients with HF and reduced ejection fraction that are naive for sacubitril/valsartan, receive low doses of angiotensin-converting enzyme inhibitors/angiotensin receptor blockers, have an estimated glomerular filtration rate <60 ml/min/1.73 m2, a systolic blood pressure 100–110 mmHg, or moderate hepatic insufficiency (or AST/ALT levels >2 upper limit of normality [ULN]) should start with sacubitril/valsartan at a dose of 24/26 mg. In our study, more than 90% of patients that started treatment with this dose met at least one of these criteria. In these patients, treatment should be titrated gradually to facilitate achieving the target dose of sacubitril/valsartan [27]. Some titration algorithms have been proposed for reaching the maximal dosage with a good tolerability profile [28].
In the PARADIGM-HF trial, compared with enalapril, sacubitril/valsartan improved functional class and health-related quality of life outcomes [29,30]. In our study, treatment with sacubitril/valsartan was associated with a significant symptom improvement (NYHA functional class improved from 2.3 to 1.8; p < 0.001), that was independent of the clinical setting in which patients were attended, and that occurred with all doses of sacubitril/valsartan. Similarly, other studies have shown that sacubitril/valsartan relieves symptoms, improves functional class and physical capability in routine practice [16,19,22,31,32]. Thus, a recent study has shown that after only 1 month of therapy with sacubitril/valsartan 97/103 mg, the mean distance walked on the 6-min walk test increased from 129 to 436 m [31].
Although some physicians may consider that many outpatients with HF are stable, the fact is that HF has a progressive nature [33]. Experimental data have shown that sacubitril/valsartan attenuates cardiac hypertrophy, fibrosis, vasculopathy, inflammation, oxidative stress and mitochondrial depletion/dysfunction [34,35]. This translates into a reduction of cardiac filling pressures and a beneficial reverse remodeling of both, systolic as diastolic function in patients with HF and reduced ejection fraction [36,37]. A small study showed that after only 3 months of treatment, sacubitril/valsartan was associated with a significant increase of left ventricular ejection fraction and a significant reduction of left ventricular diameters. In addition, the increase in ejection fraction tended to be marginally greater in the medium/high dose group as compared with the low dose group [38]. In our study, NT-proBNP levels significantly decreased, and echocardiographic parameters significantly improved. Left ventricular improvement was higher as the dose of sacubitril/valsartan increased but left ventricular ejection fraction remained unchanged among those patients that discontinued treatment with sacubitril/valsartan. These data emphasize the importance of remaining on treatment with sacubitril/valsartan when possible. Increase in CA 125 levels have been associated with adverse outcomes in patients with HF [39]. In our study, overall, CA 125 significantly decreased by 56%, and this decrease tended to be higher as the dose of sacubitril/valsartan increased.
In the PARADIGM-HF [7], during the run-in period, 12% of the patients withdrew treatment because of an adverse event (most frequently cough, hyperkalemia, renal dysfunction or hypotension). In our study that included patients without a run-in period, but the majority started with low doses, less than 9% of patients discontinued treatment with sacubitril/valsartan. Other studies have confirmed the safety of sacubitril/valsartan in routine practice [40–42].
Despite our cohort patients was old and had many comorbidities, the number of events that occurred after almost 1 year of treatment was low. Thus, during this period, the combined variable composed of any event, cardiovascular death, hospitalization for HF or decompensated HF occurred only in 17 patients (13.2 events per 100 patient-years), and no cardiovascular death occurred. The majority of events were related with hospitalizations for HF. Remarkably, in our study, although 26.8% of patients had been hospitalized for HF in the year before taking sacubitril/valsartan, only 5.4% of patients were hospitalized for HF during treatment with sacubitril/valsartan. During this period, the HF unit was established, and this could have had an impact on the reduction of outcomes. On the other hand, events were more common among patients taking sacubitril/valsartan 24/26 mg or discontinued treatment than patients taking moderate or high doses of sacubitril/valsartan. Recent studies have shown that sacubitril/valsartan is associated with a significant and early reduction in incident HF-hospitalizations in real-world patients with HF and reduced ejection fraction, but higher doses might be associated with more reduction in HF admissions [42,43]. In our study, no sudden cardiac deaths were reported. A reduction of sudden cardiac death was observed in the PARADIGM-HF [7] with sacubitril/valsartan compared with enalapril. Remarkably, it has recently been reported that in patients with HF and reduced left ventricular ejection fraction and an implantable cardioverter–defibrillator with remote monitoring, sacubitril/valsartan significantly decreases ventricular arrhythmias and appropriate implantable cardioverter–defibrillator shocks [44].
This study has some limitations. First, the study had a retrospective design without a comparator group. As a result, some bias could not be controlled. However, the aim of the study was not to ascertain causality between sacubitril/valsartan and changes of different variables over time, but to describe sacubitril/valsartan use in real-world practice. In this context, the retrospective design is the best to ascertain the clinical management of patients as physicians and patients are not influenced by participating in the study. Second, although the sample size was quite small, it was sufficient to respond the main objectives of the study. In addition, our results were in line with previous publications, which showed an improvement in clinical measurements and laboratory data after sacubitril/valsartan prescription in daily practice, as well as good drug tolerability. Third, the healthcare area of the hospital of Denia includes a significant proportion of foreign patients, not only from different countries but also from other parts of Spain. In some cases, sacubitril/valsartan was started but the patient moved to another city. Due to the retrospective design of our study, we were unable to collect reliable data of these patients, and we decided to exclude them from the analysis, as we preferred to analyze only those patients with complete data in order to assure a higher robustness of the results. Fourth, although the measures were taken at different relative times, the standardization of the protocol made that the variability of the data was small, but the robustness of the results high. Finally, this was a unicenter study. Although this may assure a higher homogeneity in the management of these patients, this could limit the generalization of the results.
In conclusion, in this cohort of ‘real-life’ patients with HF and reduced ejection fraction, improvements in NYHA functional class, surrogate variables such as NT-proBNP, CA 125 or left ventricular ejection fraction were observed after the initiation of sacubitril/valsartan. The safety profile of sacubitril/valsartan was remarkable. In addition, cardiovascular events were low, mainly associated with HF hospitalizations. Up to 39% of patients remained on the lowest dose of sacubitril/valsartan during the follow-up. More efforts should be performed to uptitrate the dose of sacubitril/valsartan as recommended by guidelines.
•
The information about the impact of sacubitril/valsartan on functional class, surrogate variables and cardiovascular outcomes in ‘real-life’ patients is warranted.
•
This study analyzed the impact of sacubitril/valsartan on functional class, surrogate parameters and clinical outcomes in clinical practice.
•
This was a retrospective and unicenter study that included patients with heart failure and reduced ejection fraction that started treatment with sacubitril/valsartan.
•
Sacubitril/valsartan was associated with improvements in NYHA functional class, surrogate variables such as NT-proBNP, CA 125 or left ventricular ejection fraction, with a good safety profile.
•
Up to 39% of patients remained on the lowest dose of sacubitril/valsartan during the follow-up.
•
During treatment with sacubitril/valsartan, cardiovascular events were low, mainly associated with HF hospitalizations.
•
There was a trend towards more events among patients taking sacubitril/valsartan 24/26 mg or those that discontinued treatment.
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
Writing and editorial assistance was provided by Content Ed Net (Madrid, Spain), with funding from Sociedad Valenciana de Cardiología.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations.
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Yandrapalli S, Khan MH, Rochlani Y, Aronow WS. Sacubitril/valsartan in cardiovascular disease: evidence to date and place in therapy. Ther. Adv. Cardiovasc. Dis. 12, 217–231 (2018).
2.
Yandrapalli S, Andries G, Biswas M, Khera S. Profile of sacubitril/valsartan in the treatment of heart failure: patient selection and perspectives. Vasc. Health Risk Manag. 13, 369–382 (2017).
3.
Rudiger A, Harjola VP, Muller A et al. Acute heart failure: clinical presentation, one-year mortality and prognostic factors. Eur. J. Heart Fail. 7, 662–670 (2005).
• Despite current heart failure (HF) therapies, morbidity and mortality of patients hospitalized with acute HF remain high.
4.
Fonarow GC, Abraham WT, Albert NM et al. Association between performance measures and clinical outcomes for patients hospitalized with heart failure. JAMA 297, 61–70 (2007).
5.
Benjamin EJ, Virani SS, Callaway CW et al. Heart disease and stroke statistics – 2018 update: a report from the American Heart Association. Circulation 137, e67–e492 (2018).
6.
Dunlay SM, Roger VL. Understanding the epidemic of heart failure: past, present, and future. Curr. Heart Fail. Rep. 11, 404–415 (2014).
7.
McMurray JJ, Packer M, Desai AS et al. Angiotensin–neprilysin inhibition versus enalapril in heart failure. N. Engl. J. Med. 371, 993–1004 (2014).
•• In the PARADIGM-HF trial, sacubitril/valsartan was superior to enalapril in reducing the risk of death and HF hospitalization among patients with HF and reduced ejection fraction.
8.
Ponikowski P, Voors AA, Anker SD et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 37, 2129–2200 (2016).
9.
Ambrosy AP, Mentz RJ, Fiuzat M et al. The role of angiotensin receptor–neprilysin inhibitors in cardiovascular disease-existing evidence, knowledge gaps, and future directions. Eur. J. Heart Fail. 20, 963–972 (2018).
10.
Joly JM, Desai AS. Sacubitril/valsartan: from clinical trials to real-world experience. Curr. Treat. Options Cardiovasc. Med. 20, 45 (2018).
11.
Sciatti E, Senni M, Lombardi CM, Gori M, Metra M. Sacubitril/valsartan: from a large clinical trial to clinical practice. J. Cardiovasc. Med. (Hagerstown) 19, 473–479 (2018).
12.
Fontes-Carvalho R. Sacubitril–valsartan in the real world: from theory to clinical practice. Rev. Port. Cardiol. 37, 497–498 (2018).
13.
Rodrigues G, Tralhão A, Aguiar C, Freitas P, Ventosa A, Mendes M. Is the PARADIGM-HF cohort representative of the real-world heart failure patient population? Rev. Port. Cardiol. 37, 491–496 (2018).
• In this cohort, only one in four patients with systolic HF fulfilled criteria for the PARADIGM-HF trial.
14.
Barrios V, Escobar C, Pallares V et al. Management of heart failure in cardiology and primary care (MICCAP) program: improving the management of patients with heart failure. Semergen 44(8), 572–578 (2018).
15.
Gagne JJ, Tsacogianis T, Bruce Wirta S et al. Characteristics of early sacubitril/valsartan patients and considerations for studies in electronic health record data. J. Comp. Eff. Res. 7(11), 1073–1082 (2018).
16.
Rodil Fraile R, Malafarina V, Tiberio López G. Sacubitril–valsartan in heart failure and multimorbidity patients. ESC Heart Fail. 5(5), 956–959 (2018).
17.
DeVore AD, Mi X, Thomas L et al. Characteristics and treatments of patients enrolled in the CHAMP-HF registry compared with patients enrolled in the PARADIGM-HF trial. J. Am. Heart Assoc. 7(12), pii: e009237 (2018).
18.
Vicent L, Esteban-Fernández A, Gómez-Bueno M et al. Clinical profile of a nonselected population treated with sacubitril/valsartan is different from PARADIGM-HF trial. J. Cardiovasc. Pharmacol. 72, 112–116 (2018).
19.
Antol DD, Casebeer AW, DeClue RW, Stemkowski S, Russo PA. An early view of real-world patient response to sacubitril/valsartan: a retrospective study of patients with heart failure with reduced ejection fraction. Adv. Ther. 35, 785–795 (2018).
• In clinical practice, sacubitril/valsartan improves symptoms and reduces hospitalizations.
20.
Wachter R, Viriato D, Klebs S et al. Early insights into the characteristics and evolution of clinical parameters in a cohort of patients prescribed sacubitril/valsartan in Germany. Postgrad. Med. 130, 308–316 (2018).
• Despite baseline demographics and clinical characteristics being similar to those from PARADIGM-HF trial, most patients were initiated on the lowest dose.
21.
Vincenzi A, Cesana F, Cirò A, Garatti L, Achilli F. Sacubitril/valsartan in “field practice” patients with advanced heart failure: a monocentric Italian experience. Cardiology 138(Suppl. 1), 13–16 (2017).
22.
Kałużna-Oleksy M, Kolasa J, Migaj J et al. Initial clinical experience with the first drug (sacubitril/valsartan) in a new class – angiotensin receptor neprilysin inhibitors in patients with heart failure with reduced left ventricular ejection fraction in Poland. Kardiol. Pol. 76, 381–387 (2018).
23.
Norberg H, Bergdahl E, Lindmark K. Eligibility of sacubitril–valsartan in a real-world heart failure population: a community-based single-centre study. ESC Heart Fail. 5, 337–343 (2018).
24.
Sangaralingham LR, Sangaralingham SJ, Shah ND, Yao X, Dunlay SM. Adoption of sacubitril/valsartan for the management of patients with heart failure. Circ. Heart Fail. 11, e004302 (2018).
25.
Tsutsui H, Momomura SI, Saito Y et al. Angiotensin receptor neprilysin inhibitor in Japanese patients with heart failure and reduced ejection fraction – baseline characteristics and treatment of PARALLEL-HF trial. Circ. J. 82(10), 2575–2583 (2018).
26.
European Medicines Agency Summary of product characteristics of sacubitril/valsartan. www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/004062/WC500197536.pdf
27.
Senni M, McMurray JJV, Wachter R et al. Impact of systolic blood pressure on the safety and tolerability of initiating and up-titrating sacubitril/valsartan in patients with heart failure and reduced ejection fraction: insights from the TITRATION study. Eur. J. Heart Fail. 20, 491–500 (2018).
•• Low systolic blood pressure should not avoid the initiation of sacubitril/valsartan when titration is performed gradually.
28.
Laflamme É, Vachon A, Gilbert S et al. Usefulness of a titration algorithm for de novo users of sacubitril/valsartan in a tertiary centre heart failure clinic. Cardiovasc. J. Afr. 29, 1–5 (2018).
29.
Lewis EF, Claggett BL, McMurray JJV et al. Health-related quality of life outcomes in PARADIGM-HF. Circ. Heart Fail. 10(8), pii: e003430 (2017).
30.
Chandra A, Lewis EF, Claggett BL et al. Effects of sacubitril/valsartan on physical and social activity limitations in patients with heart failure: a secondary analysis of the PARADIGM-HF trial. JAMA Cardiol. 3, 498–505 (2018).
31.
Sgorbini L, Rossetti A, Galati A. Sacubitril/valsartan: effect on walking test and physical capability. Cardiology 138(Suppl. 1), 17–20 (2017).
32.
Beltrán P, Palau P, Domínguez E et al. Sacubitril/valsartan and short-term changes in the 6-minute walk test: a pilot study. Int. J. Cardiol. 252, 136–139 (2018).
33.
Anand I. Stable but progressive nature of heart failure: considerations for primary care physicians. Am. J. Cardiovasc. Drugs 18(5), 333–345 (2018).
34.
Suematsu Y, Jing W, Nunes A et al. LCZ696 (sacubitril/valsartan), an angiotensin-receptor neprilysin inhibitor, attenuates cardiac hypertrophy, fibrosis, and vasculopathy in a rat model of chronic kidney disease. J. Card. Fail. 24, 266–275 (2018).
35.
Jing W, Vaziri ND, Nunes A et al. LCZ696 (Sacubitril/valsartan) ameliorates oxidative stress, inflammation, fibrosis and improves renal function beyond angiotensin receptor blockade in CKD. Am. J. Transl. Res. 9, 5473–5484 (2017).
36.
Martens P, Beliën H, Dupont M, Vandervoort P, Mullens W. The reverse remodeling response to sacubitril/valsartan therapy in heart failure with reduced ejection fraction. Cardiovasc. Ther. 36, e12435 (2018).
37.
Januzzi JL, Butler J, Fombu E et al. Rationale and methods of the prospective study of biomarkers, symptom improvement, and ventricular remodeling during sacubitril/valsartan therapy for heart failure (PROVE-HF). Am. Heart J. 199, 130–136 (2018).
38.
Almufleh A, Marbach J, Chih S et al. Ejection fraction improvement and reverse remodeling achieved with sacubitril/valsartan in heart failure with reduced ejection fraction patients. Am. J. Cardiovasc. Dis. 7, 108–113 (2017).
39.
Núñez J, Llàcer P, Bertomeu-González V et al. Carbohydrate antigen-125-guided therapy in acute heart failure: CHANCE-HF: a randomized study. JACC Heart Fail. 4, 833–843 (2016).
40.
Pogge EK, Davis LE. Evaluating the safety and tolerability of sacubitril/valsartan for HFrEF managed within a pharmacist clinic. Am. J. Cardiovasc. Drugs 18, 143–151 (2018).
41.
Moulis F, Rousseau V, Chebane L et al. Serious adverse drug reactions with sacubitril/valsartan Entresto®: a French pharmacovigilance survey. Eur. J. Clin. Pharmacol. 74, 983–984 (2018).
42.
De Vecchis R, Ariano C, Di Biase G, Noutsias M. Sacubitril/valsartan for heart failure with reduced left ventricular ejection fraction: a retrospective cohort study. Herz (2018) (Epub ahead of print).
43.
Martens P, Lambeets S, Lau C, Dupont M, Mullens W. Impact of sacubitril/valsartan on heart failure admissions: insights from real-world patient prescriptions. Acta Cardiol. 74(2), 115–122 (2019).
• In clinical practice, sacubitril/valsartan is associated with a reduction of HF hospitalizations, but higher doses might be associated with greater reductions.
44.
de Diego C, González-Torres L, Núñez JM et al. Effects of angiotensin–neprilysin inhibition compared to angiotensin inhibition on ventricular arrhythmias in reduced ejection fraction patients under continuous remote monitoring of implantable defibrillator devices. Heart Rhythm 15, 395–402 (2018).
Information & Authors
Information
Published In
Pages: 685 - 697
PubMed: 31290687
Copyright
© 2019 Future Medicine Ltd.
History
Received: 18 January 2019
Accepted: 12 April 2019
Published online: 10 July 2019
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Evolution of functional class, biochemical and echocardiographic parameters and clinical outcomes after sacubitril/valsartan initiation in daily practice. (2019) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2019-0014
Export citation
Select the citation format you wish to export for this article or chapter.