Treatment patterns and costs among biologic-naive patients initiating apremilast or biologics for psoriatic arthritis
Abstract
Aim: We evaluated treatment patterns and healthcare costs of initiating psoriatic arthritis (PsA) treatment with oral apremilast versus biologics. Methods: Claims data identified biologic-naive adults with PsA who initiated either apremilast or a biologic from 2013 to 2016. Results: Medication adherence was similar at 12 months (76.9 vs 73.4%; p = 0.175) between apremilast (n = 381) and matched biologic (n = 761) patients. Apremilast users had $12,715 lower total costs per-patient-per-month (p < 0.001), largely due to outpatient pharmacy and medical costs. Conclusion: Commercially insured patients with PsA initiating apremilast had adherence similar to those initiating biologics but lower total healthcare costs.
Approximately 30% of patients with psoriasis develop psoriatic arthritis (PsA), a progressive inflammatory arthritis often first manifesting as joint pain, stiffness and swelling [1–3]. PsA has a marked impact on patients’ quality of life [4]. The chronic yet relapsing/remitting nature of PsA and divergent responses to treatment make treatment challenging [2].
PsA severity varies from mild to severe articular forms with progressive joint deformities; triggers include seasonal exacerbations and stress [5]. An estimated third of those with psoriasis have undiagnosed PsA [6], and those who develop PsA fare worse than patients with psoriasis alone. Patients with PsA were twice as likely as patients with psoriasis to report an inability to work (31 and 67%, respectively) and being on disability (9.2 and 19.6%, respectively) [5].
The 2015 European League Against Rheumatism (EULAR) clinical practice guidelines for the pharmacologic management of PsA recommend oral drugs, such as apremilast, methotrexate, sulfasalazine and leflunomide, or biologics, such as adalimumab, etanercept or ustekinumab, which are given by injection or intravenous infusion [7]. Apremilast is an oral phosphodiesterase 4 inhibitor approved by the US FDA in 2014 for the treatment of psoriasis and PsA [8]. In clinical studies, apremilast demonstrated good efficacy and high tolerability [9–15]; however, information on the real-world benefit of apremilast is limited [16,17]. Many patients prefer apremilast over biologics even though biologics may be more effective because apremilast is administered orally and requires no laboratory monitoring. A network meta-analysis comparing the relative efficacy of apremilast and biologics has been published [18]. The current study was designed to evaluate the treatment patterns (persistence and adherence) and healthcare costs for commercially insured adults initiating apremilast compared with biologic agents for PsA in the USA.
Methods
Study design & data resource
Administrative claims from the 2013–2016 IBM MarketScan® Commercial and Medicare Supplemental Databases (Truven Health Analytics [now IBM Watson Health], MI, USA) were used for this study. The pooled healthcare experience of >100 million Commercial and Medicare Supplemental enrollees is contained in the MarketScan databases, which include inpatient and outpatient medical claims and enrollment data, such as member demographic information, eligibility and benefits data. Available data include service dates, provider reimbursement amounts, copayments and deductibles. Data records were de-identified and certified to be fully compliant with Health Insurance Portability and Accountability Act patient confidentiality requirements. Institutional review board approval to conduct this study was not required because the study uses only de-identified patient records and does not involve the collection, use or transmittal of individually identifiable data.
Patient selection criteria
The study population included patients starting treatment with apremilast or a biologic agent for psoriasis and/or PsA between 1 January 2014 and 30 June 2016. The date of the earliest apremilast or biologic treatment was the index date; biologic agents assessed included adalimumab, certolizumab, etanercept, golimumab, infliximab, secukinumab and ustekinumab; use of other biologics did not meet the time frames of the inclusion/exclusion criteria. Patients in the study population also had at least two medical claims with an International Classification of Diseases, Ninth or Tenth Revision, Clinical Modification diagnosis of psoriasis and/or PsA during the 12 months prior to or on the index date, were aged 18 years or older on the index date, and were continuously enrolled with medical and pharmacy benefits in the 12 months preceding and following the index date. Patients were excluded if they had other biologic-indicated autoimmune conditions, including ulcerative colitis, Crohn's disease, rheumatoid arthritis and other inflammatory polyarthropathies, ankylosing spondylitis and juvenile idiopathic arthritis, or cancer in the 12 months prior to or following the index date, or had multiple biologic medications administered on the index date. The study cohorts were propensity score matched based on age group, gender, health plan, payer, region, index year and urbanicity. The final analysis was limited to PsA patients with or without psoriasis who were naive to both apremilast and biologic agents; patients with psoriasis only were excluded from this analysis.
Outcome measures
Two outcomes were evaluated in this study: treatment persistence and adherence; and all-cause healthcare costs. Persistence was defined as the proportion of patients with no evidence of either discontinuation of the index medication (i.e., >60-day gap in therapy following exhaustion of the day's supply on the previous prescription claim) or a switch to apremilast or another biologic psoriasis and/or PsA medication prior to the end of the 12-month follow-up period. The duration of the post-index persistence period was defined as the total number of days from the index date to the earliest: discontinuation of the index medication based on a >60-day gap in therapy; or switch to another psoriasis and/or PsA treatment if the patient was nonpersistent on therapy; or end of the 12-month post-index period if the patient was persistent on therapy. The medication possession ratio (MPR) was computed as the sum of days’ supply for all prescription claims during the post-index persistence period divided by the total number of days in the post-index persistence period. The adherence rate was defined as the percentage of patients with an MPR ≥80%.
All-cause healthcare costs were measured per-patient per-month (PPPM) while patients were persistent on their index treatment and during the 12-month follow-up period. Costs were reported by service type (i.e., inpatient, outpatient medical [emergency department, office visits, laboratory and other outpatient services], outpatient pharmacy and total [sum of inpatient, outpatient and pharmacy costs]) and were calculated based on actual paid amounts of adjudicated claims, including insurer and health plan payments plus any patient cost sharing (e.g., copayments, deductibles, co-insurance). Costs associated with capitated arrangements were estimated using payment proxies computed based on paid claims at the procedure level using the MarketScan Commercial and Medicare Supplemental Databases. Costs were adjusted to 2016 dollars using the Medical Care Component of the Consumer Price Index.
Baseline clinical characteristics & covariates
Baseline clinical characteristics included age groups (18–24, 25–34, 35–44, 45–54, 55–64, 65–74 and ≥75 years), sex and insurance type (comprehensive, exclusive provider organization, health maintenance organization, point of service, preferred provider organization, point of service with capitation, consumer-driven health plan or other). Region according to the US Census Bureau geographic regions (e.g., Northeast, North, Central, South, West, unknown), urban/rural residence based on the metropolitan statistical area and index year was also reported. Identified comorbidities included anxiety, cardiovascular disease, depression, headache, hepatotoxicity, hypertension, serious infections, moderate or severe renal disease, osteoarthritis, osteoporosis, postmenopausal symptoms and Type 2 diabetes mellitus. Concomitant medications were antidiabetics, antidepressants, atypical antipsychotics, benzodiazepines, bisphosphonates/selective estrogen receptor modulators and opioids. Additional indicators were the Charlson Comorbidity Index, baseline total healthcare expenditures and psoriasis- and/or PsA-related medications and procedures (e.g., phototherapy, NSAIDs/COX-2 inhibitors, corticosteroids, systemic agents [acitretin, cyclosporine, methotrexate, sulfasalazine, leflunomide]).
Statistical analysis
For the descriptive statistics, all variables were summarized as means and standard deviations or counts and percentages. To evaluate for significant differences among continuous variables, t-tests and Wilcoxon rank-sum tests were used; for categorical variables, the chi-square test was used. Apremilast and biologic users were 1:2 nearest neighbor matched using propensity score methods with standardized differences and a caliper width of 0.25 standard deviation. Characteristics used for matching included age group, gender, health plan, payer, region, index year and urbanicity. To estimate the treatment effect on healthcare costs, generalized linear models with log link and γ error distribution were used to adjust for demographic characteristics, baseline clinical characteristics and baseline total costs. Models were fit separately by type of service (i.e., outpatient medical, outpatient pharmacy, total) while patients were persistent on their index treatment and during the entire 12-month post-index period.
Results
Patient characteristics
The final study population comprised 381 biologic-naive PsA patients who initiated apremilast compared with 761 biologic-naive PsA patients who initiated a biologic agent during the study period (Figure 1). The two cohorts had similar baseline patient demographics and clinical characteristics (apremilast vs biologics: mean age: 51.5 vs 50.8 years; female: 226 [59.3%] vs 458 [60.2%]; and mean Charlson Comorbidity Index score: 0.6 vs 0.6) (Table 1). Although the mean Charlson Comorbidity Index scores were similar, all the identified comorbidities were more prevalent among those initiating apremilast compared with those initiating a biologic agent (Table 1). A higher proportion of patients in the apremilast cohort than in the biologic cohort had cardiovascular disease (75 [19.7%] vs 114 [15.0%]; p < 0.05) and serious infection (127 [33.3%] vs 199 [16.1%]; p < 0.05).

Figure 1. Patient selection and attrition.
PsA: Psoriatic arthritis.
| Characteristic | Apremilast (n = 381) | Biologics† (n = 761) | p-value |
|---|---|---|---|
| Age | 51.5 (11.7) | 50.8 (11.3) | 0.363 |
| Sex: | |||
| – Male | 155 (40.7%) | 303 (39.8%) | 0.778 |
| – Female | 226 (59.3%) | 458 (60.2%) | 0.778 |
| Insurance plan type: | |||
| – HMO | 35 (9.2%) | 64 (8.4%) | 0.660 |
| – PPO | 253 (66.4%) | 532 (69.9%) | 0.228 |
| – CDHP | 40 (10.5%) | 73 (9.6%) | 0.629 |
| – Other/unknown | 53 (13.9%) | 92 (12.1%) | 0.383 |
| Geographic region: | |||
| – Northeast | 100 (26.2%) | 217 (28.5%) | 0.420 |
| – North central | 64 (16.8%) | 128 (16.8%) | 0.993 |
| – South | 172 (45.1%) | 332 (43.6%) | 0.626 |
| – West | 45 (11.8%) | 82 (10.8%) | 0.600 |
| Primary payer: | |||
| – Commercial | 342 (89.8%) | 703 (92.4%) | 0.135 |
| – Medicare | 39 (10.2%) | 58 (7.6%) | 0.135 |
| Index year: | |||
| – 2014 | 196 (51.4%) | 499 (65.6%) | < 0.001 |
| – 2015 | 185 (48.6%) | 262 (34.4%) | < 0.001 |
| Index medication: | |||
| – Apremilast | 381 (100.0%) | 0 (0.0%) | < 0.001 |
| – Adalimumab | 0 (0.0%) | 463 (60.8%) | < 0.001 |
| – Certolizumab | 0 (0.0%) | 18 (2.4%) | 0.003 |
| – Etanercept | 0 (0.0%) | 200 (26.3%) | < 0.001 |
| – Golimumab | 0 (0.0%) | 8 (1.1%) | 0.058 |
| – Infliximab | 0 (0.0%) | 41 (5.4%) | < 0.001 |
| – Secukinumab | 0 (0.0%) | 4 (0.5%) | 0.308 |
| – Ustekinumab | 0 (0.0%) | 27 (3.5%) | < 0.001 |
| Charlson Comorbidity Index | 0.65 (1.05) | 0.62 (1.13) | 0.685 |
| Baseline comorbid conditions: | |||
| – Cardiovascular disease | 75 (19.7%) | 114 (15.0%) | 0.044 |
| – Hypertension | 159 (41.7%) | 283 (37.2%) | 0.137 |
| – Serious infection‡ | 127 (33.3%) | 199 (26.1%) | 0.011 |
| – Osteoarthritis | 107 (28.1%) | 199 (26.1%) | 0.487 |
| – Type 2 diabetes mellitus | 62 (16.3%) | 119 (15.6%) | 0.782 |
| Concomitant medications: | |||
| – Antidepressants | 135 (35.4%) | 268 (35.2%) | 0.943 |
| – Benzodiazepines | 84 (22.0%) | 153 (20.1%) | 0.445 |
| – Opioids | 143 (37.5%) | 284 (37.3%) | 0.944 |
| Psoriasis- and PsA-related therapies: | |||
| – Systemic agents | 174 (45.7%) | 395 (51.9%) | 0.047 |
| – Acitretin | 6 (1.6%) | 4 (0.5%) | 0.093 |
| – Cyclosporine | 14 (3.7%) | 14 (1.8%) | 0.059 |
| – Methotrexate | 124 (32.5%) | 341 (44.8%) | < 0.001 |
| – Sulfasalazine | 38 (10.0%) | 57 (7.5%) | 0.152 |
| – Leflunomide | 17 (4.5%) | 28 (3.7%) | 0.522 |
| – NSAIDs/COX-2 inhibitors | 206 (54.1) | 396 (52.0) | 0.517 |
| – Corticosteroids | 323 (84.8) | 596 (78.3) | 0.009 |
| Preperiod total healthcare costs | $17,966 ($28,009) | $16,742 ($39,527) | 0.589 |
Values expressed as mean (standard deviation) or n (%).
†Biologic cohort included biologic-naive PsA patients initiating adalimumab, certolizumab, etanercept, golimumab, infliximab, secukinumab or ustekinumab.
‡Including acute upper respiratory tract infection, cellulitis, fungal infections, intestinal infections, Helicobacter pylori, herpes zoster, infectious arthritis, influenza, meningitis, methicillin-resistant Staphylococcus aureus, osteomyelitis, pneumonia, sepsis, tuberculosis, or urinary tract/renal infections.
CDHP: Consumer-driven health plan; HMO: Health maintenance organization; NSAID: Nonsteroidal anti-inflammatory drug; PPO: Preferred provider organization; PsA: Psoriatic arthritis; SD: Standard deviation.
Persistence & adherence
At 12 months post-index, treatment persistence was similar for PsA patients initiating apremilast compared with PsA patients initiating biologics (162 [42.5%] vs 365 [48.0%]; p = 0.082; Table 2). Similarly, the proportions of patients discontinuing based on a >60-day gap between treatments with or without a medication restart (203 [53.3%] vs 359 [47.2%]; p = 0.052) or switching to another biologic (16 [4.2%] vs 37 [4.9%]; p = 0.616) were similar for both groups. Persistence-based MPRs for patients initiating apremilast compared with patients initiating biologics were also nearly identical (0.87 vs 0.85, respectively; p = 0.056), as were adherence rates (apremilast vs biologics: 293 [76.9%] vs 557 [73.2%]; p = 0.175).
| Parameter | Apremilast (n = 381) | Biologics† (n = 761) | p-value |
|---|---|---|---|
| Persistent patients | |||
| – Yes | 162 (42.5%) | 365 (48.0%) | 0.082 |
| – No | 219 (57.5%) | 396 (52.0%) | 0.082 |
| Days in persistence period (all patients) | 225.9 (136.0) | 242.6 (131.0) | 0.046 |
| Days to nonpersistence | 124.7 (87.2) | 131.6 (82.6) | 0.194 |
| Reason for nonpersistence: | |||
| – 60-day gap | 203 (53.3%) | 359 (47.2%) | 0.052 |
| – 60-day gap with restart of index medication | 48 (12.6%) | 121 (15.9%) | 0.139 |
| – Switch biologics | 16 (4.2%) | 37 (4.9%) | 0.616 |
| Treatment to which a patient switches: | |||
| – Adalimumab | 0 (0.0%) | 0 (0.0%) | – |
| – Apremilast | 0 (0.0%) | 5 (0.7%) | 0.176 |
| – Certolizumab | 1 (0.3%) | 0 (0.0%) | 0.334 |
| – Etanercept | 6 (1.6%) | 14 (1.8%) | 0.748 |
| – Golimumab | 1 (0.3%) | 1 (0.1%) | 1.000 |
| – Infliximab | 1 (0.3%) | 2 (0.3%) | 1.000 |
| – Secukinumab | 2 (0.5%) | 1 (0.1%) | 0.260 |
| – Ustekinumab | 5 (1.3%) | 14 (1.8%) | 0.511 |
| Adherence while persistent on index agent: | |||
| – MPR | 0.87 (0.11) | 0.85 (0.15) | 0.056 |
| – Adherence, MPR ≥80% | 293 (76.9%) | 557 (73.2%) | 0.175 |
Values expressed as mean (standard deviation) or n (%).
†Biologic cohort included biologic-naive PsA patients initiating adalimumab, certolizumab, etanercept, golimumab, infliximab, secukinumab or ustekinumab.
MPR: Medication possession ratio; PsA: Psoriatic arthritis.
Costs
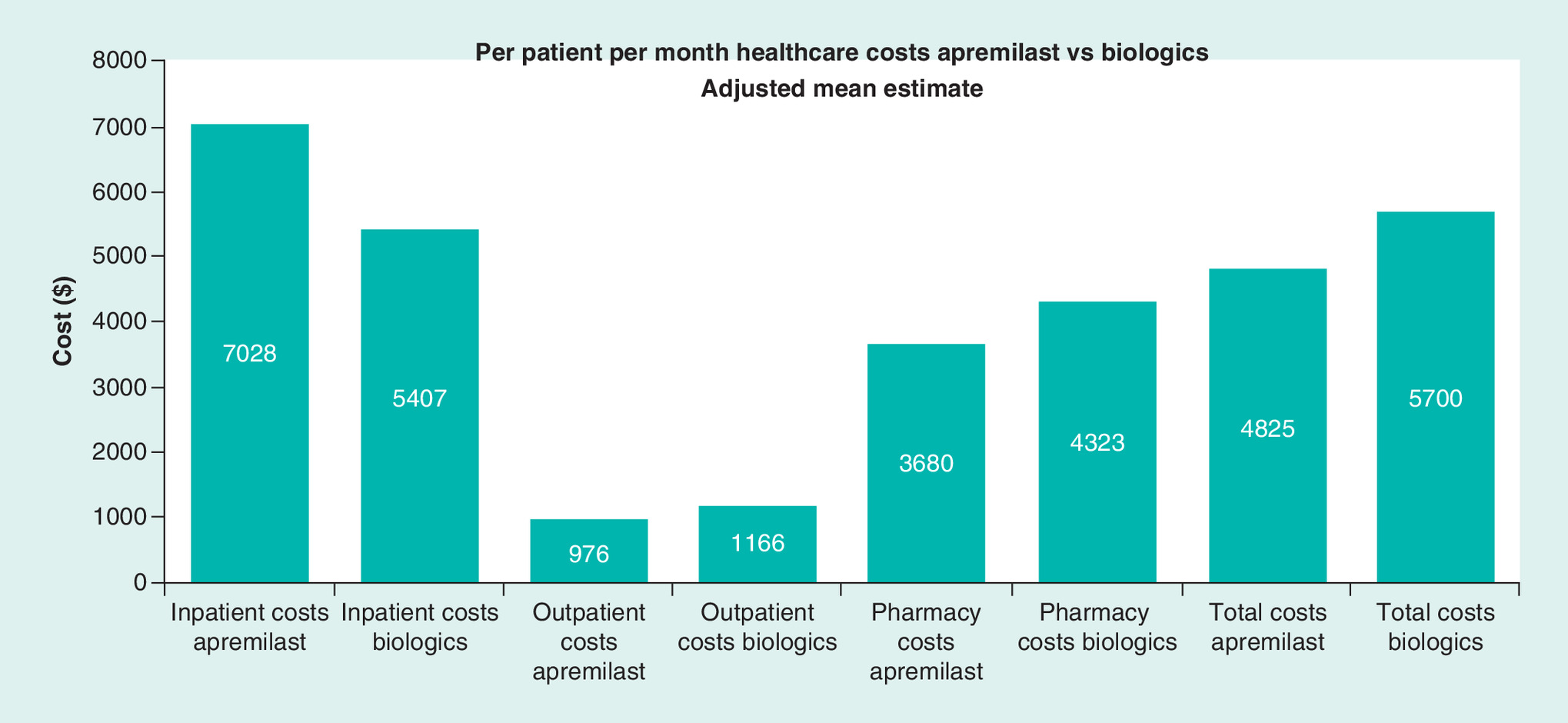
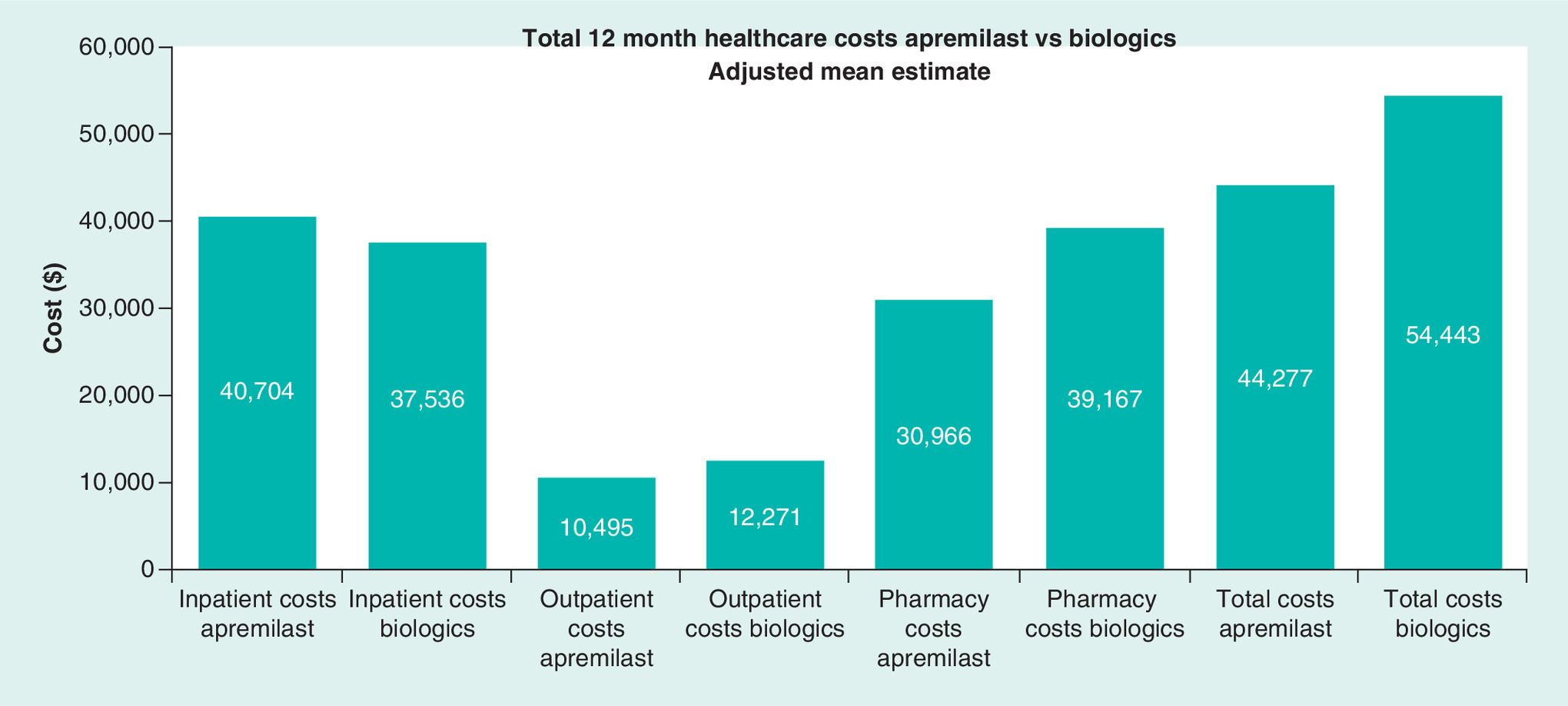
While persistent on therapy, apremilast versus biologic users had lower total PPPM costs ($875 difference) after adjusting for differences in baseline patient demographics and clinical characteristics using generalized linear models ($4825 vs $5700, p < 0.001; Figure 2), a difference mainly driven by outpatient pharmacy costs ($643 difference; p < 0.001). Total adjusted costs over 12 months were lower for apremilast patients compared with biologic patients ($44,277 vs $54,443; p < 0.001), again because of lower total outpatient pharmacy costs ($30,966 vs $39,167; p < 0.001; Figure 3).
Discussion
In this real-world study of commercially insured patients with PsA, we found similar treatment patterns and lower total healthcare costs for individuals initiating apremilast compared with those initiating a biologic agent. Treatment persistence, persistence-based MPR and adherence rates were similar for the two treatment groups. After adjusting for differences in baseline clinical characteristics using generalized linear models, apremilast users had lower adjusted PPPM total costs while persistent on their index therapy, as well as during the 12-month follow-up period, largely due to lower outpatient pharmacy costs, which accounted for three quarters of the total healthcare costs, and lower outpatient medical costs.
Our study of biologic-naive patients with PsA expands on a prior analysis that evaluated treatment patterns and healthcare costs among biologic-naive patients initiating treatment for psoriasis with apremilast or a biologic agent [19]. The current study used the same data source and similar methodology to study the PsA population specifically and complements the prior analysis, which excluded patients with PsA [19]. Patients with psoriasis who initiated apremilast had similar persistence rates, persistence-based MPR and adherence rates and significantly lower total and PPPM healthcare costs compared with patients who initiated biologics, which is consistent with the findings in the current study of patients with PsA [19]. In both analyses, the cost advantage with apremilast resulted from significantly lower outpatient pharmacy and medical costs during the 12-month follow-up period [19]. Together, these studies suggest that initiating treatment with apremilast can reduce costs for biologic-naive patients with psoriasis and/or PsA versus starting treatment with a biologic agent.
Direct annual healthcare costs related to PsA are estimated to be at least $2 billion (US dollars) [20], and total indirect costs account for half to three quarters of total costs, both of which increase with disease severity [20]. For patients with PsA, current treatment guidelines recommend first-line treatment with systemic oral disease-modifying antirheumatic drugs (DMARDs), followed by progression to highly effective yet costly biologic treatments [21]. Although clinical evidence suggests that these therapies are effective, very little real-world data are available regarding the patient experience, prescribing patterns, health resource utilization and overall healthcare costs comparing the various biologics to apremilast [20,22].
Oral apremilast has favorable tolerability in clinical trials [9–15], and this experience transfers to a real-world application, as evidenced by the observed persistence and adherence rates in this study. The present study also confers perspective on the current (2016 US dollars) total annual cost of PsA, which we estimated to be $54,433 annually for PsA patients initiating biologics and $44,277 annually for PsA patients initiating apremilast. Patients treated with apremilast have lower pharmacy costs in addition to lower outpatient medical costs and lower total healthcare costs, suggesting that savings may be related to reductions in expenditures for outpatient care or laboratory fees to monitor or treat adverse events that have been associated with biologics. Comparison to previous administrative-based claims analyses of patients with PsA is challenging due to differences in study methodology; however, our 1-year total direct cost results for PsA patients treated with biologics were consistent with previous publications that evaluated the total costs and total pharmacy costs for PsA patients treated with biologics [23,24]. Our 1-year total pharmacy cost estimates were slightly lower than one previous study that included apremilast and estimated the 1-year pharmacy costs per responding patient to be $53,704 for apremilast, $56,273 for adalimumab and $65,750 for etanercept (2014 US dollars) [25]. Results of this analysis may be useful for providers and payers in optimizing PsA care while reducing healthcare costs. We also observed numerically higher, but not significantly different, inpatient costs among apremilast users compared with biologic users (p = 0.121). Despite propensity score matching and comparable Charlson Comorbidity Index score in the matched apremilast and biologic cohorts, apremilast users had significantly more comorbidities at treatment initiation, including higher rates of cardiovascular disease and serious infections (Table 1). It is possible that this difference in comorbidity profile could account for the higher inpatient costs observed among apremilast users versus biologic users.
Although efficacy outcomes, including symptom relief, are not captured by claims databases and were not available for our analysis, measures of persistence and adherence are valid and informative markers of real-world treatment effectiveness, which can complement data from clinical trials [26]. Poor treatment adherence has been associated with worse outcomes for patients with chronic conditions overall [27,28]; patients with PsA often report poor adherence, and maximizing adherence is important for optimizing the therapeutic management of the disease [29–31]. Although no head-to-head studies have yet compared the efficacy of apremilast versus biologic agents, a network meta-analysis of clinical trial data has compared efficacy outcomes with apremilast, TNF-α inhibitors and interleukin inhibitors in patients with PsA [18].
This analysis may be subject to several limitations. Systematic differences between the study cohorts could account for differences in treatment patterns, healthcare utilization and costs. Therefore, differences between cohorts were controlled for by matching and by multivariate regressions; however, adjustment was limited to those characteristics that were measured from administrative claims. Administrative claims data do not provide clinical details such as disease activity or severity, and consequently, unmeasured imbalances in baseline disease activity or severity may contribute to the observed differences in healthcare costs. Results may be impacted by the possibility of underdiagnosis of PsA among patients insofar as we excluded PsA patients who were untreated or did not have a relevant diagnosis recorded on their medical claims. Additionally, our analysis was limited to medications licensed prior to the selection period and available for 12 months of post-index follow-up; thus, newer biologic DMARDs were not included (e.g., ixekizumab). Medication persistence and adherence measures were based on filled prescriptions, and it was assumed that patients took the medication as prescribed. The requirement that patients must have 12 months of continuous enrollment prior to and following the index date may mean that the experience of our study population differs from the broader population with PsA because it necessarily excluded those who no longer had health insurance. Therefore, the study population may appear to be healthier than the total population of patients in the database. As this study did not collect radiographic data, it was not possible to evaluate the effect of reducing the progression of joint damage on healthcare costs with apremilast versus biologic agents. Although the impact of treatment on radiographic progression has previously been studied for some, but not all, of these medications [32,33], they all have anti-inflammatory effects, and it is possible that they may provide radiographic benefits for patients with PsA. Additional research is needed to address differences in radiographic data between PsA treatments and to evaluate the impact on healthcare costs. Finally, the findings presented here may not be generalizable to PsA patients without commercial or private Medicare supplemental coverage.
Conclusion
In this large study of biologic-naive, commercially insured adults with PsA, adherence to treatment was similar for those initiating apremilast compared with those initiating a biologic agent, while initiation with apremilast resulted in lower total healthcare costs. Apremilast can be offered to patients before biologics, particularly those who prefer an oral option that does not require laboratory monitoring. While adherence to apremilast was good, further improving adherence to apremilast may help lower costs by avoiding more costly biologics.
The 2015 European League Against Rheumatism (EULAR) clinical practice guidelines for the pharmacologic management of PsA recommend oral drugs, such as apremilast, methotrexate, sulfasalazine and leflunomide, or biologics, such as adalimumab, etanercept or ustekinumab, which are given by injection or intravenous infusion [7].
This is a large US claims-based study of patients starting treatment with apremilast or a biologic agent for psoriasis and/or PsA between 1 January 2014 and 30 June 2016. Two outcomes were evaluated in this study: treatment persistence and adherence; and all-cause healthcare costs.
Similar treatment patterns and lower total healthcare costs were found for individuals initiating apremilast compared with those initiating a biologic agent.
Treatment persistence, persistence-based medication possession ratio and adherence rates were similar for the two treatment groups.
After adjusting for differences in baseline clinical characteristics using generalized linear models, apremilast users had lower adjusted per-patient per-month total costs while persistent on their index therapy, as well as during the 12-month follow-up period, largely due to lower outpatient pharmacy costs, which accounted for three quarters of the total healthcare costs, and lower outpatient medical costs.
Author contributions
This study was conceived and designed by SR Feldman, CL Pelletier, KL Wilson, RK Mehta, MA Brouillette and MM Bonafede. Data collection and statistical analysis were done by KL Wilson, MA Brouillette, D Smith and MM Bonafede. All authors contributed to the data interpretation, drafting, revision and approval of the submitted report, and all authors had full access to all of the data.
Acknowledgments
The authors gratefully acknowledge the research and editorial contributions of A Krug, MPH.
Financial & competing interests disclosure
This study was funded by Celgene Corporation. SR Feldman has received research support from and served as a consultant and speaker for AbbVie, Celgene Corporation, Eli Lilly, Janssen, Novartis and Ortho Dermatology. CL Pelletier and RK Mehta are employees of Celgene Corporation. KL Wilson, MA Brouillette, D Smith and MM Bonafede are employees of IBM Watson Health. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The authors state that all database records were de-identified and fully compliant with US patient confidentiality requirements, including the Health Insurance Portability and Accountability Act of 1996. Institutional review board approval to conduct this study was not required because the study uses only de-identified patient records and does not involve the collection, use or transmittal of individually identifiable data.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Ogdie A, Weiss P. The epidemiology of psoriatic arthritis. Rheum. Dis. Clin. North Am. 41(4), 545–568 (2015).
2.
Wittkowski KM, Leonardi C, Gottlieb A et al. Clinical symptoms of skin, nails, and joints manifest independently in patients with concomitant psoriasis and psoriatic arthritis. PLoS ONE 6(6), e20279 (2011).
3.
Truong B, Rich-Garg N, Ehst BD et al. Demographics, clinical disease characteristics, and quality of life in a large cohort of psoriasis patients with and without psoriatic arthritis. Clin. Cosmet. Investig. Dermatol. 8, 563–569 (2015).
• Provides direct clinical data on psoriatic arthritis and nonpsoriatic arthritis populations.
4.
Rosen CF, Mussani F, Chandran V et al. Patients with psoriatic arthritis have worse quality of life than those with psoriasis alone. Rheumatology (Oxford) 51(3), 571–576 (2012).
• Further demonstrates negative quality-of-life impact.
5.
Gladman DD, Antoni C, Mease P et al. Psoriatic arthritis: epidemiology, clinical features, course, and outcome. Ann. Rheum. Dis. 64(Suppl. 2), ii14–ii17 (2005).
6.
Haroon M, Kirby B, Fitzgerald O. High prevalence of psoriatic arthritis in patients with severe psoriasis with suboptimal performance of screening questionnaires. Ann. Rheum. Dis. 72(5), 736–740 (2013).
7.
Gossec L, Smolen JS, Gaujoux-Viala C et al. European League Against Rheumatism recommendations for the management of psoriatic arthritis with pharmacological therapies. Ann. Rheum. Dis. 71(1), 4–12 (2012).
•• Describes original accepted guidelines for treatment.
8.
Otezla, package insert. Celgene Corporation, NJ, USA.
9.
Zerilli T, Ocheretyaner E. Apremilast (Otezla): a new oral treatment for adults with psoriasis and psoriatic arthritis. P.T. 40(8), 495–500 (2015).
10.
Kavanaugh A, Mease PJ, Gomez-Reino JJ et al. Treatment of psoriatic arthritis in a Phase 3 randomized, placebo-controlled trial with apremilast, an oral phosphodiesterase 4 inhibitor. Ann. Rheum. Dis. 73(6), 1020–1026 (2014).
11.
Kavanaugh A, Mease PJ, Gomez-Reino JJ et al. Longterm (52-week) results of a Phase III randomized, controlled trial of apremilast in patients with psoriatic arthritis. J. Rheumatol. 42(3), 479–488 (2015).
12.
Edwards CJ, Blanco FJ, Crowley J et al. Apremilast, an oral phosphodiesterase 4 inhibitor, in patients with psoriatic arthritis and current skin involvement: a Phase III, randomised, controlled trial (PALACE 3). Ann. Rheum. Dis. 75(6), 1065–1073 (2016).
13.
Papp K, Reich K, Leonardi CL et al. Apremilast, an oral phosphodiesterase 4 (PDE4) inhibitor, in patients with moderate to severe plaque psoriasis: results of a Phase III, randomized, controlled trial (Efficacy and Safety Trial Evaluating the Effects of Apremilast in Psoriasis [ESTEEM 1]). J. Am. Acad. Dermatol. 73(1), 37–49 (2015).
14.
Paul C, Cather J, Gooderham M et al. Efficacy and safety of apremilast, an oral phosphodiesterase 4 inhibitor, in patients with moderate to severe plaque psoriasis over 52 weeks: a Phase III, randomized, controlled trial (ESTEEM 2). Br. J. Dermatol. 173(6), 1387–1399 (2015).
15.
Young M, Roebuck HL. Apremilast, an oral phosphodiesterase 4 (PDE4) inhibitor: a novel treatment option for nurse practitioners treating patients with psoriatic disease. J. Am. Assoc. Nurse Pract. 28(12), 683–695 (2016).
16.
Mayba JN, Gooderham MJ. Real-world experience with apremilast in treating psoriasis. J. Cutan. Med. Surg. 21(2), 145–151 (2017).
17.
Lee MP, Lii J, Jin Y et al. Patterns of systemic treatment for psoriatic arthritis in the US: 2004–2015. Arthritis Care Res. (Hoboken) 70(5), 791–796 (2018).
18.
Strand V, Elaine Husni M, Betts KA et al. Network meta-analysis and cost per responder of targeted immunomodulators in the treatment of active psoriatic arthritis. BMC Rheumatol. 2, 3 (2018).
19.
Feldman SR, Pelletier CL, Wilson KL et al. Real-world US healthcare costs of psoriasis for biologic-naive patients initiating apremilast or biologics. J. Comp. Eff. Res. 8(1), 45–54 (2019).
•• Sister publication on a related, but different, population using same methods as the present study.
20.
Palmer JB, Li Y, Herrera V et al. Treatment patterns and costs for anti-TNFα biologic therapy in patients with psoriatic arthritis. BMC Musculoskelet. Disord. 17, 261 (2016).
• Describes costs for related treatments for psoriatic arthritis.
21.
Gossec L, Smolen JS, Ramiro S et al. European League Against Rheumatism (EULAR) recommendations for the management of psoriatic arthritis with pharmacological therapies: 2015 update. Ann. Rheum. Dis. 75(3), 499–510 (2016).
•• Describes updated treatment guidelines for psoriatic arthritis.
22.
Atzinger CB, Guo JJ. Biologic disease-modifying antirheumatic drugs in a national, privately insured population: utilization, expenditures, and price trends. Am. Health Drug Benefits 10(1), 27–36 (2017).
23.
Chastek B, White J, Van Voorhis D et al. A retrospective cohort study comparing utilization and costs of biologic therapies and JAK inhibitor therapy across four common inflammatory indications in adult US managed care patients. Adv. Ther. 33(4), 626–642 (2016).
24.
Schwartzman S, Li Y, Zhou H et al. Economic impact of biologic utilization patterns in patients with psoriatic arthritis. Clin. Rheumatol. 36(7), 1579–1588 (2017).
• Describes the economic impact of biologic treatment patterns for psoriatic arthritis.
25.
Tencer T, Clancy Z, Zhang F. Cost per responder of apremilast versus etanercept and adalimumab in patients with active psoriatic arthritis [abstract]. Value Health 17(7), A376 (2014).
26.
Costanzo A, Malara G, Pelucchi C et al. Effectiveness end points in real-world studies on biological therapies in psoriasis: systematic review with focus on drug survival. Dermatology 234(1–2), 1–12 (2018).
27.
Osterberg L, Blaschke T. Adherence to medication. N. Engl. J. Med. 353(5), 487–497 (2005).
28.
De Geest S, Sabate E. Adherence to long-term therapies: evidence for action. Eur. J. Cardiovasc. Nurs. 2(4), 323 (2003).
29.
Gottlieb A, Gratacos J, Dikranian A et al. Treatment patterns, unmet need, and impact on patient-reported outcomes of psoriatic arthritis in the United States and Europe. Rheumatol. Int. 39(1), 121–130 (2019).
30.
Visalli E, Crispino N, Foti R. Multidisciplinary management of psoriatic arthritis: the benefits of a comprehensive approach. Adv. Ther. 36(4), 806–816 (2019).
31.
Xu Y, Sudharshan L, Hsu MA et al. Patient preferences associated with therapies for psoriatic arthritis: a conjoint analysis. Am. Health Drug Benefits 11(8), 408–417 (2018).
32.
Kavanaugh A, Ritchlin C, Rahman P et al. Ustekinumab, an anti-IL-12/23 p40 monoclonal antibody, inhibits radiographic progression in patients with active psoriatic arthritis: results of an integrated analysis of radiographic data from the Phase 3, multicentre, randomised, double-blind, placebo-controlled PSUMMIT-1 and PSUMMIT-2 trials. Ann. Rheum. Dis. 73(6), 1000–1006 (2014).
33.
van der Heijde D, Landewe RB, Mease PJ et al. Brief report: secukinumab provides significant and sustained inhibition of joint structural damage in a Phase III study of active psoriatic arthritis. Arthritis Rheumatol. 68(8), 1914–1921 (2016).
Information & Authors
Information
Published In
Copyright
© 2019 Steven R Feldman.
History
Received: 12 March 2019
Accepted: 12 April 2019
Published online: 13 May 2019
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Treatment patterns and costs among biologic-naive patients initiating apremilast or biologics for psoriatic arthritis. (2019) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2019-0034
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Vered Rosenberg, Howard Amital, Gabriel Chodick, Freddy Faccin, Omer Gendelman, Real-World Drug Survival of Biologics and Targeted Synthetic Disease-Modifying Anti-rheumatic Drugs Among Patients with Psoriatic Arthritis, Drugs & Aging, 10.1007/s40266-024-01136-7, 41, 8, (685-697), (2024).
- Amir Haddad, Nili Stein, Idit Lavi, Lisa Shynkar, Irina Bergman, Ilan Feldhamer, Arnon Dov Cohen, Walid Saliba, Devy Zisman, Treatment Persistence of Apremilast Among Patients with Psoriatic Arthritis, Biologics: Targets and Therapy, 10.2147/BTT.S425693, Volume 17, (129-136), (2023).
- M Elaine Husni, Eunice Chang, Michael S Broder, Caleb Paydar, Katalin Bognar, Pooja Desai, Yuri Klyachkin, Ibrahim Khilfeh, Biologic Initiation Rate in Systemic-Naïve Psoriatic Arthritis Patients Starting Treatment with Apremilast vs Methotrexate: 1-Year Retrospective Analysis of a US Claims Database, Open Access Rheumatology: Research and Reviews, 10.2147/OARRR.S342123, Volume 14, (123-132), (2022).
- Mwangi J Murage, Nicole Princic, Julie Park, William N Malatestinic, Baojin Zhu, Bilal Atiya, Scott A Kern, Keri B Stenger, Aubrey Trevelin Sprabery, Alexis Ogdie, Treatment patterns and health care costs among patients with psoriatic arthritis treated with biologic or targeted synthetic disease-modifying antirheumatic drugs, Journal of Managed Care & Specialty Pharmacy, 10.18553/jmcp.2022.28.2.206, 28, 2, (206-217), (2022).
- Mwangi J. Murage, Nicole Princic, Julie Park, William Malatestinic, Baojin Zhu, Bilal Atiya, Scott A. Kern, Keri B. Stenger, Aubrey Trevelin Sprabery, Alexis Ogdie, Real‐World Treatment Patterns and Healthcare Costs in Patients with Psoriatic Arthritis Treated with Ixekizumab: A Retrospective Study, ACR Open Rheumatology, 10.1002/acr2.11347, 3, 12, (879-887), (2021).
- David L Kaplan, Brian L Ung, Corey Pelletier, Chuka Udeze, Ibrahim Khilfeh, Marc Tian, Switch rates and total cost associated with apremilast and biologics in biologic-naive patients with psoriatic arthritis, Journal of Comparative Effectiveness Research, 10.2217/cer-2020-0285, 10, 12, (989-998), (2021).
- Jessica A. Walsh, Qian Cai, Iris Lin, Christopher D. Pericone, Soumya D. Chakravarty, Treatment Persistence and Adherence Among Patients With Psoriatic Arthritis Who Initiated Targeted Immune Modulators in the US: A Retrospective Cohort Study, Advances in Therapy, 10.1007/s12325-021-01687-w, 38, 5, (2353-2364), (2021).
- Andrea Picchianti-Diamanti, Francesca Romana Spinelli, Maria Manuela Rosado, Fabrizio Conti, Bruno Laganà, Inhibition of Phosphodiesterase-4 in Psoriatic Arthritis and Inflammatory Bowel Diseases, International Journal of Molecular Sciences, 10.3390/ijms22052638, 22, 5, (2638), (2021).