Comparative clinical effects and cost–effectiveness of maximum androgen blockade, docetaxel with androgen deprivation therapy and ADT alone for the treatment of mHSPC in China
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To compare the clinical effects and cost–effectiveness of maximum androgen blockade (MAB), docetaxel to androgen deprivation therapy (Doc-ADT) and ADT alone for the treatment of patients with metastatic hormone-sensitive prostate cancer in China. Methods: A network meta-analysis and a Markov model were adopted for effectiveness and economic evaluation. Results: The hazard ratios of overall survival and progression-free survival were 0.782 and 0.628 for Doc-ADT versus ADT alone; 0.897 and 0.824 for MAB versus ADT alone. Doc-ADT was cost-effective compared with MAB and ADT alone, with an incremental cost–effectiveness ratio of CNY 96,848 and CNY 67,758 per quality-adjusted life year, respectively. MAB was cost-effective compared with ADT alone, with an incremental cost–effectiveness ratio of CNY 137,487 per quality-adjusted life year. Conclusion: Doc-ADT is likely the optimal option from the perspective of both clinical outcomes and economic considerations.
Prostate cancer is the second most commonly diagnosed cancer in men worldwide. It ranks fifth and tenth in estimated deaths worldwide and in China, respectively [1]. The rate of death due to prostate cancer has been decreasing in the majority of more developed countries [2]. In contrast, rates of mortality from prostate cancer are rising in some Asian and Central and Eastern European countries, including China. In China, prostate cancer leads to 25,000 deaths annually, and the estimated 5-year survival rate is 54% [3,4]. Prostate cancer places a significant burden on healthcare systems. A study in the USA estimated that the average lifetime prostate cancer-related costs exceeded $30,000 [5].
According to both Chinese and Western guidelines, the recommended primary systemic treatment for men with metastatic prostate cancer is androgen deprivation therapy (ADT) alone, either by surgical castration or by medical suppression of testicular function with synthetic analogs of gonadotropin-releasing hormone, and addition of an antiandrogen to ADT, referred to as maximum androgen blockade (MAB) [6–8]. A meta-analysis of randomized trials comparing MAB and ADT alone reported that in advanced prostate cancer, MAB improved the 5-year survival rate by approximately 2–3%, but the range of uncertainty associated with this estimate was 0% to approximately 5% [9].
Recently, the addition of docetaxel to ADT (Doc-ADT) has been demonstrated to be superior to ADT alone and thus recommended for patients with newly diagnosed metastatic hormone-sensitive prostate cancer (mHSPC). In the E3805 (CHAARTED) trial [10,11], the addition of six cycles of Doc-ADT for mHSPC resulted in a significant increase in overall survival (OS) of 13.6 months (57.6 vs 44.0 months) and in progression-free survival (PFS) of 8.5 months (20.2 vs 11.7 months) relative to the OS and PFS with ADT alone. Similarly, in the STAMPEDE trial [12], the combination of six cycles of docetaxel with ADT in men commencing long-term ADT demonstrated a similar OS benefit over that from ADT alone, with OS increasing by a median of 10 months.
In China, Doc-ADT, MAB and ADT-alone therapies are commonly used for the treatment of advanced prostate cancer [13]. The antiandrogens prescribed as the addition to ADT in Chinese clinical practice include only flutamide and bicalutamide and not any of the other antiandrogens reported in Prostate Cancer Trialists’ Collaborative Group's study [9]. It is necessary to identify the differences in the clinical effects between flutamide and bicalutamide addition to ADT (referred to as MAB), Doc-ADT and ADT alone. Given the limited healthcare resources in China, the large number of patients with prostate cancer in this country, and the healthcare cost control policy recently announced by the Chinese government [14], it is crucial to determine the therapy that is the most cost-effective in the treatment of prostate cancer. However, to our knowledge, no studies have systematically compared the clinical effects and cost–effectiveness of these three therapies in China. Thus, the objective of this study is to compare the clinical effects of Doc-ADT, MAB and ADT alone based on a network meta-analysis (NMA) for the treatment of patients with mHSPC and to conduct a cost–effectiveness analysis (CEA) to identify the most cost-effective treatment strategy from the perspective of the Chinese healthcare system.
Network meta-analysis
Identification of eligible trials & data extraction
We conducted a systematic literature review up to 30 January 2018, to identify randomized controlled trials (RCTs) studies of adults with mHSPC in which the effects of the three treatments were compared. The commonly used antiandrogens in Chinese clinical practice are flutamide and bicalutamide; therefore, we searched for RCT studies of MAB therapy involving the addition of either antiandrogen to ADT. PubMed and Cochrane Library were searched for trials published in English; the Chinese databases CNKI and WanFang were searched for trials published in Chinese. Reference lists of identified studies and relevant systematic reviews were also screened to ensure the search strategies did not miss any relevant items. We searched both subject headings and text-word terms for ‘hormone-naive’, ‘hormone sensitive’, ‘castrate-naive’, ‘castrate sensitive’, ‘prostatic neoplasms’, ‘docetaxel’, ‘flutamide’, ‘bicalutamide’, ‘ADT’ and related and expanded terms including MeSH terms in combination with keyword searching. The primary outcomes were OS, PFS and treatment-related toxicity.
Two reviewers (S Qu, Y Liu) independently extracted all data. Disagreements were resolved by discussion and further inspection of articles. We used the Cochrane Collaboration's Risk of Bias tool to assess the risk of bias for each included study to inform the appropriateness of including studies in the NMA and assess the strength of the evidence.
Statistical methods
NMA is a meta-analysis in which multiple treatments (three or more) are compared using both direct comparisons of interventions within RCTs and indirect comparisons across trials based on a common comparator. The reported adjusted hazard ratios (HRs) of the clinical outcomes were our preferred outcome measures because they account for censoring, incorporate time-to-event information, and may be adjusted for covariables [15]. If HRs were not reported in a study, we used Wood's method [15] to incorporate the count statistics with HR statistics in a single analysis. The method avoids potential selection bias and misleading results caused by the selective inclusion of studies and accounts for the correlation among relative treatment effects in trials with more than two treatment groups [16]. Correlations among relative treatment effects in multi-arm trials are preserved by converting the relative treatment effect estimates (the HRs) to arm-specific outcomes (hazards). The deviance information criteria (DIC) was used to compare fit between the fixed- and random-effects models, with lower DIC values being preferred. In addition, sensitivity analyses were performed to determine the probability that each treatment will receive each possible ranking (first best, second best, etc.). The NMA was performed with WinBUGS 1.4.3 (MRC Biostatistics Unit, Cambridge, UK). We provide the WinBUGS codes for the NMA in the Supplementary Material.
NMA results
We identified nine trials [10,16–23] involving a total of 5168 patients: 951 (18%) patients receiving Doc-ADT, 1462 (28%) patients receiving MAB and 2755 (53%) patients receiving ADT alone. The contribution plot in Figure 1 presents the network of evidence. Noted that the STAMPEDE trial [23] includes about 30% patients with M0 disease, thus we only used the subgroup of patient in mHSPC in the analysis. An NMA flowchart and details of the included studies are provided in the Supplementary Material.
Overall survival & progression-free survival
All nine studies reported the count of deaths, and six studies [10,17,19,20,22,23] also reported HRs of death. Overall, there were a total of 3232 deaths: 1466 in the intervention arms (447 for patients receiving Doc-ADT; 1019 for patients receiving MAB) and 1767 in the ADT-alone arms. Six trials, involving 4556 enrolled patients, contributed to the PFS analysis [10,17,19,20,22,23]. Four of these trials [10,20,22,23] reported both HRs and the counts of progression, and the other two trials [17,19] reported only the counts of progression. We selected the fixed-effects model as the best model because it yielded a lower DIC value than the random-effects model for both OS (DIC: 15.077 for fixed-effects model, 16.106 for random-effects model) and PFS (DIC: 8.819 for fixed-effects model, 10.357 for random-effects model). The results are presented in Figure 2.
The pooled HR assessing OS was 0.782 (95% CI: 0.696–0.877) for Doc-ADT versus ADT alone, 0.897 (95% CI: 0.816–0.981) for MAB versus ADT alone, and 0.873 (95% CI: 0.743–1.002) for Doc-ADT versus MAB.
The pooled HR assessing PFS was 0.628 (95% CI: 0.566–0.695) for Doc-ADT versus ADT alone, 0.824 (95% CI: 0.701–0.962) for MAB versus ADT alone and 0.762 (95% CI: 0.616–0.907) for Doc-ADT versus MAB.
Sensitivity analysis of NMA results
We then conducted a sensitivity analysis of the NMA results. Figure 3 represents the uncertainty in the analysis, showing the probability that each treatment will receive each possible ranking (1st best, 2nd best, etc.). For OS, there was a very high probability (96%) that Doc-ADT is the most efficacious treatment; there was a 4% probability that it is the second-best treatment. For PFS, the probability of Doc-ADT being the most effective treatment was 100%.

Figure 1. Network of evidence and included studies.
Doc-ADT: Docetaxel to androgen deprivation therapy; MAB: Maximum androgen blockade.

Figure 2. Forest plot of NMA results for OS and PFS.
Doc-ADT: Docetaxel to androgen deprivation therapy; HR: Hazard ratio; MAB: Maximum androgen blockade; OS: Overall survival; PFS: Progression-free survival.
Treatment-related toxicity
We originally sought to examine the odds of treatment-related toxicity as measured by Grade 3–5 adverse events (AEs) in a post hoc analysis. However, we found substantial differences in definitions and ratings among studies and thus considered it inappropriate to perform an NMA on AEs.
Cost–effectiveness analysis
Following the comparisons of clinical effects performed with NMA, we conducted a CEA of the three treatment strategies from the perspective of the Chinese healthcare system.
Model overview
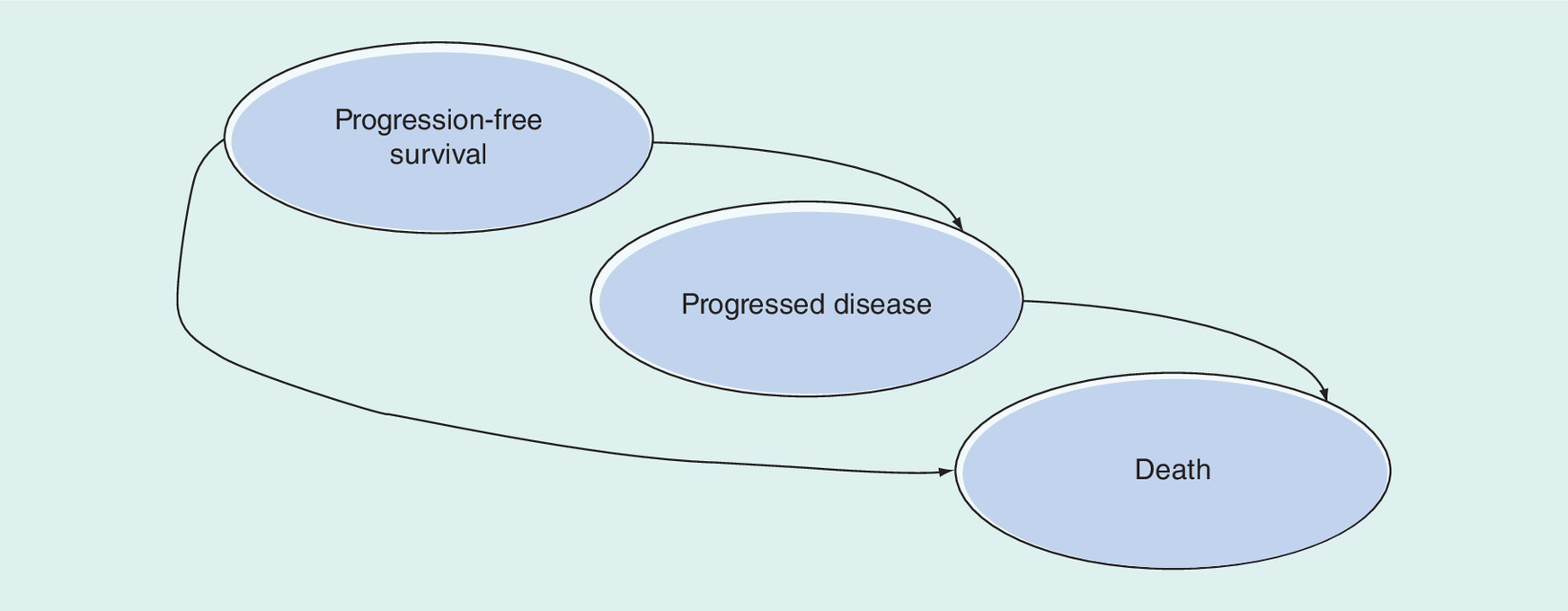
A decision-analytic model (Figure 4) was constructed to simulate the disease process of mHSPC and estimate the comparative costs of Doc-ADT, MAB and ADT-alone treatment regimens in a Chinese setting.
In the model, 1000 hypothetical mHSPC patients were simulated. Based on disease progression, we defined three health states in the model: PFS, progressed disease (PD) and death. The model began with 1000 patients in the PFS state. During each cycle, a patient in PFS could remain in PFS or advance to PD, whereas a patient in PD could remain in PD or advance to death. All the patients were followed until death. The length of each cycle was 1 month.
The key measure of effectiveness in the model was quality-adjusted life year (QALY). The main outcome measures were the incremental cost–effectiveness ratio (ICER), which was calculated as the incremental cost per additional QALY gained, and the incremental net-health benefit, which was calculated as follows: incremental net-health benefit (λ) = (μE1-μE0) - (μC1-μC0)/ λ = ΔE - ΔC/λ, where μCi and μEi are the cost and effectiveness, respectively, of the treatment arm (i = 1) and control arm (i = 0) [24] and λ is three-times the GDP per capita of China in 2017. Model development and data analysis were conducted using Microsoft® Excel 2013 (Microsoft, WA, USA).
Model input
Clinical input
The hazard ratios of disease progressing and death from NMA results were used as clinical effectiveness inputs in CEA. (Table 2) Since the follow-up times of all the included trials were limited, we extrapolated the survival curves of OS and PFS to a lifetime horizon by using Guyot methods [25]. In extrapolating survival curves, the reliability of the reconstructed data depends on the quality of the initial input and the level of information provided by the publication. We chose the ADT arm of the GETUG-AFU-15 trial [22] to reconstruct the survival curve because it had the largest sample size and provided the most detailed information among the articles.
We first reconstructed the individual patient data (IPD) of OS and PFS based on the survival analysis of the GETUG-AFU-15 trial's ADT arm [22]. Then, we fitted parametric models to the reconstructed IPD. The parametric distributions consisted of exponential, Weibull, log-normal and log-logistic distributions. Statistical tests were conducted to verify the relative and absolute validity of the findings based on the Akaike information criterion and the Bayesian information criterion values of the competing distributions. Next, we derived the equations for transition probabilities. The parameters were estimated from fitted distributions. Finally, the survival curves of the Doc-ADT and MAB arms were constructed based on the transition probabilities in the ADT arm and the HR value in the NMA. More details of the method followed are described in Guyot's paper [25]. The analyses were conducted in STATA software (version 14.0, StataCorp, TX, USA) and R 3.5.0.
The AEs rate was calculated based on the total number of reported AEs divided by the sum of the source population of each trial (Table 4).
Costs & resource use
Direct medical costs were considered, including drug and other treatment-related costs, as well as costs associated with AEs. All costs were discounted 3% annually (Table 3–4).
The unit costs of docetaxel and flutamide/bicalutamide from April 2017 to March 2018 were extracted from the IQVIA China Hospital Pharmaceutical Audit (CHPA) database. The China Hospital Pharmaceutical Audit database captures purchase statistics from over 9000 hospitals in China and reports the market prices at which the panel hospitals purchase products from wholesalers, distributors and manufacturers. Weighted average dosages from the included trials were calculated and entered into the cost analysis. Body surface area (BSA; cm2) was calculated as 0.0061 × height (cm) + 0.0128 × weight (kg) – 0.1529. An average height of 161.5 cm and an average weight of 61.8 kg, as reported in the literature [26], were used to represent a typical Chinese adult with terminal cancer.
In addition to therapy-specific costs, patients receiving docetaxel required hospitalization, whereas patients treated with MAB or ADT alone did not. There were also additional costs of inpatient bed fees and preventative chemotherapy drug costs for patients receiving docetaxel. All patients required laboratory tests including routine blood tests, blood biochemistry and liver function tests. We conducted interviews with clinicians from five major cities in China (Beijing, Shanghai, Wuhan, Chengdu and Guangzhou) to collect information on other drug costs (including monthly ADT costs and preventative chemotherapy drug costs), other medical costs (including inpatient bed fees and laboratory test costs) and the costs associated with AEs.
Postprogression treatment patterns
For patients with clinical progression, the postprogression treatment varied widely across the three therapies. Following consultation with a local clinic expert, we selected the second-line treatment pattern from the Doc-ADT and ADT-alone arms of the CHAARTED trial [10] and assumed that the pattern for the MAB arm was the same as that for the ADT-alone arm (Table 1). As the postprogression treatment option in CHAARTED trial such as cabazitaxel, sipuleucel-T, Radium 223 were not commonly used or accessed in China, we also assumed that there were no medical costs for those patients participating in the clinical trials.
| Study Arm | Post-progression treatment pattern |
|---|---|
| Doc-ADT | Doc 10 cycles: 22.7%; Abi: 44.1%; Clinical trials: 33.2% |
| MAB | Doc 10 cycles: 48%; Abi: 36.2%; Clinical trials: 15.8% |
| ADT alone | Doc 10 cycles: 48%; Abi: 36.2%; Clinical trials: 15.8% |
Doc-ADT: Docetaxel to androgen deprivation therapy; MAB: Maximum androgen blockade.
Utility
Sensitivity analysis
Several one-way sensitivity analyses were performed to test the robustness of the study results. As suggested and confirmed by a panel of local clinical experts, the costs of AEs varied by ± 50%, and those of the other parameters varied by ± 20%.
Probability sensitivity analyses were performed to test the effect of parameter uncertainty on the study results. Measures of distribution were obtained from the literature. We calculated the ICER by running 1000 Monte Carlo simulations to determine the proportions of simulations that were under predefined willingness-to-pay (WTP) thresholds of three-times the gross domestic product (GDP) per capita in 2017. Then, a cost–effectiveness acceptability curve (CEAC) was generated to summarize the uncertainty of the cost–effectiveness analysis and determine the proportions of simulations that were under the WTP thresholds.
CEA results
Based on the outputs of the regression analyses conducted on these IPD, we selected the best-fit log-logistic model to reconstruct the extrapolation of the survival curve of the ADT arm and used the results from the NMA to reconstruct the survival curves of the MAB and Doc-ADT arms. Figure 5 presents the number of patients in each health status simulated in the 1000-patient cohort model. As seen in figure, the Doc-ADT arm was associated with higher survival than were the MAB arm and ADT-alone arm.
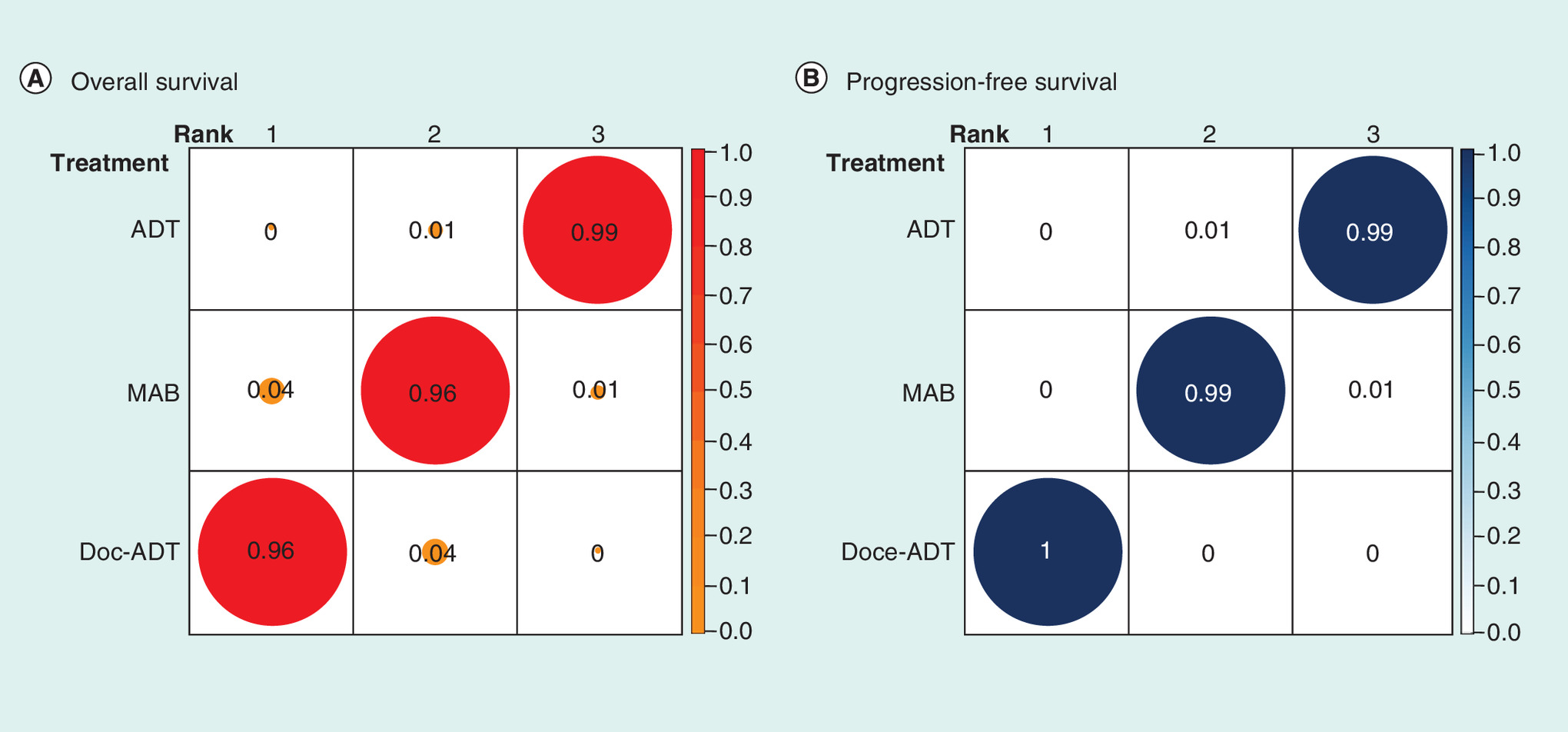
Figure 3. Probabilities of treatment rankings: (A) Overall survival and (B) progression-free survival.
Doc-ADT: Docetaxel to androgen deprivation therapy; MAB: Maximum androgen blockade; PFS: Progression-free survival.
Base-case results
Table 5 presents the base-case results. Doc-ADT, MAB and ADT alone were associated with 5.03, 4.44 and 4.02 QALY, at an average cost of CNY 424,342, 384,557 and 326,771, respectively, per patient. Doc-ADT was cost-effective, with an ICER of CNY 96,848 and CNY 67,758 per QALY gained compared with MAB and ADT alone, respectively. MAB was cost effective compared with ADT alone, with an ICER of CNY 137,487 per QALY gained.
| Parameter | Base-case value | Distribution | Range tested |
|---|---|---|---|
| Hazard ratio from NMA: | |||
| – PFS Doc-ADT vs ADT | 0.628 | Normal | ±20% |
| – PFS MAB vs ADT | 0.824 | Normal | ±20% |
| – OS Doc-ADT vs ADT | 0.782 | Normal | ±20% |
| – OS MAB vs ADT | 0.897 | Normal | ±20% |
| Utility: | |||
| – PFS | 0.76 | Beta | ±10% |
| – PD | 0.68 | Beta | ±10% |
Doc-ADT: Docetaxel to androgen deprivation therapy; MAB: Maximum androgen blockade; NMA: Network meta-analysis; OS: Overall survival; PD: Progressed disease; PFS: Progression-free survival.
| Parameter | Base-case value | Distribution | Range tested |
|---|---|---|---|
| Drug costs: | |||
| – Unit cost of docetaxel (cost per mg, CNY) | 73.62 | Gamma | ±20% |
| – Daily dosage of docetaxel (mg/m2) | 75.00 | Gamma | ±20% |
| – Average height (m) | 1.62 | Normal | ±20% |
| – Average weight (kg) | 61.80 | Normal | ±20% |
| – BSA (0.61 × height + 0.0128 × weight - 0.1529) | 1.62 | Normal | ±20% |
| – ADT cost per month (CNY) | 2,050.00 | Gamma | ±20% |
| – Weighted flutamide or bicalutamide cost per month (CNY) | 1,306.60 | Gamma | ±20% |
| – Preventive drugs for chemotherapy (CNY) | 620.00 | Gamma | ±20% |
| – Unit cost of abiraterone (cost per mg, CNY) | 0.58 | Gamma | ±20% |
| – Unit cost of prednisolone/prednisone (cost per mg, CNY) | 1.33 | Gamma | ±20% |
| – Daily dosage of abiraterone (mg) | 1000.00 | Gamma | ±20% |
| – Daily dosage of prednisolone (mg) | 5.00 | Gamma | ±20% |
| Other medical costs: | |||
| – Inpatient bed fee for chemotherapy (CNY) | 318.00 | Gamma | ±20% |
| – Laboratory test costs (CNY) | 500.00 | Gamma | ±20% |
ADT: Androgen deprivation therapy; BSA: Body surface area; CNY: Chinese yuan.
| AE | Rate | Unit cost (CNY) | ||
|---|---|---|---|---|
| Doc-ADT | MAB | ADT | ||
| Gynecomastia | – | 22.0% | 8.0% | 100 |
| Hot flushes | – | 19.3% | 16.7% | 20 |
| Pain | – | 59.0% | 63.0% | 74 |
| Diarrhea | 1.0% | 2.7% | 2.4% | 31 |
| Hepatic dysfunction | – | 2.4% | 1.9% | 18,000 |
| Nausea | – | 2.2% | 2.5% | 252 |
| Vomiting | – | 1.8% | 1.9% | 252 |
| Anemia | 1.30% | 8.5% | 5.4% | 272 |
| Neuropathy | 1% | 1.0% | 2.0% | 376 |
| Gastrointestinal disorders | – | 2.0% | 1.0% | 31 |
| Constipation | – | 7.0% | 1.0% | 84 |
| Musculoskeletal system disorders | – | 1.0% | 2.0% | 100 |
| Psychiatric disorders | – | 3.0% | 5.0% | 100 |
| Impotence | – | 4.0% | 4.0% | 100 |
| Fatigue | 4.1% | – | – | 540 |
| Allergic reaction | 2.1% | – | – | 75 |
| Stomatitis | 1.0% | – | – | 74 |
| Thromboembolism | 0.8% | – | – | 1794 |
| Sudden death | 0.3% | – | – | 3200 |
| Thrombocytopenia | 0.3% | – | – | 3518 |
| Neutropenia | 12.1% | – | – | 721 |
| Febrile neutropenia | 6.2% | – | – | 1787 |
| Infection with neutropenia | 2.3% | – | – | 14,764 |
ADT: Androgen deprivation therapy; AE: Adverse event; CNY: Chinese yuan; Doc-ADT: Docetaxel to androgen deprivation therapy; MAB: Maximum androgen blockade.
| Outcomes | Doc-ADT | MAB | ADT alone | Difference | ||
|---|---|---|---|---|---|---|
| Doc-ADT vs ADT | MAB vs ADT | Doc-ADT vs MAB | ||||
| Drug costs | ¥158,501 | ¥126,013 | ¥59,676 | ¥98,825 | ¥66,337 | ¥32,489 |
| Other medical costs | ¥31,647 | ¥18,771 | ¥14,549 | ¥17,098 | ¥4,222 | ¥12,876 |
| AE costs | ¥816 | ¥551 | ¥353 | ¥463 | ¥198 | ¥265 |
| Postprogression treatment cost | ¥233,378 | ¥239,223 | ¥252,194 | - ¥18,815 | - ¥12,971 | - ¥5,845 |
| Total cost | ¥424,342 | ¥384,557 | ¥326,771 | ¥97,571 | ¥57,786 | ¥39,785 |
| LY | 6.87 | 6.16 | 5.63 | 1.25 | 0.54 | 0.71 |
| QALY | 5.03 | 4.44 | 4.02 | 1.01 | 0.42 | 0.59 |
| ICER | 96,848 | 137,487 | 67,758 | |||
| INHB | 2.64 | 2.28 | 2.18 | 0.46 | 0.10 | 0.36 |
AE: Adverse event; Doc-ADT: Docetaxel to androgen deprivation therapy; ICER: Incremental cost–effectiveness ratio; INHB: Incremental net-health benefit; LY: Life year; MAB: Maximum androgen blockade; QALY: Quality-adjusted life year.
Sensitivity analysis results
Sensitivity analyses were performed to examine the stability and robustness of the results. The tornado diagrams in Figure 6 show that the HR values from the NMA and the utility values had significant impacts on the lifetime results. Other parameters, such as drug dosage and unit cost, had little impact on the results.

Figure 5. Number of patients in each health status simulated in the model.
Doc-ADT: Docetaxel to androgen deprivation therapy; PD: Progressed disease; PFS: Progression-free survival; MAB: Maximum androgen blockade.
Figure 7 shows the probability of being cost-effective at different WTP values in the form of CEACs. When the WTP threshold was set to 179,800 CNY per QALY gained, which is three-times the GDP per capita of China in 2017, the model predicts a 96.4% probability that the Doc-ADT is a cost-effective strategy compared with either MAB or ADT alone.
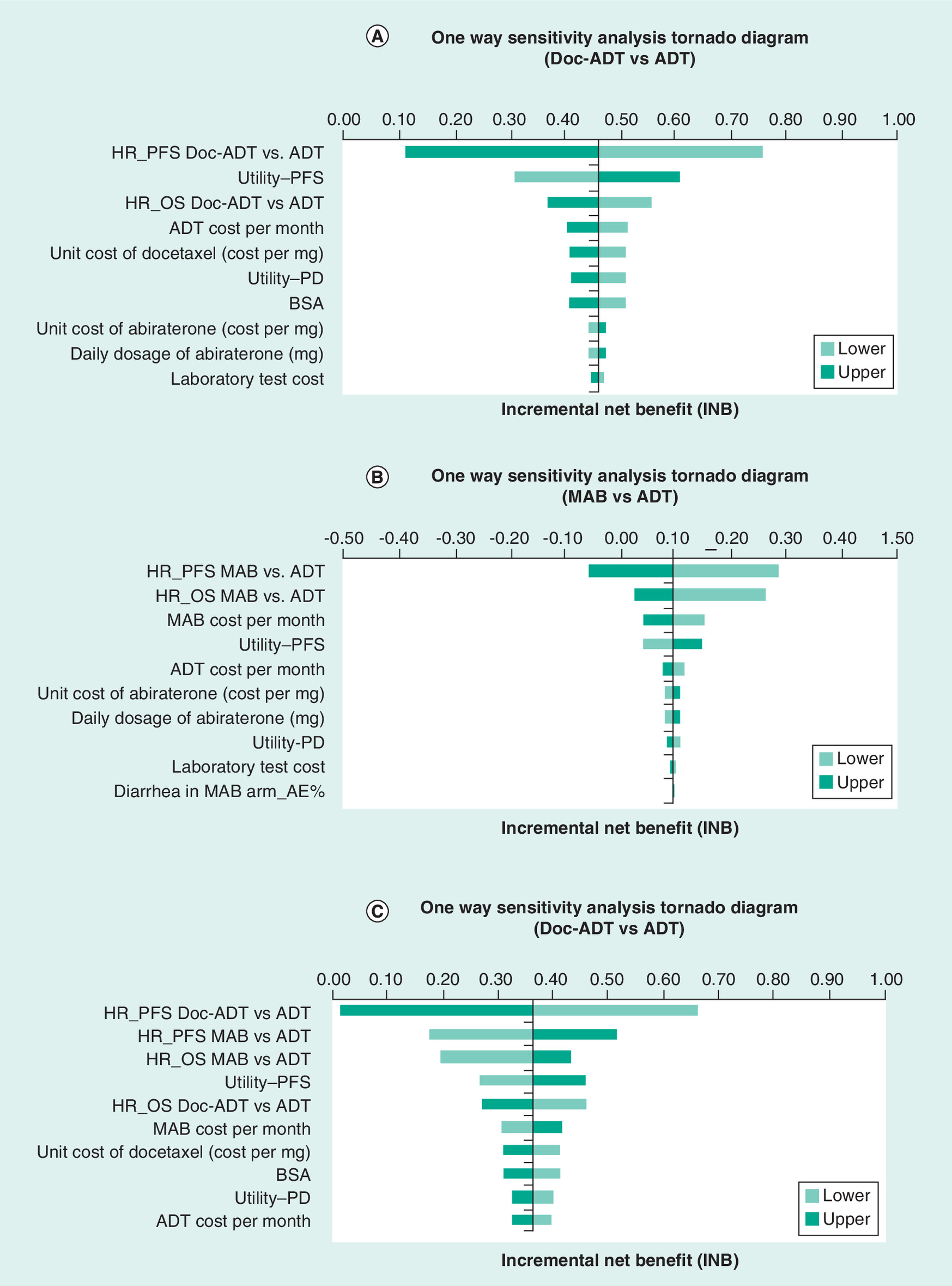
Figure 6. One-way sensitivity analysis tornado diagrams for a lifetime horizon: (A) Doc-ADT versus ADT; (B) MAB versus ADT; (C) Doc-ADT versus MAB.
ADT: Androgen deprivation therapy; BSA: Body surface area; Doc: Docetaxel; HR: HR: Hazard ratio; MAB: Maximum androgen blockade; PD: Progressed disease; PFS: Progression-free survival.
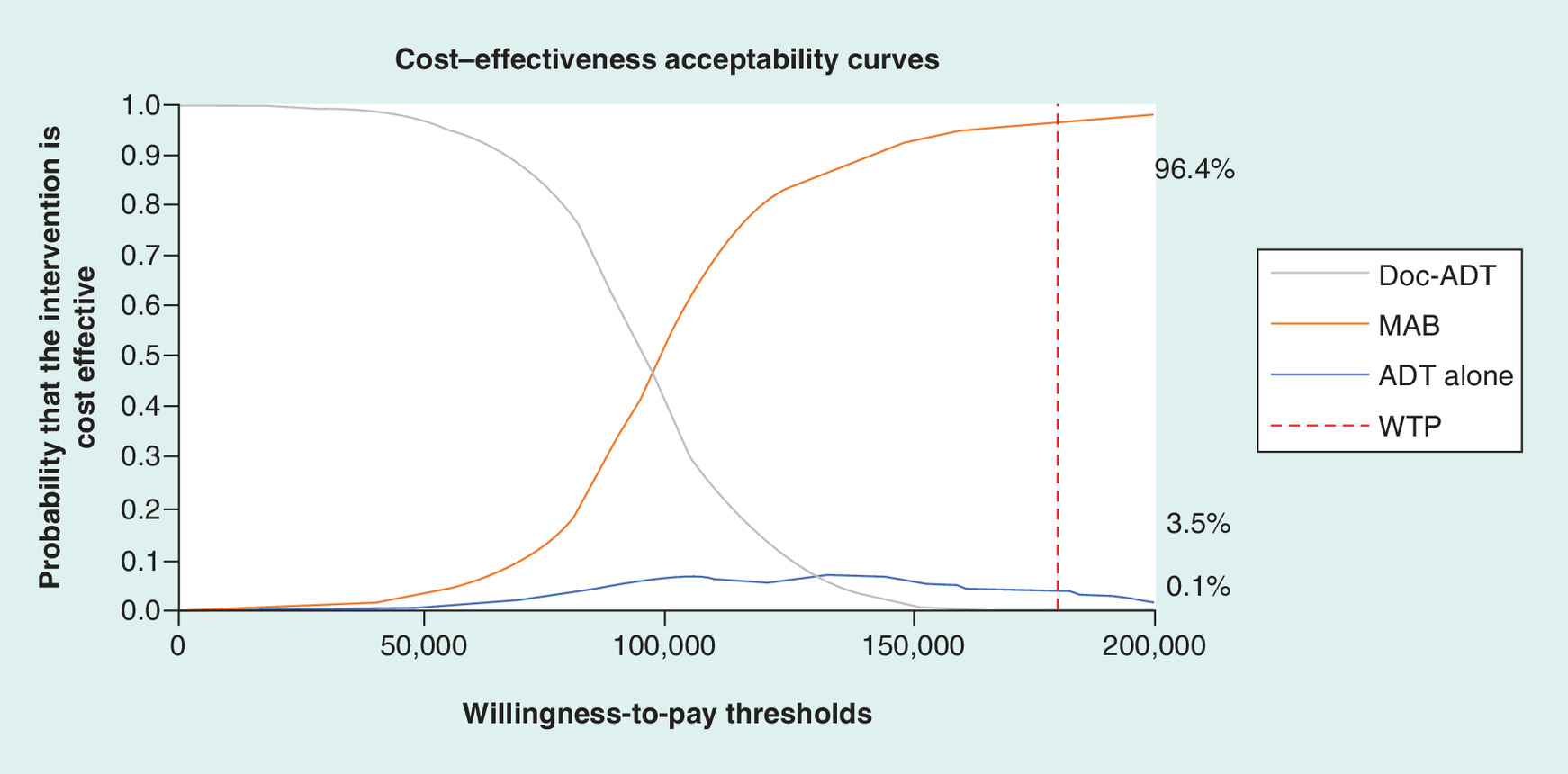
Figure 7. Cost–effectiveness acceptability curves for a lifetime horizon.
ADT: Androgen deprivation therapy; Doc: Docetaxel; MAB: Maximum androgen blockade; WTP: Willingness-to-pay threshold.
Discussion
No systematic comparison of the clinical effects and cost–effectiveness among Doc-ADT, MAB and ADT-alone therapies has been reported to date, and this study, to the best of our knowledge, is the first to compare the treatment effects of these three therapies.
We searched the RCT literatures and conducted an NMA on the log-hazard scale, combining count and hazard-ratio statistics in a single analysis. By incorporating all data presentations in a single analysis, we avoided the potential selection bias associated with analyzing a single statistic and the potential for misleading results associated with conducting separate analyses for different summary statistics. We assessed the heterogeneity among the studies included in the NMA. The presence of metastatic disease at the time of the diagnosis was very similar among the studies, as were ECOG performance score, age and previous treatment records. The findings suggested that Doc-ADT is superior to both MAB and ADT alone and that MAB is superior to ADT alone in improving OS and PFS. The sensitivity analyses indicated that the probability that Doc-ADT is the most effective treatment is 96.4%.
There was some variation in the median time of follow-up among the included studies (from 32.5 to 86.4 months). Since relative HRs were used, this variation in median follow-up time was controlled for and thus did not affect the NMA results. We found some interesting trends in median OS in the ADT arm. For studies conducted before the 2000s [16,17,19–21], the median OS of the ADT arm ranged from 26.4 to 31 months, whereas for studies conducted after the 2000s [10,18,22,23], it ranged from 47.2 to 76.8 months. We attribute this extension of survival time to improvements in prostate screening programs for the early detection of disease, improved medical and nursing conditions for orchiectomy surgery and use of several novel drugs, docetaxel, cabazitaxel, abiraterone acetate, enzalutamide, etc.
In addition to their clinical effects, the cost–effectiveness of therapies is a crucial factor to consider in selecting treatment strategies in China. Our findings suggest that among the treatments evaluated here, Doc-ADT is the most cost-effective option for the treatment of mHSPC. The extensive sensitivity analyses, both one-way and probabilistic, indicate that the results are robust.
The cost–effectiveness of prostate cancer treatments has been assessed in multiple countries in recent years. The majority of the studies involved evaluated the cost–effectiveness of prostate screening programs or the treatment of castration-resistant prostate cancer. We found two studies that assessed the same mHSPC population as ours. One of the two studies [29] led to conclusions similar to ours. It assessed the cost–effectiveness of chemohormonal therapy in patients with metastatic, hormone-sensitive prostate cancer and nonmetastatic, high-risk prostate cancer. In patients with metastatic disease, there was an increase of 0.53 QALY with the addition of Doc-ADT compared with ADT alone. The incremental cost per patient was $11,228.55 per QALY. The Doc-ADT arm was considered cost-effective in 80% of the scenarios evaluated in the probabilistic sensitivity analysis. The second study, by Zheng et al. [30], drew the conflicting conclusion that Doc-ADT was not a cost-effective treatment compared with ADT alone for mHSPC in the Chinese healthcare setting. There are several potential reasons that could explain the discrepancy. First, the monthly postprogression treatment cost in Zheng et al. study was $172.90. However, they reported that the postprogression treatment included abiraterone, which is a very expensive drug; thus, the monthly cost could not have been that low. Our analysis showed that the postprogression treatment cost for the Doc-ADT arm was less than that of the ADT arm. We suspect that the postprogression treatment cost may have been underestimated in the analysis by Zheng et al., resulting in an underestimate of the cost savings in the Doc-ADT arm. Second, the transition cycle in the Zheng et al. model is 1 year, which might be too long to simulate disease progression in patients with advanced cancer. The most commonly used cycle lengths for advanced cancer are 1 month and 21 days. Third, the clinical information used in Zheng et al. analysis was from one trial [11], and the transition probability was calculated with the simple formula p = 1-e-R; however, the authors did not state why the distribution was exponential and how the simulations extrapolated. In contrast, in our analysis, we extrapolated the survival curve to the lifetime horizon via the Guyot method, and the parameters were estimated from the best-fit distributions with the lowest Akaike information criterion and the Bayesian information criterion values based on the NMA. Finally, Zheng et al. analysis used cost data from a single Chinese hospital, which are not necessarily representative of larger regions or cities in China. The varied cost information and multiple sources of clinical data incorporated in the present study give us confidence in our results.
Some limitations of our analysis should be noted. Although NMA has been used and validated for comparing the effectiveness of three treatment arms, it is a surrogate for head-to-head treatment comparisons. Studies are needed to further assess the efficacy of the three treatments. In addition, due to the lack of published data sources for standard treatment costs and AE costs, we interviewed clinical experts to estimate the AE and other medical costs. Although we selected several main hospitals in different regions of China to obtain a representative sample, the accuracy and representativeness of these cost estimates need to be evaluated. Nonetheless, in the sensitivity analyses, where AE cost was varied within a broad range of ±50%, the cost of AE was found to have a very limited impact on the study results.
Conclusion
Among the three investigated therapies, Doc-ADT was associated with the best OS and PFS outcomes in mHSPC patients. The CEA revealed that among the therapies, Doc-ADT is the most cost-effective alternative in China. The findings of this study, which are based on local data, can inform treatment decision makers at both the level of the individual patient and the policy level.
•
In total, 5168 patients with metastatic hormone-sensitive prostate cancer from nine random control trials were included in our network meta-analysis (NMA): 951 (18%) patients receiving docetaxel to androgen deprivation therapy (Doc-ADT), 1462 (28%) patients receiving maximum androgen blockade (MAB) and 2755 (53%) patients receiving ADT alone.
•
The NMA results showed that: the hazard ratios of overall survival and progression-free survival were 0.782 (95% CI: 0.696–0.877) and 0.628 (95% CI: 0.566–0.695) for Doc-ADT versus ADT alone; 0.897 (95% CI: 0.816–0.981) and 0.824 (95% CI: 0.701–0.962) for MAB versus ADT alone; and 0.873 (95% CI: 0.743–1.002) and 0.762 (95% CI: 0.616–0.907) for Doc-ADT versus MAB.
•
A Markov model with a lifetime horizon was adopted for economic evaluation. The comparative clinical effect inputs came from the results of NMA.
•
The cost–effectiveness analysis showed that Doc-ADT was cost-effective compared with MAB and ADT alone, with an incremental cost–effectiveness ratio of CNY 96,848 and CNY 67,758 quality-adjusted life year, respectively. MAB was cost-effective compared with ADT alone, with an incremental cost–effectiveness ratio of CNY 137,487 per quality-adjusted life year.
•
Doc-ADT is likely the optimal option from the perspective of both clinical outcomes and economic considerations, followed by MAB.
Supplementary data
To view the supplementary data that accompany this paper please visit the journal website at: www.futuremedicine.com/doi/full/10.2217/cer-2018-0133
Author contributions
All the authors contributed significantly to the collection and analysis of data, reviewed and edited the manuscript, and agree to its content and submission for publication. The authors are fully responsible for all content and editorial decisions. M Liu, W Jiang and X Yao provided advice, guidance and other contributions to this paper throughout its development; S Qu and Y Liu were responsible for literature review and data analysis process.
Financial & competing interests disclosure
This study was funded by Sanofi China. X Yao is an employee of Sanofi China. S Qu and Y Liu are employees of IQVIA China. IQVIA China received research funding from Sanofi China. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
American Journal Experts assisted the article polishing process, funded by Sanofi China.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (suppl_file.docx)
- Download
- 238.58 KB
References
Papers of special note have been highlighted as: • of interest
1.
Torre LA, Bray F, Siegel RL, Ferlay J, Lortet‐Tieulent J, Jemal A. Global cancer statistics, 2012. CA Cancer J. Clin. 65(2), 87–108 (2015).
2.
Taitt HE. Global trends and prostate cancer: a review of incidence, detection, and mortality as influenced by race, ethnicity, and geographic location. Am. J. Mens Health 12(6), 1807–1823 (2018).
3.
Chen W, Zheng R, Baade PD et al. Cancer statistics in China, 2015. CA Cancer J. Clin. 66(2), 115–132 (2016).
4.
Han S, Zhang S, Chen W, Li C. Analysis of the status and trends of prostate cancer incidence in China. Chin. Clin. Oncol. 18(4), 330–334 (2013).
5.
Stokes ME, Ishak J, Proskorovsky I, Black LK, Huang Y. Lifetime economic burden of prostate cancer. BMC Health Serv. Res. 11(1), 349 (2011).
6.
Heidenreich A, Bastian PJ, Bellmunt J et al. EAU guidelines on prostate cancer. Part II: treatment of advanced, relapsing, and castration-resistant prostate cancer. Eur. Urol. 65(2), 467–479 (2014).
7.
National Health Commission of the People's Republic of China. Guidelines for the diagnosis and treatment of prostate cancer (2018). www.nhc.gov.cn/
8.
NCCN Guidelines for Patients, Prostate Cancer, Version 1. 2016. 2018 (April 27) (2016). www.nccn.org/patients/guidelines/prostate/
9.
Prostate Cancer Trialists Collaborative Group. Maximum androgen blockade in advanced prostate cancer: an overview of the randomised trials. Lancet 355(9214), 1491–1498 (2000).
10.
Sweeney C, Chen Y, Liu G et al. Long term efficacy and QOL data of chemohormonal therapy (C-HT) in low and high volume hormone naïve metastatic prostate cancer (PrCa): E3805 CHAARTED trial. Ann. Oncol. 27(Suppl. 6), vi243–vi265 (2016).
11.
Sweeney CJ, Chen Y-H, Carducci M et al. Chemohormonal therapy in metastatic hormone-sensitive prostate cancer. N. Engl. J. Med. 373(8), 737–746 (2015).
12.
James N, Mason M. Docetaxel and/or zoledronic acid for hormone-naïve prostate cancer: first survival results from STAMPEDE. J. Clin. Oncol. 33(33), 5001 (2015).
13.
Ye D. Chinese experts consensus on the treatment of metastatic prostate cancer 2018 edition. Chin. J. Surg. 56(9), 646–652 (2018).
14.
Liu GG, Vortherms SA, Hong X. China's health reform update. Ann. Rev. Public Health 38, 431–448 (2017).
15.
Woods BS, Hawkins N, Scott DA. Network meta-analysis on the log-hazard scale, combining count and hazard ratio statistics accounting for multi-arm trials: a tutorial. BMC Med. Res. Methodol. 10(1), 54 (2010).
• Provides the instruction and WinBUGS codes for network meta-analysis.
16.
Zalcberg J, Raghaven D, Marshall V, Thompson P. Bilateral orchidectomy and flutamide versus orchidectomy alone in newly diagnosed patients with metastatic carcinoma of the prostate – an Australian multicentre trial. Br. J. Urol. 77(6), 865–869 (1996).
17.
Eisenberger MA, Blumenstein BA, Crawford ED et al. Bilateral orchiectomy with or without flutamide for metastatic prostate cancer. N. Engl. J. Med. 339(15), 1036–1042 (1998).
18.
Akaza H, Hinotsu S, Usami M et al. Combined androgen blockade with bicalutamide for advanced prostate cancer: long‐term follow‐up of a Phase 3, double‐blind, randomized study for survival. Cancer 115(15), 3437–3445 (2009).
19.
Crawford ED, Blumenstein BA, Goodman PJ et al. Leuprolide with and without flutamide in advanced prostate cancer. Cancer 66, 1039–1044 (1990).
20.
Denis L, Keuppens F, Smith P et al. Maximal androgen blockade: final analysis of EORTC Phase III trial 30853. Eur. Urol. 33(2), 144–151 (1998).
21.
Tyrrell CJ, Altwein J, Klippel F et al. Comparison of an LH–RH analogue (goeserelin acetate, ‘Zoladex’) with combined androgen blockade in advanced prostate cancer: final survival results of an international multicentre randomized–trial. Eur. Urol. 37(2), 205–211 (2000).
22.
Gravis G, Boher J-M, Joly F et al. Androgen deprivation therapy (ADT) plus docetaxel versus ADT alone in metastatic non castrate prostate cancer: impact of metastatic burden and long-term survival analysis of the randomized Phase III GETUG-AFU15 trial. Eur. Urol. 70(2), 256–262 (2016).
• The reconstructed individual inpatient data of overall survival and progression-free survival were based on the survival analysis of Gravis 2016.
23.
James ND, Sydes MR, Clarke NW et al. Addition of docetaxel, zoledronic acid, or both to first-line long-term hormone therapy in prostate cancer (STAMPEDE): survival results from an adaptive, multiarm, multistage, platform randomised controlled trial. Lancet 387(10024), 1163–1177 (2016).
24.
Craig BA, Black MA. Incremental cost–effectiveness ratio and incremental net-health benefit: two sides of the same coin. Expert Rev. Pharmacoecon. Outcomes Res. 1(1), 37–46 (2001).
25.
Guyot P, Ades A, Ouwens MJ, Welton NJ. Enhanced secondary analysis of survival data: reconstructing the data from published Kaplan-Meier survival curves. BMC Med. Res. Methodol. 12(1), 9 (2012).
• Provides the methods and codes for reconstructing individual patient data from survival curve.
26.
Qin S, Kruger E, Tan SC, Cheng S, Wang N, Liang J. cost–effectiveness analysis of FOLFOX4 and sorafenib for the treatment of advanced hepatocellular carcinoma in China. Cost Eff. Resour. Alloc. 16(1), 29 (2018).
27.
Heijnsdijk EA, Wever EM, Auvinen A et al. Quality-of-life effects of prostate-specific antigen screening. N. Engl. J. Med. 367(7), 595–605 (2012).
28.
Stewart ST, Lenert L, Bhatnagar V, Kaplan RM. Utilities for prostate cancer health states in men aged 60 and older. Medical Care 347–355 (2005).
29.
Aguiar Jr PN, Barreto CMN, Gutierres BDS, Tadokoro H, Lopes Jr GDL. Cost–effectiveness of chemohormonal therapy in patients with metastatic hormone-sensitive and non-metastatic high-risk prostate cancer. Einstein (São Paulo) 15(3), 349–354 (2017).
30.
Zheng H, Wen F, Wu Y, Wheeler J, Li Q. Cost–effectiveness analysis of additional docetaxel for metastatic hormone‐sensitive prostate cancer treated with androgen‐deprivation therapy from a Chinese perspective. Eur. J. Cancer Care 26(6), e12505 (2017).
• A Chinese cost–effectiveness study that accesses the same metastatic hormone-sensitive prostate cancer population as ours, but draws a different conclusion.
Information & Authors
Information
Published In
Pages: 865 - 877
PubMed: 31476895
Copyright
© 2019 Wei Jiang. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 23 November 2018
Accepted: 15 May 2019
Published online: 3 September 2019
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Comparative clinical effects and cost–effectiveness of maximum androgen blockade, docetaxel with androgen deprivation therapy and ADT alone for the treatment of mHSPC in China. (2019) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2018-0133
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Zhou Han, Youli Xi, Jian Hu, Ye Wang, Huanyu Ni, Cost-effectiveness analysis of eight first-line treatments for metastatic hormone-sensitive prostate cancer in China, Frontiers in Pharmacology, 10.3389/fphar.2025.1684966, 16, (2025).
- Yang Yang, Ya-Qing Chen, Long-Zhuan Huang, Yong Chen, Cost-effectiveness analysis of second-generation androgen receptor antagonists for the treatment of metastatic hormone-sensitive prostate cancer, Frontiers in Public Health, 10.3389/fpubh.2025.1680002, 13, (2025).
- Christopher G Fawsitt, Elaine Gallagher, Alka Singh, Hannah Baker, Edward Kayongo, Howard Thom, Noman Paracha, Developing a Comprehensive Framework for Cost-Effectiveness Evaluation in Metastatic Castration-Sensitive Prostate Cancer: Insights from a Systematic Review, PharmacoEconomics, 10.1007/s40273-025-01532-w, 43, 11, (1323-1338), (2025).
- Cristóbal Ávila, Jaime González-Montero, Carlos I Rojas, Ravi A Madan, Mauricio Burotto, Current landscape in first-line treatment of metastatic hormone sensitive prostate cancer: a cost-effectiveness focused review, The Oncologist, 10.1093/oncolo/oyaf095, 30, 5, (2025).
- Juan Hong, Xiaohui Zeng, Wenjun Chen, Ziyuan Zhou, Yuming He, Jun Meng, Lihui Ouyang, Cost-effectiveness analysis of rezvilutamide versus bicalutamide and androgen-deprivation therapy in patients with high-volume, metastatic, hormone-sensitive prostate cancer: a Markov’s model-based evaluation, Frontiers in Public Health, 10.3389/fpubh.2025.1574780, 13, (2025).
- Poucheok Pang, Baoying Tan, Jianwei Xuan, Cost-effectiveness analysis of olaparib treatment for metastatic castration-resistant prostate cancer with BRCA 1/2 mutations following a new hormonal agent in China, Intelligent Pharmacy, 10.1016/j.ipha.2023.05.001, 1, 2, (67-72), (2023).
- Olajide A. Adekunle, Enrique Seoane-Vazquez, Lawrence M. Brown, Cost-effectiveness analysis of androgen deprivation therapy with relugolix for the treatment of advanced prostate cancer, Journal of the American Pharmacists Association, 10.1016/j.japh.2022.12.019, 63, 3, (817-824.e3), (2023).
- Rémi Pelloux-Prayer, Thomas Bataillard, Antoine Thiery-Vuillemin, Alexandre Vincent, Philippe Fagnoni, Virginie Nerich, Treatment of Patients with Metastatic Hormone-Sensitive Prostate Cancer: A Systematic Review of Economic Evaluations, Clinical Genitourinary Cancer, 10.1016/j.clgc.2022.04.014, 20, 6, (594-602), (2022).
- Michaela C. Barbier, Yuki Tomonaga, Dominik Menges, Henock G. Yebyo, Sarah R. Haile, Milo A. Puhan, Matthias Schwenkglenks, Survival modelling and cost-effectiveness analysis of treatments for newly diagnosed metastatic hormone-sensitive prostate cancer, PLOS ONE, 10.1371/journal.pone.0277282, 17, 11, (e0277282), (2022).
- Peng-Fei Zhang, Dan Xie, Qiu Li, Adding Enzalutamide to First-Line Treatment for Metastatic Hormone-Sensitive Prostate Cancer: A Cost-Effectiveness Analysis, Frontiers in Public Health, 10.3389/fpubh.2021.608375, 9, (2021).