Secukinumab for psoriatic arthritis: comparative effectiveness versus licensed biologics/apremilast: a network meta-analysis
Abstract
Aim: A network meta-analysis using randomized controlled trial data compared psoriatic arthritis (PsA) outcomes (American College of Rheumatology [ACR], Psoriasis Area Severity Index [PASI] and Psoriatic Arthritis Response Criteria [PsARC] response rates) at 12–16 weeks for secukinumab, adalimumab, apremilast, certolizumab, etanercept, golimumab, infliximab and ustekinumab. Patients & methods: Trials were identified by systematic review. Separate networks were developed for the full-study populations, biologic-naive patients and biologic-experienced patients. Results: In the full populations, secukinumab, adalimumab, golimumab and infliximab demonstrated the highest ACR response rates. Secukinumab and infliximab demonstrated the highest PASI response rates, and infliximab and etanercept demonstrated the highest PsARC response rates. Conclusion: In the full populations, secukinumab demonstrated good efficacy across all outcomes. All treatments for active PsA included in this comprehensive network meta-analysis demonstrated superiority to placebo.
Psoriatic arthritis (PsA) is characterized by chronic inflammation, with musculoskeletal and dermatological issues, and other co-morbidities [1]. The pain, stiffness and swelling associated with PsA are often accompanied by structural damage to the joints, impairing patients’ physical functioning and often resulting in severe disability [2]. The aim of treatment is to achieve sustained, low disease activity or remission, maximizing quality of life in the long term [2].
Current immune-modifying therapies, including biologics and targeted synthetic disease-modifying anti-rheumatic drugs (tsDMARDs), are recommended by several international guidelines for use if conventional DMARDs (cDMARDs), employed as first-line therapies, are not successful [3,4]. The earliest biologic therapies approved for the treatment of PsA targeted TNF. At present, five such agents (adalimumab, certolizumab, etanercept, golimumab and infliximab) have been approved, with biosimilars also now widely available. Two agents, secukinumab and ustekinumab, which have been approved more recently, are directed against cytokines that are implicated in the pathophysiology of PsA and related disorders by genetic and tissue-based pathogenesis investigations [5]. Secukinumab is a fully human monoclonal antibody targeting IL-17A, which is involved in the pathogenesis of PsA as well as other autoimmune diseases in the spondyloarthritis family [6,7]. Ustekinumab is a fully human monoclonal antibody directed against the p40 subunit of IL-12 and IL-23. Like IL-17, IL-23 has been implicated in the pathogenesis of autoimmune diseases, including PsA [8]. In addition, the tsDMARD apremilast, a small-molecule inhibitor that modulates inflammatory cytokine production via inhibition of phosphodiesterase-4, has also been approved recently for the treatment of PsA.
The optimal treatment pathway to achieve the objectives set out in guidelines merits further investigation. In particular, there is an increasing need for comparative evidence on the efficacy of the foregoing treatments. Three randomized controlled trials (RCTs) have reported direct comparisons between biologic therapies employed in the treatment of patients with psoriasis: the CLEAR trial [9], which compared secukinumab and ustekinumab (NCT02074982); the FIXTURE trial [10] between secukinumab and etanercept (NCT01358578); and the ACCEPT study between ustekinumab and etanercept (NCT00454584) [11]. The CLEAR and FIXTURE trials included subpopulation analyses for patients with both psoriasis and PsA; however, these trials were conducted to compare the effects of these treatments in patients with psoriasis, and therefore had a focus on skin outcomes rather than articular inflammation. In the CLEAR trial, among patients with psoriasis and PsA, a significantly greater proportion receiving secukinumab 300 mg achieved a Psoriasis Area Severity Index 90 (PASI90) response (i.e., an improvement of at least 90% in PASI score) as early as week 8 compared with patients who received ustekinumab. This significant difference between treatment groups was sustained from week 16 onward: approximately 80% of patients receiving secukinumab achieved a PASI90 response at all time points through to week 52 [9]. In the FIXTURE trial, patients with psoriasis and PsA receiving secukinumab 300 mg were significantly more likely to achieve a PASI75 response at week 12 compared with patients receiving etanercept [10]. Comparatively higher rates of PASI75 and PASI90 response for patients receiving secukinumab 300 mg were sustained until week 52. The efficacy of biologics and tsDMARDs in patients with PsA has been demonstrated across many placebo-controlled trials; however, to our knowledge, only two trials directly comparing treatments for PsA and powered for superiority have been initiated and are currently ongoing. EXCEED 1 is intended to compare the efficacy of secukinumab and adalimumab [12], and SPIRIT-H2H will compare ixekizumab and adalimumab [13]. Unlike previous head-to-head trials, both of these studies will examine articular outcomes as well as skin outcomes. Currently, in the absence of findings from head-to-head trials, adjusted indirect comparisons provide the best available evidence allowing differentiation between treatments for PsA.
Network meta-analysis (NMA) is an extension of traditional pairwise meta-analysis. NMA compares outcomes across a number of treatments when relevant trials can be ‘connected’ into a network directly, or indirectly by use of common comparators, or both. NMA is increasingly used and accepted in comparative effectiveness research and healthcare decision-making [14,15]. Several analyses have used NMA to compare PsA treatments [16–20]; however, not all of them have compared the full range of approved therapies. Here, we have developed networks to compare all biologics and tsDMARDs for PsA approved at the time at which our study was conducted, with a focus on pairwise comparisons against secukinumab. The current study has been carried out in line with established standards [21,22] to meet health technology assessment requirements, and provides further comparative effectiveness data for PsA therapies.
Patients & methods
Systematic literature review
A systematic review of literature published up to 6 November 2015 identified trials of approved biologic therapies and tsDMARDs for patients with active PsA who had experienced an inadequate response to cDMARDs. The therapies of interest were adalimumab, certolizumab, etanercept, golimumab, infliximab, secukinumab and ustekinumab, and the non-biologic therapy apremilast. Relevant efficacy outcomes extracted from the trials identified included American College of Rheumatology 20 (ACR20), ACR50 and ACR70 responses (indicating at least a 20/50/70% improvement in the core set of ACR measures for assessing arthritis); PASI50, PASI75 and PASI90 responses (indicating at least a 50/75/90% reduction in PASI score); and Psoriatic Arthritis Response Criteria (PsARC) responses. Further details can be found in the Supplementary Methods; trial inclusion criteria are given in Supplementary Table 1.
Treatment networks
Three treatment networks were developed: one for ACR responses, one for PASI responses and one for PsARC responses. Principal networks were developed for the full study populations (termed the ‘mixed’ populations), which included all patients, regardless of whether they had received previous biologic therapy. Networks were also developed for trials reporting data from ‘biologic-naive’ patients at study entry as a separate subpopulation. A network was developed for ‘biologic-experienced’ patients for ACR responses only, as there was insufficient evidence reported for the other outcomes. Data used in the networks were those collected at time points up to week 16, the point at which many patients receiving placebo switched to active treatment, particularly in the major trials for apremilast, certolizumab, golimumab, infliximab, secukinumab and ustekinumab.
NMA & statistical methodology
ACR and PASI responses were modeled using a Bayesian NMA with probit link function and conditional multinomial likelihood [21]. This approach can be adopted in cases in which continuous data (e.g., PASI score) are interpreted using a prespecified cut-off point to generate binomial data for analyses (e.g., response or non-response). For PsARC, a dichotomous composite measure developed specifically for use in PsA, a generalized linear model with logit link function and binomial likelihood, was used. Where feasible, for each treatment network, both random-effect and fixed-effect models were conducted. Models with baseline adjustments for placebo response were conducted where needed and feasible. Several factors were examined in order to assess the fit of each model, including the deviance information criterion (see Supplementary Methods).
The output of the Bayesian NMA was a posterior distribution of relative treatment effects, represented as median relative risks with 95% credible intervals, which were constructed from the 2.5th and 97.5th percentiles of the posterior distribution, and can be interpreted in a similar way to CIs. There was considered to be statistical evidence of superiority for a treatment over a given comparator when the relative risk of an ACR, PASI or PsARC response was >1 at both upper and lower 95% credible interval. This can be interpreted as analogous to testing a two-sided p-value at the 5% threshold.
Sensitivity analyses
When feasible, sensitivity analyses were used to examine the impact of including or excluding certain studies in each network. One sensitivity analysis examined the impact of adding adalimumab and placebo data from SPIRIT-P1 [23,24]. This study was excluded from the original network because it is a trial including ixekizumab, which was not approved at the time the analyses were carried out. Three different iterations of the analysis by time point were also performed:
Inclusion of all trials that reported at 12–16 weeks
Restriction of network to only those trials that reported at 12 weeks
Restriction of network to only those trials that reported at 16 weeks
Results
Study selection
Following full-text screening of publications identified by systematic review, 20 trials were selected for potential inclusion in the NMA. Of these, 17 included ACR20/50/70 responses, 19 included PASI50/75/90 responses and 13 included PsARC responses (Table 1). A feasibility assessment determined the degree of heterogeneity across the different trials, examined the quality of the data and established that the selected trials could be used to develop a network. Subsequently, the SPIRIT-P1 trial [23,24] was identified separately for potential inclusion. This placebo-controlled study investigating the efficacy of ixekizumab contains adalimumab as an active control arm.
| Trial name [Ref.] | Relevant treatments (number of patients randomized) | Primary endpoint(s) | Use in ACR NMA (reason for exclusion) | Use in PASI NMA (reason for exclusion) | Use in PsARC NMA (reason for exclusion) | Imputation method | Population composition† |
|---|---|---|---|---|---|---|---|
| ADEPT [25] | Adalimumab 40 mg (153) Placebo (162) | ACR20 response at 12 weeks Modified Sharp score change from baseline at 24 weeks | Yes | Yes | Yes | NRI | Biologic-naive |
| CLEAR [9] | Secukinumab 300 mg (69) Ustekinumab 45 mg (54) | PASI90 response at 16 weeks | No (ACR data not collected) | Yes | No (PsARC data not reported) | NRI | Mixed |
| ERASURE [10] | Secukinumab 150 mg (46) Secukinumab 300 mg (57) Placebo (68) | PASI75 response at 12 weeks IGA Mod 2011 at 12 weeks | No (ACR data not collected) | Yes | No (PsARC data not reported) | NRI | Mixed |
| FIXTURE [10] | Etanercept 50 mg BIW (44) Secukinumab 150 mg (49) Secukinumab 300 mg (50) Placebo (49) | PASI75 response at 12 weeks IGA Mod 2011 at 12 weeks | No (ACR data not collected) | Yes | No (PsARC data not reported) | NRI | Mixed |
| FUTURE 1 [26] | Secukinumab 150 mg (202) Secukinumab 300 mg (202) Placebo (202) | ACR20 response at 24 weeks | No (excluded owing to intravenous loading doses, which do not reflect approved posology) | No (excluded owing to intravenous loading doses, which do not reflect approved posology) | No (excluded owing to intravenous loading doses, which do not reflect approved posology) | NRI | Mixed |
| FUTURE 2 [27] | Secukinumab 150 mg (100) Secukinumab 300 mg (100) Placebo (98) | ACR20 response at 24 weeks | Yes | Yes | Yes | NRI | Mixed |
| Genovese et al. [28] | Adalimumab 40 mg (51) Placebo (51) | ACR20 response at 12 weeks | No (excluded owing to lack of 16-week data) | No (no PASI data reported) | Yes | NRI | Biologic-naive |
| GO-REVEAL [29] | Golimumab 50 mg (146) Golimumab 100 mg (146) Placebo (113) | ACR20 response at 14 weeks | Yes | Yes | Yes | LOCF | Biologic-naive |
| IMPACT [30] | Infliximab 5 mg/kg (52) Placebo (52) | ACR20 response at 14 weeks | Yes | Yes | Yes | Unclear | Biologic-naive |
| IMPACT2 [31] | Infliximab 5 mg/kg (100) Placebo (100) | ACR20 response at 14 weeks | Yes | Yes | Yes | NRI/LOCF | Biologic-naive |
| Mease et al. [32] | Etanercept 25 mg BIW (30) Placebo (30) | PsARC response at 12 weeks | No (excluded owing to lack of 16-week data) | Yes | Yes | LOCF | Not reported |
| Mease et al. [33] | Etanercept 25 mg BIW (101) Placebo (104) | ACR20 response at 12 weeks | No (excluded owing to lack of 16-week data) | No | Yes | LOCF | Not reported |
| PALACE 1 [34] | Apremilast 20 mg (168) Apremilast 30 mg (168) Placebo (168) | ACR20 response at 16 weeks | Yes | Yes | Yes | NRI | Mixed |
| PALACE 2 [35,36] | Apremilast 20 mg (163) Apremilast 30 mg (162) Placebo (159) | ACR20 response at 16 weeks | Yes | Yes | Yes | Unclear | Mixed |
| PALACE 3 [37] | Apremilast 20 mg (169) Apremilast 30 mg (167) Placebo (169) | ACR20 response at 16 weeks | Yes | Yes | Yes | NRI | Mixed |
| PRESTA [38] | Etanercept 50 mg BIW (379) Etanercept 50 mg QW (373) | Proportion of patients achieving ‘clear’ or ‘almost clear’ on the physician's global assessment of psoriasis at 12 weeks | No (reported ACR response data, but could not be linked to ACR treatment network via placebo or an active comparator) | Yes | No (PsARC data not reported) | LOCF | Biologic-naive |
| PSUMMIT1 [39] | Ustekinumab 45 mg (205) Ustekinumab 90 mg (204) Placebo (206) | ACR20 response at 24 weeks | Yes | No | No (PsARC data not reported) | LOCF | Biologic-naive |
| PSUMMIT2 [40] | Ustekinumab 45 mg (103) Ustekinumab 90 mg (105) Placebo (104) | ACR20 response at 24 weeks | Yes | No | No (PsARC data not reported) | LOCF | Mixed |
| RAPID-PsA [41] | Certolizumab 200 mg‡ (138) Certolizumab 400 mg‡ (135) Placebo (136) | ACR20 response at 12 weeks Modified total Sharp score change from baseline at 24 weeks | Yes | Yes | Yes | NRI | Mixed |
| Schett et al. [42] | Apremilast 20 mg (69) Apremilast 40 mg (67) Placebo (68) | ACR20 response at 12 weeks | No (excluded owing to lack of 16-week data) | No (no PASI data reported) | Yes | LOCF | Mixed |
| SPIRIT-P1 [23,24] | Adalimumab 40 mg (101) Placebo (106) | ACR20 response at 24 weeks | No (excluded following sensitivity analysis) | Yes | No | NRI | Biologic-naive |
†Study populations were either mixed (including both biologic-naive and biologic-experienced patients) or biologic-naive.
‡With a 400 mg loading dose.
ACR20: At least a 20% improvement in the core set of American College of Rheumatology measures for assessing arthritis; BIW: Twice per week; IGA Mod 2011: Investigator's Global Assessment (modified in 2011); LOCF: Last observation carried forward; NMA: Network meta-analysis; NRI: Non-responder imputation; PASI75/90: At least a 75/90% reduction in Psoriasis Area Severity Index score; PsARC: Psoriatic Arthritis Response Criteria; QW: Once a week.
Details of included studies’ designs and populations are given in Tables 1 & 2. For adalimumab, golimumab and infliximab, populations were entirely biologic-naive, whereas data for the remainder of the therapies came from mixed populations in which some patients were biologic-experienced. In trials that reported data from biologic-experienced populations, disparities in inclusion criteria meant that patients receiving certain agents might have experienced several previous anti-TNF therapy failures, whereas other populations were permitted to have received only one previous anti-TNF therapy. There were also differences between trials in terms of the methods used to adjust for missing data; some used nonresponder imputation (NRI), whereas others employed the less conservative last observation carried forward imputation approach.
Treatment networks
The treatment networks selected for each outcome in the mixed population are shown in Figure 1. For ACR responses, networks were limited to studies reporting data at week 16, meaning that the studies of Genovese et al. [28], Mease et al. [32,33] and Schett et al. [42] were excluded. SPIRIT-P1 [23,24] was not included. Thus, the final network contained 11 studies. For PASI responses, the evidence base was smaller when networks were restricted by time point. Therefore, available evidence was maximized by using data from 12–16-week time points, and including data from SPIRIT-P1 [23,24]; the final network contained 15 trials. For PsARC responses, data from 12–16-week time points were used. The treatment network contained 13 trials. Networks for the biologic-naive and biologic-experienced populations are shown in Supplementary Figures 1 & 2.
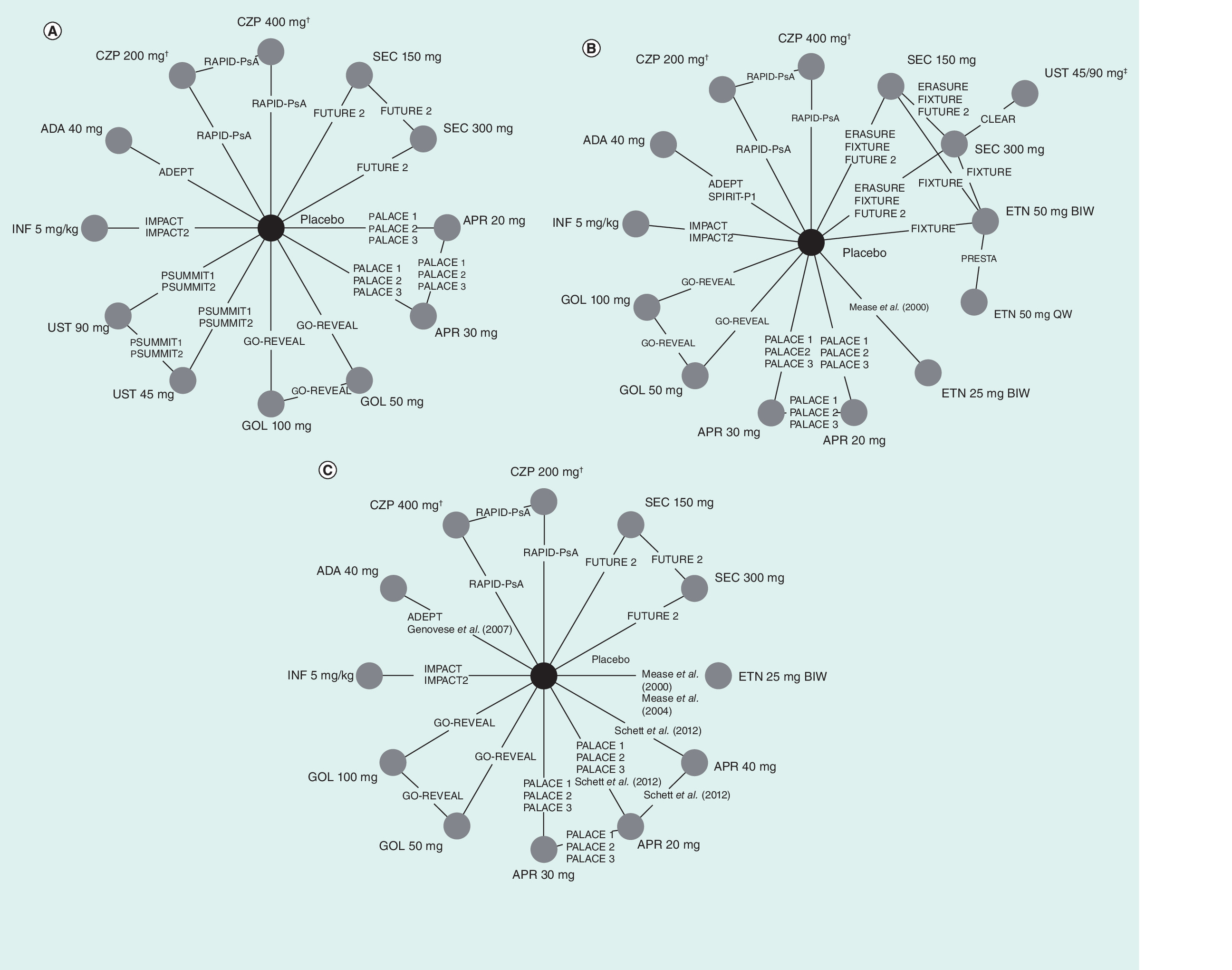
Figure 1. Treatment networks for the mixed populations of patients with PsA.
(A) ACR responses at 16 weeks, (B) PASI responses at 12–16 weeks and (C) PsARC responses at 12–16 weeks. Populations containing biologic-naive and biologic-experienced patients: apremilast, certolizumab, etanercept (for PASI data; population composition for PsARC data not reported), secukinumab, ustekinumab. Populations containing biologic-naive patients only: adalimumab, golimumab, infliximab.
†With a 400 mg loading dose.
‡Patients received ustekinumab 45 or 90 mg in the CLEAR trial, depending upon bodyweight; therefore, patients receiving either dose were treated as a single treatment group.
ACR: American College of Rheumatology; ADA: Adalimumab; APR: Apremilast; BIW: Twice per week; CZP: Certolizumab; ETN: Etanercept; GOL: Golimumab; INF: Infliximab; PASI: Psoriasis Area Severity Index; PsARC: Psoriatic Arthritis Response Criteria; QW: Once weekly; SEC: Secukinumab; UST: Ustekinumab.
Model selection
Values for the deviance information criterion were similar across models for ACR and PASI scores, regardless of adjustments for placebo response or other covariates. Thus, unadjusted models were selected for both networks. The leverage plots assessing model fit indicated that a model adjusted for placebo response was the best fit for PsARC responses in our study, and, consequently, this model was used for PsARC analyses in both mixed and biologic-naive populations. This approach has been recommended previously to avoid the introduction of bias when using data from studies in which placebo response improves over time [43]. For all mixed populations, random-effect models were selected to address the potential heterogeneity across trials identified in the feasibility assessment. The relatively smaller sizes of the biologic-naive and biologic-experienced patient populations meant that use of a random-effects model was not feasible, because there were either insufficient degrees of freedom to conduct the analysis or so few degrees of freedom that the posterior distribution of the between-study heterogeneity remained large, leading to nonsensical, posterior distributions for the efficacy parameters. Therefore, fixed-effects models were used in these populations.
ACR networks (16 weeks)
Mixed population
In the mixed population, the treatment network permitted comparisons for all therapies, with the exception of etanercept (Figure 1A). Populations for adalimumab, golimumab and infliximab were biologic-naive, whereas those for other therapies were mixed. For all treatments, there was statistical evidence of superior ACR20 response rates at 16 weeks, compared with placebo. Secukinumab 150 and 300 mg both demonstrated statistical superiority over apremilast 20 or 30 mg and ustekinumab 45 mg (Figure 2A & B). Furthermore, infliximab 5 mg/kg, golimumab 50 and 100 mg and adalimumab 40 mg demonstrated statistical superiority in terms of ACR20 response rates over apremilast 20 or 30 mg and ustekinumab 45 or 90 mg (Supplementary Table 2). These treatments were associated with similar or slightly higher response rates when compared with secukinumab, but without statistical evidence of superiority. ACR50 and ACR70 responses showed similar trends to ACR20 (Supplementary Tables 3 & 4).
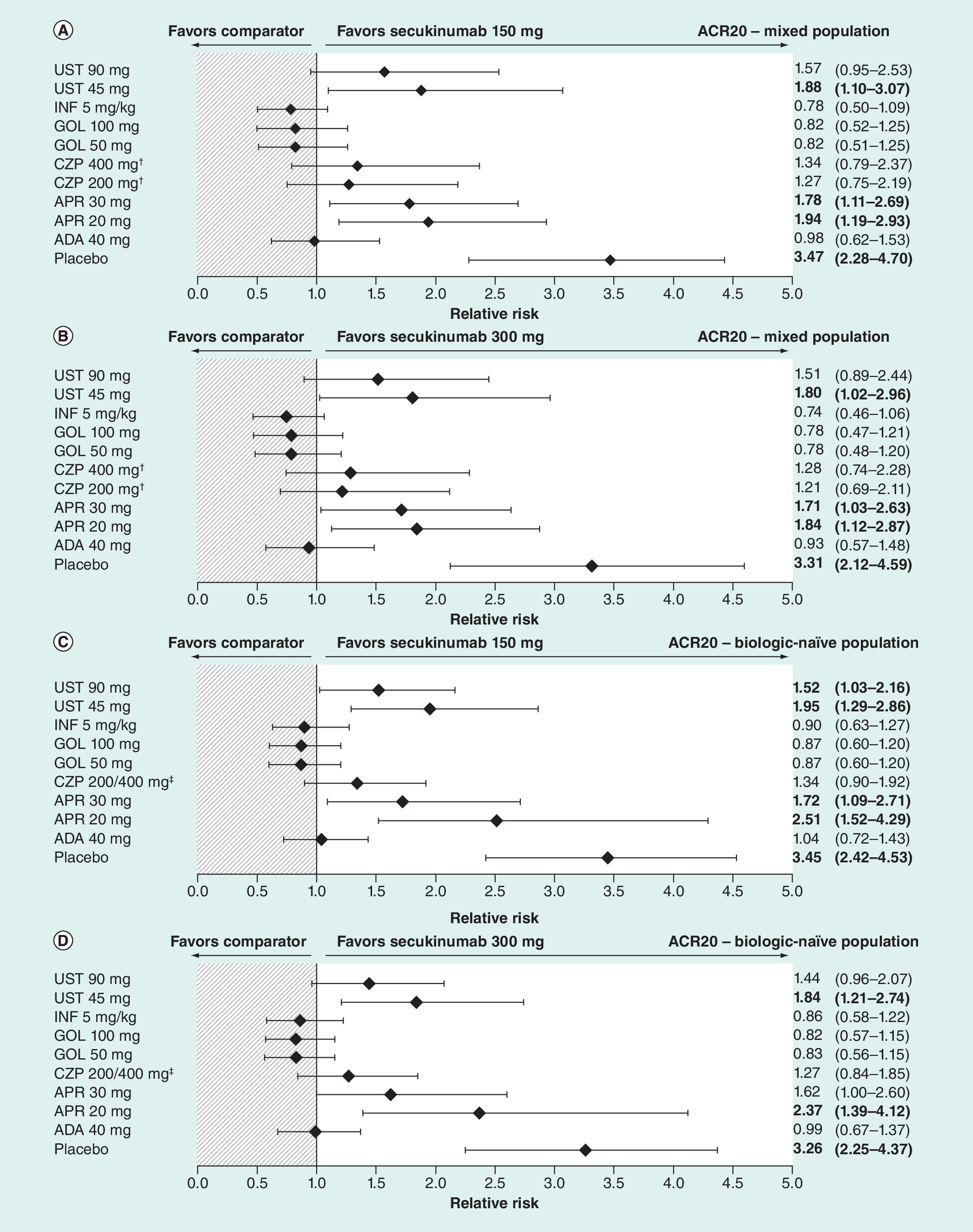
Figure 2. Relative risks of achieving an ACR20 response at 16 weeks.
(A) Secukinumab 150 mg in the mixed population; (B) secukinumab 300 mg in the mixed population; (C) secukinumab 150 mg in the biologic-naive population; and (D) secukinumab 300 mg in the biologic-naive population.
Data shown are the estimated comparative effect (relative risk [and 95% credible interval, which can be interpreted as a confidence interval]) of secukinumab versus the treatments indicated in the left-hand column. Values in bold text indicate comparisons with evidence of superiority for secukinumab. Populations containing biologic-naive and biologic-experienced patients: apremilast, certolizumab, secukinumab, ustekinumab. Populations containing biologic-naive patients only: adalimumab, golimumab, infliximab.
†With a 400 mg loading dose.
‡Results for both doses of CZP (200 and 400 mg) were combined in the biologic-naive subpopulation.
ACR20: At least a 20% improvement in the core set of American College of Rheumatology measures for assessing arthritis; ADA: Adalimumab; APR: Apremilast; CZP: Certolizumab; GOL: Golimumab; INF: Infliximab; UST: Ustekinumab.
Biologic-naive subpopulation
Eight trials were included in the treatment network for this subpopulation. In terms of ACR20, ACR50 and ACR70 response rates, all treatments demonstrated superiority over placebo. Adalimumab and secukinumab 150 mg demonstrated superiority over both doses of apremilast and both doses of ustekinumab. Secukinumab 300 mg demonstrated statistical superiority over apremilast 20 mg and ustekinumab 45 mg only; pairwise comparisons against apremilast 30 mg (RR [95% CI]: 1.62 [1.00–2.60]) and ustekinumab 90 mg (RR [95% CI]: 1.44 [0.96–2.07]) fell just short of statistical superiority in favor of secukinumab 300 mg (Figure 2C & D; Supplementary Tables 5–7). Infliximab and both doses of golimumab demonstrated statistical superiority over all treatments in the network, with the exception of adalimumab and secukinumab.
Biologic-experienced subpopulation
The NMA for ACR responses in the biologic-experienced population included four trials (see Table 2 for patient inclusion criteria). All treatments except ustekinumab 45 and 90 mg showed evidence of superiority to placebo. No therapy demonstrated statistical superiority over other treatments, except for certolizumab (200 and 400 mg doses considered as a single treatment group), which showed statistical superiority over either dose of ustekinumab (Supplementary Figure 3; Supplementary Tables 8–10).
| Trial [Ref.] | Relevant treatments | Inclusion of patients with previous primary treatment failure† | Inclusion of patients with previous secondary treatment failure‡ | Relevant inclusion criteria for biologic-experienced patients | Relevant exclusion criteria for biologic-experienced patients |
|---|---|---|---|---|---|
| CLEAR [9] | Secukinumab 300 mg Ustekinumab 45 mg | Study publication did not differentiate between primary and secondary treatment failure | Patients were eligible if their psoriasis had been poorly controlled with biologic therapy | Patients who had received secukinumab, ustekinumab or other biologic drugs targeting IL-17A or IL-17RA were excluded | |
| ERASURE [10] | Secukinumab 150 mg Secukinumab 300 mg Placebo | Study publication did not differentiate between primary and secondary treatment failure | Patients who had received previous biologic therapy were eligible; prestudy washout periods were 6 months for ustekinumab and 12 weeks for other biologics or etanercept | NA | |
| FIXTURE [10] | Etanercept 50 mg BIW Secukinumab 150 mg Secukinumab 300 mg Placebo | – | – | Patients who had received previous biologic therapy were eligible; prestudy washout periods were 6 months for ustekinumab and 12 weeks for other biologics | Patients were not permitted to have received etanercept previously |
| FUTURE 2 [27] | Secukinumab 150 mg Secukinumab 300 mg Placebo | Yes | Yes | Patients who had previously received ≤ 3 anti-TNF agents were eligible for inclusion if they had not responded to treatment or had discontinued treatment for safety or tolerability reasons | Patients who had previously received any biologic agent other than anti-TNF agents were excluded |
| PALACE 1 [34,44] | Apremilast 20 mg Apremilast 30 mg Placebo | Yes | Yes | Patients who had previously received biologics, including patients who had not responded to biologic treatment, were eligible for inclusion. TNF efficacy failures were permitted in ≤10% of included patients | Patients who had previously experienced treatment failure with >3 agents for PsA (small molecules and/or biologics) or >1 anti-TNF were excluded |
| PALACE 2 [35,44] | Apremilast 20 mg Apremilast 30 mg Placebo | Yes | Yes | Patients were permitted to have received biologics. TNF efficacy failures were permitted in ≤10% of included patients. Washout periods were 12 weeks for adalimumab, certolizumab, etanercept, golimumab or infliximab, and 24 weeks for ustekinumab | Patients who had previously experienced treatment failure with >3 agents for PsA (small molecules and/or biologics) or >1 anti-TNF were excluded |
| PALACE 3 [37,44] | Apremilast 20 mg Apremilast 30 mg Placebo | Yes | Yes | Patients were permitted to have received biologics. TNF efficacy failures were permitted in ≤10% of included patients | Patients who had previously experienced treatment failure with >3 agents for PsA (small molecules and/or biologics) or >1 anti-TNF were excluded |
| PSUMMIT2 [40] | Ustekinumab 45 mg Ustekinumab 90 mg Placebo | Yes | Yes | The protocol specified that 150–180 patients out of a total of 300 must have previously received anti-TNF agents, defined as adalimumab, certolizumab, etanercept or golimumab for at least 8 weeks, or infliximab for at least 14 weeks, or proven inability to tolerate anti-TNF therapy for 8–14 weeks | Patients who had received anti-IL-12/23 agents were excluded |
| RAPID-PsA [41] | Certolizumab 200 mg§ Certolizumab 400 mg§ Placebo | No | Yes | Up to 40% of patients included were permitted to have received one or more anti-TNF agent previously, with a washout period of >3 months before baseline visit (28 days for etanercept) | Patients who had had previous exposure to >2 biologics or >1 anti-TNF agent for the treatment of PsA or psoriasis, or primary failure of a previous anti-TNF agent, defined as no response within the first 12 weeks of treatment, were excluded |
| Schett et al. [42] | Apremilast 20 mg Apremilast 40 mg Placebo | Study publication did not differentiate between primary and secondary treatment failure | Patients were permitted to have received previous biologic therapy, with a washout period of ≥ 56 days for etanercept and ≥ 84 days for adalimumab or infliximab | NA | |
†Primary treatment failure was defined as non-response to treatment.
‡Secondary treatment failure was defined as loss of response to treatment over time.
§With a 400 mg loading dose.
Bold text indicates studies that were included in the biologic-experienced network for American College of Rheumatology responses.
BIW: Twice per week; NA: Not applicable; PsA: Psoriatic arthritis.
PASI networks (12–16 weeks)
Mixed population
The treatment network for the mixed population allowed comparisons between all therapies included in this study (Figure 1B). In CLEAR, patients received ustekinumab 45 or 90 mg, depending upon bodyweight, in line with the licensed dosing scheme [9,45]; the doses were considered as a single treatment group for this analysis. Patient populations for adalimumab, golimumab and infliximab were biologic-naive; populations for all other therapies were mixed.
In terms of response rates for PASI50, PASI75 and PASI90, all treatments demonstrated superiority over placebo. Secukinumab 150 or 300 mg demonstrated statistical superiority to apremilast 20 and 30 mg, certolizumab 200 and 400 mg, adalimumab 40 mg and etanercept 25 and 50 mg twice per week and 50 mg weekly. Furthermore, there was evidence of superiority for secukinumab 300 mg compared with golimumab 50 mg (Figure 3; Supplementary Tables 11–13). Similarly, infliximab demonstrated statistical superiority to all treatments apart from secukinumab, golimumab 100 mg and ustekinumab 45/90 mg. Infliximab was associated with slightly higher response rates than secukinumab, but without evidence of statistical superiority.
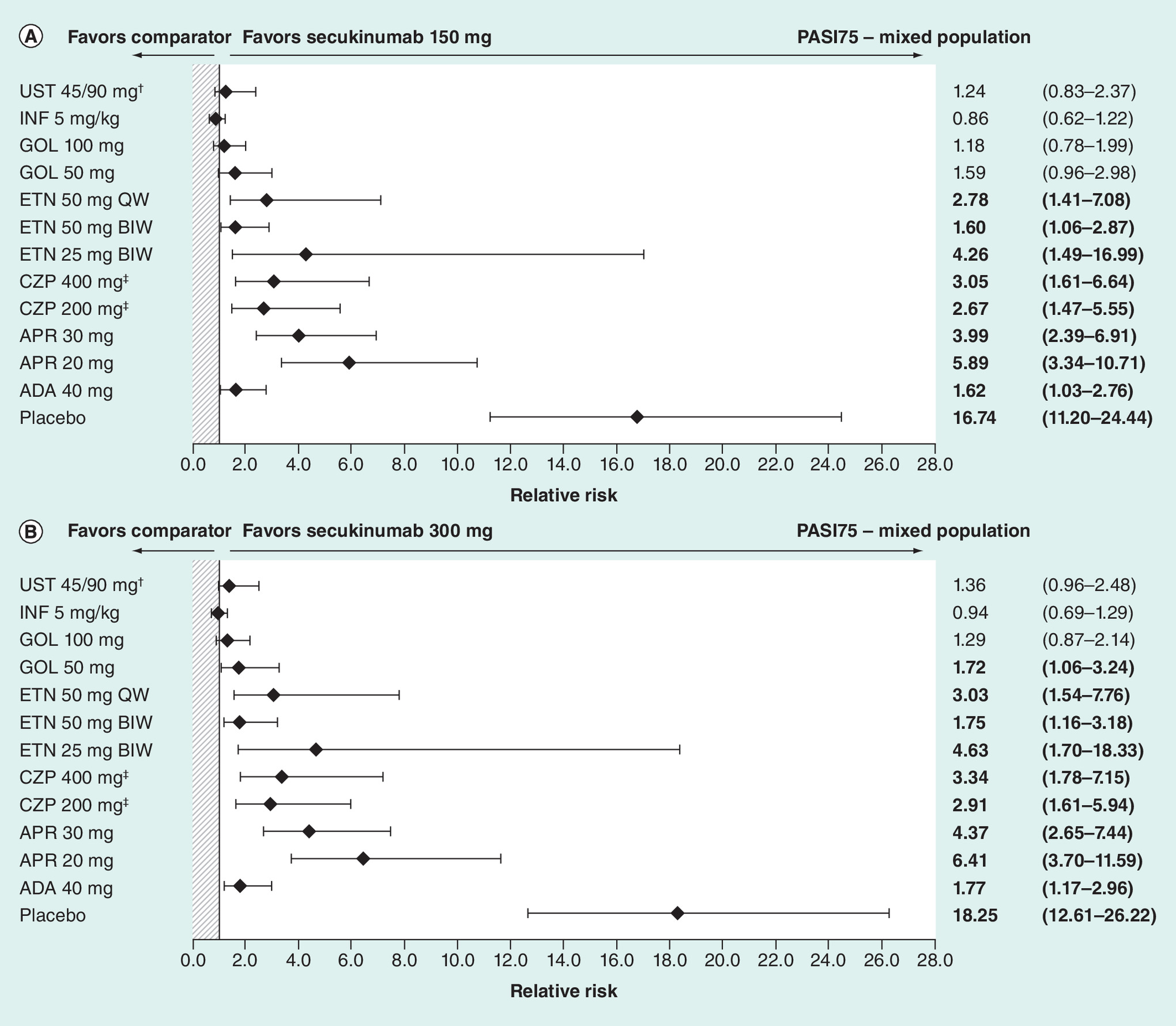
Figure 3. Relative risks of achieving at least a 75% reduction in Psoriasis Area Severity Index score responses at 12–16 weeks in the mixed population (SPIRIT-P1 trial [23,24] included).
Data shown are the estimated comparative effect (relative risk [and 95% credible interval, which can be interpreted as a CI]) of secukinumab versus the treatment indicated in the left-hand column. Values in bold text indicate comparisons with evidence of superiority for secukinumab. Populations containing biologic-naive and biologic-experienced patients: apremilast, certolizumab, secukinumab, ustekinumab. Populations containing biologic-naive patients only: adalimumab, golimumab, infliximab.
†Patients received ustekinumab 45 or 90 mg in the CLEAR trial, depending upon bodyweight; therefore, patients receiving either dose were treated as a single treatment group.
‡With a 400 mg loading dose.
ADA: Adalimumab; APR: Apremilast; BIW: Twice per week; CZP: Certolizumab; ETN: Etanercept; GOL: Golimumab; INF: Infliximab; PASI75: At least a 75% reduction in Psoriasis Area Severity Index score; QW: Once weekly; UST: Ustekinumab.
Biologic-naive subpopulation
The treatment network for the biologic-naive population included only five trials, and compared secukinumab 150 and 300 mg with adalimumab 40 mg, golimumab 50 and 100 mg and infliximab 5 mg/kg. All treatments demonstrated superiority over placebo in terms of PASI50, PASI75 and PASI90 responses. There was statistical evidence of superiority for infliximab over golimumab 50 mg and adalimumab 40 mg, and for golimumab 100 mg over golimumab 50 mg. All analyses marginally favored either dose of secukinumab over golimumab 50 mg or adalimumab 40 mg; however, none of these pairwise comparisons demonstrated evidence of statistical superiority (Supplementary Figure 4; Supplementary Tables 14–16).
PsARC responses (12–16 weeks)
Mixed population
The treatment network for PsARC in the mixed population included all therapies in this study except ustekinumab (Figure 1C). As in the other networks, patient populations were biologic-naive for some treatments and mixed for others, including secukinumab. Data for etanercept in this analysis were derived from the studies [32,33], which did not report whether included patients had received previous biologic therapy. All treatments demonstrated superiority to placebo. Etanercept 25 mg twice per week and infliximab were associated with statistical superiority over adalimumab, and apremilast 20, 30 and 40 mg. Certolizumab 200 mg and secukinumab 150 mg demonstrated superiority to all doses of apremilast, whereas certolizumab 400 mg and secukinumab 300 mg were superior only to apremilast 20 and 30 mg. Golimumab 100 mg was superior to apremilast 20 and 40 mg (Figure 4; Supplementary Table 17).

Figure 4. Relative risks of achieving Psoriatic Arthritis Response Criteria responses at 12–16 weeks in the mixed population.
Data shown are the estimated comparative effect (relative risk [and 95% credible interval, which can be interpreted as a confidence interval]) of secukinumab versus the treatment indicated in the left-hand column. Values in bold text indicate comparisons with evidence of superiority for secukinumab. Populations containing biologic-naive and biologic-experienced patients: apremilast, certolizumab, secukinumab. Populations containing biologic-naive patients only: adalimumab, golimumab, infliximab. Population composition for etanercept not reported.
†With a 400 mg loading dose.
ADA: Adalimumab; APR: Apremilast; BIW: Twice per week; CZP: Certolizumab; ETN: Etanercept; GOL: Golimumab; INF: Infliximab; PsARC: Psoriatic Arthritis Response Criteria.
Biologic-naive subpopulation
The treatment network for PsARC in the biologic-naive population included only six trials and compared five treatments. Adalimumab 40 mg, etanercept 25 mg twice per week and infliximab 5 mg/kg demonstrated statistical superiority over placebo. Infliximab 5 mg/kg, golimumab 50 and 100 mg and etanercept 25 mg twice per week were all associated with slightly higher response rates than secukinumab 150 and 300 mg; adalimumab 40 mg was associated with slightly higher response rates than secukinumab 300 mg only. There was, however, no statistical evidence of superiority for any treatment over an active comparator (Supplementary Figure 5; Supplementary Table 18).
Discussion
This study used NMA to assess the relative efficacy of secukinumab and all other non-cDMARD PsA therapies (biologics and tsDMARDs) approved at the time the analysis was conducted, with placebo as the common comparator arm. Both articular and dermatologic manifestations of disease were examined in the analyses, via the inclusion of ACR and PASI responses, respectively. An analysis of PsARC responses was also included. Although this composite measure is included more frequently as a secondary endpoint in RCTs, rather than a primary endpoint [46], it has been included in several health technology assessment submissions for biologic therapies for the treatment of PsA. A recent NICE assessment recommended adjustment for placebo response when modeling PsARC outcomes, which is reflected in the approach adopted in our analysis [47].
Disparities in inclusion criteria and patient recruitment between studies meant that ‘mixed’ networks contained some patient populations that were biologic-naive, whereas patients in other trial populations were permitted to have received one or several previous biologic therapies. Data for adalimumab, golimumab and infliximab were derived exclusively from biologic-naive populations, whereas patients receiving apremilast, certolizumab, etanercept, secukinumab or ustekinumab could have experienced previous failure of a biologic treatment.
In the mixed population, secukinumab, infliximab, golimumab and adalimumab demonstrated good efficacy in terms of ACR20, ACR50 and ACR90 responses, in some cases showing statistical superiority over comparators. Similarly, for PASI50, PASI75 and PASI90 responses, both doses of secukinumab and infliximab demonstrated superiority over most other treatments in the analysis. The analysis assessing PsARC outcomes in the mixed population favored infliximab and etanercept at dosages of 25 mg twice per week. Most treatments included in this analysis demonstrated statistical superiority to some or all of the included doses of apremilast.
When treatment effects in biologic-naive patients were assessed separately, trends were similar to those in the analyses of mixed populations for ACR outcomes, but differed slightly for PASI and PsARC outcomes; in particular, fewer pairwise comparisons showed statistical superiority for a treatment over an active comparator in these analyses. This may be due to the comparatively smaller evidence base for the biologic-naive networks, which used data from 8, 5 and 6 trials for ACR, PASI and PsARC outcomes, respectively, in some cases using data only from a subset of the included patients. In contrast, the networks for the mixed populations used data from 11, 15 and 13 full trial populations, respectively. Therefore, the statistical power of the analysis for biologic-naive populations is likely to have been lower. This lack of statistical power may explain the fact that, in the biologic-naive population, secukinumab 150 mg demonstrated statistical superiority to both doses of apremilast and both doses of ustekinumab, whereas secukinumab 300 mg was superior to apremilast 20 mg and ustekinumab 45 mg, but fell short of statistical superiority to apremilast 30 mg and ustekinumab 90 mg. Differences in dose response, for example, a smaller difference in response between the two doses of secukinumab relative to apremilast or ustekinumab, may also have had an impact upon this analysis.
ACR outcomes only were assessed in the biologic-experienced population. At present, no ACR efficacy data from RCTs are available for adalimumab, etanercept, golimumab or infliximab in biologic-experienced populations; thus, the analysis was limited to apremilast, certolizumab, secukinumab and ustekinumab. Certolizumab 200/400 mg demonstrated superiority over either dose of ustekinumab, but there was no other evidence of statistical superiority. It is likely that bias was introduced into the mixed- and biologic-experienced networks by disparities in inclusion criteria across trials of PsA treatments (Table 2). For example, patients entering the RAPID-PsA trial for certolizumab were permitted to have received no more than one previous anti-TNF treatment [41] and were excluded if they had experienced primary failure of an anti-TNF therapy, which was defined as no response within the first 12 weeks of treatment. In contrast, the FUTURE 2 trial for secukinumab permitted inclusion of patients with primary or secondary treatment failure, and patients who had previously received up to three anti-TNF treatments could be included in the study [27]. These differences meant that patients receiving secukinumab may have been more difficult to treat than those receiving apremilast or certolizumab. In addition, the relatively small numbers of patients in the overall study populations who had received previous biologic therapy meant that analyses using the biologic-experienced networks had limited statistical power and, consequently, their results should be interpreted with caution. Restriction of networks by time point also limited patient numbers in some cases; in the ACR network, restriction of trials to those reporting week 16 data meant that a number of studies were not included.
NMA, when not adjusted using meta-regression, is not able to adjust for differences in study designs or patients’ baseline characteristics that are effect modifiers. In this analysis, patient populations are likely to have differed in terms of background exposure to methotrexate or corticosteroids, disease activity, and baseline PASI scores. Consequently, heterogeneity across trials was a general limitation of this analysis, although several meta-regression models were fitted where possible (see Supplementary Methods). Meta-regression adjustment for differences in patient populations was not possible, because many of the trials in the analysis did not include biologic-experienced patients. This disparity was addressed by the development of different networks depending on patients’ previous treatment use. In biologic-naive networks, however, this introduced bias against treatments for which only a subset of trial data could be used; despite the predefined sub-analyses for biologic-naive patients in these trials, they lack the statistical power of trials containing exclusively biologic-naive patients. Some of the trials included in the networks, such as SPIRIT-P1, were not powered for noninferiority comparisons or, in the case of the CLEAR, ERASURE and FIXTURE trials, were designed to assess treatment effects in psoriasis, not PsA.
Overall, nine trials used NRI exclusively to account for missing data, whereas eight trials (for apremilast, etanercept, golimumab, infliximab and ustekinumab) used last observation carried forward (Table 1), which can bias analyses in favor of active treatment. Therefore, the NMA results may be biased against treatments for which the more conservative NRI method had been employed. For PASI and PsARC outcomes, the combination of 12- and 16-week time points may have introduced additional variation, biasing the analyses in favor of treatments for which 16-week data were used.
The short 12–16-week timeframe is a limitation of this analysis, imposed by the need to make comparisons only within the placebo-controlled phase of the trials. Although rapid treatment response is important following treatment initialization, long-term sustained control of disease is the major aim of PsA therapy due to the chronic nature of the condition [2]. For chronic conditions, meaningful treatment benefits, particularly in terms of quality of life and social functioning, are most likely to be detected in the long term. Furthermore, for some treatments, such as apremilast, maximum efficacy may not be reached until after the 12–16-week timeframe, meaning that treatment effect may not be captured by a short-term analysis. Therefore, treatment comparisons with a longer time horizon are a vital means of informing therapeutic decisions. This could be addressed by the use of an alternative method for generating comparative data, such as matching-adjusted indirect comparison (MAIC). Although MAIC can be used to compare only two treatments at the same time, whereas NMA allows for multiple pairwise comparisons, MAIC permits the included trials to be matched in terms of patient populations, disparities in imputation methods, and study design or reporting differences. Furthermore, because a common comparator is not required, MAIC allows the time horizon of analysis to be extended beyond the placebo-controlled phase. MAICs have been developed examining secukinumab and relevant comparators [48,49].
Of the five published NMAs in PsA identified by the authors, three did not include secukinumab [16,17,20] and the two that did include secukinumab had methodological limitations that impact the clinical relevance of the results [18,19]. We therefore contend that the current NMA is the most robust analysis in PsA to date. The first NMA to include secukinumab was published as a congress abstract in 2015, and compared all approved treatments using data from 14 trials [18]. The results were similar to those of the current NMA, showing adalimumab, golimumab, secukinumab (150 and 300 mg), and infliximab to be associated with the lowest numbers needed to treat for ACR20 responses at week 24 in both the mixed and biologic-naive population. For PASI75 response at week 24 in the mixed population, adalimumab, golimumab, secukinumab 300 mg and infliximab had lower numbers needed to treat than the other treatments. However, this analysis did not account for the time at which patients switched from placebo to active treatment, which was earlier than 24 weeks in most trials. This limits the validity of the results. The second NMA to include secukinumab was published in 2016 and compared all PsA treatments approved at the time of the study. This showed secukinumab to be associated with numerically greater ACR20 responses at weeks 12–24 than apremilast, certolizumab and ustekinumab, although findings were not classically statistically significant. However, the authors used pooled data for etanercept, infliximab, adalimumab and golimumab and compared this grouping (older TNF inhibitors) against the newer therapies [19]. Thus, this study did not permit pairwise comparisons between all individual treatments, and the validity of the results is compromised by this limitation in the study design.
Conclusion
This NMA is methodologically sound and is the first NMA of all approved PsA therapies to date that accounts for early placebo switching and permits for pairwise comparisons between all agents. This analysis found that secukinumab 150 and 300 mg were superior to apremilast and demonstrated good efficacy across all outcomes; furthermore, in the mixed population, both doses of secukinumab were superior to ustekinumab 45 mg in terms of ACR outcomes, and superior to adalimumab, certolizumab and etanercept in terms of PASI outcomes. Of the other treatments examined, the anti-TNF agents infliximab and golimumab also demonstrated superiority to the small-molecule inhibitor apremilast across ACR and PASI outcomes and PsARC responses.
As well as providing comparative evidence, indirect treatment comparisons can generate hypotheses that can be tested in future RCTs. Head-to-head superiority trials in PsA, such as the ongoing trial EXCEED 1 [12], which has been initiated to compare adalimumab and secukinumab, and SPIRIT-H2H [13], comparing adalimumab and secukinumab, will be needed to provide directly comparative results.
Biologics and targeted synthetic disease-modifying anti-rheumatic drugs (DMARDs) are recommended for the treatment of active psoriatic arthritis (PsA) if conventional DMARDs employed as first-line therapies are not successful.
Given the limited number of head-to-head randomized, controlled trials comparing biologics and targeted synthetic DMARDs for PsA, adjusted indirect comparisons, such as network meta-analysis, provide valuable evidence differentiating between treatments.
We conducted a systematic review to identify relevant trials for adalimumab, apremilast, certolizumab, etanercept, golimumab, infliximab, secukinumab and ustekinumab.
Separate networks were developed for full (mixed) study populations, for biologic-naive patients and for biologic-experienced patients.
In the mixed populations, secukinumab, adalimumab, golimumab and infliximab were associated with the highest response rates according to American College of Rheumatology criteria at 16 weeks.
Secukinumab and infliximab demonstrated the highest Psoriasis Area Severity Index response rates at 12–16 weeks in the mixed populations.
Infliximab and etanercept demonstrated the highest Psoriatic Arthritis Response Criteria response rates at 12–16 weeks in the mixed populations.
In this comprehensive network meta-analysis of licensed treatments for active PsA, secukinumab demonstrated good efficacy across all outcomes examined in the mixed study populations.
Supplementary data
To view the supplementary data that accompany this paper please visit the journal website at: www.futuremedicine.com/doi/full/10.2217/cer-2018-0075
Financial & competing interests disclosure
IB McInnes has received consulting fees from AbbVie, BMS, Janssen, MSD, Novartis, Pfizer and UCB, and has received research grants from AstraZeneca, BMS, Celgene and Pfizer. P Nash has received funding from Novartis Pharma AG for research, consultancy and as a speaker. C Ritchlin has received consulting fees from AbbVie, Amgen, Boehringer Ingelheim, Janssen, Novartis, Sanofi, Sun Pharma and UCB, and has received research grants from AbbVie, Amgen and UCB. EH Choy has received consulting fees from Amgen, Biogen, Chugai Pharma, Eli Lilly, Janssen, Novartis, Pfizer, Regeneron, Roche, R-Pharm and Sanofi, and has received research grants from Pfizer, Roche and UCB. S Kanters is a paid employee of Precision Health Economics and through this work has consulted for Bayer, BTG Pharmaceuticals, Boehringer Ingelheim, Genzyme/Sanofi, Merck, Novartis, Novo Nordisk, Roche and Teva. H Thom has received consulting fees from Eli Lilly, Roche, Novartis Pharma AG and Pfizer. K Gandhi and L Pricop are shareholders and paid employees of Novartis Pharmaceuticals Corporation, East Hanover, NJ, USA. SM Jugl is a shareholder and paid employee of Novartis Pharma AG, Basel, Switzerland. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Medical writing support was provided by C Freeman and P Field from PharmaGenesis Oxford Central, Oxford, UK and was funded by Novartis Pharma AG, Basel, Switzerland. Costello Medical Consulting Ltd, Cambridge, UK and RTI Health Solutions, Durham, NC, USA conducted the systematic literature review. Statistical analysis support was provided by Precision Health Economics, Vancouver, BC, Canada and was funded by Novartis Pharma AG, Basel, Switzerland.
Ethical conduct of research
This study was of non-interventional nature and did not include primary data collection (i.e., was based on published secondary data only). Therefore, ethic committee or institutional review board approval was not required. Data used were taken from published randomized controlled trials, which were conducted according to the principles of the Declaration of Helsinki and with informed consent from participants.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Garg N, van den Bosch F, Deodhar A. The concept of spondyloarthritis: where are we now? Best Pract. Res. Clin. Rheumatol. 28(5), 663–672 (2014).
• Provides an introduction to spondyloarthritis.
2.
Smolen JS, Schols M, Braun J et al. Treating axial spondyloarthritis and peripheral spondyloarthritis, especially psoriatic arthritis, to target: 2017 update of recommendations by an international task force. Ann. Rheum. Dis. 77(1), 3–17 (2018).
•• Defines treatment aims for spondyloarthritis, based on published literature and consultation with clinical experts.
3.
Coates LC, Murphy R, Helliwell PS. New GRAPPA recommendations for the management of psoriasis and psoriatic arthritis: process, challenges and implementation. Br. J. Dermatol. 174(6), 1174–1178 (2016).
4.
Gossec L, Smolen JS, Ramiro S et al. European League Against Rheumatism (EULAR) recommendations for the management of psoriatic arthritis with pharmacological therapies: 2015 update. Ann. Rheum. Dis. 75(3), 499–510 (2016).
5.
Tintle SJ, Gottlieb AB. Psoriatic arthritis for the dermatologist. Dermatol. Clin. 33(1), 127–148 (2015).
6.
Kirkham BW, Kavanaugh A, Reich K. Interleukin-17A: a unique pathway in immune-mediated diseases: psoriasis, psoriatic arthritis and rheumatoid arthritis. Immunology 141(2), 133–142 (2014).
7.
Konya C, Paz Z, Apostolidis SA, Tsokos GC. Update on the role of interleukin 17 in rheumatologic autoimmune diseases. Cytokine 75(2), 207–215 (2015).
8.
Smith JA, Colbert RA. Review: the interleukin-23/interleukin-17 axis in spondyloarthritis pathogenesis: Th17 and beyond. Arthritis Rheumatol. 66(2), 231–241 (2014).
9.
Blauvelt A, Reich K, Tsai TF et al. Secukinumab is superior to ustekinumab in clearing skin of subjects with moderate-to-severe plaque psoriasis up to 1 year: results from the CLEAR study. J. Am. Acad. Dermatol. 76(1), 60–69, e69 (2017).
10.
Gottlieb AB, Langley RG, Philipp S et al. Secukinumab improves physical function in subjects with plaque psoriasis and psoriatic arthritis: results from two randomized, Phase III trials. J. Drugs Dermatol. 14(8), 821–833 (2015).
11.
Griffiths CE, Strober BE, van de Kerkhof P et al. Comparison of ustekinumab and etanercept for moderate-to-severe psoriasis. N. Engl. J. Med. 362(2), 118–128 (2010).
12.
ClinicalTrials.gov. NCT02745080. Efficacy of secukinumab compared to adalimumab in patients with psoriatic arthritis (EXCEED 1). https://clinicaltrials.gov/ct2/show/NCT02745080 (Accessed 29 June 2018).
13.
ClinicalTrials.gov. A study of ixekizumab (LY2439821) versus adalimumab in participants with psoriatic arthritis (SPIRIT-H2H). https://clinicaltrials.gov/ct2/show/NCT03151551 (Accessed 29 June 2018).
14.
Dias S, Welton NJ, Sutton AJ, Ades AE. Evidence synthesis for decision making 1: introduction. Med. Decis. Making 33(5), 597–606 (2013).
• Provides an overarching introduction to evidence synthesis methods for decision making.
15.
Greco T, Biondi-Zoccai G, Saleh O et al. The attractiveness of network meta-analysis: a comprehensive systematic and narrative review. Heart Lung Vessel 7(2), 133–142 (2015).
16.
Betts KA, Griffith J, Friedman A, Zhou ZY, Signorovitch JE, Ganguli A. An indirect comparison and cost per responder analysis of adalimumab, methotrexate and apremilast in the treatment of methotrexate-naive patients with psoriatic arthritis. Curr. Med. Res. Opin. 32(4), 721–729 (2016).
17.
Cawson MR, Mitchell SA, Knight C et al. Systematic review, network meta-analysis and economic evaluation of biological therapy for the management of active psoriatic arthritis. BMC Musculoskelet. Disord. 15, 26 (2014).
18.
Strand V, Husni ME, Reichmann W et al. Network meta-analysis of tumor necrosis factor, interleukins, and phosphodiesterase-4 inhibitor in the treatment of psoriatic arthritis. Presented at: The 2015 ACR/ARHP Annual Meeting, CA, USA, 6–11 November 2015.
19.
Ungprasert P, Thongprayoon C, Davis JM 3rd. Indirect comparisons of the efficacy of biological agents in patients with psoriatic arthritis with an inadequate response to traditional disease-modifying anti-rheumatic drugs or to non-steroidal anti-inflammatory drugs: a meta-analysis. Semin. Arthritis Rheum. 45(4), 428–438 (2016).
20.
Van Sanden S, Diels J, Van Laer J, Hemels M. Network meta-analysis with baseline risk adjustment to assess the relative efficacy of ustekinumab in adult patients with active psoriatic arthritis. Value Health 17(7), A373 (2014).
21.
Dias S, Sutton AJ, Ades AE, Welton NJ. Evidence synthesis for decision making 2: a generalized linear modeling framework for pairwise and network meta-analysis of randomized controlled trials. Med. Decis. Making 33(5), 607–617 (2013).
•• Sets out established standards for the modeling methodology used in our study.
22.
Jansen JP, Fleurence R, Devine B et al. Interpreting indirect treatment comparisons and network meta-analysis for health-care decision making: report of the ISPOR Task Force on Indirect Treatment Comparisons Good Research Practices: part 1. Value Health 14(4), 417–428 (2011).
• Discusses good research practices for indirect treatment comparisons.
23.
Mease PJ, Van der Heijde D, Ritchlin CT et al. A randomized, double-blind, active- and placebo-controlled Phase III study of efficacy and safety of ixekizumab, adalimumab, and placebo therapy in patients naive to biologic disease modifying anti-rheumatic drugs with active psoriatic arthritis. Arthritis Rheumatol. 67(Suppl. 10), (2015).
24.
Mease PJ, van der Heijde D, Ritchlin CT et al. Ixekizumab, an interleukin-17A specific monoclonal antibody, for the treatment of biologic-naive patients with active psoriatic arthritis: results from the 24-week randomised, double-blind, placebo-controlled and active (adalimumab)-controlled period of the Phase III trial SPIRIT-P1. Ann. Rheum. Dis. (2016) (Epub ahead of print).
25.
Mease PJ, Gladman DD, Ritchlin CT et al. Adalimumab for the treatment of patients with moderately to severely active psoriatic arthritis: results of a double-blind, randomized, placebo-controlled trial. Arthritis Rheum. 52(10), 3279–3289 (2005).
26.
Mease PJ, McInnes IB, Kirkham B et al. Secukinumab inhibition of interleukin-17A in patients with psoriatic arthritis. N. Engl. J. Med. 373(14), 1329–1339 (2015).
27.
McInnes IB, Mease PJ, Kirkham B et al. Secukinumab, a human anti-interleukin-17A monoclonal antibody, in patients with psoriatic arthritis (FUTURE 2): a randomised, double-blind, placebo-controlled, Phase III trial. Lancet 386(9999), 1137–1146 (2015).
•• This is the primary trial publication for the secukinumab data used in our analysis.
28.
Genovese MC, Mease PJ, Thomson GT et al. Safety and efficacy of adalimumab in treatment of patients with psoriatic arthritis who had failed disease modifying anti-rheumatic drug therapy. J. Rheumatol. 34(5), 1040–1050 (2007).
29.
Kavanaugh A, McInnes I, Mease P et al. Golimumab, a new human tumor necrosis factor alpha antibody, administered every four weeks as a subcutaneous injection in psoriatic arthritis: twenty-four-week efficacy and safety results of a randomized, placebo-controlled study. Arthritis Rheum. 60(4), 976–986 (2009).
30.
Antoni CE, Kavanaugh A, Kirkham B et al. Sustained benefits of infliximab therapy for dermatologic and articular manifestations of psoriatic arthritis: results from the infliximab multinational psoriatic arthritis controlled trial (IMPACT). Arthritis Rheum. 52(4), 1227–1236 (2005).
31.
Antoni C, Krueger GG, de Vlam K et al. Infliximab improves signs and symptoms of psoriatic arthritis: results of the IMPACT 2 trial. Ann. Rheum. Dis. 64(8), 1150–1157 (2005).
32.
Mease PJ, Goffe BS, Metz J, VanderStoep A, Finck B, Burge DJ. Etanercept in the treatment of psoriatic arthritis and psoriasis: a randomised trial. Lancet 356(9227), 385–390 (2000).
33.
Mease PJ, Kivitz AJ, Burch FX et al. Etanercept treatment of psoriatic arthritis: safety, efficacy, and effect on disease progression. Arthritis Rheum. 50(7), 2264–2272 (2004).
34.
Kavanaugh A, Mease PJ, Gomez-Reino JJ et al. Treatment of psoriatic arthritis in a Phase III randomised, placebo-controlled trial with apremilast, an oral phosphodiesterase 4 inhibitor. Ann. Rheum. Dis. 73(6), 1020–1026 (2014).
35.
Cutolo M, Myerson GE, Fleischmann RM et al. A Phase III, randomized, controlled trial of apremilast in patients with psoriatic arthritis: results of the PALACE 2 trial. J. Rheumatol. 43(9), 1724–1734 (2016).
36.
Cutolo M, Myerson GE, Fleischmann RM et al. Long-term (52-week) results of a Phase III, randomized, controlled trial of apremilast, an oral phosphodiesterase 4 inhibitor, in patients with psoriatic arthritis (PALACE 2). Arthritis Rheum. 65(Suppl. 10), 815 (2013).
37.
Birbara C, Blanco FJ, Crowley JJ, Hu C, Stevens R, Edwards CJ. Apremilast, an oral phosphodiesterase 4 inhibitor, in patients with psoriatic arthritis including current skin involvement: results of a Phase III, randomized, controlled trial. Ann. Rheum. Dis. 72(Suppl. 3), A85–A86 (2013).
38.
Sterry W, Ortonne JP, Kirkham B et al. Comparison of two etanercept regimens for treatment of psoriasis and psoriatic arthritis: PRESTA randomised double blind multicentre trial. BMJ 340, c147 (2010).
39.
McInnes IB, Kavanaugh A, Gottlieb AB et al. Efficacy and safety of ustekinumab in patients with active psoriatic arthritis: 1 year results of the Phase III, multicentre, double-blind, placebo-controlled PSUMMIT 1 trial. Lancet 382(9894), 780–789 (2013).
40.
Ritchlin C, Rahman P, Kavanaugh A et al. Efficacy and safety of the anti-IL-12/23 p40 monoclonal antibody, ustekinumab, in patients with active psoriatic arthritis despite conventional non-biological and biological anti-tumour necrosis factor therapy: 6-month and 1-year results of the Phase III, multicentre, double-blind, placebo-controlled, randomised PSUMMIT 2 trial. Ann. Rheum. Dis. 73(6), 990–999 (2014).
41.
Mease PJ, Fleischmann R, Deodhar AA et al. Effect of certolizumab pegol on signs and symptoms in patients with psoriatic arthritis: 24-week results of a Phase III double-blind randomised placebo-controlled study (RAPID-PsA). Ann. Rheum. Dis. 73(1), 48–55 (2014).
42.
Schett G, Wollenhaupt J, Papp K et al. Oral apremilast in the treatment of active psoriatic arthritis: results of a multicenter, randomized, double-blind, placebo-controlled study. Arthritis Rheum. 64(10), 3156–3167 (2012).
43.
Dias S, Sutton AJ, Welton NJ, Ades AE. National Institute for Health and Care Excellence Decision Support Unit technical support document no. 3. Heterogeneity: subgroups, meta-regression, bias and bias-adjustment (2012). www.nicedsu.org.uk.
44.
European Medicines Agency (EMA). Assessment report: Otezla. International non-proprietary name: apremilast (2014). www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Public_assessment_report/human/003746/WC500182629.pdf.
45.
European Medicines Agency (EMA). EPAR summary for the public. Stelara (ustekinumab) (2016). www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Summary_for_the_public/human/000958/WC500058509.pdf.
46.
Orbai AM, Ogdie A. Patient-reported outcomes in psoriatic arthritis. Rheum. Dis. Clin. North Am. 42(2), 265–283 (2016).
47.
National Institute for Health and Care Excellence (NICE). Multiple technology appraisal. Certolizumab pegol and secukinumab for treating active psoriatic arthritis following inadequate response to disease modifying anti-rheumatic drugs [ID579]. Committee papers (2016). www.nice.org.uk/guidance/GID-TAG521/documents/committee-papers.
48.
Phillippo DM, Ades AE, Dias S, Palmer S, Abrams KR, Welton NJ. NICE DSU technical support document 18: methods for population-adjusted indirect comparisons in submissions to NICE. Report by the Decision Support Unit (2016). http://research-information.bristol.ac.uk/files/94868463/Population_adjustment_TSD_FINAL.pdf.
49.
Nash P, McInnes IB, Mease PJ et al. Secukinumab versus adalimumab for psoriatic arthritis: comparative effectiveness up to 48 weeks using a matching-adjusted indirect comparison. Rheumatol. Ther. 5(1), 99–122 (2018).
Information & Authors
Information
Published In
Copyright
© 2018 Steffen M Jugl.
History
Received: 19 July 2018
Accepted: 3 September 2018
Published online: 19 September 2018
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Secukinumab for psoriatic arthritis: comparative effectiveness versus licensed biologics/apremilast: a network meta-analysis. (2018) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2018-0075
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Matthew L. Stoll, Peter A. Nigrovic, Psoriatic Juvenile Idiopathic Arthritis, Textbook of Pediatric Rheumatology, 10.1016/B978-0-443-11980-4.00021-0, (286-297), (2027).
- Muhammad Saad Khan, Saim Mahmood Khan, Rabia Farooq, Aliza Arif, Abiha Murshid, Muhammad Abdullah, Ayesha Ismail, Jawairya Muhammad Hussain, Shayan Rahim, Syeda Neha Ahmed, Surraiya Riaz Mahmood Khan, Efficacy, Safety, and Tolerability of Secukinumab in Psoriatic Arthritis: A Systematic Review and Meta-Analysis, Annals of Pharmacotherapy, 10.1177/10600280261442115, (2026).
- Maria E. Ramos-Nino, Operationalizing Chronic Inflammation: An Endotype-to-Care Framework for Precision and Equity, Clinics and Practice, 10.3390/clinpract15120233, 15, 12, (233), (2025).
- Epipode Ntawuyamara, Baoqing Deng, Yanhua Liang, Cutaneous and systemic improvements in psoriasis patients after different biologic treatments in a real-world longitudinal prospective study, Scientific Reports, 10.1038/s41598-025-99075-9, 15, 1, (2025).
- Kevin L Winthrop, Philip Mease, Andreas Kerschbaumer, Reinhard E Voll, Ferdinand C Breedveld, Josef S Smolen, Jacques-Eric Gottenberg, Xenofon Baraliakos, Hans P Kiener, Daniel Aletaha, John D Isaacs, Maya H Buch, Mary K Crow, Jonathan Kay, Leslie Crofford, Ronald F van Vollenhoven, Caroline Ospelt, Stefan Siebert, Margreet Kloppenburg, Iain B McInnes, Tom WJ Huizinga, Ellen M Gravallese, Unmet need in rheumatology: reports from the Advances in Targeted Therapies meeting, 2023, Annals of the Rheumatic Diseases, 10.1136/ard-2023-224916, 83, 4, (409-416), (2024).
- Thais Montezuma, Livia Fernandes Probst, Matheus Oliveira Almeida, Effectiveness and safety of biological and target synthetic drugs treatment for psoriatic arthritis: a systematic review with network meta-analysis, Advances in Rheumatology, 10.1186/s42358-024-00361-3, 64, 1, (2024).
- Peter Nash, Jan P Dutz, Steve Peterson, Barkha P Patel, Kiefer Eaton, May Shawi, Federico Zazzetti, James Cheng-Chung Wei, Systematic literature review and network meta-analysis of therapies for psoriatic arthritis on patient-reported outcomes, BMJ Open, 10.1136/bmjopen-2022-062306, 13, 11, (e062306), (2023).
- Bente Glintborg, Daniela Di Giuseppe, Johan Karlsson Wallman, Dan C Nordström, Bjorn Gudbjornsson, Merete Lund Hetland, Johan Askling, Gerdur Grondal, Tuulikki Sokka, Sella A Provan, Brigitte Michelsen, Eirik Klami Kristianslund, Lene Dreyer, Thorvardur Jon Love, Ulf Lindström, Uptake and effectiveness of newer biologic and targeted synthetic disease-modifying antirheumatic drugs in psoriatic arthritis: results from five Nordic biologics registries, Annals of the Rheumatic Diseases, 10.1136/ard-2022-223650, 82, 6, (820-828), (2023).
- Piyameth Dilokthornsakul, Ratree Sawangjit, Manathip Osiri, Praveena Chiowchanwisawakit, Worawit Louthrenoo, Unchalee Permsuwan, Cost-Utility Analysis of Biologic Disease-Modifying Antirheumatic Drugs for Patients With Psoriatic Arthritis in Thailand, Value in Health Regional Issues, 10.1016/j.vhri.2022.10.005, 34, (40-47), (2023).
- Iain B McInnes, Laura M Sawyer, Kristen Markus, Corinne LeReun, Celia Sabry-Grant, Philip S Helliwell, Targeted systemic therapies for psoriatic arthritis: a systematic review and comparative synthesis of short-term articular, dermatological, enthesitis and dactylitis outcomes, RMD Open, 10.1136/rmdopen-2021-002074, 8, 1, (e002074), (2022).