The economic and humanistic burden of patients in receipt of current available therapies for nAMD
Abstract
Aim: To determine the economic and humanistic burden of neovascular age-related macular degeneration (nAMD) in a cohort of patients treated with anti-VEGF in Europe and the US. Patients & methods: 79 respondents from the EU and 63 from the US with a self-reported diagnosis of nAMD and in current receipt of treatment, as reported in an international, general population survey, were compared with non-nAMD controls. Results: Anti-VEGF-treated nAMD patients in the EU had a greater utilization of healthcare resources, poorer quality of life and greater overall activity impairment versus non-nAMD controls. In the US cohort, treated nAMD patients had significantly greater resource utilization for ophthalmologist visits only. Conclusion: The burden of care associated with nAMD on EU and US healthcare systems, and on patients who are in receipt of nAMD therapy, is significant and likely to be unsustainable.
Age-related macular degeneration (AMD) is a disease of the macular region of the retina, which is characterized by degeneration of photoreceptors, ultimately leading to a loss of central vision. In its advanced form, AMD may be classified as neovascular (also referred to as ‘wet’ AMD) or geographic atrophy, and although neovascular AMD (nAMD) is less prevalent than geographic atrophy, it is responsible for the majority of AMD-related blindness.
A recent systemic review and meta-analysis estimated global prevalence of all forms of AMD taken together to be 8.69%[1]. Due to the rapidly aging population, it has been predicted that the number of persons having AMD in the US is to increase by 50% to almost 3 million between years 2000 and 2020 [2]. Similarly, in Europe, recent data suggest the prevalence of advanced AMD will increase from 2.7 million people in 2016 to 3.9 million people in 2040 [3].
Current standard of care for nAMD is regular intravitreal injections of anti-VEGF. The efficacy and safety of anti-VEGF therapy has been demonstrated in several clinical trials [4–6]. The visual gains observed in clinical trials have been replicated in real world settings, [7] although this is dependent on adequate treatment, which is not always achieved in routine clinical practice [8]. Nevertheless, in a study by Bressler et al., it was estimated that in comparison to no treatment, monthly anti-VEGF therapy has the potential to reduce the number of nAMD patients in the US progressing to legal blindness by 72% [9].
From an economic standpoint, the burden of nAMD is significant. Brown et al. estimated in 2005 that total yearly loss to the GDP in the US due to lost wages among all people with nAMD was over 5 billion USD [10]. Similarly from the patient's perspective, the physical and physiological impact of vision loss represents a significant burden. Vision loss in nAMD has been shown to affect health-related quality of life (HRQoL) scores, be related to a greater likelihood of depression, [11] and to affect work productivity and overall health status [12,13].
Much of the evidence relating to the burden of nAMD on patients and health resources was published prior to advent of anti-VEGF therapy. This retrospective, cross-sectional study was designed to determine the humanistic and economic burden of illness of patients in receipt of current available therapies.
Patients & methods
The primary objective of this retrospective, cross-sectional analysis was to estimate the burden of illness associated with nAMD in patients who reported receiving treatment for the disease in terms of health-resource use through matched comparison with adults without nAMD, as reported in the National Health and Wellbeing Survey (NHWS). Secondary objectives included an estimation of illness burden associated with nAMD in terms of HRQoL, activity impairment and health status through matched comparison with adults without nAMD.
The NHWS from Kantar Health is the largest international self-reported patient outcomes study in the healthcare industry. The database provides disease-specific measures, including the experience, diagnosis, and treatment of nAMD. To maximize sample size for patients with nAMD in the EU5, we combined 2010, 2011 and 2013 NHWS datasets (the nAMD module was not included in the 2012 survey, hence data were unavailable for analysis) and used the US 2015 dataset. At the time the study was conducted, the most recently available data were used to provide a reasonable sample size in order to detect an increase in healthcare resource use.
A total of 79 respondents from the EU5 countries and 63 from the US, aged 50 years or older, who reported having AMD, received a diagnosis of nAMD and who were treated therapeutically for nAMD were included in our final analysis. Propensity matching (1-to-4 ratio of treated nAMD patients to non-AMD patients) was used to construct a comparison group of respondents without nAMD. The baseline characteristics of those non-nAMD controls are presented in Table 1. The matching process was based on results of the bivariate comparisons between treated nAMD and non-AMD groups, whereby statistically significant (p < 0.100) variables were included in the logistic model used to create propensity scores. Variables included in the matching process were country, year of survey, age, sex, possession of private health insurance and an indicator of socioeconomic status. A greedy matching algorithm was then applied to the resultant propensity scores to create the match. A post-match assessment was conducted. Any differences that remained statistically significant after matching were controlled for in subsequent regression analysis (i.e., doubly robust matching). Adjustment using multivariate analysis was only required for the EU cohort due to residual confounding that remained and identified using standardized mean differences for covariates >0.2.
| Characteristic | EU5 cohort | US cohort | ||
|---|---|---|---|---|
| Non-nAMD n = 72,036 | nAMD n = 79 | Non-nAMD n = 41,351 | nAMD n = 63 | |
| Age mean (SD), years | 61.9 (7.9) | 69.3 (7.5) | 62.9 (8.2) | 71.6 (7.1) |
| Gender (%): | 53.3 | 54.4 | 47.2 | 54.0 |
| – Male | 46.7 | 45.6 | 52.8 | 46.0 |
| – Female | ||||
| Race/ethnicity:† | – | – | 7.3 | 1.6 |
| – African American | – | – | 0.3 | 0.0 |
| – American Indian | – | – | 2.8 | 1.6 |
| – Asian | – | – | 4.7 | 0.0 |
| – Hispanic | – | – | 80.2 | 93.7 |
| – White | – | – | 4.3 | 3.2 |
| – Mixed | – | – | 0.5 | 0.0 |
| – Other | ||||
| Mean (SD) Charlson comorbidity index | 0.47 (0.93) | 1.27 (3.97)‡ | 0.68 (1.19) | 1.59 (1.92)‡ |
| Alcohol use (%): | 13.7 | 11.4 | 7.2 | 12.7 |
| – Daily | 63.6 | 55.7 | 55.6 | 33.3 |
| – Less than daily | 22.7 | 32.9 | 37.2 | 54.0 |
| – None | ||||
| BMI (%): | 40.0 | 54.4 | 34.9 | 36.5 |
| – Overweight | 22.5 | 13.9 | 34.3 | 38.1 |
| – Obese | ||||
| Smoking status (%): | 21.8 | 20.3 | 15.2 | 7.9 |
| – Current | 42.1 | 49.4 | 34.4 | 55.6 |
| – Former | 36.1 | 30.4 | 50.4 | 36.5 |
| – Never | ||||
| Employment status (%): | 41.8 | 13.9 | 44.6 | 20.6 |
| – Employed | 58.2 | 86.1 | 55.4 | 79.4 |
| – Unemployed | ||||
†US only.
‡Statistically significant (0.000).
<2% of the total sample had missing/‘don't know’ data.
BMI: Body mass index; nAMD: Neovascular age-related macular degeneration; SD: Standard deviation.
Healthcare resources utilization was assessed in the NHWS as all-cause healthcare provider (HCP) visits, ophthalmologist visits, emergency room (ER) visits and hospitalizations in the past 6 months. HRQoL was assessed using the Medical Outcomes Study Short Form Survey Instrument 12-Item (SF-12v2) or 36-Item v2 (SF-32v2), which provides the same metrics [14]. This is a multipurpose, generic HRQoL instrument with two calculated summary scores: the physical component score (PCS) an index of overall physical functioning, and the mental component summary score, an index of overall mental functioning. The PCS and mental component summary scores have a mean of 50 and a standard deviation of ten for the US population. Scores can be interpreted relative to this population average of 50 as well as with other comparison groups of interest. Higher scores indicate better quality of life. This scale also generated the SF-6D score, a health state utility index. This index has interval scoring properties and yields summary scores on a theoretical 0–1 scale with higher scores indicating better quality of life.
Activity impairment was assessed using the Work Productivity and Activity Impairment (WPAI-GH) questionnaire, a six-item validated instrument [15]. Since most of the patients are not employed, the focus of this scale is on activity impairment which measures the percentage of impairment in daily activities because of one's health in the past 7 days.
Self-report of anxiety was identified as respondents having experienced one of more of the following anxieties in the preceding 12 months: anxiety, general anxiety disorder, panic disorder, phobia, post-traumatic stress and obsessive-compulsive disorder. Self-reported depression was defined as experienced depression in the previous 12 months. Self-reported sleep problems was defined as respondents who experienced either insomnia or sleep difficulties in the previous 12 months.
Analyses were performed in Statistical Package for the Social Sciences version 22. Outcome variables included health status questions for healthcare resource use, physical and mental health status, work productivity and psychological complaints (anxiety, depression and sleep difficulties). Demographic and patient characteristic differences between those being treated for nAMD and those without nAMD were examined. For categorical variables, chi-square tests were used to determine significant differences, while t-tests were used for continuous variables. Generalized linear mixed models taking the matched structure of the data into account were used to assess the association between presence of nAMD and work and health outcomes. Covariates included patient characteristics such as demographics (e.g., age, gender, race [US only] and employment status), general health characteristics and the Charlson comorbidity index [16].
Results
A total of 167,631 subjects completed the NHWS in the EU5, while 97,700 subjects completed the survey in the US. After applying the exclusion criteria, 79 subjects and 63 subjects from the EU5 and the US, respectively, were eligible for inclusion in the analysis. Subject flow charts for the EU5 and the US are presented in Figures 1 and 2, respectively.
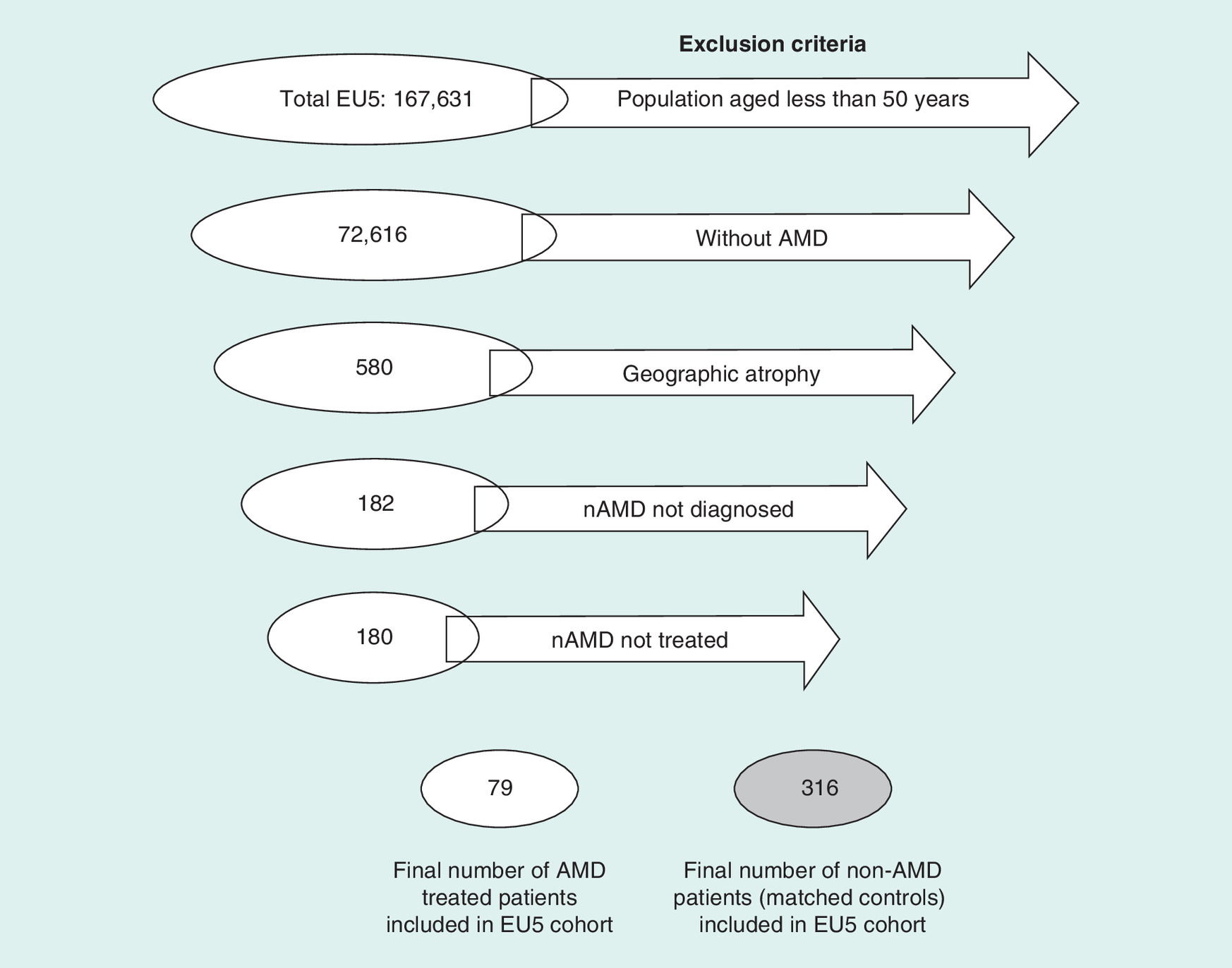
Figure 1. EU5 cohort flow chart.
AMD: Age-related macular degeneration; nAMD: Neovascular age-related macular degeneration.
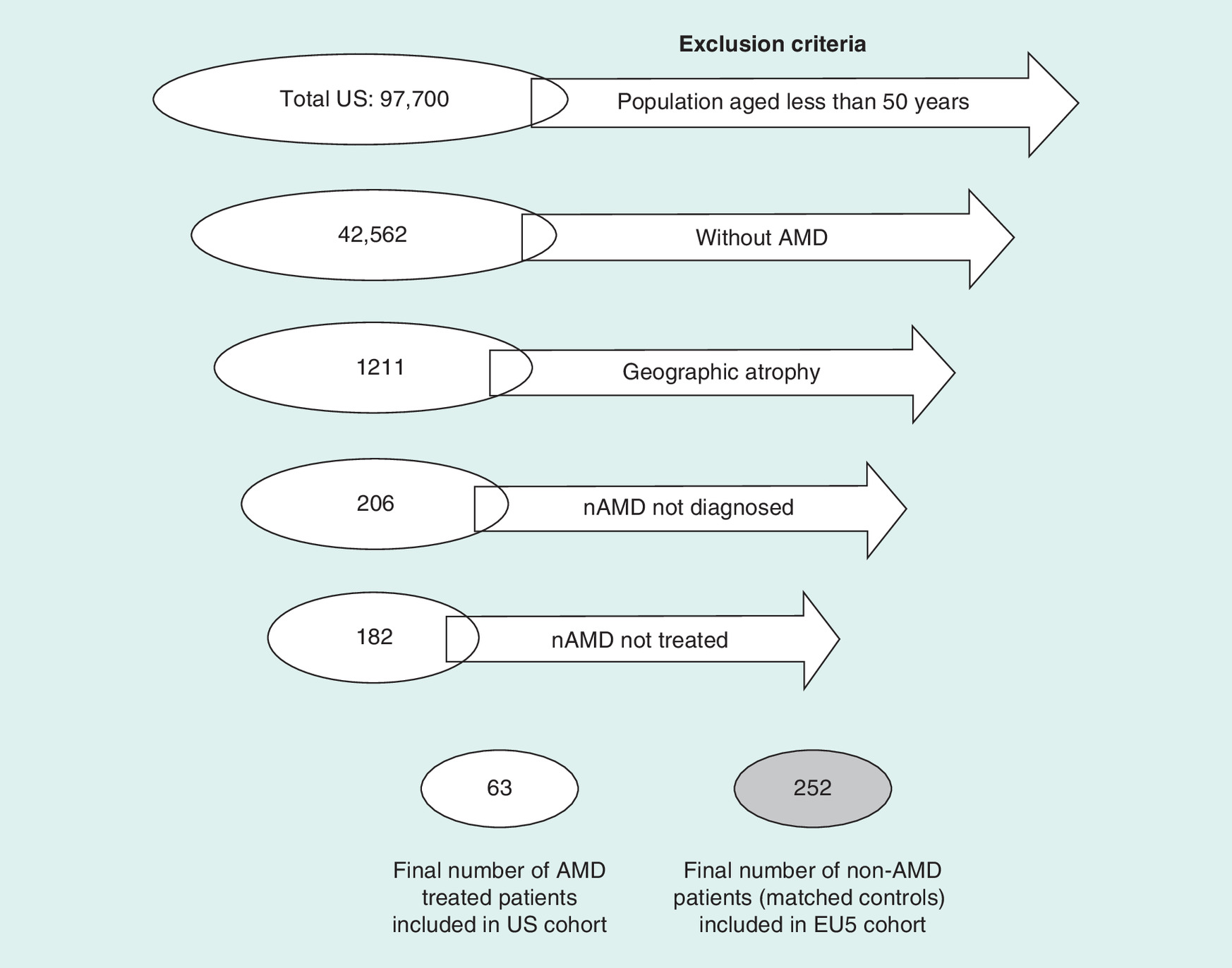
Figure 2. US cohort flow chart.
AMD: Age-related macular degeneration; nAMD: Neovascular age-related macular degeneration.
The survey is cross-sectional and therefore each question reflects a snapshot of the nAMD patient at a specific point in time. All nAMD respondents received a diagnosis of nAMD and were therapeutically treated at the time of the survey. Data for length of diagnosis were available for only 40% of EU patients and 100% of US patients, with an average length of diagnosis of 8.5 ± 8.6 years or 5.2 ± 6.2 years for EU and US patients, respectively.
Baseline demographics for those in the EU5 cohort and in the US cohort are presented in Table 1.
EU5
Healthcare resource utilization
In adjusted models of the EU5 cohort, healthcare resource use varied between groups. A greater number of nAMD patients reported visiting any HCP in the previous 6 months (99%; 95% CI: 93–100%) compared with controls (92%; CI: 87-95%, p = 0.001). A greater number of nAMD patients reported visiting an ophthalmologist in the previous 6 months (75%; 95% CI: 64-84%) compared with controls (22%; 95% CI: 17–28%, p = 0.000). The average number of visits in the previous 6 months were greater for nAMD patients than their non-nAMD matched controls for HCP visits (14.80 versus 6.28, p = 0.000), ophthalmologist visits (2.77 versus 0.33, p = 0.000), hospitalizations (0.48 versus 0.18, p = 0.004) and ER visits (0.62 versus 0.26, p = 0.007).
Health-related quality of life
Patients with nAMD had lower PCS scores compared with controls: 42.07 (95% CI: 39.74–44.41) versus 45.92 (95% CI: 44.64–47.21) (p = 0.003). This represented a minimally important difference (>3 point difference in PCS score). Compared with controls, patients with nAMD had lower health utility scores (SF-6D): 0.67 (95% CI: 0.64–0.70) versus 0.72 (95% CI: 0.70–0.73) (p = 0.004). This represented a minimally important difference (>0.041 difference in health utility score).
Activity impairment
Patients with nAMD had greater overall activity impairment compared with their matched controls (39.24% [95% CI: 30.98–49.71] vs 28.52% [95% CI: 25.13–32.38]; p = 0.026).
Health status
Health status parameters were comparable between groups. The percentage of patients experiencing anxiety was 15% in both groups (p = 0.988). The percentage of patients experiencing depression in the nAMD group versus the control group was 8 versus 12% (p = 0.352). The percentage of patients experiencing sleep problems in the nAMD group versus the control group was 24 versus 32% (p = 0.190).
US
Healthcare resource utilization
In the US cohort, no differences were observed between groups with respect to the percentage of patients visiting any HCP in the previous 6 months: 100% nAMD versus 96.4% for controls (p = 0.128). There was a significant difference in the percentage of patients who visited their ophthalmologist in the previous 6 months (49.2% for nAMD patients compared with 25.8% for controls in the 6 months previously [p = 0.000]). The average number of HCP visits in the previous 6 months were comparable between both groups (7.46 visits for nAMD patients versus 6.19 for non-nAMD matched controls; p = 0.153). The average number of ophthalmologist visits in the previous 6 months were greater for nAMD patients than their non-nAMD matched controls (1.67 versus 0.33; p = 0.000).
Health-related quality of life
No group differences were observed in PCS scores between nAMD subjects and controls (45.51 versus 45.65, respectively; p = 0.925). Similarly, health utility scores (SF-6D) were comparable between both groups (0.74 versus 0.72; p = 0.465).
Health status
Health status parameters were comparable between groups. The percentage of patients experiencing anxiety in the nAMD group versus the control group was 26% versus 19% (p = 0.265). The percentage of patients experiencing depression in the nAMD group versus the control group was 18 versus 19% (p = 0.768). The percentage of patients experiencing sleep problems in the nAMD group versus the control group was 29 versus 30% (p = 0.902).
Discussion
This study was designed to examine the economic and humanistic burden of disease in nAMD in a patient population where the predominant treatment was anti-VEGF therapy, and to determine if differences exist in disease burden between patients in the EU and the US. In brief, we report that nAMD patients in the EU utilize healthcare resources to a greater extent than non-nAMD patients, which is reflected in a greater number of HCP visits, ER visits, hospitalizations and ophthalmologist visits. EU nAMD patients also reported poorer quality of life compared with non-nAMD patients, manifesting in lower PCS scores, health utility scores and impaired overall activity. EU nAMD patients also had greater overall activity impairment compared with their matched controls. In the US cohort, we report that nAMD patients had significantly greater healthcare resource utilization for ophthalmologist visits only. Of note, no differences were found between US nAMD patients and their matched controls with respect to any HRQoL measures, activity impairment measures or overall health status. Since most of the patients were unemployed, work productivity was not assessed.
To our knowledge, this is the first study to compare and contrast the illness burden of nAMD on patients versus non-nAMD controls since the advent of anti-VEGF therapy as the standard of care. Our results suggest that in the EU5, nAMD patients place a significant demand on health resources. This is unsurprising as the number of nAMD patients continues to grow in parallel with the aging population [3]. In the US, the impact on health resource use appears to primarily affect ophthalmologists, but not other health resources, in other words, hospitalizations, ER visits and HCP visits.
The quality of life of nAMD patients in the EU5 is also affected by their disease. They tend to be less physically able than non-nAMD patients, as reflected in lower PCS scores. This finding is consistent with previous studies in EU populations, [17,18] where nAMD and its associated vision loss significantly lessens the patients quality of life. Interestingly, HRQoL appeared to be unaffected between those with and without nAMD in the US population. This unexpected finding may be attributable to the lower mean age of nAMD patients who completed the NHWS survey. The mean patient age was 69 years, which is a relatively young and may not represent the typical nAMD patient, who, on average, would be approximately 10 years older and have additional comorbidities [19].
In the interpretation of these findings, it is important to acknowledge the study limitations. First, both the EU and the US sample size were small and composed of relatively young nAMD patients, potentially impacting the representativeness and generalizability of the findings to the typical nAMD population. Furthermore, the data collection methodology was based on patient recall and therefore open to recall bias, for example, healthcare utilization data based on recall from the previous 6 months. Furthermore, the data were collected via an online survey. Therefore, no data were collected relating to visual acuity or ocular comorbidities which may have influenced the frequency of visits to their ophthalmologist. Furthermore, those with poorer VA may not be captured as severity of visual impairment may impact their ability to complete the survey. Although matching and regression adjustment addressed confounders of measured variables, analytical groups (those with and without nAMD) may differ on unmeasured variables, potentially biasing the results. It should also be noted that healthcare systems/reimbursement across the EU varies widely and we were unable to control for this in our analysis. Finally, no formal comparison was conducted between the EU and the US cohorts preventing any meaningful comment on the apparent differences observed in the disease burden between these two populations.
Conclusion
These results suggest that nAMD results in a broad treatment burden on patients and healthcare providers. For the EU in particular, nAMD patients appear to place a significant demand on health resources. Future therapies should focus on reducing the treatment burden of regular intravitreal injections while maintaining high standards of efficacy and safety. In doing so, it may be possible to lessen the treatment burden of nAMD on healthcare systems.
Future perspective
The prevalence of nAMD is projected to increase markedly owing to an ageing population. This will place further demands on healthcare systems. Advancements in the provision of care for nAMD patients will be necessary to alleviate the burden placed on healthcare systems, patients and their caregivers.
In terms of healthcare utilization, in the EU, a greater number of neovascular age-related macular degeneration (nAMD) patients reported visiting any healthcare professional (HCP) and visiting an ophthalmologist in the previous 6 months compared with non-nAMD controls.
The frequency of visits to the ophthalmologist, hospital and emergency room were also greater in the nAMD group.
nAMD subjects in the EU cohort also displayed lower physical component summary (PCS) scores and lower health utility scores compared with non-nAMD controls.
In the US cohort, nAMD patients had significantly greater resource utilization for ophthalmologist visits only.
These results confirm that nAMD results in a broad treatment burden on patients and healthcare providers. For the EU in particular, nAMD patients place a significant demand on health resources.
Acknowledgments
The authors thank Judit Banhazi for her valuable contributions to the manuscript content.
Financial & competing interests disclosure
This study was supported by funding from Novartis Pharma AG, Basel, Switzerland. D H. Jaffe is an employee of Kantar Health, which has received funding from Novartis Pharma AG. W Chan, V Bezlyak and A Skelly are employees of Novartis. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing assistance was provided by M Kirby from Novartis Ireland Limited.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
References
1.
Wong WL, Su X, Li X et al. Global prevalence of age-related macular degeneration and disease burden projection for 2020 and 2040: a systematic review and meta-analysis. Lancet Glob. Health. 2(2), e106–e116 (2014).
2.
Friedman DS, O'Colmain BJ, Munoz B et al. Prevalence of age-related macular degeneration in the United States. Arch. Ophthalmol. 122(4), 564–572 (2004).
3.
Colijn JM, Buitendijk GHS, Prokofyeva E et al. Prevalence of age-related macular degeneration in Europe: the past and the future. Ophthalmology 124(12), 1753–1763 (2017).
4.
Brown DM, Michels M, Kaiser PK et al. Ranibizumab versus verteporfin photodynamic therapy for neovascular age-related macular degeneration: two-year results of the ANCHOR study. Ophthalmology 116(1), 57–65.e5 (2009).
5.
Ho AC, Busbee BG, Regillo CD et al. Twenty-four-month efficacy and safety of 0.5 mg or 2.0 mg ranibizumab in patients with subfoveal neovascular age-related macular degeneration. Ophthalmology 121(11), 2181–2192 (2014).
6.
Schmidt-Erfurth U, Kaiser PK, Korobelnik JF et al. Intravitreal aflibercept injection for neovascular age-related macular degeneration: ninety-six-week results of the VIEW studies. Ophthalmology 121(1), 193–201 (2014).
7.
Peden MC, Suner IJ, Hammer ME et al. Long-term outcomes in eyes receiving fixed-interval dosing of anti-vascular endothelial growth factor agents for wet age-related macular degeneration. Ophthalmology 122(4), 803–808 (2015).
8.
Razi F, Haq A, Tonne P et al. Three-year follow-up of ranibizumab treatment of wet age-related macular degeneration: influence of baseline visual acuity and injection frequency on visual outcomes. Clin. Ophthalmol. 10, 313–319 (2016).
9.
Bressler NM, Doan QV, Varma R et al. Estimated cases of legal blindness and visual impairment avoided using ranibizumab for choroidal neovascularization: non-Hispanic white population in the United States with age-related macular degeneration. Arch. Ophthalmol. 129(6), 709–717 (2011).
10.
Brown MM, Brown GC, Stein JD et al. Age-related macular degeneration: economic burden and value-based medicine analysis. Can. J. Ophthalmol. 40(3), 277–287 (2005).
11.
Dawson SR, Mallen CD, Gouldstone MB et al. The prevalence of anxiety and depression in people with age-related macular degeneration: a systematic review of observational study data. BMC Ophthalmol. 14, 78 (2014).
12.
Bandello F, Lafuma A, Berdeaux G. Public health impact of neovascular age-related macular degeneration treatments extrapolated from visual acuity. Invest. Ophthalmol. Vis. Sci. 48(1), 96–103 (2007).
13.
Dong LM, Childs AL, Mangione CM et al. Health- and vision-related quality of life among patients with choroidal neovascularization secondary to age-related macular degeneration at enrollment in randomized trials of submacular surgery: SST report no. 4. Am. J. Ophthalmol. 138(1), 91–108 (2004).
14.
Huo T, Guo Y, Shenkman E et al. Assessing the reliability of the short form 12 (SF-12) health survey in adults with mental health conditions: a report from the wellness incentive and navigation (WIN) study. Health Qual. Life Outcomes 16(1), 34 (2018).
15.
Zhang W, Bansback N, Boonen A et al. Validity of the work productivity and activity impairment questionnaire – general health version in patients with rheumatoid arthritis. Arthritis Res. Ther. 12(5), R177 (2010).
16.
Chaudhry S, Jin L, Meltzer D. Use of a self-report-generated Charlson Comorbidity Index for predicting mortality. Med. Care 43(6), 607–615 (2005).
17.
Ruiz-Moreno JM, Coco RM, Garcia-Arumi J et al. Burden of illness of bilateral neovascular age-related macular degeneration in Spain. Curr. Med. Res. Opin. 24(7), 2103–2111 (2008).
18.
Sahel JA, Bandello F, Augustin A et al. Health-related quality of life and utility in patients with age-related macular degeneration. Arch. Ophthalmol. 125(7), 945–951 (2007).
19.
Mehta H, Tufail A, Daien V et al. Real-world outcomes in patients with neovascular age-related macular degeneration treated with intravitreal vascular endothelial growth factor inhibitors. Prog. Retin. Eye Res. 65, 127–146 (2018).
Information & Authors
Information
Published In
Copyright
© 2018 Jaffe, Chan, Bezlyak, Skelly.
History
Received: 22 June 2018
Accepted: 3 August 2018
Published online: 21 September 2018
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
The economic and humanistic burden of patients in receipt of current available therapies for nAMD. (2018) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2018-0058
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Qianyi Deng, Kazumasa Kishimoto, Osamu Sugiyama, Masahiro Miyake, Hiroshi Tamura, Automatic selection of optical coherence tomography images for prognostic prediction models in age-related macular degeneration, Computer Methods and Programs in Biomedicine, 10.1016/j.cmpb.2026.109384, 282, (109384), (2026).
- Billal Hossain, Sabrina Rahmatullah, Tanvir Ahmed, Efficacy of brolucizumab and ranibizumab in diabetic macular edema and neovascular age-related macular degeneration: insights from a case series, Annals of Medicine & Surgery, 10.1097/MS9.0000000000003363, (2026).
- Xiuli Chen, Hong Bian, Zhifeng Wu, Validation of the Chinese version of the financial toxicity scale in patients with wet age-related macular degeneration, Journal of Patient-Reported Outcomes, 10.1186/s41687-025-00909-x, 9, 1, (2025).
- Seenu M. Hariprasad, Frank G. Holz, Carl V. Asche, Amine Issa, Oriol Mora, Simon Keady, Mourad F. Rezk, Phil Sarocco, Steven Simoens, Clinical and Socioeconomic Burden of Retinal Diseases: Can Biosimilars Add Value? A Narrative Review, Ophthalmology and Therapy, 10.1007/s40123-025-01104-3, 14, 4, (621-641), (2025).
- Alexander J. E. Foss, David Almeida, Chui Ming Gemmy Cheung, Yuichiro Ogura, Eduard de Cock, Theo Empeslidis, To Treat or Not to Treat? Resolving the Question of Subretinal and Intraretinal Fluid in Age-Related Macular Degeneration: A Narrative Review, Ophthalmology and Therapy, 10.1007/s40123-025-01093-3, 14, 3, (489-514), (2025).
- David T Wong, Shaheer Aboobaker, David Maberley, Sanjay Sharma, Pradeepa Yoganathan, Switching to faricimab from the current anti-VEGF therapy: evidence-based expert recommendations, BMJ Open Ophthalmology, 10.1136/bmjophth-2024-001967, 10, 1, (e001967), (2025).
- Jared S. Nielsen, Andrew Chang, Nancy M. Holekamp, Melina Cavichini-Cordeiro, Stephanie L. Lin, Dominic Heinrich, Katie F. Maass, Alicia Menezes, Natasha Singh, Dante J. Pieramici, Supplemental Intravitreal Ranibizumab Injections in Eyes Treated with the Port Delivery System with Ranibizumab in the Archway Trial, Ophthalmology Retina, 10.1016/j.oret.2024.06.012, 8, 12, (1127-1139), (2024).
- Prem A.H. Nichani, Marko M. Popovic, Andrew Mihalache, Ananya Pathak, Rajeev H. Muni, David T.W. Wong, Peter J. Kertes, Efficacy and Safety of Intravitreal Faricimab in Neovascular Age-Related Macular Degeneration, Diabetic Macular Edema, and Retinal Vein Occlusion: A Meta-Analysis, Ophthalmologica, 10.1159/000541662, 247, 5-6, (355-372), (2024).
- Sunil Patel, Philip P. Storey, Mark R. Barakat, Vrinda Hershberger, William Z. Bridges, David A. Eichenbaum, David R. Lally, David S. Boyer, Sophie J. Bakri, Monica Roy, Dario A. Paggiarino, Phase I DAVIO Trial: EYP-1901 Bioerodible, Sustained-Delivery Vorolanib Insert in Patients With Wet Age-Related Macular Degeneration, Ophthalmology Science, 10.1016/j.xops.2024.100527, 4, 5, (100527), (2024).
- Anna-Maria Kubin, Ida Korva-Gurung, Pasi Ohtonen, Nina Hautala, Health-related quality of life in patients with neovascular age-related macular degeneration: a prospective cohort study, Journal of Patient-Reported Outcomes, 10.1186/s41687-024-00775-z, 8, 1, (2024).
- See more