Systematic review and network meta-analysis: effect of biologics on radiographic progression in rheumatoid arthritis
Abstract
Aim: To evaluate the comparative effectiveness of biologics in inhibiting radiographic progression among rheumatoid arthritis (RA) patients. Materials & methods: Bayesian network meta-analysis of published trials investigating the USA FDA approved biologics treatment in RA patients, using methotrexate (MTX) as the reference comparator. Results: Nine trials met the inclusion criteria for base case analysis. Compared with MTX, most biologics (except golimumab) + MTX had significantly lower rates of radiographic progression at 1 year. Mean difference in radiographic progression rates between MTX monotherapy and biologics + MTX was highest for adalimumab + MTX (-3.8) and lowest for tocilizumab + MTX (-0.7). Inhibition of radiographic progression was sustained. Conclusion: Biologics inhibit radiographic progression in patients with RA at 1 year; however, published evidence beyond 1 year is limited.
Rheumatoid arthritis (RA) is a costly, debilitating chronic inflammatory autoimmune disease that significantly reduces patients’ ability to work and decreases their quality of life if left untreated [1]. The treat-to-target recommendations for patients with RA suggest that the long-term goal of treating patients should be to maximize their health-related quality of life by controlling signs and symptoms, normalizing physical function, inhibiting radiographic disease progress and maintaining work productivity [2]. Previously, systematic reviews and meta-analyses have examined the clinical, functional or structural efficacy of biologics in treating patients with RA [3–5]. However, the comparative efficacy of biologics in inhibiting radiographic progression is still not fully understood.
To better understand the efficacy of biologics, we compared the 1-year radiographic efficacy of biologics in patients with RA through a Bayesian network meta-analysis (NMA) of published clinical trial data. We further qualitatively reviewed radiographic data with 2–10 years of follow-up because of the absence of a sufficient number of published clinical trials available to build a robust NMA model beyond 1 year.
Materials & methods
Search & screening strategy
A systematic literature search was conducted in MEDLINE, Embase and Cochrane Central Register of Controlled Trials (CENTRAL) databases from inception through 9 September 2015 to identify published randomized controlled trials matching the predefined protocol based on the Patients, Interventions, Comparisons, Outcomes (PICO) framework (Supplementary Table 1). Additionally, available conference proceedings of American College of Rheumatology (ACR) and European League Against Rheumatism (EULAR) meetings were searched from 2006 to 2014 and 2001 to 2015 for ACR and EULAR, respectively. The search strategy used to identify articles and abstracts is provided in Supplementary Table 2. Title and abstract screening were performed by two independent reviewers, and full text screening was completed by two reviewers on any studies that fit the eligibility criteria. If assessments between the first and second reviewers differed, then a third reviewer was brought in to adjudicate.
Studies eligible for the review and meta-analysis evaluated adult patients with RA and included populations who were at least 80% biologic-naive and those with unspecified prior biologic use as they were assumed to have little or no prior biologic use. Interventions included the USA FDA approved marketed biologic therapies (abatacept 10 mg every 4 weeks, adalimumab 40 mg every 2 weeks, certolizumab 200 mg every 2 weeks, etanercept 50 mg every week, golimumab 50 mg every 4 weeks, infliximab 3 mg/kg at weeks 0, 2 and 6 then every 8 weeks, rituximab two 1000 mg infusions separated by 2 weeks (one course) every 24 weeks and tocilizumab 4 mg/kg every 4 weeks) indicated for RA in combination with methotrexate (MTX) or tocilizumab (8 mg/kg every 4 weeks) alone. Selected studies included those evaluating any of the approved biologic interventions + MTX versus MTX alone, or those evaluating tocilizumab ± MTX versus MTX alone. Randomized controlled trials, blinded and open-label extension studies, and/or follow-up studies with relevant data were included. The key outcome in each selected study was the assessment of radiographic progression (assessed using Total Sharp scores) at a minimum of 1 year. Selected studies had to have a sample size of at least 100 participants (total per study) and patients had to receive treatment for ≥4 weeks. Studies with duplicate source populations, those without the outcome of interest at the relevant analysis time point, and those using regimens not approved by the FDA were excluded from analysis.
Data extraction
Data extraction was conducted using the DOC™ Data version 2.0 software platform (Doctor Evidence LLC, CA, USA) and its universal electronic extraction form. Before data extraction began, a standardized data configuration protocol was used to define the study level variables, intervention variables, patient characteristics and specific outcomes to be digitized from eligible studies. The following data variables were extracted: publication information (including author and year), trial name, demographics (mean age, percentage of females), clinical characteristics (duration of RA), and details of interventions (dose, frequency and duration of treatment). Relevant outcome data included the mean change from baseline in Sharp score and a corresponding measure of uncertainty (e.g., standard error or confidence interval). Data were extracted from text manually by an analyst. Figure data were collected using data-point estimation software. Data reported in text and tables were used preferentially over figure estimates. Each collected data point was verified manually against the source article by a second independent reviewer. Any differences noted between the first and second reviewers were adjudicated by a third reviewer. Synonymous terms (outcomes and characteristics) were unified using the DOC Data Ontology management system (Doctor Evidence LLC). This allowed synonyms to be merged into a single preferred term while preserving the original author-reported term.
Risk of bias assessment
The Cochrane Collaboration's tool for assessing risk of bias in randomized trials was used to assess the studies identified for the analysis [6]. This instrument is used to evaluate seven domains of bias at the study and outcome level: random sequence generation (selection bias), allocation concealment (selection bias), blinding of participants and personnel (performance bias), blinding of outcome assessment (detection bias), incomplete outcome data (attrition bias), selective reporting (reporting bias) and other sources of bias (other bias). These assessments were conducted by the authors and the data were stored and managed in Microsoft Excel™ (WA, USA).
Homogeneity, similarity & consistency assessment
Similarity was assessed for the 16 studies selected for analysis by examining baseline characteristics of the patient populations and the trial design and characteristics for each study. The patient characteristics assessed included severity of RA, type of radiographic measure used, early versus established RA, age, use of disease-modifying antirheumatic drugs (DMARDs), use of previous biologics and study duration. Based on clinical judgment and assessment of study methodology, we concluded that the studies were similar enough to warrant inclusion in our analyses and provide valid outcomes. Consistency between direct and indirect evidence for a particular comparison could not be assessed because direct comparisons of the biologics were not available. Homogeneity of evidence for each comparison could also not be completely assessed because of the lack of availability of multiple studies for each comparison of interest. However, there were two comparators (certolizumab and infliximab), with multiple studies available. Although, the results were not identical, the effect estimates for the primary outcome across the individual studies with common comparators were in the same direction and of a similar magnitude. We therefore concluded that these trials were similar enough to meet the homogeneity assumption and be included in our analysis.
Study outcomes
Structural damage was analyzed as the change from baseline using the modified van der Heijde Total Sharp Score (vdHS) [7]. All studies reporting vdHS at 1 year were synthesized in the base case analysis. In addition, because the studies reported different modifications of Sharp scores, those studies reporting any version of the Sharp score at 1 year were analyzed by calculating standardized mean differences (SMD). SMD accounted for the differences in the scales by expressing the Sharp score in terms of the size of the treatment effect relative to the standard deviation in each study.
For the qualitative analysis spanning 2–10 years, data were extracted manually from published clinical trials or abstracts reporting radiographic data (change in Sharp scores) in patients treated with biologics indicated for RA as provided above. [8–32].
Subgroup analyses
We also conducted subgroup analyses for the subset of studies with early (<4 years mean RA duration) and established (≥ 4 years mean RA duration) disease.
Statistical approach
Data were synthesized by means of a fixed-effect NMA using a Bayesian framework. For all analyses, the NMA models correspond to a generalized linear model with the identity link. Noninformative prior distributions were used for all model parameters. The initial 10,000 iterations of the models were discarded as ‘burn-ins’, and inferences were based on an additional 20,000 iterations using three chains. Convergence of the chains was assessed by the Gelman−Rubin statistic and visual inspection of trace and density plots.
Results of the analyses are expressed as point estimates and 95% credible intervals for each intervention versus all other interventions. The relative differences of each intervention versus MTX are provided in the main text, and all pairwise results are available in Supplementary Table 3. Analyses were conducted with the DOC Data 2.0 platform. The platform calls on the R software (version 3.3.1) and runs the Bayesian NMA in the ‘GeMTC’ package [33–35].
Results
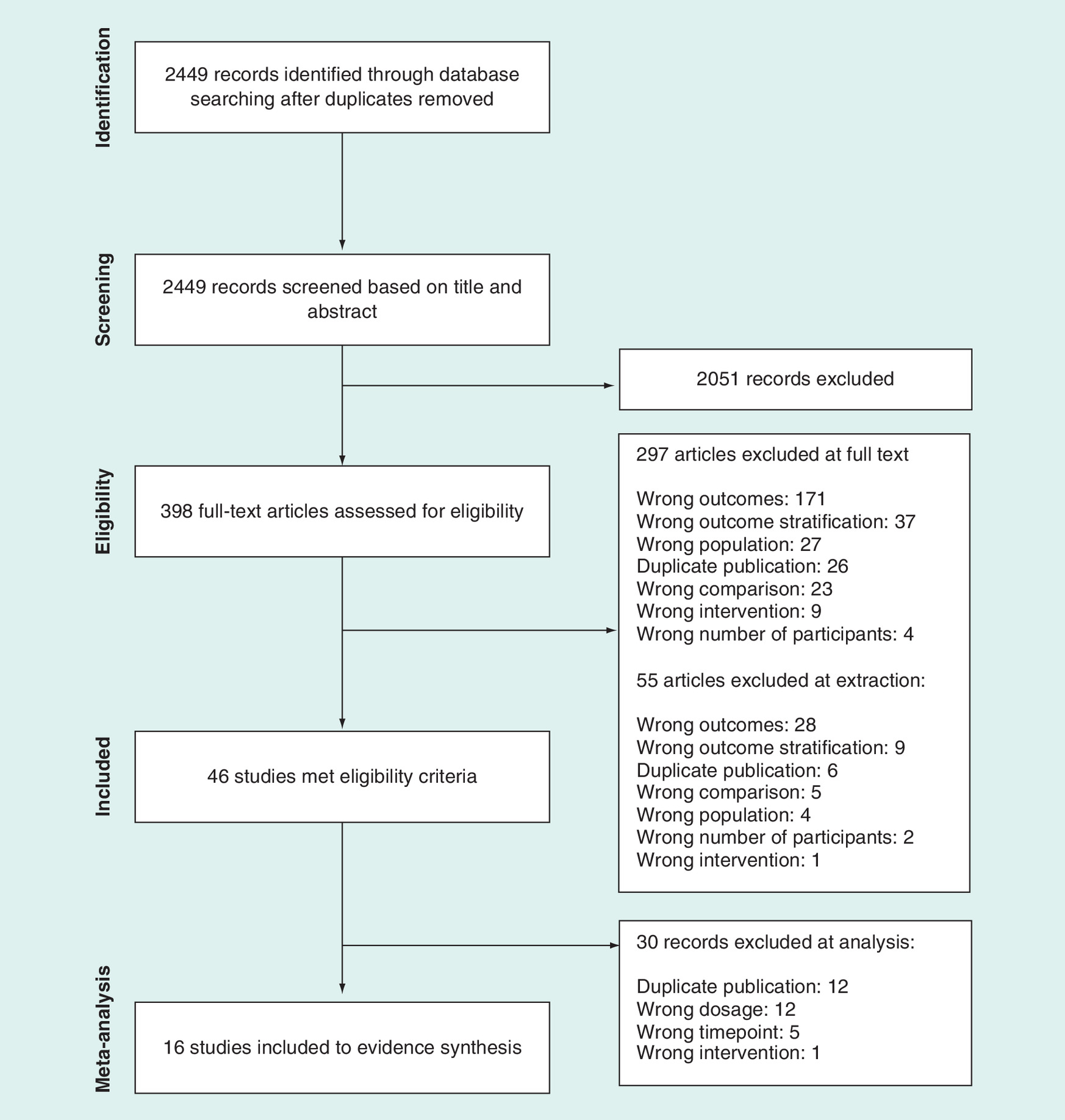
As shown in Figure 1, of the 2449 nonduplicate records screened, 46 studies met the PICO eligibility criteria and were included in the systematic review. Of these 46 studies, 16 studies were included in evidence synthesis: two abatacept studies [36,37], three adalimumab studies [38–40], three certolizumab studies [41–43], one etanercept study [44], one golimumab study [45], two infliximab studies [46,47], two rituximab studies [32,48] and two tocilizumab studies [49,50]. Common reasons for exclusion from analysis include overlapping study populations and insufficient data for analysis (missing variance or population numbers). All 16 studies enrolled patients with moderately to severely active RA. Of the analyzed studies, most did not specify whether patients used biologics before study entry and were assumed to have little or no prior biologic use. Only four studies reported potential biologic use before study entry. The greatest prior biologic use was reported in LITHE at 12% [49] and very low numbers were reported in AIM at 5% [36] and GO-BEFORE at 1% [45]. There was no indication that patients enrolled in RAPID 1 were excluded for previous biologic use; however, a drug washout period was allowed [43]. Table 1 summarizes the main characteristics of these 16 studies including the intervention and change in Sharp score from baseline to year 1 for each study. Not all baseline characteristics were reported for every study. The mean age across the groups ranged from 47 to 56 years, the majority (>67%) of patients were female, and mean duration of RA ranged from approximately 6 weeks to 11 years. Additional baseline characteristics of the study population are summarized in Supplementary Table 4.
| Study (year) | Acronym | Intervention | Patients (n) | Mean age (years) | Female (%) | Mean disease duration (months) | DMARD-naive (%) | Radiographic measure | Change in Sharp score | Included in base case | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Genant HK (2006) [36] | AIM | ABA + MTX MTX | 433 219 | – | – | – | 0 0 | Modified Genant | ABA + MTX: 1.1 MTX: 2.4 | No |
| 2 | Westhovens R (2009) [37] | AGREE | ABA + MTX MTX | 256 253 | 50.1 49.7 | 76.6 78.7 | 6.2 6.7 | 100 100 | Modified Genant | ABA + MTX: 0.6 MTX: 1.1 | No |
| 3 | Detert J (2013) [38] | HIT HARD | ADA + MTX MTX | 87 85 | 47.2 52.5 | 70.1 67.1 | 1.8 1.6 | 100 100 | Modified vdHS | ADA + MTX: 2.6 MTX: 6.4 | Yes |
| 4 | Breedveld FC (2006) [39] | PREMIER | ADA + MTX MTX | 268 257 | 51.9 52.0 | 72.0 73.9 | 8.4 9.6 | 67.5 68.5 | Modified Sharp score | ADA + MTX: 1.3 MTX: 5.7 | No |
| 5 | Keystone EC (2004) [40] | DE019 | ADA + MTX MTX | 207 200 | 56.1 56.1 | 76.3 73.0 | 132 131 | 0 0 | Modified Sharp score | ADA + MTX: 0.1 MTX: 2.7 | No |
| 6 | Emery P (2015) [42] | C-EARLY | CZP + MTX MTX | 660 219 | – | – | – | 100 100 | Modified vdHS | CZP + MTX: 0.2 MTX: 1.9 | Yes |
| 7 | van der Heijde D (2007) [43] | RAPID 1 | CZP + MTX MTX | 393 199 | – | – | – | 0 0 | Modified vdHS | CZP + MTX: 0.4 MTX: 2.8 | Yes |
| 8 | Atsumi T (2016) [41] | C-OPERA | CZP + MTX MTX | 159 157 | 49.4 49.0 | 81.1 80.9 | 4.0 4.3 | 80.5 81.5 | Modified vdHS | CZP + MTX: 0.4 MTX: 1.6 | Yes |
| 9 | Emery P (2013) [45] | GO-BEFORE | GOL + MTX MTX | 159 160 | 50.9 48.6 | 84.9 83.8 | 42.0 34.8 | 100 100 | Modified vdHS | GOL+ MTX: 0.7 MTX: 1.4 | Yes |
| 10 | Emery P (2008) [44] | COMET | ETN + MTX MTX | 274 268 | 50.5 52.3 | 74 73 | 8.8 9.3 | 82 76 | Modified vdHS | ETN + MTX: 0.3 MTX: 2.4 | Yes |
| 11 | Lipsky PE (2000) [47] | ATTRACT | INF + MTX MTX | 86 88 | 54 51 | 81 80 | 120 132 | 0 0 | Modified vdHS | INF + MTX: 1.3 MTX: 7.0 | Yes |
| 12 | Smolen JS (2006) [46] | ASPIRE | INF + MTX MTX | 373 298 | 51 50 | 71 75 | 9.6 10.8 | 71 65 | Modified vdHS | INF + MTX: 0.4 MTX: 3.7 | Yes |
| 13 | Peterfy C (2016) [48] | SCORE | RTX + MTX MTX | 60 63 | 50.7 50.3 | 83.8 76.2 | 58.8 52.8 | 0 0 | Modified Genant | RTX + MTX: 0.3 MTX: 1.4 | No |
| 14 | Tak PP (2012) [32] | IMAGE | RTX + MTX MTX | 251 252 | 47.9 48.1 | 85 77 | 11.0 10.9 | 69 70 | Modified Genant | RTX + MTX: 0.2 MTX: 1.3 | No |
| 15 | Kremer J (2009) [49] | LITHE | TCZ 4 mg + MTX MTX | 401 394 | – | – | – | 0 0 | Modified Genant | TCZ4 + MTX: 0.3 MTX: 1.1 | No |
| 16 | Burmester G (2013) [50] | FUNCTION | TCZ 4 mg + MTX MTX TCZ 8 mg | 288 287 292 | – | – | – | 100 | Modified vdHS | TCZ4 + MTX: 0.4 MTX: 1.1 TCZ8: 0.3 | Yes |
All of the studies listed in this table were included in the SMD analysis.
ABA: Abatacept; ADA: Adalimumab; CZP: Certolizumab pegol; DMARD: Disease-modifying antirheumatic drugs; DMARD-naive: Did not receive prior DMARD therapy; ETN: Etanercept; GOL: Golimumab; INF: Infliximab; MTX: Methotrexate; RTX: Rituximab; SMD: Standardized mean difference; TCZ: Tocilizumab; vdHS: van der Heijde Total Sharp Score.
Of the 16 clinical trials identified, nine used vdHS to assess radiographic progression [38,41–47,50] and were included in the base case NMA model (Figure 2). All biologics in combination with MTX and tocilizumab without MTX showed decreased radiographic progression at 1 year compared with MTX alone, as defined by negative mean difference in vdHS change (Figure 3). Most interventions showed a statistically significant effect versus MTX alone, except for golimumab 50 mg every 4 weeks and tocilizumab 8 mg/kg every 4 weeks. Among all the included biologics, the largest statistically significant mean difference at 1 year was in adalimumab, where the increase in vdHS was 3.8 fewer units in patients administered adalimumab 40 mg every 2 weeks + MTX compared with those receiving MTX alone. The patients treated with infliximab 3 mg/kg every 8 weeks had the next highest relative effect at 3.7 fewer units versus MTX alone.

Figure 2. Network of nine base case studies evaluating the effect of biologics on radiographic progression in rheumatoid arthritis at 1 year.
Circles represent the drug being evaluated; lines represent direct comparisons of the biologic with MTX; numbers in white boxes represent the number of studies included in each comparison.
ADA: Adalimumab; CZP: Certolizumab pegol; ETN: Etanercept; GOL: Golimumab; INF: Infliximab; MTX: Methotrexate; RA: Rheumatoid arthritis; TCZ: Tocilizumab.
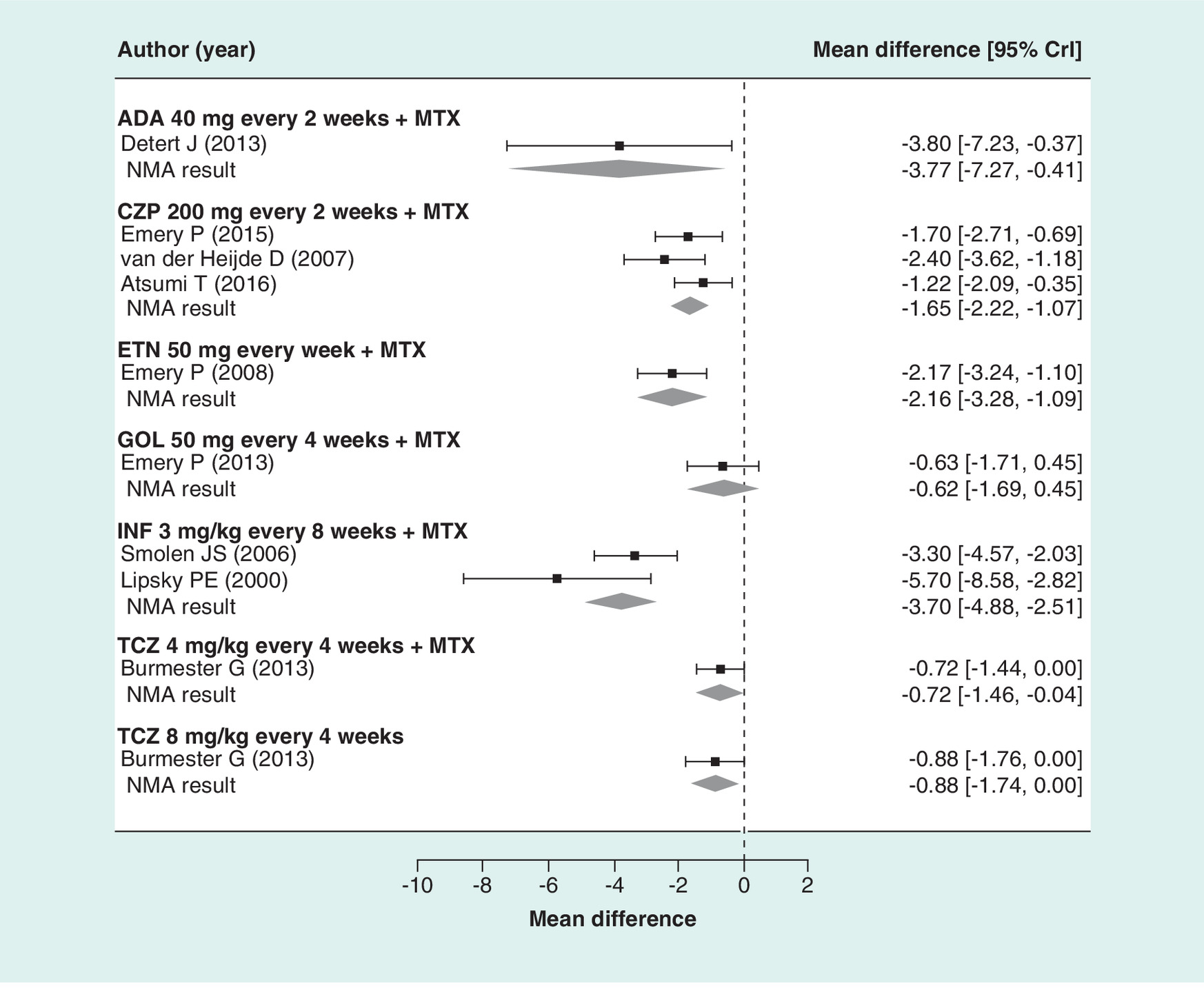
Figure 3. van der Heijde Total Sharp Score at 1 year: base case (nine studies).
ADA: Adalimumab; CrI: Credible interval; CZP: Certolizumab pegol; ETN: Etanercept; GOL: Golimumab; INF: Infliximab; MTX: Methotrexate; NMA: Network meta-analysis; TCZ: Tocilizumab.
Results of the subgroup analyses are provided in Table 2. Biologics in combination with MTX and tocilizumab without MTX decreased radiographic progression at 1 year compared with MTX alone among patients with early RA and as well as those with established RA. Of the 16 studies analyzed, seven studies had data for patients with early RA. Among patients with early RA, decreases in radiographic progression were seen for the biologics + MTX and for tocilizumab without MTX. Results of the subgroup analysis showed significant mean differences at 1 year for adalimumab + MTX (-3.83), infliximab + MTX (-3.30), etanercept + MTX (-2.18), certolizumab + MTX (-1.42) and tocilizumab 8 mg every 4 weeks without MTX (-0.87). Among patients with established RA, data were available for only two biologics (certolizumab and infliximab). For both interventions, the mean difference at 1 year was greater in patients with established RA compared with those with early RA (infliximab: -5.65 versus -3.30, respectively; certolizumab: -2.42 versus -1.42, respectively).
| Interventions | Early RA | Established RA | SMD |
|---|---|---|---|
| ABA 10 mg every 4 weeks + MTX | NA | NA | -0.27 (-0.46, -0.09) |
| ADA 40 mg every 2 weeks + MTX | -3.83 (-7.12, -0.31) | NA | -0.34, (-0.53, -0.18) |
| CZP 200 mg every 2 weeks + MTX | -1.42 (-2.08, -0.76) | -2.42 (-3.66, -1.21) | -0.33 (-0.49, -0.17) |
| ETN 50 mg every week + MTX | -2.18 (-3.27, -1.08) | NA | -0.35 (-0.61, -0.09) |
| GOL 50 mg every 4 weeks + MTX | -0.64 (-1.76, 0.44) | NA | -0.13 (-0.42, 0.17) |
| INF 3 mg every 8 weeks + MTX | -3.30 (-4.58, -2.02) | -5.65 (-8.48, -2.70) | -0.49 (-0.73, -0.29) |
| RTX 1000 mg + MTX | NA | NA | -0.34 (-0.57, -0.13) |
| TCZ 4 mg every 4 weeks + MTX | -0.72 (-1.42, 0.002) | NA | -0.25 (-0.42, -0.07) |
| TCZ 8 mg every 4 weeks | -0.87 (-1.75, -0.03) | NA | -0.23 (-0.47, 0.01) |
| Number of studies | 7 | 2 | 16 |
ABA: Abatacept; ADA: Adalimumab; CZP: Certolizumab pegol; ETN: Etanercept; GOL: Golimumab; INF: Infliximab; MTX: Methotrexate; NA: Not applicable; RA: Rheumatoid arthritis; RTX: Rituximab; SMD: Standardized mean difference; TCZ: Tocilizumab; vdHS: van der Heijde Total Sharp Score.
The SMD analysis (see Table 2) included data from 16 studies (9 base case studies reporting vdHS and 7 studies reporting different modifications of Sharp scores). Results of the SMD analysis were consistent with those of the base case analysis, which showed that all biologics in combination with MTX and tocilizumab without MTX decrease radiographic progression compared with MTX alone. Most interventions showed a statistically significant effect compared with MTX alone, except for golimumab 50 mg every 4 weeks and tocilizumab 8 mg every 4 weeks without MTX.
Results of pairwise comparisons for each intervention in the base case, SMD and subgroup analyses support the results obtained with the NMA model and SMD analyses (Supplementary Table 3). The pairwise comparisons generally showed that radiographic progression in patients with moderately to severely active RA was significantly decreased at 1 year in those treated with biologics in combination with MTX compared with those treated with MTX alone. Pairwise comparisons across the biologic agents did not reveal significant differences in radiographic progression changes which conclusively favored one biologic agent versus the other biologic comparators.
Risk of bias assessments were conducted on the 16 trials included in the analysis [32,36–50]. In the case of the five conference abstracts [36,42,43,49,50] respective full-text publications were used for the assessments [51–55]. A summary of the risk of bias assessment is presented in Table 3. In the 16 trials, the risk of selection bias was mainly low or unclear for random sequence generation and allocation concealment. The risk of performance bias, pertaining to blinding of participants and personnel, was mainly unclear as study authors simply described the study as ‘double-blind’ with no further details on how blinding was done and maintained throughout the trial. The risk of detection bias (pertaining to blinding of outcome assessors) and attrition bias (pertaining to incomplete outcome data) was mainly low. In the ATTRACT trial, the risk of attrition bias was assessed as high [47]. In this trial, no methods were employed to impute missing data; participants with missing data were excluded from analysis. Additionally, discontinuations were greater in the methotrexate alone group (50%) compared with all the groups that received infliximab plus methotrexate (21%), with lack of efficacy as the reason for discontinuation also being greater in the group that received methotrexate alone (36 vs 12%) [47]. All trials had low risk of reporting bias (pertaining to selective reporting of outcomes) and other sources of bias.
| Trial | Selection bias | Performance bias | Detection bias | Attrition bias | Reporting bias | Other sources of bias | |
|---|---|---|---|---|---|---|---|
| Random sequence generation | Allocation concealment | Blinding of participants and personnel | Blinding of outcome assessment | Incomplete outcome data | Selective reporting bias | ||
| AGREE [37] | Unclear risk | Unclear risk | Low risk | Low risk | Low risk | Low risk | Low risk |
| AIM [36,51] | Low risk | Low risk | Unclear risk | Low risk | Low risk | Low risk | Low risk |
| ASPIRE [46] | Low risk | Low risk | Unclear risk | Unclear risk | Low risk | Low risk | Low risk |
| ATTRACT [47] | Unclear risk | Unclear risk | Unclear risk | Unclear risk | High risk | Low risk | Low risk |
| C-EARLY [42,52] | Low risk | Low risk | Low risk | Unclear risk | Low risk | Low risk | Low risk |
| COMET [44] | Low risk | Low risk | Low risk | Low risk | Low risk | Low risk | Low risk |
| C-OPERA [41] | Low risk | Low risk | Unclear risk | Low risk | Low risk | Low risk | Low risk |
| DE019 [40] | Unclear risk | Unclear risk | Unclear risk | Low risk | Low risk | Low risk | Low risk |
| FUNCTION [50,53] | Unclear risk | Unclear risk | Unclear risk | Unclear risk | Low risk | Low risk | Low risk |
| GO-BEFORE [45] | Low risk | Low risk | Low risk | Unclear risk | Low risk | Low risk | Low risk |
| HIT HARD [38] | Unclear risk | Unclear risk | Unclear risk | Low risk | Low risk | Low risk | Low risk |
| IMAGE [32] | Unclear risk | Unclear risk | Low risk | Low risk | Low risk | Low risk | Low risk |
| LITHE [49,55] | Unclear risk | Unclear risk | Unclear risk | Low risk | Low risk | Low risk | Low risk |
| PREMIER [39] | Unclear risk | Unclear risk | Unclear risk | Low risk | Low risk | Low risk | Low risk |
| RAPID 1 [43,54] | Unclear risk | Unclear risk | Unclear risk | Low risk | Low risk | Low risk | Low risk |
| SCORE [48] | Low risk | Low risk | Unclear risk | Low risk | Low risk | Low risk | Low risk |
As shown in Table 4, radiographic data (spanning 2–10 years of follow-up) were found in 17 unique trials [8–32]. Direct comparisons of these trials are difficult because the study designs are different. For example in some studies, patients could cross over to treatment with the biologic agent (early escape) if defined study criteria were met during the double-blind treatment phase of the study [21–25], and in other studies patients crossed over to the treatment with the biologic when they entered the open-label extension phase of the study after completing the double-blind phase [8–12,14–16]. Despite the differences in study design, results of these studies demonstrate sustained slowing of radiographic progression for the biologics (abatacept, adalimumab, certolizumab, etanercept, golimumab and infliximab) in combination with MTX and for tocilizumab ± MTX.
| Intervention | Study acronym | Follow-up | Radiographic progression results | Conclusions |
|---|---|---|---|---|
| ABA + MTX | AGREE [8] | 2, 3, 5 years | AGREE – ABA 10 mg every 4 weeks + MTX Mean change in Genant score from BL to year 2: ABA + MTX, 0.84; MTX: 1.75; no radiographic progression from BL to year 2 in 56.8 and 43.8% of patients, respectively | Early treatment with ABA + MTX resulted in sustained clinical, functional and radiographic benefits compared with MTX alone |
| AIM [9–11] | – | AIM – ABA 10 mg every 4 weeks + MTX Mean change in Genant score from BL to year 2: ABA + MTX, 1.55; MTX, 3.17; Mean change from year 2 to year 3: ABA + MTX, 0.37;Mean change from year 3 to year 4: ABA + MTX, 0.34;Mean change from year 4 to year 5: ABA + MTX, 0.26; no radiographic progression from year 1 to 5 in 71.9% of ABA + MTX-treated patients | – | |
| ADA + MTX | PREMIER [12–14] | 2, 3, 5, 10 years | PREMIER – ADA 40 mg every 2 weeks + MTX Mean change in vdHS from BL to 2-year: ADA + MTX, 1.2; MTX, 6.6; BL to year 3: ADA + MTX, 1.6; MTX, 8.2; Mean change from BL to year 5: ADA + MTX, 2.9; MTX, 9.7; Mean change from BL to year 10: ADA + MTX, 4.0; MTX, 11.0; no radiographic progression in 66.7% of patients | Long-term ADA + MTX treatment resulted in clinical and functional disease control and dramatically slowed annual radiographic progression over 10 years |
| DE019 [13,15] | – | DE019 – ADA 40 mg every 2 weeks + MTX Mean change in vdHS from BL to year 3: ADA + MTX, 0.0; MTX, 3.7; Mean change from BL to year 5: ADA + MTX, 0.8; MTX, 3.9; Mean change from BL to year 10: ADA + MTX, 0.7; MTX, 6.2 | – | |
| CZP + MTX | RAPID 1 [16] | 2 years | RAPID 1 – CZP 200 mg every 2 weeks + MTX Mean change in vdHS from BL to year 2: CZP + MTX, 0.85; no radiographic progression in 72.4 and 51.5% of patients treated with CZP + MTX and MTX, respectively | CZP + MTX treatment provided 2-year inhibition of radiographic progression and sustained improvements in RA clinical signs and symptoms |
| ETN + MTX | JESMR [17] | 2, 3 years | JESMR – ETN 50 mg every week + MTX Mean change in vdHS from BL to year 2: ETN + MTX, 1.2; ETN, 6.6 | ETN + MTX treatment resulted in disease remission and sustained inhibition of radiographic progression over 3 years |
| COMET [18] | – | COMET – ETN 50 mg every week + MTX Mean change in vdHS from BL to year 2: ETN + MTX, 0.33; MTX, 4.65; no radiographic progression in 90 and 67% of patients, respectively | – | |
| TEMPO [19,20] | – | TEMPO – ETN 50 mg every week + MTX Mean change in vdHS from BL to year 2: ETN + MTX, -0.56; MTX, 3.34; Mean change from BL to year 3: ETN + MTX, -0.14; MTX, 5.95; no radiographic progression at year 3 in 76 and 51% of patients, respectively | – | |
| GOL + MTX | GO-FURTHER [21] | 2, 3, 5 years | GO-FURTHER – GOL 2 mg/kg every 8 weeks Mean change in vdHS from BL to year 2: GOL + MTX, 0.74; MTX: 2.10; no radiographic progression at year 2 in 61.8 and 54.8% of patients in the GOL + MTX and MTX groups, respectively | Clinical response including minimal radiographic progression was maintained during long-term treatment with GOL + MTX |
| GO-BEFORE [22] | – | GO-BEFORE – GOL 50 mg every 4 weeks Mean change in vdHS from BL to year 5: GOL + MTX, 0.72; MTX, 2.28; no radiographic progression in 62.5 and 54.2% of patients, respectively | – | |
| GO-FORWARD [23,24] | – | GO-FORWARD – GOL 50 mg every 4 weeks Mean change in vdHS from BL to year 2: GOL + MTX, 0.51; MTX, 1.15; no radiographic progression in 67.5 and 20.9% of patients in GOL + MTX and MTX groups, respectively. Mean change from BL to year 5: MTX + GOL, 2.44; MTX, 3.17; no radiographic progression in 59.5 and 54.7% of patients in the GOL + MTX and MTX groups, respectively | – | |
| GO-FORTH [25] | – | GO-FORTH – GOL 50 mg every 4 weeks Mean change in vdHS from BL to year 2: GOL 50 mg + MTX, 2.3; MTX, 1.5; no radiographic progression in 83.6 and 89.9% of patients, respectively. Mean change from BL to year 3: GOL 50 mg + MTX, 4.1; MTX, -0.2; no radiographic progression in 79.4 and 89.9% of patients, respectively | – | |
| INF + MTX | ATTRACT [26] | 2 years | ATTRACT – INF 3 mg every 8 weeks + MTX Change in median vdHS from BL to year 2 was 4-times greater in the MTX group vs INF + MTX group | INF + MTX inhibited the progression of structural damage in patients with early RA during the 2-year treatment period |
| TCZ + MTX | ACT-RAY [27] | 2, 3, 5 years | ACT-RAY – 8 mg/kg TCZ + MTX; 8 mg/kg TCZ Mean change in Genant score from BL to year 2: 8 mg/kg TCZ + MTX, 0.35; 8 mg/kg TCZ, 0.95; no radiographic progression in 94.4 and 91.1% of patients, respectively | Greater inhibition of radiographic progression in patients treated long-term with TCZ + MTX compared with MTX; clinical benefit (response, remission and physical function) was maintained |
| FUNCTION [28] | – | FUNCTION – 4 mg/kg TCZ + MTX; 8 mg/kg TCZ + MTX; 8 mg/kg TCZ Mean change in vdHS from BL to year 2: 4 mg/kg TCZ + MTX, 1.43; 8 mg/kg TCZ + MTX, 0.19; 8 mg/kg TCZ, 0.62; MTX, 1.88; no radiographic progression in 73, 83, 80 and 68% of patients, respectively | – | |
| LITHE [29–31] | – | LITHE – 4 mg/kg TCZ + MTX; 8 mg/kg TCZ + MTX Mean change in Genant score from BL to 2 years: 4 mg/kg TCZ + MTX, 0.58; 8 mg/kg TCZ + MTX, 0.37; MTX, 1.96; no radiographic progression from year 1 to year 2 in 80.6, 93.4 and 86.8% of patients, respectively. Mean change from BL to 3 years: 4 mg/kg TCZ + MTX, 0.71; 8 mg/kg TCZ + MTX, 0.72; MTX, 1.78; no radiographic progression from BL to year 3 in 67, 69 and 51% of patients, respectively. Mean change from BL to year 5: 4 mg/kg or 8 mg/kg TCZ + MTX, 1.34, MTX, 3.02; no radiographic progression from BL to year 5 in 52.7 and 34.9% of patients, respectively | – | |
| RTX + MTX | IMAGE [32] | 2 years | IMAGE – 1000 mg RTX + MTX Mean change in Genant score from BL to year 2: RTX + MTX, 0.41; MTX, 1.95; no radiographic progression in 57 and 37% of patients, respectively | Treatment with RTX + MTX over 2 years was associated with sustained improvements in radiographic, clinical and functional outcomes |
Italic text represents outcome name and timepoint.
ABA: Abatacept; ADA: Adalimumab; BL: Baseline; CZP: Certolizumab pegol; ETN: Etanercept; GOL: Golimumab; INF: Infliximab; MTX: Methotrexate; RTX: Rituximab; TCZ: Tocilizumab; vdHS: Modified van der Heijde Total Sharp Score.
Two trials (PREMIER and DE019) assessed the effect of a biologic agent on radiographic progression in RA over a 10-year period of time [12,56]. The PREMIER study examined the effects of adalimumab with and without methotrexate in patients with early RA [12]. In PREMIER, patients were randomly assigned to receive adalimumab + MTX, adalimumab alone or MTX alone for 2 years. Following the 2-year double-blinded period, patients were given adalimumab for up to 8 additional years, beginning as monotherapy; MTX could be added at the investigator's discretion. Results of PREMIER demonstrated that radiographic progression was prevented to a greater extent in patients initially randomized to adalimumab + MTX than in those initially receiving adalimumab alone or MTX alone (vdHS: 4.0, 8.8 and 11.0 at year 10, respectively) [12]. DE019 examined the long-term effectiveness of adalimumab in patients with established RA. In DE019, patients received adalimumab 20 mg weekly + MTX, adalimumab 40 mg every 2 weeks + MTX, or MTX alone during the 1-year double-blind treatment phase. The patients who completed DE019 could receive open-label adalimumab 40 mg every 2 weeks + MTX for an additional 9 years. Inhibition of radiographic progression was sustained in patients who received ADA + MTX [56]. It was noted that patients who initially received adalimumab + MTX had significantly lower mean change in vdHS at year 10 than those who received MTX alone (0.7 vs 6.2, respectively; p = 0.001) [56] suggesting that it is possible to prevent irreversible damage in patients with established RA. Results of a longitudinal, integrated analysis of the data from PREMIER and DE019 showed that treatment of RA with ADA ± MTX dramatically slowed annual radiographic progression over 10 years [13].
Discussion
Our systematic literature search identified 16 studies that matched the predefined criteria for PICO to evaluate the effects of biologics + MTX compared with MTX alone on 1-year radiographic progression using total Sharp scores in patients with RA; all 16 were included in evidence synthesis [32,36–50] and nine were included in the base case NMA model [38,41–47,50]. Findings of the current study support the value of biologics in the inhibition of radiographic progression among patients with RA. Some biologics like adalimumab have up to 10 years of radiographic inhibition evidence in patients with early and established RA reported in the literature [13,56]; future studies are required to confirm these long-term findings for other biologics.
Similarity was assessed by examining clinical and study-level sources of variation including differences across studies in early versus established RA and type of Sharp score used. Results in patients with early RA were slightly better for some biologics suggesting that patients who initiated treatment early may experience less radiographic progression. However, results of this subgroup analysis should be interpreted with caution because of the limited number of studies available. Although, all the studies we selected for analysis measured radiographic progression in patients with RA, there are several versions of the Sharp radiographic scoring method (modified van der Heijde, modified Genant and others), which have different scales [57,58]. As a result, the base-case model included only those studies that reported the modified vdHS as this was the most commonly used outcome measure across the various biologics. In order to include all available trials in a single analysis, we performed a sensitivity analysis by standardizing the means of radiographic progression scores across the multiple radiographic progression scoring systems (i.e., SMD analysis). The findings of the SMD analysis revealed similar trends as the base case analysis, in other words, all biologics in combination with MTX decreased radiographic progression compared with MTX alone.
We qualitatively reviewed data on long-term radiographic progression because randomized clinical trials assessing radiographic progression beyond the 1-year time frame for all of the biologics are lacking. Although our qualitative assessment shows that within each of the reviewed randomized clinical trials all the examined biologics inhibited radiographic progression beyond the 1-year time point, there may be differences in the rates of radiographic progression between these agents. It is possible that these variable inhibition rates may result in differences in the magnitude of the efficacy of the various biologics beyond 1 year. Future randomized clinical trials should consider long-term, open-label extension studies to confirm that the shorter-term findings of the efficacy of biologics in inhibiting radiographic progression are maintained over a longer treatment period.
The clinical relevance of inhibiting radiographic progression among patients with moderately to severely active RA is clear. A published systematic review of studies examining the association between joint damage and functional disability among patients with RA showed that an increase in joint damage is associated with an increase in disability over time [59]. Thus, preserving the structural integrity of the joints is important, not only to prevent loss of physical function, but also to reduce pain and fatigue, all of which can improve attendance at work, productivity at work and performance of various tasks at home, as well as participation in social and leisure activities [60]. Results of our base case analysis showed that adalimumab + MTX and infliximab + MTX decreased radiographic progression at 1 year to a greater extent than the other biologics (certolizumab pegol, etanercept, golimumab or tocilizumab) + MTX compared with MTX alone. Similar results were seen in the subgroup population with early RA.
As imaging technology, such as MRI, has become more recognized as an important tool in the assessment of patients with RA, its use in the early detection and prognosis of RA is being evaluated [61]. Studies have shown that progressive erosive disease can occur in 19–40% of patients who are in clinical remission [62–64]. These findings have raised the issue of whether remission criteria should be extended to include imaging criteria in treat-to-target guidelines. Future studies are needed to examine the relationship between imaging results and synovial pathobiology in patients with RA before and after therapeutic interventions [61] to determine criteria for imaging remission despite clinical remission. The patients with RA who attain remission show better function, health-related quality of life and productivity even when compared with a low-disease activity state [65]. From a cost perspective, those with higher states of disease activity incur higher direct and indirect costs, making remission a worthwhile goal to reduce the burden to both patients and society [65].
Other recent network meta-analyses have assessed the radiographic progression benefits associated with biologics in RA patients who were naive to MTX and in those who had an inadequate response to MTX or other DMARDs [66–68]. Hazelwood et al. [68] found that MTX in combination with adalimumab, etanercept, certolizumab or infliximab was statistically superior to MTX alone in preventing joint damage at 1 year in MTX-naive patients, though not in patients with a previous inadequate response to MTX. Conversely, Singh et al. [66] found no benefit of using biologics + MTX versus MTX alone to prevent radiographic progression in MTX-naive patients, but did find a statistically significant benefit in favor of biologics among patients who had an inadequate response to MTX or other DMARDs [67]. In our study, patients were predominantly MTX/DMARD-naive and biologic-naive. All studies had to have radiographic progression assessed at a minimum of 1 year (using total Sharp scores) and patients had to receive treatment for ≥4 weeks. Results of our analyses generally agree with those of Hazlewood et al. [68]. In our base case analysis (Figure 3), we found that radiographic progression at 1 year was statistically significantly inhibited in those on adalimumab, certolizumab, etanercept, infliximab and tocilizumab in combination with MTX compared with those on MTX alone. In our SMD analysis (Table 2), radiographic progression at 1 year was significantly inhibited with all biologics, except golimumab, in combination with MTX compared with MTX alone.
Head-to-head trials assessing the comparative effect of biologics on radiographic progression are limited. The current study, using Bayesian NMA, provides a means of making comparisons among biologics to fill this gap in the literature and is among the first to review the radiographic efficacy of biologics. NMA relies on the following assumptions: there is similarity across studies in the patients included and common comparators, the treatment effects are transitive, and that there is consistency of evidence [69–72]. We were limited to the aggregate (study-level) reported data in our assessment of differences across studies. The availability of patient-level data for the entire evidence base would allow for a more complete exploration of homogeneity and similarity. We are also limited in our ability to perform subgroup analysis of biologic-naive versus biologic-experienced patients. Although many of the studies had low levels of patients with previous biologic use, outcomes are not reported for this subgroup of patients. Results of some studies may not have been published yet. We attempted to address this limitation by including conference abstracts for the data that were analyzed, but this was not an exhaustive process. Finally, while the relative effect was the largest for adalimumab, the CI was wide suggesting that additional studies are needed to decrease the uncertainty and confirm the findings of this analysis.
Conclusion
Results of this meta-analysis demonstrate that in patients with RA, biologics and MTX provide additional inhibition of radiographic progression as compared with MTX alone. Some biologics like adalimumab have published evidence of inhibition of radiographic progression in patients with early and established RA for up to 10-years of follow-up. Longer-term studies are needed to provide further evidence of the inhibition of radiographic progression beyond 1 year.
Future perspective
The current treat-to-target guidelines for RA recommend clinical remission be the therapeutic target as defined by ACR-EULAR remission criteria [73] because clinical trials and practice and most of the inflammatory rheumatology literature addressing radiographic changes, disability and quality of life among patients with RA is based on clinical observations and not on observations using imaging techniques [74]. However, it is recognized that inflammation may still be present in patients who are in clinical remission and there is discussion about expanding remission criteria by adding imaging criteria to the clinical composite indices in the ‘treat-to-target’ recommendations. In order to include radiographic progression as a target, decisions need to be made about the level of inflammation that can be tolerated, what imaging method should be used (radiography, CT scan, MRI and ultrasound), what joints should be assessed, and which cut-off point should be used [75]. We expect that the relationship between imaging technology and synovial pathobiology will be defined as future studies use this technology to examine synovial tissue along with joint damage at different disease stages before and after treatment with established and newly emerging biologic therapies.
In addition, a greater number of clinical trials in RA in the future are likely to have longer-term open-label follow-up periods due to the growing interest in understanding the efficacy of such therapies beyond the typical time-frame of a clinical trial. Radiographic data are also more likely to be gathered through real-world sources such as patient registries. We also expect to see more meta-analyses published in RA on the topic of radiographic progression as well as other patient-centric outcomes such as pain, fatigue, physical functioning, work productivity and disease remission.
Information on comparative efficacy of biologics in inhibiting radiographic progression in rheumatoid arthritis is limited.
We conducted Bayesian network meta-analysis (NMA) of published clinical trials to compare 1-year radiographic efficacy of biologics in patients with rheumatoid arthritis.
We qualitatively reviewed radiographic data beyond 1 year, in the absence of published clinical trials to build NMA models beyond 1 year.
In the base case NMA model at 1 year, all biologics in combination with MTX and tocilizumab without MTX showed decreased radiographic progression at 1 year compared with MTX alone.
Qualitatively, long-term radiographic data (spanning 2–10 years of follow-up) showed sustained slowing of radiographic progression for biologics; however, only a few biologics have radiographic progression data beyond 2 years with adalimumab having up to 10 years of published data available.
Long-term, open-label extension studies are needed to confirm that inhibition of radiographic progression is sustained beyond 1 year.
Financial & competing interests disclosure
The design, study conduct, and financial support for the study/trial were provided by AbbVie. AbbVie participated in the interpretation of data, review and approval of this publication. E Murray is an employee of Doctor Evidence and received funding from AbbVie to conduct this research. A Ellis and Y Butylkova were employees of Doctor Evidence at the time this study was conducted and received funding from AbbVie to conduct this research. Y Butylkova is a current employee of Amgen. M Skup, J Kalabic and V Garg are employees of AbbVie and may hold stocks or stock options in AbbVie.
Medical writing assistance was provided by Joann Hettasch, of Fishawack Facilitate Ltd, Conshohocken, PA, USA, and was funded by AbbVie.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary data
To view the supplementary data that accompany this paper please visit the journal website at: www.futuremedicine.com/doi/full/10.2217/cer-2017-0106
Supplementary Material
File (suppl_file.doc)
- Download
- 220.00 KB
References
Papers of special note have been highlighted as: • of interest
1.
Sokka T. Work disability in early rheumatoid arthritis. Clin. Exp. Rheumatol. 21(5) (Suppl. 31), S71–S74 (2003).
2.
Smolen JS, Aletaha D, Bijlsma JW et al. Treating rheumatoid arthritis to target: recommendations of an international task force. Ann. Rheum. Dis. 69(4), 631–637 (2010).
3.
Aaltonen KJ, Virkki LM, Malmivaara A, Konttinen YT, Nordstrom DC, Blom M. Systematic review and meta-analysis of the efficacy and safety of existing TNF blocking agents in treatment of rheumatoid arthritis. PLoS ONE 7(1), e30275 (2012).
4.
Chen YF, Jobanputra P, Barton P et al. A systematic review of the effectiveness of adalimumab, etanercept and infliximab for the treatment of rheumatoid arthritis in adults and an economic evaluation of their cost-effectiveness. Health Technol. Assess. 10(42), iii–iv, xi–xiii, 1–229 (2006).
5.
Alfonso-Cristancho R, Armstrong N, Arjunji R et al. Comparative effectiveness of biologics for the management of rheumatoid arthritis: systematic review and network meta-analysis. Clin. Rheumatol. 36(1), 25–34 (2017).
6.
Higgins JP, Altman DG, Gotzsche PC et al. The Cochrane Collaboration's tool for assessing risk of bias in randomised trials. BMJ 343, d5928 (2011).
7.
van der Heijde D. How to read radiographs according to the Sharp/van der Heijde method. J. Rheumatol. 27(1), 261–263 (2000).
8.
Bathon J, Robles M, Ximenes AC et al. Sustained disease remission and inhibition of radiographic progression in methotrexate-naive patients with rheumatoid arthritis and poor prognostic factors treated with abatacept: 2-year outcomes. Ann. Rheum. Dis. 70(11), 1949–1956 (2011).
9.
Genant HK, Peterfy CG, Westhovens R et al. Abatacept inhibits progression of structural damage in rheumatoid arthritis: results from the long-term extension of the AIM trial. Ann. Rheum. Dis. 67(8), 1084–1089 (2008).
10.
Westhovens R, Dougados M, Hall S et al. Disease remission, radiographic non-progression and normalization of function achieved at year 1 are sustained long-term in a majority of patients: 5-year outcomes with abatacept in biologic-naive patients. Arthritis Rheum. 60(Suppl. 10), 1657 (2009).
11.
Kremer JM, Peterfy C, Russell AS et al. Longterm safety, efficacy, and inhibition of structural damage progression over 5 years of treatment with abatacept in patients with rheumatoid arthritis in the abatacept in inadequate responders to methotrexate trial. J. Rheumatol. 41(6), 1077–1087 (2014).
12.
Keystone EC, Breedveld FC, van der Heijde D et al. Longterm effect of delaying combination therapy with tumor necrosis factor inhibitor in patients with aggressive early rheumatoid arthritis: 10-year efficacy and safety of adalimumab from the randomized controlled PREMIER trial with open-label extension. J. Rheumatol. 41(1), 5–14 (2014).
13.
Landewe R, Ostergaard M, Keystone EC, Florentinus S, Liu S, van der Heijde D. Analysis of integrated radiographic data from two long-term, open-label extension studies of adalimumab for the treatment of rheumatoid arthritis. Arthritis Care Res. (Hoboken) 67(2), 180–186 (2015).
14.
van der Heijde D, Breedveld FC, Kavanaugh A et al. Disease activity, physical function, and radiographic progression after longterm therapy with adalimumab plus methotrexate: 5-year results of PREMIER. J. Rheumatol. 37(11), 2237–2246 (2010).
15.
Keystone EC, Kavanaugh A, Weinblatt ME, Patra K, Pangan AL. Clinical consequences of delayed addition of adalimumab to methotrexate therapy over 5 years in patients with rheumatoid arthritis. J. Rheumatol. 38(5), 855–862 (2011).
16.
Keystone EC, Combe B, Smolen J et al. Sustained efficacy of certolizumab pegol added to methotrexate in the treatment of rheumatoid arthritis: 2-year results from the RAPID 1 trial. Rheumatology (Oxford) 51(9), 1628–1638 (2012).
17.
Kameda H, Kanbe K, Sato E et al. Etanercept (ETN) plus methotrexate (MTX) combination therapy resulted in better clinical and radiographic outcomes than ETN monotherapy even in patients with active rheumatoid arthritis despite MTX treatment: 104-week results from the JESMR study. Ann. Rheum. Dis. 69(Suppl 3), 204 (2010).
18.
Emery P, Breedveld F, van der Heijde D et al. Two-year clinical and radiographic results with combination etanercept-methotrexate therapy versus monotherapy in early rheumatoid arthritis: a two-year, double-blind, randomized study. Arthritis Rheum. 62(3), 674–682 (2010).
19.
van der Heijde D, Klareskog L, Landewe R et al. Disease remission and sustained halting of radiographic progression with combination etanercept and methotrexate in patients with rheumatoid arthritis. Arthritis Rheum. 56(12), 3928–3939 (2007).
20.
van der Heijde D, Klareskog L, Rodriguez-Valverde V et al. Comparison of etanercept and methotrexate, alone and combined, in the treatment of rheumatoid arthritis: two-year clinical and radiographic results from the TEMPO study, a double-blind, randomized trial. Arthritis Rheum. 54(4), 1063–1074 (2006).
21.
Bingham CO 3rd, Mendelsohn AM, Kim L et al. Maintenance of clinical and radiographic benefit with intravenous golimumab therapy in patients with active rheumatoid arthritis despite methotrexate therapy: week-112 efficacy and safety results of the open-label long-term extension of a Phase III, double-blind, randomized, placebo-controlled trial. Arthritis Care Res. (Hoboken) 67(12), 1627–1636 (2015).
22.
Emery P, Fleischmann RM, Strusberg I et al. Efficacy and safety of subcutaneous golimumab in methotrexate-naive patients with rheumatoid arthritis: five-year results of a randomized clinical trial. Arthritis Care Res. (Hoboken) 68(6), 744–752 (2016).
23.
Keystone EC, Genovese MC, Hall S et al. Golimumab in patients with active rheumatoid arthritis despite methotrexate therapy: results through 2 years of the GO-FORWARD study extension. J. Rheumatol. 40(7), 1097–1103 (2013).
24.
Keystone EC, Genovese MC, Hall S et al. Safety and efficacy of subcutaneous golimumab in patients with active rheumatoid arthritis despite methotrexate therapy: final 5-year Results of the GO-FORWARD Trial. J. Rheumatol. 43(2), 298–306 (2016).
25.
Tanaka Y, Harigai M, Takeuchi T et al. Clinical efficacy, radiographic progression, and safety through 156 weeks of therapy with subcutaneous golimumab in combination with methotrexate in Japanese patients with active rheumatoid arthritis despite prior methotrexate therapy: final results of the randomized GO-FORTH trial. Mod. Rheumatol. 26(4), 481–490 (2016).
26.
Breedveld FC, Emery P, Keystone E et al. Infliximab in active early rheumatoid arthritis. Ann. Rheum. Dis. 63(2), 149–155 (2004).
27.
Huizinga TW, Conaghan PG, Martin-Mola E et al. Clinical and radiographic outcomes at 2 years and the effect of tocilizumab discontinuation following sustained remission in the second and third year of the ACT-RAY study. Ann. Rheum. Dis. 74(1), 35–43 (2015).
28.
Burmester GR, Rigby WF, van Vollenhoven RF et al. Tocilizumab combination therapy or monotherapy or methotrexate monotherapy in methotrexate-naive patients with early rheumatoid arthritis: 2-year clinical and radiographic results from the randomised, placebo-controlled FUNCTION trial. Ann. Rheum. Dis. 76 (7), 1279–1284 (2017).
29.
Fleischmann RM, Halland AM, Brzosko M et al. Tocilizumab inhibits structural joint damage and improves physical function in patients with rheumatoid arthritis and inadequate responses to methotrexate: LITHE study 2-year results. J. Rheumatol. 40(2), 113–126 (2013).
30.
Kremer JM, Blanco R, Halland AM et al. Clinical efficacy and safety maintained up to 5 years in patients with rheumatoid arthritis treated with tocilizumab in a randomised trial. Clin. Exp. Rheumatol. 34(4), 625–633 (2016).
31.
Kremer JM, Furst DE, Burgos-Vargas R et al. LITHE: tocilizumab inhibits radiographic progression and improves physical function in rheumatoid arthritis patients at 3 years with maintenance of clinical efficacy over time. Arthritis Rheum. 62(Suppl. 10), 1819 (2010).
32.
Tak PP, Rigby W, Rubbert-Roth A et al. Sustained inhibition of progressive joint damage with rituximab plus methotrexate in early active rheumatoid arthritis: 2-year results from the randomised controlled trial IMAGE. Ann. Rheum. Dis. 71(3), 351–357 (2012).
33.
van Valkenhoef G, Lu G, De Brock B, Hillege H, Ades AE, Welton NJ. Automating network meta-analysis. Res. Synth. Methods 3(4), 285–299 (2012).
34.
R Development Core Team. A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria, ISBN 3–000051-07-0 www.R-project.org.
35.
van Valkenhoef G, Kuiper J. gemtc: network meta-analysis using bayesian methods. R package version 0.6-1 (2014). http://CRAN.R-project.org/package=gemtc.
36.
Genant HK, Peterfy C, Westhovens R et al. Abatacept sustains inhibition of radiographic progression over 2 years in rheumatoid arthritis patients with an inadequate response to methotrexate: results from the long-term extension of the AIM trial. Ann. Rheum. Dis. 65(Suppl. II), 57 (2006).
37.
Westhovens R, Robles M, Ximenes AC et al. Clinical efficacy and safety of abatacept in methotrexate-naive patients with early rheumatoid arthritis and poor prognostic factors. Ann. Rheum. Dis. 68(12), 1870–1877 (2009).
38.
Detert J, Bastian H, Listing J et al. Induction therapy with adalimumab plus methotrexate for 24 weeks followed by methotrexate monotherapy up to week 48 versus methotrexate therapy alone for DMARD-naive patients with early rheumatoid arthritis: HIT HARD, an investigator-initiated study. Ann. Rheum. Dis. 72(6), 844–850 (2013).
• Combination therapy with adalimumab plus methotrexate leads to rapid disease improvement and reduces structural joint damage in patients with active early rheumatoid arthritis (RA).
39.
Breedveld FC, Weisman MH, Kavanaugh AF et al. The PREMIER study: a multicenter, randomized, double-blind clinical trial of combination therapy with adalimumab plus methotrexate versus methotrexate alone or adalimumab alone in patients with early, aggressive rheumatoid arthritis who had not had previous methotrexate treatment. Arthritis Rheum. 54(1), 26–37 (2006).
40.
Keystone EC, Kavanaugh AF, Sharp JT et al. Radiographic, clinical, and functional outcomes of treatment with adalimumab (a human anti-tumor necrosis factor monoclonal antibody) in patients with active rheumatoid arthritis receiving concomitant methotrexate therapy: a randomized, placebo-controlled, 52-week trial. Arthritis Rheum. 50(5), 1400–1411 (2004).
41.
Atsumi T, Yamamoto K, Takeuchi T et al. The first double-blind, randomised, parallel-group certolizumab pegol study in methotrexate-naive early rheumatoid arthritis patients with poor prognostic factors, C-OPERA, shows inhibition of radiographic progression. Ann. Rheum. Dis. 75(1), 75–83 (2016).
• Certolizumab plus methotrexate significantly inhibits structural damage and reduces RA symptoms in methotrexate-naive early RA patients with poor prognostic factors.
42.
Emery P, Bingham CO, Burmester GR et al. The first study of certolizumab pegol in combination with methotrexate in DMARD-naive early rheumatoid arthritis patients led to sustained clinical response and inhibition of radiographic progression at 52 weeks: The C-EARLY randomized, double-blind, controlled Phase III study. Ann. Rheum. Dis. 74(Suppl. 2), 712 (2015).
• Combination therapy of certolizumab plus methotrexate results in sustained clinical response and inhibition of radiographic progression in disease-modifying antirheumatic drug-naive early RA patients.
43.
van der Heijde D, Strand V, Keystone E, Landewe R. Inhibition of radiographic progression by lyophilized certolizumab pegol added to methotrexate in comparison with methotrexate alone in patients with rheumatoid arthritis: the RAPID 1 trial. ACR Annual Conference, MA, USA, Abstract 940 (2007).
• Combination therapy with certolizumab plus methotrexate leads to inhibition of radiographic progression in RA patients who are inadequate responders to disease-modifying antirheumatic drug therapy.
44.
Emery P, Breedveld FC, Hall S et al. Comparison of methotrexate monotherapy with a combination of methotrexate and etanercept in active, early, moderate to severe rheumatoid arthritis (COMET): a randomised, double-blind, parallel treatment trial. Lancet 372(9636), 375–382 (2008).
• Clinical remission and radiographic non-progression are achievable goals in patients with early severe RA treated with etanercept plus methotrexate.
45.
Emery P, Fleischmann RM, Doyle MK et al. Golimumab, a human anti-tumor necrosis factor monoclonal antibody, injected subcutaneously every 4 weeks in patients with active rheumatoid arthritis who had never taken methotrexate: 1-year and 2-year clinical, radiologic, and physical function findings of a phase III, multicenter, randomized, double-blind, placebo-controlled study. Arthritis Care Res. (Hoboken) 65(11), 1732–1742 (2013).
• Sustained improvements in clinical signs and symptoms, physical function and radiographic progression were observed in methotrexate-naive RA patients treated with golimumab plus methotrexate.
46.
Smolen JS, van der Heijde DM, St Clair EW et al. Predictors of joint damage in patients with early rheumatoid arthritis treated with high-dose methotrexate with or without concomitant infliximab: results from the ASPIRE trial. Arthritis Rheum. 54(3), 702–710 (2006).
• Combination therapy with infliximab plus methotrexate inhibited radiographic progression in methotrexate-naive RA patients with persistent disease activity.
47.
Lipsky PE, van der Heijde DM, St Clair EW et al. Infliximab and methotrexate in the treatment of rheumatoid arthritis. Anti-tumor necrosis factor trial in rheumatoid arthritis with concomitant therapy study group. N. Engl. J. Med. 343(22), 1594–1602 (2000).
• In patients with active RA who were inadequate responders to methotrexate therapy, combination therapy with infliximab plus methotrexate resulted in clinical benefit and halted progression of joint damage.
48.
Peterfy C, Emery P, Tak PP et al. MRI assessment of suppression of structural damage in patients with rheumatoid arthritis receiving rituximab: results from the randomised, placebo-controlled, double-blind RA-SCORE study. Ann. Rheum. Dis. 75(1), 170–177 (2016).
49.
Kremer J, Fleischmann R, Brzezicki P et al. Tocilizumab inhibits structural joint damage, improves physical function, and increases DAS28 remission rates in RA patients who respond inadequately to methotrexate: the LITHE study. Ann. Rheum. Dis. 68(Suppl. 3), 122 (2009).
50.
Burmester G, Rigby W, van Vollenhoven R et al. Tocilizumab in combination therapy and monotherapy versus methotrexated in methotrexate-naive patients with early rheumatoid arthritis: clinical and radiographic outcomes from a randomized, placebo-controlled trial. Arthritis Rheum. 65(Suppl. 10), 2767 (2013).
• Combination therapy with tocilizumab plus methotrexate resulted in improvements in clinical symptoms, physical function and inhibition of structural joint damage in methotrexate-naive patients with early active RA.
51.
Kremer JM, Genant HK, Moreland LW et al. Effects of abatacept in patients with methotrexate-resistant active rheumatoid arthritis: a randomized trial. Ann. Intern. Med. 144(12), 865–876 (2006).
52.
Emery P, Bingham CO 3rd, Burmester GR et al. Certolizumab pegol in combination with dose-optimised methotrexate in DMARD-naive patients with early, active rheumatoid arthritis with poor prognostic factors: 1-year results from C-EARLY, a randomised, double-blind, placebo-controlled Phase III study. Ann. Rheum. Dis. 76(1), 96–104 (2017).
53.
Burmester GR, Rigby WF, van Vollenhoven RF et al. Tocilizumab in early progressive rheumatoid arthritis: FUNCTION, a randomised controlled trial. Ann. Rheum. Dis. 75(6), 1081–1091 (2016).
54.
Keystone E, Heijde D, Mason D Jr et al. Certolizumab pegol plus methotrexate is significantly more effective than placebo plus methotrexate in active rheumatoid arthritis: findings of a fifty-two-week, phase III, multicenter, randomized, double-blind, placebo-controlled, parallel-group study. Arthritis Rheum. 58(11), 3319–3329 (2008).
55.
Kremer JM, Blanco R, Brzosko M et al. Tocilizumab inhibits structural joint damage in rheumatoid arthritis patients with inadequate responses to methotrexate: results from the double-blind treatment phase of a randomized placebo-controlled trial of tocilizumab safety and prevention of structural joint damage at one year. Arthritis Rheum. 63(3), 609–621 (2011).
56.
Keystone EC, van der Heijde D, Kavanaugh A et al. Clinical, functional, and radiographic benefits of longterm adalimumab plus methotrexate: final 10-year data in longstanding rheumatoid arthritis. J. Rheumatol. 40(9), 1487–1497 (2013).
57.
Ory PA. Interpreting radiographic data in rheumatoid arthritis. Ann. Rheum. Dis. 62(7), 597–604 (2003).
58.
Landewe R, van der Heijde D. Radiographic progression in rheumatoid arthritis. Clin. Exp. Rheumatol. 23(5) (Suppl. 39), S63–S68 (2005).
59.
Bombardier C, Barbieri M, Parthan A et al. The relationship between joint damage and functional disability in rheumatoid arthritis: a systematic review. Ann. Rheum. Dis. 71(6), 836–844 (2012).
60.
Strand V, Khanna D. The impact of rheumatoid arthritis and treatment on patients’ lives. Clin. Exp. Rheumatol. 28(3) (Suppl. 59), S32–S40 (2010).
61.
Humby F, Mahto A, Ahmed M et al. The relationship between synovial pathobiology and magnetic resonance imaging abnormalities in rheumatoid arthritis: a systematic review. J. Rheumatol. 44(9), 1311–1324 (2017).
62.
Sewerin P, Vordenbaeumen S, Hoyer A et al. Silent progression in patients with rheumatoid arthritis: is DAS28 remission an insufficient goal in RA? Results from the German Remission-plus cohort. BMC Musculoskelet. Disord. 18(1), 163 (2017).
63.
Lillegraven S, Prince FH, Shadick NA et al. Remission and radiographic outcome in rheumatoid arthritis: application of the 2011 ACR/EULAR remission criteria in an observational cohort. Ann. Rheum. Dis. 71(5), 681–686 (2012).
64.
Brown AK, Conaghan PG, Karim Z et al. An explanation for the apparent dissociation between clinical remission and continued structural deterioration in rheumatoid arthritis. Arthritis Rheum. 58(10), 2958–2967 (2008).
65.
Radner H, Smolen JS, Aletaha D. Remission in rheumatoid arthritis: benefit over low disease activity in patient-reported outcomes and costs. Arthritis Res. Ther. 16(1), R56 (2014).
66.
Singh JA, Hossain A, Mudano AS et al. Biologics or tofacitinib for people with rheumatoid arthritis naive to methotrexate: a systematic review and network meta-analysis. Cochrane Database Syst. Rev. 5, Cd012657 (2017).
67.
Singh JA, Hossain A, Tanjong Ghogomu E et al. Biologics or tofacitinib for rheumatoid arthritis in incomplete responders to methotrexate or other traditional disease-modifying anti-rheumatic drugs: a systematic review and network meta-analysis. Cochrane Database Syst. Rev. Cd012183 (2016).
68.
Hazlewood GS, Barnabe C, Tomlinson G, Marshall D, Devoe DJ, Bombardier C. Methotrexate monotherapy and methotrexate combination therapy with traditional and biologic disease modifying anti-rheumatic drugs for rheumatoid arthritis: a network meta-analysis. Cochrane Database Syst. Rev. Cd010227 (2016).
69.
Donegan S, Williamson P, D'alessandro U, Tudur Smith C. Assessing key assumptions of network meta-analysis: a review of methods. Res. Synth. Methods 4(4), 291–323 (2013).
70.
Higgins JP, Jackson D, Barrett JK, Lu G, Ades AE, White IR. Consistency and inconsistency in network meta-analysis: concepts and models for multi-arm studies. Res. Synth. Methods 3(2), 98–110 (2012).
71.
Salanti G. Indirect and mixed-treatment comparison, network, or multiple-treatments meta-analysis: many names, many benefits, many concerns for the next generation evidence synthesis tool. Res. Synth. Methods 3(2), 80–97 (2012).
72.
Salanti G, Higgins JP, Ades AE, Ioannidis JP. Evaluation of networks of randomized trials. Stat. Methods Med. Res. 17(3), 279–301 (2008).
73.
Felson DT, Smolen JS, Wells G et al. American College of Rheumatology/European League against Rheumatism provisional definition of remission in rheumatoid arthritis for clinical trials. Ann. Rheum. Dis. 70(3), 404–413 (2011).
74.
Smolen JS, Breedveld FC, Burmester GR et al. Treating rheumatoid arthritis to target: 2014 update of the recommendations of an international task force. Ann. Rheum. Dis. 75(1), 3–15 (2016).
75.
van der Heijde D. Remission by imaging in rheumatoid arthritis: should this be the ultimate goal? Ann. Rheum. Dis. 71(Suppl. 2), i89–92 (2012).
Information & Authors
Information
Published In
Copyright
© 2018 Abbvie.
History
Received: 22 December 2017
Accepted: 3 July 2018
Published online: 21 August 2018
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Systematic review and network meta-analysis: effect of biologics on radiographic progression in rheumatoid arthritis. (2018) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2017-0106
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Rory Sheppard, Myrsini Gianatsi, Ian Thomas, Sophie King, David Gillespie, Philip Pallmann, Sara Marsal Barril, Ernest Choy, Decision on Optimal Combinatorial Therapies in Immune-mediated inflammatory diseases using Systems approaches (DocTIS): protocol for a single-arm, adaptive basket trial in rheumatoid and psoriatic arthritis, Rheumatology Advances in Practice, 10.1093/rap/rkag036, 10, 2, (2026).
- Fowzia Ibrahim, David L. Scott, Ian C. Scott, The impact of intensive management on pain intensity in patients with rheumatoid arthritis and psoriatic arthritis: secondary analysis of three clinical trials, BMC Rheumatology, 10.1186/s41927-025-00493-z, 9, 1, (2025).
- Jacopo Ciaffi, Lorenzo Bianchi, Alberto Di Martino, Cesare Faldini, Francesco Ursini, Is Total Joint Arthroplasty an Effective and Safe Option for Psoriatic Arthritis Patients? A Scoping Review, Journal of Clinical Medicine, 10.3390/jcm13185552, 13, 18, (5552), (2024).
- Nicola Humphry, The Efficacy of Anti-TNFs in Immune-Mediated Disease, EMJ Gastroenterology, 10.33590/emjgastroenterol/10102824, (2-9), (2022).
- Maarten Boers, Linda Hartman, Daniela Opris-Belinski, Reinhard Bos, Marc R Kok, Jose AP Da Silva, Eduard N Griep, Ruth Klaasen, Cornelia F Allaart, Paul Baudoin, Hennie G Raterman, Zoltan Szekanecz, Frank Buttgereit, Pavol Masaryk, L Thomas Klausch, Sabrina Paolino, Annemarie M Schilder, Willem F Lems, Maurizio Cutolo, LM Middelink, V Dekker, N van den Bulk, RMA Pinto, L Doerwald, S Manger, J Redol, K Prinsen, M Scholte-Voshaar, TLTA Jansen, C Codreanu, E Molenaar, JM van Laar, YPM Ruiterman, AERCH Boonen, AERCH Boonen, M Micaelo, J Costa, M Sieburg, JPL Spoorenberg, U Prothmann, MJ Saavedra, I Silva, MT Nurmohamed, JWG Jacobs, SW Tas, JWJ Bijlsma, R Christensen, YM Smulders, SH Ralston, DMFM van der Heijde, AF Marsman, WF Lems, C Rusthoven, M Bakkers, E Frazão Mateus, G Mendes, C Elling-Audersch, D Borucki, A Celano, P Corduta, O Constantinescu, P Richards, GJ Aanerud, Low dose, add-on prednisolone in patients with rheumatoid arthritis aged 65+: the pragmatic randomised, double-blind placebo-controlled GLORIA trial, Annals of the Rheumatic Diseases, 10.1136/annrheumdis-2021-221957, 81, 7, (925-936), (2022).
- Youngjae Park, Mei-Ling Li, Ji-Won Kim, Jung Hee Koh, Yune-Jung Park, Wan-Uk Kim, Time-integrated Cumulative Parameters Predictive of Radiographic Progression of Rheumatoid Arthritis: Real-world Data From a Prospective Single-center Cohort, Journal of Rheumatic Diseases, 10.4078/jrd.2022.29.2.98, 29, 2, (98-107), (2022).
- Kazuhiro Maeda, Ken Yoshida, Tetsuro Nishizawa, Kazuhiro Otani, Yu Yamashita, Hinako Okabe, Yuka Hadano, Tomohiro Kayama, Daitaro Kurosaka, Mitsuru Saito, Inflammation and Bone Metabolism in Rheumatoid Arthritis: Molecular Mechanisms of Joint Destruction and Pharmacological Treatments, International Journal of Molecular Sciences, 10.3390/ijms23052871, 23, 5, (2871), (2022).
- V.D. Sokolova, V.V. Mladov, N.A. Sableva, D.G. Tolkacheva, Efficacy of biologics and targeted synthetic disease-modifying antirheumatic drugs approved in the Russian Federation to treat adults with active rheumatoid arthritis: a systematic review and network meta-analysis, Medical Technologies. Assessment and Choice, 10.17116/medtech20224401150, 1, (50), (2022).
- Fabrizio Cantini, Delia Goletti, Maurizio Benucci, Rosario Foti, Arianna Damiani, Laura Niccoli, Tailored first-line biologic and targeted synthetic disease modifying anti-rheumatic drugs therapy in patients with rheumatoid arthritis: 2021 updated ITABIO statements, Expert Opinion on Drug Safety, 10.1080/14740338.2022.2020247, 21, 5, (613-623), (2021).
- Charles G Peterfy, Vibeke Strand, Alan Friedman, Stephen Hall, Eduardo Mysler, Patrick Durez, Xenofon Baraliakos, Jeffrey V Enejosa, Tim Shaw, Yihan Li, Su Chen, In-Ho Song, Inhibition of structural joint damage progression with upadacitinib in rheumatoid arthritis: 1-year outcomes from the SELECT phase 3 program, Rheumatology, 10.1093/rheumatology/keab861, 61, 8, (3246-3256), (2021).