Comparing outcomes between barbed and conventional sutures in patients undergoing knee or hip arthroplasty
Abstract
Aim: To compare outcomes between barbed sutures and conventional sutures among patients undergoing knee or hip arthroplasty. Materials & methods: Retrospective study of patients (aged ≥18 years) undergoing elective knee/hip arthroplasty for osteoarthritis between 1 January 2013 and 1 September 2015. Patients were classified as: any Stratafix™ Knotless Tissue Control Devices (barbed suture group) used for closure vs. conventional sutures only (conventional suture group). Results: Compared with the conventional suture group, the barbed suture group had statistically significant: shorter length of stay, knee = 0.2 d; hip = 0.3 d and operating room time, knee = 7 min; hip = 22 min and lower rate of discharge to skilled nursing facility/nonhome setting (knee = 3.0%; hip = 6.8%). Conclusion: Use of barbed sutures was associated with shorter length of stay, operating room time and less resource intensive discharge status as compared with conventional sutures alone.
Joint arthroplasty procedures, including knee arthroplasty and hip arthroplasty, are the two most common nonmaternal/nonneonatal operations performed during inpatients stays in the USA: in 2014, there were an estimated 660,876 inpatient stays with a principal procedure of knee arthroplasty and 441,490 inpatient stays with a principal procedure of hip arthroplasty, which were associated with combined hospital costs exceeding US$17 billion [1,2]. During the decade spanning 2005 through 2014, the combined rate of knee and hip arthroplasty increased by approximately 25%, a trend which is likely to continue with the aging of the US population [2].
Given the costs and commonness of joint arthroplasty procedures, their quality of care and outcomes are important areas of attention for US payers; particularly for the Centers for Medicare and Medicaid Services (CMS), which in 2014 was the primary payer for more than 50% of knee and hip arthroplasties in the USA [2]. Accordingly, CMS has implemented multiple efforts to incentivize hospitals to improve outcomes among patients undergoing joint arthroplasty and/or share financial risk associated with undesirable outcomes such as hospital readmission. These include the comprehensive care for joint replacement model, the hospital quality initiative, and the readmissions reduction program [3–5]. Hospitals and provider alike are therefore presently facing increasing pressure to optimize outcomes of joint arthroplasty procedures.
Successful wound closure of joint arthroplasty procedures, for which suturing can play a critical role, influences healing, surgical site infection (SSI) risk, self-care and postacute care follow-up [6–12]. Whether the use of knotless/barbed sutures in the wound closure of joint arthroplasty results in different outcomes as compared with conventional sutures alone has been the focus of several small randomized controlled trials, small retrospective analyses and systematic meta-analyses [6–12]. These studies have consistently found that barbed sutures are associated with shorter wound closure time, but have reported conflicting results with respect to wound complication, with some finding significantly lower rates of wound complications associated with barbed sutures [6,7], some finding no difference [7,8,11] and some finding significantly higher rates of wound complications associated with barbed sutures [9,10]. Furthermore, these studies have generally not examined certain important healthcare utilization outcomes such as hospital length of stay (LOS) or readmissions. Among the barbed sutures that are available today, the Stratafix™ Knotless Tissue Control Devices (SFX KTCD; Ethicon, Inc., Bridgewater, NJ, USA) comprise a portfolio of knotless barbed suture devices which can be used at various tissue layers, most of which have a triclosan coating which is intended to inhibit bacterial colonization [13].
The aforementioned studies have provided important understanding of how barbed sutures generally compare with traditional sutures for wound closure of joint arthroplasty in a controlled setting; however, to our knowledge, there have been no large retrospective, observational studies that have examined this subject in the setting of routine clinical practice, or specifically for SFX KTCD. Thus, the objective of this study was to compare economic and clinical outcomes between SFX KTCD (henceforth referred to as the ‘barbed suture group’) and conventional sutures among patients undergoing knee or hip arthroplasty in real world clinical practice.
Materials & methods
Data & patient selection
This was a retrospective, observational study. The data source for this study was the Premier Hospital Database®, which comprises hospital administrative and billing information for all hospital discharges occurring within more than 700 hospitals throughout the USA. The database contains discharge level information on all International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) diagnoses and procedures recorded during each admission, a date-stamped log and cost of all billed items by cost-accounting department, administrative records on LOS and discharge status and selected information on patient, provider, hospital and insurance characteristics. Although the database excludes federally funded hospitals (e.g., Veterans Affairs), the hospitals included therein are nationally representative based on bed size, geographic region, location (urban/rural) and teaching status. The Premier Healthcare Database represents approximately twenty percent of annual US inpatient discharges [14].
Figure 1 shows the study's patient selection process. Patients included for study had a hospital discharge with a primary procedure code for knee arthroplasty (ICD-9-CM = 81.54) or hip arthroplasty (ICD-9-CM = 81.51, 81.52) between 1 January 2013 and 1 September 2015 (SFX KTCD was launched in October 2012). For each joint arthroplasty type (knee, hip) separately, the first hospital discharge for the specified joint arthroplasty type during this period was defined as the index discharge. Patients were required to be at least 18 years of age at the time of the index discharge, have a principal discharge diagnosis of osteoarthritis (ICD-9-CM = 715.xx) and to have undergone an elective procedure; the latter two criteria were applied to eliminate patients undergoing joint arthroplasty for acute reasons such as trauma or fracture, which may substantially complicate wound closure. Patients were excluded from the study if they had missing data on demographics (e.g., gender) or hospital costs, or if they had values for operating room time, as recorded in the database, which were less than 30 min or greater than 24 h, which may have been anomalous or incorrect values in the context of joint replacement procedures.
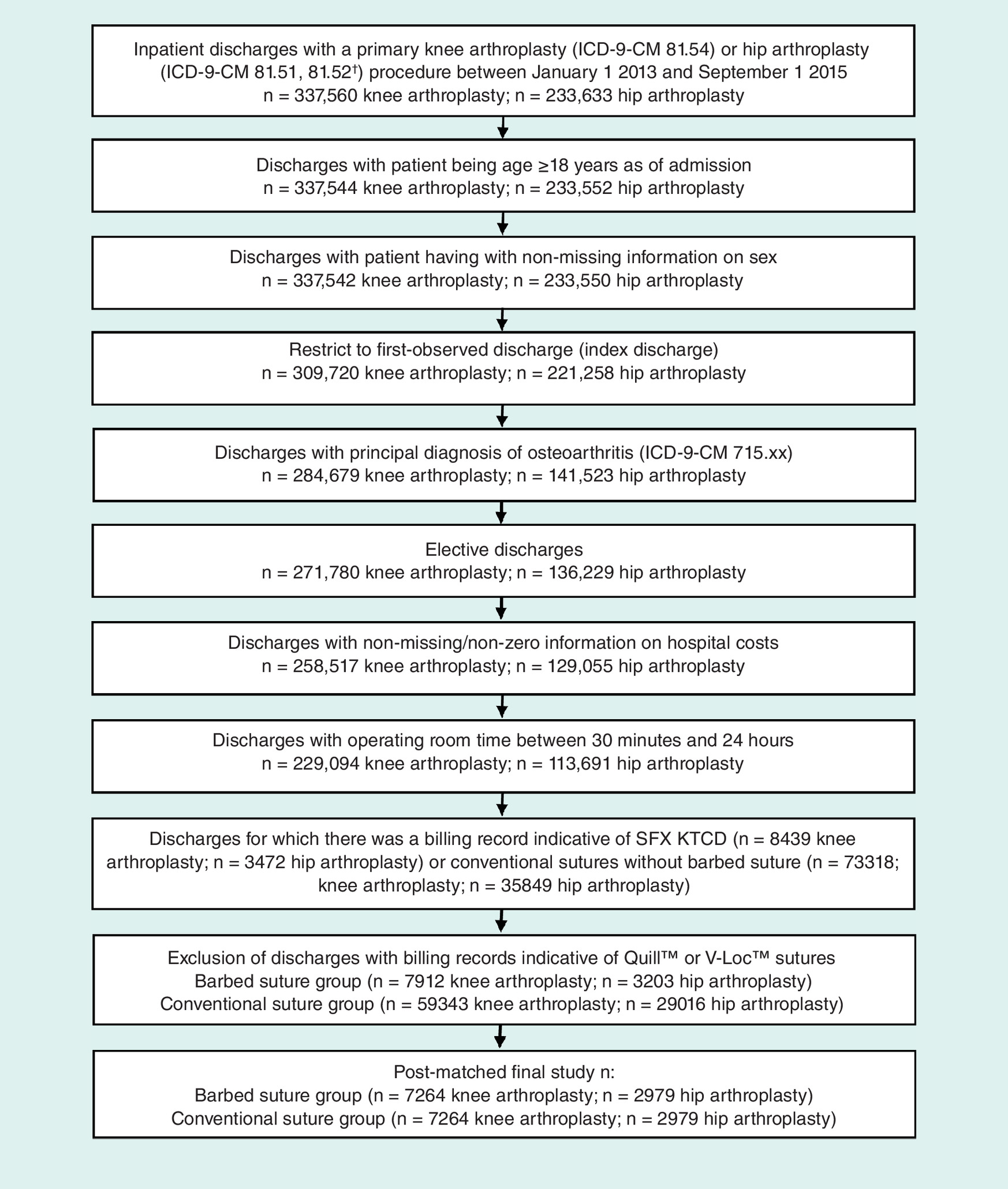
Figure 1. Patient selection.
†Ultimately, only six discharges in the barbed suture group and five discharges in the conventional sutures group (p = 0.763) had primary procedures corresponding to partial hip arthroplasty (ICD-9-CM 81.52).
ICD-9-CM: International Classification of Diseases, 9th Revision, Clinical Modification; SFX KTCD: STRATAFIX Knotless Tissue Control Device.
Use of either SFX KTCD or conventional sutures (Caprosyn™, Maxon™, Monocryl®, PDS, Polysorb™, and Vicryl®), during the index discharge was identified from hospital administrative records (charge descriptions) by searching for combinations of product names and abbreviations (e.g., ‘STRATAFIX’, ‘SFX’, ‘VICRYL’, ‘VCRL’) and/or model numbers (e.g., ‘SXMD1B101’, ‘VCP494H’). In an effort to maximize the classification accuracy of the product identification algorithms, charge descriptions were manually reviewed by two separate reviewers. Patients were ultimately classified into either the barbed suture group or the conventional suture group. To ensure mutual exclusivity of the patient groups, patients with any billing record for use of SFX KTCD during the index discharge were classified into the barbed suture group while patients in the conventional suture group were not allowed to have charge descriptions for SFX KTCD. Furthermore, patients in both the barbed suture and conventional suture groups were excluded if they had any charge descriptions that were consistent with other suture brands in the barbed suture category, namely Quill™ or V-Loc™ sutures. Information on wound closure protocols was not available in the database.
Measurement of patient & hospital/provider characteristics
Patient demographics measured during index discharge included: age, gender, marital status, race, payer type (e.g., Medicare) and year of index discharge. Patient clinical characteristics measured during the index discharge included: Quan and colleagues’ adaptation of the Charlson Comorbidity Index Score [15], which is a risk adjustment score based on ICD diagnosis coding that has been validated as being predictive of in-hospital mortality; selected individual comorbidities (chronic and/or risk factors for infection) from the Charlson Comorbidity Index and Elixhauser index defined per the ICD coding conventions outlined by Quan and colleagues [15] (cancer, chronic pulmonary disease, coagulopathy, depression, diabetes, hypertension, hypothyroidism, liver disease, obesity, other neurological disorders, peripheral vascular disorders, pulmonary circulation disorders, renal failure, rheumatoid arthritis/collagen and valvular disease); and binary indicator for tobacco use disorder (ICD-9-CM 305.1x), also a risk factor for infection. All comorbidities were adjusted to exclude instances wherein they were indicated as specifically not being ‘present on admission’.
Hospital/provider characteristics measured during index discharge included: urban versus rural hospital, hospital teaching status, hospital geographic region, hospital bed size, hospital annual joint procedure volume (separately calculated for knee arthroplasty and hip arthroplasty), procedural physician specialty (orthopedic surgery vs other), robotic assistance, day on which the joint arthroplasty procedure was performed relative to admission and an indicator for whether hospital costs are derived from a cost-to-charge ratio versus procedural costing.
Measurement of economic & clinical outcomes
Primary outcomes measured during index discharge included hospital LOS, total hospital costs (i.e., the costs of the index discharge from the hospital's perspective) and discharge to a skilled nursing facility or other nonhome setting versus discharge to home with or without home healthcare assistance. Total hospital costs were inflation adjusted to 2015 US dollars using the Medical Care component of the US Bureau of Labor Statistics Consumer Price Index. Exploratory outcomes measured during index discharge, unless otherwise noted, included operating room time, all cause readmissions, to the same hospital in which the joint arthroplasty was performed, within 30, 60, and 90 days postdischarge from index discharge, SSIs (identified through ICD-9-CM diagnosis codes indicated as not being ‘Present on Admission’), and nonprophylactic antibiotic use (antibiotic initiated ≥2 days postsurgery, with duration ≥2 days and an alternative variant which used duration ≥5 days) [16]. In order to eliminate nonprophylactic antibiotic use which may be associated with non-SSI postoperative infections such as urinary tract infection, patients with ICD-9-CM diagnosis codes associated with catheter-related blood stream infections, endocarditis, meningitis, pneumonia, sepsis, or urinary tract infections were excluded from being flagged as having nonprophylactic antibiotic use. ICD-9-CM codes used to identify the SSIs and non-SSI postoperative infections are shown in Supplementary Table A1.
Statistical analyses
Propensity score matching was used to adjust for observable biases which are inherent to observational studies. Patients in the barbed suture groups were propensity score matched to those in conventional sutures groups at a 1:1 ratio, without replacement, applying a caliper equal to 0.10 of the propensity score. The propensity score was derived from a multivariable logistic regression in which the dependent variable was membership in the barbed suture group (vs conventional suture group as reference) and the independent variables were all patient and hospital/provider characteristics described above. After matching, the standardized differences of the matching covariates were examined to identify whether any were imbalanced as indicated by an absolute value greater than 0.10 [17]. When necessary, outcomes were compared between the barbed suture and conventional suture groups using doubly robust estimation whereby any such imbalanced variables were entered into multivariable generalized estimating equations (GEE) or mixed models [18]. These models also accounted for hospital level-clustering, which can result when patients within a given single hospital receive more homogenous care, but differential care is provided from hospital-to-hospital. The GEE models used an exchangeable working correlation structure, which was chosen based on a qualitative understanding of the potential nature of clustering within hospitals. Each model used a link function and error distribution which was tailored to the empirical distribution of the outcome variable, specifically: hospital LOS and operating room time, log link/Poisson error; total hospital cost, log link/gamma error; all binary outcomes, logit link/binomial error distribution. Mixed models were used in lieu of GEE models only for binary outcomes and only if the GEE model would not converge. Adjusted outcomes were generated for each of the study groups using the least squares means approach based on observed margins. In the GEE models, inference was based on empirical (robust) standard error estimates. A two-sided critical value of 0.05 was used to determine statistical significance and statistical significance testing was performed only in the context of the adjusted analyses. All statistical analyses were performed using SAS version 9.3.
Results
Propensity score matching
A total of 67,255 patients undergoing knee arthroplasty and 32,219 patients undergoing hip arthroplasty met all inclusion/exclusion criteria prior to matching (Figure 1: knee arthroplasty: barbed suture n = 7912; conventional suture n = 59,343; hip arthroplasty: barbed suture n = 3203; conventional suture n = 29,016). After 1:1 propensity score matching, there were 7264 patients in each suture comparison group among those undergoing knee arthroplasty (14,528 total patients) and 2979 patients in each suture comparison group among those undergoing hip arthroplasty (5958 total patients). Plots of standardized differences for matching covariates before versus after propensity score matching are shown in Figures 2A (knee arthroplasty) and 2B (hip arthroplasty). The groups were well-balanced on matching covariates after propensity score matching, with only teaching versus nonteaching hospital having a standardized difference greater than 0.10 among patients undergoing knee arthroplasty. All other matching variables fell within the standardized difference threshold of not exceeding an absolute value of 0.10 and thus were deemed to be adequately balanced across the suture comparison groups. Prematch descriptive statistics on patient demographics, patient clinical characteristics and hospital/provider characteristics are shown in Supplementary Tables A2–A4, respectively.
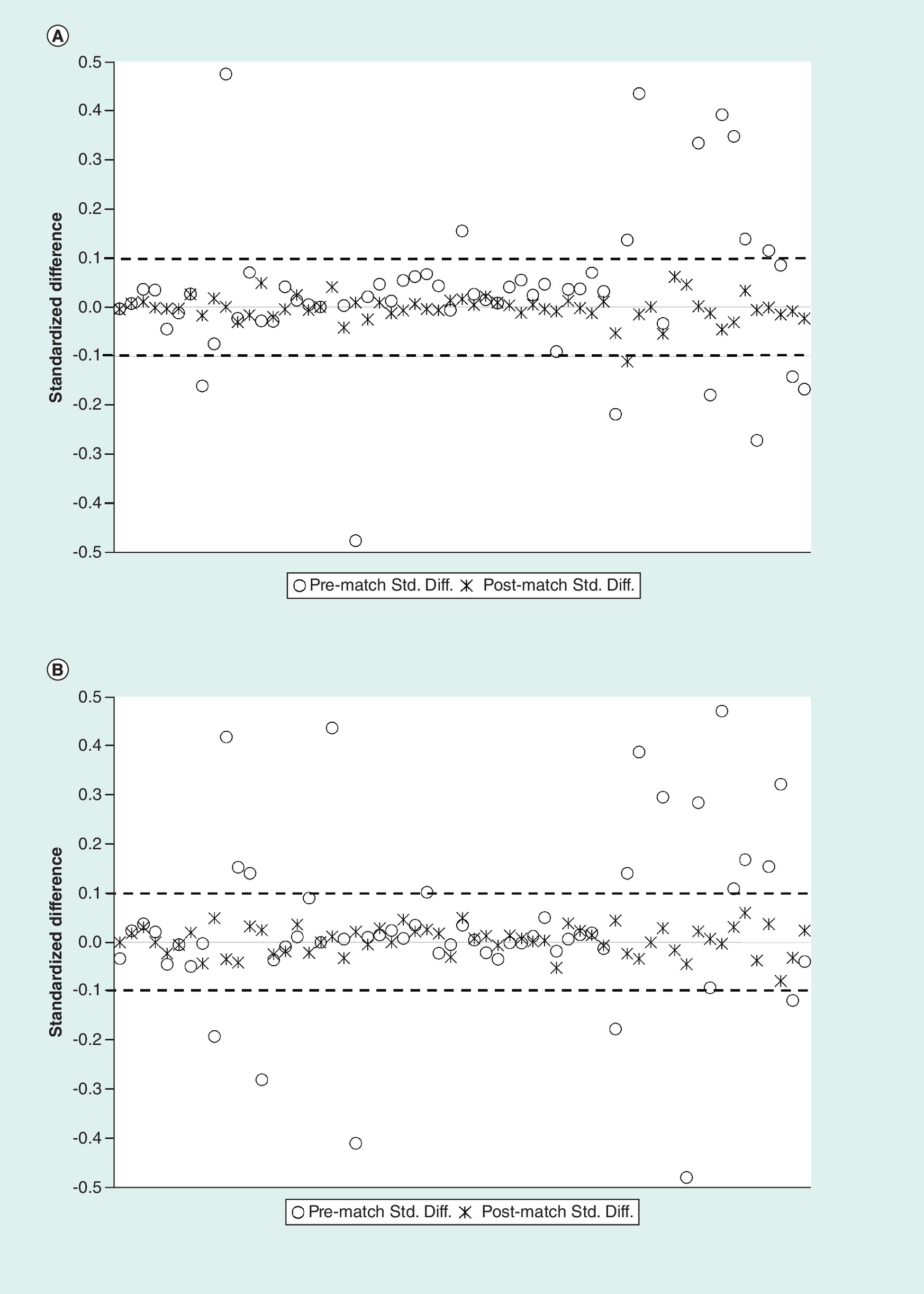
Figure 2. Propensity score matching results.
(A) Plot of standardized differences before versus after propensity score matching: knee arthroplasty. Each marker corresponds to a standardized difference value for a single covariate. Markers which fall outside of the dashed lines are considered to be imbalanced between the barbed and conventional suture groups. After matching, only one marker fell outside of the dashed line, which corresponded to the variable teaching hospital. This variable was included for doubly-robust estimation in multivariable models used to compare outcomes between the study groups. (B) Plot of standardized differences before versus after propensity score matching: hip arthroplasty. Each marker corresponds to a standardized difference value for a single covariate. Markers which fall outside of the dashed lines are considered to be imbalanced between the barbed and conventional suture groups. After matching, all markers fell between the dashed lines.
Std. Diff.: Standardized difference.
Patient & hospital/provider characteristics
Postmatch descriptive statistics on patient demographics, patient clinical characteristics and hospital/provider characteristics are shown in in Tables 1–3, respectively. Among patients undergoing knee arthroplasty, patients had an average age of approximately 67 years and the majority of patients were female (61.2–62.4%). Among patients undergoing hip arthroplasty, patients had an average age of approximately 66 years and the majority of patients were female (58.0–59.0%). The majority of patients were white (knee arthroplasty: 78.2% barbed suture, 76.9% conventional suture; hip arthroplasty: 74.1% barbed suture, 72.3% conventional suture). Among the examined comorbidities, the three most commonly diagnosed were hypertension (knee arthroplasty: 68.3% barbed suture, 68.1% conventional suture; hip arthroplasty: 59.7% barbed suture, 60.9% conventional suture), obesity (knee arthroplasty: 23.2% barbed suture, 23.9% conventional suture; hip arthroplasty: 19.9% barbed suture, 21.9% conventional suture) and diabetes (knee arthroplasty: 20.9% barbed suture, 21.2% conventional suture; hip arthroplasty: 15.0% barbed suture, 15.8% conventional suture). Procedures were performed predominantly in urban hospitals (knee arthroplasty: 84.3% barbed suture, 86.2% conventional suture; hip arthroplasty: 86.7% barbed suture, 85.2% conventional suture), in hospitals having annual knee/hip arthroplasty volume between 151 and 300 procedures per year (knee arthroplasty: 38.6% barbed suture, 38.3% conventional suture; hip arthroplasty: 50.5% barbed suture, 48.6% conventional suture), and predominantly by orthopedic surgeons (knee arthroplasty: 96.0% barbed suture, 95.8% conventional suture; hip arthroplasty: 95.4% barbed suture, 94.7% conventional suture).
| Demographic characteristics | Knee arthroplasty | Hip arthroplasty | ||||
|---|---|---|---|---|---|---|
| Barbed suture group 7264 (%) | Conventional suture group 7264 (%) | Std. Diff. | Barbed suture group 2979 (%) | Conventional suture group 2979 (%) | Std. Diff. | |
| Age, mean (SD; years) | 66.5 (9.6) | 66.5 (9.5) | -0.00 | 66.0 (10.9) | 65.6 (11.0) | -0.03 |
| Age category (%): | ||||||
| – 18–34 | 0.1 | 0.1 | 0.00 | 0.6 | 0.6 | 0.00 |
| – 35–44 | 1.3 | 1.3 | 0.01 | 2.0 | 2.3 | 0.02 |
| – 45–54 | 9.4 | 9.7 | 0.01 | 11.8 | 12.8 | 0.03 |
| – 55–64 | 28.7 | 28.6 | 0.00 | 28.4 | 28.4 | 0.00 |
| – 65–74 | 39.7 | 39.5 | 0.00 | 34.9 | 33.8 | -0.02 |
| – 75 plus | 20.9 | 20.8 | 0.00 | 22.2 | 22.0 | 0.00 |
| Female, % | 61.2 | 62.4 | 0.03 | 58.0 | 59.0 | 0.02 |
| Marital status (N/%): | ||||||
| – Married | 62.2 | 61.4 | -0.02 | 54.5 | 52.3 | -0.04 |
| – Single | 36.9 | 37.7 | 0.02 | 44.6 | 47.0 | 0.05 |
| – Other | 0.9 | 0.9 | 0.00 | 0.9 | 0.6 | -0.03 |
| Race (%): | ||||||
| – White | 78.2 | 76.9 | -0.03 | 74.1 | 72.3 | -0.04 |
| – African–American | 8.1 | 7.6 | -0.02 | 6.0 | 6.8 | 0.03 |
| – Other | 13.7 | 15.5 | 0.05 | 19.9 | 20.9 | 0.03 |
| Payer (%): | ||||||
| – Medicare | 60.6 | 59.6 | -0.02 | 57.2 | 56.0 | -0.02 |
| – Medicaid | 2.5 | 2.4 | 0.00 | 2.9 | 2.6 | -0.02 |
| – Commercial | 34.4 | 35.5 | 0.02 | 38.1 | 39.9 | 0.04 |
| – Other | 2.6 | 2.5 | -0.01 | 1.8 | 1.5 | -0.02 |
| Year of index discharge's discharge date (%): | ||||||
| – 2013 | 17.5 | 19.1 | 0.04 | 18.6 | 19.1 | 0.01 |
| – 2014 | 37.7 | 35.7 | -0.04 | 37.7 | 36.2 | -0.03 |
| – 2015 | 44.8 | 45.3 | 0.01 | 43.7 | 44.8 | 0.02 |
Variables for which one or more level had a standardized difference exceeding an absolute value of 0.10 were considered to be imbalanced and were adjusted for in the multivariable regressions.
SD: Standard deviation; Std. Diff.: Standardized difference.
| Clinical characteristics | Knee arthroplasty | Hip arthroplasty | ||||
|---|---|---|---|---|---|---|
| Barbed suture group 7264 (%) | Conventional suture group 7264 (%) | Std. Diff. | Barbed suture group 2979 (%) | Conventional suture group 2979 (%) | Std. Diff. | |
| Comorbidities (%): | ||||||
| – Cancer | 0.5% | 0.3% | -0.03 | 0.7% | 0.7% | 0.00 |
| – Chronic pulmonary disease | 15.3% | 15.6% | 0.01 | 14.0% | 15.0% | 0.03 |
| – Coagulopathy | 1.0% | 0.9% | -0.01 | 1.1% | 1.1% | 0.00 |
| – Depression | 15.0% | 14.7% | -0.01 | 13.9% | 15.6% | 0.05 |
| – Diabetes | 20.9% | 21.2% | 0.01 | 15.0% | 15.8% | 0.02 |
| – Hypertension | 68.3% | 68.1% | 0.00 | 59.7% | 60.9% | 0.03 |
| – Hypothyroidism | 17.0% | 16.7% | -0.01 | 15.8% | 16.5% | 0.02 |
| – Liver disease | 1.5% | 1.7% | 0.01 | 1.4% | 1.1% | -0.03 |
| – Obesity | 23.2% | 23.9% | 0.02 | 19.9% | 21.9% | 0.05 |
| – Other neurological disorders | 1.7% | 1.7% | 0.00 | 1.6% | 1.7% | 0.01 |
| – Peripheral vascular disorders | 2.3% | 2.7% | 0.02 | 3.1% | 3.4% | 0.01 |
| – Pulmonary circulation disorders | 0.8% | 0.9% | 0.01 | 1.2% | 1.1% | -0.01 |
| – Renal failure | 5.5% | 5.6% | 0.00 | 5.7% | 6.0% | 0.01 |
| – Rheumatoid arthritis/collagen | 3.7% | 3.5% | -0.01 | 4.2% | 4.4% | 0.01 |
| – Tobacco use disorder | 7.4% | 7.5% | 0.00 | 10.4% | 10.5% | 0.00 |
| – Valvular disease | 3.2% | 3.1% | 0.00 | 3.1% | 3.2% | 0.00 |
| CCI score (%): | ||||||
| – 0 | 58.2% | 57.7% | -0.01 | 62.2% | 59.7% | -0.05 |
| – 1 | 26.8% | 27.4% | 0.01 | 23.7% | 25.4% | 0.04 |
| – 2 | 9.7% | 9.7% | 0.00 | 8.3% | 9.0% | 0.02 |
| – 3 | 3.0% | 2.8% | -0.01 | 3.3% | 3.6% | 0.01 |
| – ≥4 | 2.3% | 2.5% | 0.01 | 2.5% | 2.4% | -0.01 |
Variables for which one or more level had a standardized difference exceeding an absolute value of 0.10 were considered to be imbalanced and were adjusted for in the multivariable regressions.
CCI: Charlson Comorbidity Index; SD: Standard deviation; Std. Diff.: Standardized difference.
| Hospital/Provider Characteristic | Knee arthroplasty | Hip arthroplasty | ||||
|---|---|---|---|---|---|---|
| Barbed suture group 7264 (%) | Conventional suture group 7264 (%) | Std. Diff. | Barbed suture group 2979 (%) | Conventional suture group 2979 (%) | Std. Diff. | |
| Rural hospital (%) | 15.7 | 13.8 | -0.05 | 13.3 | 14.8 | 0.04 |
| Urban hospital (%) | 84.3 | 86.2 | 0.05 | 86.7 | 85.2 | -0.04 |
| Teaching hospital (%) | 25.4 | 20.7 | -0.11§ | 29.6 | 28.6 | -0.02 |
| Geographic region (%): | ||||||
| – Midwest | 3.0 | 2.8 | -0.01 | 4.1 | 3.5 | -0.03 |
| – Northeast | 0.0 | 0.0 | – | 0.0 | 0.0 | – |
| – South | 69.7 | 67.2 | -0.05 | 47.9 | 49.3 | 0.03 |
| – West | 27.3 | 30.1 | 0.06 | 48.0 | 47.2 | -0.02 |
| Hospital bed size (%): | ||||||
| – <200 | 45.0 | 47.3 | 0.05 | 42.6 | 40.4 | -0.04 |
| – 200–299 | 10.9 | 10.9 | 0.00 | 9.5 | 10.2 | 0.02 |
| – 300–399 | 30.9 | 30.3 | -0.01 | 29.0 | 29.3 | 0.01 |
| – 400–499 | 4.1 | 3.2 | -0.05 | 1.5 | 1.5 | 0.00 |
| – ≥500 | 9.2 | 8.3 | -0.03 | 17.4 | 18.6 | 0.03 |
| Hospital annual knee/hip arthroplasty volume (%): | ||||||
| – 1–150 | 11.8 | 12.9 | 0.03 | 21.8 | 24.4 | 0.06 |
| – 151–300 | 38.6 | 38.3 | -0.01 | 50.5 | 48.6 | -0.04 |
| – 300–450 | 15.1 | 15.1 | 0.00 | 18.1 | 19.6 | 0.04 |
| – ≥451 | 34.5 | 33.8 | -0.02 | 9.6 | 7.5 | -0.08 |
| Procedural physician specialty (%): | ||||||
| – Orthopedic surgery | 96.0 | 95.8 | -0.01 | 95.4 | 94.7 | -0.03 |
| – Other specialty | 4.0 | 4.2 | 0.01 | 4.6 | 5.3 | 0.03 |
| Robotic assistance (%) | 1.4 | 1.1 | -0.02 | 0.6 | 0.8 | 0.02 |
| Day of procedure†, mean (SD) | 1.0 (0.1) | 1.0 (0.1) | 0.02 | 1.0 (0.3) | 1.0 (0.1) | 0.01 |
| Cost-to-charge ratio‡ (%) | 23.4 | 20.3 | -0.08 | 33.1 | 30.0 | -0.07 |
†Day on which the knee/hip arthroplasty was performed relative to admission day for index discharge.
‡Hospital costs are derived from a cost-to-charge ratio versus procedural costing.
§Variables for which one or more level had a standardized difference exceeding an absolute value of 0.10 were considered to be imbalanced and were adjusted for in the multivariable regressions.
SD: Standard deviation; Std. Diff.: Standardized difference.
Propensity score matched analysis of outcomes in patients undergoing knee arthroplasty
Results of the propensity score matched analysis of outcomes are shown in Table 4. Among patients undergoing knee arthroplasty: mean adjusted hospital LOS was lower in the barbed suture group than in the conventional sutures group (2.7 vs 2.9 days; p = 0.006). Mean adjusted total hospital costs were nonsignificantly lower in the barbed suture group than in the conventional sutures group (US$17,038 vs US$18,144; p = 0.103). The adjusted percentage of patients being discharged to a SNF or other nonhome setting was lower in the barbed suture group than in the conventional sutures group (25.7 vs 28.7%; p = 0.013). Mean adjusted total operating room time was lower in the barbed suture group than in the conventional sutures group (183 vs 190 min; p = 0.0235). With respect to the other secondary outcomes of the percentage of patients with all-cause readmissions at 30, 60 and 90 days postdischarge and the percentage of patients with SSI and/or nonprophylactic antibiotics, nearly all values were nonsignificantly lower in the barbed suture group than in the conventional sutures group; however, the differences met statistical significance for the outcome of ≥2 days of nonprophylactic antibiotics (1.6 vs 2.5%; p = 0.002).
| Knee arthroplasty | Hip arthroplasty | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Barbed suture group | Conv. | Effect† suture group | 95% CI | p-value | Barbed suture group | Conv. | Effect† suture group | 95% CI | p-value | |||
| Hospital LOS | 2.7 | 2.9 | 0.94 | 0.90 | 0.98 | 0.006 | 2.5 | 2.8 | 0.88 | 0.81 | 0.96 | 0.002 |
| Discharge to SNF/other nonhome setting‡ | 25.7% | 28.7% | 0.86 | 0.77 | 0.97 | 0.013 | 21.7% | 28.5% | 0.70 | 0.58 | 0.83 | <.0001 |
| Total hospital cost | US$17,039 | US$18,144 | 0.94 | 0.87 | 1.01 | 0.103 | US$16,668 | US$18,759 | 0.89 | 0.79 | 1.00 | 0.051 |
| Total operating room time | 183 | 190 | 0.96 | 0.93 | 1.00 | 0.024 | 184 | 206 | 0.89 | 0.82 | 0.97 | 0.009 |
| All-cause readmissions (%): | ||||||||||||
| 30 days postdischarge | 2.4% | 2.8% | 0.85 | 0.68 | 1.08 | 0.177 | 1.4% | 1.4% | 1.01 | 0.67 | 1.52 | 0.962 |
| 60 days postdischarge | 3.9% | 4.1% | 0.97 | 0.80 | 1.16 | 0.725 | 3.4% | 4.0% | 0.84 | 0.64 | 1.12 | 0.233 |
| 90 days postdischarge | 5.9% | 6.3% | 0.94 | 0.80 | 1.09 | 0.406 | 5.5% | 6.3% | 0.87 | 0.67 | 0.67 | 0.316 |
| SSI and nonprophylactic antibiotic outcomes (%): | ||||||||||||
| SSI, diagnosis only | 0.2% | 0.3% | 0.70 | 0.35 | 1.39 | 0.306 | 0.2% | 0.4% | 0.45 | 0.16 | 1.31 | 0.143 |
| SSI + 2 days of nonprophylactic antibiotics | 0.1% | 0.2% | 0.71 | 0.32 | 1.61 | 0.416 | 0.1% | 0.3% | 0.44 | 0.14 | 1.44 | 0.177 |
| SSI + 5 days of nonprophylactic antibiotics | 0.0% | 0.1% | 0.50 | 0.13 | 2.0 | 0.327 | 3 events in conventional, 0 SFX KTCD | |||||
| ≥2 days of nonprophylactic antibiotics | 1.6% | 2.5% | 0.65 | 0.50 | 0.85 | 0.002 | 1.4% | 2.2% | 0.65 | 0.40 | 1.04 | 0.074 |
| ≥5 days of nonprophylactic antibiotics | 0.2% | 0.3% | 0.54 | 0.27 | 1.07 | 0.079 | 0.1% | 0.3% | 0.47 | 0.16 | 1.39 | 0.172 |
†For hospital LOS, effect is an incidence rate ratio; for total hospital cost and total operating room time, the effect is a ratio of means (exponentiated beta coefficient from model); for all other outcomes (all binary), the effect is an odds ratio.
‡Versus home/home health care; among patients discharged to SNF/other nonhome setting: 66.3% (knee arthroplasty) and 69.7% (hip arthroplasty) were discharged to SNF, 25.3% (knee arthroplasty) and 22.4% (hip arthroplasty) were discharged to ‘other rehab’, and the remaining 8.4% (knee arthroplasty) and 7.9% (hip arthroplasty) were discharged to other settings.
Conv.: Conventional; LOS: Length of stay; SNF: Skilled nursing facility; SSI: Surgical site infection.
Propensity score matched analysis of outcomes in patients undergoing hip arthroplasty
Similar results were observed among patients undergoing hip arthroplasty (Table 4). Mean adjusted hospital LOS was lower in the barbed suture group than in the conventional sutures group (2.5 vs 2.8 days; p = 0.002). Mean adjusted total hospital costs were nonsignificantly lower in the barbed suture group than in the conventional sutures group (US$16,668 vs US$18,759; p = 0.051). The adjusted percentage of patients being discharged to a SNF or other nonhome setting was lower in the barbed suture group than in the conventional sutures group (21.7 vs 28.5%; p < 0.001). Mean adjusted total operating room time was lower in the barbed suture group than in the conventional sutures group (184 vs 206 min; p = 0.009). With respect to the other secondary outcomes of the percentage of patients with all-cause readmissions at 30, 60, and 90-days postdischarge and the percentage of patients with SSI and/or nonprophylactic antibiotics, all values were nonsignificantly lower in the barbed suture group than in the conventional sutures group.
Discussion
To our knowledge, this is one of the first and largest retrospective, observational studies to compare economic and clinical outcomes between the SFX KTCD variety of barbed sutures and conventional sutures among patients undergoing knee or hip arthroplasty in real world clinical practice. After propensity score matching to reduce bias, patients for whom the wound closure was performed using barbed sutures were observed to differ significantly on several important outcomes as compared with those for whom the wound closure was performed using conventional sutures alone. Although many of the statistically significant differences may be viewed as modest in magnitude at an individual per-patient level, at a hospital or health system level, the accumulative impact of these differences may be substantial, especially for higher volume institutions.
Patients for whom the wound closure was performed using barbed sutures had significantly shorter hospital LOS as compared with patients for whom the wound closure was performed using conventional sutures alone (7% shorter for knee arthroplasty; p = 0.006; 11% shorter for hip arthroplasty; p = 0.002). To our knowledge, only one prior study has reported a comparison of hospital LOS between barbed sutures (Quill bidirectional barbed sutures [Quill SRS; Angiotech, Reading, PA]) and conventional sutures (combination of Vicryl and Monocryl; Ethicon, Inc., NJ, USA), and it was specifically conducted among patients undergoing total knee arthroplasty [11]. In that single-center, single surgeon study based on 90 procedures (performed between November 2007 and September 2008) using barbed sutures and 88 procedures (performed between January 2007 and November 2007) using conventional sutures alone, no significant differences were reported between the groups for hospital LOS. The present study differs substantially from the prior study in terms of its relatively larger size (14,528 knee arthroplasty procedures vs 178), multi-institutional nature, time frame (2013–2015) and type of barbed suture (SFX KTCD, most of which are triclosan (antibacterial)-coated whereas Quill sutures are not, a factor which may influence wound infection). A retrospective study using the Nationwide Inpatient Sample found that mechanical wound complications and infection were drivers of hospital LOS for knee arthroplasty [19]. Although the present study did not examine mechanical wound complications, the barbed suture group was associated with a nonsignificantly lower rate of SSIs as compared with the conventional sutures group, which could partially drive this finding. Furthermore, among patients undergoing knee arthroplasty, the rate of nonprophylactic antibiotic use for a duration of two or more days, a potential marker of SSI, was significantly lower in the barbed suture group as compared with the conventional sutures group. The barbed suture group was also associated with nonsignificantly lower rates of nonprophylactic antibiotics among patients undergoing hip arthroplasty. With respect to generalizability, the present study's overall findings on duration of hospital LOS (ranging 2.5–2.9 days across the groups) compare well to that of data from the Nationwide Inpatient Sample, which in 2014 report a mean hospital LOS of 2.8 days for both total knee and total hip arthroplasty [2]. Ultimately, further research to corroborate and to identify the specific underlying causes of these findings related to hospital LOS would be useful.
Patients for whom the wound closure was performed using barbed sutures had significantly lower rates of discharge to SNF or other nonhome settings as compared with patients for whom the wound closure was performed using conventional sutures alone (10.5% lower for knee arthroplasty; p = 0.013; 23.9% lower for hip arthroplasty; p < 0.001). Although it is not possible to pinpoint the underlying causes of this difference, the same factors which may have driven shorter hospital LOS in the barbed suture group could have a similar influence on being discharged to SNF or other nonhome settings versus the home setting. This finding has important economic implications because prior analyses have shown that nonhome discharge destinations can impose a substantial financial burden to both patients and payers [20].
Patients for whom the wound closure was performed using barbed sutures had significantly shorter total operating room times as compared with patients for whom the wound closure was performed using conventional sutures alone (7 min shorter for knee arthroplasty, p = 0.024; 22 min shorter for hip arthroplasty; p = 0.009). Differences in wound closure time between barbed and conventional sutures have been reported in numerous randomized trials and systematic meta-analyses, nearly all of which have reported significantly shorter wound closure time for barbed sutures as compared with conventional sutures [6–11]. In the present study, total operating room time represents not only the wound closure time, which can reportedly represent 10–20% of the overall surgical procedure time [21], but the duration of time for which the operating room is used for the entire procedure. Thus, other factors which influence operating room time could have an impact on the findings.
Total hospital costs were nonsignificantly lower for the barbed suture group as compared with the conventional sutures group (marginally so for patients undergoing hip arthroplasty [p = 0.051]). This was likely driven by both the hospital LOS for barbed suture and the shorter total operating room time. The absolute magnitude of the differences in adjusted mean total hospital costs were nontrivial: US$1105 among patients undergoing knee arthroplasty and US$2091 among patients undergoing hip arthroplasty. Several prior studies have reported significant cost savings associated with the use of barbed sutures as compared with conventional sutures alone, ranging from US$48.70–US$549.59 per case, driven by shorter wound closure time and less suture material usage [6,7,10,22]. In an unadjusted, post hoc analysis of subcategories of costs in the propensity score matched groups, the barbed suture group had numerically lower mean costs for each category (Supplementary Table A5). In the present study, our findings of significantly lower operating room time and LOS, but insignificantly lower total hospital costs may have been a function of the comparatively less normal distribution of costs versus operating room and LOS and by the fact that together, operating room costs and room and board costs (which would be reflective of operating time and LOS differences) did not account for a majority (31–33%) of total hospital costs. Importantly, the cost differences observed in the present study do not account for costs incurred in the postdischarge setting, for which the conventional sutures group had more resource intensive discharge statuses.
Although SSI rates were non-significantly lower for the barbed suture group as compared with the conventional suture group, SSIs during the index admission was rare, occurring in only approximately 0.2–0.4% of patients. However, SSIs rates tend to be low in knee and hip arthroplasty procedures and tend to develop after discharge from the index admission. For example, a study by Yokoe and colleagues (2013) found that among 121,640 total knee arthroplasty procedures and 91,121 total hip arthroplasty procedures performed in California hospitals between 2006 and 2009, the SSI rate was 2.0% and 2.3% over a 365-day period following the knee and hip arthroplasty procedures, respectively [23]. Of these, only 12.2% (0.24% total rate) and 15.0% (0.35%) of infection in knee and hip arthroplasties, respectively, were identified during the initial hospitalization. Those findings both corroborate the present study's findings regarding the low SSI rate during the index admissions and underscore the need for future research to understand any potential long-term differences in SSIs between barbed suture and conventional sutures alone. Prior studies have generally reported little by way of differences between barbed and conventional sutures in terms of infection and other complications [7–9], though some have found statistically significant differences in favor of barbed sutures [6] or of conventional sutures [24].
Finally, all-cause readmission rates at 30, 60, and 90 days postdischarge from the index discharge were nonsignificantly lower for the barbed suture group as compared with the conventional suture group. The readmission outcome was designated as ‘exploratory’ due to an inherent limitation of the Premier Healthcare Database, which is that only readmissions which occur within the same hospital as the index discharge (i.e., initial procedure) are identifiable. One driver of the observed, albeit nonsignificant, differences in all-cause readmission rates could be the shorter hospital LOS in the barbed suture group: a prior analysis by Williams and colleagues (2017) reported that among Medicare patients undergoing knee or hip arthroplasty, increased hospital LOS was a significant risk factor for 90-day readmission [25].
Limitations
The present study is subject to some additional limitations beyond those discussed above. First, the nonrandomized, observational nature of this study does not allow for causal inference regarding the effect of suture type on the study outcomes. All findings of the present study must be interpreted as associations. To address potential observable bias, propensity score matching was implemented to account for a large number of patient, provider, hospital and procedural characteristics, resulting in very well-balanced comparison groups. Although 7–9% of patients in the prematched barbed suture group could not be matched to a patient in the conventional suture group due to divergent propensity score distributions, this study favored a statistical approach to maximize internal validity.
However, the study's results may be subject to residual confounding based on unmeasured factors which could plausibly bias the study results, such as the other medical devices (e.g., knee implant type) and wound closure technologies (e.g., topical skin adhesives, staples) used in the procedures, or the performance of the procedural physician and supporting operating room staff (e.g., differences between early adopters vs nonadopters of newer suture technology).
This premier healthcare database is a nonprobability sample and thus this study's results may not be generalizable to all hospitals and patients in the USA. However, this study is perhaps the largest of its kind to date, spanning multiple institutions and years, and thus can be viewed as being more reflective of real-world clinical practice than single-center or small randomized trials. Furthermore, the study results were generally consistent across two different major orthopedic procedures, which is suggestive of robust internal validity.
Devices such as sutures currently possess a Unique Device Identifiers; however, this coding system is not currently well-disseminated into large observational data sources such as the Premier Healthcare Database. Consequently, device identification was based upon on free-text string searches to identify the use of barbed and conventional sutures. Because some sutures may be low cost, it is possible that hospitals may not choose to bill separate line items for such materials, and hence the absence of a record for a given device is not necessarily proof that it was not used. Presumably sutures with a price premium such as barbed sutures would be more likely to be billed separately, which would reduce the likelihood of misclassification of patients between the barbed suture group and the conventional suture group. Although it is not possible to determine the exact accuracy of the method for classification of patients into study groups, if patients who used barbed sutures were indeed inaccurately placed in the conventional suture group, this would have tended to bias the study results away from favoring the barbed suture group.
The hospital billing records also indicate only that the suture was billed for, but not the layer of tissue in which it was used. Information on wound closure protocols was not available in the database. Future studies which account for wound closure protocol and sub-analyze the tissue layers at which barbed sutures are used would be useful.
Conclusion
In conclusion, among patients undergoing knee or hip arthroplasty for osteoarthritis in real world clinical practice, use of barbed sutures was associated with shorter hospital LOS, shorter operating room time and less resource intensive discharge status as compared with conventional sutures alone.
The present study was a retrospective, observational study using the Premier Hospital Database®, which comprises hospital administrative and billing information for all hospital discharges occurring within more than 700 hospitals throughout the USA.
Patients (aged ≥18 years) were selected for study if they had elective knee or hip arthroplasty for osteoarthritis between 1 January 2013 and 1 September 2015. Patients were classified into mutually-exclusive study groups based on suture usage: any SFX KTCD (barbed suture group) versus conventional sutures alone (conventional suture group).
Primary outcomes were hospital length of stay, total hospital costs, and discharge status; exploratory outcomes included total operating room time, all-cause readmissions at 30/60/90 days postdischarge, surgical site infection diagnosis and nonprophylactic antibiotic use.
After matching, the analysis included 14,528 (7264 per group) and 5958 (2979 per group) patients undergoing knee or hip arthroplasty, respectively.
This study found that after propensity score matching to address confounding, use of barbed sutures was associated with shorter hospital length of stay, shorter operating room time and less resource intensive discharge status as compared with conventional sutures alone.
Differences in wound closure time between barbed and conventional sutures have been reported in numerous randomized trials and systematic meta-analyses, nearly all of which have reported significantly shorter wound closure time for barbed sutures as compared with conventional sutures.
This study is perhaps the largest of its kind to date, spanning multiple institutions and years, and thus can be viewed as being more reflective of real-world clinical practice than single-center or small randomized trials.
Supplementary data
To view the supplementary data that accompany this paper please visit the journal website at: Supplementary Material
Acknowledgements
The authors thank A Pardasani of Johnson & Johnson for contributing to the paper. Outcomes, Inc assisted with the preparation of this manuscript.
Financial & competing interest disclosure
This study is funded by Johnson & Johnson. All authors are paid employees of Johnson & Johnson. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Supplementary Material
File (supplementary_data.docx)
- Download
- 33.48 KB
References
Papers of special note have been highlighted as: • of interest
1.
HCUP Fast Stats. Healthcare Cost and Utilization Project (HCUP). Agency for Healthcare Research and Quality, Rockville, MD (2017). www.hcup-us.ahrq.gov/faststats/national/inpatientcommonprocedures.jsp.
2.
HCUPnet, Healthcare Cost and Utilization Project. Agency for Healthcare Research and Quality, Rockville, MD (2017). https://hcupnet.ahrq.gov/#setup.
3.
Centers for Medicare & Medicaid Services. Comprehensive care for joint replacement model (2017). https://innovation.cms.gov/initiatives/CJR.
4.
Centers for Medicare & Medicaid Services. Hospital quality initiative: outcome measures (2017). www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/HospitalQualityInits/OutcomeMeasures.html.
5.
Centers for Medicare & Medicaid Services. Readmissions reduction program (HRRP) (2017). www.cms.gov/medicare/medicare-fee-for-service-payment/acuteinpatientpps/readmissions-reduction-program.html.
6.
Chan VWK, Chan PK, Chiu KY, Yan CH, Ng FY. Does barbed suture lower cost and improve outcome in total knee arthroplasty? A randomized controlled trial. J. Arthroplasty 32(5), 1474–1477 (2017).
• Article of interest due to also having comparison between barbed and conventional sutures.
7.
Zhang W, Xue D, Yin H et al. Barbed versus traditional sutures for wound closure in knee arthroplasty: a systematic review and meta-analysis. Sci. Rep. 25(6), 19764 (2016).
• Article of interest due to also having comparison between barbed and conventional sutures.
8.
Borzio RW, Pivec R, Kapadia BH, Jauregui JJ, Maheshwari AV. Barbed sutures in total hip and knee arthroplasty: what is the evidence? A meta-analysis. Int. Orthop. 40(2), 225–231 (2016).
9.
Meena S, Gangary S, Sharma P, Chowdhury B. Barbed versus standard sutures in total knee arthroplasty: a meta-analysis. Eur. J. Orthop. Surg. Traumatol. 25(6), 1105–1110 (2015).
10.
Smith EL, DiSegna ST, Shukla PY, Matzkin EG. Barbed versus traditional sutures: closure time, cost, and wound related outcomes in total joint arthroplasty. J. Arthroplasty 29(2), 283–287 (2014).
• Article of interest due to also having comparison between barbed and conventional sutures.
11.
Eickmann T, Quane E. Total knee arthroplasty closure with barbed sutures. J. Knee Surg. 23(3), 163–167 (2010).
12.
Levine BR, Ting N, Della Valle CJ. Use of a barbed suture in the closure of hip and knee arthroplasty wounds. Orthopedics 34(9), e473–e475 (2011).
13.
Ethicon. STRATAFIX™ Knotless Tissue Control Devices (2017). www.ethicon.com/healthcare-professionals/products/wound-closure/tissue-control-devices.
14.
Premier Healthcare Database White Paper: Data that informs and performs. Premier Applied Sciences, Premier Inc (2018). www.premierinc.com/transforming-healthcare/healthcareperformance-improvement/premier-applied-sciences/.
15.
Quan H et al. Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data. Med. Care 43(11), 1130–1139 (2005).
16.
Yokoe DS, Noskin GA, Cunningham SM et al. Enhanced identification of postoperative infections among Inpatients. Emerg. Infect. Dis. 10(11), 1924–1930 (2004).
17.
D'Agostino RB Jr. Propensity score methods for bias reduction in the comparison of a treatment to a non-randomized control group. Stat. Med. 17, 2265–2281 (1998).
18.
Hardin JW, Hilbe JM. Generalized Estimating Equations (2nd Edition). Chapman & Hall/CRC, FLUSA (2013).
19.
El Bitar YF, Illingworth KD, Scaife SL et al. Hospital length of stay following primary total knee arthroplasty: data from the nationwide inpatient sample database. J. Arthroplasty 30, 1710–1715 (2015).
20.
Nichols CI, Vose JG. Clinical outcomes and costs within 90 days of primary or revision total joint arthroplasty. J. Arthroplasty 31(7), 1400–1406 (2016).
21.
Levine BR, Ting N, Della Valle CJ. Use of a barbed suture in the closure of hip and knee arthroplasty wounds. Orthopedics 34(9), e473–e475 (2011).
22.
Sah AP. Is there an advantage to knotless barbed suture in TKA wound closure? A randomized trial in simultaneous bilateral TKAs. Clin. Orthop. Relat. Res. 473(6), 2019–2027 (2015).
23.
Yokoe DS1, Avery TR, Platt R, Huang SS. Reporting surgical site infections following total hip and knee arthroplasty: impact of limiting surveillance to the operative hospital. Clin Infect Dis. 57(9), 1282–1288 (2013).
24.
Austin DC, Keeney BJ, Dempsey BE, Koenig KM. Are barbed sutures associated with 90-day reoperation rates after primary TKA? Clin. Orthop. Relat. Res. 475(11), 2655–2665 (2017).
25.
Williams J, Kester BS, Bosco JA, Slover JD, Iorio R, Schwarzkopf R. The association between hospital length of stay and 90-day readmission risk within a total joint arthroplasty bundled payment initiative. J. Arthroplasty 32(3), 714–718 (2017).
Information & Authors
Information
Published In
Copyright
© 2018 Future Medicine Ltd.
History
Received: 24 May 2018
Accepted: 10 July 2018
Published online: 2 August 2018
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Comparing outcomes between barbed and conventional sutures in patients undergoing knee or hip arthroplasty. (2018) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2018-0047
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Neeku Salehi, P Maxwell Courtney, Chad A Krueger, Eric B Smith, David N Kugelman, Current Concepts on Suture Types in Total Joint Arthroplasty, The Guthrie Clinic Journal of Medicine, 10.3138/guthrie-2024-0028, 77, 1, (50-66), (2025).
- Barbara H Johnson, Sinchana T, Stephen S Johnston, Najmuddin Gunja, Trends in adoption of knotless tissue control devices in robotic surgery, Journal of Comparative Effectiveness Research, 10.57264/cer-2024-0229, 14, 4, (2025).
- Stephen S. Johnston, Najmuddin Gunja, Aakash Jha, Jörg Tomaszewski, Walter Danker, Economic and clinical outcomes of cesarean deliveries with skin closure using 2-octyl cyanoacrylate plus polymer mesh tape versus conventional smooth sutures plus waterproof wound dressings, The Journal of Maternal-Fetal & Neonatal Medicine, 10.1080/14767058.2025.2463390, 38, 1, (2025).
- Pablo Sanz-Ruiz, José Ramón Caeiro-Rey, Juan Carlos Martínez-Pastor, José Luis Martín-Alguacil, Antonio Murcia-Asensio, Jesús Moreta, Consensus document on the management of wound closure in orthopaedic surgery, EFORT Open Reviews, 10.1530/EOR-24-0002, 10, 2, (82-94), (2025).
- Khalid Sarhan, Reem Reda Elmahdi, Rashad G. Mohamed, Ibrahim Serag, Mohamed Abouzid, Barbed sutures versus conventional sutures for wound closure in spine surgeries: a systematic review and meta-analysis, Neurosurgical Review, 10.1007/s10143-024-02909-9, 47, 1, (2024).
- Steven R. Glener, Pious D. Patel, Stephanie N. Serva, Dwight Mitchell Self, Joshua E. Heller, Prospective analysis of STRATAFIX™ symmetric PDS plus suture for fascial closure in spinal surgery: a pilot study, Neurosurgical Review, 10.1007/s10143-024-02671-y, 47, 1, (2024).
- Jana Flener, Brian Chen, Frank Ernst, Aaron Libolt, Najmuddin Gunja, William Barrett, Advanced Multi-Layer Watertight Closure versus Conventional Closure in Total Hip and Knee Replacement Surgery, Pragmatic and Observational Research, 10.2147/POR.S450183, Volume 15, (93-102), (2024).
- Antonio Russo, Michele Centola, Alberto Nicodemo, Alessandro Massè, The Use of Barbed Sutures in Total Hip Arthroplasty: A Systematic Review on Clinical–Surgical Outcomes, Costs, and Complications, Healthcare, 10.3390/healthcare12111063, 12, 11, (1063), (2024).
- Emilio Romanini, Gustavo A. Zanoli, Tiziana Ascione, Giovanni Balato, Andrea Baldini, Emanuela Foglia, Antonio V. Pellegrini, Francesco Verde, Stefano Zaffagnini, Barbed sutures and skin adhesives improve wound closure in hip and knee arthroplasty, Knee Surgery, Sports Traumatology, Arthroscopy, 10.1002/ksa.12055, 32, 2, (303-310), (2024).
- Rajesh N. Maniar, Bharat Mody, Hemant M. Wakankar, Indrajit Sardar, Neeraj Adkar, Rajkumar Natesan, Sameer Ali Paravath, Sanjay Pai, Unmesh S. Mahajan, Expert Consensus on Best Practices for Optimal Wound Closure in Total Knee Arthroplasty: A STRIDE Initiative for Orthopedic Surgeons of India, Indian Journal of Orthopaedics, 10.1007/s43465-023-00922-6, 57, 12, (2066-2072), (2023).