Trends in adoption of knotless tissue control devices in robotic surgery
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Trends in the use and comparative outcomes for barbed and conventional sutures have not been well-reported for robotic surgery. Materials & methods: This retrospective study used hospital discharge data in the US to assess suture use during robotic colorectal surgery (CR), total hysterectomy (TH) and ventral hernia repair (VHR) performed between 1 October 2015 and 30 June 2022. We first examined quarterly trends in use of barbed sutures, (specifically STRATAFIX™ knotless tissue control devices [KTCD]) and then compared clinical and economic outcomes between KTCD and conventional sutures. Outcomes included wound-related complications (infection/wound dehiscence) through 90 days post discharge, operating room (OR) time, hospital costs and 30/60/90 days readmissions. Propensity score weighting was used to address potential confounding in the comparisons of outcomes, performed separately for each procedure. Generalized linear models, accounting for hospital-level clustering, with link functions and error distributions tailored to the empirical distribution of outcomes were used to test for statistically significant differences in outcomes between the KTCD and conventional suture cohorts. Results: We identified 15,875 patients with CR (668 KTCD), 175,963 patients with TH (15,075 KTCD) and 32,469 patients with VHR (6776 KTCD). Over the study period, the proportion of robotic surgeries using KTCD tripled for CR (2.0–6.4%) and TH (2.9–10.4%) and more than doubled for VHR (12.2–25.3%). Compared with conventional sutures, KTCD was associated with significantly shorter OR time for TH (-19.1 min, 95% CI: [-30.2, -8.0]) and VHR (-17.3 min, 95% CI: [-31.4, -3.2]), and was numerically shorter, but did not reach statistical significance for CR (-23.2 min 95% CI: [-48.1 to 1.7]). All other outcomes were similar between the two suture cohorts for all procedures, apart from CR 90-day readmissions, which were lower for the KTCD cohort (-2.8%, 95% CI: [-5.2 to -0.4%]). Conclusion: Adoption of KTCD has grown substantially over the past 6 years. While most clinical and economic outcomes were similar between the two groups, KTCD was associated with lower OR time versus conventional sutures for TH and VHR and lower 90-day readmissions for CR.
Plain language summary
What is this article about?
The use of robotic assistance for surgical procedures has increased dramatically over the last two decades. Concurrent development and innovation of knotless tissue control devices (KTCD; also known as barbed sutures) has taken place and an uptake in the use of such sutures has been observed in robotically assisted procedures.
Researchers have compared various outcomes for barbed and conventional sutures in surgeries where a laparoscopic approach was used, however, to our knowledge, this type of comparative research has not been well-reported for robotic surgeries.
This study uses real-world data to address this important evidence gap from two perspectives. The first perspective examines the temporal trends in the use of KTCD during robotic ventral hernia repair (VHR), total hysterectomy (TH) and colorectal surgery in the US The second perspective compares selected outcomes in these robotic surgeries in which KTCD were used for wound closure as compared with conventional sutures.
What were the results?
KTCD use in robotic VHR, TH and colorectal surgery has grown substantially over the past 6 years. In addition, KTCD was associated with lower operating room time versus conventional sutures for VHR and TH.
What do the results mean?
In addition to the potential cost-savings associated with reductions in the operating room time needed for VHR and TH, these efficiency gains associated with KTCD may increase hospitals’ and surgical centers’ opportunity to serve more patients in any given day.
Background
The use of robotic assistance for surgical procedures has increased dramatically over the last two decades, impacting the standard practice for multiple different specialties – including gynecology, colorectal, urinary and general surgical procedures, among others [1–4]. Assisted suturing has been one of the key potential benefits touted for robotic platforms [5]. Concurrent development and innovation of knotless tissue control devices (KTCD; also known as barbed sutures) has taken place and an uptake in the use of such sutures has been observed in robotically assisted procedures [6].
In general, the design of barbed sutures addresses several important limitations of conventional sutures. The very process of knotting sutures may not only slow the surgeon’s progress, but inherently reduces the overall tensile strength of the suture material across the wound closure and results in naturally higher tension at the knot which can negatively impact healing [7]. Surgeons’ concern about slippage may also lead to over-tightening of their knots, potentially compounding this issue [7,8]. By removing the need for tying knots altogether, barbed sutures offer both greater and more even tensile strength and security across the wound closure, and their use has been associated with improved operating room (OR) efficiency compared with conventional sutures [6,8–11].
The clinical and other benefits of barbed sutures have been evaluated in a wide range of surgery types, including bariatric [12], obstetrics and gynecology [13–15], prostatectomy [16], orthopedics [17] and anastomosis in general surgery [18]. Researchers have also compared various outcomes for barbed and conventional sutures in surgeries where a laparoscopic approach was used, however, to our knowledge, this type of comparative research has not been well-reported for robotic surgeries [7,19–22]. This study addresses this important evidence gap from two perspectives. The first perspective examines the temporal trends in the use of knotless tissue control devices (KTCD, specifically STRATAFIX™ Ethicon, Inc.) during robotic surgeries in the routine practice setting in the US. The second perspective compares selected outcomes in robotic surgeries in which KTCD were used for wound closure as compared with conventional sutures.
Materials & methods
This retrospective, observational cohort study used discharge-level data from the PINC AI™ Healthcare Database (PHD), formerly known as the Premier Healthcare Database. This all-payer database contains data on inpatient and outpatient discharge, healthcare utilization and patient demographics, as well as detailed billing information and data on select characteristics of the over 1000 hospitals across the US that contribute data. This population-based data source represents approximately 25% of annual inpatient discharges in the US. Although federally funded hospitals (e.g., Veterans Affairs) do not contribute to this database, comparisons of the member hospital characteristics (bed size, geographic region, location [urban/rural] and teaching status) from the PHD with those from the American Hospital Association demonstrate a similar distribution [23].
This analysis of the PHD was conducted under an exemption from Institutional Review Board oversight for US-based studies using de-identified healthcare records, as dictated by Title 45 Code of Federal Regulations (45 CFR 46.104(d)(4)(ii)) (https://www.ecfr.gov/current/title-45/subtitle-A/subchapter-A/part-46/subpart-A/section-46.104). As PHD data do not contain direct identifiers of individuals, employers, households or providers, Institutional Review Board approval is not required.
We selected patients from the PHD who were age ≥18 years at the time of an inpatient or outpatient elective surgical admission with a combination of primary and secondary procedure codes indicative of a robotic ventral hernia repair (VHR), total hysterectomy (TH), or colorectal surgery performed between 1 October 2015 and 30 June 2022. The first such admission for each patient was considered the ‘index’ admission. Study patients were also required to have evidence of either STRATAFIX™-branded KTCD (including all varieties of STRATAFIX™: Symmetric PDS™ Plus, Spiral MONOCRYL™ Plus, Spiral PDS™ Plus, Spiral Polypropylene) or conventional (e.g., silk, non-barbed monofilament and braided multifilament) suture use on the day of the index procedure. The hospital in which their surgery occurred must have continued contributing data to the PHD for at least 90 days after their discharge date. As this analysis was designed to specifically examine use of STRATAFIX™-branded KTCD, patients with evidence suggesting that other branded or unbranded barbed sutures were used were excluded. Patients whose index admission resulted from a hospital transfer or who had missing data on sex, multiple procedure types of interest, or incomplete or inaccurate cost data were also excluded.
Analyses were conducted separately for each procedure type, and no comparisons were made between procedure types. Descriptive statistics were used to evaluate quarterly KTCD utilization trends as a proportion of all robotic procedures for the time from the fourth quarter (Q4) 2015 through the second quarter (Q2) 2022.
Inferential statistics were used to compare the occurrence of the following prespecified outcomes in the two treatment cohorts: wound-related complications (a composite measure of surgical site infection and/or wound dehiscence) occurring any time during the index admission through 90 days post discharge, OR time, total hospital costs and all-cause inpatient readmissions at 30, 60, and 90 days post discharge. These outcomes were selected based on their clinical and economic relevance to the use of sutures and availability within the database. The number of inpatient admissions for colorectal surgeries was also sufficient to assess length of stay for those index procedures. To address the fact that patients and treating hospitals in the KTCD and conventional suture cohorts might differ on important characteristics that could influence the outcomes being assessed, patients in the conventional suture cohort were weighted to mimic the patients in the KTCD cohort using average treatment effect on the treated propensity score weighting [24]. In this method the full KTCD cohort is retained as an unweighted sample and the conventional suture cohort is weighted to resemble KTCD. Variables used in the weighting included patient demographics (e.g., age, gender and race), clinical characteristics (i.e., surgical indication, Elixhauser comorbidities), procedural characteristics (e.g., index year and setting of care) and hospital/provider characteristics (e.g., teaching/non-teaching, bed size and surgeon specialty). Weighting was performed individually within each procedure. Generalized linear models, accounting for hospital-level clustering, with link functions and error distributions tailored to the empirical distribution of outcomes were used to test for statistically significant differences in outcomes between the KTCD and conventional suture cohorts.
Results
From an initial population of 358,765 patients with one or more of the three robotic procedures of interest during the study period, 224,307 patients met all selection criteria. Of these patients, 15,875 underwent colorectal procedures (668 with KTCD), 175,963 had a TH (15,075 with KTCD) and 32,469 had a VHR (6776 with KTCD). Patient characteristics, prior to weighting, stratified by suture cohort and procedure are provided in Table 1. Among patients who had colorectal procedures, between-cohort differences were most apparent for payer type, race and ethnicity and surgical indication. Among patients who had total hysterectomies, differences between the two suture cohorts were most apparent in the distributions of race and ethnicity. Among patients who had VHR procedures, patients in the two suture cohorts differed primarily in terms of race, ethnicity, marital status and payer type. Provider and hospital characteristics are described in Supplementary Table 1. Within each procedure type there were distinct differences between the two suture cohorts for most of the characteristics examined including geographic location, hospital size and procedure volume, teaching status and specialty of the provider who performed the index procedure.
| Colorectal procedures | Total hysterectomy | Ventral hernia repair | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Smooth suture | KTCD | Smooth suture | KTCD | Smooth suture | KTCD | |||||||
| n | % | n | % | n | % | n | % | n | % | n | % | |
| All | 15,207 | 100.0 | 668 | 100.0 | 160,888 | 100.0 | 15,075 | 100.0 | 25,693 | 100.0 | 6776 | 100.0 |
| Age category (years, range) | ||||||||||||
| 18–34 | 503 | 3.3 | 18 | 2.7 | 13,160 | 8.2 | 1156 | 7.7 | 1745 | 6.8 | 527 | 7.8 |
| 35–44 | 1096 | 7.2 | 54 | 8.1 | 49,208 | 30.6 | 4593 | 30.5 | 3681 | 14.3 | 930 | 13.7 |
| 45–54 | 2657 | 17.5 | 122 | 18.3 | 48,212 | 30.0 | 4682 | 31.1 | 5365 | 20.9 | 1480 | 21.8 |
| 55–64 | 4076 | 26.8 | 188 | 28.1 | 25,567 | 15.9 | 2412 | 16.0 | 6761 | 26.3 | 1778 | 26.2 |
| 65–74 | 4363 | 28.7 | 185 | 27.7 | 18,276 | 11.4 | 1682 | 11.2 | 5654 | 22.0 | 1475 | 21.8 |
| 75+ | 2512 | 16.5 | 101 | 15.1 | 6465 | 4.0 | 550 | 3.6 | 2487 | 9.7 | 586 | 8.6 |
| Mean | 61.71 | 61.20 | 49.85 | 49.81 | 56.68 | 56.13 | ||||||
| SD | 13.25 | 12.79 | 12.53 | 12.25 | 13.92 | 13.88 | ||||||
| Median | 63.00 | 62.00 | 47.00 | 47.00 | 58.00 | 57.00 | ||||||
| Gender | ||||||||||||
| Female | 7873 | 51.8 | 357 | 53.4 | 160,888 | 100.0 | 15,075 | 100.0 | 14,334 | 55.8 | 3612 | 53.3 |
| Male | 7334 | 48.2 | 311 | 46.6 | 0 | 0.0 | 0 | 0.0 | 11,359 | 44.2 | 3164 | 46.7 |
| Race | ||||||||||||
| African–American | 1270 | 8.4 | 72 | 10.8 | 17,279 | 10.7 | 2242 | 14.9 | 2376 | 9.2 | 759 | 11.2 |
| Asian | 291 | 1.9 | 6 | 0.9 | 2778 | 1.7 | 322 | 2.1 | 209 | 0.8 | 31 | 0.5 |
| Other | 938 | 6.2 | 21 | 3.1 | 10,146 | 6.3 | 797 | 5.3 | 1472 | 5.7 | 246 | 3.6 |
| Unknown | 291 | 1.9 | 6 | 0.9 | 3722 | 2.3 | 335 | 2.2 | 467 | 1.8 | 82 | 1.2 |
| White | 12,417 | 81.7 | 563 | 84.3 | 126,963 | 78.9 | 11,379 | 75.5 | 21,169 | 82.4 | 5658 | 83.5 |
| Ethnicity | ||||||||||||
| Hispanic | 837 | 5.5 | 110 | 16.5 | 12,870 | 8.0 | 2806 | 18.6 | 2151 | 8.4 | 786 | 11.6 |
| Non-Hispanic | 11,734 | 77.2 | 505 | 75.6 | 116,803 | 72.6 | 10,640 | 70.6 | 18,210 | 70.9 | 5706 | 84.2 |
| Unknown | 2636 | 17.3 | 53 | 7.9 | 31,215 | 19.4 | 1629 | 10.8 | 5332 | 20.8 | 284 | 4.2 |
| Marital status | ||||||||||||
| Married | 8415 | 55.3 | 392 | 58.7 | 96,028 | 59.7 | 9028 | 59.9 | 14,772 | 57.5 | 4135 | 61.0 |
| Other | 1,110 | 7.3 | 22 | 3.3 | 6157 | 3.8 | 336 | 2.2 | 1025 | 4.0 | 128 | 1.9 |
| Single | 5682 | 37.4 | 254 | 38.0 | 58,703 | 36.5 | 5711 | 37.9 | 9896 | 38.5 | 2513 | 37.1 |
| Payor category | ||||||||||||
| Commercial | 6624 | 43.6 | 317 | 47.5 | 102,756 | 63.9 | 9521 | 63.2 | 12,016 | 46.8 | 3396 | 50.1 |
| Medicaid | 1076 | 7.1 | 48 | 7.2 | 21,445 | 13.3 | 1926 | 12.8 | 3279 | 12.8 | 692 | 10.2 |
| Medicare | 6880 | 45.2 | 284 | 42.5 | 27,581 | 17.1 | 2573 | 17.1 | 8927 | 34.7 | 2276 | 33.6 |
| Other | 627 | 4.1 | 19 | 2.8 | 9106 | 5.7 | 1055 | 7.0 | 1471 | 5.7 | 412 | 6.1 |
| Surgical Indication | ||||||||||||
| Cancer | 6715 | 44.2 | 254 | 38.0 | 30,343 | 18.9 | 2698 | 17.9 | 0 | 0.0 | 0 | 0.0 |
| Non-Cancer | 8492 | 55.8 | 414 | 62.0 | 130,545 | 81.1 | 12,377 | 82.1 | 25,693 | 100.0 | 6776 | 100.0 |
KTCD: Knotless tissue control device; N: Number; SD: Standard deviation.
The relative utilization of KTCD, quantified as a percentage of all procedures of each type in every calendar quarter during the study period is presented in Figures 1A through 1C. As illustrated in Figure 1A & B, KTCD utilization essentially tripled from Q4 2015 through Q2 2022 for both robotic colorectal procedures (2.0–6.4%) and robotic hysterectomies (2.9–10.4%), although utilization at the beginning of this interval was low. KTCD were more commonly used in robotic VHRs in 2015 than in the other two procedures of interest. That said, KTCD utilization still more than doubled in this procedure by the end of Q2 2022 (12.2–25.3%).
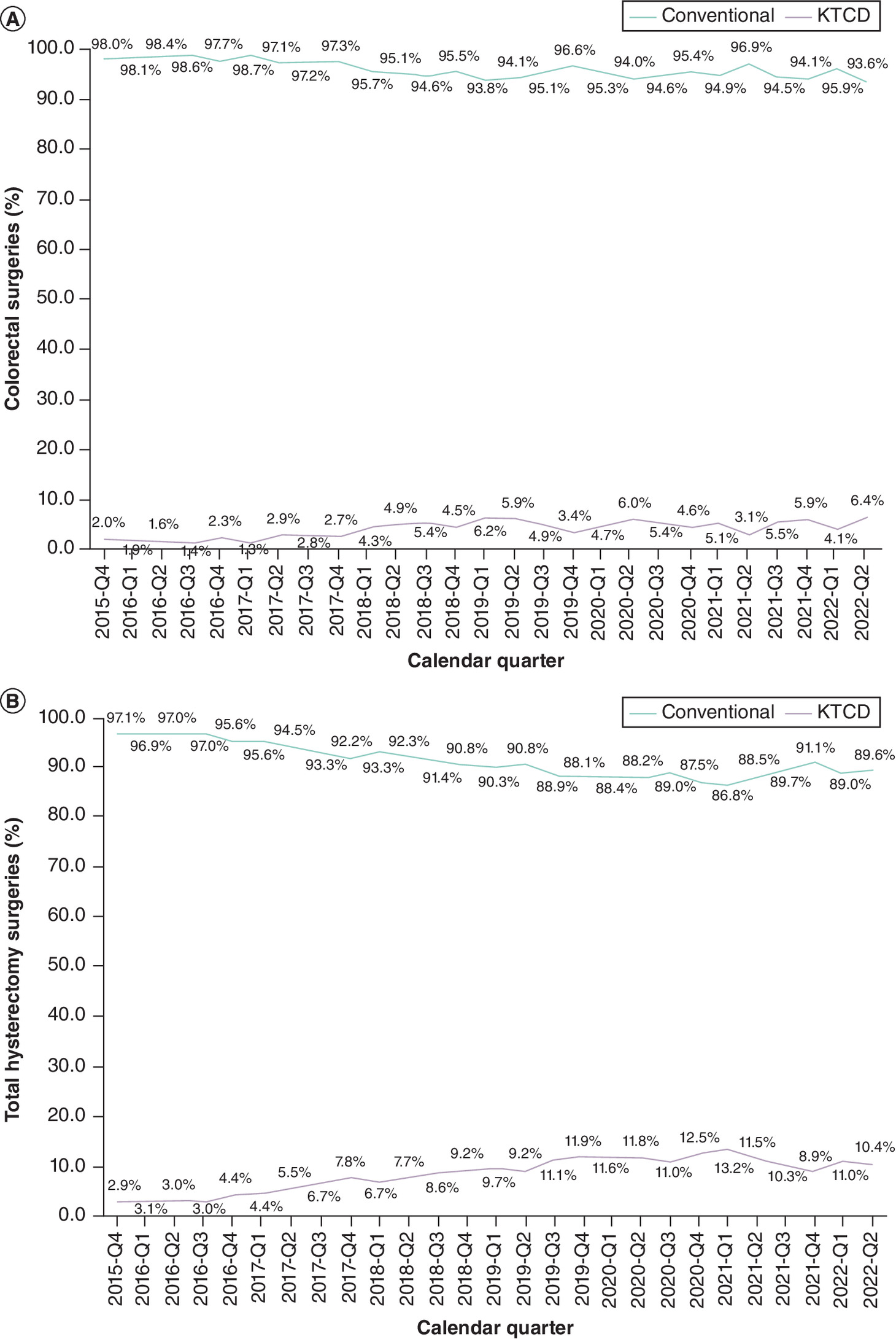
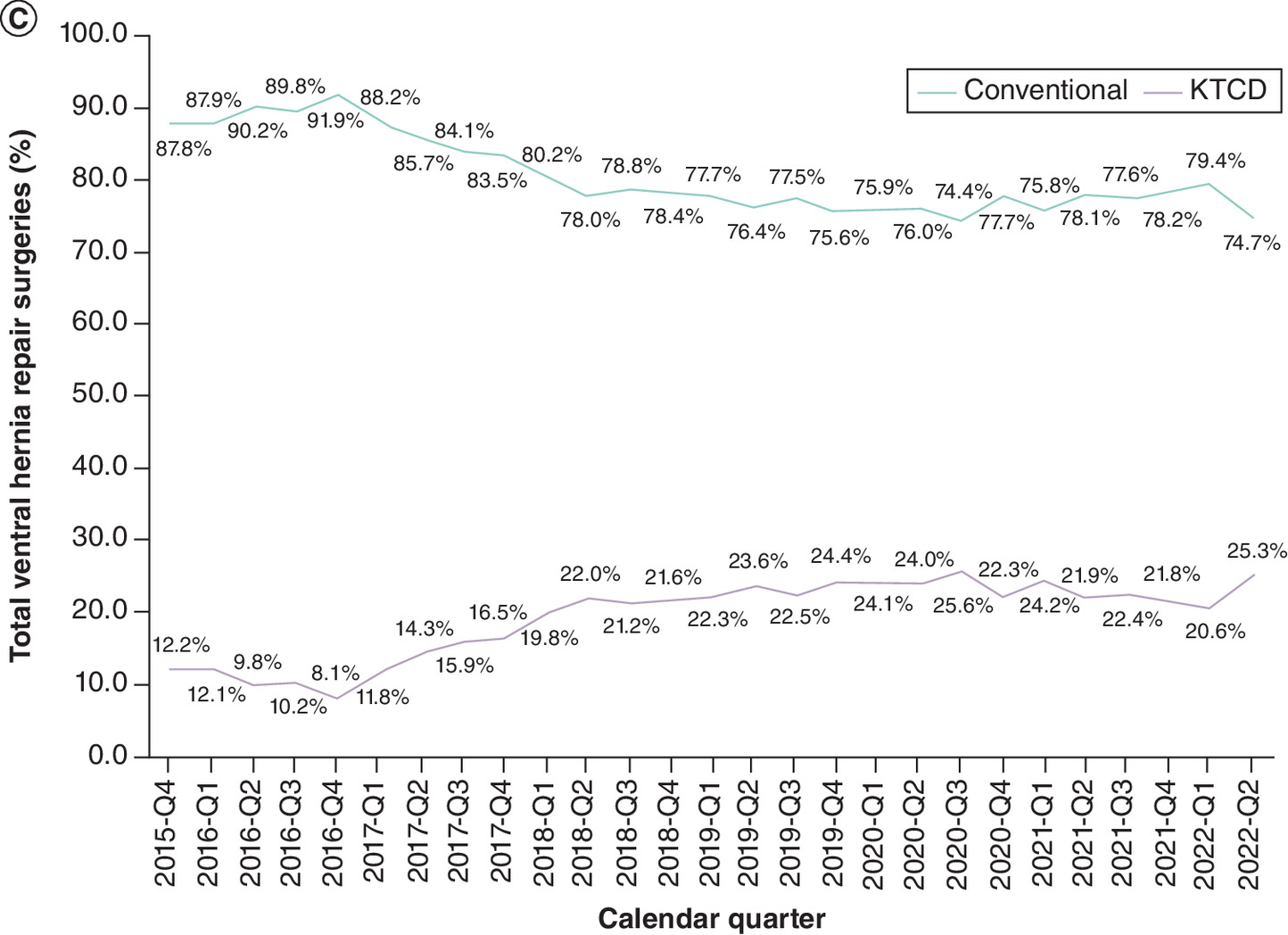
Figure 1. Temporal trends in use of knotless tissue control device in robotic procedures (2015–2022).
(A) Temporal trends in use of KTCD in robotic colorectal procedures, 2015–2022. (B) Temporal trends in use of KTCD in robotic total hysterectomy procedures, 2015–2022. (C) Temporal trends in use of KTCD in robotic ventral hernia repair procedures, 2015–2022.
KTCD: Knotless tissue control device.
Before comparing outcomes between suture cohorts within each procedure type, propensity score weighting was conducted to adjust for between-cohort differences in nearly 60 baseline hospital, provider and patient characteristics. After weighting, the cohorts were well-balanced within each procedure, with post-weighting standardized mean differences for all covariates of ≤0.10 (Supplementary Figures 1A through 1C). Compared with conventional sutures, KTCD was associated with significantly shorter OR time for total hysterectomies (-19.1 min, 95% CI: [-30.2, -8.0]) and VHRs (-17.3 min, 95% CI: [-31.4, -3.2]). OR time was also shorter for colorectal procedures though it did not reach statistical significance (-23.2 min 95% CI: [-48.1 to 1.7]). The incidence of wound-related complications and total hospital costs were similar between the two suture cohorts for each procedure (Table 2), and the same was true for length of stay for colorectal surgeries. All-cause readmissions within 30, 60 and 90 days post discharge were lower for the KTCD cohort in all three procedures, but only reached statistical significance in colorectal 90-day readmissions (-2.8%, 95% CI: [-5.2 to -0.4%]).
| Outcome | Conventional suture | KTCD | Mean incremental difference of KTCD vs conventional suture (95% CI) | p-value |
|---|---|---|---|---|
| Colorectal procedures | ||||
| ESS = 6837 | ESS = 668 | |||
| Operating room surgical time (minutes) | 294.5 | 271.3 | -23.2 (-48.1 to 1.7) | 0.068 |
| Length of stay (days) | 4.9 | 4.6 | -0.30 (-0.79 to 0.20) | 0.239 |
| Total hospital costs† | $25,034 | $24,898 | -$136 (-3,869 to 3,597) | 0.943 |
| Incidence proportion of wound-related complications‡ | 5.6% | 5.7% | -0.1% (-1.5% to 1.8%) | 0.886 |
| Incidence proportion of 30-days all-cause readmissions | 10.5% | 9.0% | -1.5% (-3.3% to 0.4%) | 0.120 |
| Incidence proportion of 60-days all-cause readmissions | 13.2% | 11.4% | -1.8% (-4.0% to 0.4%) | 0.108 |
| Incidence proportion of 90-days all-cause readmissions | 15.6% | 12.9% | -2.8% (-5.2% to -0.4%) | 0.025 |
| Total hysterectomy | ||||
| ESS = 100,924 | ESS = 15,075 | |||
| Operating room surgical time (minutes) | 174.4 | 155.3 | -19.1 (-30.2 to -8.0) | 0.001 |
| Total hospital costs† | $11,320 | $10,734 | -$586 (-1,934 to 762) | 0.394 |
| Incidence proportion of wound-related complications‡ | 1.5% | 1.4% | 0.0% (-0.3% to 0.3%) | 0.899 |
| Incidence proportion of 30-days all-cause readmissions | 2.3% | 2.3% | 0.0% (-0.30% to 0.40%) | 0.786 |
| Incidence proportion of 60-days all-cause readmissions | 2.7% | 2.5% | -0.2% (-0.57% to 0.21%) | 0.367 |
| Incidence proportion of 90-days all-cause readmissions | 3.1% | 2.8% | -0.2% (-0.70% to 0.22%) | 0.316 |
| Ventral hernia repair | ||||
| ESS = 15,003 | ESS = 6776 | |||
| Operating room surgical time (in minutes) | 171.6 | 154.3 | -17.3 (-31.4 to -3.2) | 0.016 |
| Total hospital costs† | $10,702 | $10,708 | $5 (-1,100 to 1,110) | 0.992 |
| Incidence proportion of wound-related complications‡ | 0.94% | 0.90% | 0.0% (-0.34% to 0.27%) | 0.818 |
| Incidence proportion of 30-days all-cause readmissions | 3.0% | 2.6% | -0.4% (-0.90 to 0.14) | 0.149 |
| Incidence proportion of 60-days all-cause readmissions | 3.6% | 3.3% | -0.3% (-0.89 to 0.24) | 0.256 |
| Incidence proportion of 90-days all-cause readmissions | 4.1% | 3.8% | -0.4% (-1.04 to 0.27) | 0.251 |
Bold values indicate a significant finding.
†
Constant 2022 US dollars.
‡
Composite measure of surgical site infection and wound dehiscence.
CI: Confidence interval; ESS: Effect sample size after weighting; KTCD: Knotless tissue control device.
Discussion
Barbed sutures offer a variety of clinical and logistical advantages over conventional sutures, and their use and associated outcomes have been documented for a diverse set of surgical procedures, including those using a laparoscopic approach [1–4]. This analysis of data from a nationwide all-payer database provides important insights on the use of KTCD in the robotic surgical approach. With large sample sizes and multiyear follow-up, we documented substantially increasing use of KTCD in three common robotic surgery procedures (colorectal procedures, TH, VHR), and with well-balanced suture cohorts, we documented a significant OR time savings for KTCD over conventional sutures.
Although the utilization level of KTCD in late 2015 differed across the three robotic surgery procedures studied, KTCD use increased twofold to threefold by mid-2022. This trend suggests a growing acceptance and confidence in KTCD, although KTCD is still used in a minority of these procedures. That said, it is likely that KTCD use will continue expanding as the preferences of surgeons and surgical facilities and departments continue to shift. Additional comparative real-world research may play an important role in shaping the speed and extent to which KTCD and other alternatives to conventional sutures shift the surgical landscape.
In a 2023 review paper, Gowri et al. [6] provide an extensive summary and review of the published literature on the evolution and use of barbed sutures in various medical domains (e.g., emergency room, general surgery, obstetrics/gynecology, orthopedics, plastic and cosmetic surgery), and of outcomes of particular interest associated with the use of this type of suture. Interestingly, this paper does not report on the use of barbed sutures in general or KTCD in particular for robotic-assisted procedures, which highlights the evidence gap that our study was designed to begin narrowing.
The Gowri review notes that the published literature documents a variety of clinical (e.g., lower incidence of wound complications) and logistical (e.g., surgical incision closure time, OR time) advantages for barbed sutures, and also mentions that previous meta-analyses have shown these sutures to be cost-effective even when complication rates are similar to those for conventional sutures [6]. Although our study did not show statistically significant differences between KTCD and conventional sutures in terms of wound complication incidence, length of stay for the index hospitalization (assessed for colorectal surgeries only), or total cost, we did find a similar OR time advantage as reported in the Gowri review. In addition, in colorectal surgery we saw a statistically significant difference in 90-day readmissions with a preceding favorable trend at 30 and 60 days. As similar trends were not seen in the TH or VHR cohorts, these findings merit further exploration but could also be explained by the low statistical power to detect a statistically significant difference in event rates with 3 or 6% expected rate and relatively small effect sizes.
OR times were shorter for all three procedures examined when performed with KTCD versus conventional sutures, reaching statistical significance in both total hysterectomies and VHRs. This positive finding for KTCD use in the setting of robotic surgery concurs with results from previous studies demonstrating that KTCD use is associated with significantly shorter OR times compared with conventional sutures [11,12,25,26]. To put this finding into context, published data from acute care hospitals in California suggests that, based on the 2014 fiscal year, the mean per-minute cost of OR time was $36 to $37 with $20 to $21 covering direct costs and the remainder attributed to wages, benefits and surgical supplies [27]. While the objectives of this study did not include a cost–effectiveness component, if we were to apply the $37 per min cost to the estimated mean time savings of 19.1 min for total hysterectomies and 17.3 min for VHRs performed with KTCD it would suggest a rough cost savings estimate of approximately $700 and $640 per procedure, respectively. These are likely very conservative estimates, however, given that healthcare costs have risen in each of the 9 years since 2014. A more recent review paper reports that per-minute OR costs may reach $113 [28]. With that figure, the rough cost savings estimate would be $2158 and $1955, respectively. In addition to the potential cost-savings associated with reductions in the OR time needed for each procedure, these efficiency gains associated with KTCD may increase hospitals’ and surgical centers’ opportunity to serve more patients in any given day.
As with all research, this study has limitations that provide important context for interpretation of the results. This study was designed to specifically evaluate the use of STRATAFIX™, and therefore does not reflect the use of all barbed sutures in robotic-assisted surgeries. We acknowledge that the source data may be incomplete or inaccurate in some instances and have attempted to mitigate that potential issue with the extensive logic and data quality checks conducted prior to analyzing the data. The identification of suture cohort was based upon the hospital charge master, which may be subject to misclassification if the wrong product was entered in the charge master. Although we used a rigorous statistical methodology to balance the cohorts on measurable characteristics, there is no single data source (aside from a randomized controlled trial) that can rule out the potential for residual confounding from unmeasured factors such as the skill of the surgeon and their supporting clinical team, the complexity of a patient’s anatomy, and lifestyle factors (e.g., nutrition-related factors, smoking and alcohol consumption) which play an important role in wound healing and may affect the study outcomes. It is important to note that hospital readmissions which do not occur within the same hospital as the index hospital admission are not captured in the PHD and therefore may be underestimated. Lastly, the study results will not necessarily be generalizable to all hospitals in the US.
Conclusion
This study extends the existing knowledge base by providing data and insights regarding temporal trends in the use of KTCD in three common types of robotic procedures (colorectal surgeries, total hysterectomies and VHRs) in the US, and by comparing important clinical, logistical and economic outcomes associated with the use of either KTCD or conventional sutures. This study documented increasing use of KTCD in these robotic procedures over time and procedure-specific benefits including shorter OR times for both total hysterectomies and VHRs without additional costs.
Summary points
•
While several published studies have compared barbed versus conventional sutures for wound closure using a laparoscopic surgical approach, there is an evidence gap regarding the use of knotless tissue control devices (KTCD) versus conventional sutures for wound closure in robotic surgery.
•
This retrospective, observational cohort study used 2015–2022 discharge-level data from the PINC AI™ Healthcare Database.
•
Study subjects were ≥18 years old and had a surgical admission for robotic ventral hernia repair (VHR), total hysterectomy (TH), or colorectal surgery (CR) between 1 October 2015 and 30 June 2022. Quarterly KTCD utilization trends as a proportion of all robotic procedures between Q4 2015 and Q2 2022 were measured.
•
Outcomes included in-hospital through 90-day post discharge wound-related complications (composite measure of surgical site infection and wound dehiscence), total hospital costs, operating room time and 30, 60 and 90 days all-cause inpatient readmissions.
•
Generalized linear models, accounting for hospital-level clustering, with link functions and error distributions tailored to the empirical distribution of outcomes were used to test for statistically significant differences in outcomes between the KTCD and conventional suture cohorts.
•
Before comparing outcomes between suture cohorts within each procedure type, propensity score weighting was conducted to adjust for between-cohort differences in nearly 60 baseline hospitals, providers and patient characteristics. After weighting, the cohorts were well-balanced within each procedure, with post weighting standardized mean differences for all covariates of ≤0.10.
•
We identified 15,875 patients with CR (668 KTCD), 175,963 patients with TH (15,075 KTCD) and 32,469 patients with VHR (6776 KTCD). Over the study period, the proportion of robotic surgeries using KTCD tripled for CR (2.0–6.4%) and TH (2.9–10.4%) and more than doubled for VHR (12.2–25.3%).
•
Compared with conventional sutures, KTCD was associated with significantly shorter OR time for TH and VHR and lower 90-day readmissions for CR.
•
In addition to the potential cost-savings associated with reductions in the OR time needed for VHR and TH, these efficiency gains associated with KTCD may increase hospitals’ and surgical centers’ opportunity to serve more patients in any given day.
Author contributions
The corresponding author attests that all listed authors meet ICMJE authorship criteria and that no others meeting the criteria have been omitted. All authors have read and approved the manuscript. BH Johnson: Conceptualization, formal analysis, investigation, methodology and writing – review and editing. SS Johnston: Conceptualization, formal analysis, investigation, methodology and writing – review and editing. Sinchana T: Formal analysis, investigation, methodology and writing – review and editing. N Gunja: Conceptualization, methodology, investigation and writing – review and editing.
Acknowledgments
The authors thank S Wade (Wade Outcomes Research and Consulting, UT, USA) for medical writing assistance.
Financial disclosure
This study was funded by Johnson & Johnson. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Competing interests disclosure
BH Johnson, SS Johnston and N Gunja are employees and stockholders of Johnson & Johnson. Sinchana T is employed by Mu Sigma; Mu Sigma was paid by Johnson & Johnson for data programming services. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing disclosure
Medical writing support was provided by S Wade of Wade Outcomes Research and Consulting and was funded by Johnson & Johnson.
Ethical conduct of research
This analysis of the PHD was conducted under an exemption from Institutional Review Board oversight for US-based studies using de-identified healthcare records, as dictated by Title 45 Code of Federal Regulations.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Jeong IG, Khandwala YS, Kim JH et al. Association of robotic-assisted vs laparoscopic radical nephrectomy with perioperative outcomes and health care costs, 2003 to 2015. J. Am. Med. Assoc. 318(16), 1561–1568 (2017).
2.
Mederos MA, Jacob RL, Ward R et al. Trends in robot-assisted procedures for general surgery in the Veterans Health Administration. J. Surg. Res. 279, 788–795 (2022).
• This retrospective cohort study illustrates the increasing trend of robotic assistance in common surgical procedures among patients in the Veterans Health Administration.
3.
Bankar GR, Keoliya A. Robot-assisted surgery in gynecology. Cureus 14(9), e29190 (2022).
4.
Ravendran K, Abiola E, Balagumar K et al. A review of robotic surgery in colorectal surgery. Cureus 15(4), e37337 (2023).
5.
Kaan HL, Ho KY. Endoscopic robotic suturing: the way forward. Saudi J. Gastroenterol. 25(5), 272–276 (2019).
6.
Gowri KN, King MW. A review of barbed sutures—evolution, applications and clinical significance. Bioengineering (Basel) 10(4), 419 (2023).
•• Discusses how barbed sutures evolved from their start in the 1960’s to their increasing role in surgical procedures today.
7.
Greenberg JA, Goldman RH. Barbed suture: a review of the technology and clinical uses in obstetrics and gynecology. Rev. Obstet. Gynecol. 6(3–4), 107–115 (2013).
8.
Stone IK, von Fraunhofer JA, Masterson BJ. The biomechanical effects of tight suture closure upon fascia. Surg. Gynecol. Obstet. 163(5), 448–452 (1986).
9.
Lee S, Kee T, Jung MY, Yoon PW. A comparison of barbed continuous suture versus conventional interrupted suture for fascial closure in total hip arthroplasty. Sci. Rep. 12, 3942 (2022).
• Comparison between barbed and conventional sutures.
10.
Wang W, Yan S, Liu F et al. A symmetric anchor designed barbed suture versus conventional interrupted sutures in total knee arthroplasty: a multicenter, randomized controlled trial. J. Orthop. Surg. (Hong Kong) 28(3), 2309499020965681 (2020).
11.
Johnston SS, Chen BPH, Tommaselli GA, Jain S, Pracyk JB. Barbed and conventional sutures in spinal surgery patients: an economic and clinical outcomes comparison. J. Wound Care 29(Suppl. 5A), S9–S20 (2020).
• Comparison between barbed and conventional sutures.
12.
Lin Y, Long Y, Lai S et al. The effectiveness and safety of barbed sutures in the bariatric surgery: a systematic review and meta-analysis. Obes. Surg. 29(6), 1756–1764 (2019).
13.
Peleg D, Ahmad RS, Warsof SL, Marcus-Braun N, Sciaky-Tamir Y, Ben Shachar I. A randomized clinical trial of knotless barbed suture vs conventional suture for closure of the uterine incision at cesarean delivery. Am. J. Obstet. Gynecol. 218(3), 343.e1–343.e7 (2018).
• Comparison between barbed and conventional sutures.
14.
Karacan T, Ozyurek E, Usta T et al. Comparison of barbed unidirectional suture with figure-of-eight standard sutures in vaginal cuff closure in total laparoscopic hysterectomy. J. Obstet. Gynaecol. 38(6), 842–847 (2018).
• Comparison between barbed and conventional sutures.
15.
Zhou Y, Guthrie G, Chuang A, Faro JP, Ali V. Unidirectional barbed suture versus interrupted vicryl suture in vaginal cuff healing during robotic-assisted laparoscopic hysterectomy. J. Robotic Surg. 8(3), 201–205 (2014).
•• Comparison between barbed and conventional sutures in robotic-assisted surgery.
16.
Lin YF, Lai SK, Liu QY et al. Efficacy and safety of barbed suture in minimally invasive radical prostatectomy: a systematic review and meta-analysis. Kaohsiung J. Med. Sci. 33(3), 107–115 (2017).
17.
Sundaram K, Piuzzi NS, Klika AK et al. Barbed sutures reduce arthrotomy closure duration and suture utilisation compared to interrupted conventional sutures for primary total hip arthroplasty: a randomised controlled trial. Hip Int. 31(5), 582–588 (2021).
18.
Manigrasso M, Velotti N, Calculli F et al. Barbed suture and gastrointestinal surgery. A retrospective analysis. Open Med. (War) 14, 503–508 (2019).
19.
Paul MD. Bidirectional barbed sutures for wound closure: evolution and applications. J. Am. Col. Certif. Wound Spec. 1(2), 51–57 (2009).
20.
Giampaolino P, De Rosa N, Tommaselli GA et al. Comparison of bidirectional barbed suture Stratafix and conventional suture with intracorporeal knots in laparoscopic myomectomy by office transvaginal hydrolaparoscopic follow-up: a preliminary report. Eur. J. Obstet. Gynecol. Reprod. Biol. 195, 146–150 (2015).
21.
Greenberg JA, Einarsson JI. The use of bidirectional barbed suture in laparoscopic myomectomy and total laparoscopic hysterectomy. J. Minim. Invasive Gynecol. 15(5), 621–623 (2008).
22.
Round KJ, Yost CC, Rosen JL et al. Feasibility of robotic mitral valve repair using barbed nonabsorbable sutures: a preliminary single-center experience. Innovations 18(3), 254–261 (2023).
23.
PINC AI™ Applied Sciences, Premier Inc. PINC AI™ Healthcare Database: data that informs and performs (White Paper). (2023). Available at: https://offers.premierinc.com/rs/381-NBB-525/images/Premier-Healthcare-DatabaseWhitepaper-Final.pdf
24.
Austin PC. An introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivariate Behav. Res. 46(3), 399–424 (2011).
25.
Nawrocki JG, Nonnenmann H, Mooney M, Sutton N, Schmitz ND. A high-strength, absorbable, antibacterial knotless tissue control device for fascial closure. Curr. Obstet. Gynecol. Rep. 6(2), 175–181 (2017).
26.
Sutton N, Schmitz ND, Johnston SS. Comparing outcomes between barbed and conventional sutures in patients undergoing knee or hip arthroplasty. J. Comp. Eff. Res. 7(10), 975–987 (2018).
• Comparison between barbed and conventional sutures.
27.
Childers CP, Maggard-Gibbons M. Understanding costs of care in the operating room. JAMA Surg. 153(4), e176233 (2018).
28.
Christou CD, Athanasiadou EC, Tooulias AI, Tzamalis A, Tsoulfas G. The process of estimating the cost of surgery: providing a practical framework for surgeons. Int. J. Health Plann. Manage 37(4), 1926–1940 (2022).
Information & Authors
Information
Published In
Copyright
© 2025 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 6 December 2024
Accepted: 7 February 2025
Published online: 17 March 2025
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Trends in adoption of knotless tissue control devices in robotic surgery. (2025) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2024-0229
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Luis Arias-Espinosa, Ethan Shyu, Jorge Humberto Rodriguez-Quintero, Xavier Pereira, Gustavo Romero-Velez, Li-Ching Huang, Athanasios Sevdalis, Ruben Salas, Tanuja Damani, Flavio Malcher, Barbed sutures in ventral hernia repair: A propensity-matched analysis of the Abdominal Core Health Quality Collaborative database, Surgery, 10.1016/j.surg.2025.109715, 188, (109715), (2025).
- Renata Pajtak, Krinal Mori, Small Bowel Obstructions Caused by Barbed Sutures in Robotic Surgery: A Systematic Review, Reproductive Medicine, 10.3390/reprodmed6020011, 6, 2, (11), (2025).