Pharmacoeconomic study comparing carbetocin with oxytocin for the prevention of hemorrhage following cesarean delivery in Lima, Peru
Abstract
Postpartum hemorrhage is one of the main causes of maternal death. Oxytocin has traditionally been used to prevent postpartum hemorrhage. Aim: To compare oxytocin with carbetocin, a long-acting analog of oxytocin, for prevention of uterine hemorrhage after cesarean delivery. Materials & methods: Clinical data were retrieved from the 2012 Cochrane meta-analysis “Carbetocin for preventing postpartum hemorrhage”. A decision tree was constructed. The direct costs were those of medications from the Peruvian official price list (DIGEMID). Costs associated with additional oxytocic drugs, blood transfusions, postpartum hemorrhage kits and hysterectomy were obtained from Hospital Nacional Edgardo Rebagliati Martins. The perspective of the study was that of the payer. The time horizon for calculating quality-adjusted life years (QALYs) was 1 year (2015). Results: Patients who received carbetocin required fewer additional uterotonic agents, had fewer hemorrhages and received fewer blood transfusions. Therefore, the costs associated with these interventions were lower. The incremental cost–effectiveness ratio was S/. 49,918 per QALY gained, which is lower than the threshold we estimated for Peru. Conclusion: Carbetocin is more cost-effective than oxytocin for prevention of uterine hemorrhage after cesarean delivery.
Postpartum hemorrhage is one of the main causes of maternal mortality in both developed and developing countries. According to WHO, approximately 800 women per-day die of complications associated with pregnancy or childbirth throughout the world. Similarly, severe postpartum hemorrhage is reported in around 11% of livebirths [1].
In 2015, a total of 414 maternal deaths were reported in Peru; of these, approximately 42% were due to hemorrhage [2]. During 2014, The Peruvian National Health System (ESSALUD) recorded 49 maternal deaths, that is, 11% of all maternal deaths in the country. In the ESSALUD, uterine hemorrhage is the third cause of maternal death, occurring in 10% of all births (4% for vaginal delivery and 6% for cesarean delivery) [3].
The risk of postpartum hemorrhage is much greater in cesarean delivery, especially in developing countries, where most operations are performed as emergency procedures [4]. In most cases, excessive bleeding during or after childbirth is caused by uterine atony [5]. Women are also exposed to the risks arising from massive blood transfusions and radical surgical procedures such as hysterectomy [6].
Several systematic reviews have shown that prophylaxis with uterotonic agents significantly reduces the risk of postpartum hemorrhage [7]. The most commonly studied and widely used drug for this purpose is oxytocin; in fact, the WHO recommends oxytocin for management of the third stage of labor [8]. Pharmacological management of postpartum hemorrhage has been studied for several years, and one of the options considered is carbetocin, an oxytocin agonist. Carbetocin is a long-acting synthetic analog of oxytocin with a half-life of 40 min. After 2 min of intravenous administration, it can induce tetanic uterine contractions that last for 6 min [9,10].
A 2004 study found that 100 μg of intramuscular carbetocin was as effective as 10 units of oxytocin and reduced the need for uterotonic interventions [11]. Since then, there have been some clinical studies comparing the effectiveness of carbetocin and oxitocyn in preventing postpartum hemorrhage [12,13–15].
In 2012, data from these studies were pooled to determine a general effect of treatment in a meta-analysis with the aim of knowing whether carbetocin was as efficacious as conventional uterotonic agents for the prevention of postpartum hemorrhage (PPH). A systematic review of the literature on this field and a meta-analysis were performed to evaluate the efficacy and safety profile of carbetocin for prevention of PPH. Current evidence shows that compared with oxytocin, carbetocin significantly reduces the need for additional uterotonic agents and uterine massage in women undergoing cesarean delivery [16].
Once the efficacy and safety profile of an alternative has been demonstrated, efficiency must be assessed in terms of costs and benefits in order to optimize the use of healthcare resources and access to more efficient therapy.
In 2006 in Mexico, Del Angel-García et al. [17] performed the first comparison of the cost–effectiveness of carbetocin and oxytocin for prevention of bleeding after cesarean delivery. Their results showed that the mean cost per woman was significantly lower with carbetocin than with oxytocin. The study was only published as a summary and data are missing from the analysis.
Given the paucity of data on the cost–effectiveness of carbetocin, further research is necessary to address this important question, which is the subject of the present analysis.
The term quality-adjusted life year (QALY) was first used by Zeckhauser and Shepard in 1976 as a measure of health outcomes that combined duration and quality of life. A QALY is a unit of measure of an individual's preferences with respect to his/her quality of life after a healthcare intervention combined with the years of life gained with respect to a specific state of health. Therefore, QALYs are highly valued as a basic component in the evaluation of costs of healthcare interventions when taking decisions. QALYs have made it possible to resolve the lack of comparability of results when evaluating the usefulness of different healthcare programs in different healthcare areas [18]. The incremental cost–effectiveness ratio (ICER) considers the increased cost of gaining a QALY after the introduction of a new therapy or healthcare technology compared with the previous one. Therefore, it provides the cost per extra unit of the results of one healthcare strategy compared with another. The incremental cost–effectiveness threshold depends on the country where the study is performed. This information is not available for Peru. The WHO recognizes that a healthcare intervention is cost-effective if the cost per QALY is less than 3× gross domestic product (GDP) per capita. Since the GDP for the year 2015 in Peru was US$12,638 (World Bank), a cost-effective intervention would be to consider the gain of a QALY by comparing two alternatives of less than US$37,914, (S/. 132,699). The threshold defined for Colombia and Chile is 1× GDP per capita, although it must be remembered that the GDP per capita in these countries is greater than in Peru.
The objective of the present study was to compare the cost–effectiveness of carbetocin with that of oxytocin for the prevention of PPH after cesarean delivery by evaluating the results obtained from the literature and those obtained at Hospital Nacional Edgardo Rebagliati Martins, Lima, Peru during the year 2015.
Materials & methods
We compared the alternatives evaluated in the Cochrane meta-analysis “Carbetocin for preventing postpartum haemorrhage” [16].
The clinical results were obtained from the studies in the meta-analysis that compared the use of carbetocin with oxytocin for the prevention of uterine hemorrhage after cesarean delivery (The Cochrane Library, 2012) and from the other bibliographic references of the present report [19,20].
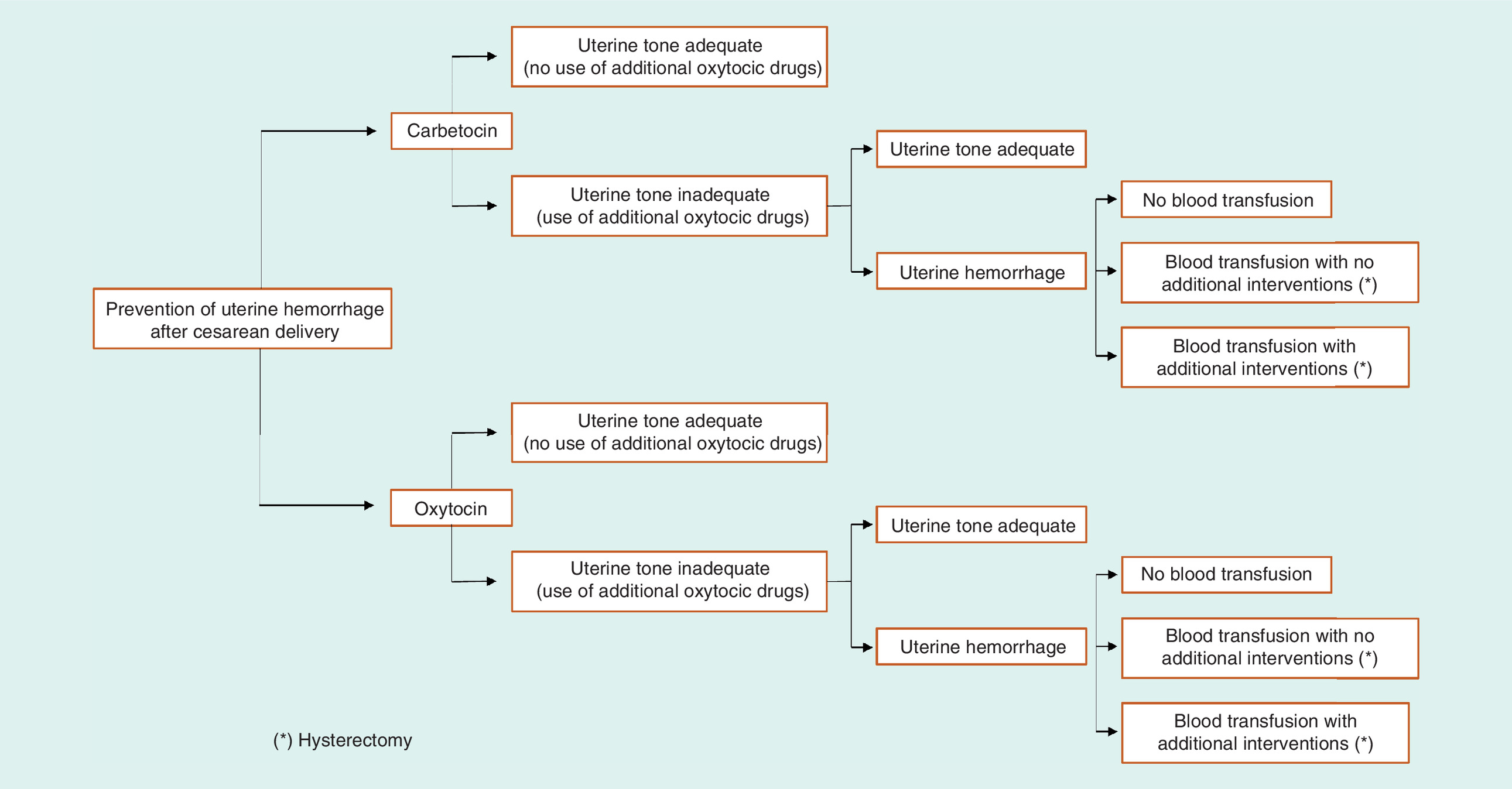
We used this information to construct a decision tree, which was applied for the model (Figure 1).
The direct costs were obtained from the Office for Accounting and Costs of Hospital Nacional Edgardo Rebagliati Martins, mainly from the SAP R/3 system and correspond to the year 2015 (cost template in Excel).
Table 1 shows the costs that were taken into consideration for data processing.
| Item | Unit cost in soles | Unit cost in soles (S/.) |
|---|---|---|
| Blood transfusion | 312.57 | 643.13 |
| Cost of hemorrhage kit | 223.08 | 223.08 |
| Cost of additional oxytocic drugs | 16.67 | 16.67 |
| Oxytocin | 0.85 | 0.85 |
| Misoprostol | 2.25 | 2.25 |
| Ergometrine | 0.40 | 0.4 |
| Duratocin (carbetocin) | 62.07 | 62.07 |
| Atropine | 0.25 | 0.25 |
| Hysterectomy | 2845.01 | 2845.01 |
Costs are for every 100 patients.
It is noteworthy that drug costs were taken from the Peruvian official price list (DIGEMID-MINSA). The minimum price of the different products for the public sector was taken into consideration, with the exception of oxytocin, for which the average public sector price was calculated (in contrast with information for other drugs, the web page of the official price list gives a minimum and maximum price for oxytocin). The average price was S/. 0.825. The price of carbetocin was provided by the distributor of this product in Peru (S/. 62.5). All prices include sales tax. The dose of oxytocin was that used in the study by Cordovani et al. [10] for prevention of uterine hemorrhage (6.5 ampoules).
An interview was held with the head of the Blood Bank to determine the costs of consumables for blood transfusions. Similarly, the cost of consumables for control of uterine hemorrhage was also calculated (posthemorrhage kit from Guía de Práctica Clínica de Manejo de la hemorragia de la segunda mitad del embarazo y postparto – ESSALUD 2014 [Clinical Practice Guidelines on the management of hemorrhage during the second half of pregnancy and postpartum - ESSALUD 2014]). An average of two transfusions were considered necessary to control uterine hemorrhage.
The costs included in the model were those of medication, hysterectomy and control of bleeding. The analysis was made from the payer's perspective.
The time horizon was 1 year (2015) for the calculation of QALYs. In Peru, there is no cost–effectiveness threshold for healthcare interventions.
The results of the model are provided based on a deterministic approach using the ICER. A series of sensitivity analyses were subsequently performed to determine the effect of uncertainty with respect to the parameters and to the structure. First, we performed a univariate sensitivity analysis in which the costs used in the model were increased and decreased by 10% to determine how the outcome changed (ICER). Second, we performed a probabilistic sensitivity analysis in which each parameter was assigned a probability distribution; a value for the distribution was taken randomly. This process was repeated 1000-times, and the mean value of the ICER was taken. Thus, it was possible to compare whether the uncertainty (variability) of the parameters used in the model generated changes in the result.
Excel 2013 was used to enter and process data according to the decision tree model.
Results
According to the meta-analysis examined in the present study, patients who received carbetocin require uterotonic agents significantly less frequently than patients who received oxytocin (relative risk: 0.64; 95% CI: 0.51–0.81) [16].
Carbetocin was clearly associated with fewer hemorrhages, fewer transfusions and, therefore, with lower costs stemming from these interventions (Table 2). Similarly, carbetocin was associated with a higher number of QALYs.
| Variables | Carbetocin | Oxytocin |
|---|---|---|
| Hemorrhages | 3.398 | 13.729 |
| Transfusions | 0.072 | 0.363 |
| Cost of hemorrhage (S/.) | 758.06 | 3062.64 |
| Cost of transfusion (S/.) | 93.91 | 808.25 |
| Total costs (S/.) | 64,369.54 | 13,306.13 |
| Total QALYs | 833.88 | 832.86A |
Number of hemorrhages for every 1000 patients.
The resulting ICER was S/. 49,918 per QALY, that is, below the threshold we estimated for Peru, as observed on the cost–effectiveness plane (Figure 2).
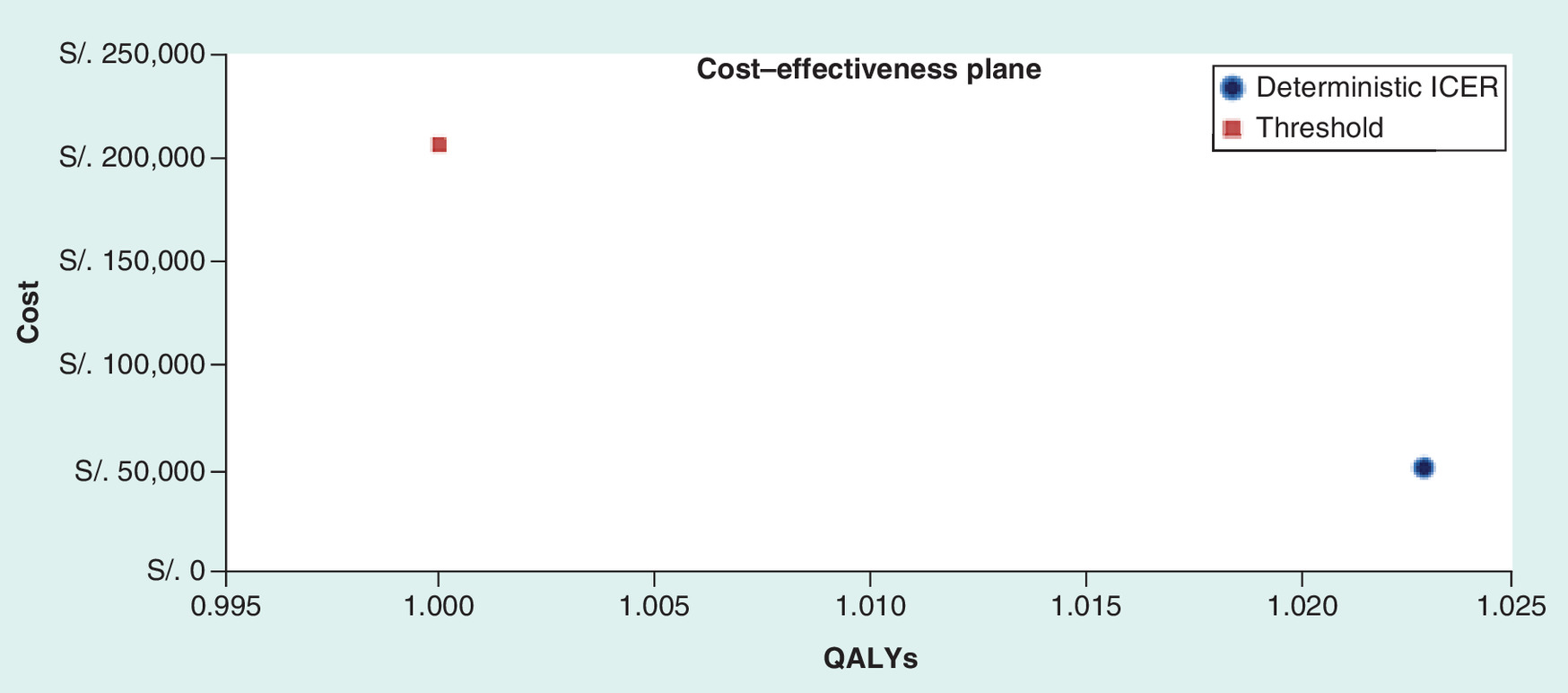
Figure 2. Cost–effectiveness.
ICER: Incremental cost–effectiveness ratio; QALY: Quality-adjusted life years.
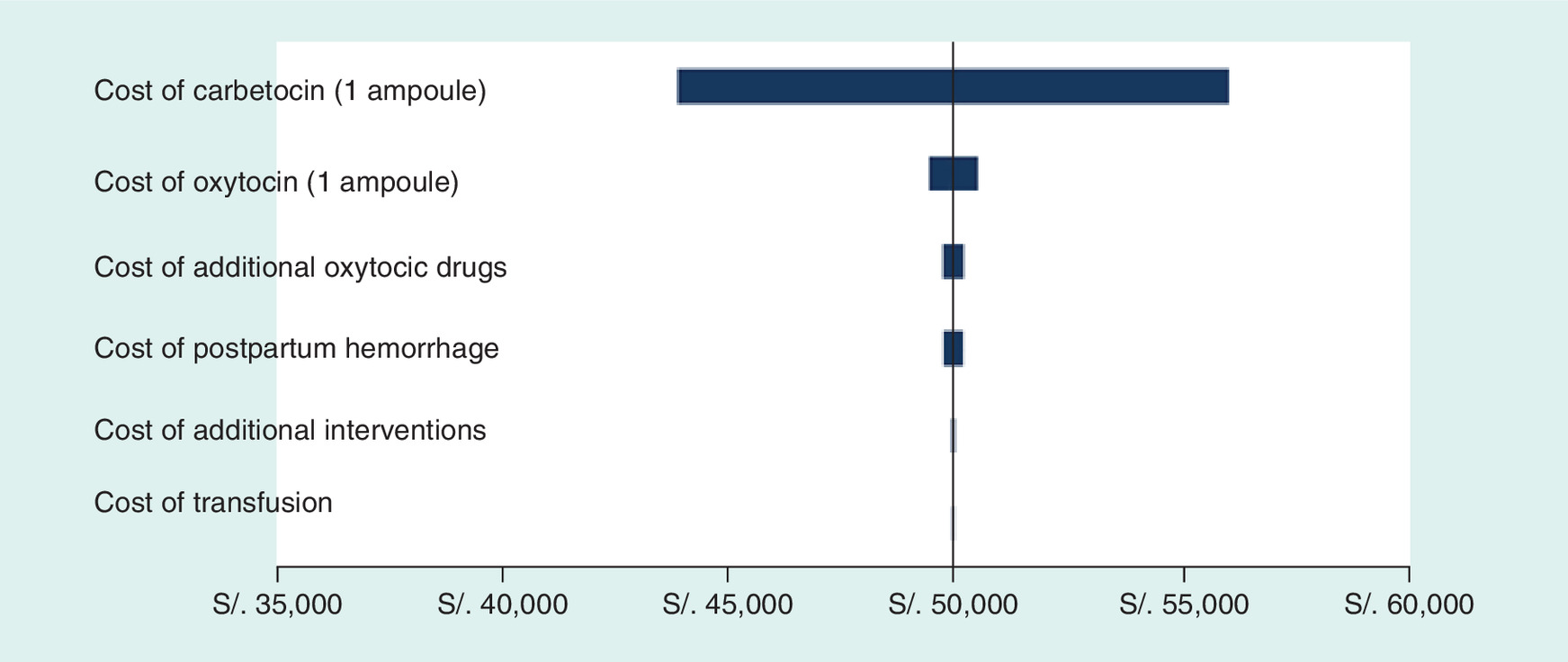
The univariate analysis revealed the cost of carbetocin to be a relevant parameter in the model, leading the result to vary by only 10% for the base case. When the price of carbetocin varies (± 10%), the ICER increases or decreases by 12% without changing the direction of the result, that is, it does not change in favor of oxytocin. The remaining parameters do not vary the result (ICER) more than 1% (Figure 3).
This analysis was followed by a second analysis to investigate the change in the result depending on the relationship between the cost of oxytocin and the cost of carbetocin (cost of carbetocin/cost of oxytocin). The costs of both drugs were taken from studies performed in Colombia and the UK in order to analyze the ratio and its association with the ICER. The results of the analysis can be seen in Figure 2, which shows that when the cost of carbetocin falls with respect to that of oxytocin, the ICER decreases. This means that in situations where oxytocin is more expensive, the price of carbetocin can be higher and lead to an ICER that favors carbetocin; however, in situations where oxytocin is inexpensive (e.g., in Peru), the price of carbetocin cannot be expensive, since the ICER increases considerably (Figure 4).
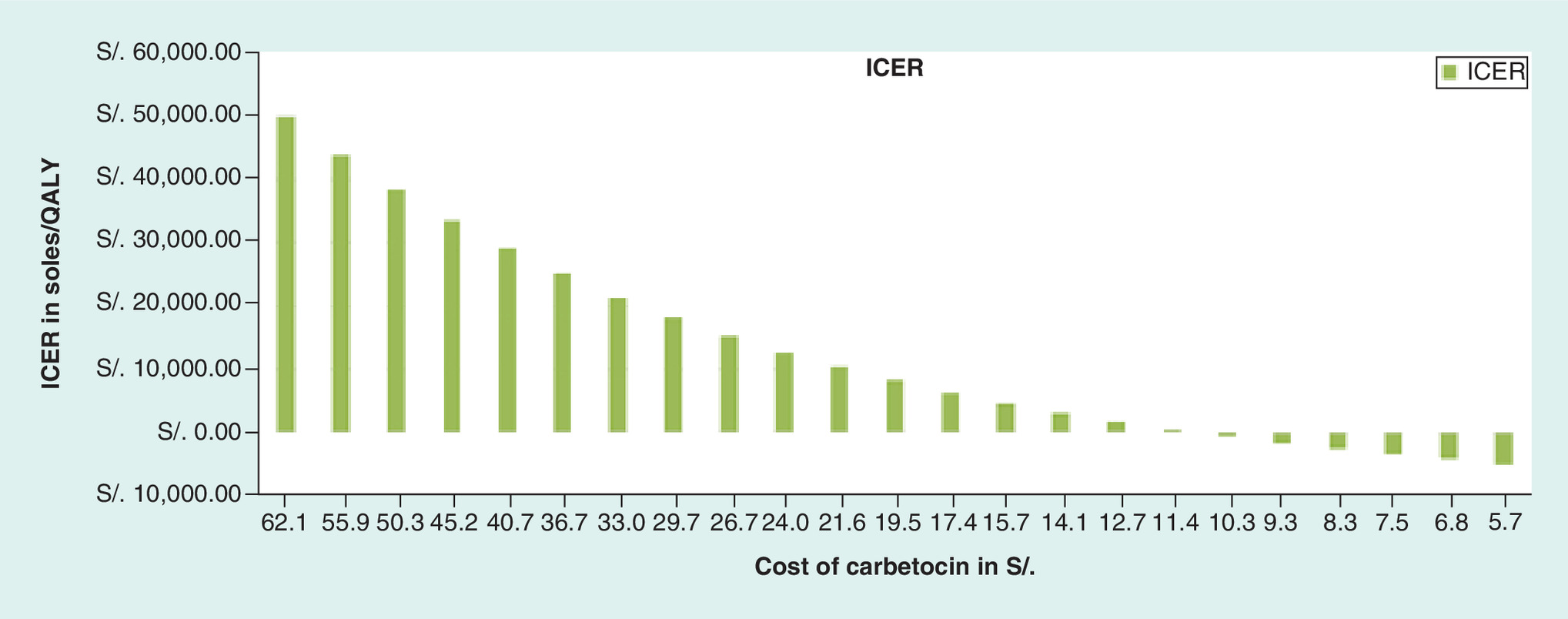
Figure 4. Association between the carbetocin/oxytocin ratio and the incremental cost–effectiveness ratio.
ICER: Incremental cost–effectiveness ratio; QALY: Quality-adjusted life years.
Discussion
Our results show that, when compared with oxytocin, therapy with carbetocin for the prevention of hemorrhage following cesarean delivery is associated with an ICER of S/. 49,918 per QALY, thus situating therapy with carbetocin below the cost–effectiveness threshold for the present study. It is important to remember that the greater cost of carbetocin in relation to oxytocin affects the result of the ICER.
Probabilistic sensitivity analysis indicates that carbetocin continues to be associated with fewer events (hemorrhages and transfusions) and, therefore, lower costs. It is also associated with the results of the deterministic analysis in terms of total cost. However, owing to the uncertainty surrounding the useful data, the ICER of the probabilistic sensitivity analysis is S/. 119,178 per QALY, among others, carbetocin is more efficient than oxytocin: 51.7% of the iterations had an acceptance threshold of S/. 207,800 per QALY.
Conclusion
Carbetocin is safe and effective in clinical practice. In addition, it is more cost-effective than oxytocin for the prevention of uterine hemorrhage in women undergoing cesarean delivery, thus making it possible to avoid blood transfusion, additional uterotonic agents to control bleeding and, potentially, hysterectomy in extreme cases. Carbetocin also makes it possible to reduce the cost of these interventions.
Postpartum hemorrhage is one of the main causes of maternal death throughout the world.
The risk of postpartum hemorrhage is much greater in cesarean delivery, especially in developing countries, where most operations are performed as emergency procedures.
Prophylaxis with uterotonic agents significantly reduces the risk of postpartum hemorrhage.
Carbetocin is more cost-effective than oxytocin for the prevention of postpartum hemorrhage in women undergoing cesarean delivery.
Compared with oxytocin, administration of carbetocin makes it possible to avoid blood transfusion, additional uterotonic agents to control bleeding and hysterectomy.
Probabilistic sensitivity analysis indicates that carbetocin is associated with fewer events (hemorrhages and transfusions) and, therefore, lower costs.
Carbetocin is safe and effective in clinical practice.
Financial & competing interests disclosure
This study was funded by Laboratorios Ferring. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Content Ed Net (Madrid, Spain) provided editorial assistance for the publication of this manuscript with financial aid from Laboratorios Ferring.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
AbouZahr C. The global burden of maternal death and disability. Br. Med. Bull. 67, 1–11 (2003).
2.
Dirección General de Epidemiología. Sistema de vigilancia epidemiológica de la Dirección General de Epidemiología. MINSA – Perú.
3.
ESSALUD. Guía de práctica clínica basada en evidencias: manejo de la hemorragia de la segunda mitad del embarazo y postparto (2014).
4.
Ozumba BC, Ezegwui HU. Blood transfusion and caesarean section in a developing country. J. Obstet. Gynaecol. 26, 746–748 (2006).
5.
World Health Organization. Global estimates of maternal mortality for 1995: results of an in-depth review analysis and estimation strategy (statement). Geneva, Switzerland (2001).
6.
Waterstone M, Bewley MS, Wolfe C. Incidence and predictors of severe obstetric morbidity: case-control study. BMJ 322, 1089–1093 (2001).
7.
Cotter AM, Ness A, Tolosa JE. Prophylactic oxytocin for the third stage of labour. Cochrane Database Syst. Rev. (4), CD001808 (2007).
8.
Gulmezoglu AM, Villar J, Ngoc NT et al. The WHO multicentre randomized trial of misoprostol in the management of the third stage of labour. Lancet 358, 689–695 (2001).
9.
Hunter DJ, Schulz P, Wassenaar W. Effect of carbetocin, a long acting oxytocin analog on the postpartum uterus. Clin. Pharmacol. Ther. 52, 60–67 (1992).
10.
Cordovani D, Carvalho JCA, Boucher M et al. Carbetocin for the prevention of postpartum hemorrhage. The Global Library of Women's Medicine, Postpartum Hemorrhage, Chapter 44. www.glowm.com/pdf/PPH_2nd_edn_Prelims.pdf.
11.
Boucher M, Nimrod CA, Tawagi GF, Meeker TA, Rennicks White RE, Varin J. Comparison of carbetocin and oxytocin for the prevention of postpartum hemorrhage following vaginal delivery: a double-blind randomized trial. J. Obstet. Gynaecol. Can. 26, 481–488 (2004).
12.
Boucher M, Horbay GLA, Griffin P et al. Double-blind, randomized comparison of the effect of carbetocin and oxytocin on intraoperative blood loss and uterine tone of patients undergoing cesarean section. J. Perinatol. 18, 202–207 (1998).
• It was one of the first studies that proved that a lower amount of carbetocin was needed when using extra therapeutic uterotonic, comparing with oxytocin.
13.
Dansereau J, Joshi AK, Helewa ME et al. Double-blind comparison of carbetocin versus oxytocin in prevention of uterine atony after cesarean section. Am. J. Obstet. Gynecol. 180, 670–676 (1999).
•• It is the first large-scale clinical trial that compared effectiveness and safety of carbetocin in prevention of postpartum hemorrhage.
14.
Borruto F, Treisser A, Comparetto C. Utilization of carbetocin for prevention of postpartum hemorrhage after cesarean section: a randomized clinical trial. Arch. Gynecol. Obstet. 280, 707–712 (2009).
• Involves pregnant women with at least one risk factor for postpartum hemorrhage.
15.
Attilakos G, Psaroudakis D, Ash J et al. Carbetocin versus oxytocin for the prevention of postpartum haemorrhage following caesarean section: the results of a double-blind randomized trial. BJOG 117, 929–936 (2010).
•• It is the study with the lowest bias risk in its methodological design that was used in the meta-analysis.
16.
Su LL, Chong YS, Samuel M. Carbetocin for preventing postpartum haemorrhage. Cochrane Database Syst. Rev. (2), CD005457 (2012).
•• It is a meta-analysis (higher level of evidence) based on studies that existed in that date, to evaluate effectiveness and safety of carbetocin in prevention of postpartum hemorrhage.
17.
Del Angel-Garcia G, Garcia-Contreras F, Constantino Casas P et al. Economic evaluation of carbetocin for the prevention of uterine atony in patients with risk factors in Mexico. Value in Health 9(6), A254 (2006).
•• In this study we show that the average cost–effectiveness ratio with carbetocin is lower than with oxytocin.
18.
Alvis N, Valenzuela MT. Los QALYs y DALYs como indicadores sintéticos de salud. Rev. Méd. Chile. 138(Suppl. 2), 83–87 (2010).
• Reviews the origin and use of the measures QALY and DALY.
19.
Holleboom CA, van Eyck J, Koenen SV et al. Carbetocin in comparison with oxytocin in several dosing regimens for the prevention of uterine atony after elective caesarean section in The Netherlands. Arch. Gynecol. Obstet. 287, 1111–1117 (2013).
• Compares carbetocine with some oxytocin dosage regimes to prevent uterine atony in patients undergoing caesarean section.
20.
O'Sullivan AK, Thompson D, Chu P, Lee DW, Stewart EA, Weinstein MC. Cost–effectiveness of magnetic resonance guided focused ultrasound for the treatment of uterine fibroids. Int. J. Technol. Assess. healthcare. 25, 14–25 (2009).
21.
Iczkovitz S, Laberge M, Coyte P. Carbetocin vs oxytocin for prevention of uterine atony after caesarean section: a meta-analysis and economic evaluation. Institute of Health Policy, Management and Evaluation, University of Toronto, Ferring Inc (2012).
22.
Cáceres LA, Rueda C, Caicedo A. Costo efectividad de carbetocina comparada con oxitocina para prevenir hemorragia postparto por atonía uterina en pacientes con factores de riesgo. Value in Health 16(7), 709–710 (2013).
Information & Authors
Information
Published In
Copyright
© 2017 Future Medicine Ltd.
History
Received: 15 February 2017
Accepted: 13 July 2017
Published online: 21 December 2017
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Pharmacoeconomic study comparing carbetocin with oxytocin for the prevention of hemorrhage following cesarean delivery in Lima, Peru. (2017) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2017-0012
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Mansoureh Samimi, Reza Hosseiniara, Hossein Akbari, Delaram Beyrami, Carbetocin versus oxytocin with or without tranexamic acid for preventing postpartum hemorrhage in cesarean delivery: a randomized controlled trial, BMC Pregnancy and Childbirth, 10.1186/s12884-026-08674-5, (2026).
- Joshua F. Ginnane, Samia Aziz, Saima Sultana, Connor Luke Allen, Annie McDougall, Katherine E. Eddy, Nick Scott, Joshua P. Vogel, The cost-effectiveness of preventing, diagnosing, and treating postpartum haemorrhage: A systematic review of economic evaluations, PLOS Medicine, 10.1371/journal.pmed.1004461, 21, 9, (e1004461), (2024).
- A. Tareef, K. Downey, B. Ma, W. Whittle, J. Carvalho, Carbetocin Versus Oxytocin Following Vaginal and Cesarean Delivery: A Before-After Study, Obstetric Anesthesia Digest, 10.1097/01.aoa.0000891656.66489.88, 42, 4, (187-189), (2022).
- Suzette Matthijsse, Fredrik L. Andersson, Michael Gargano, Yum L. Yip Sonderegger, Cost-effectiveness analysis of carbetocin versus oxytocin for the prevention of postpartum hemorrhage following vaginal birth in the United Kingdom, Journal of Medical Economics, 10.1080/13696998.2022.2027669, 25, 1, (129-137), (2022).
- Jamaica Roanne Briones, Pattarawalai Talungchit, Montarat Thavorncharoensap, Usa Chaikledkaew, Economic evaluation of carbetocin as prophylaxis for postpartum hemorrhage in the Philippines, BMC Health Services Research, 10.1186/s12913-020-05834-x, 20, 1, (2020).
- Pan Sun, Hongzhi Xiao, Jianzhong Wang, Suxia Zhang, Xingyuan Cao, Pharmacokinetics and bioavailability of carbetocin after intravenous and intramuscular administration in cows and gilts, Journal of Veterinary Pharmacology and Therapeutics, 10.1111/jvp.12830, 43, 2, (237-240), (2019).
- Theresa A. Lawrie, Ewelina Rogozińska, Pauline Sobiesuo, Joshua P. Vogel, Laura Ternent, Olufemi T. Oladapo, A systematic review of the cost‐effectiveness of uterotonic agents for the prevention of postpartum hemorrhage, International Journal of Gynecology & Obstetrics, 10.1002/ijgo.12836, 146, 1, (56-64), (2019).
- Laura Dormer, Introducing Volume 7 of the Journal of Comparative Effectiveness Research , Journal of Comparative Effectiveness Research, 10.2217/cer-2017-0087, 7, 1, (1-4), (2018).