Real-world cost–effectiveness of infliximab for moderate-to-severe rheumatoid arthritis in a medium-sized city of China
Abstract
Aim: To assess the cost–effectiveness of infliximab-containing therapy (ICT) for moderate-to-severe rheumatoid arthritis (RA) in a medium-sized Chinese city. Methods: A Chinese prospective cohort study comparing ICT (25 patients) versus conventional disease-modified antirheumatic drugs (24 patients) for RA was used to assess the cost–effectiveness of ICT. Results: The cohort study observed significantly reduced disease activity score of 28 joints (coefficient -2.718, p < 0.001), improved EQ-5D (coefficient 0.453, p < 0.001) and increased medical costs (coefficient 1.289, p < 0.001) associated with ICT. The incremental cost–effectiveness ratio per gained quality-adjusted life year for ICT versus disease-modified antirheumatic drugs was 1.897-times of the local gross domestic product per capita. Conclusion: Infliximab was a favorable cost-effective alternative option for moderate-to-severe RA in a medium-sized city of China.
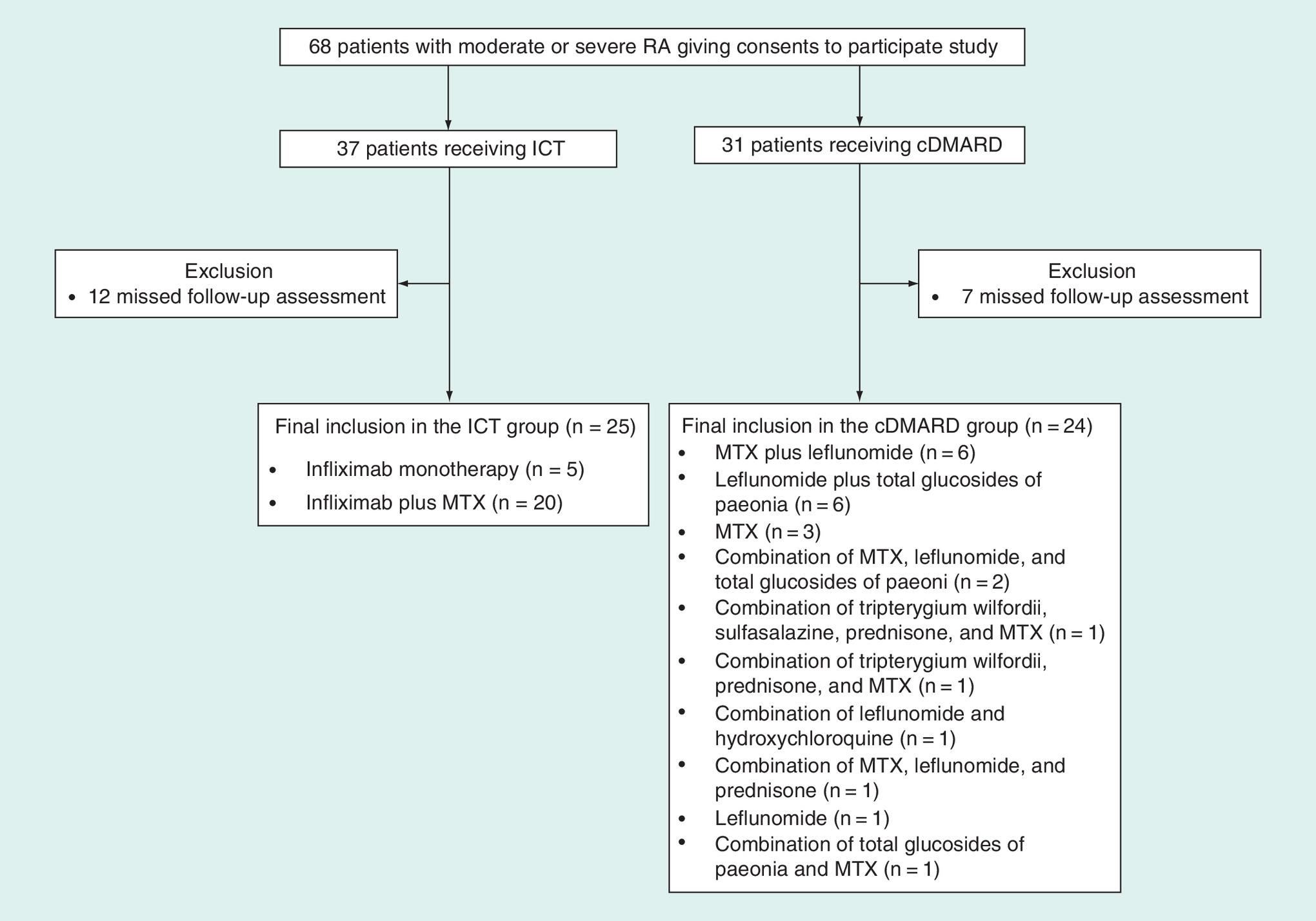
Figure 1. The flow chart of patient enrollment process to create infliximab-containing therapy treatment group and conventional disease-modified antirheumatic drugs group.
cDMARD: Conventional disease-modified antirheumatic drug; ICT: Infliximab-containing therapy; MTX: Methotrexate; RA: Rheumatoid arthritis.
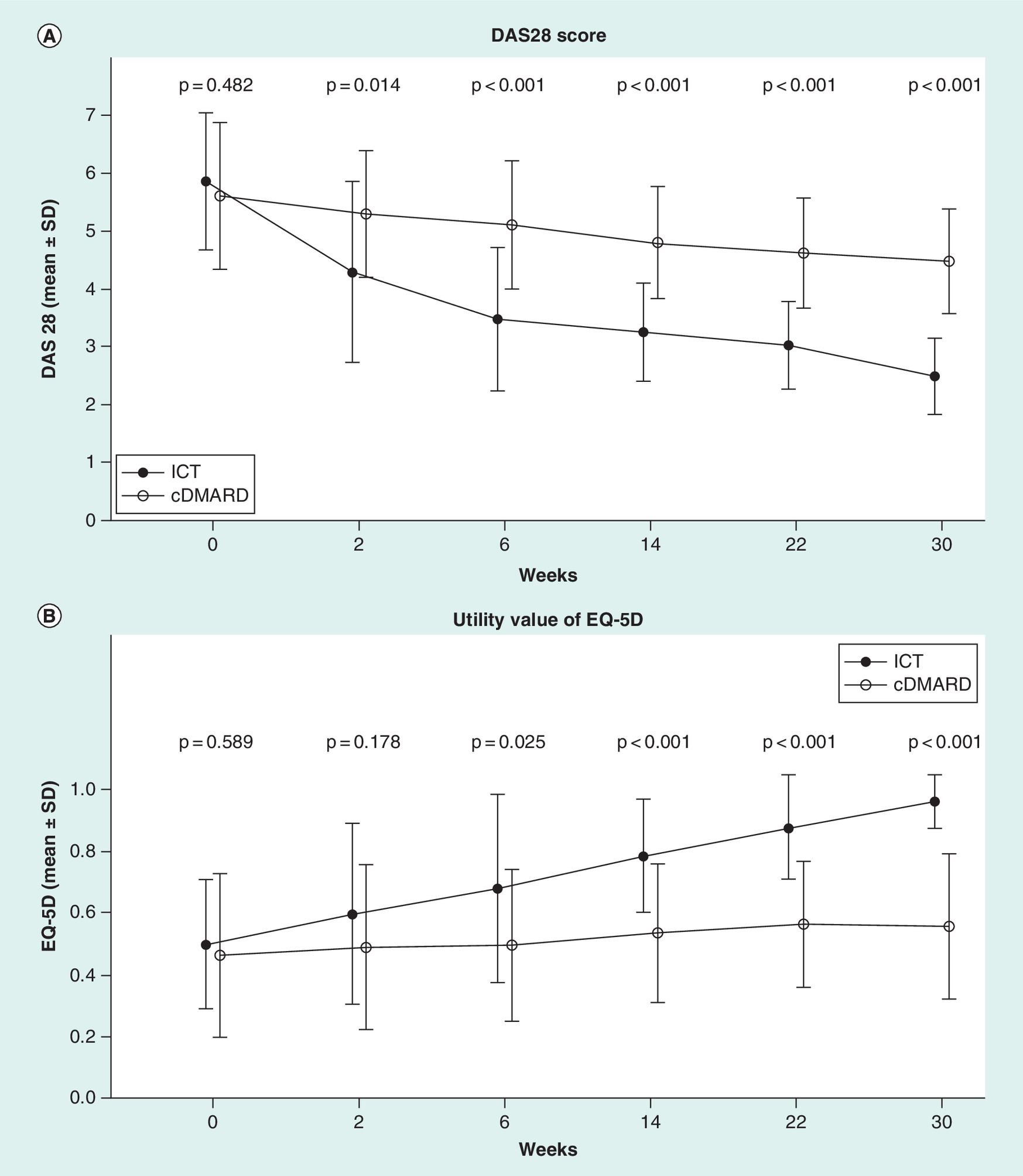
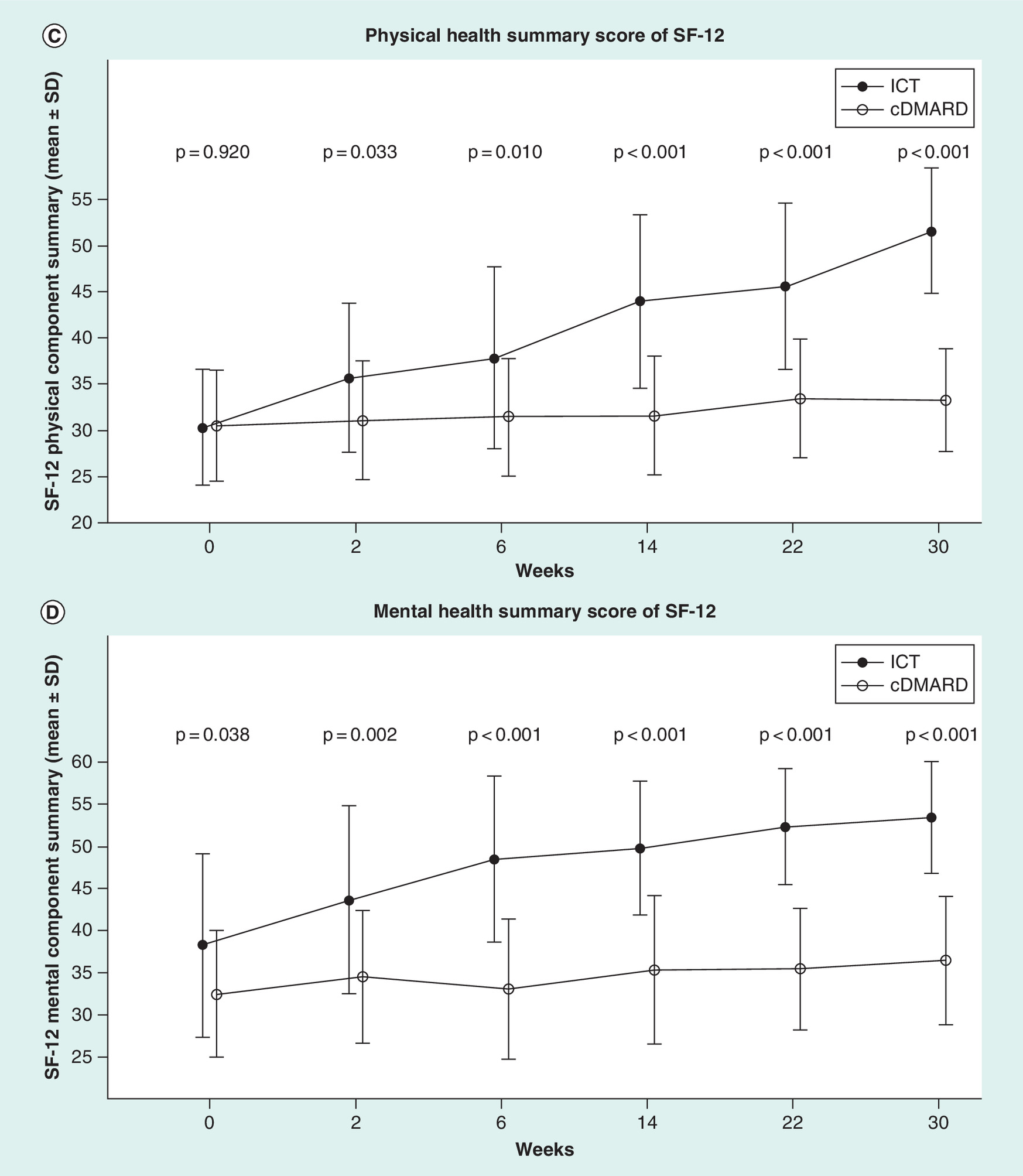
Figure 2. Unadjusted comparisons of measured health outcomes associated with each follow-up assessment over 30-week follow-up for infliximab-containing therapy versus conventional disease-modified antirheumatic drugs.
(A) DAS28 score. (B) Utility value of EQ-5D. (C) Physical health summary score of SF-12. (D) Mental health summary score of SF-12.
cDMARD: Conventional disease-modified antirheumatic drug; DAS28: Disease activity score of 28 joints; ICT: Infliximab-containing therapy; SD; Standard deviation.
First draft submitted: 29 July 2016; Accepted for publication: 28 November 2016; Published online: 20 December 2016
The prevalence of rheumatoid arthritis (RA) in China is 0.2–0.37% [1]; RA is recognized as a major health problem in China because of its substantial burden on patients, patients’ families, healthcare system and society [2]. Infliximab, a chimeric monoclonal antibody specific for the key proinflammatory cytokine tumor necrosis factor, is effective at relieving the signs and symptoms of RA, as well as improving functional status and preventing the progression of joint damage [3,4]. Infliximab is the first biologic treatment approved for RA in 2007 in China. However, the access to biologics for RA is limited in China. According to a large RA treatment survey in 21 large tertiary hospitals across China, the biologics treatment rate was 10.2% [5].
Since the launch of infliximab in China, a few studies were conducted in first-tier cities in China. A large prospective cohort study in Beijing observed that infliximab significantly improved RA-related symptoms and quality of life in patients [6]. A Phase II/III randomized trial also demonstrated that infliximab was superior to methotrexate (MTX) and placebo regarding treatment response defined by American College of Rheumatology response criteria and disease activity score of 28 joints (DAS28) in RA patients living in Guangzhou [7]. Even though the cost–effectiveness of infliximab relative to conventional disease-modified antirheumatic drugs (cDMARD) was found to be acceptable in Shanghai [8], one of the largest cities in China, the economic gap associated with city size in China could substantially impact disease management and reimbursement policies, the two well-recognized driving factors in the cost–effectiveness analysis. Thus, we conducted this study to generate real-world evidence to confirm the cost–effectiveness of infliximab treatment for moderate-to-severe RA in a medium-sized city in China.
Patients & methods
This prospective cohort study compared infliximab-containing therapy (ICT) with cDMARD for disease severity, quality of life and direct medical costs over 30-week follow-up time in moderate-to-severe RA patients living in Zhuzhou, a typical medium-sized city with a population of 3.88 million in the central-south of China. The data collected from this observational study was further applied to a cost–effectiveness model comparing ICT with cDMARD for moderate-to-severe RA over lifetime horizon from the perspective of a local public health system in Zhuzhou. The study protocol was reviewed and approved by the ethics board of the Zhuzhou Hospital, where study patients were enrolled.
Prospective cohort study comparing ICT with cDMARD for real-world health outcomes & direct medical costs
Patient enrollment started in the department of rheumatology of Zhuzhou Hospital in July 2013. The defined inclusion criteria were patients with age above 18 years; patients with RA confirmed by 1987 American Society of Rheumatology diagnosis criteria [9]; patients with moderate-to-severe RA that was defined as DAS28 score >3.2; and, patients receiving infliximab and/or cDMARD. cDMARD in this study included azathioprine, cyclophosphamide, cyclosporine, hydroxychloroquine, leflunomide, MTX and sulfasalazine; patients gave their consents to participate in this study and also agreed to be regularly followed up. In order to control potential bias, the study excluded patients previously treated with biologics; patients with other rheumatic diseases (Lyme disease, psoriatic arthritis, spondyloarthropathy, systemic lupus erythematosus, infectious or reactive arthritis, or Reiter's syndrome); or patients with any solid organ or hematologic malignancies. The patient enrollment time was 1 year (July 2013–June 2014), and the enrolled patients were followed up for 30 weeks. The follow-up assessments were conducted among all enrolled patients according to the infliximab treatment schedule, three starter doses at 0, 2 and 6 weeks and every 8 weeks after the three starter doses. The treatment dose of infliximab was 3 mg/kg per infusion. The collected patient baseline characteristics included patient demographics, insurance type, occupation, comorbidity, DAS28 assessment, morning stiff time and quality of life measured by EQ-5D and SF-12. The follow-up assessment included DAS28 assessment, quality of life measured by EQ-5D and SF-12, and direct medical costs for treatments, inpatient care and outpatient care.
Data conversion was conducted for DAS28 score, EQ-5D-derived utility and SF-12 physical and mental health summary scores. DAS28 score was calculated using the collected data for the tender joint count, swollen joint count, erythrocyte sedimentation rate (mm/h) and visual analog scale for general health (mm) [10]. The generated health state from EQ-5D questionnaire was converted to utility value using a Chinese general population-based time trade-off values for EQ-5D health states [11]. The collected SF-12 physical and mental health summary scales were scored using the regression weights for physical and mental health derived from a US general population [12]. After the data conversion, student's t-test and Fisher's exact test were conducted to compare the two treatment groups for patient baseline characteristics and measured outcomes for DAS28, EQ-5D utility value, and the physical and mental health summary scores of SF-12. Wilcoxon rank sum test was performed to compare the two treatments for the measured cost outcomes. Multiple linear regression analyses were conducted for the comparisons of ICT versus cDMARD for DAS28, EQ-5D utility value, and SF-12 physical and mental health summary scores after full adjustment of the collected patient baseline characteristics. Multiple generalized linear regression analysis was conducted to compare ICT with cDMARD for direct medical costs after full adjustment of the obtained patient baseline characteristics. The statistical significance defined in these data analyses was two-sided p-value <0.05. SAS 9.2 (Cary, NC, USA) was used to perform the data analyses described earlier.
Cost–effectiveness analysis comparing ICT with cDMARD
A decision analytic model was constructed using Markov model to simulate quality-adjusted life years (QALY) and direct medical costs associated with ICT or cDMARD over lifetime horizon in moderate-to-severe RA patients in Zhuzhou. The patient cohort in the prospective cohort study was taken as the model cohort, which was assumed to continue ICT or cDMARD beyond the 30-week follow-up time. Thus, the impact of ICT and cDMARD on disease activity and quality of life at the 30th week were assumed to remain until patients were deceased. The disease analytic model did not simulate RA-related complications due to the paucity of evidence. Thus, the Markov model only included two health states, alive and dead, in each model cycle, which was set as 1 year. Both future health benefits and direct medical costs in our model were discounted as 3% per annum to follow the Chinese guideline for pharmacoeconomic evaluation [13]. Multiple generalized linear regression analyses derived from the prospective cohort study created equations simulating the impact of age, gender and treatment (ICT vs cDMARD) on outcome measures (AS 28, EQ-5D utility and direct medical costs) in the Markov model. Our prospective cohort study did not have a follow-up longer enough to assess the impact of DAS28 on mortality. Additionally, the impact of DAS28 on mortality in Chinese RA patients was rarely studied. Thus, the hazard ratio of mortality associated with high DAS28 score relative to low DAS28 in our model was estimated from an extensive German registry study comparing highly active disease (mean DAS28 >5.1) versus persistently low disease activity (mean DAS28 <3.2) for mortality risk in 8908 RA patients over 31,378 patient-years [14]. Our model further assumed that the patients with low disease activity were comparable as the Chinese general population regarding mortality and the most recent age, and gender-stratified life table of the Chinese general population [15] was used as the reference for the mortality associated with low disease activity of RA. The decision analytic model was constructed in the 2013 Microsoft Excel. The model input data applied to the cost–effectiveness analysis can be found in Table 4, which summarizes the results of the one-way sensitivity analyses on the uncertainty of each model input.
The constructed decision analytic model was run to perform the base case cost–effectiveness analysis to estimate the incremental cost–effectiveness ratio (ICER) per gained QALY for ICT relative to cDMARD in our study cohort with moderate-to-severe RA from the perspective of local healthcare payer in Zhuzhou. One-way sensitivity analysis was performed to assess the impact of uncertainty of each model variable on the cost–effectiveness of ICT by varying the model variables within their 95% CIs or ± 25% of their baseline values. Probabilistic sensitivity analysis (PSA) was performed using Monte Carlo simulation method with 5000 iterations in the decision analytic model under the β-distributions of model variables. The generated 5000 ICERs from the simulations were plotted to estimate the 95% credible interval. The cost–effectiveness for ICT relative to cDMARD was converted to the times of the local gross domestic product per capita (GDPPC) in 2015 (RMB58,952 or US$8838) [16] in Zhuzhou to compare with the cost–effectiveness threshold (three-times of GDPPC) recommended by both WHO [18] and Chinese pharmacoeconomic evaluation guidelines [13].
Results
The study enrolled a total of 68 patients, including 37 patients receiving ICT and 31 patients receiving cDMARD. After exclusion of 12 dropouts in the infliximab group and 7 dropouts in the cDMARD group, the final data analyses included 49 patients, 25 patients receiving ICT (5 receiving infliximab monotherapy and 20 receiving the combination of infliximab and MTX) and 24 patients receiving cDMARD, which included monotherapy with MTX (n = 3) and combination treatments (n = 21). The patient enrollment process is illustrated in Figure 1.
Comparisons of patient baseline characteristics between ICT & cDMARD
The two treatment groups (ICT vs cDMARD) had comparable patient baseline characteristics regarding baseline morning stiff time, DAS28 score and EQ-5D utility value (Table 1). However, the unadjusted comparisons did observe significant differences in some patient baseline characteristics. For example, the infliximab group was associated with significantly lower proportion of patients with public urban worker insurance plan (32 vs 75%, p = 0.004), significantly lower proportion of retired patients (32 vs 62.5%, p = 0.047) and significantly higher baseline mental health summary score of SF-12 (38.2 vs 32.5, p = 0.038). Multiple logistic regression analysis for treatment selection observed a strong but nonsignificant association between patient baseline DAS28 score and ICT in the included patients (odds ratio [OR]: 11.048; p = 0.113).
Comparisons of health outcomes between ICT & cDMARD
Unadjusted comparisons of the measured health outcomes between the two treatment groups along the 30-week follow-up observed significantly faster decline of the DAS28 score and significantly faster increases in EQ-5D utility, and physical and mental health summary scores of SF-12 associated with ICT group. Additionally, the significant differences in DAS28, EQ-5D utility, and physical and mental health summary score of SF-12 between the two treatment groups started at week 2. The unadjusted comparisons of the measured health outcomes between the two treatment groups over the 30-week follow-up time are illustrated in Figure 2. Further unadjusted comparisons of overall changes in the measured health outcomes over the follow-up observed significantly reduced DAS28 (3.4 vs 1.1, p < 0.001), significantly increased EQ-5D utility value (0.5 vs 0.1, p < 0.001), and significantly increased physical (21.2 vs 2.8, p < 0.001) and mental health summary scores (15.2 vs 4.0, p < 0.001) of SF-12 in the patients receiving ICT treatment (Table 2). Multiple linear regression analysis with full adjustment of patient baseline characteristics confirmed the significant reduction of DAS28 (coefficient -2.718, p < 0.001) and significant increases of EQ-5D utility (coefficient 0.453, p < 0.001) and SF-12 physical (coefficient 19.918, p < 0.001) and mental health summary scores (coefficient 16.359, p < 0.001) associated with ICT. The results of the multiple linear regression analyses are summarized in Table 3.
Comparisons of direct medical costs between ICT & cDMARD
Unadjusted comparisons of health resources utilization associated with the two treatment groups observed comparable out-patient visits but significantly longer hospital stay length (30.2 vs 14.0 days, p = 0.012) associated with ICT group. Additionally, the ICT group was associated with significantly higher aggregated direct medical costs over 30-week follow-up time than the cDMARD group (RMB 60,416 vs RMB 15,071, p < 0.001). The drug costs accounted for the increased direct medical costs associated with ICT treatment (RMB 52,799 vs RMB 7788, p < 0.001) as the two treatment groups had comparable nondrug costs (RMB 7617 vs RMB 7283, p = 0.881) (Table 2). Multiple generalized linear model with full adjustment of patient baseline characteristics confirmed significantly higher direct medical costs (coefficient 1.289, p < 0.001) in the patients receiving ICT.
Cost–effectiveness of ICT relative to cDMARD for moderate-to-severe RA
The constructed disease analytic model with the baseline values of model variables projected that ICT could obtain additional 3.857 life years (14.174 vs 10.317 years) and 7.982 QALYs (13.609 vs 5.627 QALYs) when compared with cDMARD over lifetime time horizon. However, ICT was associated with higher lifetime direct medical costs (RMB 956,647 vs RMB 171,217, difference: RMB 785,430) than cDMARD. The base case ICER per gained QALY for ICT relative to cDMARD was RMB 98,395, or 1.669-times of the GDPPC in 2015, 55.6% of the WHO cost–effectiveness threshold. One-way sensitivity analyses indicated that the ICER per gained QALY for ICT versus cDMARD ranged from 0.882 to 3.157 GDPPC when model variables varied within their ranges (Table 4). The identified driving model variables for the cost–effectiveness of ICT included the impact of ICT on the utility value of EQ-5D (ICER range: 2.438–1.269 GDPPC per gained QALY) and the baseline direct medical costs associated with severe RA (ICER range: 0.882–3.156 GDPPC per gained QALY). The distribution of the generated 5000 ICERs in the PSA was slightly skewed to better cost–effectiveness with 95% credible interval from 0.504 to 5.936 GDPPC per gained QALY. The proportion of being cost effective for ICT relative to cDMARD was 82.1% if the willingness-to-pay was 3 GDPPC.
Discussion
This study includes a prospective cohort study and a cost–effectiveness analysis assessing ICT for moderate-to-severe RA patients living in a medium-sized city of China. The observed improvement of health outcomes associated with ICT in our study was consistent with previous studies evaluating infliximab for RA [17]. Based on the prospective cohort study, the cost-effective analysis suggested that the ICT could be an attractive treatment option for moderate-to-severe RA in Zhuzhou, a typical medium-sized city of China.
Similar to previous studies reporting reduced disease activity associated with infliximab treatment for moderate-to-severe RA, our multiple linear regression analysis with adjustment for potential confounding effects associated with patient baseline characteristics confirmed the significant reduction of the DAS28 score by 2.7 when compared with cDMARD in our prospective cohort study. The observed reduction of DAS28-associated infliximab in our study was comparable with the observation in a Phase III trial, which reported the infliximab treatment could reduce DAS28 by 2.4 from 6.7 to 4.3 over the same time horizon as our study (30 weeks) [19]. Because RA disease activity is strongly associated with economic disparity [20] and the RA patients living in small or medium-sized cities of China are likely to have higher activity disease due to poorer management and limited health resources, the treatment response to infliximab in our study cohort was likely to be better than that in patients who have been well managed in large cities.
Similar to the impact of infliximab on DAS28, the improvement of the quality of life in our patients receiving infliximab was substantial and significant. Our study used two well-validated quality of life measurement instruments, EQ-5D and SF-12, to demonstrate the impact of infliximab on the overall quality of life, physical function and mental health. The two instruments showed good consistence to the reduction of the DAS28 score in our prospective cohort study by showing a similar trend of increasing EQ-5D utility values, and physical and mental health summary scores of SF-12. According to the study results, 30-week treatment with infliximab could reduce DAS28 score by 2.55, about 40% of the baseline DAS28 score. The adjusted increase of EQ-5D utility value associated with 30-week infliximab treatment was 0.453, which made the patients almost have a comparable quality of life as general healthy people. The observed better treatment response of EQ-5D to infliximab treatment in our patients may suggest that the reduced disease activity was likely to generate more health benefits contributing to improving the overall quality of life further [21]. Different from EQ-5D, SF-12 was designed to measure the quality of life classified by physical function and mental health [22]. According to our study results, SF-12 had slightly different responses to infliximab treatment by increasing the physical and mental health summary scores by 52 and 37%, respectively, when compared with the baseline. Because DAS28 score is mainly based on the counts of tender and swollen joints, any reduced DAS28 score should indicate the improvement of tender and swollen joints and lead to improved physical function, a significant contributor to quality of life. Thus, the SF-12 results in our study confirmed that the improved physical function but not mental health accounts for the major improvement of the quality of life associated with infliximab treatment.
Even though the improved health outcomes are supposed to reduce health resources utilization and save direct medical costs, our cost analysis did not observe any trends of reducing health resources or direct medical costs in our patients receiving infliximab treatment. We suspected that the current hospitalization-based reimbursement policy in China could lead to hospital infliximab infusions that significantly extended hospital stay length and offset the potential economic benefits associated with improved health outcomes in patients receiving infliximab. Thus, future studies should further clarify the potential confounding effects associated with hospital-based reimbursement policy on health resources utilization and explore a more appropriate reimbursement mode that could maximize potential economic benefits of infliximab.
Even though infliximab treatment was associated with high acquisition costs and also increased health resources utilization related to current hospital-based reimbursement policy in our study cohort, infliximab treatment would be an acceptable treatment option for moderate-to-severe RA patients living in medium-sized cities of China from the cost–effectiveness perspective. According to the cost–effectiveness analysis based on the real-world data from our cohort study, the base case estimation of ICER per gained QALY for infliximab relative to cDMARD was about half of the recommended cost–effectiveness threshold. The PSA further suggested that the chance of infliximab therapy being cost effective was 82.1% under the recommended cost–effectiveness threshold (three-times of local GDPPC). Given the fact that our cost–effectiveness analysis did not take into account potential health benefits and economic benefits associated with potentially reduced RA-related complications in patients receiving infliximab, the cost–effectiveness of infliximab could be even more attractive in moderate-to-severe RA patients living in medium-sized cities of China. Additionally, the external validity of our cost–effectiveness analysis was confirmed by a previous cost–effectiveness analysis assessing infliximab for moderate-to-severe RA in Shanghai, China [8] and also in European countries [22] and the USA [23].
Our study has several major limitations that could bias our study results. First, the small sample size and nonrandomization design of our prospective cohort study could not minimize the uncertainty and confounding effects associated with outcome measurement. Additionally, selection bias could exist in our study as our patients receiving infliximab, which was much costlier than cDMARD, were likely to have a higher income than those receiving cDMARD. The RA patients with higher social economic status could have better response to quality of life [24,25]. Thus, the potential confounding effects associated with these factors could make the observed improvement of EQ-5D utility value associated with infliximab (0.453) in our prospective cohort study higher than the estimation in previous studies (over 0.20) [26,27]. Second, our study was unable to obtain accurate information for medical costs associated with patient visits to other hospitals and clinics. The missing information for direct medical costs in other clinic settings could substantially bias the comparisons of direct medical costs between the two treatment groups. Third, SF-12 physical and mental health summary scores in our study were calculated using the weights based on US general population due to the lack of the reference for the Chinese population. Thus, system bias could exist in the calculation of the SF-12 results. Fourth, our prospective cohort study did not meet all data needs of a robust cost–effectiveness analysis. For example, our prospective cohort study only followed up the enrolled patients for 30 weeks, which was not longer enough to observe the impact of the two treatments on mortality, the main driving factor in the cost–effectiveness. Our study had to use a German RA registry study for the estimation of the hazard ratio of mortality associated with severe RA. Additionally, our model assumption on the maintained treatment effects beyond the follow-up time did not factor the real-world setting in which treatment compliance usually drops over time. Our cost–effectiveness analysis did not simulate the RA-related complications, which could be reduced by long-term use of infliximab treatment [28,29]. Thus, caution is needed when leveraging the estimated cost–effectiveness of infliximab treatment in our study for decision making. Finally, our study was unable to conduct head-to-head comparisons among all treatments in our study cohort because the sample size associated with each treatment was unlikely to have sufficient power to detect any differences in the measured outcome measures. The observed effects associated with ICT (mixed with infliximab monotherapy and infliximab combination treatment) and cDMARD mixed with all nonbiologic medications could have limited generalizability to address the differences in measured outcomes between two specific medications for moderate-to-severe RA.
Conclusion
Our study confirmed the significantly reduced disease activity and improved quality of life associated with infliximab when compared with cDMARD for moderate-to-severe RA in a medium-sized city in China. Additional cost–effectiveness analysis suggested that infliximab treatment was a favorable cost–effective alternative option for moderate-to-severe RA patients living in the medium-sized cities of China. However, future studies with larger sample size and better study design are needed to confirm our study findings that could be biased by small sample size and nonrandomization design.
| Treatment group | ICT (n = 25) | cDMARD (n = 24) | p-value | ||
|---|---|---|---|---|---|
| Mean/% | SD | Mean/% | SD | ||
| Age (years) | 57.5 | 11.7 | 62.4 | 11.9 | 0.154 |
| Male gender (%) | 28.0 | – | 20.8 | – | 0.742 |
| Body weight (kg) | 57.3 | 8.8 | 53.7 | 7.7 | 0.139 |
| Marital status (%): | |||||
| – Single | 0.0 | – | 4.2 | – | 0.490 |
| – Married | 92.0 | – | 95.8 | – | 1.000 |
| Health insurance plan (%): | |||||
| – Urban workers | 32.0 | – | 75.0 | – | 0.004 |
| – Urban residents | 32.0 | – | 12.5 | – | 0.171 |
| – New rural cooperative | 28.0 | – | 12.5 | – | 0.289 |
| – Commercial | 4.0 | – | 0.0 | – | 1.000 |
| Occupation (%): | |||||
| – State employee | 8.0 | – | 0.0 | – | 0.490 |
| – Employee of public company | 0.0 | – | 0.0 | – | 1.000 |
| – Employee of private company | 4.0 | – | 0.0 | – | 1.000 |
| – Self-employed | 20.0 | – | 8.3 | – | 0.417 |
| – Retired | 32.0 | – | 62.5 | – | 0.047 |
| – Unemployed | 36.0 | – | 29.2 | – | 0.762 |
| Comorbidities (%): | |||||
| – Any comorbidities | 36.0 | – | 41.7 | – | 0.773 |
| – Hypertension | 20.0 | – | 16.7 | – | 1.000 |
| – Coronary heart disease | 8.0 | – | 0.0 | – | 0.490 |
| – Diabetes | 4.0 | – | 8.3 | – | 0.609 |
| – Hyperlipidemia | 4.0 | – | 4.2 | – | 1.000 |
| – Osteoarthritis | 4.0 | – | 16.7 | – | 0.190 |
| – Stroke | 4.0 | – | 4.2 | – | 1.000 |
| Baseline disease activity: | |||||
| – Morning stiff time (min) | 81.6 | 96.7 | 85.8 | 138.7 | 0.902 |
| – DAS28 score | 5.9 | 1.2 | 5.6 | 1.3 | 0.482 |
| Baseline quality of life: | |||||
| – EQ-5D utility value | 0.5 | 0.2 | 0.5 | 0.3 | 0.589 |
| – Physical health summary score of SF-12 | 30.3 | 6.3 | 30.5 | 6.1 | 0.919 |
| – Mental health summary score of SF-12 | 38.2 | 10.9 | 32.5 | 7.5 | 0.038 |
Values that are bold indicate a p value of less than 0.05.
cDMARD: Conventional disease-modified antirheumatic drug; DAS28: Disease activity score of 28 joints; ICT: Infliximab-containing therapy; SD: Standard deviation.
| Treatment group | ICT (n = 25) | cDMARD (n = 24) | p-value | ||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||
| Changes of health outcomes: | |||||
| – DAS28 score | -3.4 | 1.3 | -1.1 | 1.1 | < 0.001 |
| – EQ-5D utility value | 0.5 | 0.2 | 0.1 | 0.2 | < 0.001 |
| – Physical health summary score of SF-12 | 21.2 | 6.7 | 2.8 | 6.6 | < 0.001 |
| – Mental health summary score of SF-12 | 15.2 | 12.9 | 4.0 | 7.2 | < 0.001 |
| Health resource utilization: | |||||
| – RA-related out-patient clinic visits | 6.3 | 5.1 | 6.5 | 3.7 | 0.889 |
| – RA-related hospital days | 30.2 | 26.6 | 14.0 | 14.7 | 0.012 |
| Direct medical costs: | |||||
| – Drug costs | ¥52,799 | ¥12,440 | ¥7788 | ¥5016 | < 0.001 |
| – Nondrug costs | ¥7617 | ¥3940 | ¥7283 | ¥2554 | 0.881 |
| – Total costs | ¥60,416 | ¥11,680 | ¥15,071 | ¥4804 | < 0.001 |
cDMARD: Conventional disease-modified antirheumatic drug; DAS28: Disease activity score of 28 joints; ICT: Infliximab-containing therapy; RA: Rheumatoid arthritis; SD: Standard deviation.
| Outcome measure | Change of DAS28 score | Change of EQ-5D utility value | Change of SF-12 physical summary score | Changes of SF-12 mental health summary score | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Variable | Coefficient | 95% CI of coefficient | p-value | Coefficient | 95% CI of coefficient | p-value | Coefficient | 95% CI of coefficient | p-value | Coefficient | 95% CI of coefficient | p-value | ||||
| Lower | Upper | Lower | Upper | Lower | Upper | Lower | Upper | |||||||||
| Infliximab-containing therapy vs cDMARD | -2.718 | -3.321 | -2.115 | < 0.001 | 0.453 | 0.260 | 0.647 | < 0.001 | 19.918 | 14.025 | 25.812 | < 0.001 | 16.359 | 8.593 | 24.124 | < 0.001 |
| Demography: | ||||||||||||||||
| – Age (years) | -0.003 | -0.032 | 0.027 | 0.846 | -0.002 | -0.010 | 0.007 | 0.677 | 0.183 | -0.065 | 0.432 | 0.139 | 0.209 | -0.118 | 0.536 | 0.197 |
| – Male gender (%) | -0.490 | -1.440 | 0.461 | 0.293 | -0.075 | -0.358 | 0.208 | 0.584 | 3.038 | -5.584 | 11.659 | 0.470 | -0.169 | -11.529 | 11.191 | 0.976 |
| – Body weight (kg) | 0.032 | -0.019 | 0.083 | 0.206 | 0.000 | -0.015 | 0.015 | 0.985 | -0.119 | -0.569 | 0.331 | 0.585 | 0.103 | -0.490 | 0.695 | 0.721 |
| Marital status (%): | ||||||||||||||||
| – Single | -2.237 | -4.145 | -0.328 | 0.024 | 0.229 | -0.406 | 0.865 | 0.460 | 3.595 | -15.768 | 22.957 | 0.702 | 10.261 | -15.252 | 35.774 | 0.410 |
| – Married | -2.044 | -3.599 | -0.489 | 0.013 | 0.185 | -0.320 | 0.689 | 0.453 | 5.806 | -9.560 | 21.172 | 0.439 | 17.485 | -2.761 | 37.732 | 0.087 |
| Health insurance plan (%): | ||||||||||||||||
| – Urban workers | -1.610 | -3.268 | 0.048 | 0.056 | 0.169 | -0.385 | 0.723 | 0.531 | 1.641 | -15.221 | 18.504 | 0.841 | 11.568 | -10.650 | 33.787 | 0.289 |
| – Urban residents | -0.749 | -2.388 | 0.890 | 0.348 | 0.035 | -0.515 | 0.586 | 0.894 | -0.765 | -17.523 | 15.994 | 0.925 | 8.831 | -13.251 | 30.913 | 0.413 |
| – New rural cooperative | -0.990 | -2.710 | 0.730 | 0.241 | 0.196 | -0.381 | 0.772 | 0.486 | 2.440 | -15.115 | 19.994 | 0.774 | 10.742 | -12.389 | 33.873 | 0.343 |
| – Commercial | -3.045 | -6.039 | -0.052 | 0.047 | 0.293 | -0.629 | 1.214 | 0.514 | 15.036 | -13.024 | 43.095 | 0.276 | 17.648 | -19.325 | 54.620 | 0.330 |
| Occupation (%): | ||||||||||||||||
| – State employee | -0.513 | -1.641 | 0.614 | 0.350 | -0.071 | -0.449 | 0.307 | 0.699 | 0.954 | -10.549 | 12.456 | 0.864 | -1.657 | -16.813 | 13.500 | 0.822 |
| – Employee of public company | 0.000 | – | – | – | 0.000 | – | – | – | 0.000 | – | – | – | 0.000 | – | – | – |
| – Employee of private company | 1.206 | -0.304 | 2.715 | 0.110 | -0.084 | -0.587 | 0.418 | 0.729 | 7.898 | -7.406 | 23.202 | 0.294 | -0.878 | -21.043 | 19.287 | 0.928 |
| – Self-employed | -0.533 | -1.407 | 0.341 | 0.216 | -0.011 | -0.281 | 0.258 | 0.930 | 4.224 | -3.974 | 12.421 | 0.294 | 3.388 | -7.413 | 14.190 | 0.519 |
| – Retired | -0.258 | -1.008 | 0.493 | 0.479 | 0.091 | -0.135 | 0.316 | 0.410 | 3.882 | -2.973 | 10.738 | 0.251 | -1.945 | -10.979 | 7.088 | 0.657 |
| Comorbidities (%): | ||||||||||||||||
| – Any comorbidities | 1.702 | 0.725 | 2.680 | 0.002 | -0.127 | -0.454 | 0.199 | 0.425 | -6.312 | -16.257 | 3.632 | 0.200 | -8.466 | -21.569 | 4.637 | 0.192 |
| – Hypertension | -0.374 | -1.282 | 0.533 | 0.396 | 0.007 | -0.283 | 0.297 | 0.959 | 1.517 | -7.319 | 10.353 | 0.723 | 2.019 | -9.624 | 13.662 | 0.721 |
| – Coronary heart disease | -0.330 | -1.815 | 1.155 | 0.645 | 0.143 | -0.352 | 0.637 | 0.553 | -3.909 | -18.965 | 11.147 | 0.593 | 7.968 | -11.870 | 27.806 | 0.411 |
| – Diabetes | -0.780 | -1.712 | 0.152 | 0.095 | -0.029 | -0.342 | 0.285 | 0.851 | 8.731 | -0.820 | 18.282 | 0.071 | -0.613 | -13.198 | 11.972 | 0.920 |
| – Hyperlipidemia | -2.643 | -3.918 | -1.368 | 0.000 | 0.236 | -0.181 | 0.652 | 0.251 | 9.213 | -3.470 | 21.897 | 0.145 | 10.461 | -6.251 | 27.174 | 0.206 |
| – Osteoarthritis | -1.318 | -2.290 | -0.345 | 0.011 | 0.063 | -0.258 | 0.384 | 0.685 | 0.444 | -9.331 | 10.219 | 0.925 | 5.161 | -7.719 | 18.041 | 0.412 |
| – Stroke | 0.323 | -0.895 | 1.541 | 0.583 | 0.017 | -0.377 | 0.411 | 0.928 | -3.663 | -15.660 | 8.334 | 0.530 | -2.042 | -17.850 | 13.766 | 0.790 |
| Baseline disease activity: | ||||||||||||||||
| – Morning stiff time (min) | 0.001 | -0.002 | 0.003 | 0.557 | -0.001 | -0.002 | 0.000 | 0.076 | 0.007 | -0.018 | 0.033 | 0.553 | 0.011 | -0.022 | 0.044 | 0.501 |
| – DAS28 score | -0.474 | -0.720 | -0.228 | 0.001 | -0.023 | -0.102 | 0.056 | 0.557 | -1.495 | -3.900 | 0.910 | 0.209 | -0.650 | -3.819 | 2.519 | 0.673 |
| Baseline quality of life: | ||||||||||||||||
| EQ-5D utility value | 2.352 | 0.588 | 4.116 | 0.012 | -1.037 | -1.621 | -0.453 | 0.002 | -17.110 | -34.905 | 0.686 | 0.059 | -6.416 | -29.865 | 17.032 | 0.574 |
| – Physical health summary score of SF-12 | 0.006 | -0.047 | 0.059 | 0.800 | -0.002 | -0.020 | 0.016 | 0.822 | -0.579 | -1.122 | -0.035 | 0.038 | 0.182 | -0.534 | 0.898 | 0.601 |
| – Mental health summary score of SF-12 | -0.016 | -0.055 | 0.024 | 0.418 | 0.004 | -0.009 | 0.017 | 0.511 | 0.237 | -0.150 | 0.624 | 0.215 | -0.650 | -1.160 | -0.140 | 0.015 |
cDMARD: Conventional disease-modified antirheumatic drug; DAS28: Disease activity score of 28 joints; ICT: Infliximab-containing therapy.
| Model variable | Baseline | Range | ICER per gained QALY (GDPPC) | |||
|---|---|---|---|---|---|---|
| Low value | High value | For low value | For high value | Difference | ||
| Age (years) | 59.9 | 56.6 | 63.2 | 1.666 | 1.672 | 0.006 |
| Male proportion | 0.245 | 0.145 | 0.383 | 1.664 | 1.678 | 0.014 |
| Patient baseline DAS28 score | 5.753 | 5.403 | 6.103 | 1.671 | 1.668 | -0.003 |
| Hazard ratio associated with mortality for high DAS28 score (5.1) vs low DAS28 score (3.2) | 2.43 | 1.64 | 3.61 | 1.821 | 1.549 | -0.272 |
| DAS28 score reduction associated with ICT | 3.400 | 2.890 | 3.910 | 1.744 | 1.604 | -0.14 |
| DAS28 score reduction associated with cDMARD | 1.100 | 0.660 | 1.540 | 1.61 | 1.733 | 0.124 |
| Annual discount rate for QALY | 0.03 | 0 | 0.05 | 1.174 | 2.039 | 0.866 |
| Annual discount rate for direct medical costs | 0.03 | 0 | 0.05 | 2.275 | 1.402 | -0.873 |
| Coefficients associated with variables in the multiple linear regression analysis for quality of life | ||||||
| Intercept | 0.920 | 0.471 | 1.369 | 2.131 | 1.371 | -0.759 |
| ICT versus cDMARD | 0.253 | 0.075 | 0.430 | 2.438 | 1.269 | -1.169 |
| Age | -0.001 | -0.006 | 0.004 | 2.03 | 1.417 | -0.612 |
| Male gender | 0.041 | -0.082 | 0.164 | 1.693 | 1.645 | -0.048 |
| DAS28 score | -0.071 | -0.141 | -0.002 | 1.481 | 1.913 | 0.432 |
| Coefficients associated with variables in the multiple generalized linear model for direct medical costs | ||||||
| Intercept | 7.967 | 7.329 | 8.604 | 0.882 | 3.156 | 2.274 |
| ICT versus cDMARD | 1.312 | 1.058 | 1.566 | 1.213 | 2.257 | 1.044 |
| Age | 0.000 | -0.007 | 0.007 | 1.035 | 2.7 | 1.665 |
| Male gender | 0.065 | -0.109 | 0.238 | 1.584 | 1.757 | 0.172 |
| DAS28 score | -0.037 | -0.135 | 0.062 | 1.382 | 1.989 | 0.607 |
Values that are bold indicate a p value of less than 0.05.
cDMARD: Conventional disease-modified antirheumatic drug; GDPPC: Gross domestic production per capita; ICER: Incremental cost–effectiveness ratio; ICT: Infliximab-containing therapy; QALY: Quality-adjusted life year; RA: Rheumatoid arthritis.
Superior effectiveness of infliximab for moderate-to-severe rheumatoid arthritis was confirmed in a medium-sized city of China
Similar to previous studies reporting superior treatment effectiveness of infliximab for moderate-to-severe rheumatoid arthritis in western countries, our study confirmed the significantly reduced disease severity and improved quality of life in Chinese patients receiving infliximab for their moderate-to-severe rheumatoid arthritis.
Infliximab was associated with an acceptable cost–effectiveness for moderate-to-severe rheumatoid arthritis in a medium-sized city of China
Infliximab treatment was projected to gain more health benefits and cost more than cDMARD over lifetime horizon in Chinese moderate-to-severe rheumatoid arthritis patients living in a medium-sized city of China. The incremental cost–effectiveness ratio per gained QALY for infliximab relative to cDMARD was about half of the WHO cost–effectiveness threshold, the three times of the 2015 local GDPPC.
Authors’ contributions
J Li formulated the research idea and worked with Z Wen, A Cai, F Tian, L Zhang, Y Luo, L Deng and J He to enroll patients and prospectively collect follow-up data. Y Yang contributed to health economic model development and interpretation of the results of cost–effectiveness analysis. W Chen supervised the data analysis and manuscript development.
Financial & competing interests disclosure
The main funding source of this study was a clinical research grant from Zhuzhou Hospital. The cost–effectiveness analysis in this study was sponsored by Xian Janssen. Y Yang is an employee of Xian Janssen. W Chen is the founder of Nomin Health, a research consulting company receiving industry funds to conduct health economics and outcomes research in China and Canada. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.
References
1.
Felson DT. Comparing the prevalence of rheumatic diseases in China with the rest of the world. Arthritis Res. Ther. 10(1), 1–2 (2008).
2.
Zeng XF, Zhu SL, Tan AC, Xie XP. Disease burden and quality of life of rheumatoid arthritis in China: a systematic review. Chin. J. Evid. Med. 13(3), 300–307 (2013).
3.
Maini R, St Clair EW, Breedveld F et al. Infliximab (chimeric antitumour necrosis factor alpha monoclonal antibody) versus placebo in rheumatoid arthritis patients receiving concomitant methotrexate: a randomised Phase III trial. ATTRACT Study Group. Lancet 354, 1932–1939 (1999).
4.
Lipsky PE, van der Heijde DM, St Clair EW et al. Infliximab and methotrexate in the treatment of rheumatoid arthritis. N. Engl. J. Med. 343, 1594–1602 (2000).
5.
Wang XR, Su Y, An Y et al. [Survey of tumor necrosis factor inhibitors application in patients with rheumatoid arthritis in China]. Beijing da xue xue bao. Yi xue ban 44(2), 182–187 (2012).
6.
Zhang W, Shi Q, Wu DH et al. [Efficacy and safety of infliximab in patients with rheumatoid arthritis]. Zhonghua yi xue za zhi. 89(27), 1876–1880 (2009).
7.
Gao GH, Li J, Xie HW, Lü Z. [Therapeutic effect of infliximab on moderate and severe active rheumatoid arthritis]. Nan fang yi ke da xue xue bao 30(4), 724–726 (2010).
8.
Wu B, Wilson A, Wang FF et al. Cost effectiveness of different treatment strategies in the treatment of patients with moderate to severe rheumatoid arthritis in China. PLoS ONE 7(10), e47373 (2012).
9.
Arnett FC, Edworthy SM, Bloch DA et al. The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis. Arthrit. Rheum. 31(3), 315–324 (1988).
10.
Fransen J, Stucki G, van Riel PL. Rheumatoid arthritis measures: disease activity score (DAS), disease activity score-28 (DAS28), rapid assessment of disease activity in rheumatology (RADAR), and rheumatoid arthritis disease activity index (RADAI). Arthrit. Care Res. 49(S5), S214–S224 (2003).
11.
Liu GG, Wu H, Li M, Gao C, Luo N. Chinese time trade-off values for EQ-5D health states. Value Health 17(5), 597–604 (2014).
12.
Ware JE, Kosinski M, Keller SD. SF-12: How to Score the SF-12 Physical and Mental Health Summary Scales (2nd Edition). New England Medical Center, The Health Institute, MA, USA (1995).
13.
China guidelines for pharmacoeconomic evaluations. www.ispor.org/workpaper/ispor_comments/China-Guidelines-for-Pharmacoeconomic-Evaluations_V8.pdf.
14.
Listing J, Kekow J, Manger B et al. Mortality in rheumatoid arthritis: the impact of disease activity, treatment with glucocorticoids, TNFα inhibitors and rituximab. Ann. Rheum. Dis. 74(2), 415–421 (2013).
15.
WHO. Life tables by country: China. http://apps.who.int/gho/data/?theme=main&vid=60340.
16.
China: gross domestic product (GDP) per capita in current prices from 2010 to 2020 (in US dollars). www.statista.com/statistics/263775/gross-domestic-product-gdp-per-capita-in-china/.
17.
Chen YF, Jobanputra P, Barton P et al. A systematic review of the effectiveness of adalimumab, etanercept and infliximab for the treatment of rheumatoid arthritis in adults and an economic evaluation of their cost–effectiveness. Health Tech. Assess. 10(42), 1–266 (2006).
18.
Marseille E, Larson B, Kazi DS, Kahn JG, Rosen S. Thresholds for the cost–effectiveness of interventions: alternative approaches. Bull. World Health Org. 93(2), 118–124 (2015).
19.
Yoo DH, Racewicz A, Brzezicki J et al. A Phase III randomized study to evaluate the efficacy and safety of CT-P13 compared with reference infliximab in patients with active rheumatoid arthritis: 54-week results from the PLANETRA study. Arthrit. Res. Ther. 18(1), 1–12 (2016).
20.
Sokka T, Kautiainen H, Pincus T et al. Disparities in rheumatoid arthritis disease activity according to gross domestic product in 25 countries in the QUEST-RA database. Ann. Rheum. Dis. 68(11), 1666–1672 (2009).
21.
Linde L, Sørensen J, Østergaard M, Hørslev-Petersen K, Hetland ML. Health-related quality of life: validity, reliability, and responsiveness of SF-36, EQ-15D, EQ-5D, RAQoL, and HAQ in patients with rheumatoid arthritis. J. Rheumatol. 35(8), 1528–1537 (2008).
22.
Kobelt G, Jönsson L, Young A, Eberhardt K. The cost–effectiveness of infliximab (Remicade®) in the treatment of rheumatoid arthritis in Sweden and the United Kingdom based on the ATTRACT study. Rheumatology 42(2), 326–335 (2003).
23.
Wong JB, Singh G, Kavanaugh A. Estimating the cost–effectiveness of 54 weeks of infliximab for rheumatoid arthritis. Am. J. Med. 113(5), 400–408 (2002).
24.
Linde L, Sørensen J, Østergaard M et al. What factors influence the health status of patients with rheumatoid arthritis measured by the SF-12v2 health survey and the health assessment questionnaire? J. Rheumatol. 36(10), 2183–2189 (2009).
25.
Groessl EJ, Ganiats TG, Sarkin AJ. Sociodemographic differences in quality of life in rheumatoid arthritis. Pharmacoeconomics 24(2), 109–121 (2006).
26.
Kievit W, Fransen J, Adang EMM et al. Long-term effectiveness and safety of TNF-blocking agents in daily clinical practice: results from the Dutch Rheumatoid Arthritis Monitoring register. J. Rheumatol. 50(1), 196–203 (2011).
27.
Kobelt G, Eberhardt K, Geborek P. TNF inhibitors in the treatment of rheumatoid arthritis in clinical practice: costs and outcomes in a follow up study of patients with RA treated with etanercept or infliximab in southern Sweden. Ann. Rheum. Dis. 63(1), 4–10 (2004).
28.
Chopin F, Garnero P, le Henanff A et al. Long-term effects of infliximab on bone and cartilage turnover markers in patients with rheumatoid arthritis. Ann. Rheum. Dis. 67(3), 353–357 (2008).
29.
Dahlqvist SR, Engstrand S, Berglin E, Johnson O. Conversion towards an atherogenic lipid profile in rheumatoid arthritis patients during long-term infliximab therapy. Scand. J. Rheum. 35(2), 107–111 (2006).
Information & Authors
Information
Published In
Copyright
© Future Medicine Ltd.
History
Published online: 20 December 2016
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Real-world cost–effectiveness of infliximab for moderate-to-severe rheumatoid arthritis in a medium-sized city of China. (2016) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2016-0086
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Chuchuan Wan, Yuankai Huang, Qiqi Wang, Pei Wang, Xiaoyu Xi, Health utility of patients with established rheumatoid arthritis and its influencing factors: a multi-center study in China, Scientific Reports, 10.1038/s41598-024-64772-4, 14, 1, (2024).
- Zixuan He, Xianqin Huang, Dingyi Chen, Guoan Wang, Yuezhen Zhu, Huangqianyu Li, Sheng Han, Luwen Shi, Xiaodong Guan, Sponsorship bias in published pharmacoeconomic evaluations of national reimbursement negotiation drugs in China: a systematic review, BMJ Global Health, 10.1136/bmjgh-2023-012780, 8, 11, (e012780), (2023).
- Sajith Kumar, Bhavani Shankara Bagepally, Cost-effectiveness of tumor necrosis factor-alpha inhibitors: a systematic review and meta-analysis of cost-utility studies, Expert Review of Pharmacoeconomics & Outcomes Research, 10.1080/14737167.2023.2249610, 23, 9, (1027-1040), (2023).
- Chuchuan Wan, Qiqi Wang, Zhaoqi Xu, Yuankai Huang, Xiaoyu Xi, Mapping health assessment questionnaire disability index onto EQ-5D-5L in China, Frontiers in Public Health, 10.3389/fpubh.2023.1123552, 11, (2023).
- Madhumitha Haridoss, Bhavani Shankara Bagepally, Meenakumari Natarajan, Health‐related quality of life in rheumatoid arthritis: Systematic review and meta‐analysis of EuroQoL (EQ‐5D) utility scores from Asia, International Journal of Rheumatic Diseases, 10.1111/1756-185X.14066, 24, 3, (314-326), (2021).
- Lei Tian, Xiaomo Xiong, Qiang Guo, Yixi Chen, Luying Wang, Peng Dong, Aixia Ma, Cost-Effectiveness of Tofacitinib for Patients with Moderate-to-Severe Rheumatoid Arthritis in China, PharmacoEconomics, 10.1007/s40273-020-00961-z, 38, 12, (1345-1358), (2020).
- Qiang Yao, Chaojie Liu, Yaoguang Zhang, Ling Xu, Changes in health-related quality of life of Chinese populations measured by the EQ-5D-3 L: a comparison of the 2008 and 2013 National Health Services Surveys, Health and Quality of Life Outcomes, 10.1186/s12955-019-1109-x, 17, 1, (2019).
- Sanskriti Varma, Jun Hu, Ambar Mehta, Yiran Song, Angela Park, Min Zhi, Susan Hutfless, Initial medical and surgical management of inflammatory bowel disease in the biologic era: A comparison between the United States and China, JGH Open, 10.1002/jgh3.12146, 3, 3, (234-241), (2019).