Patient, caregiver and clinician use of comparative effectiveness research findings in care decisions: results from a national study
Abstract
Aim: To assess awareness, use and attitudes concerning comparative effectiveness research (CER) findings. Materials & methods: Online surveys of patients and caregivers managing rare (n = 560 patients, n = 609 caregivers) or chronic conditions (n = 762 patients, n = 776 caregivers), and practicing clinicians (n = 638). Results: Less than half of patients and caregivers reported exposure to any type of CER findings in the past 12 months. Of those, over half identify healthcare professionals as the information source, yet only 10% of clinicians indicated they were ‘very familiar’ with CER. Clinicians were concerned about the time required to find relevant evidence and the appropriateness of comparisons in available health research. Conclusion: Clinicians, patients and caregivers indicate unmet need for incorporating CER research findings into clinical decision-making.

Figure 1. Patient and caregiver report of treatment option information provided by their clinicians.
Among those who were made aware of treatment options for their condition by their clinician.
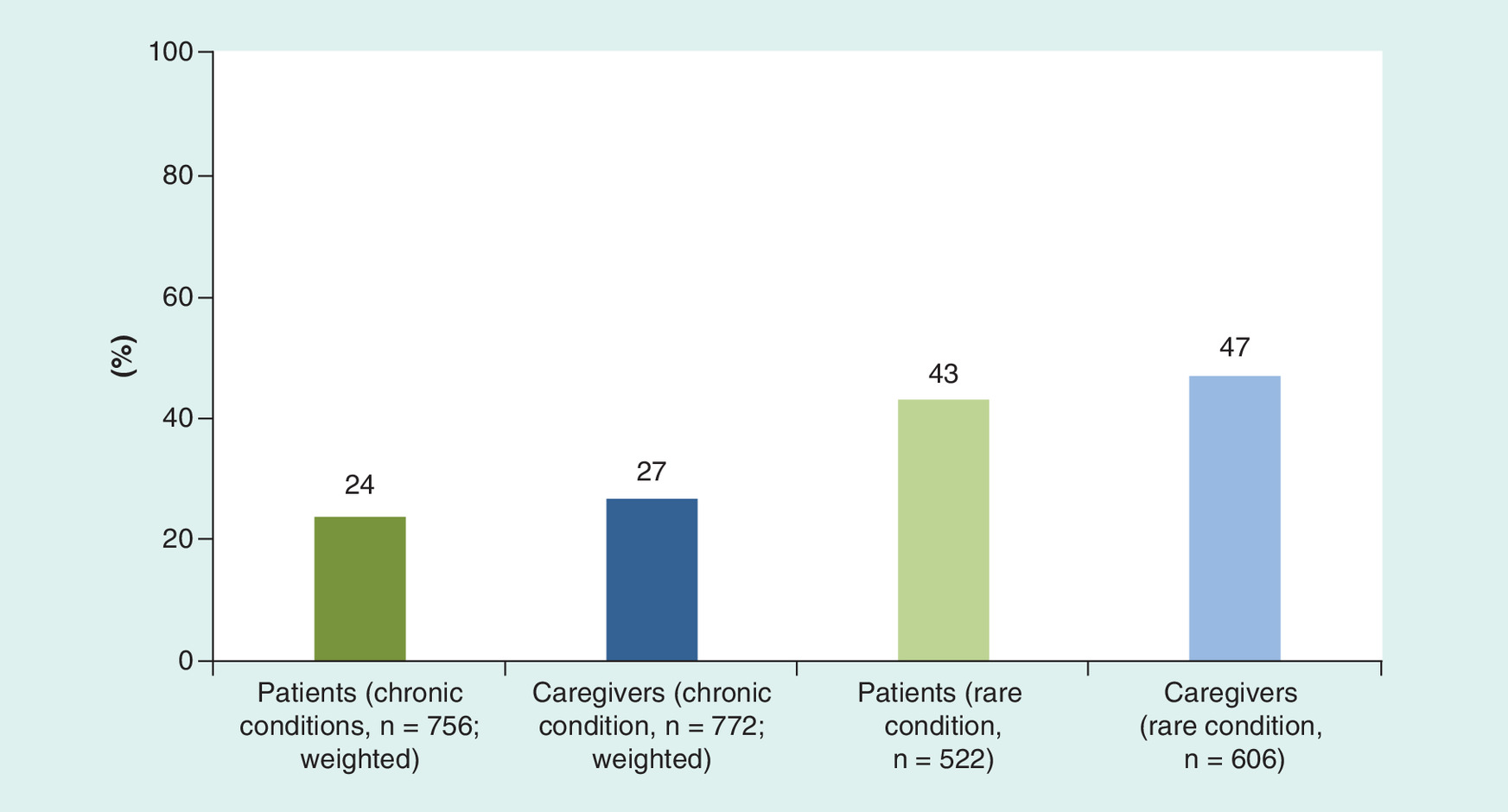
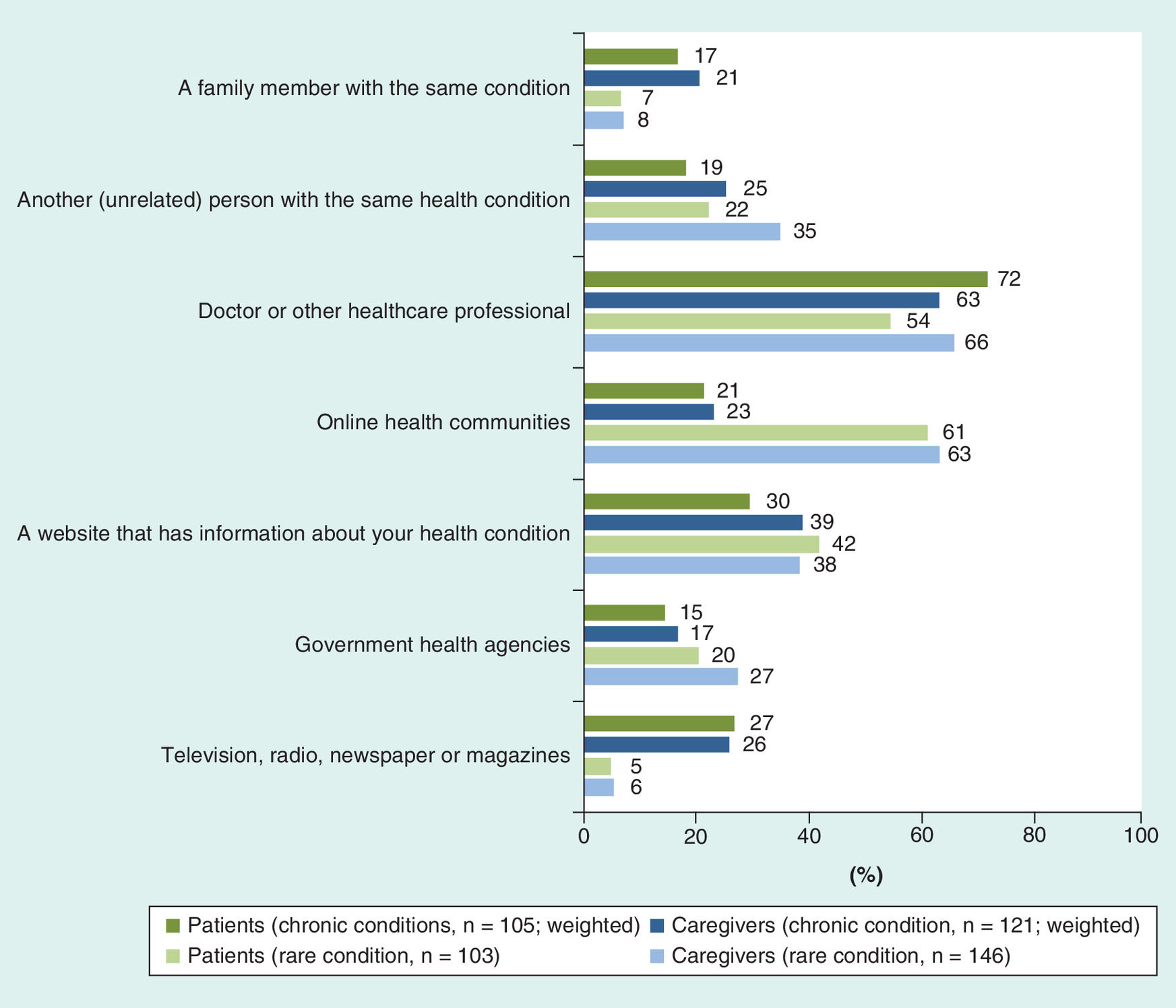
Figure 3. Patient and caregiver sources of comparative effectiveness research findings.
Among those who have read or heard about comparative effectiveness research in the last 12 months.

First draft submitted: 30 August 2016; Accepted for publication: 15 December 2016; Published online: 8 February 2017
Comparative effectiveness research (CER), which evaluates the effectiveness and safety of different preventive, diagnostic and treatment options, shows particular promise in generating evidence to inform decisions about what care is best for an individual patient [1–3]. Increased federal funding for CER [4,5] has expanded the growing interest in generating and disseminating CER findings to assist patient, caregiver and clinician decision-making [6].
Several studies have measured patient and clinician familiarity with or attitudes about CER, consistently finding limited awareness of CER, but generally favorable attitudes toward the concept [7–9]. However, there is little understanding of how patients, caregivers and clinicians access and use CER findings to inform care decisions. Given the importance of clinician/patient communication to health decision-making, such understanding is critical to ensuring that CER findings are available, accessible and actionable by the patients, caregivers and clinicians they are intended to help.
This study sought to assess attitudes toward and the use of health information and CER findings among patients, caregivers and clinicians managing rare and chronic conditions, as part of a larger effort by the Patient-Centered Outcomes Research Institute (PCORI) to understand healthcare stakeholder perceptions toward CER and engagement in research.
Materials & methods
Stakeholder input
An 11-member advisory group was formed with representatives of patient advocacy organizations, medical societies, health services researchers and CER researchers. Three separate eight-member working groups were then formed: one for chronic and rare disease patients, one for caregivers of patients with chronic or rare diseases, and one for clinicians. The advisory group and working groups assisted with development of the survey domains, item review and provided input on sampling plans. At the conclusion of the survey they aided with interpretation of results and dissemination activities (e.g., webinars, manuscript review [10,11]).
Measures
Surveys were developed and administered to: patients managing rare conditions; patients managing chronic conditions; caregivers of patients managing rare conditions; and caregivers of patients managing chronic conditions. An analogous survey was developed and administered to practicing clinicians, including physicians, physician assistants and nurse practitioners. Items were developed to address experiences and attitudes regarding the availability and use of information when making decisions about a test or treatment, and level of awareness and perceived value of CER. As part of the larger study, two additional survey domains (reported elsewhere [11]) explored awareness of and attitudes toward engagement in research, and the facilitators and barriers for research engagement. A review of the literature and key informant interviews identified existing information about the level of awareness of CER among patients, caregivers and clinicians and explored previous studies’ methodological challenges and issues. Participants were from the National Business Group on Health, the US Department of Veteran Affairs/University of California at San Francisco, and the National Pharmaceutical Council. Relevant survey items from related studies were reviewed [7,12–15] as were items from prior PCORI data collection efforts [8].
Draft survey items were reviewed and revised by the advisory group and working groups. These items were tested and revised for each audience through cognitive interviews to ensure clarity and relevance; cognitive interview participants did not have an affiliation with the project and were recruited specifically for item testing. Spanish language versions of items and instructions were developed following completion of English language items. The items were translated following the method used in the CAHPS II Cultural Comparability team [15].
Two versions of the clinician survey were developed a core survey (18 questions); and an extended version (core questions plus 25 supplemental questions assessing general practice approaches for patients managing chronic or rare conditions and clinician engagement in research). See the Supplementary Material for full instruments.
Patient & caregiver awareness of treatment options
Patients and caregivers were asked if they had knowledge of treatment options for their chronic or rare condition (yes/no/unsure) and whether a doctor or healthcare professional had provided information about treatment options for the condition (yes/no). If responding yes, patients and caregivers selected what kind of information was provided (i.e., the clinician's personal recommendation, information about what each treatment involves, information about the benefits and risks of each option based on your personal situation, advice about how to make a decision).
Patient & caregiver satisfaction with research evidence to support health decisions
4-point Likert ratings were used to collect information on patient and caregiver views of helpfulness of research results for making test or treatment decisions and how often they believed the information about the benefits and harms of different tests or treatments left them with unanswered questions. Yes/no response was used to address whether they believe they have sufficient information to make decisions about their condition.
Patient & caregiver preferences for information when making decisions
Patients and caregivers rated the importance of multiple characteristics of information related to treatment options (4-point scale from very important to not at all important).
Clinician satisfaction with research evidence
Clinicians rated their level of agreement with six statements regarding possible limitations of research evidence (4-point scale from strongly agree to strongly disagree).
Patient, caregiver & clinician awareness of and exposure to CER findings
Patients, caregivers and clinicians rated their familiarity with the term ‘comparative effectiveness research’ (4-point scale from very important to not at all important). Patients and caregivers were asked whether they had read or heard about CER findings related to their condition and to identify the source of the information from a list of possible responses.
Patient, caregiver & clinician attitudes toward CER
Patients and caregivers were asked whether they believe that information from research comparing the possible benefits and harms of different treatments would be useful in making decisions. Clinicians were asked whether CER findings would be useful in making recommendations for patients with chronic or rare conditions. Clinicians also were asked about their level of agreement with the statement, “Comparative effectiveness research will be used to restrict my freedom to choose treatments for my patients”.
Sampling & data collection
Distinct sampling approaches were applied for each target survey population. Online surveys of patients managing rare or chronic conditions were administered between September and October 2014 and were completed in English or Spanish, based on the respondent's preference. Surveys of caregivers for patients managing rare or chronic conditions were administered online in January 2015 in English only. The clinician survey was administered between December 2014 and January 2015. The American Institutes for Research Institutional Review Board approved this study.
Patients & caregivers managing rare conditions
Nationally representative sampling frames do not exist for patients or caregivers of patients managing rare conditions. Thus, we employed a two-stage mixed-sampling approach (convenience sampling followed by an attempted census) through Genetic Alliance, a nonprofit health advocacy organization with a network of more than 1500 condition-specific advocacy organizations with a total membership of 25 million people. Organizations willing to participate in the study emailed invitations to their members with a link to the online survey. Respondents received a US$5 Amazon.com gift card within 2 weeks of survey completion. Due to the sampling strategy, response rates cannot be calculated for these surveys.
Patients & caregivers managing chronic conditions
A sample of patients and caregivers managing chronic conditions was drawn using the web-enabled KnowledgePanel®, a probability-based panel designed to be representative of the US population. Study-specific invitations were sent to patient and caregiver panelists with links for survey completion. Respondents completing the survey received points equal to US$5 through Knowledge Panel's® points system, which can be redeemed for gift cards, prizes or cash. Survey completion rates, representing those who responded to the survey invitation, were 57 and 65%, respectively.
Practicing clinicians
The clinician sample – comprised of physicians, nurse practitioners and physician assistants – was drawn from multiple sources: physicians, including doctors of medicine (MD) and osteopathy (DO), were drawn from the American Medical Association's (AMA) Master File, and physician assistants (PA) and nurse practitioners (NP) were drawn from a proprietary database maintained by DMD Marketing Corporation. The clinician survey used a stratified random sample design: primary care physicians, specialty physicians and PAs and NPs. Eligible respondents were defined as clinicians currently practicing in the USA who care for patients managing chronic or rare diseases. Medical specialties with limited direct patient interaction (e.g., radiologists, anesthesiologists and pathologists) were excluded.
The clinician survey was administered using a mixed-mode approach (online and mail with phone follow-up) [16–18]. A prenotification letter with a US$2 bill was mailed to 3900 sampled clinicians informing them of the survey opportunity. Nonrespondents received an email invitation, a mailed survey, a reminder postcard and a second copy of the survey sent two weeks after the postcard; 250 clinicians were selected to receive the second copy of the survey via FedEx. Reminder telephone calls were placed, and clinicians received another reminder to complete the survey via email. To increase the response rate, a final mailing of the 18-item core survey was sent to all nonrespondents. These efforts resulted in a final response rate of 17% for the core survey and 9% for the extended survey. Clinician survey findings are based on the core survey items unless otherwise noted.
Analysis
All analyses were performed using Stata 13.1 [19]. Given the different sampling designs applied (i.e., nonprobability-based for the rare condition samples vs probability-based for the chronic condition samples), separate analyses were conducted for each survey sample. All survey data for the probability-based samples of patients and caregivers for patients managing chronic conditions and clinicians were weighted to adjust for the respondent's probability of selection and nonresponse. As a result, findings for these samples are nationally representative. Descriptive statistical analyses (e.g., frequencies) were performed and are interpreted based on the response scale.
Of specific interest were any differences in beliefs, values and attitudes across samples (i.e., patients, caregivers and clinicians) and within each sample across specific demographic characteristics. Due to the different sampling approaches applied across the patient, caregiver and clinician samples, direct statistical comparisons between samples were not performed. However, due to the presence of analogous survey items, responses across samples were descriptively compared. To examine differences within samples based on demographic characteristics (i.e., age, education, income level and number of health conditions for patients and caregivers; and age, gender, practice setting and practice type for clinicians), bivariate analyses (i.e., Chi-square tests) were conducted.
Results
Survey participants
Demographic characteristics for all survey respondents are shown in Table 1. Compared with rare disease patients and caregivers who participated in the survey, chronic condition patient and caregiver respondents were older, had less education and more had public health insurance coverage. High blood pressure (18%) and diabetes (11%) were the highest reported chronic conditions among patients. 62% of clinician respondents were MDs or DOs, 24% were NPs, and 14% were PAs. Most practiced in urban (45%) or suburban (34%) settings.
Patient & caregiver awareness of treatment options
Two-thirds of patients with chronic conditions and caregivers of patients with chronic conditions were aware of treatment options, and the majority of those (89%) were informed by a clinician. Just over half of patients with rare conditions and caregivers of those with rare conditions reported awareness of treatment options for their (or their loved ones’) condition. Of those who were aware of treatment options, the majority (82%) were informed of options by a clinician. Education was positively correlated with treatment option awareness for both patient populations; more patients with rare or chronic conditions who had a 4-year college degree or greater were aware of treatment options than those with less education (rare: 65 vs 44% of those with some college or 2-year degree and 33% of those with a high school diploma, GED, or less [χ2 (4, n = 468) = 30.1, p ≤ 0.001]; chronic: 83 vs 72% of those with some college of 2-year degree and 58% of those with a high school diploma, GED, or less [χ2 (4, n = 761) = 46.5, p ≤ 0.001]). Additionally, significantly more patients with rare conditions who had household incomes over $100,000 reported being aware of treatment options than those with lower incomes (63 vs 55% of patients with total annual household incomes between $40,000 and 100,000 and 43% of those with incomes less than $40,000 [χ2 (4, n = 452) = 14.8, p ≤ 0.01]). Income level was not found to correlate to awareness of treatment options among patients with chronic conditions.
Clinicians were identified as the primary source of information about treatment options for the majority of patients and caregivers reporting awareness of treatment options. Although most patients and caregivers reported being informed about available treatment options by their clinician (82–89% across all samples), nearly one-third of these patients and caregivers reported that their clinician did not share information specifically pertaining to the benefits and harms of those options (Figure 1). Few patients and caregivers (24–30% across all samples) reported that clinicians gave guidance about how to decide between treatment options.
Awareness of & exposure to CER findings
Few patients and caregivers were familiar with the term ‘comparative effectiveness research’ across all four samples (22–27%). Age was associated with CER familiarity for patients with chronic conditions; 64% of patients aged 18–34 years old reported being not at all familiar with CER compared with 80% of patients 35–64 years of age, and 84% of patients aged 65 years or older (χ2 [6, n = 756] = 38.4, p ≤ 0.001). No other demographic associations with CER familiarity were identified across the four samples.
When the term comparative effectiveness research was defined, patient and caregiver exposure to research evidence comparing the benefits and harms of treatment options was low. Approximately 25% of chronic condition patients and caregivers reported exposure to any type of CER findings in the past 12 months, compared with over 40% of rare condition patients and caregivers (Figure 2). Clinicians were cited as a source of CER findings by more than half of these groups, and by 72% of patients with chronic conditions. Online health communities were cited as a source of CER by 61% of rare disease patients and 63% of rare disease caregivers, compared with just 21% of chronic disease patients and 23% of chronic disease caregivers (Figure 3).
Two-thirds of clinicians reported any familiarity with the term ‘comparative effectiveness research’; with only 10% reporting being ‘very familiar’ with CER, 31% reporting being ‘somewhat’ familiar, and 26% reporting being only ‘slightly’ familiar; and one third indicating they were not at all familiar with CER. Significantly more clinicians practicing in urban settings (14%) reported being ‘very familiar’ with CER than those from suburban (6%), small-town (7%) or rural settings (10%) (χ2 [9, n = 559] = 19.9, p ≤ 0.05).
Patient & caregiver satisfaction with research evidence to make health decisions
Among patients and caregivers hearing or reading about CER for their condition, between 30 and 38% (across chronic and rare disease groups) found CER to be not at all or only slightly helpful. The most common reasons for lack of helpfulness were that the research was inconclusive, the information was similar to information they had already seen, and the information was not specific enough to help them make decisions. The majority of patients and caregivers who had read or heard about CER reported that they were left with unanswered questions at least ‘sometimes’ and between 15 and 41% endorsed ‘usually’ or ‘always’. More patients with rare conditions reported that they did not have enough information to make decisions (32 vs 9% of patients with chronic conditions).
Clinician satisfaction with existing research evidence to guide clinical decision-making
Clinician satisfaction with existing research evidence was mixed. A majority strongly or somewhat agreed (55%) that “research evidence to inform my clinical decisions takes too long to find”, and 47% strongly or somewhat agreed that “research evidence does not compare the appropriate treatments to inform my clinical decisions”.
Patient & caregiver preferences for information when making decisions
Characteristics of information about treatment options that were ‘very important’ to patients and caregivers were consistent across all groups (Figure 4). Information from a trusted source was cited as ‘very important’ when making a health decision by patient and caregiver respondents (75–92%). A clear pattern emerged of characteristics most patients and caregivers viewed as very important or important: information written in plain and understandable language (76- 80% across samples), information is actionable (68–83% across samples) and information helps you decide between treatment options (67–80% across samples).
Patient, caregiver & clinician attitudes toward CER
Despite a lack of familiarity with CER, the majority of patients and caregivers (83–97% across samples) believed that research examining the benefits and harms of different test or treatment options would be useful in making decisions. The perception of CER's usefulness ranged from 83% among caregivers of patients with chronic conditions to 97% among clinicians. More caregivers of patients with multiple health conditions report CER is useful for decision-making than those caring for patients with a single condition in both rare and chronic samples (Rare: 97 vs 91%, respectively [χ2 (1, n = 604) = 9.3, p ≤ 0.01]; Chronic: 88 vs 75%, respectively [χ2 (1, n = 753) = 19.3, p ≤ 0.001]). Overall, the majority of clinicians (69%) disagreed or strongly disagreed with the statement “CER will be used to restrict my freedom to choose treatments for my patients.”
Discussion
Given the growing interest and significant funding now dedicated to CER, understanding patient, caregiver and clinician attitudes toward and use of CER can provide critical insights on the role of research evidence in the changing healthcare landscape. Increased reliance on CER for health decision-making offers promise for patients, clinicians, insurers and policy makers to make more informed decisions at individual and population levels [1], as well as concerns about how CER will be used to inform health policy and coverage decisions [20]. Understanding how patients, caregivers and clinicians perceive, access and use research evidence, including CER specifically, can inform how CER is conducted and how findings are translated and disseminated.
The data from this study suggest that there are several critical gaps between the growing supply of CER and its current use in clinical settings. First, familiarity with CER across patients, caregivers and clinicians remains low, consistent with earlier study findings [7–9]. Once the concept is defined, CER is viewed favorably among these samples.
The second critical gap between the supply and use of CER in clinical settings is the attitudes of clinicians regarding the availability of information. More than a third of clinicians indicated concerns about the availability of research information, the time it takes to find evidence, and the appropriateness of treatment option comparisons and outcomes assessed. The growing availability of CER research from PCORI, Agency for Healthcare Research and Quality (AHRQ), NIH and other funders should improve availability of CER findings for clinicians and patients. These results indicate clinicians’ need for easy access to research evidence. Clinician views of evidence needs should be examined.
Another key finding is the disconnect between the finding that clinicians are the trusted information source on treatment options, benefits and harms for many patients, and the finding of limited clinician access to or discussion of that evidence, with implications for implementing shared decision-making [21–23]. Efforts to increase the availability of CER may be ineffective if a majority of clinicians do not discuss the evidence about the benefits and harms of treatments with their patients. Whether the increasing availability of CER findings increases use by clinicians and patients in clinical interactions will be instructive for evaluating implementation and shared decision-making strategies.
The data also suggest that online health communities are an important source of CER findings for patients with rare conditions and caregivers of patients with rare conditions. Condition-specific and population-specific online health communities have grown significantly, and CER outreach and dissemination efforts could benefit from greater focus on condition-specific online communities as channels to reach patients and caregivers.
Lastly, these gaps suggest it is critical to engage stakeholders on study design in order to build relevance and confidence in results. Patients and caregivers frequently expressed dissatisfaction with available research evidence. Commonly cited limitations include information that is inconclusive, lacks specificity or leaves patients with unanswered questions. Involving end-users in the formation of research questions and the selection of study populations, comparators and outcomes may help ensure studies address the information needs of clinicians, patients and caregivers.
Although the current study fills a critical gap in the CER evidence base, several limitations should be considered. First, because of the distinct sampling methods applied, findings for each patient and caregiver group are interpreted separately with no direct statistical comparison of findings. Second, the use of convenience samples for the rare condition samples limits external validity. Findings for these groups are only generalizable to the participating organizations reported among the final respondent samples (11 organizations for patients managing rare conditions; 21 organizations for caregivers for patients managing rare conditions). Additionally, although the sampling frames for patients and caregivers managing chronic conditions, and for clinicians were nationally representative, the extent to which respondents’ views reflect those of the broader target populations is unknown, particularly for clinicians given the lower response rates. These results rely on respondent recall and are subject to known recall biases such as salience, primacy and recency. Patient rating of options presented to them by clinicians reflect their perception only, as it cannot be known whether their clinicians truly present the full or just a partial set of the range of existing options. Further, the bivariate tests conducted were exploratory in nature and thus, no causal inferences can be made from the observed associations. Finally, new items developed through input from stakeholders and cognitive testing warrant further refinement and validation, particularly given the focus on concepts that are unfamiliar to the general public.
Future perspective
The current results indicate the need to educate patents, caregivers and clinicians about the increasing availability of CER findings and identify ways to facilitate access to and use of evidence in clinical decision-making. Over the next 5 years, we anticipate that familiarity with CER will increase as more CER research is conducted and dissemination efforts continue to grow, particularly as patients, caregivers and clinicians are increasing involved in disseminating CER findings. PCORI's process for sharing lay and clinician abstracts for all studies in a timely manner after study completion through the PCORI Translation Center is intended to support clinician and consumer access to relevant CER findings. Legislatively mandated dissemination activities for research funded through the PCOR Trust Fund pursued by the Agency for Healthcare Research and Quality (AHRQ) are particularly well suited to meeting clinician need for CER information. For example, the AHRQ web-based Systematic Review Data Repository provides increased transparency for CER reviews [24]. Even with good dissemination channels in place, the research must be useful. Ionaiddis [25] succinctly summarizes major reasons for the limited usefulness of much clinical research and cites patient-centeredness of research as one remedy. Patient-centered CER―CER that is guided by patients, caregivers and clinicians through the planning, conduct and dissemination of the research – may better meet real-world health decision-making needs.
| Demographic characteristic | Rare condition | Chronic condition | Clinicians (n = 638), % | ||
|---|---|---|---|---|---|
| Patients (n = 560), % | Caregivers (n = 609), % | Patients (n = 762), % | Caregivers (n = 776), % | ||
| Provider type: | |||||
| – Physician (MD, DO) | 62 | ||||
| – Physician's Assistant (PA) | 14 | ||||
| – Nurse Practitioner (NP/DNP) | 24 | ||||
| Practice setting: | |||||
| – Urban | 45 | ||||
| – Suburban | 34 | ||||
| – Small town | 16 | ||||
| – Rural setting | 5 | ||||
| Age: | |||||
| – 18–34 years | 15 | 18 | 21 | 25 | 9† |
| – 35–54 years | 27 | 53 | 29 | 37 | 50 |
| – 55–74 years | 39 | 28 | 42 | 32 | 41 |
| – 75 years or older | 19 | 1 | 7 | 6 | N/A† |
| Gender: | |||||
| – Female | 74 | 79 | 52 | 57 | 55 |
| Race: | |||||
| – White, non-Hispanic | 84 | 88 | 67 | 61 | 73 |
| – Black or African–American, non-Hispanic | 3 | 1 | 13 | 12 | 7 |
| – Other specified, non-Hispanic | 7 | 4 | 7 | 9 | 15 |
| – Hispanic | 5 | 7 | 13 | 18 | 6 |
| Education: | |||||
| – High school graduate, GED, or less | 11 | 8 | 44 | 42 | |
| – Some college or 2–year college graduate | 31 | 29 | 29 | 29 | |
| – 4-year college graduate or more | 58 | 62 | 27 | 29 | |
| Total household income: | |||||
| – Less than US$40,000 | 24 | 16 | 35 | 39 | |
| – US$40,000 or more | 77 | 84 | 65 | 61 | |
| Employment status: | |||||
| – Employed | 50 | 62 | 48 | 42 | |
| – Retired or disabled | 38 | 13 | 36 | 28 | |
| – Unemployed or other | 12 | 25 | 16 | 20 | |
| Insurance status: | |||||
| – A plan through an employer or a plan purchased yourself | 58 | 61 | 48 | 34 | |
| – Medicare or Medicaid | 30 | 26 | 34 | 48 | |
| – Some other government program or you get health insurance from somewhere else | 9 | 10 | 9 | 8 | |
| – Uninsured | 3 | 3 | 9 | 10 | |
†Clinician inclusion criteria for age ranged from 25 to 74 years.
DO: Doctors of osteopathy; DNP: Doctor of nursing practice; MD: Doctor of medicine; NP: Nurse practitioner; PA: Physician assistant.
Background
Recent initiatives have increased funding for comparative effectiveness research (CER), but little is known about patient, caregiver and clinician attitudes toward and use of CER.
While CER may be an important channel for improving health decision-making, more information about the availability and use of CER in the clinician/patient dyad is needed.
Methods
Online surveys of patients and caregivers managing rare and chronic conditions, and practicing clinicians were administered.
Results
Familiarity with the concept of CER is limited among all groups surveyed, including clinicians.
Approximately 25% of chronic condition patients and caregivers reported seeing any type of CER findings in the past 12 months, compared with over 40% of rare condition patients and caregivers. Among those who reported exposure to CER, over half of patients and caregivers cite healthcare professionals as a source of that information.
Only 10% of clinicians indicated they were ‘very familiar’ with CER, pointing to a functional obstacle to patient access to CER data to inform health decisions.
Less than a third of patients and caregivers who learned about treatment options for their condition from their clinician reported that clinicians also gave guidance about how to decide between treatment options.
Satisfaction with existing research was also limited; more than 1/3 of patients and caregivers who reported exposure to CER felt it left them with unanswered questions and about half of clinicians expressed concerns about the time it takes to find research and the appropriateness of the treatments that are compared.
Future perspective
Clinicians, patients and caregivers indicate unmet need for incorporating CER findings into clinical decision-making.
Despite being an important source of CER information, a gap exits in the incorporation of comparative information about treatment benefits and harms into clinician discussions with patients.
CER that is guided by patients, caregivers and clinicians through the planning, conduct and dissemination of the research may better meet real-world health decision-making needs.
Acknowledgements
The authors gratefully acknowledge the contributions of the Advisory and Working group members; partner organizations; and patients, caregivers and clinicians involved in this study.
Disclaimer
The views expressed in this paper are those of the authors and do not necessarily reflect the official views of the Patient Centered Outcomes Research Institute, nor of the American Institutes for Research.
Financial and competing interests disclosure
The study was funded by the Patient-Centered Outcomes Research Institute (contract # PCO-SCISRV2013). The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (suppl_material.pdf)
- Download
- 2.15 MB
References
Papers of special note have been highlighted as: •• of considerable interest
1.
Sox H, Greenfield S. Comparative effectiveness research: a report from the Institutes of Medicine. Ann. Intern. Med. 151(3), 203–205 (2009).
2.
Darling H. Employee attitudes toward health information and comparative effectiveness research (2011). www.changehealthcare.com/downloads/industry/02.01.2011%20NBGH%20EE%20Attitudes.pdf.
3.
Williams SS, Frost SL. Differences among consumer segments with regard to perceptions of comparative effectiveness research. J. Comp. Eff. Res. 3(6), 617–622 (2014).
4.
US Senate and House of Representatives. The Patient Protection and Affordable Care Act, Public Law. 111–148 111th Congres (2010). https://www.gpo.gov/fdsys/pkg/BILLS-111hr3590enr/pdf/BILLS-111hr3590enr.pdf.
5.
US Senate and House of Representatives. American Recovery and Reinvestment Act (ARRA) of 2009, Public Law. 111–115 111th Congress (2009). https://www.gpo.gov/fdsys/pkg/BILLS-111hr1enr/pdf/BILLS-111hr1enr.pdf.
6.
Esposito D, Yong PL, Rich E, Geonnotti K, Kimmey LD. The ARRA investment in CER: a description of the midstream evaluation and how the funds were allocated and CER priorities addressed. J. Comp. Eff. Res. 3(6), 581–589 (2014).
7.
Forsythe LP, Frank L, Walker KO et al. Patient and clinician views on comparative effectiveness research and engagement in research. J. Comp. Eff. Res. 4(1), 11–25 (2015).
•• Results from prior research that was used in the development and analysis of the current study.
8.
Cornwell D, Hu M, Esposito D. Public perceptions of comparative effectiveness research and use of evidence in healthcare decision-making. J. Comp. Eff. Res. 3(6), 623–634 (2014).
•• Prior research used to inform the current study.
9.
Keyhani S, Woodward M, Federman AD. Physician views on the use of comparative effectiveness research: a national survey. Ann. Intern. Med. 153(8), 551–552 (2010).
•• Results from prior research that was used in the development and analysis of the current study.
10.
Forsythe LP, Frank LB, Workman TA et al. Health researcher views on comparative effectiveness research and research engagement. J. Comp. Eff. Res. (2016) (Epub ahead of print).
11.
Forsythe LP, Frank LB, Workman TA, Hilliard T, Harwell D, Fayish L. Patient, caregiver, and clinician views on engagement in comparative effectiveness research. J. Comp. Eff. Res. (2016) (Epub ahead of print).
12.
Lowry SJ, Loggers ET, Bowles E, Wagner EH. Evidence gaps in advanced cancer care: community-based clinicians’ perspectives and priorities for CER. Am. J. Manag. Care 18(5 Spec No. 2), SP77–83 (2012).
13.
Reynolds C, Martin D, Dubois RW, Westrich K. Comparative effectiveness research: do employers care? What will they do? (2011). www.npcnow.org/publication/comparative-effectiveness-research-do-employers-care-what-will-they-do.
14.
Schneider EC, Epstein AM. Use of public performance reports: a survey of patients undergoing cardiac surgery. J. Am. Med. Assoc. 279(20), 1638–1642 (1998).
15.
Weidmer B, Hurtado M, Weech-Maldonado R, Ngo-Metzger Q, Bogen K. Guidelines for translating CAHPS surveys. Prepared by the CAHPS II Cultural Comparability Team (2006). https://www.ahrq.gov/cahps/surveys-guidance/helpful-resources/resources/cahpsGuidelines_Translation.html.
16.
Dillman Don A, Smyth JD, Christian LM. Internet, mail and mixed-mode surveys. John Wiley & Sons, Hoboken, NJ, USA (2009).
17.
Ziegenfuss JY, Burmeister KR, Harris A, Holubar SD, Beebe TJ. Telephone follow-up to a mail survey: when to offer an interview compared to a reminder call. BMC Med. Res. Methodol. 12(1), 32 (2012).
18.
Braddock C, Fihn S, Levinson W, Jonsen A, Pearlman R. How doctors and patients discuss routine clinical decisions: informed decision making in the outpatient setting. J. Gen. Intern. Med. 12(6), 339–345 (1997).
19.
Statacorp. Stata Statistical Software: Release 13. StataCorp LP, College Station, TX, USA (2013).
20.
Rich EC. From concept to policy: 10 years after the call for a US center for comparative effectiveness information. J. Comp. Eff. Res. 6(1), 9–11 (2016).
21.
Brom L, Hopmans W, Pasman HR, Timmermans DR, Widdershoven GA, Onwuteaka-Philipsen BD. Congruence between patients’ preferred and perceived participation in medical decision-making: a review of the literature. BMC Med. Inform. Decis. Mak. 14, 25 (2014).
22.
Bouniols N, Leclère B, Moret L. Evaluating the quality of shared decision making during the patient-carer encounter: a systematic review of tools. BMC Res. Notes 9(1), 382 (2016).
23.
Eijk MVD, Faber M, Aarts J, Kremer J, Munneke M, Bloem B. Using online communities to deliver patient-centered care to people with chronic conditions. J. Med. Internet Res. 15(6), e115 (2013).
24.
Agency for Healthcare Research and Quality. AHRQ Projects funded by the Patient-Centered Outcomes Research Trust Fund (2016). www.ahrq.gov/funding/training-grants/pcor/pcortf-di.html.
25.
Ioannidis JP. Why most clinical research is not useful. PLoS Med. 13(6), e1002049 (2016).
Information & Authors
Information
Published In
Copyright
© PCORI.
History
Published online: 8 February 2017
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Patient, caregiver and clinician use of comparative effectiveness research findings in care decisions: results from a national study. (2017) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2016-0061
Export citation
Select the citation format you wish to export for this article or chapter.