Patient, caregiver and clinician views on engagement in comparative effectiveness research
Abstract
Aim: Describe patient, caregiver and clinician views toward engagement as partners in health research. Materials & methods: Online surveys of patients and caregivers managing rare (n = 560 patients, n = 609 caregivers) or chronic conditions (n = 762 patients, n = 776 caregivers) and practicing clinicians (n = 638). Results: Over half of respondents were unfamiliar with the concept of partnering with researchers but most expressed interest in working in a research partnership. Potential facilitators endorsed were ensuring research is meaningful, applying results in an understandable way, and sharing results. Lack of time is a potential barrier. Clinicians were most interested in helping researchers decide on intervention comparisons and identifying implications for clinical practice. Conclusion: Patients, caregivers and clinicians are interested in research roles that emphasize usefulness and understandability of research.

Figure 1. Stakeholder knowledge, attitudes and experiences of comparative effectiveness research engagement.
Percentages are weighted for patients managing chronic conditions and clinicians. For patient and caregiver samples, the past experience with research question was only asked of those who reported being at all familiar with studies that include patients and/or caregivers. The percentage shown represents the proportion of those with past experience as research partners out of the respective whole sample. Patients and caregivers were not asked about their familiarity with clinician–researcher partnerships.
CER: Comparative effectiveness research.
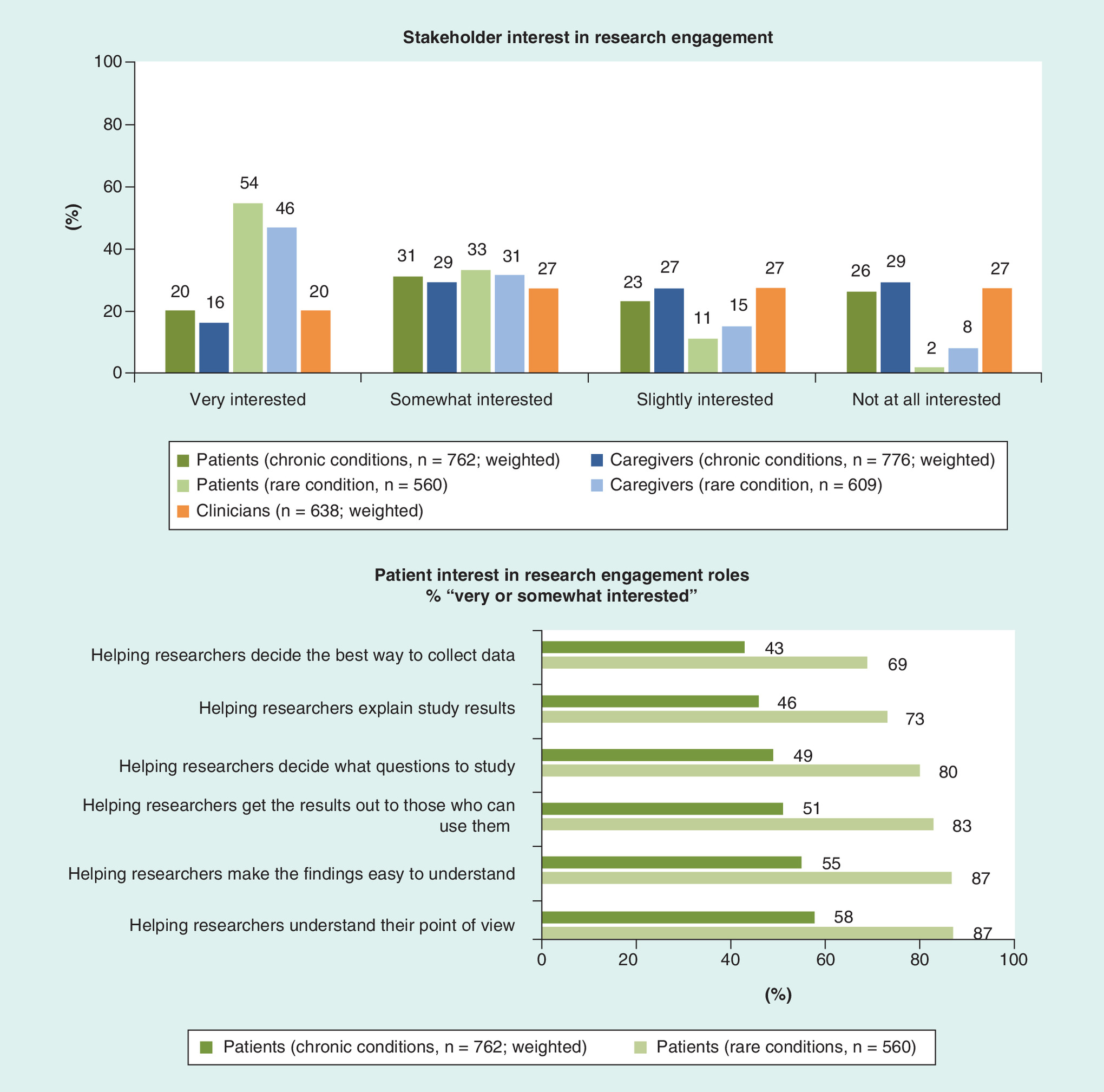
Figure 2. Stakeholder interest in comparative effectiveness research engagement.
Percentages are weighted for patients managing chronic conditions and clinicians. Caregiver interest in engagement roles was nearly identical to that of patients within each condition type and thus, results for caregivers are not shown.
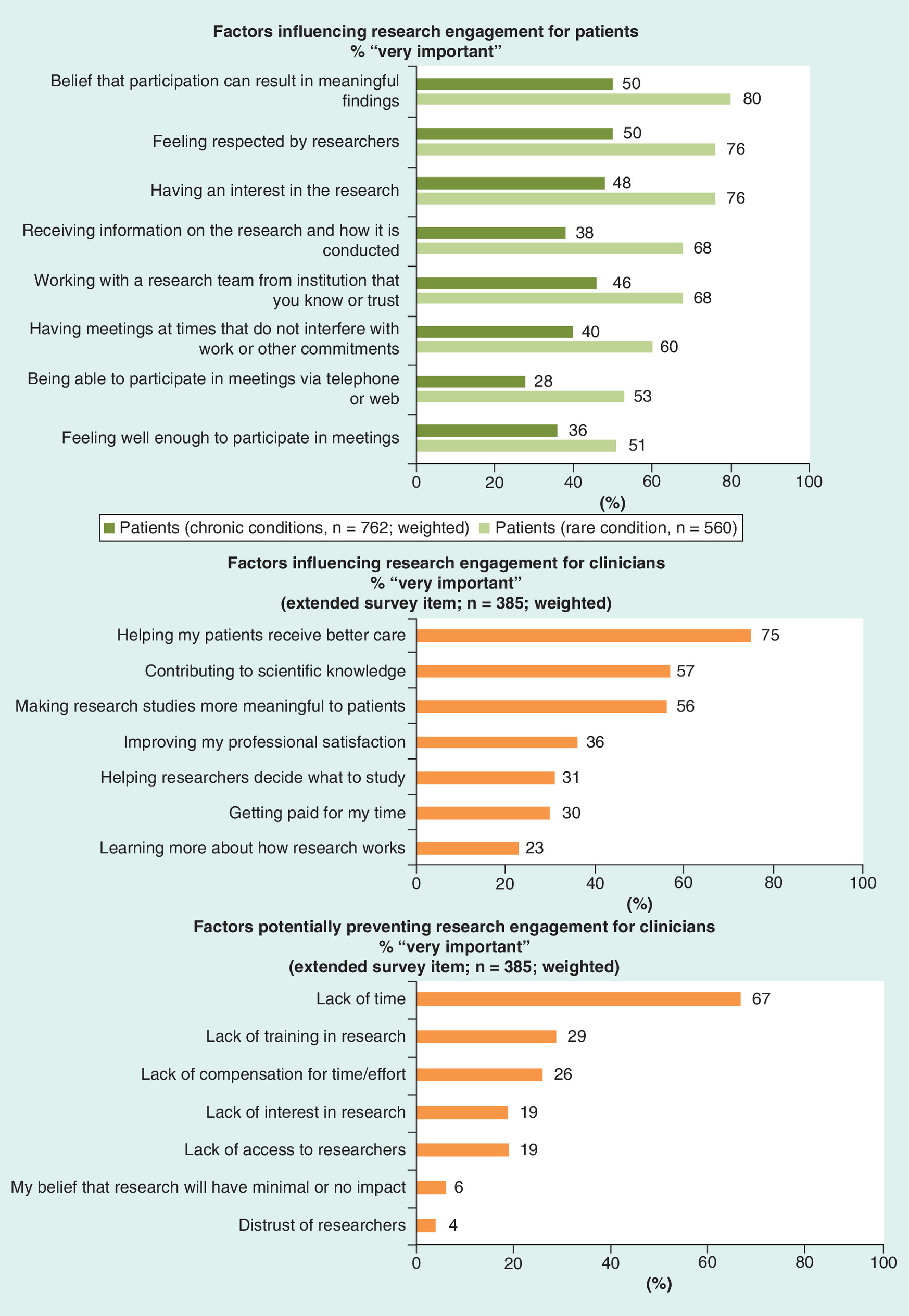
Figure 3. Factors influencing stakeholder engagement in research.
Percentages are weighted for patients managing chronic conditions and clinicians. Caregiver endorsement of factors influencing research engagement was nearly identical to that of patients with each condition type and thus, results for caregivers are not shown.
First draft submitted: 30 August 2016; Accepted for publication: 15 December 2016; Published online: 8 February 2017
Comparative effectiveness research (CER) evaluates the effectiveness and safety of different preventive, diagnostic and treatment options, and CER findings are intended to enhance the evidence base for clinical decision-making [1]. Interest in engaging patients, caregivers and clinicians in the design, conduct and dissemination of CER has grown as the practice of ‘patient-centered’ outcomes research has expanded [2,3]. For example, US FDA and the UK's National Health Service actively involve stakeholders in the research process [4–7], and the Patient-Centered Outcomes Research Institute (PCORI) requires research engagement in the patient-centered CER it funds [8]. Engaging patients, caregivers, clinicians and others in CER as research partners may offer potential benefits including improved researcher understanding of the target population, more relevant and patient-focused objectives, research questions and outcomes, and improved translation into clinical practice [4,9–13]. While the evidence of the impact of engagement in research is emerging, little is known about stakeholder views on engaging in research.
Previous studies have found that patients and clinicians believe that engagement can increase research value and usefulness [14,15]. Evidence on strategies to facilitate research engagement is still lacking, however. Specifically, there are no data on these stakeholders’ awareness of opportunities for research engagement, what partnership roles are most meaningful to them, and what factors affect their decisions to engage [16]. There is evidence that health researchers perceive specific challenges to engagement: finding the appropriate research engagement partners, establishing trust with stakeholders and gaps in training on effective stakeholder–researcher partnerships [13]. Understanding the perceived challenges to engagement and the nuances of creating and sustaining partnerships from the perspective of potential partners is critical to identifying promising practices for engagement and strategies to support research engagement. Prior studies used relatively small, self-selected samples, and the prior survey study used opt-in crowd-sources samples with associated selection bias. To fill these gaps, PCORI commissioned surveys to assess patient, caregiver and clinician views of partnering with researchers in the planning, conduct and dissemination of CER. Caregivers are included as key stakeholders given that in the USA over 40 million people serve as informal caregivers for loved ones and given their involvement in medical decision-making based on health information [17]. While patients as a group are important healthcare stakeholders, prior work indicates differences by chronic and rare disease status in health information seeking and use [14], and PCORI's legislative mandate requires attention to chronic disease and rare disease. Understanding the needs of these two types of patient groups separately is therefore warranted. The surveys are part of a larger effort to understand the beliefs, values and needs of various stakeholder groups, including researchers, about CER, patient-centered approaches to research and the use of evidence-based information in health decisions.
Materials & methods
Stakeholder input
Survey design was informed by a project-specific advisory group comprised of 11 representatives of patient advocacy organizations, medical societies, patient engagement researchers and comparative effectiveness researchers; along with three, eight-member working groups specific to each survey audience – patients, caregivers and clinicians. These groups assisted in the development of the final set of survey domains, guided revisions based on cognitive testing, provided suggestions for sampling and input into interpretation of the results, contributed to the determination of key findings and their implications for PCORI and patient-centered outcomes research, and provided input for dissemination activities (e.g., webinars).
Measures
Surveys were developed and administered to: patients managing rare conditions; patients managing chronic conditions; caregivers of patients managing rare conditions; and caregivers of patients managing chronic conditions. An analogous survey was developed for practicing clinicians. A literature review and key informant interviews with stakeholder representatives revealed several evidence gaps relative to stakeholder views of and experiences with research engagement.
Primary survey domains included:
The level of awareness and perceived value among stakeholders of CER engagement;
Past experience with and interest and preferred roles in partnering with researchers to produce CER; and
Perceived facilitators of, and perceived challenges to, engaging in research partnerships.
Other survey domains (findings reported separately) assessed level of awareness and perceived value of CER and patient-centered CER, as well as experiences and attitudes regarding the availability and use of information when deciding about a test or treatment. Relevant survey items from related studies were reviewed, as were items from prior PCORI data collection efforts [15,18–22]. Items were created to address domains for which no existing item could be found. Draft surveys were tested and revised for each audience through cognitive interviews to ensure clarity and relevance. Spanish language versions of the patient survey items and instructions were developed [23]. Two independent and certified translators from two different countries of origin completed forward translation of the survey items and those versions were reconciled by three additional reviewers.
Two versions of the clinician survey were developed: a core survey consisting of 18 questions; and an extended version that included the core survey questions and 25 supplemental questions assessing general practice approaches for patients with chronic or rare conditions and clinician engagement in research. See the Supplementary Material for full instruments.
Familiarity with CER engagement
Patient and caregiver involvement in medical research was defined on the survey as getting involved in other ways besides being research subjects, to: ‘help decide what research is done and how it is done; help decide the best way to collect data; help researchers explain the results of the study; and help researchers understand the patient and caregiver points of view’. Patients and caregivers then reported their level of familiarity with studies where patients or caregivers partner with the research team to decide what research is done and how it is done on a 4-point scale from 1 (very familiar) to 4 (not at all familiar). On the clinician survey, patient engagement in research was defined as partnering with researchers to: ‘decide which interventions to compare, identify and collect data, analyze the data, identify key findings for clinical practice and communicate study findings’. Clinicians reported their level of familiarity with research that included patients as partners (4-point scale from very familiar to not at all familiar), and were also asked about their level of familiarity with including clinicians as partners to decide what research is done or how it is done in a separate question.
Perceptions of the value of CER engagement
Patients, caregivers and clinicians selected one of the two statements indicating which represented their view regarding whether stakeholders partnering with researchers would improve the value of medical research for informing treatment decisions. Patients and caregivers also indicated how likely it is that such partnerships would improve the quality of information available to help patients and families make medical decisions (4-point scale from very likely to not at all likely). The extended clinician survey asked clinicians to indicate how valuable (4-point scale from very valuable to not at all valuable) the involvement of clinicians as partners would be to specific types of research.
Experience engaging with researchers as partners
Patients and caregivers reported whether they had ever partnered with a research team to decide what research is done and how it is done (i.e., dichotomous yes or no response). Clinicians reported whether they had ever engaged with researchers and in what roles by selecting all that applied (i.e., 0 = unselected/1 = selected binary response) from an item list.
Interest in research engagement
Patients, caregivers and clinicians indicated their overall interest in partnering with a research team to plan or conduct a study (4-point scale from very interested to not at all interested). Patients, caregivers and clinicians (extended survey) also indicated their level of interest in partnering with researchers in specific roles.
Barriers & facilitators to research engagement
Patients and caregivers were asked to indicate how important each factor from a list of potential facilitators and barriers was in determining whether they would participate as part of a research team (4-point scale from very important to not at all important; Patient Survey item 25, Caregiver Survey item 35). The list of facilitators and barriers was developed from literature on participation in clinical trials and engagement in research, and refined through prior survey testing with patients and clinicians [15]. The extended clinician survey included separate questions assessing the importance of specific factors in facilitating and preventing them from partnering with researchers to design or conduct research (4-point scale from very important to not at all important; Clinician Survey items 26–27). Clinicians were also asked to select the top three benefits of partnering with a research team to plan or conduct a study from a list of potential outcomes.
Sampling & data collection
Distinct sampling approaches were developed and applied for each of the target populations. Online surveys for patients managing rare or chronic conditions were administered between September and October 2014. Patient surveys were completed in English or Spanish, based on the participant's preference. Surveys of caregivers for patients managing rare or chronic conditions were administered online in January 2015 in English only. The clinician survey was administered between December 2014 and January 2015. The American Institutes for Research Institutional Review Board approved this study.
Patients & caregivers managing rare conditions
Nationally representative sampling frames do not exist for patients or caregivers managing rare conditions. Thus, we employed a two-stage mixed sampling approach (convenience sampling followed by an attempted census). Genetic Alliance, a nonprofit health advocacy organization with a network including more than 1500 condition-specific advocacy organizations, provided access to 25 million people with a wide variety of rare genetic conditions. Genetic Alliance distributed survey invitations with a link to the online survey to interested rare condition advocacy organizations for distribution to their entire membership via email. Respondents received a US$5 electronic gift card for Amazon.com within 2 weeks of survey completion. Due to the sampling strategy, survey response rates cannot be calculated for these samples.
Patients & caregivers managing chronic conditions
The samples of patients and caregivers managing chronic conditions were conducted using the web-enabled KnowledgePanel®, a probability-based panel designed to be representative of the US population. Patients were defined as self-identifying individuals as having one of a list of 26 common chronic conditions. Caregivers were defined as self-identifying individuals providing unpaid care for someone with a chronic condition, including “taking a family member or friend of any age to the doctor or helping them with medical decisions or other caregiving responsibilities”. Persons in randomly selected households using telephone numbers and residential addresses are then invited by telephone or by mail to participate in the web-enabled KnowledgePanel. For those who agree to participate but who do not already have internet access, KnowledgePanel provides at no cost a laptop and ISP connection. Panelists then receive unique log-in information for accessing surveys online and are sent emails inviting them to participate in research. Study-specific invitations were sent to patient and caregiver panelists with links for survey completion. Respondents received points equivalent to US$5 through KnowledgePanel's points system for completing the survey, which could be redeemed for gift cards, prizes or cash. Survey completion rates (panelists who responded to the survey invitation) for patient and caregiver panelists managing chronic conditions were 57 and 65%, respectively.
Practicing clinicians
The clinician survey used a stratified random sample design with three strata: primary care physicians; specialty physicians; and physician assistants (PAs) and nurse practitioners (NPs) obtained from the American Medical Association's Master File and a proprietary database from DMD Marketing Corporation. Eligible respondents were defined as clinicians (i.e., doctors of medicine [MD] and osteopathy [DO], PAs and NPs) currently practicing in the USA (50 states and the DC), excluding US possessions and territories, who have direct patient contact and care for patients managing chronic or rare diseases. Medical specialties with limited direct patient interaction (e.g., radiologists, anesthesiologists and pathologists) were excluded.
The clinician survey was administered using a mixed-mode approach (online and mail with phone follow-up), according to best practices for maximizing response rates [24–26]. A prenotification letter, including a US$2 bill, was mailed to 3900 sampled clinicians informing them of the survey opportunity. Within 2 weeks of the prenotification letter, the extended survey was distributed by mail, and a URL and pin number were emailed to clinicians with an available email address for online survey completion. This was followed by reminder post cards and emails, a second mailing of the extended survey, and reminder telephone calls. To boost the response rate, a final mailing of the 18-item core survey was sent to all nonrespondents. Potential respondents received up to six invitations or reminders about the survey. These efforts resulted in a final clinician survey response rate of 17% for the core survey and 9% for the extended survey. Reported clinician survey findings correspond to responses to the core survey items unless otherwise noted.
Analysis
All analyses were performed using Stata 13.1 [27]. Given the different sampling designs applied (i.e., nonprobability based for the rare condition samples vs probability based for the chronic condition samples), separate analyses were conducted for each survey sample. All survey data for the probability-based samples of patients and caregivers for patients managing chronic conditions, and clinicians were weighted to adjust for the respondent's probability of selection and nonresponse; findings for these samples are nationally representative. Descriptive statistical analyses (e.g., frequencies) were performed and are interpreted based on the response scale.
Results
Survey participants
The final survey samples included 560 patients and 609 caregivers of patients managing rare conditions and 762 patients and 776 caregivers of patients managing chronic conditions. The core clinician survey was completed by 638 providers; 60% (n = 385) of these clinicians responded to additional items on the extended survey.
Demographic characteristics for all survey respondents are shown in Table 1. Samples of patients and caregivers were predominantly white, non-Hispanic; female; with reported annual household income of US$40,000 or more. More patients and caregivers managing chronic conditions reported being over the age of 55 years, having a high school degree or less, and coverage through public health insurance programs than patients and caregivers managing rare conditions. Transverse myelitis (26%) and pemphigus (20%) were the highest reported rare conditions among patients, and high-blood pressure (18%) and diabetes (11%) were the highest reported chronic conditions among patients. Most clinicians were female (55%), white, non-Hispanic (73%), and reported practicing in an urban (45%) or suburban (34%) setting. Sixty-two percent of clinician respondents were MDs or DOs, 24% were NPs and 14% were PAs.
Patient, caregiver & clinician knowledge, attitudes and experiences of CER engagement
Across all outcomes, findings for patients and caregivers managing rare conditions were similar, as were findings for patients and caregivers managing chronic conditions. Awareness of research studies in which patients and/or caregivers are engaged as partners “to decide what research is done and how it is done” was limited across stakeholders (Figure 1). Over half of the patients, caregivers and clinicians reported no familiarity with patient and/or caregiver research partnerships. Clinicians were more familiar with clinician–researcher partnerships: 60% reporting being very, somewhat or slightly familiar with this type of engagement.
The majority of stakeholders reported that patients partnering with researchers would improve both the value of research and the quality of information available for informing treatment decisions. Nearly all patients (97%) and caregivers (95%) managing rare conditions endorsed the view that engagement would improve the value of research (i.e., a yes response), compared with 86 and 79% of patients and caregivers managing chronic conditions, respectively. Further, 96% of patients and 95% of caregivers of patients managing rare conditions reported that research engagement was very or somewhat likely to improve information quality, compared with 80% of patients and 71% of caregivers for patients managing chronic conditions.
Clinicians were also optimistic about stakeholder partnerships improving the value of research; 97% endorsed clinician–researcher partnerships and 83% endorsed patient–researcher partnerships as improving the value of research. In the extended survey, most clinicians reported that clinician engagement as partners would be very valuable to studies that compare different treatments to each other (61%) and randomized controlled trials (56%); less than half of clinicians considered clinician partnerships to be very useful for systematic reviews or meta-analyses (45%), studies comparing different populations (44%), cost–effectiveness studies (43%) and observational studies (42%).
More clinicians reported having engaged with researchers as partners in the past than patients and caregivers (38% of clinicians compared with <7% of patient and caregivers). Among clinicians who reported a personal history of engagement with researchers, the most common role was helping researchers identify and collect data (33%). Fifteen percent or fewer reported ever helping researchers decide which interventions to compare, helping researchers analyze data, helping researchers identify key findings and implications for clinical practice, helping researchers communicate study findings to other clinicians or developing clinical guidelines based on study findings.
Stakeholder interest in research engagement
Two-thirds of patients and caregivers managing rare conditions reported being very or somewhat interested in research engagement (Figure 2). About half of the patients and caregivers managing chronic conditions reported this level of interest. While respondents expressed interest in a variety of roles, patients and caregivers had the most interest in helping researchers understand patient/caregiver points of view about needed information, make findings easier to understand, and get results to those who can use them. Close to half of the patients and caregivers also reported wanting to help researchers decide what research questions to study and explain the study results to other patients and caregivers. Less interest was expressed in helping researchers decide the best way to collect data. Interest in specific partnership roles was higher among patients and caregivers managing rare conditions compared with those managing chronic conditions.
Nearly half of the clinicians reported being very or somewhat interested in research engagement. As reported on the extended survey, clinicians were most interested in helping researchers decide which interventions to compare (60%), identifying key implications of study findings for clinical practice (56%), communicating findings to other clinicians (55%), developing clinical guidelines based on research findings (55%) and determining how to collect data from patients and/or clinicians (52%). Clinicians were least interested in helping researchers analyze data (34%).
Factors influencing patient, caregiver and clinician engagement in research
The most commonly cited factors influencing patient and caregiver decisions to engage in research were the belief that their participation could result in meaningful findings, feeling respected by the researchers, and having an interest in the research being conducted (Figure 3). Patients also commonly endorsed working with a research team from an institution or healthcare organization that they know or trust (68% of patients managing rare conditions and 46% of patients managing chronic conditions); receiving information on the research and how it is conducted (68% of patients managing rare conditions and 38% of patients managing chronic conditions); having meetings at times that do not interfere with work or other commitments (60% of patients managing rare conditions and 40% of patients managing chronic conditions); and being able to participate in meetings virtually via telephone or web (53% of patients managing rare conditions and 28% of patients managing chronic conditions).
More than half (51%) of the patients managing rare conditions reported that feeling well enough to participate in meetings was a very important factor affecting engagement compared with 36% of patients managing chronic conditions. In addition, close to half (46%) of patients managing rare conditions reported having family support as a key factor in deciding whether to engage in research partnerships compared with a third of patients managing chronic conditions. Further, about a third of patients and caregivers managing rare conditions reported that encouragement to participate by a research team, healthcare professionals and patient advocacy or support groups was important in deciding whether to engage in research.
Facilitators of engagement most commonly identified as very important among clinicians (extended survey) were helping patients receive better care (75%), contributing to scientific knowledge (57%) and making studies more meaningful to patients (56%). Fewer clinicians identified improving their professional satisfaction (36%), helping researchers decide what to study (31%), getting paid for their time (30%) and learning more about how research works (23%) as very important factors. The top perceived benefits of partnering with researchers reported by clinicians (extended survey) were: the improvement of treatment decisions resulting from the study (84%); the evidence that clinicians could help create to inform their practice and better assist their patients (70%); the value that they could bring as a clinician to inform the research (45%); and the knowledge they would gain about the research process (41%). Less than 20% of clinicians reported developing long-term relationships with a research team, the financial remuneration received (14%), the support or approval that they would receive from their health delivery organization (14%) and potential career advancement from participating (9%) as benefits of engagement.
Clinicians overwhelmingly reported lack of time as a potential barrier to research engagement (67% endorsed as ‘very important’). Other potential barriers commonly cited as ‘very important’ include lack of training in research (29%), lack of compensation for time and effort (26%) and lack of access to researchers (19%). Few clinicians cited the potential that the research would have minimal or no impact on their patients’ health (6%) and distrust of researchers (4%) as potential barriers.
Discussion
Although patients, caregivers and clinicians reported limited awareness of and experience with engagement in CER, the majority of each group perceived such partnerships as valuable to producing research that improves medical decision-making. As most medical research has operated from the traditional paradigm in which clinicians provide access to or recruit patients and caregivers as study subjects, it is not surprising that clinicians are more familiar with clinician–researcher partnerships than partnerships that engage patients and caregivers in the conduct of research. Research paradigms are evolving toward more to active involvement of stakeholders in the research process, and stakeholder awareness and experience will be of interest as these changes spread.
Patients and caregivers managing chronic or rare conditions, as well as clinicians, expressed interest in working with researchers as partners, suggesting there are a variety of potential partners within the healthcare community. A particularly large proportion of rare-condition respondents expressed interest in engagement. Patients and caregivers managing rare conditions may be particularly drawn to engagement because of frustrations with the general lack of resources for rare conditions compared with chronic conditions [28]. These patients and caregivers may also be more activated for engagement in research as a result of affiliations with advocacy organizations [29]. Such organizations continue to play a vital role in engaging patients, families and communities in clinical and translational research [11,30–32].
Patients and caregivers in this study expressed interest in engaging in the research process in multiple ways but were particularly interested in helping researchers understand what kind of information they need, making results easy to understand, and disseminating findings to others who can use them. Similarly, clinicians were especially interested in helping researchers determine the interventions that are most meaningful to compare, assess implications for clinical practice and disseminate findings. While there has been growing emphasis on engagement in research topic prioritization and question development, partnership in translation and dissemination of results presents an opportunity to involve partners in ways they perceive as meaningful and to potentially enhance the uptake of findings in health decision-making.
Patients, caregivers and clinicians all endorsed the importance of making research more meaningful to patients and improving patient care as motivating decisions to engage with researchers. Patients and caregivers also highlighted the importance of respect from the researchers and trust in the team, as well as interest in the work. However, practical barriers to participation, such as lack of time because of work or caregiver responsibilities, can pose challenges. Differences between types of patients bear further attention. The finding that proportionately more rare-condition than chronic-condition patients cited feeling well enough to participate and family support for their participation as facilitators of research engagement may relate to differences among those with rare versus chronic conditions in disease severity and/or impacts of the conditions functioning.
Lack of time was the predominant barrier to research partnerships for clinicians. A shift toward involving clinicians on those areas that are perceived as most meaningful (e.g., determining interventions to compare, and interpreting and disseminate findings) may optimize their input and minimize their time commitments relative to more traditional roles like study-participant recruitment. A notable portion of clinicians in this study also reported that lack of training in research would be a barrier to engagement. Equipping both researchers and partners with the skills to support successful partnerships has been a focus for PCORI and others [33]. PCORI supports several efforts to address these issues, including funding opportunities for developing research partnerships and for developing training and building capacity for engagement [34,35].
Taken together, the survey findings point to practical steps researchers seeking to partner with patients, caregivers and clinicians can take to optimize the reach and value of CER. When approaching stakeholders about partnerships, researchers should clearly identify upfront the potential of the study to provide meaningful information for real-world decision-making. Drawing links between the research and possible effects on related treatment decisions, as well as potential benefits for other patients, caregivers or providers may aid in attracting committed research partners. Further, acknowledging and incorporating mechanisms to address practical barriers to partnerships for these stakeholders, establishing rapport and mutually respectful relationships through every interaction, and creating a culture of transparency in research are ways the research community potentially can foster stronger relationships with patients, caregivers and clinicians in conducting CER.
A foundational step in facilitating greater stakeholder engagement is to establish an organizational research culture that values engagement. Interest in patient-engaged research has grown considerably in recent years, and has been bolstered by provisions in the American Recovery and Reinvestment Act, as well as efforts by PCORI and endorsements from leaders across the field of health research [12]. Research teams can promote engagement as an important element of the research process by partnering with patients and other stakeholders for planning and conducting their research; participating in cultural competency and other training to ensure the research team is cognizant of sensitivities; and evaluating the impact of engaging stakeholders in their research and communicating best strategies to other investigators.
Researchers also can use technology, such as interactive video, to involve partners with less intrusion on their time. The literature suggests that hands-on training and user-friendly tools and resources for stakeholder engagement would help researchers better integrate engagement into their research projects [4,16]. Researchers have also expressed a need for more training on research partnerships. Funders, advocacy organizations and researchers can leverage existing PCORI resources or create new avenues for facilitating clinician education and strengthening their expertise in CER concepts and applications. Several PCORI initiatives, such as Pipeline to Proposals, provide a foundation for researchers to engage diverse stakeholder groups through tailored approaches, underscoring the importance of stakeholders as valued research partners [34].
This work fills a critical gap in the CER evidence base, given limited sample size and limited generalizability of prior studies (e.g., 14). However, several limitations should be considered. First, because of the distinct sampling methods applied, findings for each patient and caregiver group are interpreted separately with no direct statistical comparison of findings. Second, given the use of convenience samples for the rare condition samples, findings have limited generalizability beyond the membership of the participating organizations (11 organizations for patients managing rare conditions; 21 organizations for caregivers for patients managing rare conditions). Additionally, although the sampling frames for patients and caregivers managing chronic conditions and for clinicians were nationally representative, the extent to which respondents’ views reflect those of the broader target populations is unknown, particularly for clinicians given the lower response rates. Whether condition severity is related to attitudes toward research engagement cannot be discerned from this sample. Further, although this study included a variety of clinicians including physicians, PAs and NPs, other types of clinicians, such as pharmacists or mental healthcare providers, may have different experiences and attitudes. Finally, new items developed through input from stakeholders and cognitive testing warrant further refinement and validation, particularly given the focus on concepts that are unfamiliar to the general public.
Future perspective
As patient-engaged research becomes available to the public that can be used in healthcare decision-making, we foresee an increased demand for CER that fully incorporates stakeholder needs and interests. Given the interest of all of these stakeholder groups in engaging in roles that emphasize the usefulness, meaningfulness and understandability of research results, we envision a shift from involvement of research partners in primarily research topic prioritization and research subject recruitment to meaningful contributions in all phases of the research process including results translation and dissemination. Early evidence indicates net positive benefits to research engagement, and should that trend continue, the culture of stakeholder engagement in CER is likely to strengthen. Within the last 5 years the FDA, European Medicines Agency, and national research funding authorities like PCORI and the National Institute for Health Research (NIHR) in the UK have expanded attention to research partnerships. As research paradigms shift toward end-user participation, empirically based information will be increasingly needed to support strategies for efficient and meaningful research partnership formation and maintenance.
| Demographic characteristic | Rare condition | Chronic condition | Clinicians (n = 638), % | ||
|---|---|---|---|---|---|
| Patients (n = 560), % | Caregivers (n = 609), % | Patients (n = 762), % | Caregivers (n = 776), % | ||
| Provider type: | |||||
| – Physician (MD, DO) | 62 | ||||
| – Physician's assistant (PA) | 14 | ||||
| – Nurse practitioner (NP/DNP) | 24 | ||||
| Practice setting: | |||||
| – Urban | 45 | ||||
| – Suburban | 34 | ||||
| – Small town | 16 | ||||
| – Rural setting | 5 | ||||
| Age: | |||||
| – 18–34 years | 15 | 18 | 21 | 25 | 9† |
| – 35–54 years | 27 | 53 | 29 | 37 | 50 |
| – 55–74 years | 39 | 28 | 42 | 32 | 41 |
| – 75 years or older | 19 | 1 | 7 | 6 | N/A |
| Gender: | |||||
| – Female | 74 | 79 | 52 | 57 | 55 |
| Race: | |||||
| – White, non-Hispanic | 84 | 88 | 67 | 61 | 73 |
| – Black or African–American, non-Hispanic | 3 | 1 | 13 | 12 | 7 |
| – Other specified, non-Hispanic | 7 | 4 | 7 | 9 | 15 |
| – Hispanic | 5 | 7 | 13 | 18 | 6 |
| Education: | |||||
| – High school graduate, GED or less | 11 | 8 | 44 | 42 | |
| – Some college or 2-year college graduate | 31 | 29 | 29 | 29 | |
| – 4-year college graduate or more | 58 | 62 | 27 | 29 | |
| Total household income: | |||||
| – Less than US$40,000 | 24 | 16 | 35 | 39 | |
| – US$40,000 or more | 77 | 84 | 65 | 61 | |
| Employment status: | |||||
| – Employed | 50 | 62 | 48 | 42 | |
| – Retired or disabled | 38 | 13 | 36 | 28 | |
| – Unemployed or other | 12 | 25 | 16 | 20 | |
| Insurance status: | |||||
| – A plan through an employer or a plan purchased yourself | 58 | 61 | 48 | 34 | |
| – Medicare or Medicaid | 30 | 26 | 34 | 48 | |
| – Some other government program or you get health insurance from somewhere else | 9 | 10 | 9 | 8 | |
| – Uninsured | 3 | 3 | 9 | 10 | |
Percentages are weighted for patients and caregivers managing chronic conditions and clinicians. Shaded cells indicate N/A survey items.
†Inclusion criteria for practicing clinicians sampled only those from age 25 to 74 years.
DO: Doctor of osteopathy; DNP: Doctor of nursing practice; GED: General education development or graduate equivalency degree; MD: Doctor of medicine; N/A: Not applicable; PA: Physician assistant.
Background
Partnerships among researchers, patients, caregivers and clinicians can help ensure that comparative effectiveness research (CER) focuses on the needs of patients in real-world clinical settings, but little is known about stakeholder views on engaging in research.
Methods
Surveys of patients and caregivers managing rare and chronic conditions, and practicing clinicians were administered to examine attitudes toward research engagement.
Results
Familiarity with stakeholder-engaged CER is limited among patients and caregivers managing rare or chronic conditions, and clinicians. These stakeholders support such partnerships as likely to improve the value of research and quality of information available to inform medical decision-making.
Patients and caregivers were most interested in helping researchers understand their points of view, making research findings easier to understand, and helping the results reach others who would benefit from the information.
Primary facilitators of engagement for patients and caregivers were in the belief that their contribution would result in meaningful findings, feeling respected by researchers, and being interested in the research. Partnering with researchers from trusted institutions and receiving adequate information on the research to be done were also important factors. Potential obstacles include not feeling well enough to participate in meetings and interference with work or other life commitments.
Clinicians were most interested in helping researchers decide which interventions to compare, determining clinical practice implications and sharing CER information with other clinicians.
Facilitators of engagement among clinicians were motivation to help patients receive better care, contributing to scientific knowledge and increasing the meaningfulness of research studies for patients. The most commonly reported barrier was lack of time, followed by lack of training in research.
Future perspective
Patients, caregivers and clinicians expressed interest in partnering with researchers, suggesting that there are a variety of potential partners within the healthcare community.
Patient, caregiver and clinician interest in research roles that emphasize the usefulness, meaningfulness and understandability of research may point the way for researchers to facilitate multistakeholder partnerships.
Researchers seeking to engage these stakeholders as partners are encouraged to clearly convey how their research project may impact-related treatment decisions and may benefit other patients, caregivers or clinicians at the onset of recruitment.
Acknowledgements
We gratefully acknowledge the contributions of the Advisory and Working group members; partner organizations; and patients, caregivers and clinicians involved in this study.
Disclaimer
The views expressed in this paper are those of the authors and do not necessarily reflect the official views of the Patient Centered Outcomes Research Institute, nor of the American Institutes for Research.
Financial and competing interests disclosure
The study was funded by the Patient-Centered Outcomes Research Institute (contract # PCO-SCISRV2013). The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (suppl_material.pdf)
- Download
- 2.15 MB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Sox H, Greenfield S. Comparative effectiveness research: a report from the Institutes of Medicine. Ann. Intern. Med. 151(3), 203–205 (2009).
2.
D'arcy LP, Rich EC. From comparative effectiveness research to patient-centered outcomes research: policy history and future directions. Neurosurg. Focus 33(1), E7 (2012).
•• Provides a context for patient engagement in comparative effectiveness research.
3.
Selby JV, Forsythe L, Sox HC. Stakeholder-driven comparative effectiveness research: an update from PCORI. J. Am. Med. Assoc. 314(21), 2235–2236 (2015).
4.
Domecq JP, Prutsky G, Elraiyah T et al. Patient engagement in research: a systematic review. BMC Health Serv. Res. 14(1), 89 (2014).
5.
Food and Drug Administration. The Voice of the Patient: A Series of Reports from FDA's Patient-Focused Drug Development Initiative (2016). www.fda.gov/ForIndustry/UserFees/PrescriptionDrugUserFee/ucm368342.htm.
6.
National Institute for Health Research. INVOLVE Project (2015). www.invo.org.uk/about-involve/.
7.
Uk Department of Health. Equity and excellence: liberating the NHS (2010). www.gov.uk/government/uploads/system/uploads/attachment_data/file/213823/dh_117794.pdf.
8.
Patient-Centered Outcomes Research Institute. Vision & Mission (2015). www.pcori.org/vision-mission.
9.
Staley K. Exploring Impact: Public Involvement In NHS, Public Health And Social Care Research. INVOLVE, Eastleigh, UK (2009).
10.
Brett J, Staniszewska S, Mockford C et al. Mapping the impact of patient and public involvement on health and social care research: a systematic review. Health Expect. 17(5), 637–650 (2014).
11.
Forsythe LP, Szydlowski V, Murad MH et al. A systematic review of approaches for engaging patients for research on rare diseases. J. Gen. Intern. Med. 29(Suppl. 3), S788–S800 (2014).
12.
Esmail L, Moore E, Rein A. Evaluating patient and stakeholder engagement in research: moving from theory to practice. J. Comp. Eff. Res. 4(2), 133–145 (2015).
•• Provides practical context for the engagement of patients and stakeholders in research.
13.
Forsythe LP, Ellis LE, Edmundson L et al. Patient and stakeholder engagement in the PCORI pilot projects: description and lessons learned. J. Gen. Intern. Med. 31(1), 13–21 (2015).
• Prior research used for development of the current study.
14.
Williams SS, Esposito D, Rich EC. Patients and clinicians as stakeholders in comparative effectiveness research: multiple perspectives and evolving roles. J. Comp. Eff. Res. 3(6), 573–575 (2014).
15.
Forsythe LP, Frank L, Walker KO et al. Patient and clinician views on comparative effectiveness research and engagement in research. J. Comp. Eff. Res. 4(1), 11–25 (2015).
•• Results from prior research that were used in the development and analysis of the current study.
16.
Concannon TW, Fuster M, Saunders T et al. A systematic review of stakeholder engagement in comparative effectiveness and patient-centered outcomes research. J. Gen. Intern. Med. 29(12), 1692–1701 (2014).
17.
National Alliance for Caregiving, American Association of Retired Persons. Caregiving in the US. The National Alliance for Caregiving, Bethesda, MD, USA (2015).
18.
Lowry SJ, Loggers ET, Bowles E, Wagner EH. Evidence gaps in advanced cancer care: community-based clinicians’ perspectives and priorities for CER. Am. J. Manag. Care 18(5 Spec No. 2), SP77–SP83 (2012).
19.
Dubois RW, Reynolds C. Comparative effectiveness research: do employers care? What will they do? What about productivity outcomes? J. Occup. Environ. Med. 53(7), 708–710 (2011).
20.
Cornwell D, Hu M, Esposito D. Public perceptions of comparative effectiveness research and use of evidence in healthcare decision-making. J. Comp. Eff. Res. 3(6), 623–634 (2014).
• Prior research used to inform the current study.
21.
Frank LB, Forsythe LP, Workman TA et al. Patient, caregiver, and clinician use of cer findings in care decisions: results from a national study. J. Comp. Eff. Res. (2017) (Epub ahead of print).
22.
Forsythe LP, Frank LB, Workman TA et al. Health researcher views on comparative effectiveness research and research engagement. J. Comp. Eff. Res. (2017) (Epub ahead of print).
23.
Miles JN, Marshall GN, Schell TL. Spanish and English versions of the PTSD checklist–civilian version (PCL-C): testing for differential item functioning. J. Trauma. Stress 21(4), 369 (2008).
24.
De Leeuw ED. To mix or not to mix data collection modes in surveys. J. Off. Stat. 21(2), 233 (2005).
25.
Dillman DA, Smyth JD, Christian LM. Internet, Mail, And Mixed-Mode Surveys: The Tailored Design Method. John Wiley & Sons, Hoboken, NJ, USA (2009).
26.
Ziegenfuss JY, Burmeister KR, Harris A, Holubar SD, Beebe TJ. Telephone follow-up to a mail survey: when to offer an interview compared with a reminder call. BMC Med. Res. Methodol. 12(1), 32 (2012).
27.
Statacorp. Stata statistical software: release 13. StataCorp LP, College Station, TX, USA. (2013).
28.
Andersen T. The political empowerment of rare disease patient advocates both at EU and national level. Orphanet J. Rare. Dis. 7(2), 1 (2012).
29.
National Organization for Rare Disorders. Rare Disease Information (2016). http://rarediseases.org/for-patients-and-families/information-resources/rare-disease-information/?_sm_au_=iVVq6fRrfWMpWnn7.
30.
Terry SF. Disease advocacy organizations catalyze translational research. Front. Genet. 4, 101 (2013).
31.
Landy DC, Brinich MA, Colten ME, Horn EJ, Terry SF, Sharp RR. How disease advocacy organizations participate in clinical research: a survey of genetic organizations. Genet. Med. 14(2), 223–228 (2012).
32.
Terry SF, Terry PF, Rauen KA, Uitto J, Bercovitch LG. Advocacy groups as research organizations: the PXE International example. Nat. Rev. Genet. 8(2), 157–164 (2007).
33.
Costlow MR, Landsittel DP, James AE, Kahn JM, Morton SC. Model for a patient-centered comparative effectiveness research center. Clin. Transl. Sci. 8(2), 155–159 (2015).
34.
Patient-Centered Outcomes Research Institute. Pipeline to Proposal Awards (2015). www.pcori.org/funding-opportunities/pipeline-to-proposal-awards/.
35.
Patient-Centered Outcomes Research Institute. Eugene Washington PCORI Engagement Awards (2016). www.pcori.org/funding-opportunities/eugene-washington-pcori-engagement-awards/.
Information & Authors
Information
Published In
Copyright
© PCORI.
History
Published online: 8 February 2017
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Patient, caregiver and clinician views on engagement in comparative effectiveness research. (2017) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2016-0062
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- James Odom, Nicole Henderson, Tanvi Padalkar, Macy Stockdill, Reed Bratches, Etzael Olguin, Gabrielle Rocque, Leveraging Electronic Patient-Reported Symptoms to Optimize Cancer Family Caregivers’ Symptom Support: Qualitative Formative Evaluation of the FamilyAWARE Intervention Concept (Preprint), JMIR Formative Research, 10.2196/101699, (2026).
- Lisa M. Vaughn, A Socially Engaged Approach to Research: Finding Common Ground Within Qualitative Research and Action Research, International Review of Qualitative Research, 10.1177/19408447251387996, (2025).
- Kayla R. Mehl, Stephanie R. Morain, Jeremy Sugarman, Empirical research related to the ethics of pragmatic clinical trials: A scoping review, Learning Health Systems, 10.1002/lrh2.70041, 10, 1, (2025).
- Jessica A. Palakshappa, Megan L. Rischall, Ashley E. Strahley, Alexa E. Cecil, Matthew E. Prekker, Brian E. Driver, Brianna H. Denny, Kevin W. Gibbs, Eliciting Patient Preferences for Pragmatic Critical Care Trials: A Qualitative Study, Annals of the American Thoracic Society, 10.1513/AnnalsATS.202410-1122OC, 22, 7, (1027-1034), (2025).
- Katherine J. Holzer, Haley E. Bernstein, Christin Veasley, Simon Haroutounian, Dagmar Amtmann, Aderonke Bamgbose Pederson, Bryce B. Reeve, Dennis C. Turk, Robert H. Dworkin, Dale J. Langford, Attitudes toward patient engagement in clinical pain research: Insights from individuals with chronic pain in the United States, The Journal of Pain, 10.1016/j.jpain.2025.105358, 32, (105358), (2025).
- Anabel Granja-Dominguez, Carmen Martin-Gomez, Juan Darío Ortigoza-Escobar, Rocío Rodriguez-Lopez, Lourdes Gonzalez-Bermudez, Stefania Dantone, Stefano Pavanello, Juan Antonio Blasco-Amaro, A proposal to involve people living with rare and complex conditions in the development of clinical practice guidelines, Patient Education and Counseling, 10.1016/j.pec.2025.108708, 135, (108708), (2025).
- Stephanie L. Graff, Emily C. Freeman, Meaghan Roach, Rozanne Wilson, Claire Cagle, Sarah Lunsford, Melissa Culhane Maravic, Ricki Fairley, Mary Gullatte, Jeanne Stemland, Paulina Wochal, Julie Katz, Brianna Hoffner, Julie M. Scott, Suepattra G. May, Investigating the Salience of Clinical Meaningfulness and Clinically Meaningful Outcomes in Metastatic Breast Cancer Care Delivery, JCO Oncology Practice, 10.1200/OP.24.00228, 21, 4, (518-525), (2025).
- Sally A Dews, Lynne Corner, Rebecca Butfield, Mary Araghi, Hannah Monelle, Polly Westergaard, Susan Moloney, Viola Wontor, Alexia Campbell Burton, Co-creating tools for embedding meaningful patient and public involvement and engagement in real-world data and evidence research in the pharmaceutical industry setting: a multistakeholder participatory co-design study, BMJ Open, 10.1136/bmjopen-2024-088914, 15, 2, (e088914), (2025).
- Jaclyn L. Papadakis, Madeleine C. Suhs, Alexander O’Donnell, Michael A. Harris, Lindsay M. Anderson, Kimberly P. Garza, Lindsey Weil, Jill Weissberg-Benchell, Focused on the Family: Development of a Family-Based Intervention Promoting the Transition to Adult Health Care for Adolescents with Type 1 Diabetes, Children, 10.3390/children11111304, 11, 11, (1304), (2024).
- Alexis Richards, Marissa Raymond-Flesch, Shana D. Hughes, Yinglan Zhou, Kimberly A. Koester, Lessons Learned with a Triad of Stakeholder Advisory Boards: Working with Adolescents, Mothers, and Clinicians to Design the TRUST Study, Children, 10.3390/children10030483, 10, 3, (483), (2023).