Health researcher views on comparative effectiveness research and research engagement
Abstract
Aim: To understand researcher capability for and interest in patient-centered comparative effectiveness research (PC-CER), particularly related to engaging with patients/caregivers. Materials & methods: Web-based survey of 508 health researchers recruited via professional health research organizations. Results: Most respondents (94%) were familiar with CER and many (69%) reported having previously conducting some form of CER. Most respondents were familiar with (81%) and interested in (87%) partnering with patients and/or caregivers in research. Resources to assist in training, coordination of partners, guidance in apply for funding and improved infrastructure were commonly cited factors that would help researchers conduct PC-CER. Conclusion: There is a significant opportunity for researchers to engage patients and caregivers as partners in CER. Researchers recognize the need for additional training and expertise to leverage those opportunities.

First draft submitted: 30 August 2016; Accepted for publication: 15 December 2016; Published online: 8 February 2017
For nearly two decades, there has been growing interest in and funding for comparative effectiveness research (CER) [1–3]. CER compares the effectiveness and safety of preventive, diagnostic and treatment options to produce evidence that is useful for making informed decisions in real-world clinical settings [4]. In the USA, the US$1.1 billion for CER provided by the American Recovery and Reinvestment Act of 2009, which also mandated prioritization of CER topics by the Institute of Medicine, reinforced an already growing interest for CER to help improve decision-making about medical interventions for both patients and clinicians [5–11].
At the same time, interest has grown in greater patient and other stakeholder involvement in healthcare decision-making and research. Patient-centeredness, a concept that orients healthcare around the preferences and needs of patients through active and respectful partnerships between clinicians, patients and families, has become a central approach to healthcare delivery in the USA [12]. Both American Recovery and Reinvestment Act, and the Patient Protection and Affordable Care Act of 2010, which established the Patient-Centered Outcomes Research Institute (PCORI), emphasized the active role of patients and other stakeholders, such as caregivers in the planning, conduct and dissemination of research studies, which extended the concept of patient-centeredness from healthcare delivery to research [13]. Growing evidence suggests that this approach, known as patient-centered CER (PC-CER), fosters comparative studies that more closely align to the outcomes of greatest interest to patients and clinicians [9,14–16]. Engaging patients/caregivers is a critical component of PC-CER, as it can help to ensure that the research conducted is meaningful, relevant and useful to patients and their families in making health decisions [13]. Evaluations of PC-CER both in the USA and the UK indicate that involving patients and caregivers in the research process can increase study-enrollment rates; help researchers choose relevant and patient-focused research questions, objectives and outcomes; and provide patient perspectives on data interpretation [17–19].
Despite increased interest in PC-CER, little is known about health researchers’ experiences, attitudes and needs related to conducting CER and engaging patients and caregivers as research partners. Surveys assessing stakeholder's attitudes toward CER and research engagement have primarily focused on patients, clinicians, Medicaid directors and other groups of CER stakeholders, rather than researchers [9,14,20–24]. Qualitative research with a limited number of researchers suggests that health researchers recognize the value of engaging patients, but face challenges in doing so [25,26]. With clear gaps in the evidence, additional quantitative and qualitative research is needed to better understand health researchers’ perceptions on the value of engagement, as well as facilitators and barriers to engagement of patients and caregivers. Expanding the knowledge base in this area can help promote researcher collaboration with patients, caregivers and others interested in encouraging more informed and evidence-based clinical decisions [14], and can inform PCORI and other funders on increasing the quality and impact of CER.
In 2014, PCORI commissioned the current survey study to: understand healthcare researchers’ attitudes toward and experiences with, conducting PC-CER; assess facilitators and barriers to conducting CER and partnering with patients and caregivers for this research; and understand the influence of PCORI on the conduct of PC-CER from a broad set of researchers. This study was part of a larger PCORI effort to understand the beliefs, values and attitudes of various audiences, including patients with rare and chronic diseases, caregivers, clinicians and researchers about CER and PC-CER; the engagement of patients in the research process; and the use of evidence-based information in clinical decision-making.
Materials & methods
Stakeholder input
The project was guided by an Advisory Group comprised of 11 representatives of patient advocacy organizations, medical societies, researchers with expertise in patient engagement and comparative effectiveness researchers. A Working Group of eight health researchers also guided the project. These groups assisted in the development of the final set of survey domains, guided revisions based on cognitive testing, provided suggestions for sampling, provided input into interpretation of the results, and contributed to the determination of key findings and their implications for PCORI.
Survey development
Survey development was guided by an environmental scan of the literature (n = 33 relevant articles), key informant interviews (n = 4) to assess general knowledge and lessons learned from existing surveys on researcher involvement with or use of CER, and input from the Advisory Group and Researcher Working Group. The survey was tested through cognitive interviews (n = 12) with researchers.
Measures
The survey included 40 individual survey items exploring: the type of research the respondent conducted and the setting; respondent knowledge and attitudes regarding the conduct of CER; respondent knowledge, experience and attitudes about engaging patients/caregivers as partners in research; respondent knowledge and perceived impact of PCORI; and general respondent demographics. In addition, we sought to understand whether there were significant differences in attitudes, beliefs, and perceptions of CER and interest in patient engagement among researchers based on specific demographic characteristics (e.g., years of research experience and clinician vs nonclinician researchers). Response options included: 3- and 4-point Likert scales (e.g., from very important to not important at all), mark all that apply and binary yes/no options (see Supplementary Material for the full survey instrument).
Sampling & population
We defined healthcare researchers as clinical, health services and health outcomes researchers. Since a comprehensive list of healthcare researchers does not exist, we used a convenience sample of members of professional research organizations or groups. The final list of 24 organizations was developed with the goal of ensuring representation of clinical, health services and health outcome researchers who currently conduct CER, or who are likely to conduct CER given that the field of CER research is relatively new to some (see Supplementary Material for a full list of the organizations). The target number of completed surveys was 500–1000 to meet our analytic goals, such as the ability to detect subgroup differences. Because of using a convenience sample where the number of individuals invited to participate who meet our eligibility criteria cannot be accurately determined, a survey response rate was not calculated. However, because a unique survey URL was created for each participating organization, we were able to determine the percentage of completed surveys that were linked to each organization (n = 508):
40.4% – research organizations, such as, Kaiser Permanente Division of Research, Center for Effectiveness & Safety Research and North American Primary Care Research Group;
32.6% – PCORI mailing lists (random sample);
12.4% – institutions previously part of the Agency for Healthcare Research and Quality (AHRQ) Innovative Adaptation and Dissemination of AHRQ CER Product grants;
11.2% – evidence-based practice centers;
2.0% – institutions previously part of the AHRQ Centers for Education and Research on Therapeutics (CERTs);
1.4% – institutions previously part of the Developing Evidence to Inform Decisions about Effectiveness Network.
Data collection
The web-based survey was open from October 2014 to November 2014. Invitations to complete the survey were distributed via an email invitation from most organizations; two organizations: the International Society for Public Opinion Research and AcademyHealth, announced the survey in their respective newsletters. Respondents completing the survey were eligible to receive a $5 gift card. A total of 508 researchers completed the survey. The American Institutes for Research Institutional Review Board (IRB) approved this study.
Analysis
Descriptive statistical analyses (e.g., frequencies) were performed using STATA version 13 software and are interpreted based on the response scale. We examined frequency distributions for each question and collapsed or top-coded responses as needed for analyses to account for imbalanced response categories or to appropriately dichotomize scaled responses. Bivariate analyses, such as cross tabulations using Chi Square or Fisher's exact tests, were conducted to compare beliefs, values and attitudes of researchers about CER across all collected demographic characteristics (e.g., years of research experience, institution type and clinician vs nonclinician researcher) to identify differences among subgroups; statistically significant associations are reported.
Results
Survey participants
Among those who reported demographic information, the majority were white (85%) and non-Hispanic (96%). More than half (61%) were female. Nearly a third (31%) of respondents was aged 35–44 years, and 41% had worked in the research field for 16 or more years. In addition, most had been a principal investigator (78%); were not a practicing healthcare clinician (67%); were affiliated with a medical school, academic institution or teaching hospital (68%); had conducted CER – defined as an assessment of prevention, diagnosis or treatment options (69%); and recently had conducted health services research projects (60%). Respondents earned their highest degree from a variety of disciplines, including medicine (28%), psychology (12%), epidemiology (10%) and others (18%) such as anthropology, education, nutrition, public policy and social work (see Table 1).
Familiarity with & value of CER
A majority of respondents (94%) were familiar with CER, with 60% reporting they were ‘very familiar’ (see Figure 1). Approximately two-thirds of respondents reported experience conducting some form of this type of research: of those, 74% had conducted observational studies, 64% had conducted secondary data analysis, 54% had conducted randomized trials, 27% had conducted pragmatic trials, 41% had conducted systematic reviews and 37% had conducted dissemination and implementation. Of those who had not conducted any form of CER, nearly half (47%) identified lack of alignment with their training and expertise as the reason, one-quarter (26%) selected lack of funding opportunities and nearly one-quarter (22%) reported not obtaining funding despite trying. Most researchers perceived CER as ‘very valuable’ for supplying evidence relevant to clinical decision-making (83%) and helping patients make treatment choices (71%).
Conducting PC-CER
Nearly half of the respondents had conducted PC-CER (49%). Of those who had not, their reasons included lack of alignment of PC-CER with their training and expertise (36%), lack of funding opportunities (29%) and not obtaining funding despite trying (23%). Compared with groups with less experience, researchers who have been conducting research for 16-plus years were more likely to have conducted PC-CER (p = 0.002).
Engagement with patients &/or caregivers
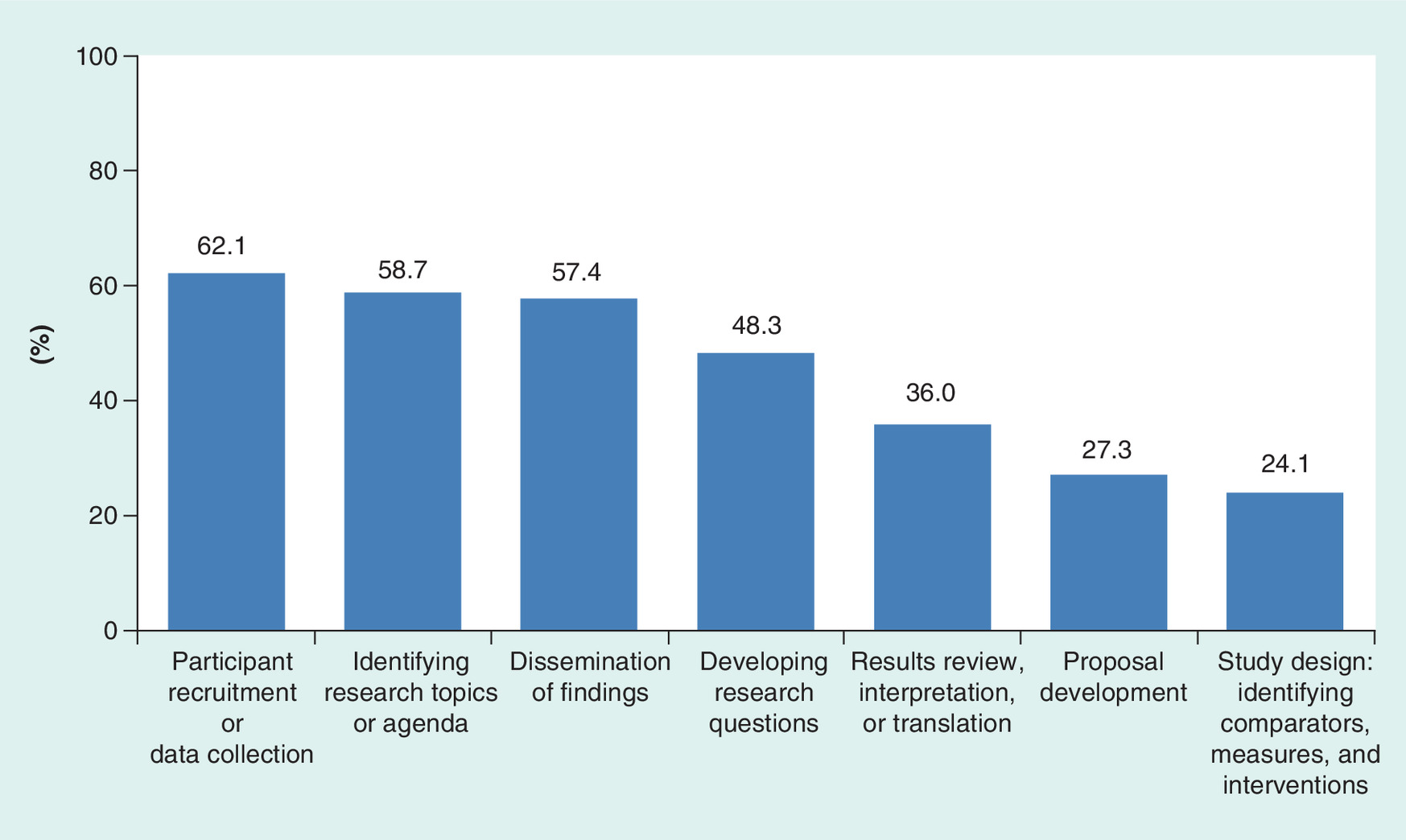
Most respondents were familiar with engaging patients and/or caregivers as partners in research (43% ‘very familiar’ and 38% ‘familiar’). Researchers with 16-plus years of experience were more likely to be very familiar with patient/caregiver involvement (p = 0.007). Further, 65% of the researcher sample reported experience engaging with patients and/or caregivers in research. Of those who had engaged patients/caregivers in research, the most common roles patients/caregivers played were identifying research topics or agendas (62%), developing research questions (59%), participant recruitment or data collection (58%), results review, interpretation or translation (53%) and dissemination of findings (47%) (see Table 2).
Further, among those researchers who had engaged with patients or caregivers, nearly 56% said it was ‘very valuable’ and almost a third (32%) said it was ‘somewhat valuable’ to their research. See Figure 2 for details on perceived value of engaging patients and/or caregivers in several specific activities. A majority of these researchers cited recruitment or data collection (62%), identifying research topics and agendas (59%), and disseminating findings (57%) as ‘very valuable’ roles for research engagement with patients or caregivers. Approximately a third (36%) endorsed engagement for assisting with results review and interpretation as ‘very valuable’.
A majority of respondents (87%) expressed interest in engaging patients and caregivers as research partners in the future, with 63% being ‘very interested’. Factors that respondents said were ‘very important’ for determining whether they would involve patients and/or caregivers as partners in research included being able to conduct research is relevant to patient needs (78%), the ability to recruit participants (57%), the uptake of findings in clinical practice (50%), and potential speed of dissemination of research results with patient and caregiver help (41%).
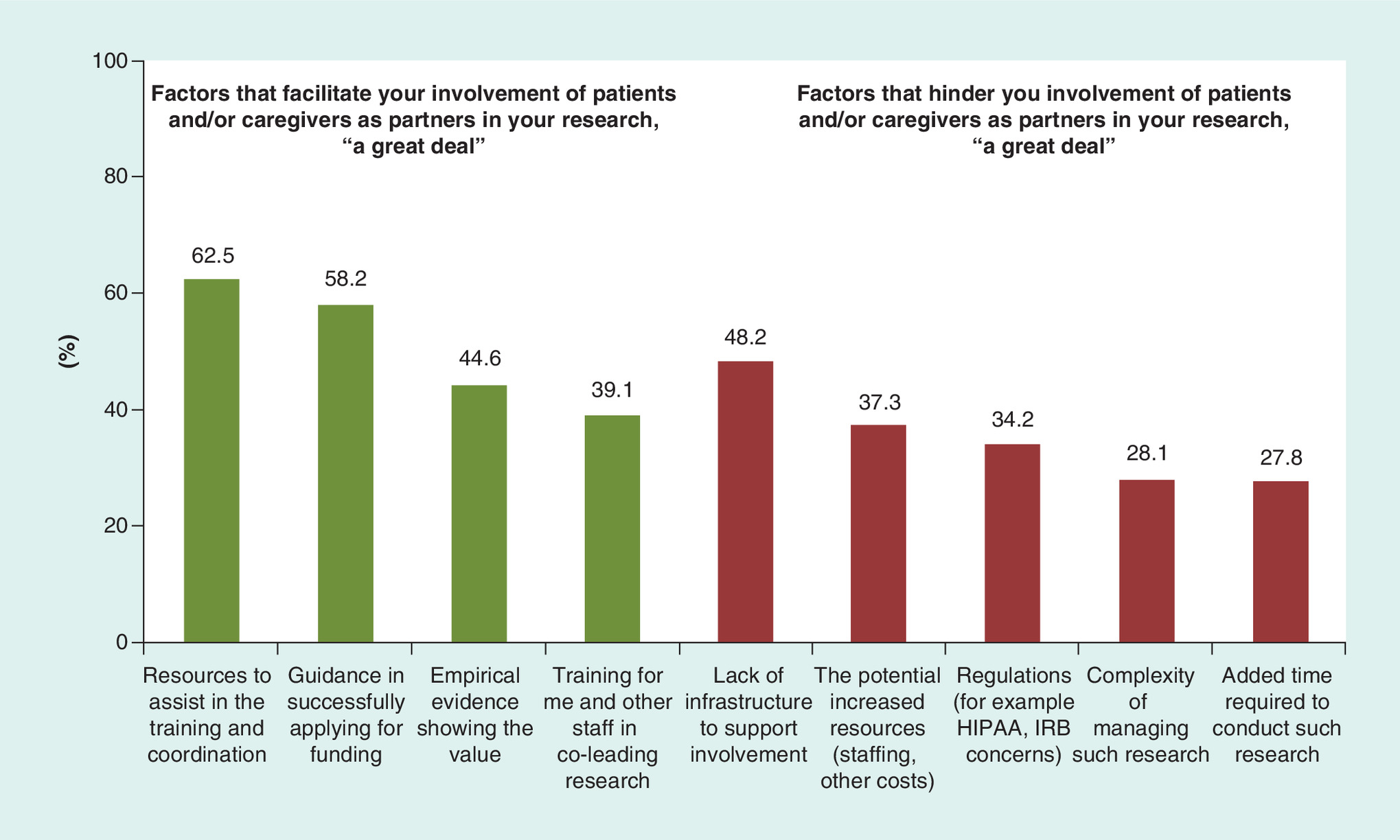
Facilitators & barriers to engaging patients/caregivers in the research process
Respondents were asked to indicate how much a variety of factors would facilitate or hinder their involvement of patients/caregivers in research. The factors most commonly cited as facilitating engagement ‘a great deal’ were resources to assist in the training and coordination of patient and/or caregiver partners (63%) and guidance in applying for funding of research that requires patient/caregiver partners (58%). The factors most commonly cited as hindering engagement ‘a great deal’ were lack of infrastructure to support involving patients as partners (48%), potential increased resources (staffing, other costs) to work with patients and/or caregivers (37%) and regulations (34%) – for example, HIPAA (Health Insurance Portability and Accountability Act of 1996) and IRB concerns (see Figure 3).
In addition, there was variation between clinician and nonclinician researchers in the reported barriers. More nonclinician researchers (24%) than clinician researchers (14%) reported limited access to patients/caregivers interested in becoming research partners as hindering their involvement of patients/caregivers ‘a great deal’ (p = 0.016). Reported barriers and facilitators did not differ significantly between researchers who reported that they had or had not ever conducted CER or PC-CER (all p > 0.05).
Familiarity with PCORI
Respondents were largely familiar with PCORI (52% ‘very familiar’ and 38% ‘somewhat familiar’). Among those familiar with PCORI, 60% reported that PCORI had influenced their decision to conduct CER (26% ‘a great deal’ and 34% ‘some’) and 65% reported that PCORI had influenced their decision to involve patients as partners (32% ‘a great deal’ and 32% ‘some’). Fewer researchers with 16-plus years of experience reported PCORI had influenced their decisions a great deal (p = 0.023). But, researchers with 1–6 years of experience who were familiar with PCORI were more likely to report that PCORI's efforts were very valuable (p = 0.033).
Discussion
An understanding of researchers’ experiences, attitudes, and needs related to CER and engaging patients and caregivers as partners in the research process is a necessary foundation for facilitating future PC-CER. Across a sample of 508 healthcare researchers, there was a high level of awareness of CER, engaging patients/caregivers as research partners and PCORI, and significant agreement that CER is valuable in supplying evidence relevant to clinical decision-making and helping patients make treatment choices. However, only two-thirds of the surveyed researchers reported experience actually conducting CER studies and less than half reported conducting PC-CER. Further, even fewer had conducted randomized CER trials or pragmatic trials. These findings suggest that while there is a clear cohort of researchers interested in producing PC-CER, there is room for expansion across the larger population of researchers, particularly for approaches like pragmatic trials which are recognized as offering important benefits over traditional methods [27] and are increasingly becoming the focus of PCORI funding.
Not surprisingly, training and expertise in CER and PC-CER were consistently cited by researchers as the primary reason for not conducting this type of research. This finding suggests a need for expanded training opportunities to increase the number of researchers who feel competent in CER and PC-CER. However, a significant percentage of researchers also cited a lack of funding opportunities or inability to obtain funding despite trying as reasons for not conducting PC-CER. This suggests that additional outreach to the research community regarding funding opportunities and strategies to support application success may be helpful, as is further evaluation of the extent to which existing funding availability meets the need for research support.
Most researchers expressed familiarity with engaging patients/caregivers as partners in research. More than half reported engaging with patients or caregivers as research partners, and most of this group described the engagement experience as valuable to their research. Further, the majority of the health researchers who responded to the survey expressed interest in engaging with patients and caregivers on future studies. Taken together, these findings suggest there is a pool of researchers ready and willing to adopt patient-centered approaches to health research. However, researchers appear to have limited experience with the roles that patients/caregivers can play in the research process, with respondents most commonly reporting experience engaging with partners on identifying research topics, recruiting participants, interpreting results or disseminating findings. Consistent with other literature [18,28], these findings suggest that more work needs to be done to support researchers in engaging with patient/caregiver partners, with particular emphasis on those where experience is the lowest (defining comparators or data analysis) and those most commonly viewed as valuable (data collection, identifying topics and dissemination). Researchers’ perceived value of engagement of patients and caregivers for improving participant recruitment and data collection is not surprising given that failures in participant enrollment is a common reason for trial failure [29], but it is notable that researchers recognized the value of engagement at a variety of phases in the research process.
Although there were few demographic subgroup differences in these findings, a few trends are notable. Researchers with fewer years of research experience reported less experience with PC-CER and less familiarity with patient/caregiver engagement. Interestingly, they perceived more PCORI influence on the kinds of research they conduct, so early-career researchers may be particularly important targets for training and career development opportunities. These early-career researchers may need additional support and mentorship from more senior researchers in order to gain experience in the field. Another opportunity to expand the field is with nonclinician researchers, because they were more likely to report that limited access to patients/caregivers hindered their involvement of patients/caregivers in research. This suggests that researchers who do not regularly work with patients need new mechanisms to connect with patients.
An enhanced understanding of the barriers to and facilitators of conducting PC-CER is critical to supporting and expanding the pool of researchers able to conduct successful PC-CER. The finding that health researchers identified a number of potential barriers to conducting PC-CER is consistent with prior literature, which cites issues of institutional structure, policy and even philosophy, along with competing needs for a limited supply of time and resources, as major challenges to patient engagement in CER that must be addressed [17–19,30]. The specific infrastructure challenges noted by researchers here can be the basis for an action agenda on the part of research organization administrators and planners, particularly the lack of institutional infrastructure to engage patients as partners rather than as subjects and the limited resources for preparing researchers and stakeholders for partnership. In spite of the efforts by the National Center for Advancing Translational Sciences’ Clinical and Translational Science Awards Program (CTSA) and others to train and support research teams in engaging diverse patients and communities in translational research [31], researchers also indicated need for resources to increase their training and expertise in PC-CER, particularly in the areas of recruiting and interacting successfully with patient/caregiver partners. This, too, can be part of an action agenda for research organizations and for research advocacy groups as well. As patient/caregiver engagement is often a condition of CER funding, addressing these barriers should be a high priority for research institutions and funders. The researchers participating in this survey identified clear areas where additional support is needed, including additional training, increased funding and additional resources to identify and train patients to serve in research partner roles. While PCORI has created a broad set of resources for research professionals interested in developing skills in this area through its website (e.g., the PCORI engagement rubric [32], compensation framework, and sample patient engagement plans), these may need to be tied more closely to academic centers training future health researchers or CTSA program networks to facilitate the uptake of these and other available resources.
The motivation identified by the majority of health researchers to conduct PC-CER – the study's ability to meet patient decisional needs – signals a need to ensure better communication of patient needs to researchers, and perhaps, more opportunities for interactions between patient and consumer groups and the research community. Traditionally, researchers and patients/caregivers have remained separate. Research funders and others could help to foster meaningful dialogue among researchers and patients/caregivers about gaps in the information patients need in the treatment choices. PC-CER may be further advanced through the formal integration of patients and caregivers into research conferences and journals as active contributors. Tools like the ‘Patients Included’ charter can help research organizations operationalize and demonstrate that their events or activities are committed to incorporating patients as coexperts, while ensuring that they are neither excluded nor exploited [33,34]. Likewise, encouraging researcher involvement in patient support or advocacy organizations could also yield better inspiration for PC-CER projects and sustainable partnerships. Last, taking steps to better accommodate patients or caregivers as research partners, such as minimizing time commitments; providing compensation; offering engagement opportunities throughout the research process; and leveraging mobile and web-based technology for interactions and information exchange, can promote participation within the context of their busy lives.
The data also show that PCORI has had an influence within the research community regarding PC-CER, even after just 2 years of initiating its research funding program, suggesting that the existence of a national institution to promote, inform, develop and fund PC-CER may be critical to ensuring the sustainability of a robust community of PC-CER researchers. Future work could address the extent to which researcher engagement behavior follows growth in the evidence base on engagement.
Limitations
There are several limitations to this study. First, the survey was based on a convenience sample since there was no existing comprehensive national panel of health researchers. Thus, the results of this survey cannot be extrapolated beyond these respondents. This study, by design, sought to understand experiences with and attitudes toward CER and engagement among those who were conducting or were likely to conduct CER to better understand the meaningful barriers and facilitators to this type of research. Thus, respondents tended to be from health research organizations with a strong focus on CER (e.g., PCORI's mailing lists, the evidence-based practice centers and Innovative Adaptation and Dissemination of AHRQ CER Product grantees) who may have a greater working knowledge of CER and PC-CER than healthcare researchers who are not affiliated with such organizations. This commonality could also explain the limited differences in primary CER outcomes found across demographic subgroups within this pool of respondents. Future studies should attempt to include researchers from other groups who may be familiar with engagement, including investigators associated with the CTSAs, and also healthcare researchers who may not be as familiar with CER or PC-CER to more fully understand attitudes toward CER and engagement from a broader perspective. Future studies should also consider collecting specific information from respondents regarding participation in PC-CER training or working with senior mentors experienced in PC-CER. Second, as this is an evolving field, these findings from late 2014 may not accurately reflect the current state of researcher attitudes and beliefs about, or experiences with CER. Third, racial/ethnic diversity among survey respondents was limited, highlighting the need for more targeted sampling strategies to better understand the experiences and attitudes of diverse researchers, particularly in light of efforts to facilitate the conduct of patient-centeredness not only among researchers from diverse backgrounds but also with diverse patient and caregiver partners. Further research is needed to examine researcher attitudes toward and experience with conducting CER with other stakeholders beyond patients and caregivers (e.g., clinicians, administrators, payers), as well as to assess frequency and level of engagement with patients, caregivers or other stakeholders. Last, although some researchers in the study reported conducting PC-CER, this study cannot confirm the consistency or fidelity of PC-CER practices among them. More in-depth studies are needed to examine concordance of researcher-reported PC-CER activities and intent with actual experiences. A larger mixed-methods research effort with a sample of health researchers that reflects a wider range of experience (or lack thereof) with patient-centered approaches to research would further build the evidence base in this area.
Future perspective
As patient-engaged research becomes available to the public that can be used in healthcare decision-making, we foresee an increased demand for CER that fully incorporates stakeholder needs and interests at every level of the process. In order to meet this demand, evolution of the current healthcare research arena is likely to occur in three areas. First, the structure, policies and procedures at research institutions will evolve to enable patients, caregivers and other nonresearcher stakeholders to serve as partners and coinvestigators in CER. Research institutions will need to innovate new policies and procedures that open access to stakeholder partners who are not serving as subjects. This is likely to impact a wide range of institutional procedures from the IRB to the Sponsored Programs. Second, we envision an expanded curriculum for academic and research institutions involved in training new healthcare researchers that incorporates the methods and best practices of stakeholder-engaged CER. Finally, we expect to see patient-engaged CER become fully realized and legitimized as a form of healthcare research alongside more traditional medical research. We expect to see increased development of a researcher community that is able to continue the evolution of patient-engaged CER by improving its methods, disseminating findings and expanding its application to the field of healthcare.
| Demographic characteristic | Frequency, n (%) |
|---|---|
| Sex: | |
| – Male | 182 (39.2) |
| – Female | 282 (60.8) |
| Race (mark all that apply): | |
| – White | 390 (85.0) |
| – Black or African–American | 19 (4.1) |
| – American–Indian or Alaska native | 0 (0.0) |
| – Asian | 54 (11.8) |
| – Native Hawaiian or other Pacific Islander | 3 (0.7) |
| Age (years): | |
| – 18–24 | 2 (0.4) |
| – 25–34 | 53 (11.4) |
| – 35–44 | 143 (30.7) |
| – 45–54 | 125 (26.8) |
| – 55–64 | 112 (24.0) |
| – 65 or older | 31 (6.6) |
| Hispanic, Latino/a or Spanish: | |
| – Yes | 19 (4.1) |
| – No | 444 (95.9) |
| Number of years in research field: | |
| – 1–6 | 98 (20.8) |
| – 7–15 | 179 (38.0) |
| – 16 or more | 194 (41.2) |
| Respondent is practicing healthcare clinician: | |
| – Yes | 157 (33.5) |
| – No | 312 (66.5) |
| Type of research institution (mark all that apply): | |
| – Medical school, academic institution or teaching hospital | 322 (68.4) |
| – Nonprofit, nonacademic research organization | 116 (24.6) |
| – Corporate organization | 39 (8.3) |
| – State or Federal government agency | 20 (4.2) |
| – Other | 18 (3.8) |
| Types of recent research projects (mark all that apply): | |
| – Clinical research | 219 (47.0) |
| – Health services research | 280 (60.1) |
| – Health economics | 50 (10.7) |
| – Health outcomes research | 227 (48.7) |
| – Community-based participatory research | 119 (25.5) |
| – Comparative effectiveness research | 199 (42.7) |
| Areas have ever conducted research (mark all that apply): | |
| – Assessment of prevention, diagnosis or treatment options | 321 (68.6) |
| – Improving healthcare systems | 221 (47.2) |
| – Communication and dissemination of research findings | 161 (34.4) |
| – Disparities in health and healthcare delivery | 231 (49.4) |
| – Improving methods for comparative effectiveness research | 114 (24.4) |
| – I have not conducted research in any of these areas | 19 (4.1) |
| Principal investigator: | |
| – Yes | 369 (78.3) |
| – No | 102 (21.7) |
Total respondent sample = 508. Percentages based on available demographic data.
| Survey topic | Frequency, n (%) |
|---|---|
| Have you ever engaged patients and/or caregivers in the planning, design, monitoring, interpretation, or dissemination or a research study?: | |
| – Yes | 315 (65.1) |
| What role have patients and/or caregivers played in your research study or project? (if engaged patients/caregivers; mark all that apply): | |
| – Identifying research topics or agenda | 192 (61.5) |
| – Developing the research questions | 183 (58.7) |
| – Proposal development | 130 (41.7) |
| – Study design: defining comparators | 89 (28.5) |
| – Study design: defining and/or measuring outcomes | 155 (49.7) |
| – Study design: selection or development of interventions | 134 (43.0) |
| – Participant recruitment or data collection | 181 (58.0) |
| – Data analysis | 38 (12.2) |
| – Results review, interpretation or translation | 166 (53.2) |
| – Dissemination of findings | 148 (47.4) |
| – Other, please specify | 11 (3.5) |
| How valuable was engaging patients and/or caregivers to your research?: | |
| – Very valuable | 172 (55.8) |
| – Somewhat valuable | 97 (31.5) |
| – Slightly valuable | 34 (11.0) |
| – Not at all valuable | 5 (1.6) |
Background
Despite increased funding for comparative effectiveness research (CER), significant knowledge gaps exist about researcher's interest in CER, barriers and facilitators to conducting CER, and attitudes and experiences engaging and partnering with patients on patient-centered CER (PC-CER).
This study informs ongoing efforts to develop and support researcher's interest in and capacity to conduct CER and PC-CER.
Methods
Web-based survey of 508 clinical, health services and health outcome researchers recruited through a convenience sample using professional organizations.
Results
An overwhelming majority of respondents (94%) were familiar with CER.
Approximately two-thirds (69%) reported ever conducting some form of CER. Nearly half of those who had not conducted any form of CER cited lack of alignment with their training and expertise as the reason.
Most respondents were familiar with partnering with patients and/or caregivers (81%) in research, and most (87%) expressed interest in engaging patients/caregivers as research partners.
The most commonly cited factors that would help researchers involve patients/caregivers in studies were resources to assist in the training and coordination of patient and/or caregiver partners (62%) and guidance in applying for funding of PC-CER (58%).
Lack of infrastructure to support patients as partners in research was the most commonly cited barrier (48%).
These findings suggest a need for expanded curriculum on patient-engaged research at training institutions or better integration with existing resources, such as Clinical and Translational Science Awards Programs, to increase the number of researchers who feel competent to conduct CER and PC-CER.
Conclusion & future perspective
These findings indicate there is a significant opportunity for an action agenda on the part of researchers to engage patients and caregivers as partners rather than subjects and to provide resources for preparing researchers and patients/caregivers for meaningful and sustainable partnerships.
Acknowledgements
We gratefully acknowledge the contributions of the Advisory and Working group members; partner organizations; and researchers involved in this study.
Disclaimer
The views expressed in this paper are those of the authors and do not necessarily reflect the official views of the PCORI, nor of the American Institutes for Research.
Financial & competing interests disclosure
The study was funded by the PCORI (contract # PCO-SCISRV2013). The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The authors state that they have obtained appropriate IRB approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (suppl_material.pdf)
- Download
- 2.15 MB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Rich EC, Esposito D, Kimmey LD, Valenzano CS, Yong PL. Assessing the long-term impact of public investments in comparative effectiveness research: conceptual framework and lessons learned. J. Comp. Eff. Res. 3(6), 657–666 (2014).
•• Describes the larger context of comparative effectiveness funding and patient engagement created through the Affordable Care Act.
2.
Segal C, Holve E. American Recovery and Reinvestment Act-comparative effectiveness research infrastructure investments: emerging data resources, tools and publications. J. Comp. Eff. Res. 3(6), 647–655 (2014).
3.
D'arcy LP, Rich EC. From comparative effectiveness research to patient-centered outcomes research: policy history and future directions. Neurosurg. Focus 33(1), E7 (2012).
•• Provides context for the movement toward patient-engaged research.
4.
Institute of Medicine. Initial National Priorities for Comparative Effectiveness Research (2009). www.nap.edu/read/12648/chapter/1.
5.
National Business Group on Health's Position Statement on Comparative Effectiveness (2014). http://www.businessgrouphealth.org/pub/f3144e45-2354-d714-51a2-1cae568ae480.
6.
Lowry SJ, Loggers ET, Bowles E, Wagner EH. Evidence gaps in advanced cancer care: community-based clinicians’ perspectives and priorities for CER. Am. J. Manag. Care 18(5 Spec No. 2), SP77–SP83 (2012).
7.
Alston C. Consumer Attitudes About Comparative Effectiveness. Presented at: National Comparative Effectiveness Summit. Washington, DC, USA, 16–18 September 2013.
8.
Impaq International. Evaluation of ARRA Comparative–Effectiveness Research Dissemination Contract Efforts - Consumer and Clinician Survey Analysis Report: Second Survey Administration and Longitudinal Report (2013). www.ahrq.gov/research/findings/final-reports/arracer/index.html.
9.
Williams SS, Esposito D, Rich EC. Patients and clinicians as stakeholders in comparative effectiveness research: multiple perspectives and evolving roles (2014). www.mathematica-mpr.com/our-publications-and-findings/publications/patients-and-clinicians-as-stakeholders-in-comparative-effectiveness-research-multiple-perspectives.
10.
Sox H, Greenfield S. Comparative effectiveness research: a report from the Institutes of Medicine. Ann. Intern. Med. 151(3), 203–205 (2009).
11.
Gibson TB, Ehrlich ED, Graff J et al. Real-world impact of comparative effectiveness research findings on clinical practice. Am. J. Manag. Care 20(6), e208–e220 (2014).
12.
Shaller D. Patient-Centered Care: What Does It Take? Commonwealth Fund, NY, USA (2007).
13.
Frank L, Basch E, Selby JV. The PCORI perspective on patient-centered outcomes research. J. Am. Med. Assoc. 312(15), 1513–1514 (2014).
14.
Forsythe LP, Frank L, Walker KO et al. Patient and clinician views on comparative effectiveness research and engagement in research. J. Comp. Eff. Res. 4(1), 11–25 (2015).
• Provides prior study results that were used in formulating and expanding the current study.
15.
Holve E, Segal C. Infrastructure to support learning health systems: are we there yet? Innovative solutions and lessons learned from American Recovery and Reinvestment Act CER investments. J. Comp. Eff. Res. 3(6), 635–645 (2014).
16.
Hamilton Lopez M, Holve E, Rein A, Winkler J. Involving patients and consumers in research: new opportunities for meaningful engagement in research and quality improvement (2012). http://repository.edm-forum.org/cgi/viewcontent.cgi?article=1001&context=edm_briefs.
17.
Brett J, Staniszewska S, Mockford C et al. Mapping the impact of patient and public involvement on health and social care research: a systematic review. Health Expect. 17(5), 637–650 (2014).
18.
Domecq JP, Prutsky G, Elraiyah T et al. Patient engagement in research: a systematic review. BMC Health Serv. Res. 14(1), 89 (2014).
19.
Staley K. Exploring Impact: Public Involvement In NHS, Public Health And Social Care Research. National Institute for Health Research (2009). www.invo.org.uk/posttypepublication/exploring-impact-public-involvement-in-nhs-public-health-and-social-care-research/.
20.
Keyhani S, Woodward M, Federman AD. Physician views on the use of comparative effectiveness research: a national survey. Ann. Intern. Med. 153(8), 551–552 (2010).
21.
Weissman JS, Westrich K, Hargraves JL et al. Translating comparative effectiveness research into Medicaid payment policy: views from medical and pharmacy directors. J. Comp. Eff. Res. 4(2), 79–88 (2015).
22.
Comparative effectiveness research and the environment for health care decision-making. National Pharmaceutical Council (2016).http://www.npcnow.org/system/files/research/download/NPC_ChartPack_v04_highres.pdf.
23.
Williams SS, Frost SL. Differences among consumer segments with regard to perceptions of comparative effectiveness research. J. Comp. Eff. Res. 3(6), 617–622 (2014).
24.
Cornwell D, Hu M, Esposito D. Public perceptions of comparative effectiveness research and use of evidence in healthcare decision-making. J. Comp. Eff. Res. 3(6), 623–634 (2014).
25.
Thompson J, Barber R, Ward PR et al. Health researchers’ attitudes towards public involvement in health research. Health Expect. 12(2), 209–220 (2009).
26.
Ward PR, Thompson J, Barber R et al. Critical perspectives on ‘consumer involvement’ in health research epistemological dissonance and the know-do gap. J. Sociol. 46(1), 63–82 (2010).
27.
Ware JH, Hamel MB. Pragmatic trials--guides to better patient care. N. Engl. J. Med. 364(18), 1685–1687 (2011).
28.
Concannon TW, Fuster M, Saunders T et al. A systematic review of stakeholder engagement in comparative effectiveness and patient-centered outcomes research. J. Gen. Intern. Med. 29(12), 1692–1701 (2014).
• Provides a general perspective on the assessment of stakeholder engagement in comparative effectiveness research.
29.
Kasenda B, Von Elm E, You J et al. Prevalence, characteristics, and publication of discontinued randomized trials. J. Am. Med. Assoc. 311(10), 1045–1052 (2014).
30.
Workman T, Maurer M, Carman K. Unresolved tensions in consumer engagement in CER: a US research perspective. J. Comp. Eff. Res. 2(2), 127–134 (2013).
31.
National Center for Advancing Translational Sciences. About the CTSA program (2016). https://ncats.nih.gov/ctsa/about.
32.
Frank L, Forsythe L, Ellis L et al. Conceptual and practical foundations of patient engagement in research at the Patient-Centered Outcomes Research Institute. Qual. Life Res. 24(5), 1033–1041 (2015).
•• Provides a full context of patient-engaged research from Patient-Centered Outcomes Research Institute's perspective.
33.
Reshape & Innovation Center. Patients Included. https://patientsincluded.org/.
34.
Carolyn Thomas. ‘My open letter to ‘Patients Included’ conferences’ [Blog post], 6 March 2016. http://myheartsisters.org/2016/03/06/my-open-letter-to-patients-included-conferences/.
Information & Authors
Information
Published In
Copyright
© PCORI.
History
Published online: 8 February 2017
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Health researcher views on comparative effectiveness research and research engagement. (2017) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2016-0063
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Kayla R. Mehl, Stephanie R. Morain, Jeremy Sugarman, Empirical research related to the ethics of pragmatic clinical trials: A scoping review, Learning Health Systems, 10.1002/lrh2.70041, 10, 1, (2025).
- Prajakta Adsul, Shannon Sanchez-Youngman, Elizabeth Dickson, Belkis Jacquez, Alena Kuhlemeier, Michael Muhammad, Katherine J. Briant, Bridgette Hempstead, Jason A. Mendoza, Lisa G. Rosas, Anisha Patel, Patricia Rodriguez Espinosa, Tabia Akintobi, Paige Castro-Reyes, Lori Carter-Edwards, Nina Wallerstein, Assessing the context within academic health institutions toward improving equity-based, community and patient-engaged research, Journal of Clinical and Translational Science, 10.1017/cts.2024.675, 9, 1, (2024).
- Eveline Zbären, Srividhya Padmanabhan, Sandra Jent, Monitoring/Evaluation in Nutritional Therapy for People with Gastrointestinal Complaints: Online Survey with Dietitians, Aktuelle Ernährungsmedizin, 10.1055/a-1895-2430, 48, 01, (27-36), (2022).
- Deborah J Johnson, Mary F Brunette, Daisy J Goodman, Meagan Adams, Cheri Bryer, Julie R Doherty, Victoria Flanagan, Julia R Frew, Sarah Mullins, Farrah Sheehan, Allison Tobar-Santamaria, Sarah Whitney, Sarah Lord, Promoting community stakeholder engagement in research on treatment for pregnant women with opioid use disorder, Journal of Comparative Effectiveness Research, 10.2217/cer-2022-0090, 11, 15, (1085-1094), (2022).
- Roses Parker, Eve Tomlinson, Thomas W. Concannon, Elie Akl, Jennifer Petkovic, Vivian A. Welch, Sally Crowe, Marisha Palm, Ana Marusic, Comfort Ekanem, Imad Bou Akl, Michael Saginur, Lorenzo Moja, Tanja Kuchenmüller, Nevilene Slingers, Ligia Teixeira, Laura Dormer, Eddy Lang, Thurayya Arayssi, Regina Greer-Smith, Asma Ben Brahem, Marc Avey, Peter Tugwell, Factors to Consider During Identification and Invitation of Individuals in a Multi-stakeholder Research Partnership, Journal of General Internal Medicine, 10.1007/s11606-022-07411-w, 37, 16, (4047-4053), (2022).
- Emily M. Godfrey, Erin K. Thayer, Laura Mentch, Traci M. Kazmerski, Georgia Brown, Molly Pam, Morhaf Al Achkar, Development and evaluation of a virtual patient-centered outcomes research training program for the cystic fibrosis community, Research Involvement and Engagement, 10.1186/s40900-021-00328-4, 7, 1, (2021).
- C. Cavens, C. Imms, G. Drake, N. Garrity, M. Wallen, Perspectives of children and adolescents with cerebral palsy about involvement as research partners: a qualitative study, Disability and Rehabilitation, 10.1080/09638288.2021.1900927, 44, 16, (4293-4302), (2021).
- Rachel Hemphill, Laura P. Forsythe, Andrea L. Heckert, Andrew Amolegbe, Maureen Maurer, Kristin L. Carman, Rikki Mangrum, Lisa Stewart, Ninma Fearon, Laura Esmail, What motivates patients and caregivers to engage in health research and how engagement affects their lives: Qualitative survey findings, Health Expectations, 10.1111/hex.12979, 23, 2, (328-336), (2019).
- Elizabeth L Ciemins, Brenda L Mollis, Jeannine M Brant, Laurie A Hassell, Sandra Albritton, Paul Amoroso, Angela Lloyd, Jodi M Smith, Bethann M Pflugeisen, Katherine R Tuttle, Laura-Mae Baldwin, Clinician engagement in research as a path toward the learning health system: A regional survey across the northwestern United States, Health Services Management Research, 10.1177/0951484819858830, 33, 1, (33-42), (2019).
- Lee A. Lindquist, Anne Seltzer, Chris Forcucci, Norine Wong, Vanessa Ramirez-Zohfeld, Leveraging Patient/Community Partnerships to Disseminate Patient Centered Outcomes Research in Geriatrics, Geriatrics, 10.3390/geriatrics4020035, 4, 2, (35), (2019).