Efficacy of selpercatinib as a first-line treatment for RET-fusion positive non-small-cell lung cancer: a novel two-stage Bayesian network meta-analysis
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Single-arm trial data is frequently used during the reimbursement of new oncology interventions. Evaluating treatment effects relative to multiple relevant comparators via network meta-analysis (NMA) using data from single-arm trials; however, remains a challenge. This work introduces a two-stage approach to incorporate single-arm trial data into an NMA and applies this to the LIBRETTO-001 (NCT03157128) trial where selpercatinib (a selective rearranged during transfection [RET] inhibitor) was trialed as a treatment for RET-fusion positive, nonsquamous non-small-cell lung cancer in the first line setting. Materials & methods: Using data from KEYNOTE-189 (NCT02578680) and a real-world database, a pseudo comparator arm was constructed by propensity score matching and adjusted via an acceleration factor to account for the prognostic effect of RET status. NMAs were conducted using a Bayesian random-effects model. Results: The hazard ratios of selpercatinib relative to pemetrexed + platinum-based chemotherapy (the most common comparator in the network used) were found to be 0.304 (95% credible interval [CrI] 0.165, 0.553) and 0.368 (95% CrI 0.178, 0.757) for progression-free survival and overall survival, respectively. The validation of the NMA results could be assessed for progression-free survival of selpercatinib versus pembrolizumab + pemetrexed + platinum-based chemotherapy. A good agreement with published results from the Phase III LIBRETTO-431 trial (NCT04194944) was found (0.586 [95% CrI 0.302,1.123] from the NMA vs 0.46 [95% CI 0.31, 0.70] from LIBRETTO-431 the intention to treat [pembrolizumab] population). Conclusion: The two-stage approach to incorporate single-arm trial data within NMAs is readily applicable within health technology assessment. Enabling the earlier assessment of single-arm trials, via pseudo comparator arms, will provide payers with greater confidence in anticipated treatment effects. In light of the joint clinical assessment, incorporation of single-arm trials within NMA facilitates the reporting of predicted treatment effects relative to multiple relevant comparators, which is important when considering the use of interventions for the global market.
Plain language summary: Using single-arm cancer trials to compare treatments: an example in RET-fusion positive non-small-cell lung cancer
What is this article about?
New cancer medicines are often tested in single-arm trials, where all patients receive the same treatment and there is no direct comparison group. While these studies can show how well a treatment works, they make it difficult to compare new treatments with existing options, which is important for reimbursement and decision making by healthcare payers. In this study, a new two-stage method that allows results from single-arm trials to be included in network meta-analyses is presented. Network meta-analysis is a type of analysis used to compare multiple treatments at the same time. Selpercatinib is a targeted treatment for people with a specific type of lung cancer known as RET-fusion positive non-small-cell lung cancer and a clinical trial of selpercatinib was used as an example for this method. First, a ‘pseudo’ comparison group using data from another clinical trial was created, matching patients as closely as possible to those in the selpercatinib trial. Differences in efficacy related to RET status were then simulated and compared treatments using a Bayesian statistical model.
What were the results?
Our results suggest that selpercatinib improves both the time before disease worsens and overall survival compared with standard chemotherapy. Importantly, our findings were consistent with results from a later Phase III trial, providing reassurance about the validity of the approach.
Why is this important?
This method can help decision makers assess promising cancer treatments earlier and with greater confidence, even when only single-arm trial data are available.
The use of single-arm trial data for conditional approval of oncology drugs is not uncommon, especially in the context of rare cancers or interventions with accelerated approval pathways [1]. However, payers ultimately require some comparison of the new interventions against existing comparators, for instance, through the comparison of progression-free survival (PFS) or overall survival (OS). The efficacy of new interventions must be assessed in relation to appropriate comparators; however, when evidence comes from single-arm trials, this requires reliance on indirect treatment comparisons.
Traditional approaches for generating comparative evidence from single-arm trials rely primarily on indirect treatment comparison methods, with matching-adjusted indirect comparison (MAIC) being the most established technique [2]. MAIC is fundamentally limited to pairwise comparisons and requires individual patient-level data (IPD) from the intervention arm, restricting its applicability when multiple comparators are relevant or when IPD is unavailable. Moreover, unanchored MAIC analyses are increasingly scrutinized by health technology assessment (HTA) bodies due to their sensitivity to unmeasured confounding and the risk of residual bias from incomplete covariate adjustment [3]. Recent work by Rolfo et al. introduced an alternative approach where external data is used to generate a pseudo comparator arm for the single-arm trial, thus retaining the comparison of efficacy within the population of interest. The new approach uses propensity score matching (PSM), propensity score weighting (PSW) or doubly robust methods in order to generate the pseudo comparator arm [4]. Additionally, the approach accounts for different treatment effects in genetically selected populations via the application of acceleration factors derived from external data sets.
This alternative approach to generate efficacy comparisons for single-arm trials has been applied within the context of nonsquamous non-small-cell lung cancer (NSCLC). Rearrangements and/or mutations during transfection (RET) fusions have been identified in 1–2% of nonsquamous NSCLC patients [5]. The prognostic effect of RET status in NSCLC is unclear, but some studies suggest RET-fusion positive patients may have better survival outcomes, although this is may be related to patients' baseline covariates such as younger age, better performance status scores or nonsmoking history [6,7].
The LIBRETTO-001 (NCT03157128) trial was a single-arm trial of first-line use of selpercatinib (Retevmo® or Retsevmo®), a novel, adenosine triphosphate-competitive, highly selective small-molecule inhibitor of RET kinase, in a RET-fusion positive population [8]. Prior to data availability from Phase III trials such as LIBRETTO-431 (NCT04194944) [9,10], the effectiveness of selpercatinib needed to be demonstrated without mature head-to-head data against relevant comparators. Rolfo et al. simulated a comparator arm within the RET fusion positive population for the single-arm LIBRETTO-001 trial and used the Flatiron Health (Foundation Medicine Clinico-Genomics Database [CGDB]) to select real-world control cases. Additionally, historical trials (KEYNOTE-189 [NCT02578680] [11] and REVEL [NCT01168973] [12]) were also used to construct pseudo comparator arms. Selpercatinib was subsequently approved for use in RET-positive NSCLC by the US Food and Drug Administration (FDA) and European Medicines Agency (EMA) based on single-arm data from LIBRETTO-001.
Some trials include only genetically specified groups. In the case of the example presented by Rolfo et al. patient RET status was not assessed in the historical trials. Therefore, acceleration failure time (AFT) models were fit to data from the Flatiron database and the acceleration factors applied to the matched comparator arms to simulate the prognostic effect of RET status on survival [4].
Within this work, we build on the approach described by Rolfo et al. which presented estimates of comparative efficacy relative to the pseudo comparators only. We therefore introduce a two-stage approach to facilitate the incorporation of single-arm trial data within a Bayesian network meta-analysis (NMA) to enable the comparison with multiple relevant comparators. The two-stage approach includes the construction of a pseudo comparator arm, as in Rolfo et al., and the inclusion of the single arm trial data within an NMA via the pseudo comparator arm. This work demonstrates how single-arm trial data can be combined within a network of evidence, which subsequently allows for the comparison with any connected relevant comparator, which is highly relevant given the introduction of the European Joint Clinical Assessment.
Here, we present this two-stage approach through the lens of the LIBRETTO-001 case study. We present the relative efficacy of selpercatinib versus relevant comparators identified within a systematic literature review (SLR). Hazard ratios (HRs) for PFS and OS were evaluated using the pseudo comparator arm with and without the adjustment for RET status and are subsequently incorporated within an NMA. The results of the NMA of PFS are subsequently compared with recently published Phase III trial results from the LIBRETTO-431 trial. This work highlights the potential value of this two-stage methodology for the analysis of single-arm trials within a HTA context and the subsequent assurance that could be provided to payers should this methodology be adopted more broadly [9,10].
Materials & methods
Systematic literature review
A systematic literature review (SLR), in accordance with the PRISMA guidelines [13], was conducted to identify recent randomized controlled trials (using the SLR update conducted in July 2021) which report the efficacy of selpercatinib or relevant comparators for treatment-naive (first-line) patients with nonsquamous NSCLC for inclusion within the NMA. Study eligibility was based on the inclusion criteria defined via patients, interventions, comparators, outcome and study design, this is summarized in Supplementary Material 1 which highlights the overall strategy.
The SLR was conducted and updated at four timepoints, referred to as SLR1-SLR4. Screening was conducted using Endnote X71 and then exported to Microsoft Excel for SLR1 and SLR2, and the DistillerSR® tool was used for SLR3 and SLR4. Two researchers screened the identified studies according to the inclusion criteria, and any disagreements were resolved by consensus or via consultation with a third researcher. Screening was conducted first according to the title and abstracts and secondly via full text review. Data were then extracted by a single researcher and validated by a second researcher. Any discrepancies between the extracted data were discussed and reviewed by a third researcher.
Simulation of a pseudo comparator arm for the LIBRETTO-001 trial
The KEYNOTE-189 trial was selected for use in construction of the pseudo comparator arm for the LIBRETTO-001 trial primarily as this was the only study identified within the SLR with available IPD. Additionally, the comparator arm, pemetrexed + platinum-based chemotherapy (PEMc + PLATi), is a common comparator in clinical trials of immunotherapies for nonsquamous NSCLC. Further to this, PEMc + PLATi was identified as the most common comparator identified within the SLR and thus the choice of the KEYNOTE-189 trial promoted a larger likelihood of a connected network within the NMA.
The pseudo comparator arm was generated using the approach introduced by Rolfo et al. [4], by matching for all available covariate data including; age, proportion of female patients, proportion of patients who have never smoked, Eastern Cooperative Oncology Group (ECOG) performance status score, race and stage at diagnosis. Matching replicated randomization by identifying control individuals who are similar to the treated individuals in one or more characteristics. The aim when generating the pseudo comparator arm was to weigh or match the comparator data (from KEYNOTE-189) such that the baseline characteristics matched the reported characteristics of the LIBRETTO-001 data, this approach therefore produces an average treatment effect among the treated patients with the treated population as the target population.
Several matching approaches were trialed including; PSM, genetic matching, PSW using logistic regression (via the ‘twang’ package in R) and doubly robust targeted minimum loss-based estimation (TMLE) [14]. The program code for the PSM and PSW approaches are included in Supplementary Materials 2 & 3, respectively. The detailed methods used for TMLE are included in Supplementary Material 4. These matching approaches rely on adequate overlap of baseline characteristics between trial populations. While baseline characteristics were reviewed qualitatively, no formal quantitative assessment of overlap was conducted, which may impact the robustness of the estimates. Matching and balance diagnostics were used to assess the success of the matching or weighting approaches. The effective sample size of the PSW approach was also considered. Standard model diagnostics were assessed as part of the TMLE process, including checks on model convergence and stability of estimates.
Adjustment for RET status
Following the approach presented in Rolfo et al. the Weibull, log-normal and log-logistic AFT models were fit to the Flatiron dataset and subsequently the best fitting model identified via consideration of the R2 statistic. The R2 statistic was used as supportive evidence for our model selection; however, more standard measures of statistical fit such as the Akaike Information Criterion or the Bayesian Information Criterion, are typically preferred when comparing alternative model specifications in applied comparative analyses [15–17]. The corresponding acceleration factor was then used to adjust the pseudo comparator data to account for RET status. Separate acceleration factors for PFS and OS were evaluated. The acceleration factors provide an interpretable measure of how RET status modifies the expected time to progression or death, enabling direct adjustment of survival times in the comparator cohort for a more accurate indirect comparison.
Estimation of treatment effects
OS was defined as the time between randomization (or start of treatment for LIBRETTO-001) and the date of death due to any cause. PFS was defined as the time between randomization (or start of treatment for LIBRETTO-001) and the date of progressive disease or death, respectively. Treatment efficacy for OS and PFS was summarised by assuming proportional hazards and reporting the estimated HRs. The proportional hazards assumption was assessed using the method described by Grambsch and Therneau via the cox.zph function in R [18].
For studies where IPD was not available and the HR was not reported, Kaplan–Meier curves were digitized using WebPlotDigitizer [19] and the IPD reconstructed using the Guyot algorithm [20]. The reconstructed IPD was then used to evaluate the HR and the 95% CI via a Cox proportional hazards model. The HR corresponding to the comparison of selpercatinib and PEMc + PLATi from the LIBRETTO-001 trial and pseudo comparator arm, was evaluated using the available IPD.
NMA of hazard ratios
Networks of evidence were generated for OS and PFS using the included studies identified in the SLR. The LIBRETTO-001 trial was connected to the networks via the simulated pseudo comparator arm.
To synthesize the HRs of OS and PFS, a Bayesian random-effects approach was chosen as a base case to enable the explicit modelling of the heterogeneity between studies, see Supplementary Material 5 for the model formulation. A Bayesian fixed-effects NMA was also implemented and assessed for model fit, see Supplementary Material 6 for the model formulation. The models were based on the methodology by Woods et al. for time-to-event analyses [21].
Priors on the study-specific baseline terms and the treatment effects were assumed to be normal with a mean of zero and variance of 1002, as recommended in NICE Technical Support Document 2 [22]. For the random-effects model, both noninformative uniform priors bounded between 0 and 8 and informative priors were trialed for the between study variance [23]. The informative priors for the between-study variance for the OS and PFS analyses correspond to the priors recommended by Turner et al. [23]. These were log normal distributions with parameters (-4.18, 1.412) and (-3.95, 1.792), respectively, and were chosen in cases where there was low convergence or implausible reported credible intervals (CrI).
The Bayesian NMA models were evaluated using Markov chain Monte Carlo and convergence and autocorrelation between subsequent samples was assessed via caterpillar, density, Brooks–Gelman–Rubin, and autocorrelation plots [24]. A burn-in period of 50,000 samples was chosen, and a further 100,000 samples recorded to generate treatment effect posterior distributions. No thinning of the chains was applied. The NMA was performed using JAGS (Just Another Gibbs Sampler) [25]. In cases where convergence was not evident or there was high correlation, an increase to the number of (burn-in) samples and thinning was considered.
Model fit
In order to assess the fit of the random-effects and fixed-effect models, the deviance (D) was measured and compared between models. The model deviance information criterion was used to assess relative model fits. The total residual deviances for each of the models were also compared with the respective number of data points to assess absolute model fit [26].
Assessment of inconsistency & heterogeneity
Inconsistency was assessed via the inconsistency versus consistency method which compares the residual deviances between the two approaches [27].
Heterogeneity was assessed by considering: (1) whether the trial populations were sufficiently similar and therefore combinable, and (2) whether treatment effects were consistent across trials.
Study to validate NMA results
The LIBRETTO-431 trial is a Phase III trial of treatment with selpercatinib or pemetrexed + platinum-based chemotherapy with or without pembrolizumab. The study reports the HR for PFS and was selected to allow for comparison of the predicted PFS HR using the new two-stage approach to incorporate the LIBRETTO-001 trial data within an NMA. As a biomarker-selected, head-to-head Phase III trial with mature PFS data, LIBRETTO-431 was chosen to validate NMA outputs because it provides an internally controlled, population-relevant estimate of treatment effect against commonly used comparators.
Results
SLR & networks of evidence
A total of 70 studies reported in 77 peer-reviewed publications and 44 conference abstracts were included within the SLR which focused on first-line and first-line to progression treatment. Out of these studies, 58 studies reported first-line to progression treatment and included comparators of interest for selpercatinib. Detailed reasons for study exclusion within the SLR are included in Supplementary Material 7.
Out of the 58 studies, 35 were connected within networks and could be analyzed in the NMA; 34 studies reporting OS and 29 studies reporting PFS, Figures 1 & 2 & Supplementary Material 8. In addition to these studies, the LIBRETTO-001 trial was connected to the network via the pseudo comparator arm generated from the KEYNOTE-189 trial, as detailed in the following section.
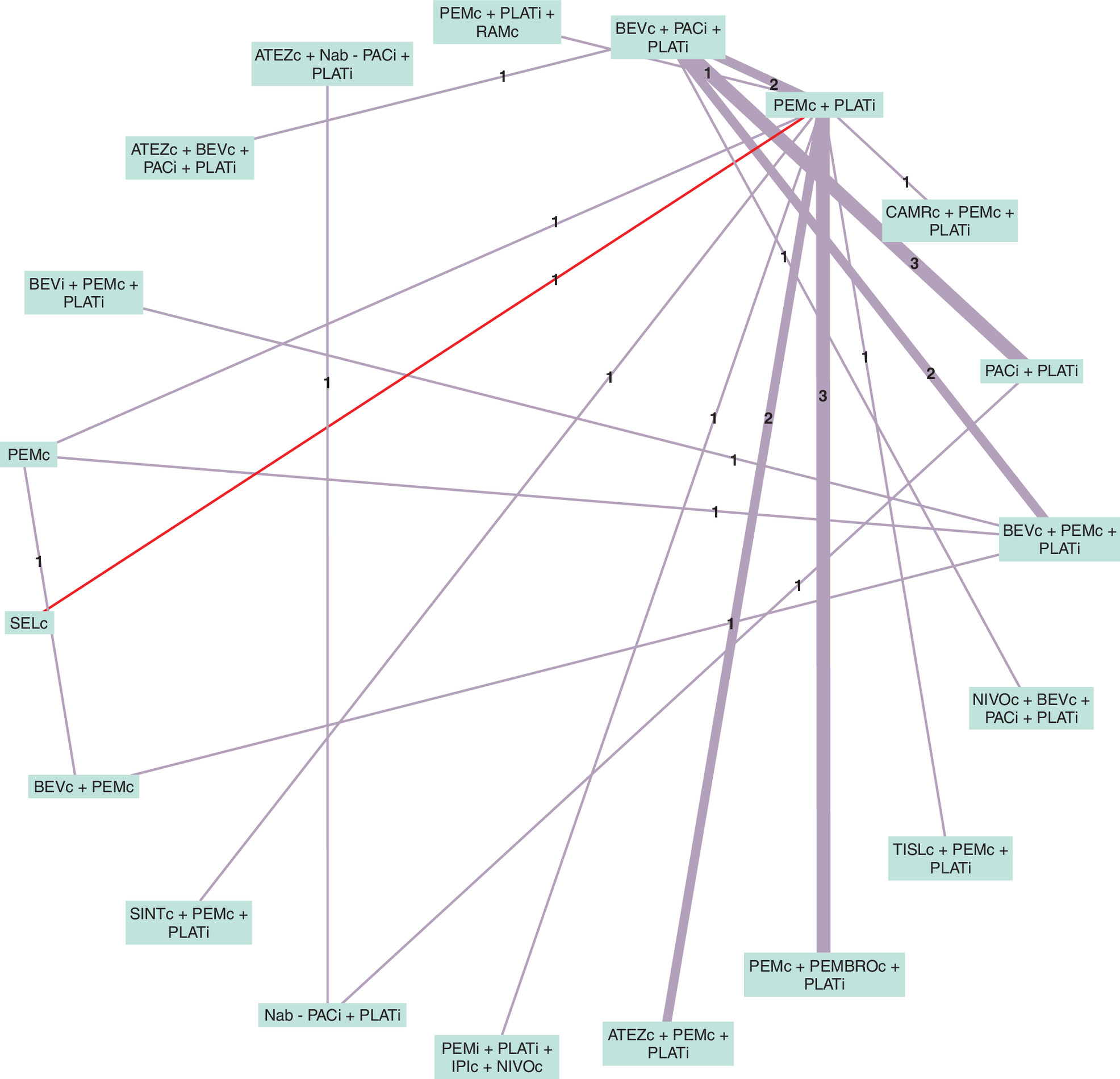
Figure 1. Network diagram for progression-free survival.
Numbers on edges are the number of studies with direct evidence of that comparison. Red edge indicates the pseudo comparator comparison for selpercatinib. Numbers on edges are the number of studies with direct evidence of that comparison.
ATEZ: Atezolizumab; BEV: Bevacizumab; c: Continuous; CAMR: Camrelizumab; CEMIPL: Cemiplimab; i: Induction; IPI: Ipilimumab: Nab-PAC: Nab-paclitaxel; NIVO: Nivolumab; PAC: Paclitaxel; PEM: Pemetrexed; PEMBRO: Pembrolizumab; PLAT: Platinum; RAM: Ramucirumab; SEL: Selpercatinib; SINT: Sintilimab; TISL: Tislelizumab.
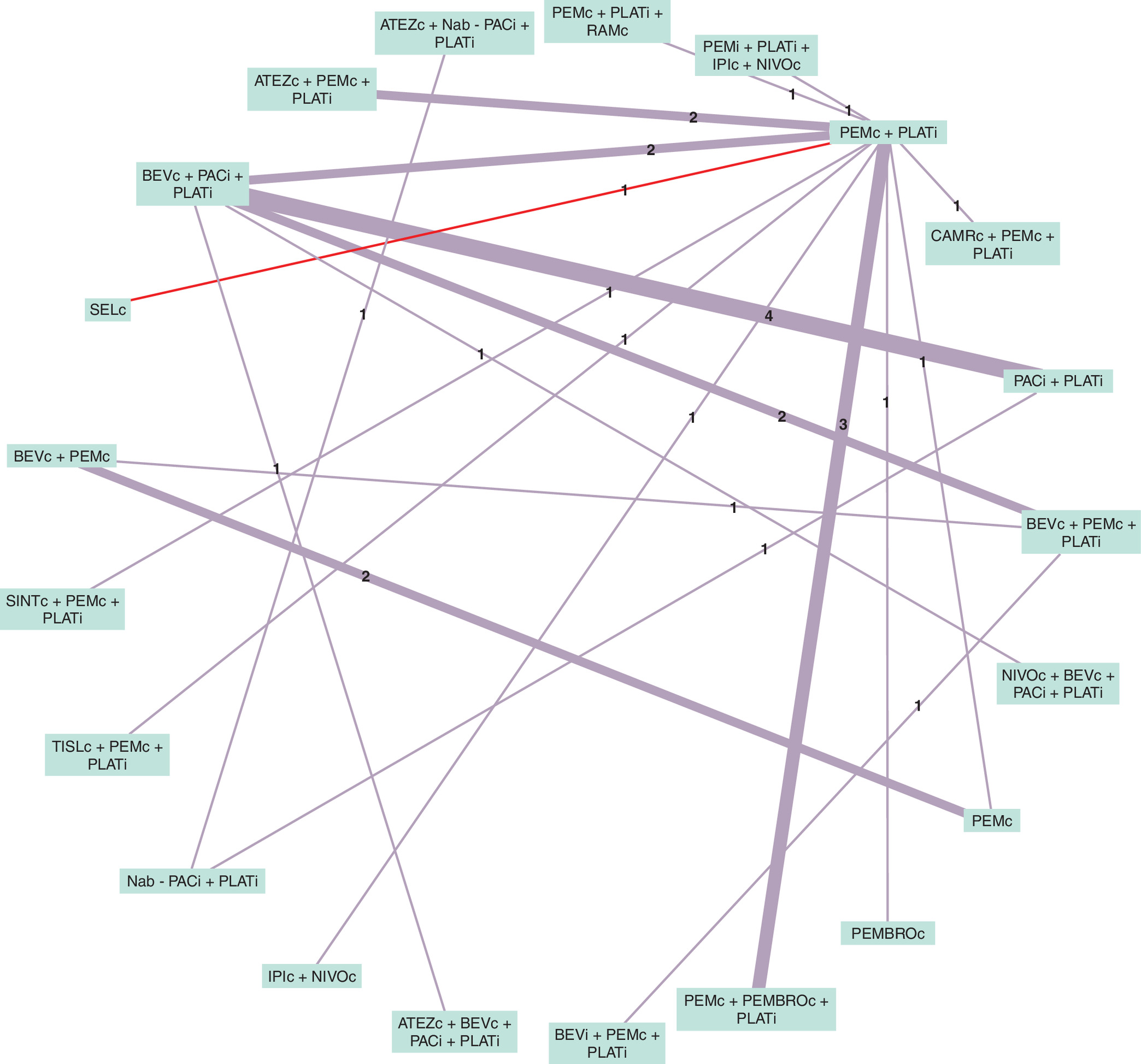
Figure 2. Network diagram for overall survival.
Numbers on edges are the number of studies with direct evidence of that comparison. Red edge indicates the pseudo comparator comparison for selpercatinib.
ATEZ: Atezolizumab; BEV: Bevacizumab; c: Continuous; CAMR: Camrelizumab; CEMIPL: Cemiplimab; i: Induction; IPI: Ipilimumab: Nab-PAC: Nab-paclitaxel; NIVO: Nivolumab; PAC: Paclitaxel; PEM: Pemetrexed; PEMBRO: Pembrolizumab; PLAT: Platinum; RAM: Ramucirumab; SEL: Selpercatinib; SINT: Sintilimab; TISL: Tislelizumab.
Generation of a pseudo comparator arm for selpercatinib
To facilitate the matching of patients between the LIBRETTO-001 trial and the KEYNOTE-189 comparator arm, five patients from the LIBRETTO-001 were excluded due to missing data or ECOG performance status scores equal to 2 at baseline which was not represented within the KEYNOTE-189 comparator arm.
Four approaches to match patients from the KEYNOTE-189 comparator arm to the LIBRETTO-001 were trialed: PSM, genetic matching, PSW (logistic regression) and TMLE. All approaches substantially improved the similarity in patient characteristics between the KEYNOTE-189 and LIBRETTO-001 arms, Table 1 & Supplementary Material 9. Based on clinical plausibility and the decision to present conservative estimates, results from the PSM approach are presented here and used within the subsequent NMA. The utilization of the PSM approach resulted in the most conservative estimations of treatment effect. This was due to the PSM approach resulting in the highest median PFS and OS for the pemetrexed plus platinum chemotherapy arm compared with the other three approaches. This was deemed to be externally valid as patients in the LIBRETTO-001 trial were typically younger and healthier than the broader advanced NSCLC population generally. As a result, the mean age of the pemetrexed plus platinum chemotherapy arm of the KEYNOTE-189 trial was reduced in the adjustment process thus resulting in increased median PFS and OS. The standardized differences and variance ratio plot before and after propensity matching is presented in Supplementary Material 9. Adjusted baseline characteristics and resulting Kaplan–Meier survival curves for the three other matching/weighting approaches are included in Supplementary Material 9.
| LIBRETTO-001 | KEYNOTE-189 | ||
|---|---|---|---|
| Characteristic | Selpercatinib (N = 64) | Before PSM | After PSM |
| PEMc + PLATi (N = 206) | PEMc + PLATi (N = 64) | ||
| Age (mean, years) | 60.64 | 62.84 | 61.19 |
| ECOG performance status = 1, % | 60.9% | 60.8% | 68.8% |
| Female, % | 60.9% | 47.1% | 59.4% |
| Never smoked, % | 68.8% | 12.3% | 39.1% |
| Race: Asian, % | 18.8% | 3.9% | 12.5% |
| Race: Other (non-white, non-Asian, unknown), % | 10.9% | 1.5% | 4.7% |
| Stage III, % | 3.1% | 0.5% | 1.6% |
| Stage IV, % | 93.8% | 99.5% | 98.4% |
c: Continuous; ECOG: Eastern Cooperative Oncology Group; i: Induction; PEM: Pemetrexed; PLAT: Platinum; PSM: Propensity score matching.
The Kaplan–Meier curves for PFS and OS were generated for the LIBRETTO-001 data and the matched pseudo comparator arm from the KEYNOTE-001 (using PSM without adjustment for RET status), Figure 3.
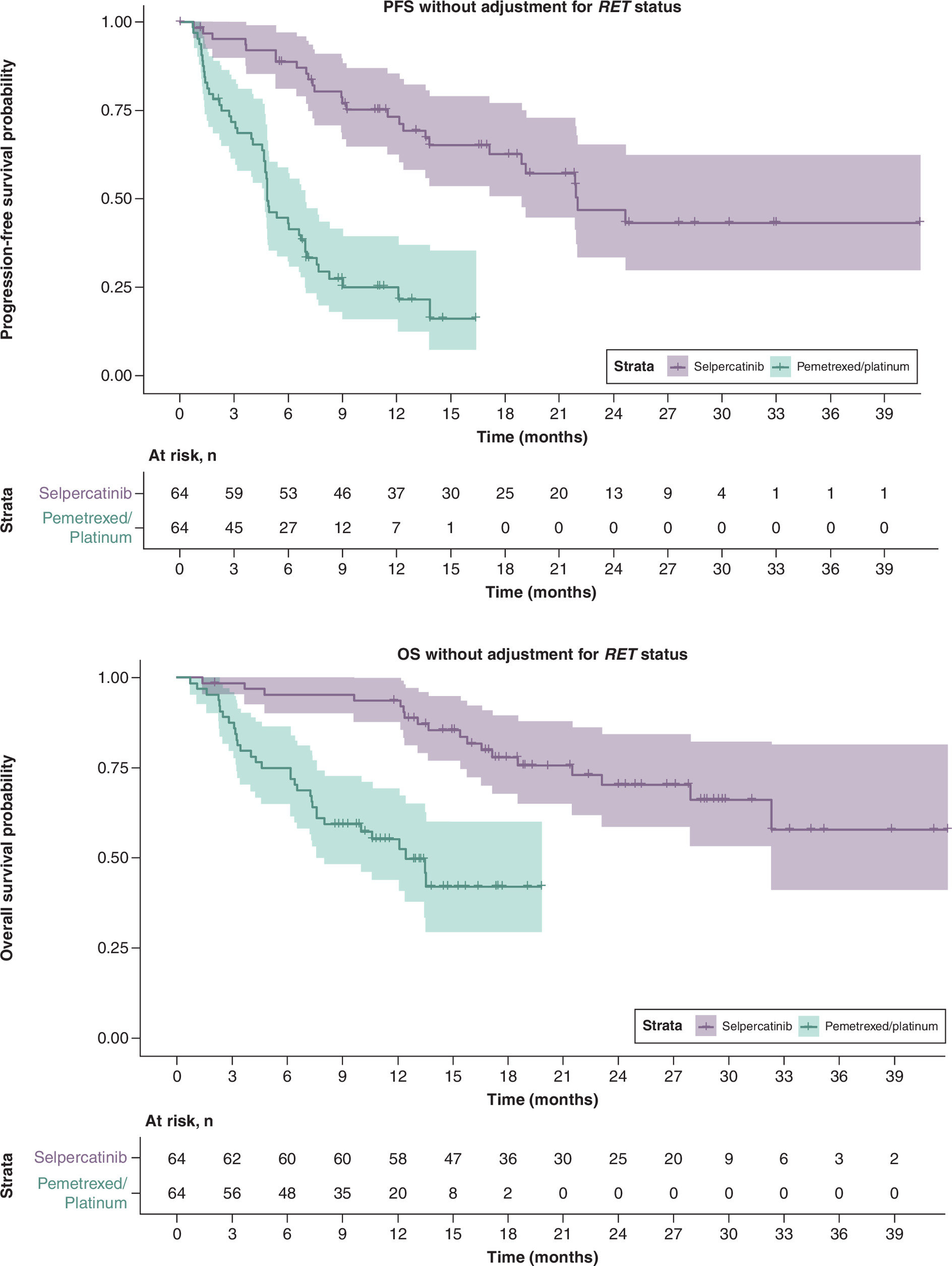
Figure 3. Kaplan–Meier curves for progression-free survival and overall survival of the LIBRETTO-001 data and the pseudo comparator arm generated by propensity score matching of KEYNOTE-189 individual patient-level data, respectively, without adjustment for RET status.
OS: Overall survival; PFS: Progression-free survival.
The nonparametric log rank test and Cox regressions were performed to obtain estimates of the HR and 95% CI for OS and PFS. Statistically significant differences in risk of death or progression event were found between the selpercatinib arm and pseudo comparator arm (PEMc + PLATi), with p < 0.001 for both OS and PFS. The HR was estimated to be 0.203 (95% CI; 0.118, 0.350) for PFS and 0.205 (95% CI; 0.106, 0.399) for OS, indicating a significantly reduced hazard of death or progression for patients treated with selpercatinib relative to those treated with PEMc + PLATi.
RET status adjustment
In addition to the matching of baseline characteristics, the potential prognostic effect of RET status was simulated within the pseudo comparator arm. The log-logistic AFT model was found to be the best fitting model to the Flatiron dataset for both PFS and OS according to the R2 values. The acceleration factors were 0.4281 (standard error (SE); 0.1659) and 0.5715 (SE; 0.2246) for PFS and OS, respectively. The Weibull and log-normal AFT models were also fitted, model R2 statistics derived from the Weibull and lognormal models are reported in Supplementary Material 10.
The acceleration factors were applied to the PSM pseudo comparator arm, and the HRs re-evaluated using Cox proportional hazards. The acceleration factors were applied to patients in the pseudo comparator arm as in Rolfo et al. Analytic Strategy 3, as patient RET status was not known in the KEYNOTE-189 trial. The updated HRs were equal to 0.304 (95% CI; 0.177, 0.520) and 0.369 (95% CI; 0.181, 0.752) for PFS and OS, respectively, and the Kaplan–Meier curves were updated, Figure 4.
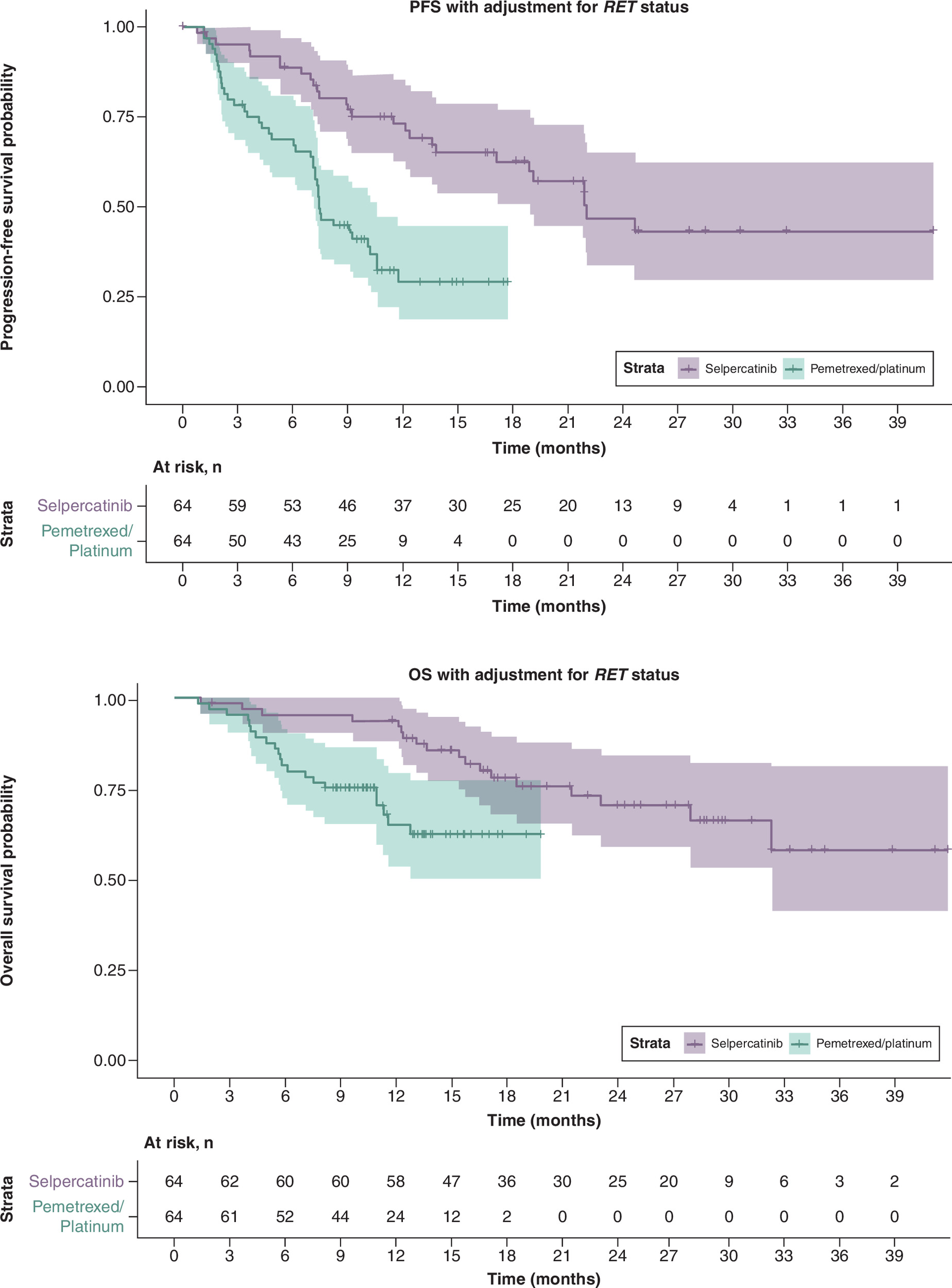
Figure 4. Kaplan–Meier curves for progression-free survival and overall survival of the LIBRETTO-001 data and the pseudo comparator arm generated by propensity score matching of KEYNOTE-189 individual patient-level data, respectively, with adjustment for RET status.
OS: Overall survival; PFS: Progression-free survival.
Adjusted Kaplan–Meier survival curves for the three other matching/weighting approaches with adjustment for RET status are included in Supplementary Material 9.
Network meta-analyses of PFS & OS
The HRs for each study within the network were evaluated using reconstructed individual patient data if not reported within the trial publications, and all studies were subject to testing of the proportional hazards assumption. Six studies were identified to potentially violate the proportional hazards assumption within the PFS and OS networks. Details are provided in Supplementary Material 8.
Random-effects models were chosen to account for the effects of between-study heterogeneity. Noninformative priors were chosen to analyze OS and PFS due to minimal differences in deviance information criterion between the random-effects and fixed-effect models, see Supplementary Material 11. Additionally, when the informative priors were used, model fit statistics were not significantly improved. No inconsistency was detected in the PFS and OS networks, see Supplementary Material 11.
Progression-free survival
The forest plot of the posterior median HR for comparators versus PEMc + PLATi for PFS, where adjustment for RET status was performed when generating the pseudo comparator arm for the LIBRETTO-001 trial, is shown in Figure 5. The NMA of PFS showed that treatment with selpercatinib [HR [95% CrI]; 0.304 [0.165, 0.553]), SINTc + PEMc+PLATi (0.482 [0.323, 0.720]), PEMc + PEMBROc+PLATi (0.516 [0.402, 0.681]), NIVOc + BEVc+PACi + PLATi (0.569 [0.361, 0.906]), ATEZc + BEVc+PACi + PLATi (0.577 [0.382, 0.887]), ATEZc + PEMc+PLATi (0.600 [0.467, 0.811]) and CAMRc + PEMc+PLATi (0.601 [0.403, 0.890]) have statistically significant, lower hazards of progression or death when compared to treatment with PEMc + PLATi, Figure 5. This was mirrored in the analysis when adjustment for RET status was not included during simulation of the pseudo comparator arm, Supplementary Material 12. Treatment with PACi + PLATi (1.757 [1.275, 2.581]) and Nab-PACi + PLATi (1.640 [1.027, 2.828]) were shown to increase hazard of progression or death relative to treatment with PEMc + PLATi, both with and without adjustment for RET status, Figure 5 & Supplementary Material 12. All other treatments had comparable HRs relative to PEMc + PLATi.
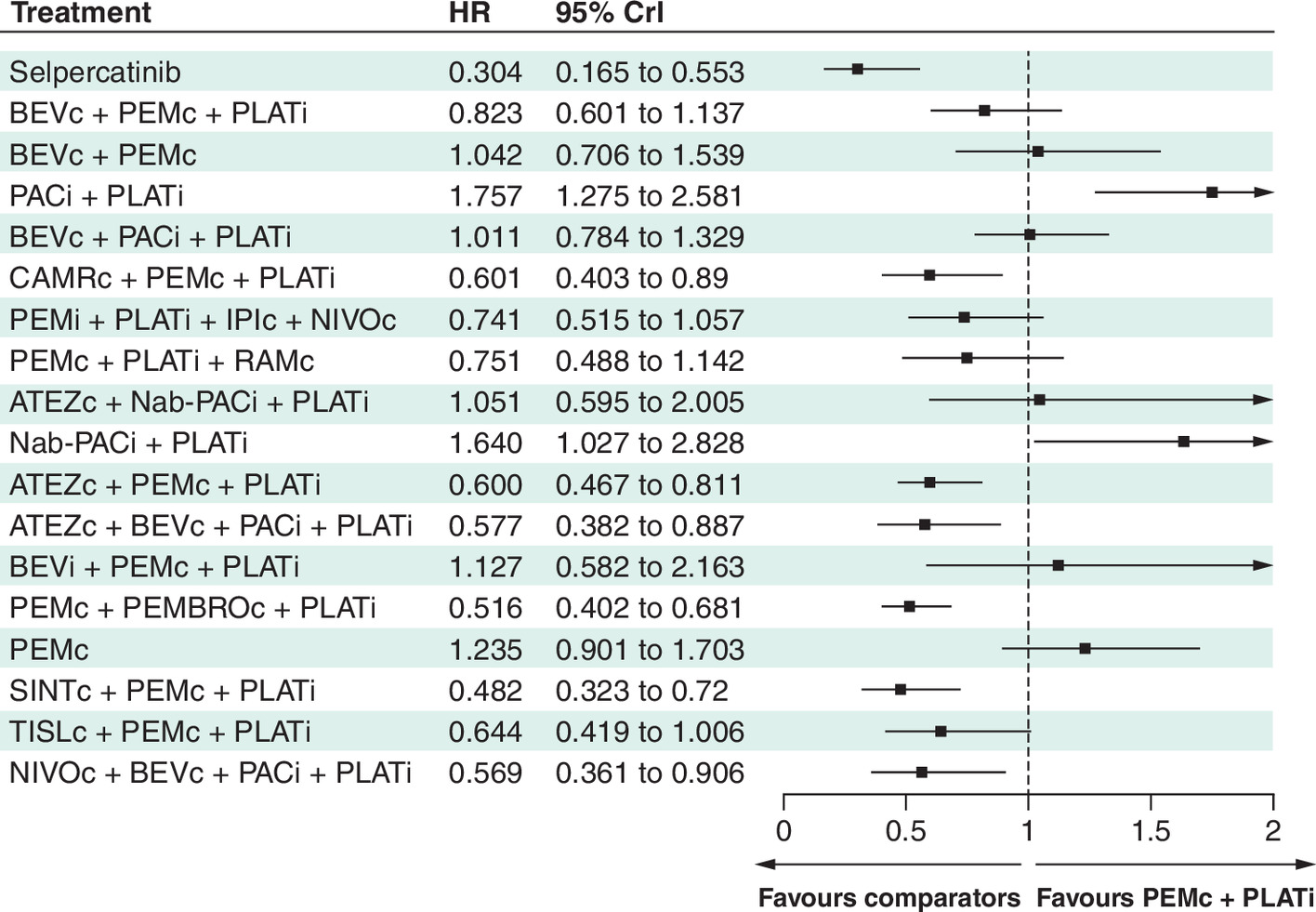
Figure 5. Forest plot, posterior median progression-free survival hazard ratio and the 95% credible intervals of comparators versus PEMc + PLATi.
Null HR value of one indicated with grey dashed line.
ATEZ: Atezolizumab; BEV: Bevacizumab; c: Continuous; CAMR: Camrelizumab; CEMIPL: Cemiplimab; Crl: Credible interval; HR: Hazard ratio; i: Induction; IPI: Ipilimumab: Nab-PAC: Nab-paclitaxel; NIVO: Nivolumab; PAC: Paclitaxel; PEM: Pemetrexed; PEMBRO: Pembrolizumab; PLAT: Platinum; RAM: Ramucirumab; SINT: Sintilimab; TISL: Tislelizumab.
Forest plots comparing the efficacy of comparator interventions, relative to selpercatinib show the superior efficacy of selpercatinib for PFS relative to existing alternative comparators, Supplementary Material 13. Pairwise HRs for PFS are presented in Supplementary Material 14.
Overall survival
Figure 6 shows the forest plot of the posterior median HR of comparators versus PEMc + PLATi for OS where the HR for selpercatinib versus PEMc + PLATi was adjusted to account for RET status. The NMA of OS suggested that treatment with selpercatinib (HR [95% CrI]; 0.368 [0.178,0.757]), SINTc + PEMc+PLATi (0.608 [0.384,0.961]), PEMc + PEMBROc+PLATi (0.609 [0.490,0.761]) and PEMi + PLATi+IPIc + NIVOc (0.691 [0.510,0.931]), have statistically significant, lower hazards of death relative to treatment with PEMc + PLATi, Figure 6. As for the analysis of PFS, predicted treatment effects were mirrored in the analysis without adjustment for RET status, Supplementary Material 12. All other treatments had HRs comparable to treatment with PEMc + PLATi. Forest plots comparing the efficacy of comparators, relative to selpercatinib show the greater efficacy of selpercatinib relative to other comparators for OS, Supplementary Material 13. Pairwise HRs for OS are presented in Supplementary Material 15.
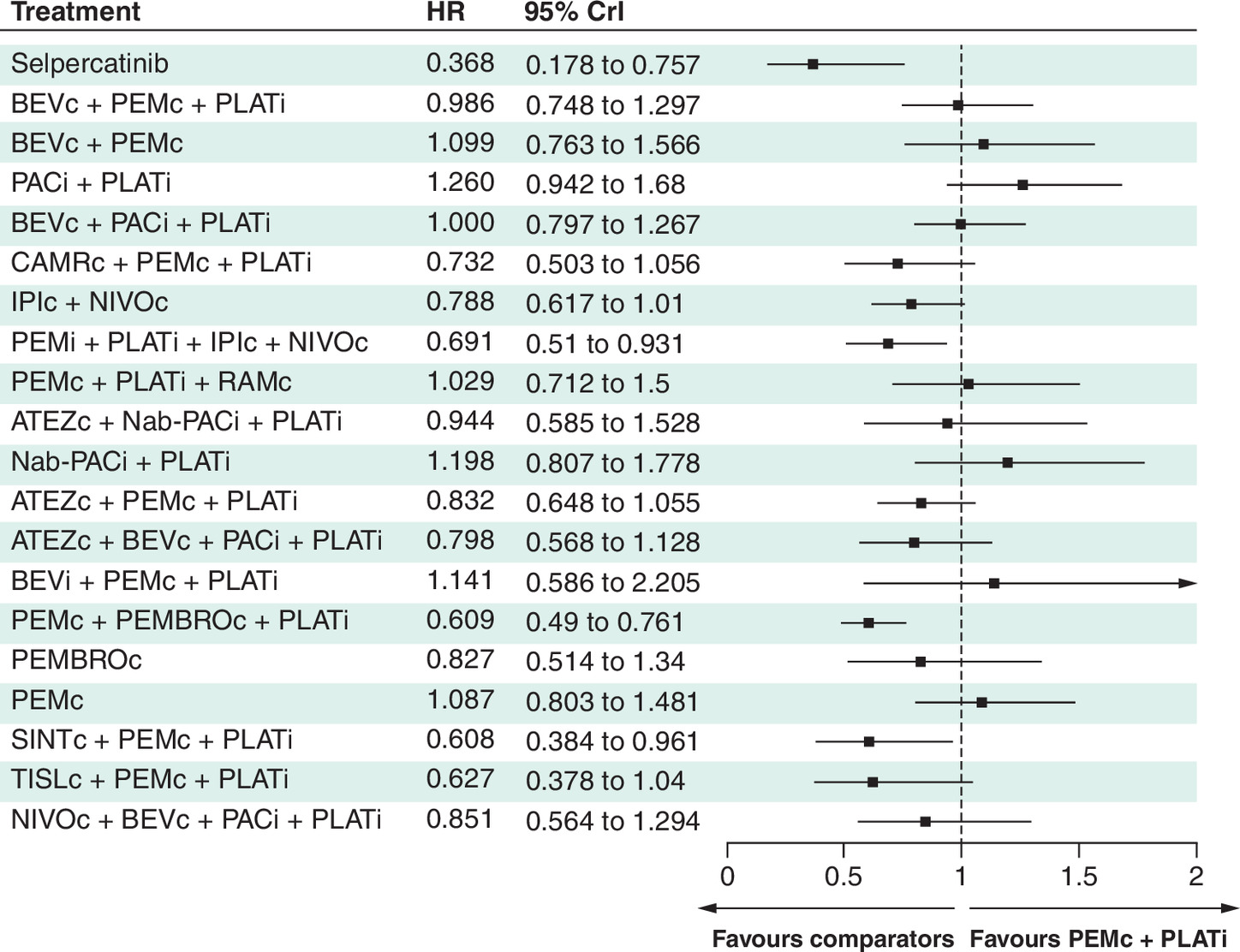
Figure 6. Forest plot, posterior median overall survival hazard ratio and the 95% credible intervals of comparators versus PEMc + PLATi with RET status adjustment.
Null HR value of one indicated with grey dashed line.
ATEZ: Atezolizumab; BEV: Bevacizumab; c: Continuous; CAMR: Camrelizumab; CEMIPL: Cemiplimab; Crl: Credible interval; HR: Hazard ratio; i: Induction; IPI: Ipilimumab: Nab-PAC: Nab-paclitaxel; NIVO: Nivolumab; PAC: Paclitaxel; PEM: Pemetrexed; PEMBRO: Pembrolizumab; PLAT: Platinum; RAM: Ramucirumab; SINT: Sintilimab; TISL: Tislelizumab.
Discussion
We present a two-stage approach to incorporate single-arm studies into NMA. Additionally, we demonstrate that, through the use of acceleration factors when generating the pseudo comparator arm, impacts to intervention efficacy due to genetically selected populations can be accounted for.
The implementation of the proposed approach is demonstrated using the single-arm LIBRETTO-001 trial which assessed the effectiveness of selpercatinib in patients with RET fusion-positive nonsquamous NSCLC as a first-line therapy but was not designed to assess the relative treatment effect of selpercatinib versus other relevant comparators. The relative efficacy of selpercatinib, using OS and PFS end points was evaluated through the generation of a pseudo comparator arm based on individual patient data from the KEYNOTE-189 trial. As the KEYNOTE-189 trial did not select patients based on RET status, the potential prognostic effect of RET positive tumors was simulated through adjustment via an acceleration factor derived from the Flatiron dataset. The generation of the pseudo comparator arm, followed the methods first presented by Rolfo et al. [4], but the subsequent incorporation of the single arm trial into an NMA via the pseudo comparator arm represents a novel, two-stage, approach to facilitate earlier assessment of Phase I/II trial data and the generation of predicted treatment effects relative to multiple potential comparators.
Recently published results from LIBRETTO-431, a Phase III trial of treatment with selpercatinib or pemetrexed + platinum-based chemotherapy with or without pembrolizumab, reports HRs for PFS. For the intention to treat with pembrolizumab group, the reported PFS HR was equal to 0.46 [95% CI 0.31, 0.70] [9]. We are able to therefore compare the HR derived from the NMA for selpercatinib versus pemetrexed + platinum-based chemotherapy + pembrolizumab with the HR for the intention to treat (pembrolizumab) group in LIBRETTO-431. The HR from the NMA was 0.586 [95% CrI 0.302,1.123] when the potential prognostic effect of RET status was incorporated into the generation of the pseudo comparator arm. The point estimate from the NMA is reasonably close to that from LIBRETTO-431 but has a wider 95% CrI that spans HR = 1. The NMA estimate reflects a treatment effect averaged over a more heterogeneous population than that of the LIBRETTO-431 trial, and this greater heterogeneity contributes to the broader credible interval. Notably, the confidence interval from LIBRETTO-431 is entirely contained within the NMA credible interval, indicating good agreement between the results and reflecting the narrower, more homogeneous trial population. Although we have applied this two-stage approach within a case study which now has a markedly different treatment landscape due to the routine use of immunotherapies, the approach presented within this work could be readily applied within other disease areas and treatment networks.
As mentioned previously, an alternative approach to provide estimations of selpercatinib efficacy using single arm trial data relative to comparators, could include MAIC whereby the individual patient data from the LIBRETTO-001 trial is matched to summary baseline characteristics of the comparator from a second trial. This approach is widely used within HTA but can suffer from several limitations. The incorporation of single arm trials via a pseudo comparator arm within an NMA therefore, offers an attractive alternative, where relative efficacy can be readily reported relative to all relevant comparators in the appropriate target population.
Within this analysis there remained some uncertainty around the estimated treatment effects due to the choice of matching/weighting methodology to generate the pseudo comparator arm. A wide variety of matching/weighting procedures have been proposed in the literature and, currently, there is no consensus on the optimum procedure, this is therefore an area primed for additional research [28]. However, by trialing multiple methods, scenarios of efficacy can be provided to provide payers with an appreciation of potential uncertainty relating to methodological choices.
The use of an acceleration factor derived from external data represents a limitation, as it assumes that the effect of RET status on survival is preserved and transportable to the KEYNOTE-189 population. This requires comparability in patient characteristics, treatment context, and the absence of substantial effect modification, which cannot be fully verified.
A limitation of the current analysis is the reliance on the proportional hazards assumption, which may be violated in some studies within the network. While synthesis of HRs under this assumption is standard practice in HTA, we acknowledge that alternative approaches could be applied to address potential nonproportional hazards. For example, time-varying hazard models, such as fractional polynomial models or piecewise hazard approaches, could be considered where the proportional hazards assumption does not hold. Future work could explore these methods to assess robustness of treatment effect estimates under more flexible hazard structures.
Additionally, within this NMA it is assumed that the treatment effects in other trials within the network are independent of RET fusion status, as in they would be assumed to be unchanged if the patients were all RET fusion positive. This assumption is considered reasonable based on the mechanisms of action of these treatments. Standard chemotherapies exert their effects through nonspecific cytotoxic mechanisms that target rapidly dividing cells, independent of oncogenic driver mutations such as RET fusions. Similarly, immune checkpoint inhibitors act by modulating the host immune response rather than directly targeting tumor-specific genetic alterations. As RET fusions primarily act as oncogenic drivers that are specifically targeted by RET inhibitors, there is limited biological plausibility that RET fusion status would materially modify the efficacy of these nontargeted treatment modalities. In the absence of evidence suggesting differential treatment effect by RET status for chemotherapy or immunotherapy in this disease setting, it is therefore a reasonable simplifying assumption to treat the relative effects of these comparators as invariant across RET fusion-positive and unselected populations within the network meta-analysis. That said, we acknowledge that empirical data directly assessing effect modification by RET status are limited, and this represents an assumption that introduces some uncertainty into the analysis.
The use of informative heterogeneity priors to address convergence issues also represents a potential limitation, as results may be sensitive to the choice of prior. Although not explored here due to the methodological focus of the study, sensitivity analyses to alternative prior specifications would be important in applied settings. Incomplete data are often present within randomized controlled trials and the issue of missing data could limit the applicability of this approach as exclusions or imputation decisions may introduce bias or affect generalizability. The potential implications of missing data should therefore be handled carefully and transparently.
More generally, the limitations in evidence include small sample sizes, the lack of a comparison group, and failure to adjust for other baseline prognostic factors such as programmed death ligand-1 (PD-L1) expression or smoking status during generation of the pseudo comparator arm [29–36].
To the best of the authors' knowledge this is the first time this two-stage approach has been used to incorporate data from a single-arm trial within an NMA and subsequently predict relative treatment effects close to those emerging from Phase III trials. Considering the limitations stated above, results of relative efficacy when using this approach should be considered with some degree of caution and this methodology should not be considered as a replacement for randomized controlled trials. The implementation of this two-stage approach should be considered in alternative treatment areas in different indications to assess the potential impact of this approach more broadly. However, the methodology presented within this work, demonstrates a potential approach to assess early trial data arising from single-arm trial designs. This will help to provide estimates of relative efficacy, earlier within the assessment process and better inform payers. This will in turn better inform decision-making relating to subsequent trials and increase patient access to potentially highly effective treatments.
Summary points
•
Single-arm trials are commonly used to support reimbursement submissions for new oncology therapies, but they pose challenges for comparative effectiveness assessment.
•
Incorporating single-arm trial evidence into network meta-analyses (NMAs) requires methods to address the absence of a randomized comparator.
•
This study proposes a two-stage Bayesian framework to integrate single-arm trial data within an NMA.
•
The approach was applied to the LIBRETTO-001 trial of selpercatinib in first-line RET-fusion positive, nonsquamous non-small-cell lung cancer.
•
A pseudo comparator arm was constructed using propensity score matching based on data from KEYNOTE-189 and a real-world database.
•
An acceleration factor was applied to adjust for the prognostic effect of RET status on survival outcomes.
•
Treatment effects were estimated using Bayesian random-effects NMAs for progression-free survival and overall survival.
•
Selpercatinib demonstrated favorable hazard ratios versus pemetrexed plus platinum-based chemotherapy for both outcomes.
•
Validation against results from the Phase III LIBRETTO-431 trial showed good agreement, supporting the credibility and applicability of the proposed method in health technology assessment.
Author contributions
Authors M-H Jen, U Kiiskinen and T Puri were responsible for study conception and design; authors M-H Jen, M Khanal and R Goel were responsible for acquisition of data; authors M-H Jen, MD Sonksen, X Wang, M Khanal, R Goel and JE Forsyth were responsible for data analysis, and drafting and revision of the manuscript.
Financial disclosure
The compilation of the draft manuscript by JE Forsyth was supported by funding from Eli Lilly & Company (IN, USA). The authors have received no other financial and/or material support for this research or the creation of this work apart from that disclosed.
Competing interests disclosure
M-H Jen, T Puri, M Khanal, U Kiiskinen, A Jyothi, R Goel, MD Sonksen and X Wang are all full-time employees of Eli Lilly and Company with stock options. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Ethical conduct of research
This study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki. The research is based on analysis of previously published and/or de-identified secondary data and does not involve direct interaction with human participants. As such, no additional ethical approval or informed consent was required.
Data sharing statement
The authors certify that this manuscript reports original clinical trial data. The data will not be made publicly available.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary material.docx)
- Download
- 1.12 MB
References
Papers of special note have been highlighted as: • of interest
1.
Tenhunen O, Lasch F, Schiel A, Turpeinen M. Single-arm clinical trials as pivotal evidence for cancer drug approval: a retrospective cohort study of centralized European marketing authorizations between 2010 and 2019. Clin. Pharmacol. Ther. 108(3), 653–660 (2020).
2.
Signorovitch JE, Wu EQ, Yu AP et al. Comparative effectiveness without head-to-head trials: a method for matching-adjusted indirect comparisons applied to psoriasis treatment with adalimumab or etanercept. Pharmacoeconomics 28(10), 935–945 (2010).
• Introduces matching-adjusted indirect comparison (MAIC) methods to estimate comparative treatment effects in the absence of head-to-head trials, illustrated using psoriasis treatments adalimumab and etanercept.
3.
Ren S, Ren S, Welton NJ, Strong M. Quantitative bias analysis for unmeasured confounding in unanchored population-adjusted indirect comparisons. Res. Synth. Meth. 16(3), 509–527 (2025).
• Presents a quantitative bias analysis method to assess and adjust for unmeasured confounding in unanchored population-adjusted indirect comparisons in evidence synthesis.
4.
Rolfo C, Hess LM, Jen MH et al. External control cohorts for the single-arm LIBRETTO-001 trial of selpercatinib in RET+ non-small-cell lung cancer. ESMO Open 7(4), 100551 (2022).
• Outlines the approach to create pseudo-compartors using matching approaches applied to historical trials and/or real-world evidence.
5.
Ferrara R, Auger N, Auclin E, Besse B. Clinical and translational implications of RET rearrangements in non–small cell lung cancer. J. Thorac. Oncol. 13(1), 27–45 (2018).
6.
Cong X-F, Yang L, Chen C, Liu Z. KIF5B-RET fusion gene and its correlation with clinicopathological and prognostic features in lung cancer: a meta-analysis. Onco. Targets Ther. 12, 4533–4542 (2019).
7.
Sireci A, Hess LM, Han Y et al. Clinical outcomes between patients with and without RET fusions in advanced/metastatic non-small cell lung cancer in the United States. J. Clin. Oncol. 38(Suppl. 15), e21693 (2020).
8.
Clinicaltrial.gov. A study of LOXO-292 in participants with advanced solid tumors, RET fusion-positive solid tumors, and medullary thyroid cancer (LIBRETTO-001). (2022). https://clinicaltrials.gov/ct2/show/NCT03157128
9.
Zhou C, Solomon B, Loong HH et al. First-line selpercatinib or chemotherapy and pembrolizumab in RET fusion positive NSCLC. N. Engl. J. Med. 389(20), 1839–1850 (2023).
• This Phase III randomized trial shows that first-line selpercatinib significantly improves progression-free survival (PFS) compared with pembrolizumab plus platinum-based chemotherapy in patients with RET fusion–positive non-small-cell lung cancer.
10.
Clinicaltrial.gov. A study of selpercatinib (LY3527723) in participants with advanced or metastatic RET fusion-positive non-small cell lung cancer (LIBRETTO-431). (2023). https://www.clinicaltrials.gov/study/NCT04194944
11.
Gandhi L, Rodríguez-Abreu D, Gadgeel S et al. Pembrolizumab plus chemotherapy in metastatic non-small-cell lung cancer. N. Engl. J. Med. 378(22), 2078–2092 (2018).
• This Phase III trial demonstrates that adding pembrolizumab to platinum-based chemotherapy significantly improves overall survival and PFS compared with chemotherapy alone in patients with metastatic non-small-cell lung cancer.
12.
Clinicaltrial.gov. A study of chemotherapy and ramucirumab versus chemotherapy alone in second line non-small cell lung cancer (NSCLC) participants who received prior first line platinum-based chemotherapy. (2013). https://clinicaltrials.gov/study/NCT01168973
13.
Page MJ, McKenzie JE, Bossuyt PM et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 372, n71 (2021).
14.
Cai W, van der Laan MJ. One-step targeted maximum likelihood estimation for time-to-event outcomes. Biometrics 76(3), 722–733 (2019).
15.
Briggs A, Sculpher M, Claxton K. Decision Modelling for Health Economic Evaluation. Oxford University Press, UK (2006).
16.
Burnham KP, Anderson DR. Multimodel inference: understanding AIC and BIC in model selection. Social. Meth. Res. 33(2), 261–304 (2004).
17.
NICER. Guide to the methods of technology appraisal 2013. (2013). https://www.nice.org.uk/process/pmg9
18.
Grambsch PM, Therneau TM. Proportional hazards tests and diagnostics based on weighted residuals. Biometrika 81(3), 515–526 (1994).
19.
WebPlotDigitizer. https://automeris.io/WebPlotDigitizer
20.
Guyot P, Ades AE, Ouwens MJ, Welton NJ. Enhanced secondary analysis of survival data: reconstructing the data from published Kaplan-Meier survival curves. BMC Med. Res. Methodol. 12, 9 (2012).
21.
Woods BS, Hawkins N, Scott DA. Network meta-analysis on the log-hazard scale, combining count and hazard ratio statistics accounting for multi-arm trials: a tutorial. BMC Med. Res. Methodol. 10, 54 (2010).
22.
Dias S, Sutton AJ, Welton NJ, Ades AE. NICE DSU Technical Support Document 3: Heterogeneity: Subgroups, Meta-Regression, Bias And Bias-Adjustment. National Institute for Health and Care Excellence, UK (2012).
23.
Turner RM, Jackson D, Wei Y, Thompson SG, Higgins JP. Predictive distributions for between-study heterogeneity and simple methods for their application in Bayesian meta-analysis. Stat. Med. 34(6), 984–998 (2015).
24.
Higgins JPT, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ 327(7414), 557–560 (2003).
25.
Plummer M. (Ed.). JAGS: a program for analysis of Bayesian graphical models using Gibbs sampling. Proceedings of the 3rd International Workshop on Distributed Statistical Computing. Vienna, Austria (2003).
26.
Ades AE, Mavranezouli I, Dias S et al. Network meta-analysis with competing risk outcomes. Value Health 13(8), 976–983 (2010).
27.
Dias S, Welton NJ, Sutton AJ et al. NICE DSU Technical Support Document 4: Inconsistency in networks of evidence based on randomised controlled trials. National Institute for Health and Care Excellence, UK (2011).
28.
Sekhon JS. Multivariate and propensity score matching software with automated balance optimization: the matching package for R. J. Stat. Soft. 42(7), 1–52 (2011).
29.
Michels S, Scheel AH, Scheffler M et al. Clinicopathological characteristics of RET rearranged lung cancer in European patients. J. Thorac. Oncol. 11(1), 122–127 (2016).
30.
Kohno T, Ichikawa H, Totoki Y et al. KIF5B-RET fusions in lung adenocarcinoma. Nat. Med. 18(3), 375–377 (2012).
31.
Song Z, Yu X, Zhang Y. Clinicopathologic characteristics, genetic variability and therapeutic options of RET rearrangements patients in lung adenocarcinoma. Lung Cancer 101, 16–21 (2016).
32.
Dugay F, Llamas-Gutierrez F, Gournay M et al. Clinicopathological characteristics of ROS1-and RET-rearranged NSCLC in caucasian patients: data from a cohort of 713 non-squamous NSCLC lacking KRAS/EGFR/HER2/BRAF/PIK3CA/ALK alterations. Oncotarget 8(32), 53336 (2017).
33.
Dudnik E, Bshara E, Grubstein A et al. Rare targetable drivers (RTDs) in non-small cell lung cancer (NSCLC): outcomes with immune check-point inhibitors (ICPi). Lung Cancer 124, 117–124 (2018).
34.
Mazieres J, Drilon A, Lusque A et al. Immune checkpoint inhibitors for patients with advanced lung cancer and oncogenic driver alterations: results from the IMMUNOTARGET registry. Ann. Oncol. 30(8), 1321–1328 (2019).
35.
Pan Y, Zhang Y, Li Y et al. ALK, ROS1 and RET fusions in 1139 lung adenocarcinomas: a comprehensive study of common and fusion pattern-specific clinicopathologic, histologic and cytologic features. Lung Cancer 84(2), 121–126 (2014).
36.
Guisier F, Dubos-Arvis C, Viñas F et al. Efficacy and safety of anti–PD-1 immunotherapy in patients with advanced NSCLC with BRAF, HER2, or MET mutations or RET translocation: GFPC 01-2018. J. Thorac. Oncol. 15(4), 628–636 (2020).
Information & Authors
Information
Published In
Copyright
© 2026 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 7 January 2026
Accepted: 7 April 2026
Published online: 29 April 2026
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Efficacy of selpercatinib as a first-line treatment for RET-fusion positive non-small-cell lung cancer: a novel two-stage Bayesian network meta-analysis. (2026) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2026-0006
Export citation
Select the citation format you wish to export for this article or chapter.