Blood neurofilament light chain as a predictive biomarker for functional outcome of acute ischemic stroke: a systematic review and meta-analysis
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Ischemic stroke continues to be a significant contributor to mortality and disability on a global scale. The blood neurofilament light chain (bNfL) as a prognostic indicator for stroke functional outcomes is a topic of ongoing debate. Thus, the objective of this systematic review is to assess the efficacy of bNfL as a predictor of stroke functional outcomes. Materials & methods: A systematic search was conducted in Pubmed, Cochrane and Embase databases from their inception to 21 October 2023. Two reviewers independently screened the search results to identify studies reporting on the association between bNfL and acute ischemic stroke outcomes. The quality of the studies was assessed using the Newcastle–Ottawa scale. Meta-analysis was conducted using the Comprehensive Meta-Analysis software Stata 12.0, utilizing a random effects model to estimate the pooled effect. Results: Nine studies involving 2302 patients were included in the analysis. A pooled analysis of adjusted odds ratios (ORs) from multivariate regression models in the meta-analysis revealed a pooled adjusted OR of 1.929 [95% CI:1.459, 2.550], suggesting that the patients with higher bNfL levels are at a greater risk of experiencing unfavorable functional outcomes compared with those with lower bNfL levels. Subgroup analysis indicated that factors such as sampling time, study region, participant age, blood specimen and sample size, may contributed to high heterogeneity in the results. After conducting a thorough analysis using funnel plot and Egger’s test, no significant evidence of publication bias was found in our study. Conclusion: In summary, bNfL demonstrates potential as a predictive biomarker for functional outcomes in acute ischemic stroke patients, albeit subject to influence from confounding variables. Additional rigorously designed and meticulously executed prospective studies on a larger scale are warranted to validate these findings.
Plain language summary
What is this article about?
Ischemic stroke, also known as ‘stroke’, is a condition with a high incidence and disability rate. Rapid and correct diagnosis is critical for the proper treatment of patients with stroke. Despite the use of many prognostic scales and methodologies, reliably predicting stroke outcomes remains a challenge. In this case, biomarkers have the potential to provide more efficient tailored strategies for prioritizing therapeutic interventions and predicting short- and long-term outcomes. The neurofilament light chain (NfL) is a neurofilament subunit that can be used as a biomarker for neurological illnesses with tissue damage. It is regarded as a direct indicator of the severity of the disease. However, the use of blood neurofilament light chain (bNfL) as a predictive indicator for stroke functional outcomes is still being debated. Thus, the goal of this study is to determine the effectiveness of bNfL as a predictor of stroke functional outcomes.
What were the results?
The analysis includes nine studies with a total of 2302 subjects. The findings revealed that patients with higher bNfL levels are more likely to experience poor functional outcomes than those with lower bNfL levels. Subgroup analysis revealed that a number of variables, including sample size, blood specimen, participant age, study region, and sampling time, may have contributed to the results’ high heterogeneity.
What do the results of the study mean?
Although it is susceptible to the influence of confounding variables, bNfL shows promise as a predictive biomarker for functional outcomes in patients who have suffered an acute ischemic stroke. It might aid medical professionals in determining a stroke patient’s prognosis.
Ischemic stroke continues to be a significant contributor to mortality and disability on a global scale [1]. Despite advancements in early detection and management strategies, such as intravenous thrombolysis therapy and mechanical thrombectomy (MT), approximate 5.5 million deaths are still reported annually [2]. Specifically, MT has shown promising results in improving the prognosis of acute ischemic stroke (AIS), particularly in cases of large vessel occlusion [3]. However, only 37% of patients treated with this intervention achieve functional independence [4]. Moreover, the accessibility of advanced healthcare technology for AIS patients is limited, particularly in low-income countries and rural areas, thereby complicating the diagnosis and treatment of stroke. Enhancing the prognosis of stroke is crucial; however, despite the utilization of various prognostic scales and approaches, accurately predicting AIS outcomes remains challenging [5].
In this instance, biomarkers have the potential to offer a more streamlined personalized strategy for enhancing treatment modalities for patients and forecasting both short- and long-term prognoses. This facilitates the prioritization of treatment interventions and determination of the extent of post-treatment unit care [6]. Neurofilament, a biomarker indicative of neuronal loss, has garnered increasing attention as a promising prognostic indicator in recent years [7]. Neurofilament light chain (NfL) is a subunit of neurofilament that may serve as biomarker for neurological conditions characterized by tissue damage, such as stroke. Abnormal levels of blood neurofilament light chain (bNfL) are indicative of such conditions, and the concentration of bNfL is also recognized as a direct indicator of disease severity [2].
Prior research has yielded varying results regarding the predictive capabilities of bNfL on stroke functional outcomes. Ferrari et al. indicated that NfL-D7 was significant predictor of 3-month scores of National Institutes of Health Stroke Scale (NIHSS) [8], while additional studies from the DAMDAS and CIRCULAR investigations demonstrated that NfL levels could forecast recurrent ischemic stroke and functional outcomes at the 3-month mark [9]. Comparable findings were noted in studies conducted in Germany and Denmark [10]. Conversely, Onatsu et al. posited that serum Neurofilament light chain (sNfL) exhibited a correlation with infarct volume but not with prognosis in cases of AIS [11]. Furthermore, previous meta-analyses lacked sufficient statistical power to draw definitive conclusions [12]. Additionally, recent studies with adequate sample sizes and novel evidence have since been published [13–16]. Consequently, we conducted a meta-analysis utilizing the recent and compelling evidence to evaluate the predictive value of bNfL in determining functional outcomes in AIS patients.
Materials & methods
Data sources & search strategy
A systematic search was conducted on the Pubmed, Cochrane Library, and Embase databases from their inception to 21 October 2023, utilizing a combination of keywords, medical subject headings (MeSH) terms, and free words. The search strategy included variations of terms such as ‘ischemic stroke’, ‘ischemia stroke’, ‘cerebral infarction’, ‘brain infarction’, as well as ‘neurofilament light chain’ or ‘NfL’. Furthermore, reference lists of included studies were manually reviewed to identify any additional relevant studies. The search strategy is listed in Supplementary Table 1.
Inclusion & exclusion criteria
The study’s inclusion criteria consisted of the inclusion of patients diagnosed with AIS, including transient ischemic attack (TIA); the provision of risk ratios (RRs) or odds ratios (ORs) along with their corresponding 95% CIs to demonstrate the association between AIS and bNfL. Excluded from consideration were reviews, case reports, letters, conference abstracts, clinical short communications, brief reports and nonhuman animal model research.
Study selection
Two independent reviewers (H-Y Xu and H-Y Lin) conducted a screening of titles and abstracts based on predetermined inclusion criteria. Studies that potentially met criteria underwent a full-text review for further evaluation. Any discrepancies in the inclusion or exclusion of studies during screening were resolved through discussion until a consensus was reached, with final discrepancies being resolved by Li Chen.
Data extraction
Two independent reviewers (H-Y Xu and H-Y Lin) extracted the following information from each study: first author, publication year, region, study design, sample size, median age, follow-up duration, sampling time, method used to detect baseline neurofilament light (bNfL), type of blood specimen, NfL levels, stroke-ascertainment criteria, etiological subtypes, recurrent ischemic events, mortality, definition and timing of outcome (all studies assessed the Modified Rankin Scale [mRS] at 90 days or later after symptom onset), correlation coefficients, and adjusted covariates. This information was then compiled into a predesigned table.
Quality assessment
The quality assessment of the included studies was conducted utilizing the Newcastle–Ottawa Scale (NOS) [17], which comprises three components (selection, comparability and outcome). The NOS scores range from 0 to 9, with the risk of bias categorized into three levels: high (0–3), moderate (4–6) and low (7–9). A higher score indicates high quality. The assessment process was independently carried out by two authors (R-X Qin and L-D Shao).
Data analysis
The meta-analysis was conducted using the Comprehensive Meta-Analysis software, Stata 12.0. Effect sizes were computed by importing the adjusted OR from multivariate logistic regression in the original study, which were then used to calculate a pooled adjusted OR representing the predictive effect of bNfL on functional outcome in AIS. Fixed-effects models were utilized when I2 was less than 50.0%, while random-effects models were employed in cases of higher heterogeneity (I2 > 50.0%). Heterogeneity was assessed using the Q test and the I2 statistic, which ranges from 0 to 100% and indicates the degree of heterogeneity across studies. An I2 value greater than 50% signifies substantial heterogeneity. Subgroup analysis was conducted to evaluate the consistency based on clinical characteristics, sample size and study design. Publication bias was evaluated through funnel plots in conjunction with Eggers’ test and Begg’s test. Two-tailed statistical tests were employed with a significance level set at p < 0.05. Sensitivity analysis was utilized to assess the reliability of the findings.
Results
Database search
Our initial search of electronic and manual databases yielded 690 records, of which 114 were duplicates. Following a review of titles and abstracts, 542 records were excluded, leaving 34 studies for full-text evaluation. Of these, 25 studies were excluded for various reasons, including being conference abstracts, comments, reviews, clinical short communication, brief report, lacking reported effect sizes or having uninteresting outcomes. Ultimately, nine studies involving 2302 participants were deemed for inclusion in the quantitative synthesis (meta-analysis) [9,10,13–16,18–20]. The flow chart for this study screening and selection is shown in Figure 1.
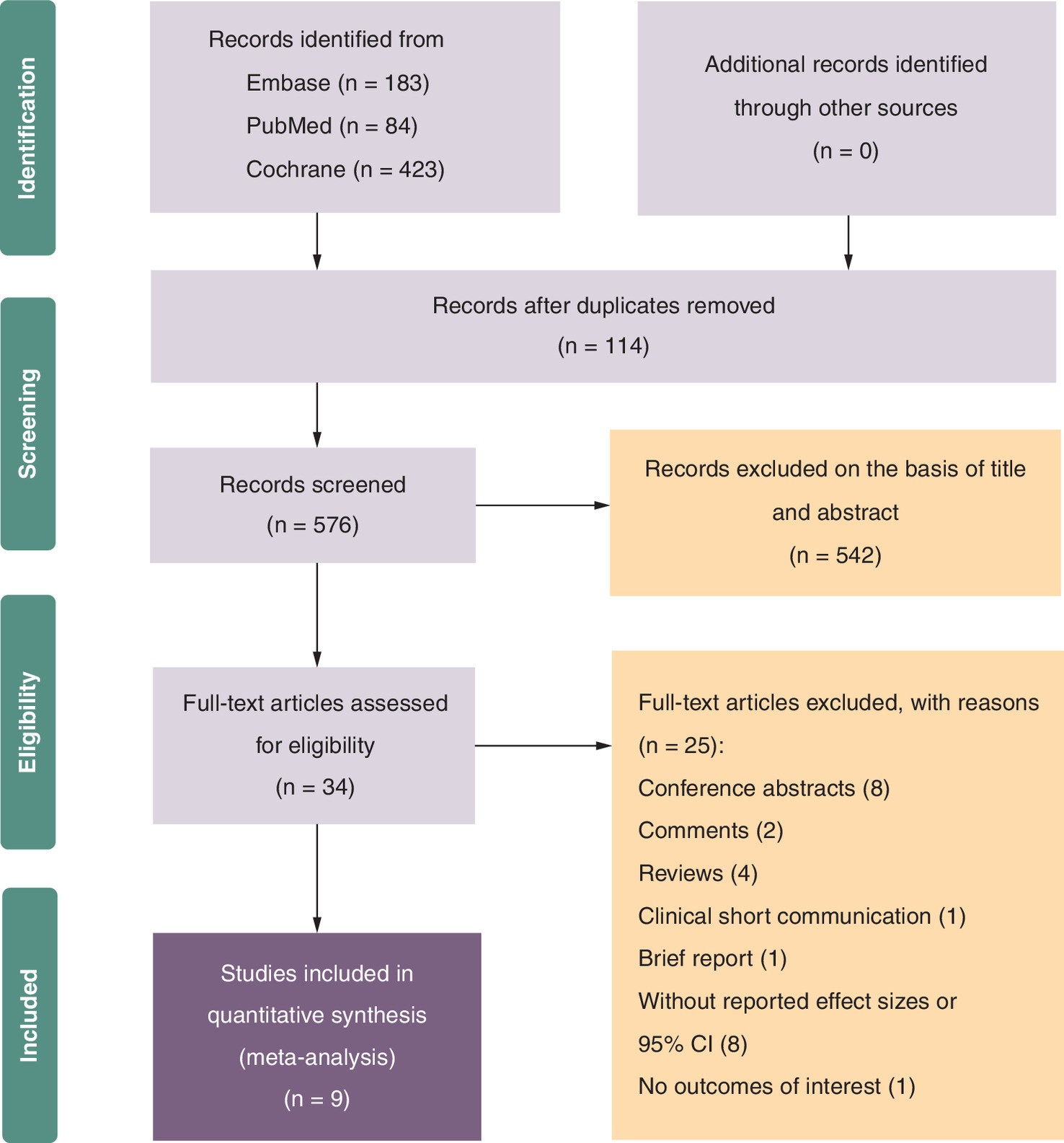
Figure 1. Flow chart for study screening and selection.
CI: Confidence interval.
Study characteristics of included studies
Table 1 displays the primary characteristics of the 9 studies incorporated in this systematic review and meta-analysis, encompassing publication dates spanning from 2015 to 2023. With the exception of three studies, all were prospective cohort studies. The sample sizes of the included studies varied from 41 to 615 participants. Of the nine studies, six originated from Europe and America, while three were from Asia. Furthermore, three studies reported recurrent ischemic events, four reported mortality rates, and three described infarct volumes. All included studies examined the association between bNfL levels and unfavorable functional outcomes in stroke patients. The NOS for all studies included in the analysis varied between 7 and 9. Upon thorough examination of the included studies, we identified some qualitative heterogeneity.
| Study | Year | Region | Study design | Sample size | Median age (y) | Follow-up time (m) | Sampling time (IQR) | Detection method of sNfL | Blood specimen | NfL Levels median (IQR) | Stroke ascertainment | Etiological subtypes, n (%) | Unfavorable functional outcome: adjusted OR (95% CI) | Definition of outcome | NOS score |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Traenka et al. | 2015 | Switzerl and Germany | Observational study | AIS: 31 TIA:10 | 42 (36.5–48.5) | 3 | 6 (3–9.5) days | Electrochemiluminescence immunoassay | Serum | AIS:108.9 (37.8–427.7) pg/ml TIA: 16.4 (8.7–36.3) pg/ml | MRI | n/a | 2.56 (0.81–8.13) | 3 months mRS | 7 |
| De Marchis et al. | 2018 | Switzerland | Prospective cohort study | AIS: 504 TIA: 111 | 68 (59–77) | 3 | 160 (91–275) min | Electrochemiluminescence immunoassay | Serum | AIS:16 (7–34) pg/ml TIA:9 (4–19) pg/ml | MR-DWI | Large-vessel disease 82 (16) Cardioembolic 186 (37) Small-artery disease 31 (6) Multiple causes 45 (9) Other known 25 (5) Undetermined 135 (27) | 1.05 (0.74–1.49) | 3 months mRS | 9 |
| Tiedt et al. | 2018 | Germany | Prospective cohort study | 196 (CIRCULAS) 95 (DEMDAS) | Median (IQR) CIRCULAS 74.9 (16.9) DEMDAS 65.0 (19.0) | 6 | 7 days | Single-molecule array | Serum | D7: 211.2 (104.7–442.6) pg/ml | diffusion-weighted MRI or delayed CT scan | Etiology of IS, n (%) (CIRCULAS) (n = 196) (DEMDAS) (n = 95) Large artery atherosclerosis 42 (21.4) 22 (23.2) Cardioembolism 62 (31.6) 21 (22.1) Small vessel occlusion 16 (8.2) 16 (16.8) Arterial dissection 5 (2.6) 3 (3.2) Undetermined 71 (36.2) 33 (34.7) | 2.35 (1.60–3.45) | 6 momths RIL 3 months mRS | 8 |
| Pedersen et al. | 2019 | Sweden | Prospective cohort study | 595 | 59 (52–65) | 3 m–7 y | 4 (3–6) days | Ultrasensitive single-molecule array | Serum | 60.2 (28.3–190.4) pg/ml 3 months 90.6 (41.8–230.3) pg/ml 7 years 18.1 (11.5–35.5) pg/ml | CT/MRI | Large-artery atherosclerosis 47(20.7) small-vessel occlusion 15(6.6) cardioembolism 87(38.3) stroke of undetermined etiology 70(30.8) stroke of other determined etiology 8(3.5) | 2.15 (1.09–4.24) | 3 months mRS 2 years mRS 7 years mRS | 8 |
| Uphaus et al. | 2019 | Germany | Prospective observational study | 211 | 68.7 (SD, ± 12.6) | 3, 12, 36 m | Within 24 h after admission | Single-molecule array | Serum | NfL (24 h) pg/ml mRs <2: 19 (12.7–24.7) mRs > = 2: 36.2 (18.7–58.5) | CT/MRI | Large-artery atherosclerosis 32(15.2) Cardioembolism 30(14.2) Small vessel occlusion 69(32.7) Other cause 5(2.4) Undetermined 75(35.5) | 1.562 (1.003–2.433) | 3 months mRS | 8 |
| Gendron et al. | 2020 | America | Prospective cohort study | 227 | 69.6 (18.8, 100.7) | 3 | D0–D8, D9–D20 | NF-light digital immunoassay | Plasma | Median (minimum, maximum) 68.9 (5.0, 13677.9) pg/ml | n/a | Large-artery atherosclerosis 47(20.7) small-vessel occlusion 15(6.6) cardioembolism 87(38.3) stroke of undetermined etiology 70(30.8) stroke of other determined etiology 8(3.5) | 2.30 (1.73, 3.21) | 3 months mRS | 8 |
| Chen et al. | 2021 | China | Prospective study | 60 | 71.2 ± 11.8 | 3 | 5.13 ± 4.47 h for T1 5.54 ± 4.66 h for T2 27.21 ± 6.23 h for T3 | Ultrasensitive single molecule array | Plasma | 33.3 (19.6, 88.9) pg/ml | CT perfusion or MRI | Cardioembolism 43 (71.7) Large-artery atherosclerosis 10 (16.7) Others 7 (11.7) | 2.22 (1.27–3.88) | 3 months mRS | 9 |
| Zhou et al. | 2022 | China | Prospective study | 110 | Median (IQR) (y) 66.00 (18.25) | 6 | At admission | Simoa | Serum | median (IQR) (pg/ml) 3.39 (1.76) | CT/MRI | n/a | 1.549 (0.973–2.465) | 6 months mRS | 7 |
| Li et al. | 2023 | China | Prospective observational study | 152 | 67.7 ± 11.1 | 3 | At admission | Simoa | Serum | 63.1 (51.2–83.4]) pg/ml | MRI | Large-artery atherosclerosis 49 (32.2) Cardio-embolism 16(10.5) Small vessel occlusion 70 (46.0) Other determined etiology 2(1.3) Undetermined etiology 15 (9.9) | 12.4 (2.7, 56.3) | END 3 months mRS | 8 |
AIS: Acute ischemic stroke; CI: Confidence interval; CT: Computed tomography; END: Early neurological deterioration; m: Months; mRS: Modified Rankin Scale; n/a: Not available; OR: Odds ratio; RIL: Recurrent ischemic lesion; TIA: Transient ischemic stroke; y: Years.
The studies by Traenka et al. [18] and De Marchis et al. [19] included TIA patients in addition to AIS patients, with the analysis of stroke functional outcomes also encompassing TIA patients. The average age of the participants in these studies exceeded 60 years old, a contrast to the studies by Traenka et al. [18] and Pedersen et al. [20]. Six studies utilized the single-molecule array method for detecting bNfL levels, a novel approach for measuring NfL levels [21]. However, the other two studies utilized the electrochemiluminescence immunoassay method for detecting the NfL levels [18,19]. Gendron et al. utilized the NF-Light digital immunoassay for this purpose [13]. Furthermore, the duration of blood sampling varied across the studies included in the analysis, with Traenka et al. collecting samples over a period of 6 (3–9.5) days, Tiedt et al. at 7 days, and Pedersen et al. at 4(3–6) days [9,18,20]. The study conducted by Gendron et al. [13] collected blood samples within two-time frames: 0–8 days and 9–20 days. Among the five studies included, blood samples were obtained within a maximum of 1 day, with De Marchis et al. [19] collecting blood at 160 (91–275) min, Uphaus et al. [10] within 24 h after admission, and Zhou et al. and Li et al. at admission [15,16]. Chen et al. [14] collected blood samples at 5.13 ± 4.47 h, 5.54 ± 4.66 h, and 27.21 ± 6.23 h. Additionally, it was noted that two studies used plasma specimens while the others used serum. All studies utilized CT or MRI to confirm stroke diagnosis, except for one study that did not provide details on stroke ascertainment [13]. Regarding the etiological subtypes of stroke, the majority of studies did not classify subtypes except for two [15,18]. Cardioembolism was found to be the most prevalent etiological subtype in three studies [13,14,19], with patients typically being younger compared with other subtypes. In the studies conducted by Tiedt et al. [9] and Uphaus et al. [10], undetermined etiology was the most common etiological subtype. However, Li et al. [16] showed that small vessel occlusion accounted for the highest proportion of the etiological subtypes.
The mRS was the predominant measure utilized to assess functional outcomes in the studies analyzed, with all NfL levels from blood samples included in the stroke outcome analysis. Furthermore, Tiedt et al. [9] defined recurrent ischemic lesions (RIL) at 6 months as an additional prognostic indicator. Li et al. [16] incorporated early neurological deterioration (END) as a functional outcome indicator in their study. Due to variations in statistical methodologies and prognostic indicators, the mRS was designated as the functional prognostic index for the meta-analysis, which aimed to quantitatively assess the predictive value of bNfL in determining functional outcomes in AIS. A mRS score of 0–2 indicates functional independence (good outcome). mRS 3–6 indicates at least moderate disability or death (poor functional outcome). A total of nine studies were included in the analysis, with some studies also examining infarct volume, recurrent ischemic events, and mortality as outcome measures. Among the included studies, three specifically analyzed infarct volume as a potential indicator of functional outcome. De Marchis et al. [19] utilized a semi-quantitative method to estimate infarct size in their study. Their findings indicated that there was no significant association between infarct size on admission MRI-DWI and sNfL levels, both in univariate analysis (p = 0.15) and after adjusting for age and NIHSS on admission (p = 0.56). In contrast, Tiedt et al. [9] employed software tools to measure infarct size and observed a positive correlation between infarct volumes and NfL levels on D7 (partial correlation coefficient r = 0.736, p = 1.5 × 10–15) and D3 (r = 0.370, p = 0.0003), although this relationship was not evident at earlier time points. Chen et al. [14] reported a final infarct volume of 13.9 (3.8–61.4) ml without detailing the method of measurement. Additionally, they observed no significant correlation between sNfL levels and infarct volume at different time points (T1, p = 0.92; T2, p = 0.99; T3, p = 0.1). Three studies included in the analysis investigated the predictive value of sNfL as a biomarker for recurrent ischemic events [9,10,18]. Traenka et al. [18] identified two stroke patients who experienced recurrent ischemic strokes at 5 and 45 days post-blood sampling, with corresponding sNfL levels of 124.0 and 427.7 pg/ml, respectively. Nineteen patients (20%) experienced RILs in the study conducted by Tiedt et al. [9]. The researchers determined that the presence of RILs served as an independent predictor of sNfL levels at 6 months post-stroke, even after adjusting for variables such as age, sex, hypertension, and infarct volume at baseline (p = 0.014). In a separate study by Uphaus et al. [10], 56 patients experienced recurrent stroke or death. Furthermore, the researchers found that sNfL levels were a valuable predictor of recurrent stroke or death (OR: 2.002; 95% CI: 1.213–3.302; p = 0.007), in addition to NIHSS, diabetes mellitus and age-related white matter change rating, as determined through multivariate regression analysis. Four of the studies included in the analysis reported mortality rates [13,14,16,20]. The detailed baseline characteristics of the studies included in the analysis are outlined in Table 1.
Risk of bias in included studies
As all of the studies incorporated in the analysis were non-randomized controlled trials, the NOS scores were utilized for evaluation. In terms of selection criteria, five studies received four stars, while four studies received three stars. Regarding comparability, eight studies were awarded two stars, with one study receiving one star. For outcome assessment, five studies were assigned three stars, while four studies were allocated two stars. Overall, the included studies were deemed to be of high quality, as evidenced by the detailed assessment provided in Table 2.
| Study | Year | Selection | Comparability | Outcome | Overall | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Representativeness | Selection of nonexposed | Ascertainment of exposure | Outcome not present at start | Comparability on most important factors | Comparability on other risk factors | Assement of outcome | Long enough follow-up (median ≥ 3 month) | Adequacy (completeness) of follow-up | |||
| Traenka et al. | 2015 | * | - | * | * | * | _ | * | * | * | 7 |
| De Marchis et al. | 2018 | * | * | * | * | * | * | * | * | * | 9 |
| Tiedt et al. | 2018 | * | * | * | * | * | * | * | * | - | 8 |
| Pedersen et al. | 2019 | * | * | * | * | * | * | * | * | - | 8 |
| Uphaus et al. | 2019 | * | - | * | * | * | * | * | * | * | 8 |
| Gendron et al. | 2020 | * | * | * | * | * | * | * | * | - | 8 |
| Chen et al. | 2021 | * | * | * | * | * | * | * | * | * | 9 |
| Zhou et al. | 2022 | * | - | * | * | * | * | * | * | - | 7 |
| Li et al. | 2023 | * | - | * | * | * | * | * | * | * | 8 |
Single asterisk indicates 1 score and dash indicates 0 scores.
Meta-analysis
Nine studies involving 2302 patients explored the relationship between bNfL levels and unfavorable functional outcomes in AIS. All ORs were calculated, revealing a high level of statistical heterogeneity (I2 = 62.8%) among the studies. Consequently, a random effects model was chosen for the meta-analysis. The results, depicted in Figure 2, showed a pooled adjusted OR of 1.929 [95% CI: 1.459–2.550], indicating that patients with higher bNfL levels are at a greater risk of unfavorable functional outcome compared with those with lower levels. The assessment of publication bias in the funnel plot is presented in Figure 3, which does not indicate significant publication bias (p = 0.466, two-tailed). Similar results were obtained from Egger’s test got similar results (p = 0.229, two-tailed). Additionally, a sensitivity analysis was conducted, as shown in Figure 4, revealing that the findings are robust.
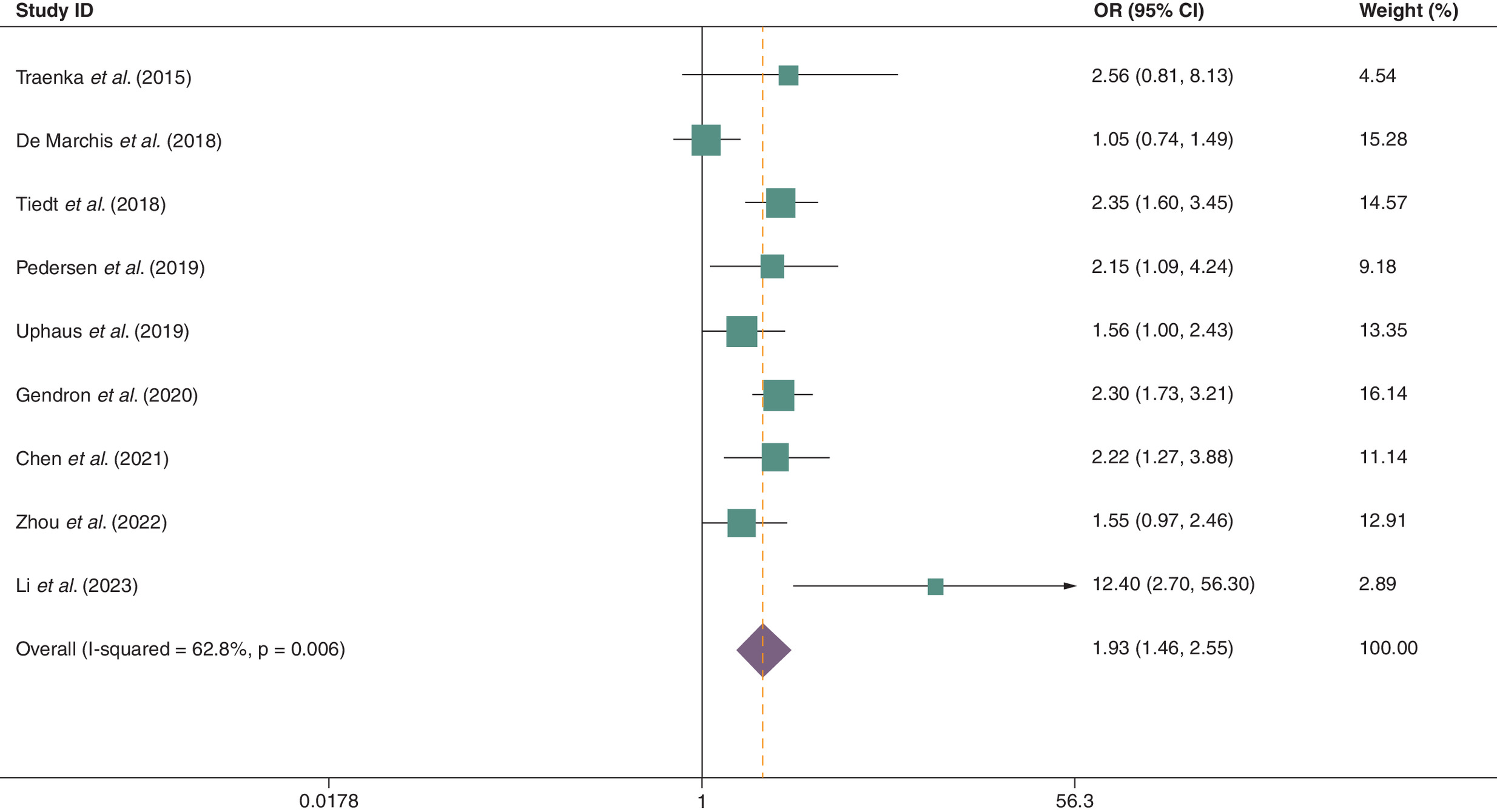
Figure 2. Forest plot of meta-analysis illustrating the association between blood neurofilament light chain levels and unfavorable functional outcome in ischemic stroke patients.
mRS 0–2 = functional independence (good outcome). mRS 3–6 = at least moderate disability or death (poor outcome).
CI: Confidence interval; OR: Odds ratio.
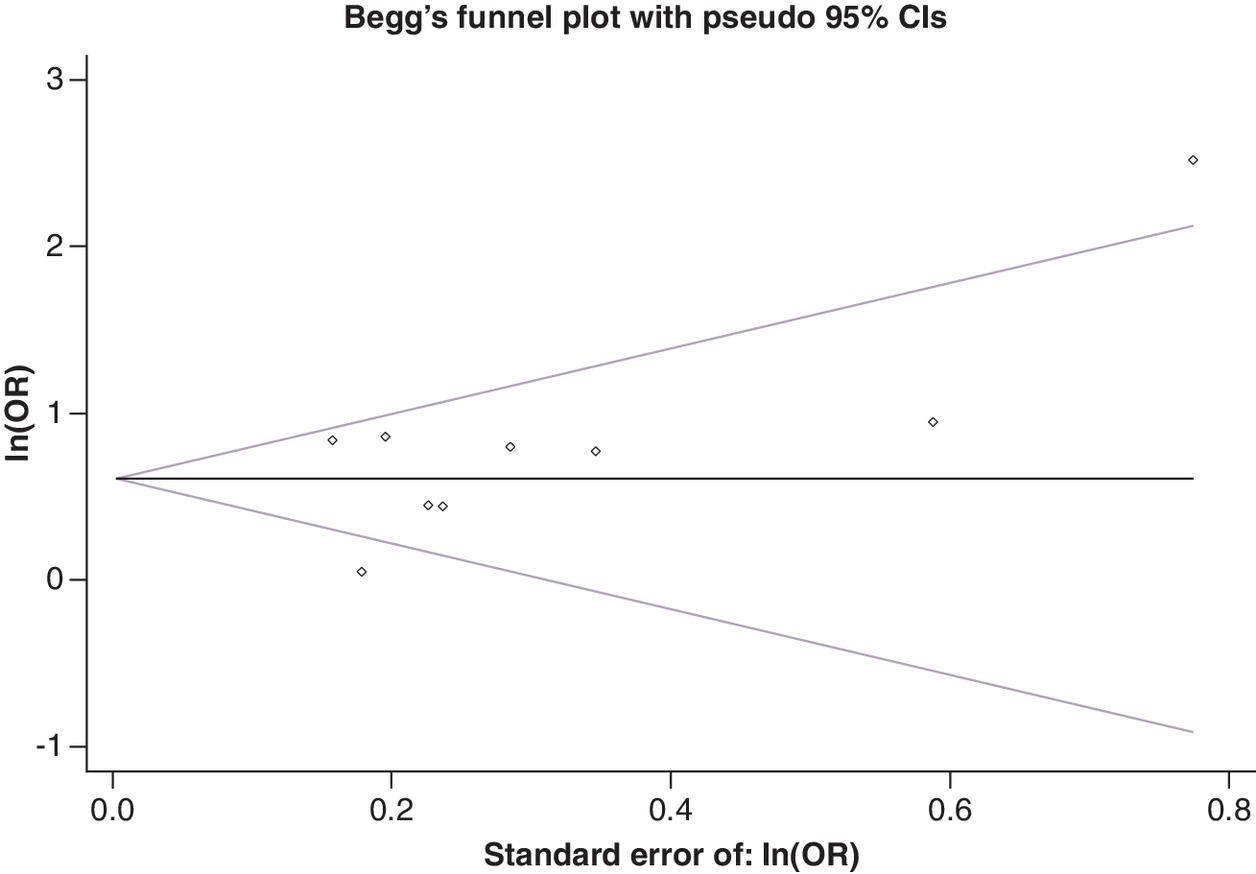
Figure 3. Funnel plot for assessment of publication bias.
CI: Confidence interval; OR: Odds ratio.
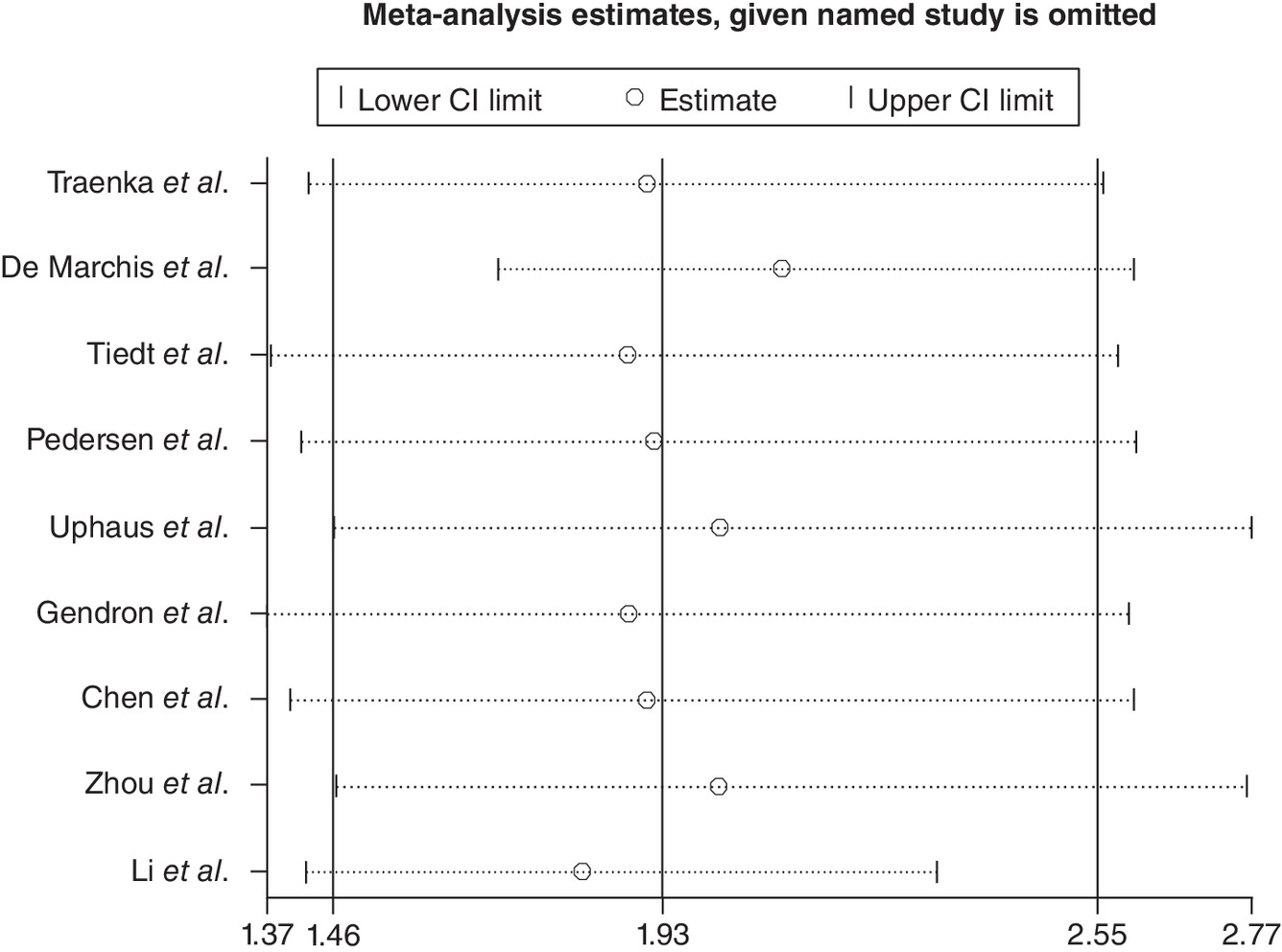
Figure 4. Sensitivity analysis for the robust assessment of the pooled effect.
CI: Confidence interval.
Subgroup of analysis
The presence of significant heterogeneity in the meta-analysis prompted an in-depth examination of its origins through an analysis of both clinical and methodological factors, such as sampling time, study region, participant age, blood specimen, sample testing method, inclusion of TIA and sample size, as detailed in Table 3. The findings revealed that nearly all subgroups exhibited potential sources of heterogeneity. The subgroup analysis revealed that studies with a sample size ≥200 (I2 = 71.3%) and participants aged ≥60 years (I2 = 71.3%) exhibited the highest heterogeneity, with I2 values of 71.3% and 71.3%, respectively. Conversely, subgroups characterized by participants aged <60 years, plasma sample collection, and sampling time of ≥4 days showed no heterogeneity (I2 = 0). Additionally, the association between bNfL levels and unfavorable outcomes remained consistent across all subgroups, except for sample testing methods and inclusion of TIA in the study design. The results of subgroup analyses are shown in Table 3 and the forest plot of subgroup analyses is depicted in Figure 5.
| Subgroup | Studies | OR (95% CI) | I2 (%) | p-value |
|---|---|---|---|---|
| Region | ||||
| Europe and America | 6 | 1.822(1.323,2.508) | 65.3 | 0.013 |
| Asia | 3 | 2.531 (1.192,5.371) | 70.8 | 0.033 |
| Age, years | ||||
| <60 | 2 | 2.249 (1.253,4.038) | 0 | 0.798 |
| ≥60 | 7 | 1.893(1.372,2.613) | 71.3 | 0.002 |
| Blood specimen | ||||
| Serum | 7 | 1.853(1.290,2.661) | 66.1 | 0.007 |
| Plasma | 2 | 1.929(1.459,2.550) | 0 | 0.913 |
| Method | ||||
| Electrochemiluminescence immunoassay | 2 | 1.374(0.616,3.065) | 52.4 | 0.147 |
| Single-molecule array | 6 | 2.050(1.522,2.761) | 42.9 | 0.119 |
| Time, days | ||||
| ≥4 | 3 | 2.319(1.682,3.197) | 0 | 0.961 |
| <4 | 5 | 1.727(1.121,2.661) | 70 | 0.01 |
| TIA | ||||
| Not Included TIA | 7 | 2.090(1.657,2.636) | 35.6 | 0.157 |
| Included TIA | 2 | 1.374(0.616,3.065) | 52.4 | 0.147 |
| Sample size, n | ||||
| <200 | 4 | 2.433(1.340,4.417) | 57.2 | 0.072 |
| ≥200 | 5 | 1.783(1.267, 2.509) | 71.5 | 0.007 |
Forest plot of subgroup analyses are presented on Supplementary Figure from 1A to 1G.
CI: Confidence interval; OR: Odds ratio; TIA: Transient ischemic attack.
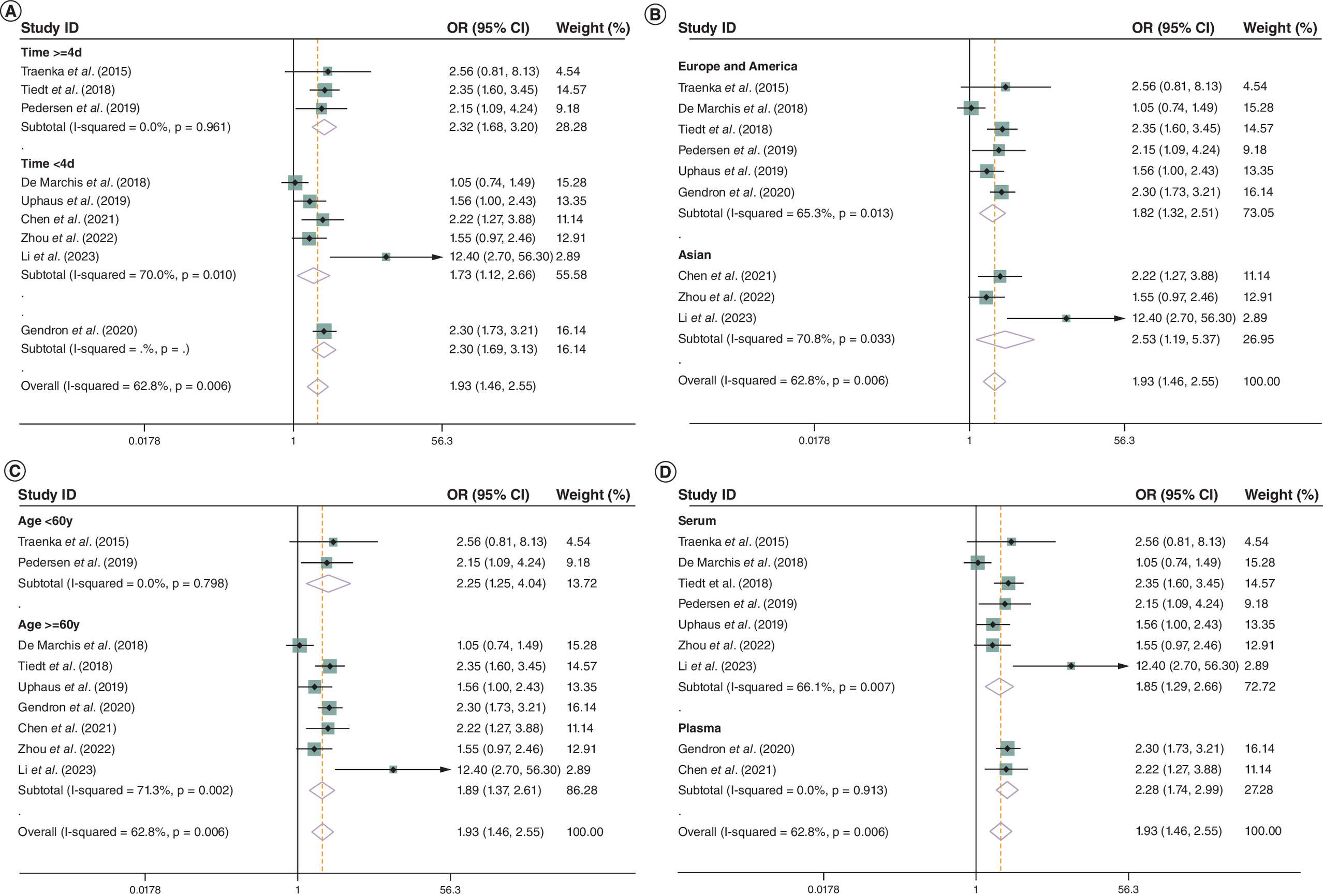
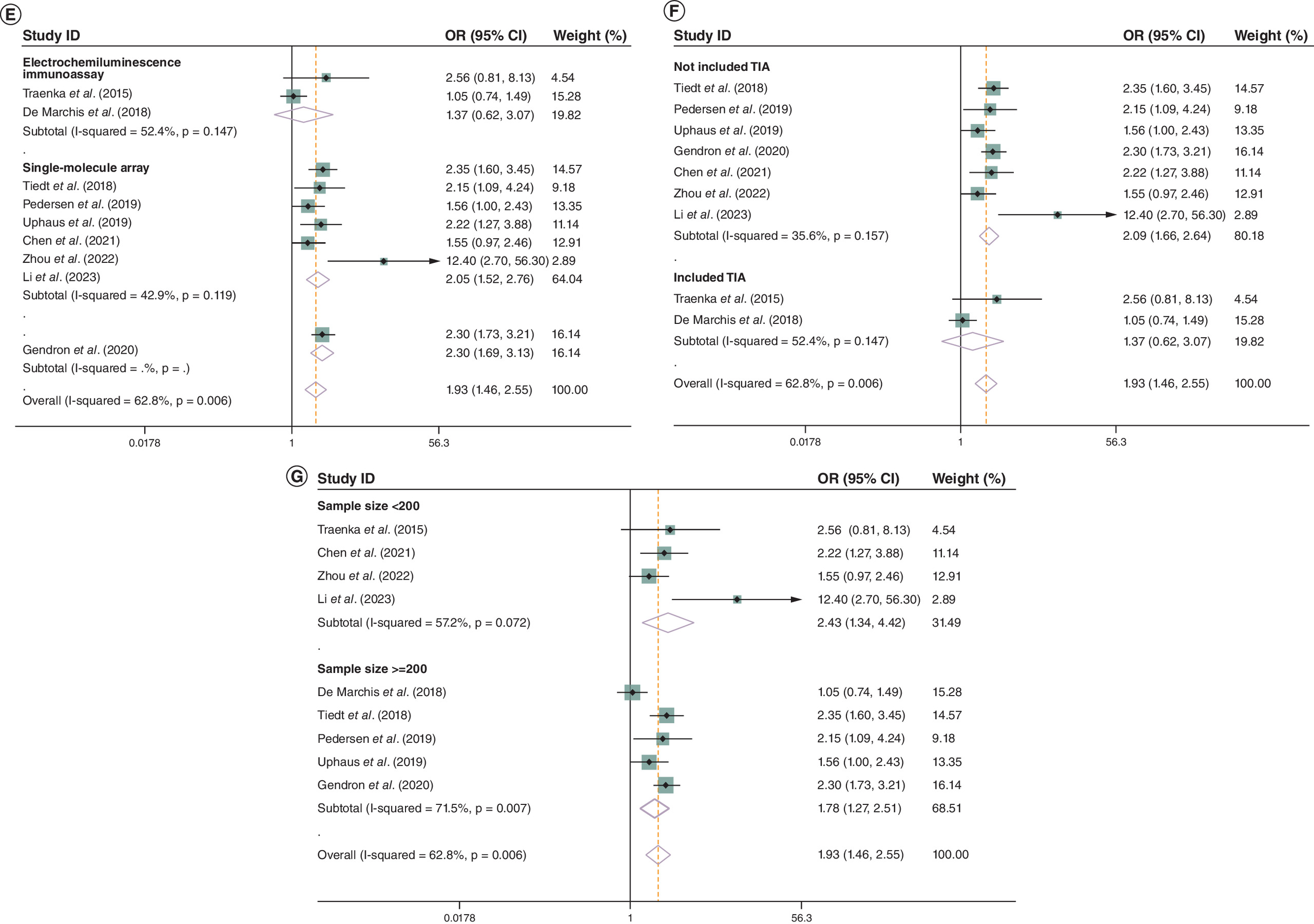
Figure 5. Forest plot of subgroup analyses.
(A) Subgroup analyses of bNfL and the risk of stroke functional outcomes stratified by the timing of blood sampling; (B) subgroup analyses of bNfL and the risk of stroke functional outcomes stratified by region; (C) subgroup analyses of bNfL and the risk of stroke functional outcomes stratified by participant age; (D) subgroup analyses of bNfL and the risk of stroke functional outcomes stratified by blood specimen; (E) subgroup analyses of bNfL and the risk of stroke functional outcomes stratified by sample testing method; (F) subgroup analyses of bNfL and the risk of stroke functional outcomes stratified by inclusion of TIA; (G) subgroup analyses of bNfL and the risk of stroke functional outcomes stratified by sample size.
bNFL: Blood neurofilament light chain; CI: Confidence interval; OR: Odds ratio; TIA: Transient ischemic attack.
Discussion
Main findings
Our meta-analysis comprehensively and systematically reviewed the current available literature and found that the patients with higher bNfL levels is associated with higher risk of unfavorable functional outcome compared that with lower bNfL levels. bNfL carries value as a functional prognostic biomarker for AIS.
Comparison with other meta-analyses
Two systematic reviews on the relationship between bNfL and stroke have been published [12,22]. While our meta-analysis aligns with the main findings of Liu et al., there are notable distinctions between the two studies. Specifically, Liu et al. [12] included data from five studies and 1346 patients, whereas our meta-analysis incorporated data from nine studies and 2302 patients. The increased statistical power resulting from the inclusion of nearly 1000 additional cases in our analysis positions it as the most up-to-date and comprehensive study on the subject, providing further support for previous findings in the literature. Furthermore, we conducted a comprehensive analysis of heterogeneity, examining both clinical and methodological factors through subgroup analysis, encompassing a total of seven aspects. In contrast, Liu et al. [12] only investigated heterogeneity based on blood sampling time. Additionally, a sensitivity analysis was performed to assess the stability of the results. Sanchez et al. [22] focused on temporal patterns of neurofilament light as a blood-based biomarker for stroke in their meta-analysis. The study encompassed a range of cerebrovascular conditions, such as AIS, and chronic cerebrovascular disease like cerebral small vessel disease and cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy. AIS cases accounted for only half of the total sample. Additionally, this meta-analysis did not conducted the pooled OR for quantitatively assessing the predictive value of bNfL in AIS functional outcomes.
Implications for clinical practice
The NfL protein, an intermediate filament protein, is indicative of primary axonal injury and secondary neurodegeneration [23]. It is released into the cerebrospinal fluid and bloodstream following neuronal tissue damage [24], demonstrating high specificity to the nervous system. Previous research has suggested that abnormal concentration of NfL serve as a direct marker of the severity of neurological diseases [2]. Our meta-analysis, following a systematic review of the existing literature, presents the most up-to-date and comprehensive evidence supporting bNfL as a predictive biomarker of AIS outcome. Consistent with previous research, our study further confirmed the correlation between bNfL and outcomes of AIS. Ferrari et al. [8] identified NfL-D7 as a significant predictor of 3-month NIHSS and the most effective biomarker for AIS patients. Tiedt et al. [9] observed a continued elevation in sNfL levels for up to 6 months post-ischemic stroke. The increase in sNfL levels during the acute phase following ischemic injury can be attributed to the significant number of neuronal axonal injuries. The elevation of bNfL levels may be attributed to various potential mechanisms. Ischemic injury is considered a significant factor, while Waller’s degeneration is also suggested to play an important role. It is noted that large myelin axons, which are abundant in neurofilaments, are susceptible to Waller’s degeneration following a stroke [25]. Additionally, post-stroke immunity responses and inflammation are believed to be significant contributing factors. Shichita et al. [26] and Yan et al. [27] have demonstrated the involvement of immune and inflammatory processes in the pathophysiology of ischemic stroke injury in both animal models and human subjects. Furthermore, certain investigations have indicated that persistent blood-brain barrier breakdown probably prompt prolonged release of bNfL [28,29]. None of the included studies provided head-to-head comparisons of bNfL-augmented models versus standard clinical scores (e.g., NIHSS + age + infarct volume). Therefore, we cannot conclude that bNfL adds incremental predictive value beyond readily available covariates.
According to the subgroup analysis, the timing of blood sampling may be as a significant factor contributing to heterogeneity. Therefore, the selection of an appropriate blood sampling time is crucial for the accurate prediction of bNfL on stroke outcomes, as shown in [8,12,20,22,30,31]. However, our study indicates that measurement taken within a time frame of less than 4 days may not capture the relationship between bNfL levels and post-stroke functional outcomes. Further investigation into the temporal pattern of bNfL post-stroke is warranted to pinpoint the peak levels, which could have implications for utilizing NfL as a predictive biomarker for stroke outcomes. In the present subgroup analysis stratified by region, it was observed that patients with higher levels of bNfL exhibited a greater risk of poor functional outcome compared with those with lower levels of bNfL in studies conducted in Asia and Europe and America. These findings suggest that bNfL may serve as a predictive biomarker for AIS across various geographical regions. Furthermore, when stratified by study sample size, it was noted that studies with larger sample sizes tended to yield larger effect sizes than smaller studies. Additionally, stratification by age revealed that studies including individuals aged 60 years and older were associated with a higher risk of poor functional outcome. This observation appears to be associated with pronounced arteriosclerosis, heightened inflammatory reaction and severe ischemic conditions. Subgroup analysis focusing on blood specimen revealed significant heterogeneity in studies utilizing serum. Despite the widespread use of ultra-sensitive single-molecule array technology in most studies, potential variations in blood NfL levels between serum and plasma measurements should be carefully considered. What is noticeable is that no significant heterogeneity were found in the sample testing method and inclusion of TIA stratification. However, these results can not completely rule out the source of heterogeneity, after all, the sample size included in TIA is not large enough and studies using Electrochemiluminescence immunoassay are limited. It should be noted that these results should be interpreted with caution, because the results of the subgroup analysis were observational and larger studies are needed to evaluate the effect of bNfL as a predictor of stroke functional outcomes in the subgroups. The statistically significant differences may be due to smaller sample sizes and fewer studies included in these subgroups, rather than an absence of effect, and differences are unlikely to be clinically significant. At present, no interventional trial has used bNfL levels to triage patients to more intensive monitoring, prolonged ICU stay, or escalation of secondary prevention. Until such trials are completed, bNfL should be considered a prognostic enrichment biomarker for research cohorts rather than a trigger for specific therapeutic decisions.
Strengths & limitations
To the best of our knowledge, this is the most recent and the comprehensive systematic review and meta-analysis on the correlation between bNfL and AIS outcomes to date. Several strengths of our study are evident. First, the results of our meta-analysis offer the most up-to-date and compelling evidence for informing updates to clinical practice. Second, we performed subgroup analyses to investigate potential sources of heterogeneity, considering both clinical and methodological factors across seven dimensions. The subgroup analysis should have improved the credibility of the study and provided a benchmark for future research. Thirdly, our meta-analysis comprised nine studies in which we sought to assess the predictive value of bNfL in determining functional outcomes following AIS. Moreover, our systematic review was not constrained by temporal or linguistic restrictions.
There are some limitations in our study that should be taken into account. First, there was notable heterogeneity among the included studies, likely stemming from variations in sampling time, study region, participant age, blood specimen and sample size. Additionally, there may be other unidentified sources of heterogeneity. Second, while some studies have reported the proportion of etiological subtypes, the precise relationship between bNfL and functional outcomes in stroke etiological subtypes remains unclear. It would be advantageous to conduct subgroup analysis according to stroke etiological subtypes. Third, it is important to note that while one study was observational, two were prospective observational studies, and the remaining studies were prospective cohort studies. Discrepancies in study designs may limit the ability to establish causality. Fourth, because all included studies dichotomised mRS at ≥3, we were unable to examine the full ordinal distribution. Future individual-patient-data meta-analyses should test whether bNfL predicts a shift across the entire mRS range. Finally, Follow-up interval differed across studies (7 days to 6 months). Because most cohorts reported only the 90-day mRS, we could not examine whether the prognostic value of bNfL attenuates or strengthens with longer follow-up. Individual-patient-data meta-analyses that incorporate repeated mRS measurements are warranted.
Conclusions
To summarize, the findings of our research indicate that bNfL has promise as a prognostic biomarker for functional outcomes among those suffering from AIS. Furthermore, compared with individuals with lower bNfL levels, those with higher levels run a higher chance of suffering from poor functional outcomes, according to the meta-analysis. Additionally, the sampling time, study region, participant age, blood specimen and sample size may be important potential confounding factors.
Summary points
•
Despite advancements in early detection and management strategies, ischemic stroke continues to be a significant contributor to mortality and disability on a global scale.
•
Prior research has yielded varying results regarding the predictive capabilities of blood neurofilament light chain (bNfL) on stroke functional outcomes.
•
The objective of this systematic review is to assess the efficacy of bNfL as a predictor of stroke functional outcomes.
•
Nine studies involving 2302 patients were included in the analysis.
•
The meta-analysis revealed a pooled adjusted OR of 1.929 (95% CI: 1.459, 2.550), suggesting that the patients with higher bNfL levels are at a greater risk of experiencing unfavorable functional outcomes compared with those with lower bNfL levels.
•
In summary, bNfL demonstrates potential as a predictive biomarker for functional outcomes in acute ischemic stroke patients.
•
The sampling time, study region, participant age, blood specimen and sample size may be important potential confounding factors.
•
Additional rigorously designed and meticulously executed prospective studies on a larger scale are warranted to validate these findings.
Author contributions
L Chen and H-Y Xu contributed to the conception and design of the study, H-Y Xu and H-Y Lin contributed to acquisition of data, analysis and interpretation of data, drafting the article. R-X Qin, L-D Shao, W Xu, Q-C Qin, X-Y Lai, and X-J Liang contributed to editing. All authors contributed to the article and approved the submitted version.
Acknowledgments
We thank all authors who helped in providing us with the data required for the analysis and for their valuable suggestions.
Financial disclosure
This study was supported by grants from the National Natural Science Foundation of China (82271371 and 82260367), the High-Level Medical Expert Training Program of Guangxi “139” Plan Funding, the Guangxi Medical and Health Appropriate Technology Development and Application Project (S2021107), the Clinical Research “Climbing” Program of the First Affiliated Hospital of Guangxi Medical University (YYZS2021002), the Advanced Innovation Teams and Xinghu Scholars Program of Guangxi Medical University.
Competing interests disclosure
The authors have no competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
Writing disclosure
No funded writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
Ethical approval and informed consent are deemed unnecessary for this study, as it solely consists of a literature review and did not entail any direct interaction with patients.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary data.docx)
- Download
- 23.49 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
GBD 2016 Stroke Collaborators. Global, regional, and national burden of stroke, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 18(5), 439–458 (2019).
2.
Rattanawong W, Ongphichetmetha T, Hemachudha T, Thanapornsangsuth P. Neurofilament light is associated with clinical outcome and hemorrhagic transformation in moderate to severe ischemic stroke. J. Cent. Nerv. Syst. Dis. 15, 11795735221147212 (2023).
• Study exploring whether neurofilament light chain (NfL) could predict clinical outcome and hemorrhagic transformation in moderate-to-severe stroke.
3.
Powers WJ, Rabinstein AA, Ackerson T et al. Guidelines for the early management of patients with acute ischemic stroke: 2019 update to the 2018 Guidelines for the early management of acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 50(12), e344–e418 (2019).
4.
Wollenweber FA, Tiedt S, Alegiani A et al. Functional outcome following stroke thrombectomy in clinical practice. Stroke 50(9), 2500–2506 (2019).
5.
van Horn N, Kniep H, Leischner H et al. Predictors of poor clinical outcome despite complete reperfusion in acute ischemic stroke patients. J. Neurointerv. Surg. 13(1), 14–18 (2021).
6.
Correia M, Silva I, Gabriel D et al. Early plasma biomarker dynamic profiles are associated with acute ischemic stroke outcomes. Eur. J. Neurol. 29(6), 1630–1642 (2022).
7.
Maas MB, Furie KL. Molecular biomarkers in stroke diagnosis and prognosis. Biomark. Med. 3(4), 363–383 (2009).
8.
Ferrari F, Rossi D, Ricciardi A et al. Quantification and prospective evaluation of serum NfL and GFAP as blood-derived biomarkers of outcome in acute ischemic stroke patients. J. Cereb. Blood Flow Metab. 43(9), 1601–1611 (2023).
9.
Tiedt S, Duering M, Barro C et al. Serum neurofilament light: a biomarker of neuroaxonal injury after ischemic stroke. Neurology 91(14), e1338–e1347 (2018).
10.
Uphaus T, Bittner S, Gröschel S et al. NfL (Neurofilament Light Chain) levels as a predictive marker for long-term outcome after ischemic stroke. Stroke 50(11), 3077–3084 (2019).
11.
Onatsu J, Vanninen R, Jäkälä P et al. Serum neurofilament light chain concentration correlates with infarct volume but not prognosis in acute ischemic stroke. J. Stroke Cerebrovasc. Dis. 28(8), 2242–2249 (2019).
12.
Liu DS, Chen J, Wang XY, Xin JL, Cao RL, Liu ZR. Serum neurofilament light chain as a predictive biomarker for ischemic stroke outcome: a systematic review and meta-analysis. J. Stroke Cerebrovasc. Dis. 29(6), 104813 (2020).
•• This meta-analysis validated the role of serum Neurofilament light chain (sNfL) as a predictive biomarker for stroke outcome and investigated heterogeneity based on blood sampling time.
13.
Gendron TF, Badi MK, Heckman MG et al. Plasma neurofilament light predicts mortality in patients with stroke. Sci. Transl. Med. 12(569), eaay1913 (2020).
14.
Chen CH, Chu HJ, Hwang YT et al. Plasma neurofilament light chain level predicts outcomes in stroke patients receiving endovascular thrombectomy. J. Neuroinflammation 18(1), 195 (2021).
15.
Zhou FY, Chen DW, Li HY et al. The association of serum neurofilament light chain and acute ischaemic stroke is influenced by effective revascularization. Dis. Markers 2022, 5236080 (2022).
16.
Li J, Zhang P, Zhu Y et al. Serum neurofilament light chain levels are associated with early neurological deterioration in minor ischemic stroke. Front. Neurol. 14, 1096358 (2023).
17.
Wells GA, Wells G, Shea B et al. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Semantic Scholar (2014). Available from: https://www.semanticscholar.org/paper/The-Newcastle-OttawaScale-(NOS)-for-Assessing-the-Wells-Wells/c293fb316b6176154c3fdbb8340a107d9c8c82bf
18.
Traenka C, Disanto G, Seiffge DJ et al. Serum neurofilament light chain levels are associated with clinical characteristics and outcome in patients with cervical artery dissection. Cerebrovasc. Dis. 40(5–6), 222–227 (2015).
19.
De MGM, Katan M, Barro C et al. Serum neurofilament light chain in patients with acute cerebrovascular events. Eur. J. Neurol. 25(3), 562–568 (2018).
20.
Pedersen A, Stanne TM, Nilsson S et al. Circulating neurofilament light in ischemic stroke: temporal profile and outcome prediction. J. Neurol. 266(11), 2796–2806 (2019).
• This systematic review and meta-analysis shows that serum neurofilament light (sNfL) dynamics vary by stroke subtype and that higher sNfL levels are associated with worse neurological and functional outcomes, independently of initial stroke severity.
21.
Kuhle J, Barro C, Andreasson U et al. Comparison of three analytical platforms for quantification of the neurofilament light chain in blood samples: ELISA, electrochemiluminescence immunoassay and Simoa. Clin. Chem. Lab. Med. 54(10), 1655–1661 (2016).
22.
Sanchez JD, Martirosian RA, Mun KT et al. Temporal patterning of neurofilament light as a blood-based biomarker for stroke: a systematic review and meta-analysis. Front. Neurol. 13, 841898 (2022).
•• This systematic review and meta-analysis highlights temporal patterns of neurofilament light as a blood-based biomarker for stroke. The study encompassed a range of cerebrovascular conditions, such as acute ischemic stroke, and chronic cerebrovascular disease like cerebral small vessel disease and cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy. Acute ischemic stroke cases accounted for only half of the total sample.
23.
Pekny M, Wilhelmsson U, Stokowska A, Tatlisumak T, Jood K, Pekna M. Neurofilament light chain (NfL) in blood – a biomarker predicting unfavourable outcome in the acute phase and improvement in the late phase after stroke. Cells 10(6), 1537 (2021).
24.
Varhaug KN, Torkildsen Ø, Myhr KM, Vedeler CA. Neurofilament light chain as a biomarker in multiple sclerosis. Front. Neurol. 10, 338 (2019).
25.
Thomalla G, Glauche V, Koch MA, Beaulieu C, Weiller C, Röther J. Diffusion tensor imaging detects early Wallerian degeneration of the pyramidal tract after ischemic stroke. Neuroimage 22(4), 1767–1774 (2004).
26.
Shichita T, Sugiyama Y, Ooboshi H et al. Pivotal role of cerebral interleukin-17-producing gammadeltaT cells in the delayed phase of ischemic brain injury. Nat. Med. 15(8), 946–950 (2009).
27.
Yan J, Greer JM, Etherington K et al. Immune activation in the peripheral blood of patients with acute ischemic stroke. J. Neuroimmunol. 206(1–2), 112–117 (2009).
28.
Khalil M, Teunissen CE, Otto M et al. Neurofilaments as biomarkers in neurological disorders. Nat. Rev. Neurol. 14(10), 577–589 (2018).
29.
Wu JX, Wu DQ, Liang YB, Zhang Z, Zhuang L, Wang ZP. Plasma neurofilament light chain: a biomarker predicting severity in patients with acute ischemic stroke. Medicine (Baltimore) 101(26), e29692 (2022).
• Found that Plasma NfL levels reflect neuronal injury after acute ischemic stroke. It changes with time and has a certain relationship with prognosis.
30.
Barry DM, Millecamps S, Julien JP, Garcia ML. New movements in neurofilament transport, turnover and disease. Exp. Cell Res. 313(10), 2110–2120 (2007).
31.
Pujol-Calderón F, Portelius E, Zetterberg H, Blennow K, Rosengren LE, Höglund K. Neurofilament changes in serum and cerebrospinal fluid after acute ischemic stroke. Neurosci. Lett. 698, 58–63 (2019).
Information & Authors
Information
Published In
Copyright
© 2025 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 28 April 2024
Accepted: 3 September 2025
Published online: 7 October 2025
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Blood neurofilament light chain as a predictive biomarker for functional outcome of acute ischemic stroke: a systematic review and meta-analysis. (2025) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2025-0130
Export citation
Select the citation format you wish to export for this article or chapter.