The role of health economic evidence in clinical practice guidelines for colorectal cancer: a comparative analysis across countries
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Colorectal cancer (CRC) is among the most prevalent malignancies globally and causes massive resource consumption and economic burden. Health economic evidence (HEE) has been used in clinical practice guidelines (CPGs) for cancer to facilitate the rational allocation of health resources. However, in certain guideline development organizations, HEE is not yet utilized as a formal decision-making criterion. This study aimed to compare the discrepancies in the utilization of health economics as evidence in CRC CPGs across different countries and review specific features of economic evidence concerning the guidelines’ applicability. Materials & methods: A systematic review was conducted using databases including Medline, Embase, CNKI, WanFang, and other guidelines databases to identify CPGs for CRC published in English or Chinese from January 2017 to September 2023. Data on the incorporation and application of HEE were extracted, and the method and quality of cost–effectiveness analysis (CEA) studies were evaluated. Descriptive analyses were used to summarize the results. Results: Out of 53 CPGs from 14 countries, most originated from the USA (n = 17 of 53 [32%]) and Canada (n = 9 of 53 [17%]). Sixty-eight percent (36/53) considered cost justification, and 57% (30/53) incorporated health economics studies as evidence. The included HEE cited in CPGs ranged from 1990 to 2021 and were not aligned with the countries in which the guidelines were issued. Among these CEA studies, 52% (26/50) were related to screening strategies, and 32% (16/50) pertained to treatment measures. The Markov model was the most frequently used (n = 27 of 50 [54%]). Based on the CHEQUE tool, the methodological quality of these CEA studies was inadequate in areas such as multiple data sources, approaches to select data sources, assessing the quality of data, and relevant equity or distribution. Conclusion: In summary, 57% of guidelines incorporated health economics studies as evidence, with a variation between different countries. The included HEE still had deficiencies in methodology and reporting quality. In the future, it is suggested that health economics research should use a standardized methodology and reporting approach to assist in clinical decision making.
Plain language summary
What is this article about?
Based on healthcare evidence and expert opinion, clinical practice guidelines (CPGs) are an important reference to help healthcare practitioners make scientific decisions. The inclusion of health economic evidence (HEE) in CPGs promotes the efficient utilization of health resources. This study aims to evaluate whether HEE was considered in developing CPGs of colorectal cancer across different countries and review the applicability, methodology, and quality of these health economics studies.
What were the results?
We included 53 CPGs and extracted 80 HEE studies from them, including 50 cost–effectiveness analysis (CEA) studies. The application of HEE in CPGs showed discrepancies between different countries and medical associations. HEE research contributed to cost-based de-escalation of treatment strategies, reporting the economic burden of the disease and elucidating the health-economic comparative benefits of the intervention. Based on the CHEQUE evaluation tool, the methodological and reporting quality of these CEA studies cited as references demonstrated deficiencies.
What do the results mean?
The incorporation of HEE into CPGs as a form of supporting evidence still varies globally. In addition, guidelines tend to ignore the applicability of results from a single HEE. The integration of HEE into CPGs remains challenging.
Health economic evidence (HEE) employs economic methodologies to allocate resources effectively, focusing on medical demand, decision-making and limited health resources. HEE can be generated through budget impact analyses, economic evaluations, cost studies and other methodological approaches [1,2]. High-quality clinical practice guidelines (CPGs) provide evidence-based recommendations to assist healthcare professionals in making decisions tailored to specific clinical situations. It has been shown that HEE can promote a fairer distribution of health by offering cost-effective alternatives [3].
The integration of HEE into CPG formulation still presents challenges globally [2,4]. The UK’s National Institute for Health and Care Excellence emphasized HEE, asserting that clinical guidelines must consider the relative costs and benefits of interventions [5]. In 2015, the American Society of Clinical Oncology (ASCO) released a statement [6] on the value of cancer treatment aiming to assist oncologists and patients in effectively integrating financial considerations into their clinical decisions, yet it did not explicitly mention economic evidence. China adopted HEE as one of the fundamental criteria for negotiating medical insurance coverage in 2017, though it lacks a standardized framework for HEE in clinical guidelines. Currently, the role of HEE in CPGs is influenced by the healthcare system, medical resources, value preferences and social welfare across different countries [2].
In 1990, the Institute of Medicine (IOM) defined CPGs as ‘‘systematically developed statements to assist practitioner and patient decisions about appropriate healthcare for specific clinical circumstances” [7]. It was revised to encompass only guidelines developed from systematic reviews in 2011 [8]. As with other evidence, guidelines could identify HEE inclusion when selecting topics, then compile available economic evidence and develop recommendations based on the strength of the evidence [9]. Hence, the validity of HEE should be a focal point of evaluation, such as population, intervention, model and time of publication.
Colorectal cancer (CRC) is the third most commonly diagnosed cancer and the second leading cause of cancer-related death worldwide. In 2020, CRC constituted approximately 1.9 million new cases and 900,000 deaths [10]. Higher incidences are found in countries with higher Human Development Index. Concurrently, nations undergoing economic development and shifts in dietary patterns and lifestyles are experiencing noticeable rising incidence rates [11,12]. The medical management of CRC is intricate and demands massive resources, imposing substantial financial burdens on patients and healthcare systems worldwide. The average annual growth rate of the medical expenditure per CRC patient in China ranged from 6.9 to 9.2%, and the 1-year out-of-pocket expenditure of a newly diagnosed patient accounted for about 60% of their previous-year household [13]. Economic considerations are increasingly integrated into the medical decision-making processes for cancer because of escalating healthcare expenditure caused by new cases and medical innovations. Therefore, the objective of this study was twofold. First, a review of current guidelines for CRC aims to identify whether HEE was used and to evaluate the role of HEE in CPGs. Second, we also aimed to identify specific features of economic evidence relative to the applicability of the guidelines and augment the probability of HEE assuming a more substantial role in the decision-making process.
Materials & methods
Guidelines sources
To ensure the comprehensive inclusion of clinical guidelines, we conducted a systematic search across renowned medical guideline databases. CPG recommendations require regular updating; however, the timing of these updates remains a subject of debate [8]. The National Comprehensive Cancer Network conducts an annual panel review every 3 years to ensure updates; the National Guideline Clearinghouse mandates that guidelines be re-examined every 5 years [8]. To ensure the inclusion of the most recent guidelines, those published between 2017 and 2023 were selected for this study, covering the period from January 2017 to September 2023. Databases searched include Medline, Embase, Guidelines International Network, National Guideline Clearinghouse, National Comprehensive Cancer Network, National Institute for Health and Care Excellence, Cancer Council Australia and Canadian Medical Association, Scottish Intercollegiate Guidelines Network, CNKI, WanFang and Yiigle. The complete electronic search strategy for PubMed is presented in Table 1.
| Concept | Search strategy |
|---|---|
| Colorectal Cancer | “colorectal cancer” OR “colorectal tumor” OR “colorectal neoplasms” OR “colorectal carcinoma” OR “colon cancer” OR “rectum cancer” |
| AND | |
| Guideline | “guideline” OR “practical guideline” |
| = | |
| Search Strategy | (“Colorectal Neoplasms”[Mesh] OR colorectal cancer[tiab] OR colorectal tumor[tiab] OR colon cancer[tiab] OR colon tumor[tiab] OR colon neoplasm[tiab] OR rectal cancer[tiab] OR rectal tumor[tiab] OR rectal neoplasm[tiab] OR rectum cancer[tiab] OR rectum tumor[tiab] OR rectum neoplasm[tiab]) AND (“Guideline”[Publication Type] OR “Guidelines as Topic”[Mesh] OR “Practice Guideline”[Publication Type]) AND (2017:2023[pdat]) Filters: from 2017–2023 |
Guidelines selection
We included guidelines for CRC published in English and Chinese. The inclusion criteria were CPGs aligned with the definition proposed by IOM in 1990, formulated or recognized by professional medical societies, academic associations, and health authorities. The following guidelines were excluded: rapid guidelines, duplicates and non-full-text publications, and those not meeting inclusion criteria. Two reviewers independently conducted a separate evaluation of the title and abstract of the guidelines to determine eligibility.
Detection of HEE
The HEEs incorporated in the study are explicitly cited in CPGs. The full text of the guidelines and references were reviewed. A scan was conducted using the keywords ‘cost’, ‘expenditure’, ‘resource’, and ‘economic’ to identify the HEE as references in the CPGs. The extracted HEEs include reviews of health economic studies, cost analysis, and cost–effectiveness analysis (CEA). The empirical study encompasses both cost analysis and CEA. Furthermore, we screened the countries of origin for the CPGs, year of publication, publishing organization, disease domain, and medical classification, then assessed the inclusion of cost within the guidelines. To evaluate the role of HEE, we analyzed the purpose for which it was cited as a reference in the CPGs.
Data extraction & quality appraisal of CEA
Abstracts, letters, posters, reviews and cost analyses were excluded. We designed the data extraction form to obtain information. For the CEA literature, the specific content extracted included country, type, disease classification, perspective, model structure, cost, verification, health outcomes, time horizon and funding sources. The Health Economic Quality Evaluation (CHEQUE) tool [14] was used to assess the quality of CEA. The CEA studies were evaluated on a scale of 0–100 with 24 items of 15 dimensions from methodological quality and reporting quality, whereby 0 represents the lowest quality and 100 highest quality. Every question and each response carried a specific weight. Method 2 was that ‘not applicable’ was omitted from the final score, and method 1 was not [14].
Result
Identified guidelines
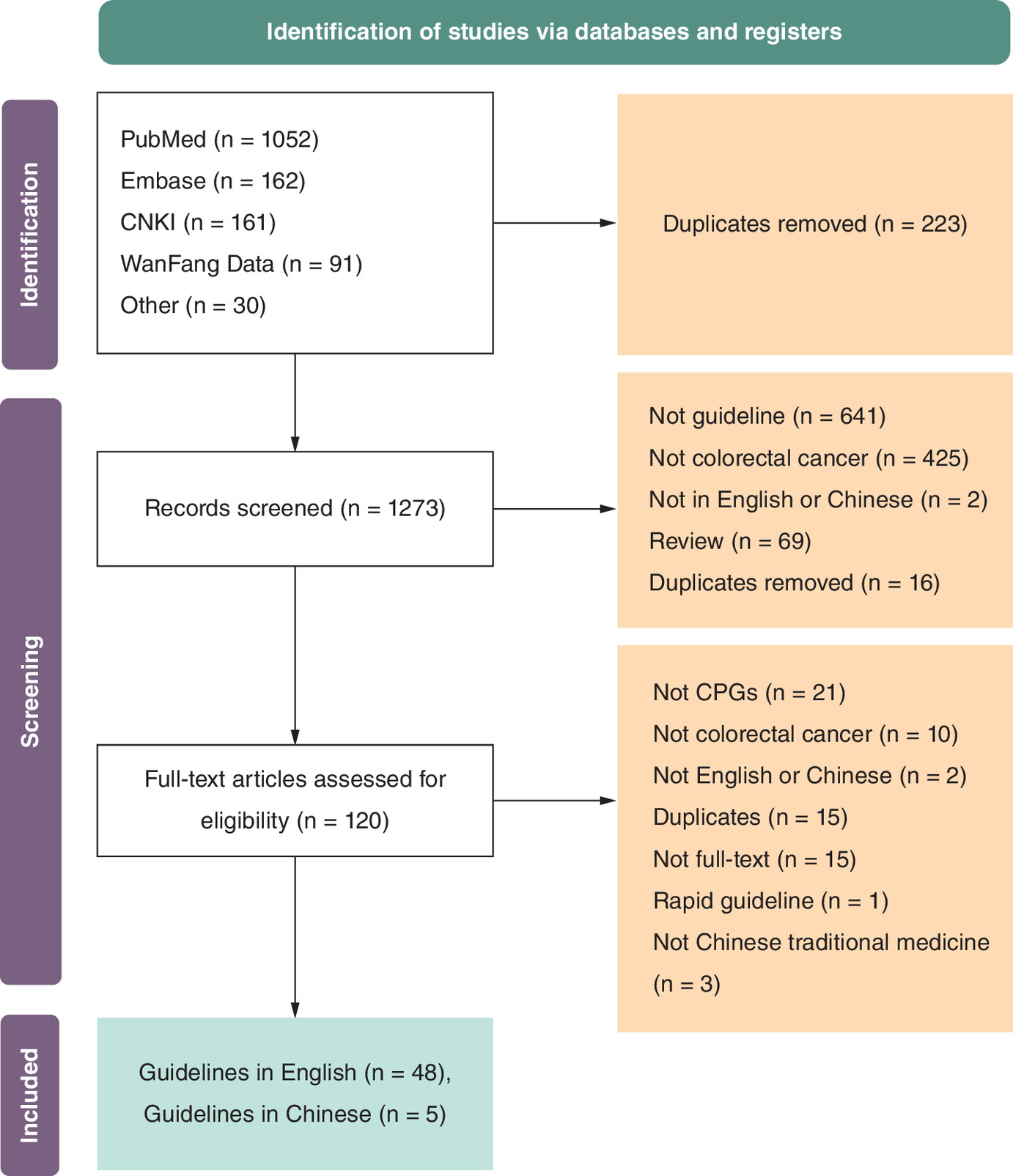
Using the inclusion and exclusion criteria, we screened the guidelines, resulting in 91% (48/53) of CPGs being in English and 9% (5/53) in Chinese. The inclusion process of guidelines is shown in Figure 1.
Overview of guidelines
Table 2 summarizes the basic information of the guidelines, which were sourced from a diverse range of 14 countries or regions. Most guidelines originated from the USA (n = 17 of 53 [32%]) and Canada (n = 9 of 53 [17%]), with 9% (5/53) from China. The comprehensive details regarding CPGs can be found in Supplementary Table 1.
| Characteristic | CPGs (n [%]) | CEA study (n [%]) |
|---|---|---|
| Year of publication | ||
| 1990–2000 | NA | 1 (2) |
| 2000–2010 | NA | 9 (18) |
| 2011–2016 | NA | 21 (42) |
| 2017–2020 | 31 (58) | 18 (36) |
| 2021–2023 | 22 (42) | 1 (2) |
| Country | ||
| USA | 17 (32) | 20 (40) |
| Canada | 9 (17) | 4 (8) |
| Europe | 5 (9) | 0 (0) |
| China | 5 (9) | 1 (2) |
| UK | 3 (6) | 8 (16) |
| Asia | 3 (6) | 0 (0) |
| France | 2 (4) | 0 (0) |
| Japanese | 2 (4) | 0 (0) |
| Spain | 2 (4) | 2 (4) |
| Germany | 1 (2) | 0 (0) |
| Italy | 1 (2) | 1 (2) |
| Malaysia | 1 (2) | 1 (2) |
| Australia | 1 (2) | 4 (8) |
| International | 1 (2) | 0 (0) |
| Other | 0 (0) | 9 (18) |
NA: ‘Not applicable’, meaning the data does not apply to the specific group.
CEA: Cost–effectiveness analysis; CPG: Clinical practice guidelines.
HEE in guidelines
Identification of HEE
Table 3 shows the inclusion of cost justification and the integration of HEE in CPGs from various countries and medical associations. Among the 53 guidelines reviewed, 68% (36/53) [15–51] considered cost factors in formulating recommendations for practice strategies. Additionally, 57% (30/53) [15–17,19–26,28,30,31,33–38,41–49,52] incorporated health economics studies as evidence, including reviews, cost analyses and CEAs. Among the five Chinese guidelines, three [49,50,53] alluded to cost or economic burden, with only one [49] involving economic evidence. Of the guidelines that did not consider cost, a CPG [54] formed in the US reported the reason the guideline was based on a patient–surgeon perspective and not a population perspective. A guideline [55] of Canadian Cancer Care Ontario stated that only clinical evidence should be considered, with costs addressed by other divisions.
| Country/region | Publishing organization | Guidelines considering cost (n[N]) | Guidelines including HEE (n[N]) | Average HEE (n) | Ref. |
|---|---|---|---|---|---|
| USA | American Society for Clinical Pathology (ASCP), etc. | 1 (1) | 0 (1) | 0.0 | [15] |
| American Society of Clinical Oncology (ASCO) | 6 (6) | 5 (6) | 3.0 | [16–21] | |
| American Cancer Society (ACS) | 1 (1) | 1 (1) | 2.0 | [22] | |
| National Comprehensive Cancer Network (NCCN) | 3 (3) | 3 (3) | 3.7 | [23–25] | |
| Society of American Gastrointestinal and Endoscopic Surgeons (SAGES), etc. | 0 (1) | 0 (1) | 0.0 | [54] | |
| American Society of Colon and Rectal Surgeons (ASCRS) | 3 (4) | 2 (4) | 0.5 | [26–29] | |
| American College of Gastroenterology (ACG) | 1 (1) | 1 (1) | 8.0 | [30] | |
| UK | National Institute for Health and Care Excellence (NICE) | 1 (1) | 1 (1) | 2.0 | [31] |
| British Society of Gastroenterology (BSG), etc. | 1 (1) | 0 (1) | 0.0 | [32] | |
| Association of Coloproctology of Great Britain and Ireland (ACPGBI), etc. | 1 (1) | 1 (1) | 1.0 | [33] | |
| Canada | Alberta Health Services | 2 (4) | 2 (4) | 0.5 | [34,35,56,57] |
| Cancer Care Ontario | 1 (4) | 2 (4) | 0.3 | [36,52,55,58] | |
| Canadian Association of Gastroenterology (CAG) | 1 (1) | 1 (1) | 6.0 | [37] | |
| France | French Society of Gastroenterology (SNFGE), etc. | 0 (1) | 0 (1) | 0.0 | [59] |
| French Society of Geriatric Oncology (SoFOG) | 0 (1) | 0 (1) | 0.0 | [60] | |
| Germany | Association of the Scientific Medical Societies (AWMF) | 1 (1) | 1 (1) | 1.0 | [38] |
| Italy | Italian Medical Oncology Association (AIOM) | 1 (1) | 0 (1) | 0.0 | [39] |
| Japanese | Japanese Society for Cancer of the Colon and Rectum (JSCCR) | 2 (2) | 1 (2) | 0.5 | [40,41] |
| Malaysia | Malaysia Health Technology Assessment Section (MaHTAS) | 1 (1) | 1 (1) | 6.0 | [42] |
| Spain | Spanish Association of Gastroenterology (AEG), etc. | 0 (1) | 0 (1) | 0.0 | [61] |
| Spanish Society of Medical Oncology (SEOM), etc. | 0 (1) | 0 (1) | 0.0 | [62] | |
| Asia | European Society for Medical Oncology (ESMO), etc. | 0 (2) | 0 (2) | 0.0 | [63,64] |
| Asian Pacific Association of Gastroenterology (APAGE) | 1 (1) | 1 (1) | 5.0 | [43] | |
| Australia | Cancer Council Australia | 1 (1) | 1 (1) | 4.0 | [44] |
| Europe | European Society for Medical Oncology (ESMO) | 0 (2) | 0 (2) | 0.0 | [65,66] |
| European Society of Gastrointestinal Endoscopy (ESGE) | 3 (3) | 3 (3) | 2.7 | [45–47] | |
| International | Delphi Initiative for Early-Onset Colorectal Cancer(DIRECt) group | 1 (1) | 1 (1) | 1.0 | [48] |
| China | Chinese Society of Colorectal Surgery, etc. | 1 (1) | 1 (1) | 1.0 | [49] |
| National Cancer Center of China | 1 (1) | 0 (1) | 0.0 | [50] | |
| Chinese Medical Association, etc. | 1 (2) | 0 (2) | 0.0 | [51,53] | |
| Society for Minimally Invasive Surgery, etc. | 0 (1) | 0 (1) | 0.0 | [67] |
HEE: Health economic evidence; N: Total number of guidelines developed by the respective academic associations.
The 53 guidelines [15–67] included a total of 80 HEE studies as references, with an average of 1.51 references per guideline. Out of these associations analyzed, only 32% (10/31) which were from seven countries or regions, had higher than 1.51 references, suggesting a potential acknowledgment of HEE. Notably, 57% (4/7) of associations in the USA exceeded this average. In contrast, associations in France, Spain, Italy and China demonstrated a slightly lower tendency to use HEE. Twelve associations did not incorporate any HEE studies.
Role of HEE in CPGs
Three ASCO guidelines [16,17,20] in the US referred explicitly to the cost justification and proposed that physicians should engage in discussions regarding the choice of more economical alternatives with patients when it is both pragmatic and viable for the course of treatment. In some CPGs, cost studies were used to delineate the significant social burden caused by the rising incidence and mortality of CRC, as well as the economic burden on patients [20,21,34,43]. In addition, cost studies can be used to demonstrate whether an intervention is economically advantageous [46].
CEA can evaluate the cost–effectiveness of the inclusion strategies in the prescription, ensuring that limited healthcare resources maximize patient outcomes. For instance, an Australian guideline on CRC [44] incorporated the cost–effectiveness of the immunochemical fecal occult blood test in the National Bowel Cancer Screening Program compared with five other screening strategies to support the review of the guideline. Additionally, CEA can also be used as part of the development of clinical pathways that consider a more comprehensive range of treatment options in a particular disease area [68]. Twelve percent (6/50) guidelines [22,27,31–33,43] referenced CEA studies to explore the necessity for extended treatment duration, targeted pharmaceutical interventions or surgical procedures in addition to the current therapeutic regimens. CEA also facilitates the regulation of expenses and mitigates the excessive medical expenditures associated with patients. Based on the economic evidence, one screening guideline [22] delineated CRC screening strategies that can decrease the financial burden.
Overview of identified CEA studies
General features
Following the screening of clinical guidelines and scrutiny of the evidence, 50 full-text CEA studies from 12 countries were incorporated for assessment (Table 2), excluding non-CRC studies and duplicates. Some studies were published between 1990 and 2010 (n = 10 of 50 [20%]), more than 5 years prior to the release of the guideline, potentially indicating the limited applicability of the data. The countries where the CEA studies were conducted did not precisely align with those in which the guidelines were issued. Supplementary Table 2 lists basic information of the identified CEA studies.Most studies originated from the US (n = 20 of 50 [40%]) and the UK (n = 8 of 50 [16%]). The majority of studies were classified under screening (n = 26 of 50 [52%]) or treatment categories (n = 16 of 50 [32%]), with payer (n = 16 of 50 [32%]) and societal (n = 12 of 50 [24%]) perspectives being the most frequently adopted. Three CEA considered both the healthcare system and societal perspective [69–71].
Modeling strategies
Details on CEA are provided in Supplementary Table 2. Of the 50 CEA articles, the most commonly used model was the Markov model (n = 27 of 50 [54%]). Three studies [72–74] using the partitioned survival model were all about monoclonal antibody therapy strategies. The partitioned survival model provided an appropriate economic comparison method, avoiding transition probability calculation and various model assumptions. Seven CEA studies [70,71,74–78], based on randomized clinical trials, prospective studies, or meta-analyses, were conducted without models.
Microsimulation models were applied in screening studies to simulate disease trajectory at the individual level. One microsimulation model frequently used was the MISCAN-Colon [79–81], which was applied to model the disease trajectory, focusing on the adenoma–carcinoma sequence. Another microsimulation model is Policy1-Bowel [82], which adds a serrated pathway to CRC based on adenoma as disease routes modeled.
Health outcomes & cost
Most CEA studies used Quality Adjusted Life Year (QALY) as a measure of health outcome (n = 31 of 50 [62%]). QALYs weigh additional years of life gained by the particular medical intervention by multiplying the mean life-years by utility. Thirty-two percent (16/50) of studies reported life years or life months without measuring health utility. Most of the studies incorporated exclusively direct costs without indirect costs (n = 45 of 50 [90%]).
Sources of funding
Eighty-four percent (42/50) of the research disclosed their funding sources, with 16% of the funding coming from companies, 48% from research institutions and academic associations, 4% from governments and 2% from universities. Thirty-eight percent (3/8) of the funding from companies announced the authors’ independence in conducting the studies and publishing the report.
The quality of CEA
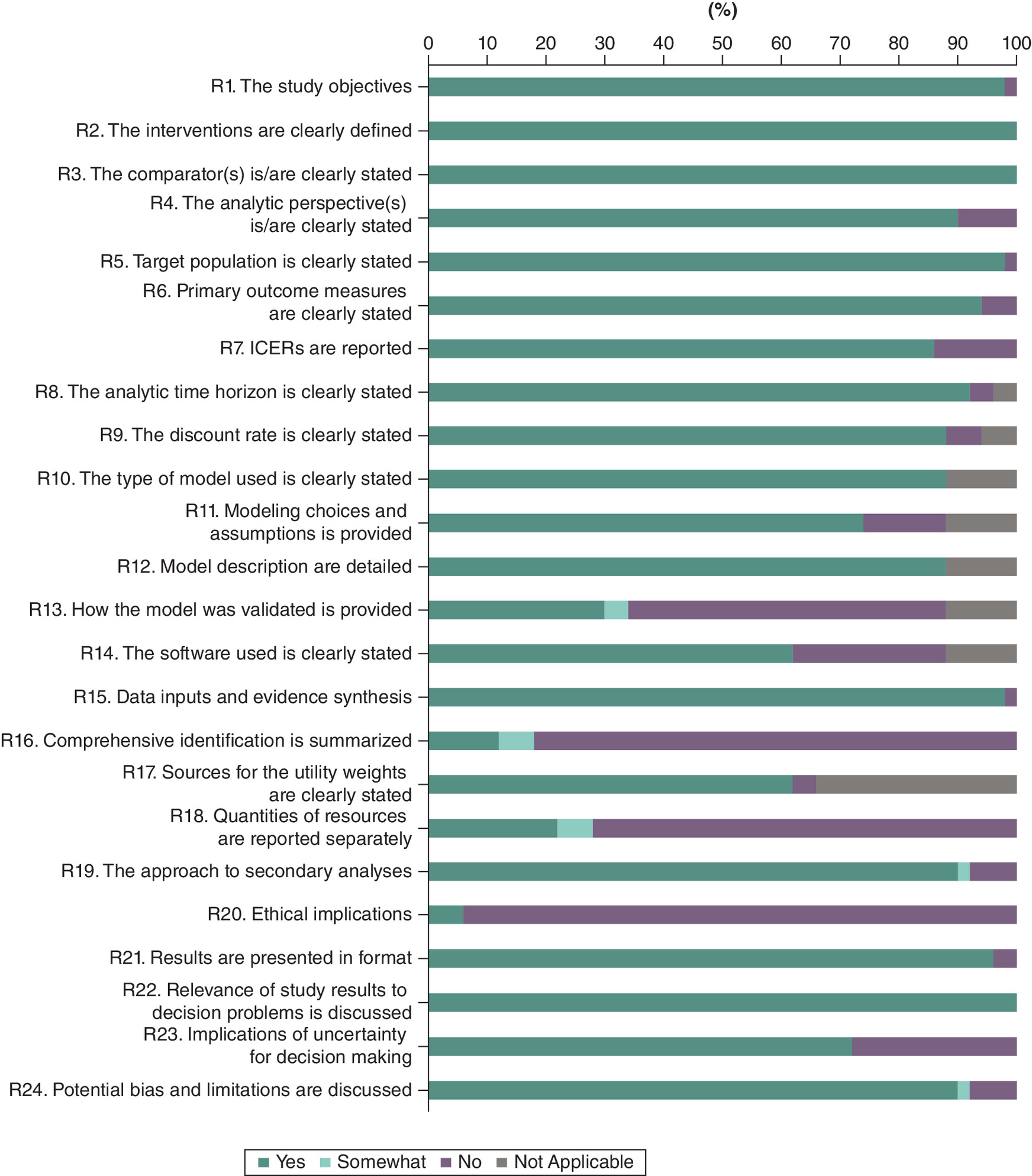
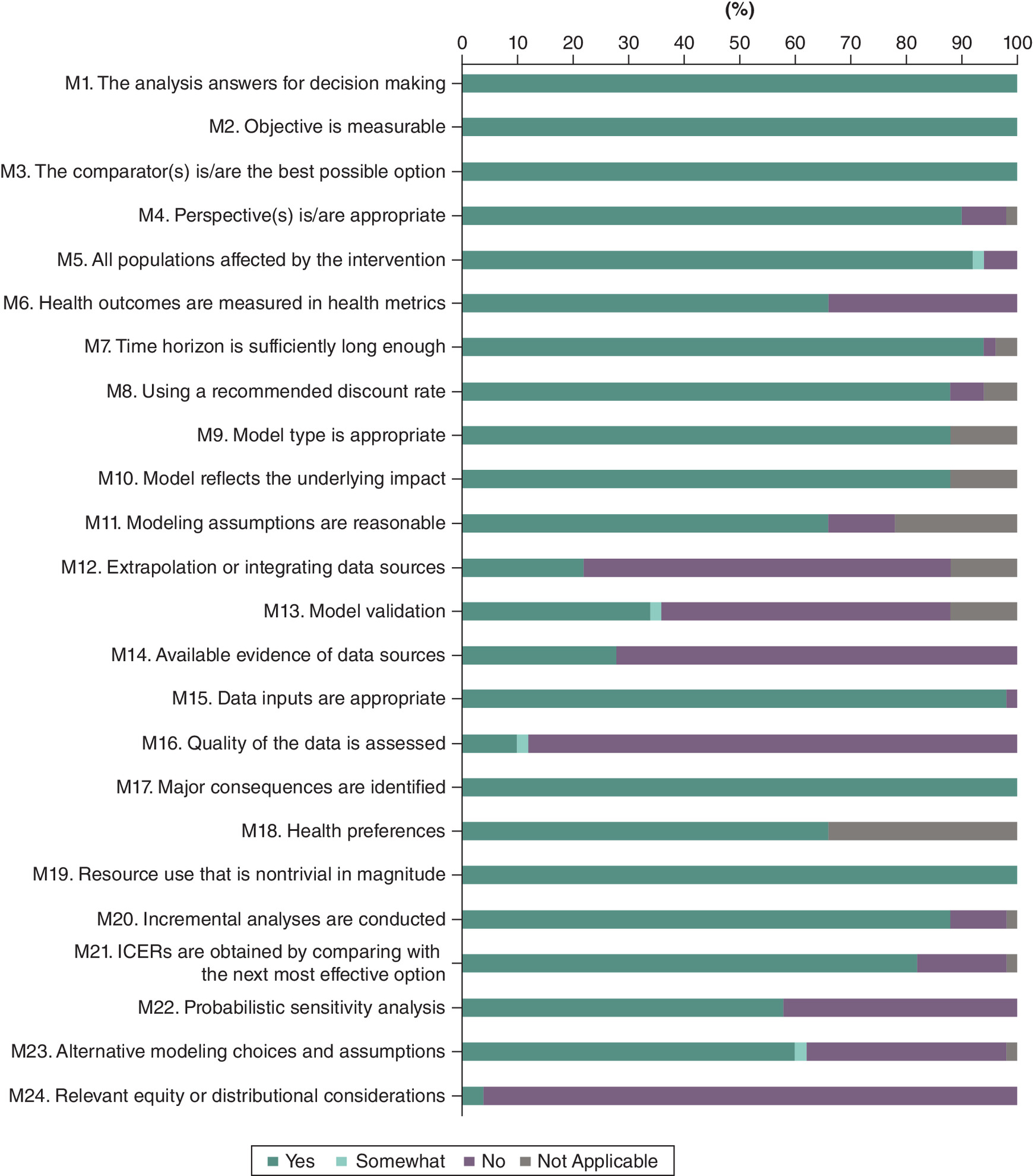
The results of the quality assessment using the CHEQUE instrument are presented in Supplementary Table 3. The reporting quality of all the included studies is at a high level (mean method 1 score: 88, mean method 2 score: 87). Model validation, separate reporting of resource costs and resource quantities, as well as ethical reporting, were observed in less than 40% of the CEA (Figure 2). For methodological quality, the items with less adequate reporting (≤40%) were multiple data sources, approaches to select data sources, the quality of data, and relevant equity or distribution (Figure 3). Figure 3 shows that less than 70% of the studies used QALY or Disability Adjusted Life Year (DALY) as a measure of health outcome. Both QALY and DALY are metrics for assessing health changes in patients.
Discussion
To our knowledge, the review represents the inaugural assessment and scrutinizes the incorporation of health economics evidence in CRC guidelines from diverse countries, further undertaking methodological and quality evaluations of the encompassed CEA evidence. As a result of screening 11 databases and reviewing 53 guidelines to identify whether and how HEE was used in guidelines, we found that 68 % took cost factors into consideration and 57% integrated health economics studies as evidentiary support. The results are higher than the proportion of guidelines using cost justification reported by the study by Zervou et al. [3]. Zervou et al. [3] reviewed guidelines for different medical areas in the USA and found that a minority of practice guidelines incorporate cost analyses utilizing only 6% of the available cost analyses.
The aim of HEE is to gain as much health as possible for the population, given the available resources. Globally, with the improving recognition of the significance of HEE in health decision-making, the acceptance and application of HEE in CPGs have witnessed a discernible upswing over the past several decades. In 2001, the NHS in England published a methodology on how to develop cost-conscious clinical guidelines, including the development of models and supporting the involvement of health economists in the development of CPG [83]. Methods for ascertaining resource utilization and acquiring cost information are distinctly proposed in the Guidelines 2.0 Checklist [84].
Additionally, the actual implementation of HEE in guidelines continues to develop and remains challenging. The development of guidelines and CEA studies exhibits non-uniformity across countries due to medical advancement, public health policies, healthcare systems and regulatory frameworks. In this study, most guidelines and HEE evidence came from the US, and we found no evidence that France and Spain considered economic factors in their guidelines. American Cancer Society defined cost as one of the values in cancer care, whereas it stated in the guidelines not to apply cost and resource use as a decision-making criterion for recommendations because of widely varying cost [22]. While health interventions with better cost–effectiveness are generally more likely to be accepted, some guidelines still consider clinical evidence exclusively [20]. A guideline from the US offers a view point about refusing HEE that guideline is from a patient-surgeon perspective, not from a population perspective [54]. Wilkinson et al. [2] surveyed the reasons that HEE is not used in CPGs depending on CPG role players, including evidence reviewers and CPG panelists. In this study, uncertainty caused by analysis methods or lack of reliable data are thought to be one possible reason for refusing HEE. Based on the CHEQUE tool, less than 40% of CEA conducted systematic reviews or meta-analyses to choose the best available evidence. Owing to the possible bias of individual clinical studies or epidemiological studies, it is better to conduct systematic reviews of data acquisition.
Moreover, this study found that some CEA were published between 2007 and 2011, meaning they predated the guidelines by more than 5 years. This can be attributed to the long time needed for the collection of evidence, validation of guidelines and consensus of experts regarding the formulated recommendations [3]. In addition, according to the results of this study, guidelines tend to ignore the generalizability of results from a single HEE that varies across regions. As to whether the HEE results are generalizable, the WHO provided a checklist to assess generalizability and transferability for economic evaluation from one developed country to another and suggested taking a revision in developing countries [4,85].
When conducting a CEA, it is recommended to employ the healthcare system and societal perspectives [86,87]. The former is similar to the way considered by health decision-makers; the latter takes resource allocation across a wide range of populations into account. In the study, three CEA considered both the healthcare system and societal perspective [69–71]. In addition, QALY as a generic measure index is widely recognized for providing more comparable results. 62% of the studies used QALY as a measure of health outcome. And it is necessary to disclose financial interests or sources of funding in CEA studies. In one report [3], it was shown that the overall high quality of reporting and the transparency of the funding source, rather than the funding source itself, significantly influenced the adaptation of cost analysis in clinical guidelines.
Although health economics is gradually developing, there are still some insufficient in some fields. ASCO conducted a literature search [54] focusing on systematic reviews of published CEA on low-resource settings for patients with early-stage CRC, and none were found. Another guideline [48] also explicitly states there is no CEA comparing fecal immunochemical tests to colonoscopies for early-onset CRC and emphasizes the need for further investigation due to the absence of sufficiently high-quality data.
A notable element of this study is that we chose the 1990 IOM definition of guidelines as the inclusion criteria to incorporate as many guidelines as feasibly achievable, primarily because the 2011 definition excludes guidelines generated by non-systematic reviews. This study has some limitations that should be noted. First, in the search for CPGs, only Chinese and English guidelines are reviewed, with the analysis of guidelines for countries with languages other than English or Chinese inevitably omitted. The search for guidelines was constrained to those published from 2017 onward, excluding any published earlier. Second, it focused on the content of guidelines, and HEE cited but did not trace whether health economists were included in the guideline expert group and where the skills of the health economist sat within such an enterprise. In future research, incorporating the impact of health policy and the role of health economics experts in the involvement in the decision-making process will provide additional information.
Conclusion
In conclusion, 57% of guidelines incorporated health economics studies as evidence with a significant variation between different nations. Without a well-defined approach to integrating HEE into CPGs, the application of HEE in guidelines remains challenging. Moreover, we found that the methods used in health economics research of the current clinical guidelines still exhibit disparities from recommendations. Therefore, it is suggested that health economics research should use a standardized methodology and reporting approach to assist in clinical decision-making.
Summary points
•
There is no global consensus on whether to incorporate health economics evidence (HEE) into clinical practice guidelines (CPGs). In some guideline development organizations, cost and health economics are not applied to the decision-making criterion for recommendations.
•
We collected CPGs from multiple databases covering the years 2017–2023 and extracted HEE, with a particular focus on analyzing cost–effectiveness analysis (CEA) studies.
•
The consideration of HEE varies across different international and academic associations.
•
HEE contributes to cost-based de-escalation of treatment strategies, reporting the economic burden of the disease and elucidating the health-economic comparative benefits of the intervention.
•
Some CEA were published between 2007 and 2011, meaning they predated the guidelines by more than 5 years, with possible inapplicability of the results.
•
Based on the CHEQUE evaluation tool, the methodological and reporting quality of these CEA studies cited as references demonstrated deficiencies.
•
The source of funding for the CEA itself can also affect quality.
•
HEE can use consistent methodologies and reporting standards to support clinical decision-making.
Author contributions
Authors H Li and X Yan were responsible for the concept and framework of the study. Author X Yan was responsible for the study design, drafting and revision of the manuscript. Authors X Yan and Y Wang were responsible for the acquisition and analysis of data. Authors A Ma and H Li were responsible for revising the manuscript critically. Author H Li was responsible for maintaining communication with the Journal.
Acknowledgments
The authors gratefully acknowledge the contribution of Y Li, China Pharmaceutical University, for valuable suggestions in study design.
Financial disclosure
The authors have no financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
Writing disclosure
No writing assistance was used in the production of this manuscript.
Competing interests disclosure
The authors have no financial and/or nonfinancial competing interests or relevant affiliations with any organization/entity to declare that are relevant to the subject matter or materials discussed in this manuscript. This includes employment, grants or research funding, consultancies, membership on scientific or other advisory boards, honoraria, stock ownership or options, paid expert testimony, patents received or pending, or royalties.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary material.docx)
- Download
- 83.62 KB
References
Papers of special note have been highlighted as: • of interest
1.
Kernick D. An introduction to the basic principles of health economics for those involved in the development and delivery of headache care. Cephalalgia 25(9), 709–714 (2005).
2.
Wilkinson M, Hofman KJ, Young T, Schmidt BM, Kredo T. Health economic evidence in clinical guidelines in South Africa: a mixed-methods study. BMC Health. Serv. Res. 21(1), 738 (2021).
• Employed an online survey of participants in clinical practice guidelines roles, who indicated that complex health economic evaluations could not be effectively considered without enhancing the application skills of evidence-based medical principles.
3.
Zervou FN, Zacharioudakis IM, Pliakos EE, Grigoras CA, Ziakas PD, Mylonakis E. Adaptation of cost analysis studies in practice guidelines. Medicine (Baltimore) 94(52), e2365 (2015).
• Analyzed 100 guidelines in the USA and found that 57% did not have cost considerations.
4.
Edejer TT. Improving the use of research evidence in guideline development: 11. Incorporating considerations of cost–effectiveness, affordability and resource implications. Health Res. Policy Syst. 4(23), 1–6 (2006).
5.
National Institute for Health and Care Excellence. Social value judgements: principles for the development of NICE guidance (Version 2). NICE. (2008). https://www.ncbi.nlm.nih.gov/books/NBK395865/
6.
Schnipper LE, Davidson NE, Wollins DS et al. American Society of Clinical Oncology statement: a conceptual framework to assess the value of cancer treatment options. J. Clin. Oncol. 33(23), 2563–2577 (2015).
7.
Committee to Advise the Public Health Service on Clinical Practice Guidelines, Institute of Medicine (US). Clinical practice guidelines: directions for a new program. National Academies Press, DC, USA (1990). Available from: https://www.ncbi.nlm.nih.gov/books/NBK235751/
• Describes the clinical practice guidelines definitions.
8.
Committee on Standards for Developing Trustworthy Clinical Practice Guidelines, Institute of Medicine (US). Clinical practice guidelines we can trust. National Academies Press, DC, USA (2011). Available from: https://nap.nationalacademies.org/catalog/1626/clinical-practice-guidelines-directions-for-a-new-program
9.
Haller MC, Vanholder R, Oberbauer R, Zoccali C, Van Biesen W. Health economics and European Renal Best Practice–is it time to bring health economics into evidence-based guideline production in Europe? Nephrol. Dial. Transplant. 29(11), 1994–1997 (2014).
10.
Sung H, Ferlay J, Siegel RL et al. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 71(3), 209–249 (2021).
11.
Dekker E, Tanis PJ, Vleugels JLA, Kasi PM, Wallace MB. Colorectal cancer. Lancet 394(10207), 1467–1480 (2019).
12.
Keum N, Giovannucci E. Global burden of colorectal cancer: emerging trends, risk factors and prevention strategies. Nat. Rev. Gastroenterol. Hepatol. 16(12), 713–732 (2019).
13.
Wang H, Cao MD, Liu CC et al. Disease burden of colorectal cancer in China: any changes in recent years? Chinese J. Epidemiology 41(10), 1633–1642 (2020).
14.
Kim DD, Do LA, Synnott PG et al. Developing criteria for health economic quality evaluation tool. Value Health 26(8), 1225–1234 (2023).
15.
Sepulveda AR, Hamilton SR, Allegra CJ et al. Molecular biomarkers for the evaluation of colorectal cancer: guideline from the American Society for Clinical Pathology, College of American Pathologists, Association for Molecular Pathology, and American Society of Clinical Oncology. Am. J. Clin. Pathol. 147(3), 221–260 (2017).
16.
Lieu C, Kennedy EB, Bergsland E et al. Duration of oxaliplatin-containing adjuvant therapy for stage III colon cancer: ASCO clinical practice guideline. J. Clin. Oncol. 37(16), 1436–1447 (2019).
17.
Chiorean EG, Nandakumar G, Fadelu T et al. Treatment of patients with late-stage colorectal cancer: ASCO resource-stratified guideline. JCO. Glob. Oncol. 6, 414–438 (2020).
18.
Lopes G, Stern MC, Temin S et al. Early detection for colorectal cancer: ASCO resource-stratified guideline. J. Glob. Oncol. 5, 1–22 (2019).
19.
Costas-Chavarri A, Temin S, Shah MA. Treatment of patients with early-stage colorectal cancer: ASCO resource-stratified guideline summary. J. Oncol. Pract. 15(5), 290–292 (2019).
20.
Baxter NN, Kennedy EB, Bergsland E et al. Adjuvant therapy for stage II colon cancer: ASCO guideline update. J. Clin. Oncol. 40(8), 892–910 (2022).
21.
Morris VK, Kennedy EB, Baxter NN et al. Treatment of metastatic colorectal cancer: ASCO guideline. J. Clin. Oncol. 41(3), 678–700 (2023).
22.
Wolf AMD, Fontham ETH, Church TR et al. Colorectal cancer screening for average-risk adults: 2018 guideline update from the American Cancer Society. CA Cancer J. Clin. 68(4), 250–281 (2018).
23.
National Comprehensive Cancer Network (NCCN). NCCN Clinical Practice Guidelines in Oncology: Colorectal Cancer Screening (Version 2). NCCN. (2023). https://www.nccn.org/guidelines/guidelines-detail?category=1&id=1429
24.
National Comprehensive Cancer Network (NCCN). NCCN Clinical Practice Guidelines in Oncology: Colon Cancer (Version 3). NCCN. (2023). https://www.nccn.org/guidelines/guidelines-detail?category=1&id=1428
25.
National Comprehensive Cancer Network (NCCN). NCCN Clinical Practice Guidelines in Oncology: Rectal Cancer (Version 2). NCCN. (2023). https://www.nccn.org/guidelines/guidelines-detail?category=1&id=1461
26.
Hardiman KM, Felder SI, Friedman G et al. The American Society of Colon and Rectal Surgeons clinical practice guidelines for the surveillance and survivorship care of patients after curative treatment of colon and rectal cancer. Dis. Colon Rectum 64(5), 517–533 (2021).
27.
Vogel JD, Felder SI, Bhama AR et al. The American Society of Colon and Rectal Surgeons clinical practice guidelines for the management of colon cancer. Dis. Colon Rectum 65(2), 148–177 (2022).
28.
Herzig DO, Buie WD, Weiser MR et al. Clinical practice guidelines for the surgical treatment of patients with Lynch syndrome. Dis. Colon Rectum 60(2), 137–143 (2017).
29.
You YN, Hardiman KM, Bafford A et al. The American Society of Colon and Rectal Surgeons clinical practice guidelines for the management of rectal cancer. Dis. Colon Rectum 63(9), 1191–1222 (2020).
30.
Shaukat A, Kahi CJ, Burke CA et al. ACG clinical guidelines: colorectal cancer screening 2021. Am. J. Gastroenterol. 116(3), 458–479 (2021).
31.
National Institute for Health and Care Excellence (NICE). Colorectal cancer (NG151): diagnosis and management. NICE. (2020). https://www.nice.org.uk/guidance/ng151
32.
Monahan KJ, Bradshaw N, Dolwani S et al. Guidelines for the management of hereditary colorectal cancer from the British Society of Gastroenterology (BSG)/Association of Coloproctology of Great Britain and Ireland (ACPGBI)/United Kingdom Cancer Genetics Group (UKCGG). Gut 69(3), 411–444 (2020).
33.
Monahan KJ, Davies MM, Abulafi M et al. Faecal immunochemical testing (FIT) in patients with signs or symptoms of suspected colorectal cancer (CRC): a joint guideline from the Association of Coloproctology of Great Britain and Ireland (ACPGBI) and the British Society of Gastroenterology (BSG). Gut 71(10), 1939–1962 (2022).
34.
Alberta Health Services. Integrating an early palliative approach into advanced colorectal cancer care (Version 2). Alberta Health Services. (2020). http://www.ahs.ca/guru
35.
Alberta Health Services. Colorectal Cancer Surveillance (Stages I, II, and III) (Version 7). Alberta Health Services. (2019). http://www.ahs.ca/guru
36.
Kennedy E, Zwaal C, Asmis T et al. An evidence-based guideline for surveillance of patients after curative treatment for colon and rectal cancer. Curr. Oncol. 29(2), 724–740 (2022).
37.
Leddin D, Lieberman DA, Tse F et al. Clinical practice guideline on screening for colorectal cancer in individuals with a family history of nonhereditary colorectal cancer or adenoma: the Canadian Association of Gastroenterology Banff Consensus. Gastroenterology 155(5), 1325–1347.e3 (2018).
38.
Vogl TJ, Pereira PL, Helmberger T et al. Updated S3 guidelines-diagnosis and treatment of colorectal carcinoma: relevance for radiological diagnosis and intervention. Rofo. 191(4), 298–310 (2019).
39.
Salvatore L, Imperatori M, Arnoldi E et al. Management of patients with early-stage colon cancer: guidelines of the Italian Medical Oncology Association. ESMO Open 5(6), e001001 (2020).
40.
Hashiguchi Y, Muro K, Saito Y et al. Japanese Society for Cancer of the Colon and Rectum (JSCCR) guidelines 2019 for the treatment of colorectal cancer. Int. J. Clin. Oncol. 25, 1–42 (2020).
41.
Tomita N, Ishida H, Tanakaya K et al. Japanese Society for Cancer of the Colon and Rectum (JSCCR) guidelines 2020 for the clinical practice of hereditary colorectal cancer. Int. J. Clin. Oncol. 26(8), 1353–1419 (2021).
42.
Ministry of Health Malaysia, Malaysian Society of Colorectal Surgeons, Malaysian Society of Gastroenterology & Hepatology, et al. Management of colorectal carcinoma. Malaysia Health Technology Assessment Section (MaHTAS), Putrajaya, Malaysia (2017). https://guidelines.ebmportal.com/management-colorectal-carcinoma
43.
Chan FKL, Wong MCS, Chan AT et al. Joint Asian Pacific Association of Gastroenterology (APAGE)-Asian Pacific Society of Digestive Endoscopy (APSDE) clinical practice guidelines on the use of non-invasive biomarkers for diagnosis of colorectal neoplasia. Gut 72(7), 1240–1254 (2023).
44.
Cancer Council Australia. Clinical Practice Guidelines for the Prevention, Early detection, and management of colorectal cancer. Cancer Council Australia. (2018). https://www.cancer.org.au/clinical-guidelines/bowel-cancer/colorectal-cancer
45.
Hassan C, Wysocki PT, Fuccio L et al. Endoscopic surveillance after surgical or endoscopic resection for colorectal cancer: European Society of Gastrointestinal Endoscopy (ESGE) and European Society of Digestive Oncology (ESDO) Guideline. Endoscopy 51(3), 266–277 (2019).
46.
Bisschops R, East JE, Hassan C et al. Advanced imaging for detection and differentiation of colorectal neoplasia: European Society of Gastrointestinal Endoscopy (ESGE) Guideline-Update 2019. Endoscopy 51(12), 1155–1179 (2019).
47.
van Leerdam ME, Roos VH, van Hooft JE et al. Endoscopic management of Lynch syndrome and of familial risk of colorectal cancer: European Society of Gastrointestinal Endoscopy (ESGE) Guideline. Endoscopy 51(11), 1082–1093 (2019).
48.
Cavestro GM, Mannucci A, Balaguer F et al. Delphi initiative for early-onset colorectal cancer (DIRECt) international management guidelines. Clin. Gastroenterol. Hepatol. 21(3), 581–603.e33 (2023).
49.
China Guideline for the Screening. Early Detection and Early Treatment of Colorectal Cancer (2020, Beijing). Chinese J. Oncol. 43(1), 16–38 (2021).
50.
Chinese Society of Colorectal Surgery, Chinese Society of Surgery, Chinese Medical Association et al. Guideline for medical imaging clinical appropriateness in patients with colorectal cancer (2021 Edition). Chinese J. Prac. Surg. 41(10), 1104–1110 (2021).
51.
Chinese College of Surgeons, Section of Gastrointestinal Surgery, Branch of Surgery et al. China guideline for diagnosis and comprehensive treatment of colorectal liver metastases (version 2023). J. Digestive Oncol. 15(2), 86–99 (2023).
52.
Kennedy E, Zwaal C, Asmis T et al. Follow-up care, surveillance protocol, and secondary prevention measures for survivors of colorectal cancer (Version 3). Ontario Health. (2021). https://guidelines.ebmportal.com/follow-care-surveillance-protocols-and-secondary-prevention-measures-survivors-colorectal-cancer
53.
Society for Minimally Invasive Surgery. Chinese Research Hospital Association, Technical guidelines for simultaneous laparoscopic and robotic resection of colorectal cancer with liver metastasis (Revised in 2017). J. Clin. Hepatol. 34(3), 494–497 (2018).
54.
Vreeland TJ, Collings AT, Ozair A et al. SAGES/AHPBA guidelines for the use of minimally invasive surgery for the surgical treatment of colorectal liver metastases (CRLM). Surg. Endosc. 37(4), 2508–2516 (2023).
• Provides an explanation for the exclusion of cost considerations, with reference to the specific populations it aims to serve.
55.
Gastrointestinal Cancer Disease Site Group. Adjuvant systemic chemotherapy for stages II and III colon cancer after complete resection. Ontario. (2019). https://www.cancercareontario.ca/en/guidelines-advice/types-of-cancer/231
56.
Alberta Health Services. Rectal cancer. Alberta Health Services. (2021). http://www.ahs.ca/guru
57.
Alberta Health Services. Metastatic colorectal cancer (Version 13). Alberta Health Services. (2023). http://www.ahs.ca/guru
58.
Biagi J, Cosby S, Wong R. Hepatic arterial infusion for colorectal liver metastases. Ontario Health. (2020). https://guidelines.ebmportal.com/hepatic-arterial-infusion-colorectal-liver-metastases
59.
Phelip JM, Tougeron D, Léonard D et al. Metastatic colorectal cancer (mCRC): french intergroup clinical practice guidelines for diagnosis, treatments and follow-up (SNFGE, FFCD, GERCOR, UNICANCER, SFCD, SFED, SFRO, SFR). Dig. Liver Dis. 51(10), 1357–1363 (2019).
60.
Aparicio T, Canouï-Poitrine F, Caillet P et al. Treatment guidelines of metastatic colorectal cancer in older patients from the French Society of Geriatric Oncology (SoFOG). Dig. Liver Dis. 52(5), 493–505 (2020).
61.
Cubiella J, Marzo-Castillejo M, Mascort-Roca JJ et al. Clinical practice guideline. Diagnosis and prevention of colorectal cancer. 2018 Update. Gastroenterol. Hepatol. 41(9), 585–596 (2018).
62.
Capdevila J, Gómez MA, Guillot M et al. SEOM-GEMCAD-TTD clinical guidelines for localized rectal cancer (2021). Clin. Transl. Oncol. 24(4), 646–657 (2022).
63.
Yoshino T, Argilés G, Oki E et al. Pan-Asian adapted ESMO Clinical Practice Guidelines for the diagnosis treatment and follow-up of patients with localised colon cancer. Ann. Oncol. 32(12), 1496–1510 (2021).
64.
Yoshino T, Arnold D, Taniguchi H et al. Pan-Asian adapted ESMO consensus guidelines for the management of patients with metastatic colorectal cancer: a JSMO-ESMO initiative endorsed by CSCO, KACO, MOS, SSO and TOS. Ann. Oncol. 29(1), 44–70 (2018).
65.
Argilés G, Tabernero J, Labianca R et al. Localised colon cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 31(10), 1291–1305 (2020).
66.
Cervantes A, Adam R, Roselló S et al. Metastatic colorectal cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann. Oncol. 34(1), 10–32 (2023).
67.
Zhang Z, Zheng M, Yao H et al. Expert consensus and surgical operation guidelines for transanal total mesorectal excision of rectal cancer (2017 version). Chinese J. Prac. Surg. 37(9), 978–984 (2017).
68.
Garrison LP Jr. Cost–effectiveness and clinical practice guidelines: have we reached a tipping point? An overview. Value Health 19(5), 512–515 (2016).
69.
Hoyle M, Crathorne L, Peters J et al. The clinical effectiveness and cost–effectiveness of cetuximab (mono- or combination chemotherapy), bevacizumab (combination with non-oxaliplatin chemotherapy) and panitumumab (monotherapy) for the treatment of metastatic colorectal cancer after first-line chemotherapy (review of technology appraisal No.150 and part review of technology appraisal No. 118): a systematic review and economic model. Health Technol. Assess 17(14), (2013).
70.
Robles-Zurita J, Boyd KA, Briggs AH, Iveson T, Kerr RS, Saunders MP et al. SCOT: a comparison of cost–effectiveness from a large randomised phase III trial of two durations of adjuvant Oxaliplatin combination chemotherapy for colorectal cancer. Br. J. Cancer 119(11), 1332–1338 (2018).
71.
Lué A, Hijos G, Sostres C, Perales A, Navarro M, Barra MV et al. The combination of quantitative faecal occult blood test and faecal calprotectin is a cost-effective strategy to avoid colonoscopies in symptomatic patients without relevant pathology. Therap. Adv. Gastroenterol. 13, 1320575954 (2020).
72.
Tappenden P, Jones R, Paisley S, Carroll C. Systematic review and economic evaluation of bevacizumab and cetuximab for the treatment of metastatic colorectal cancer. Health Technol. Assess 11(12), 1-iv (2007).
73.
Graham CN, Christodoulopoulou A, Knox HN, Sabatelli L, Hechmati G, Garawin T et al. A within-trial cost–effectiveness analysis of panitumumab compared with bevacizumab in the first-line treatment of patients with wild-type RAS metastatic colorectal cancer in the US. J. Med. Econ. 21(11), 1075–1083 (2018).
74.
Augestad KM, Norum J, Dehof S et al. Cost–effectiveness and quality of life in surgeon versus general practitioner-organised colon cancer surveillance: a randomised controlled trial. BMJ Open 3(4), e2391 (2013).
75.
Mant D, Gray A, Pugh S, Campbell H, George S, Fuller A et al. A randomised controlled trial to assess the cost–effectiveness of intensive versus no scheduled follow-up in patients who have undergone resection for colorectal cancer with curative intent. Health Technol. Assess 21(32), 1–86 (2017).
76.
Davari M, Ashrafi F, Maracy M, Aslani A, Tabatabaei M. Cost–effectiveness analysis of cetuximab in treatment of metastatic colorectal cancer in Iranian Pharmaceutical Market. Int. J. Prev. Med. 6, 63 (2015).
77.
Burm R, Thewes B, Rodwell L, Kievit W, Speckens A, van de Wal M et al. Long-term efficacy and cost–effectiveness of blended cognitive behavior therapy for high fear of recurrence in breast, prostate and colorectal cancer survivors: follow-up of the SWORD randomized controlled trial. BMC Cancer 19(1), 462 (2019).
78.
Lairson DR, DiCarlo M, Deshmuk AA, Fagan HB, Sifri R, Katurakes N et al. Cost–effectiveness of a standard intervention versus a navigated intervention on colorectal cancer screening use in primary care. Cancer 120(7), 1042–1049 (2014).
79.
van Hees F, Saini SD, Lansdorp-Vogelaar I, Vijan S, Meester RGS, de Koning HJ et al. Personalizing colonoscopy screening for elderly individuals based on screening history, cancer risk, and comorbidity status could increase cost effectiveness. Gastroenterlogy 149(6), 1425–1437 (2015).
80.
Naber SK, Knudsen AB, Zauber AG, Rutter CM, Fischer SE, Pabiniak CJ et al. Cost–effectiveness of a multitarget stool DNA test for colorectal cancer screening of Medicare beneficiaries. PLoS ONE 14(9), e220234 (2019).
81.
Goede SL, van Roon AHC, Reijerink JCIY et al. Cost–effectiveness of one versus two sample faecal immunochemical testing for colorectal cancer screening. Gut 62(5), 727–734 (2013).
82.
Lew JB, St John DJB, Macrae FA, Emery JD, Ee HC, Jenkins MA et al. Evaluation of the benefits, harms and cost? Effectiveness of potential alternatives to iFOBT testing for colorectal cancer screening in Australia. Int. J. Cancer 143(2), 269–282 (2018).
83.
Schünemann HJ, Wiercioch W, Etxeandia I et al. Guidelines 2.0: systematic development of a comprehensive checklist for a successful guideline enterprise. Can. Med. Assoc. J. 186(3), E123–E142 (2014).
84.
Boulenger S, Nixon J, Drummond M et al. Can economic evaluations be made more transferable? Eur. J. Health Econ. 6(4), 334–346 (2015).
• Assesses the transferability and applicability of economic evaluations.
85.
Sanders GD, Neumann PJ, Basu A et al. Recommendations for conduct, methodological practices, and reporting of cost–effectiveness analyses: second panel on cost–effectiveness in health and medicine. J. Am. Med. Assoc. 316(10), 1093–1103 (2016).
• Recommendations on how to conduct cost–effectiveness analysis studies.
86.
Neumann PJ, Sanders GD. Cost–effectiveness analysis 2.0. N. Engl. J. Med. 376(3), 203–205 (2017).
87.
Silva-Illanes N, Espinoza M. Critical analysis of Markov models used for the economic evaluation of colorectal cancer screening: a systematic review. Value Health 21(7), 858–873 (2018).
Information & Authors
Information
Published In
Copyright
© 2025 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 1 December 2024
Accepted: 31 January 2025
Published online: 19 February 2025
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
The role of health economic evidence in clinical practice guidelines for colorectal cancer: a comparative analysis across countries. (2025) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2024-0226
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Anand R. Habib, Omar Qureshi, Reshma Ramachandran, Joseph S. Ross, Economic and Resource Use–Related Guidance in US Medical Societies’ Clinical Practice Guidelines, JAMA Network Open, 10.1001/jamanetworkopen.2026.20297, 9, 6, (e2620297), (2026).