Evaluation of reporting in time-driven activity-based costing studies on cardiovascular diseases: a scoping review
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: This scoping review evaluates the application of the time-driven activity-based costing (TDABC) methodology in cardiovascular disease (CVD) studies. Materials & methods: The evaluation was conducted using the 32-item TDABC Healthcare Consortium Consensus Statement Checklist. A systematic search was performed in Medline, Embase and Scopus in September 2023, including only full-text, peer-reviewed studies reporting the application of TDABC in CVD research. Results: Twenty studies were included in the review. The positive response rate for individual studies ranged from 31 to 81%. The most frequently addressed checklist item was the clear definition of study objectives, while presenting costs per patient included in the analysis was the least reported item. Although 70% of the studies achieved a positive response rate above 50%, adherence to the TDABC checklist remains inconsistent. Conclusion: There is significant room for improvement in the reporting of TDABC methodology in CVD studies. Providing a more comprehensive and standardized description of the methodology would enhance the utility, reproducibility and accuracy of the information generated, supporting the development of evidence-based health policies and improving accountability in healthcare cost assessments.
Healthcare expenditure and affordability are critical concerns for health systems worldwide [1–3]. In the USA, the sector spending is expected to increase two to fourfold by 2050 [4,5]. Demographic and epidemiologic shifts characterized by aging populations, have made noncommunicable diseases led by cardiovascular diseases (CVD) – the leading cause of mortality and a major driver of disability and costs globally [4,6,7]. CVD accounts for 51% of the noncommunicable diseases costs and approximately 4% of the gross domestic product in low- and middle-income countries, with comparable budgetary impacts projected for high-income countries [4,8–10].
In this context, accurately measuring costs for health technologies during the incorporation process and throughout the care cycle is crucial [1,2,11,12]. Time-driven activity-based costing (TDABC) is a microcosting assessment method that enhances data accuracy by accounting for direct and indirect costs based on patient-specific resource use throughout the care pathway. The TDABC framework evaluates the length of time and the volume of each resource required to perform a specific activity along the care pathway, and estimates the cost per activity and resource consumed. By achieving this level of cost information granularity, TDABC methodology enhances the accuracy of cost information and enables managers to quantify costs, assess resource utilization and identify opportunities to reduce waste and increase value in healthcare [13,14].
To support the development and reporting of studies using TDABC, while maximizing the utility of the methodology and ensuring transparency, the TDABC in Healthcare Consortium proposed a standardized framework in 2020. This framework was presented as a checklist comprising 32 questions, addressing how researchers measure time variables, account for resources in the care pathway and calculate cost estimates. TDABC in Healthcare Consortium Consensus Statement Checklist was developed based on prior literature regarding microcosting studies, a focus group process to create the preliminary checklist, and validation with researchers from multiple countries with expertise in costing studies and TDABC. The checklist elements are categorized as ‘Mandatory’ and ‘Strongly suggested, but not mandatory’, with guidance on the appropriate paper sections for including each element [15].
As the body of literature on TDABC has grown in recent years, including studies focused on CVD [16], a critical assessment of these studies is necessary to examine variations in the implementation and reporting of TDABC methodologies and to identify common limitations. This scoping review aimed to systematically identify CVD studies utilizing TDABC to evaluate healthcare costs and assess the credibility of its application by using the TDABC Checklist.
Materials & methods
The scoping review was conducted following the Joanna Briggs Institute methodology [17]. The reporting of the methodology was structured in compliance with The Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for scoping reviews (Supplementary Table 1). The research question was: “How are studies on CVD using the TDABC methodology for cost analysis being reported?”. A previous protocol of this scoping review was not registered.
Eligibility criteria
Only full-text peer-reviewed studies reporting the application of TDABC on CVD (considering any intervention and process of care related to CVD) were considered eligible. Conference abstracts, reviews, opinions and letters were excluded. There was no limit regarding the date when the study was published nor restriction regarding the language for study selection.
Search strategy
Searches were performed on the following electronic databases: Medline (via PubMed), Embase and Scopus, for registers available until 4 September 2023. The search strategy included terms for TDABC and the cardiology field, using controlled vocabulary and free terms, adapted for each database. The full search strategy is available at Supplementary Table 2.
Study selection & data extraction
All registers identified in the searches were pooled in a reference manager software (EndNote 20) and duplicate records were removed [18]. The remaining records were exported and included on Rayyan, a web-based software for systematic reviews management, where the selection of titles and abstracts was performed [19]. Full-text records of potentially eligible and uncertain studies identified in this stage were retrieved for the final assessment. All the selection process was performed by two reviewers and doubts about the eligibility of studies were discussed with a third reviewer.
For the included studies, a data extraction formulary was applied by one reviewer to retrieve information about the characterization of each study, the intervention/process being assessed, and the patients included.
Assessment of reporting & analysis
We evaluated the alignment of each study with the 32 questions from the TDABC in Healthcare Consortium Consensus Statement Checklist [15]. This evaluation was conducted by one researcher and independently verified by a second reviewer. Each question was categorized as ‘Yes’, ‘No’, ‘Not applicable (NA)’, or ‘Not informed (NI)’ (Supplementary Table 3). In cases of disagreement, a third reviewer was consulted to reach a consensus.
The positive response rate was calculated for each study (the number of questions marked as ‘Yes’ divided by the total number of questions) and for each question (the number of studies with a ‘Yes’ response divided by the total number of included studies). Additionally, the median positive response rate and interquartile range (IQR) were estimated for both metrics.
Results
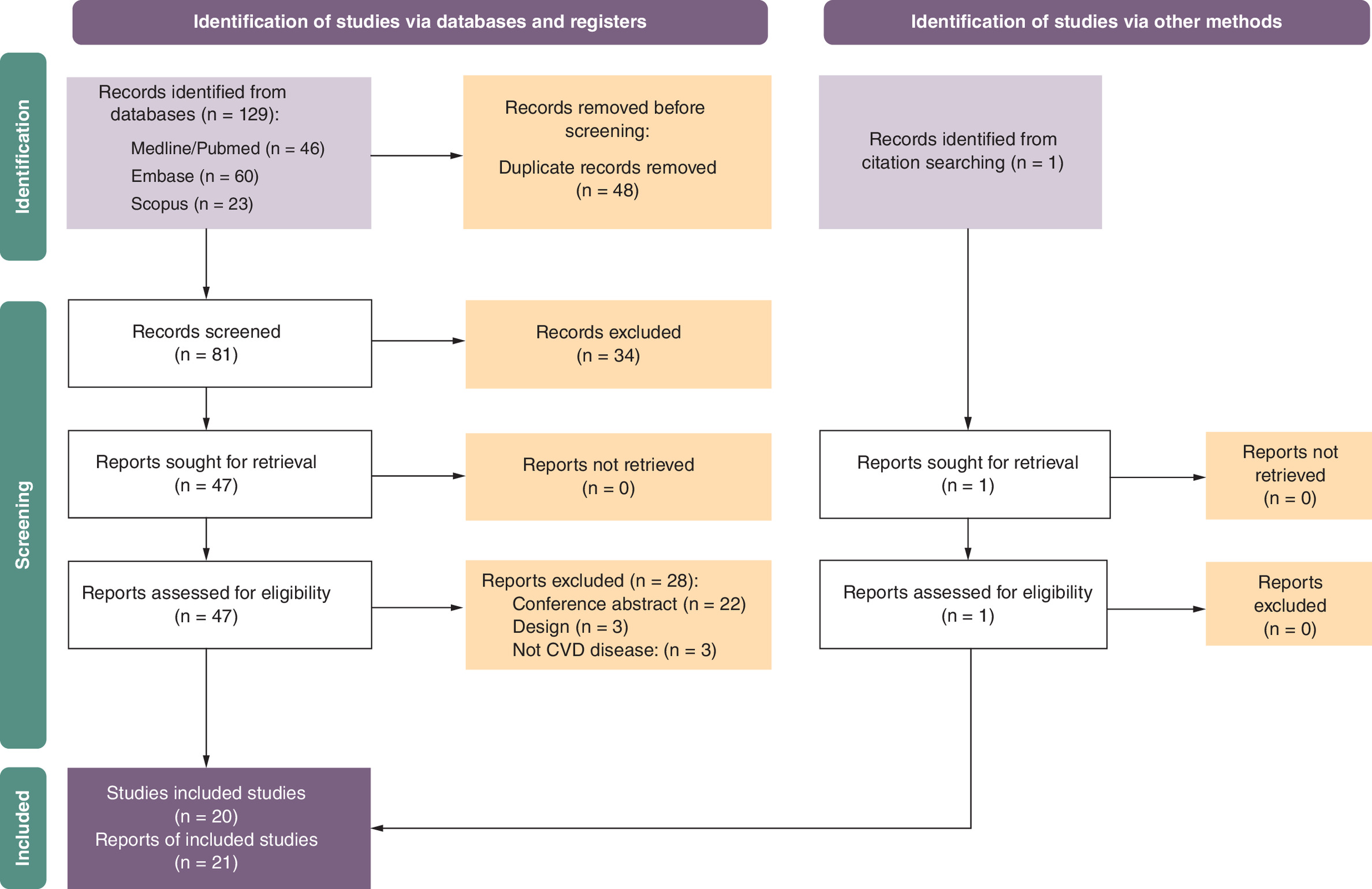
A total of 129 studies were identified through electronic searches. After removing duplicates, 81 studies were screened, and 47 were retrieved for full-text assessment. Following the selection process, 20 studies described across 21 publications were included in this review [20–40]. The detailed selection process is illustrated in Figure 1.
The characteristics of the included studies and their positive response rates are summarized in Table 1. The studies were published between 2014 and 2023 and were conducted across eight countries: the USA, India, Brazil, Germany, Uganda, Italy, France and Sweden. Most studies (n = 12) were conducted entirely or partially in the USA. Sample sizes ranged from 1 to 5526 patients, with four studies not reporting sample sizes. The conditions assessed included examinations, pharmacological treatments, telehealth services and surgical interventions for various cardiovascular conditions. The TDABC methodology was most frequently applied in hospital settings (75% of the studies) to evaluate the costs of clinical management (n = 9), surgery (n = 4) or interventional procedures (n = 4).
| Study | Publication year | Title | Country | Object of assessment | Type of healthcare | Setting | Sample size | Positive response rate All questions (mandatory questions) | Ref. |
|---|---|---|---|---|---|---|---|---|---|
| Donavan et al. | 2014 | How Cleveland clinic used TDABC to improve value | USA | Mitral valve repair, aortic valve replacement | Surgery | Hospital | NI | 41% (41%) | [20] |
| Tabit et al. | 2017 | Cardiology consultation in the Emergency Department reduces re-hospitalizations for low-socioeconomic patients with acute decompensated heart failure | USA | Guideline-directed education and intensive outpatient follow-up and early consultation with cardiologist in the Emergency Department for low-socioeconomic urban patients with acute decompensated heart failure | Clinical management | Ambulatory | 784 | 31% (27%) | [21]† |
| Chong-Yik et al. | 2018 | Cost-saving opportunities with appropriate utilization of cardiac telemetry | USA | Cardiac telemetry | Diagnosis | Hospital | 250 | 38% (36%) | [22] |
| Goldraich et al. | 2018 | Heart transplantation cost composition in Brazil: a patient level microcosting analysis and comparison with international data | Brazil | Adult patients undergoing heart transplantation | Surgery | Hospital | 27 | 38% (45%) | [23] |
| Martin et al. | 2018 | Using time-driven activity-based costing as a key component of the value platform: a pilot analysis of colonoscopy, aortic valve replacement and carpal tunnel release procedures | USA | Surgical vs. transcatheter approach for aortic valve replacement (anesthesiologist perspective) | Surgery | Hospital | NI | 63% (68%) | [24] |
| Bobade et al. | 2019 | Time-driven activity-based cost analysis for outpatient anticoagulation therapy: direct costs in a primary care setting with optimal performance | USA | Anticoagulation therapy for warfarin compared with novel oral anticoagulants | Clinical management | Ambulatory | 5526 | 34% (27%) | [25] |
| Collins et al. | 2020 | Subarachnoid hemorrhage ‘fast track’: a health economics and healthcare redesign approach for early selected hospital discharge | USA | Earlier discharge (i.e., fast track) in selected patients with subarachnoid hemorrhage compared with other patients with subarachnoid hemorrhage | Clinical management | Hospital | 200 | 69% (82%) | [26] |
| Erhun et al. | 2020 | Are cost advantages from a modern Indian hospital transferable to the USA? | USA/India | First, nonurgent, isolated and multivessel coronary artery bypass graft surgeries | Surgery | Hospital | NI | 72% (73%) | [27,28]‡ |
| Ho et al. | 2020 | Cardiovascular 3D printing: value-added assessment using time-driven activity-based costing | USA | Cardiovascular 3D printing workflow | Material | 1 | 66% (68%) | [29] | |
| Keel et al. | 2020 | Time-driven activity-based costing for patients with multiple chronic conditions: a mixed-method study to cost care in a multidisciplinary and integrated care delivery center at a university-affiliated tertiary teaching hospital in Stockholm, Sweden | Sweden | Outpatient clinical care processes for patients with at least three chronic conditions: established diabetes, cardiovascular disease and kidney disease | Clinical management | Ambulatory | 314 | 78% (86%) | [30] |
| DeWyer et al. | 2021 | Establishment of a cardiac telehealth program to support cardiovascular diagnosis and care in a remote, resource-poor setting in Uganda | Uganda | Cardiac telehealth program | Clinical management | Ambulatory | 1324 | 63% (64%) | [31] |
| Etges et al. | 2021 | Time-driven activity-based costing as a strategy to increase efficiency: an analyses of interventional coronary procedures | Brazil | Elective interventional coronary procedures | Interventional procedure | Hospital | 90 | 66% (73%) | [32] |
| Masthoff et al. | 2021 | Value improvement by assessing IR care via time-driven activity-based costing | Germany | Interventional radiology for image-guided vascular malformation treatment | Interventional procedure | Hospital | 78 | 63% (77%) | [33] |
| Zimmerman et al. | 2021 | The direct costs of coronary CT angiography relative to contrast-enhanced thoracic CT: time-driven activity-based costing | USA | Coronary CT angiography and contrast-enhanced thoracic CT as a diagnostic test for assessing coronary artery disease. | Diagnosis | Ambulatory | 54 | 56% (64%) | [34] |
| Kumar et al. | 2022 | Cost analysis of treating cardiovascular diseases in a superspecialty hospital | India | Cardiovascular diseases such as coronary artery disease, rheumatic heart disease, cardiomyopathy, congenital heart diseases and cardiac arrhythmias, etc. | Clinical management | Hospital | 100 | 31% (32%) | [35] |
| Etges et al. | 2022 | Moving the Brazilian ischemic stroke pathway to a value-based care: introduction of a risk-adjusted cost estimate model for stroke treatment | Brazil | Ischemic stroke | Clinical management | Hospital | 822 | 75% (77%) | [36] |
| Morrow et al. | 2023 | Determining the marginal cost differences of a telehealth versus an in-person occupational therapy evaluation session for stroke survivors Using time-driven activity-based costing | USA | Stroke rehabilitation | Clinical management | Hospital | 19 | 72% (73%) | [37] |
| Nurok et al. | 2022 | It is Not just the prices: time-driven activity-based costing for initiation of veno-venous extracorporeal membrane oxygenation at Three international sites—a case review | USA/France/Australia | Veno-venous extracorporeal membrane oxygenation | Interventional procedure | Hospital | NI | 56% (55%) | [38] |
| Wei et al. | 2022 | Cost of cardiac stereotactic body radioablation therapy vs catheter ablation for treatment of ventricular tachycardia | USA | Ventricular tachycardia | Interventional procedure | Hospital | 69 | 81% (82%) | [39] |
| Rognoni et al. | 2023 | Time-driven activity-based costing for capturing the complexity of healthcare processes: the case of deep vein thrombosis and leg ulcers | Italy | Venous ulcer management | Clinical management | Hospital | 88 | 63% (64%) | [40] |
†
Study included by cross-evaluation of conference abstract by the same authors.
‡
Included the published study protocol to complement assessment.
CT: Computed tomography; NI: Not informed; TDABC: Time-driven activity-based costing.
The positive response rate for each study ranged from 31 to 81%, with a median rate of 63% (IQR: 40–70%). Most studies (70%) have a positive rate greater than 50%. The positive rates for both mandatory and nonmandatory questions were similar across all manuscripts (Table 1). The median positive response rate per question was 65% (IQR: 34–80%) (Table 2), with the detailed response rate of each question presented in Table 2. Among the mandatory questions, the positive response rate among the included studies ranged from 5% (question 7.2) to 95% (question 3.2). For the nonmandatory questions, the positive response rate varied from 15% (question 7.6) to 100% (question 1.1).
| TDABC elements | Yes (%) | No (%) | NI (%) | NA (%) |
|---|---|---|---|---|
| 1.1 It is defined if the results are being explored for general health service management or redesign and value or only to assess costs? | 100.00% | 0.00% | 0.00% | 0.00% |
| 1.2 Is the clinical pathway, technology or procedure studied justified because of an interest from government, hospital, society or a health technology assessment analysis? | 85.00% | 15.00% | 0.00% | 0.00% |
| 1.3 Are study limitations being presented? | 85.00% | 15.00% | 0.00% | 0.00% |
| 1.4 Is the TDABC method selection being justified? | 90.00% | 10.00% | 0.00% | 0.00% |
| 2.1 Are authors using specific methodologies to design the care pathway? | 75.00% | 25.00% | 0.00% | 0.00% |
| 2.2 Are authors using a multidisciplinary team to apply the TDABC? (design the process, correctly consider clinical characteristics, correctly evaluate costs) | 80.00% | 0.00% | 20.00% | 0.00% |
| 2.3 Are authors reporting activities in the process map on a macro level? | 85.00% | 15.00% | 0.00% | 0.00% |
| 2.4 Are authors reporting activities in the process map on a micro level? | 30.00% | 0.00% | 0.00% | 0.00% |
| 2.5 Is the full process map (or a part of) being presented in a picture or graphic display? | 80.00% | 20.00% | 0.00% | 0.00% |
| 3.1 Is a table or a map being presented to illustrate the association between activities and resources? | 70.00% | 30.00% | 0.00% | 0.00% |
| 3.2 Are the resources that are included in the analysis being defined and justified? | 95.00% | 5.00% | 0.00% | 0.00% |
| 3.3 Are authors reporting observation in situ approach to better identify resources used in each activity? | 55.00% | 45.00% | 0.00% | 0.00% |
| 3.4 Are the authors interviewing the professionals to better identify resources used in each activity? | 70.00% | 10.00% | 20.00% | 0.00% |
| 4.1 When using hospital financial database, it is being stated how those data were collected and analyzed? | 65.00% | 25.00% | 0.00% | 10.00% |
| 4.2 Are authors defining the currency and applying discount taxes when it is necessary? | 60.00% | 40.00% | 0.00% | 0.00% |
| 4.3 When using external financial databases, is there a description of the database and how those data were accessed? | 25.00% | 15.00% | 0.00% | 60.00% |
| 4.4 When mixed financial databases are being used (for example, salaries from external reference and structural costs from the hospital) is the origin of each data variable being stated? | 40.00% | 15.00% | 0.00% | 45.00% |
| 4.5 Did the authors explaining how the overhead costs are being considered? | 70.00% | 30.00% | 0.00% | 0.00% |
| 5.1 Are authors defining if the capacity data used represents the total capacity per resource or it is being considered an expected idleness? | 60.00% | 40.00% | 0.00% | 0.00% |
| 5.2 When authors are considering an expected idleness, it is explained how actual performance data were collected and analyzed? | 40.00% | 15.00% | 0.00% | 45.00% |
| 6.1 Are authors explaining how time data were collected? | 80.00% | 20.00% | 0.00% | 0.00% |
| 6.2 Are authors using interviews with professionals crossed with medical record review to estimate time data? | 25.00% | 50.00% | 0.00% | 25.00% |
| 6.3 When using chronanalysis, it is being explained how the sample of data was defined? | 15.00% | 30.00% | 0.00% | 55.00% |
| 6.4 Is it being explained if the chronanalysis used a digital technology to collect real time data, such as mobile app, wearable, drone, etc.? | 20.00% | 20.00% | 0.00% | 60.00% |
| 7.1 Is the median or average cost per patient (or per technology) being calculated? | 70.00% | 30.00% | 0.00% | 0.00% |
| 7.2 Are authors presenting the cost per each patient included in the sample? (chart bar, table, etc.)? | 5.00% | 95.00% | 0.00% | 0.00% |
| 7.3 Is the median or average cost per activity on a macro level being presented? | 65.00% | 35.00% | 0.00% | 0.00% |
| 7.4 Is the median or average cost per activity on a micro level being presented? | 20.00% | 80.00% | 0.00% | 0.00% |
| 7.5 Is the median or average cost per resource being presented? | 60.00% | 40.00% | 0.00% | 0.00% |
| 7.6 Are authors performing capacity idleness analysis? | 15.00% | 85.00% | 0.00% | 0.00% |
| 7.7 Are authors exploring statistical analyses to better understand costs along the process of care? | 35.00% | 65.00% | 0.00% | 0.00% |
| 7.8 If the objective was to use the study to support management and value decisions, are authors reporting how value increasing was achieved or if they are planning to achieve it? | 75.00% | 0.00% | 0.00% | 25.00% |
Questions marked in bold are considered mandatory.
NA: Not applicable; NI: Not informed; TDABC: Time-driven activity-based costing.
The three most addressed items (answered ‘Yes’) in the analyzed articles were the definition of study objectives (question 1.1), justification for using the TDABC methodology (question 1.4) and the definition of included resources (question 3.2). Conversely, the three least addressed items (answered ‘No’) were presenting costs per patient included (question 7.2), presenting mean costs per activity at a micro level (question 7.4) and accounting for capacity idleness (question 7.6).
Questions with the highest rates of missing information (answered ‘NI’) were related to using a multidisciplinary team to apply TDABC (question 2.2) and interviewing professionals to better identify resources used in each activity (question 3.4). Regarding how authors collected time variables, 20% of studies did not explain their methods for collecting time data (question 6.1), 25% explicitly reported using interviews with professionals or medical record reviews to assess time data (question 6.2) and only 15% described how the sample size was determined for observing time directly (question 6.3). In terms of cost reporting, 30% of studies did not present or calculate costs at the individual or per-technology level (question 7.1), and 80% did not calculate or report costs at a micro level (question 7.4).
None of the ten studies published after the release of the TDABC checklist referenced its use in either the development or reporting of their methodology. However, nearly all studies (13/14) with a positive response rate exceeding 50% were published after 2020.
Discussion
In this scoping review, we identified 20 studies that employed the TDABC methodology to evaluate costs within the cardiovascular field. These studies were published over the last decade, aligning with the growing body of literature on TDABC in healthcare, which began approximately 15 years ago and has gained momentum in recent years [16]. Most of these studies were published in the same year as, or after, the release of the TDABC in Healthcare Consortium Consensus Statement Checklist at the end of 2020 [15]. However, among the 20 studies reviewed, the checklist was not widely utilized to guide the application or reporting of the methodology.
Applying the checklist to evaluate the implementation of TDABC in CVD studies revealed significant variation in how the methodology is described. While researchers emphasized the importance of selecting TDABC as a microcosting technique, nearly half of the checklist items were not addressed in the reviewed publications. Notably, 20% of studies failed to provide clear explanations about how time variables were collected, highlighting a gap in methodological transparency. Our review also demonstrates that the full potential of the TDABC methodology is not being realized. In many cases, costs were not reported at an individual level – whether per patient, activity or resource – thereby limiting the depth of insights that TDABC could provide.
TDABC offers significant advantages in accurately measuring costs and has the potential to facilitate care redesign and value improvement by detailing costs throughout the care pathway [14,41]. However, several challenges in the microcosting application, particularly in collecting granular data, continue to hinder its full potential in the CVD field. For example, time variables, a critical component of TDABC, can be captured using various methods such as interviews with healthcare professionals, reviewing departmental entry and exit records, or direct observation, often involving digital technology. Despite these options, only a quarter of the reviewed studies reported employing at least one of these methods, while 20% of studies did not disclose how time data were collected. Moreover, most studies were conducted with small, single-center cohorts, likely reflecting both a focus on specific services or health systems and the logistical challenges of collecting time data in multicenter TDABC applications.
This review aligns with previous studies emphasizing the need for consistent application of the TDABC methodology to enable value-based healthcare delivery. However, many studies lack transparency regarding TDABC implementation and their sources for cost estimates [16,42,43]. Standardized tools and guidelines, such as the TDABC checklist, are important for improving the methodological rigor and reporting quality in health economics research [44–46]. The checklist used in this review serves as a valuable tool for enhancing the application, reporting and reproducibility of the TDABC methodology. Widespread adoption of this checklist in TDABC studies could improve clarity and transparency, enhance the accuracy of cost calculations and increase the utility of data for redesigning care and assessing value. A thorough description of the methodology would also facilitate reproducibility, better interpretation and comparison across studies [15].
This study has some limitations. Although the reporting quality assessment was conducted by one reviewer and cross-checked by another, having two independent reviewers would have strengthened the reliability of the evaluation. Furthermore, while the TDABC checklist is a useful instrument for standardizing cost measurement and reporting, other approaches may yield different results. Through this scoping review, we found that most TDABC studies in the CVD field provide limited reporting on methodology and results, as assessed using the TDABC Consortium Checklist. This lack of comprehensiveness in describing TDABC applications reduces the utility of the results generated by the method.
Overall, this review highlights significant gaps in the application and reporting of TDABC in cardiovascular studies. The inconsistent use of the methodology limits data utility, reproducibility and the broader adoption of TDABC as a tool for cost assessment and value improvement in healthcare.
Summary points
•
In 2020, the time-driven activity-based costing (TDABC) Consortium introduced a standardized framework to support the development and reporting of studies utilizing TDABC in healthcare.
•
This scoping review aimed to identify studies in the cardiovascular field that applied TDABC and evaluate these studies using the TDABC Checklist.
•
A total of 20 studies published between 2014 and 2023 were included in this review.
•
TDABC methodology was most frequently applied in hospital settings (75% of the studies) to assess the costs of clinical management, surgeries or interventional procedures.
•
The positive response rate for individual studies ranged from 31 to 81%, with a median rate of 63% (interquartile range: 40–70%).
•
The three most commonly addressed checklist items (answered ‘Yes’) were: defining study objectives (question 1.1), providing justification for using the TDABC methodology (question 1.4) and defining the included resources (question 3.2).
•
The three least frequently addressed items (answered ‘No’) were: presenting costs per patient included in the analysis (question 7.2), presenting mean costs per activity at a microlevel (question 7.4) and accounting for capacity idleness (question 7.6).
•
Through this scoping review, we found that most TDABC studies in the cardiovascular disease field provide limited reporting on methodology and results. This lack of comprehensiveness in describing TDABC applications reduces the utility of the results generated by the method.
Author contributions
NB Schneider, EC Roos and MAZ Marcolino were responsible for study conception, data collection, analysis and manuscript writing. F Caldana, FRV do Nascimento and S Decker were responsible for data collection and manuscript writing. APB da Silva Etges and CA Polanczyk were responsible for writing and revision of the manuscript.
Financial disclosure
The authors have no financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
Competing interests disclosure
The authors have no financial and/or nonfinancial competing interests or relevant affiliations with any organization/entity to declare that are relevant to the subject matter or materials discussed in this manuscript. This includes employment, grants or research funding, consultancies, membership on scientific or other advisory boards, honoraria, stock ownership or options, paid expert testimony, patents received or pending, or royalties.
Writing disclosure
No funded writing assistance was utilized in the production of this manuscript. The authors declare that they used ChatGPT (Version 4) in the creation of this manuscript, to improve language and readability. The authors reviewed and edited the content as needed and take full responsibility for the content of the publication.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary materials.docx)
- Download
- 46.70 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
OECD. Health at a Glance 2023: OECD Indicators. OECD (2023).
2.
OECD, The World Bank. Health at a Glance: Latin America and the Caribbean 2023. OECD (2023).
3.
Abernethy A, Abrahams E, Barker A et al. Turning the tide against cancer through sustained medical innovation: the pathway to progress. Clin. Cancer Res. 20(5), 1081–1086 (2014).
4.
Kazi DS, Elkind MSV, Deutsch A et al. Forecasting the economic burden of cardiovascular disease and stroke in the United States through 2050: a Presidential Advisory from the American Heart Association. Circulation 150(4), e89–e101 (2024).
5.
Rao KD, Roberton T, Vecino-Ortiz AI et al. Future health expenditures and its determinants in Latin America and the Caribbean: a multi-country projection study. Lancet Reg. Health Am. 100781 (2024).
6.
Roth GA, Mensah GA, Johnson CO et al. Global burden of cardiovascular diseases and risk factors, 1990–2019. J. Am. Coll. Cardiol. 76(25), 2982–3021 (2020).
• Describes burden of cardiovascular diseases.
7.
Vollset SE, Ababneh HS, Abate YH et al. Burden of disease scenarios for 204 countries and territories, 2022–2050: a forecasting analysis for the Global Burden of Disease Study 2021. Lancet 403(10440), 2204–2256 (2024).
8.
Joynt Maddox KE, Elkind MSV, Aparicio HJ et al. Forecasting the burden of cardiovascular disease and stroke in the United States through 2050—prevalence of risk factors and disease: a Presidential Advisory from the American Heart Association. Circulation 150(4), e65–e88 (2024).
9.
Gheorghe A, Griffiths U, Murphy A, Legido-Quigley H, Lamptey P, Perel P. The economic burden of cardiovascular disease and hypertension in low- and middle-income countries: a systematic review. BMC Public Health 18(1), 975 (2018).
10.
Bloom DE, Chisholm D, Jané-Llopis E, Prettner K, Stein A, Feigl A. From burden to “Best Buys”: reducing the economic impact of non-communicable diseases. World Health Organization, Switzerland (2011).
11.
Wagstaff A, Flores G, Hsu J et al. Progress on catastrophic health spending in 133 countries: a retrospective observational study. Lancet Global Health 6(2), e169–e179 (2018).
12.
Lievens Y, Borras JM, Grau C. Cost calculation: a necessary step towards widespread adoption of advanced radiotherapy technology. Acta Oncologica 54(9), 1275–1281 (2015).
13.
Da Silva Etges APB, Cruz LN, Notti RK et al. An 8-step framework for implementing time-driven activity-based costing in healthcare studies. Eur. J. Health Econ. 20(8), 1133–1145 (2019).
14.
Kaplan RS. Improving value with TDABC. Healthc. Finanec. Manage. 68(6), 76–83 (2014).
• Describes the importance of time-driven activity-based costing (TDABC) methodology to value based healthcare.
15.
Etges APBDS, Polanczyk CA, Urman RD. A standardized framework to evaluate the quality of studies using TDABC in healthcare: the TDABC in Healthcare Consortium Consensus Statement. BMC Health Serv. Res. 20(1), 1107 (2020).
•• The TDABC in Healthcare Consortium Consensus Statement was published in this paper.
16.
Keel G, Savage C, Rafiq M, Mazzocato P. Time-driven activity-based costing in healthcare: a systematic review of the literature. Health Policy 121(7), 755–763 (2017).
17.
Peters MDJ, Godfrey C, McInerney P, Tricco AC, Khalil H. Chapter 11: scoping reviews. In: JBI Manual for Evidence Synthesis. Aromataris E, Munn Z (Eds). JBI, Australia, 406–451 (2020).
18.
Clarivate. Accelerate your research with EndNote 20. https://endnote.com/product-details/compare-previous-versions
19.
Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan—a web and mobile app for systematic reviews. Syst. Rev. 5(1), 210 (2016).
20.
Donovan CJ, Hopkins M, Kimmel BM, Koberna S, Montie CA. How Cleveland Clinic used TDABC to improve value. Healthc. Finance Manage. 68(6), 84–88 (2014).
• First study to report TDABC on cardiovascular disease.
21.
Tabit CE, Coplan MJ, Spencer KT et al. Cardiology consultation in the Emergency Department reduces re-hospitalizations for low-socioeconomic patients with acute decompensated heart failure. Am. J. Med. 130(9), 1112.e17–1112.e31 (2017).
22.
Chong-Yik R, Bennett AL, Milani RV, Morin DP. Cost-saving opportunities with appropriate utilization of cardiac telemetry. Am. J. Cardiol. 122(9), 1570–1573 (2018).
23.
Goldraich LA, Neyeloff JL, da Silva Etges APB et al. Heart transplantation cost composition in Brazil: a patient-level microcosting analysis and comparison with international data. J. Card. Fail. 24(12), 860–863 (2018).
24.
Martin JA, Mayhew CR, Morris AJ, Bader AM, Tsai MH, Urman RD. Using time-driven activity-based costing as a key component of the value platform: a pilot analysis of colonoscopy, aortic valve replacement and carpal tunnel release procedures. J. Clin. Med. Res. 10(4), 314–320 (2018).
25.
Bobade RA, Helmers RA, Jaeger TM, Odell LJ, Haas DA, Kaplan RS. Time-driven activity-based cost analysis for outpatient anticoagulation therapy: direct costs in a primary care setting with optimal performance. J. Med. Econ. 22(5), 471–477 (2019).
26.
Collins CI, Hasan TF, Mooney LH et al. Subarachnoid hemorrhage “Fast Track”: a health economics and health care redesign approach for early selected hospital discharge. Mayo Clin. Proc. Innov. Qual. Outcomes 4(3), 238–248 (2020).
27.
Erhun F, Kaplan RS, Narayanan VG et al. Are cost advantages from a modern Indian hospital transferable to the United States? Am. Heart J. 224, 148–155 (2020).
28.
Erhun F, Mistry B, Platchek T, Milstein A, Narayanan VG, Kaplan RS. Time-driven activity-based costing of multivessel coronary artery bypass grafting across national boundaries to identify improvement opportunities: study protocol. BMJ Open 5(8), e008765 (2015).
29.
Ho DR, Luery SE, Ghosh RM et al. Cardiovascular 3-D printing: value-added assessment using time-driven activity-based costing. J. Am. Coll. Radiol. 17(11), 1469–1474 (2020).
30.
Keel G, Muhammad R, Savage C et al. Time-driven activity-based costing for patients with multiple chronic conditions: a mixed-method study to cost care in a multidisciplinary and integrated care delivery centre at a university-affiliated tertiary teaching hospital in Stockholm, Sweden. BMJ Open 10(6), e032573 (2020).
• Study with the second highest positive rate.
31.
DeWyer A, Scheel A, Kamarembo J et al. Establishment of a cardiac telehealth program to support cardiovascular diagnosis and care in a remote, resource-poor setting in Uganda. PLOS ONE 16(8), e0255918 (2021).
32.
da Silva Etges APB, Cruz LN, Schlatter R et al. Time-driven activity-based costing as a strategy to increase efficiency: an analyses of interventional coronary procedures. Int. J. Health Plann. Manage. 37(1), 189–201 (2022).
33.
Masthoff M, Schneider KN, Schindler P et al. Value improvement by assessing IR care via time-driven activity-based costing. J. Vasc. Interv. Radiol. 32(2), 262–269 (2021).
34.
Zimmerman ME, Batlle JC, Biga C et al. The direct costs of coronary CT angiography relative to contrast-enhanced thoracic CT: time-driven activity-based costing. J. Cardiovasc. Comput. Tomogr. 15(6), 477–483 (2021).
35.
Kumar A, Siddharth V, Singh SI, Narang R. Cost analysis of treating cardiovascular diseases in a super-specialty hospital. PLOS ONE 17(1), e0262190 (2022).
36.
Etges A, Marcolino MAZ, Ogliari LA et al. Moving the Brazilian ischaemic stroke pathway to a value-based care: introduction of a risk-adjusted cost estimate model for stroke treatment. Health Policy Plan 37(9), 1098–1106 (2022).
37.
Morrow C, Woodbury M, Simpson AN, Almallouhi E, Simpson KN. Determining the marginal cost differences of a telehealth versus an in-person occupational therapy evaluation session for stroke survivors using time-driven activity-based costing. Arch. Phys. Med. Rehabil. 104(4), 547–553 (2023).
38.
Nurok M, Pellegrino V, Pineton de Chambrun M et al. It's not just the prices: time-driven activity-based costing for initiation of veno-venous extracorporeal membrane oxygenation at three international sites-a case review. Anesth. Analg. 135(4), 711–718 (2022).
39.
Wei C, Boeck M, Qian PC et al. Cost of cardiac stereotactic body radioablation therapy versus catheter ablation for treatment of ventricular tachycardia. Pacing Clin. Electrophysiol. 45(9), 1124–1131 (2022).
• Study with the highest positive rate.
40.
Rognoni C, Furnari A, Lugli M, Maleti O, Greco A, Tarricone R. Time-driven activity-based costing for capturing the complexity of healthcare processes: the case of deep vein thrombosis and leg ulcers. Int. J. Environ. Res. Public Health 20(10), 5817 (2023).
41.
Porter ME. What is value in health care? N. Engl. J. Med. 363(26), 2477–2481 (2010).
42.
Leusder M, Porte P, Ahaus K, Van Elten H. Cost measurement in value-based healthcare: a systematic review. BMJ Open 12(12), e066568 (2022).
43.
Pathak S, Snyder D, Kroshus T et al. What are the uses and limitations of time-driven activity-based costing in total joint replacement? Clin. Orthop. Relat. Res. 477(9), 2071–2081 (2019).
44.
Husereau D, Drummond M, Petrou S et al. Consolidated Health Economic Evaluation Reporting Standards (CHEERS) statement. Br. Med. J. 346(mar25 1), f1049–f1049 (2013).
45.
Sanders GD, Neumann PJ, Basu A et al. Recommendations for conduct, methodological practices, and reporting of cost–effectiveness analyses: second panel on cost–effectiveness in health and medicine. J. Am. Med. Assoc. 316(10), 1093–1103 (2016).
46.
McEvoy NL, Tume LN, Trapani J. What are publication reporting checklists and why are they so important? Nurs. Crit. Care 27(3), 291–293 (2022).
Information & Authors
Information
Published In
Copyright
© 2025 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 1 February 2024
Accepted: 15 January 2025
Published online: 26 February 2025
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Evaluation of reporting in time-driven activity-based costing studies on cardiovascular diseases: a scoping review. (2025) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2024-0013
Export citation
Select the citation format you wish to export for this article or chapter.