Association of liver biomarker values beyond current thresholds and negative clinical outcomes in primary biliary cholangitis: analysis of a real-world healthcare claims database
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To assess the predictive effect of threshold deviations for multiple liver biomarkers on negative clinical outcomes, including hepatic decompensation, liver transplantation, and death in patients with primary biliary cholangitis (PBC) using longitudinal data from a large administrative claims database. Materials & methods: A time-dependent Cox proportional hazards model with time-dependent covariates assessed time to first occurrence of hospitalization for hepatic decompensation, liver transplantation, or death in patients with PBC in the Optum Clinformatics Data Mart™ database. Separate models analyzed proportion of time outside prespecified biomarker thresholds (defined as multiples of upper limit of normal [ULN] for alkaline phosphatase [ALP], total bilirubin [TB], aspartate aminotransferase [AST], and alanine aminotransferase [ALT]; lower limit of normal for albumin). Another model evaluated both ALP and TB with the lowest relevant threshold applied for each biomarker. Results: Overall, 2402 patients were included; 85.3% were female, mean age was 63.3 years, median follow-up was 2.2 years (interquartile range: 1.1–3.9 years). On average, patients had approximately five reported measurements for each biomarker evaluated. Each 10% increase in time outside thresholds was associated with a 6.5%, 9.2%, 9.9%, 7.3% and 23.3% increase in risk of negative outcomes for ALP, TB, AST, ALT and albumin, respectively. Conclusion: In patients with PBC, values outside predefined thresholds for biomarkers including ALP, TB, AST, ALT and albumin strongly predicted negative clinical outcomes. These findings highlight the importance of managing biomarkers beyond ALP in monitoring and the treatment of patients with PBC.
Plain language summary: How abnormal liver test results are linked to worse health outcomes in patients with primary biliary cholangitis: a study using real-world health data
Why was this study done?
Patients with primary biliary cholangitis are at risk of serious health problems if the disease is not treated properly. Certain abnormal liver test results at diagnosis or shortly after starting treatment can help predict these risks. One key liver test often used is alkaline phosphatase. However, it is not known whether regularly tracking liver tests over time or including tests in addition to alkaline phosphatase (aspartate aminotransferase, alanine aminotransferase, total bilirubin and albumin) can better predict who will develop these serious outcomes.
What did this study look at?
This study used information from health insurance claims to look at whether abnormal liver test results, tracked over time, were linked to negative health problems such as hospitalization for serious liver complications (hepatic decompensation), liver transplantation or death in patients with primary biliary cholangitis.
What were the results?
Patients who spent more time with abnormal liver test values had a greater risk of serious health problems. The longer they spent outside the normal range, the higher the risk of complications.
What do the results mean?
It is important to monitor liver test results over time. In addition to ALP, other tests like aspartate aminotransferase, alanine aminotransferase, total bilirubin and albumin also play an important role in evaluating risk.
Primary biliary cholangitis (PBC) is a rare chronic liver disease characterized by the gradual destruction of the intrahepatic bile ducts. Published estimates of PBC prevalence in the US have varied between 16 and 40.2 per 100,000 persons [1–3]. A recent retrospective claims database analysis reported an adjusted 2021 estimated prevalence of 40.9 per 100,000 adults, indicating 105,506 adults with PBC in the US [4]. PBC is most prevalent in women aged older than 50 years, but male sex, younger age at onset (<45 years), and advanced disease at presentation are predictive of poorer outcomes [5]. Without sufficiently effective treatment, PBC may progress to cirrhosis and lead to negative clinical outcomes, including hepatic decompensation, liver transplantation and death [6,7].
A substantial proportion of patients have an inadequate response to ursodeoxycholic acid (UDCA), the only approved first-line therapy for PBC, and remain at risk for poor outcomes. However, the criteria for defining inadequate treatment response vary, which may hinder timely treatment decisions. For example, a previous study that used the Paris-I criteria of serum bilirubin ≤1 mg/dl, alkaline phosphatase (ALP) ≤3× the upper limit of normal (ULN), and aspartate aminotransferase (AST) ≤2 × ULN) found that approximately 40% of patients receiving first-line UDCA had an inadequate treatment response [8]. Another study, which used the Toronto criteria of reduction in ALP to <1.67 × ULN by 2 years of UCDA treatment, revealed a nonresponder rate of 24% [9].
A real-world retrospective study that evaluated multiple response criteria revealed a wide range of inadequate UCDA response rates at 12 months within the patient cohort: 9% with Paris-I criteria, 17% with ALP ≤1.67 × ULN, and 39% with the Barcelona criteria of ALP ≤1 × ULN or ALP reduction >40% [10]. Biochemical response rates among these patients improved with treatment modifications, including the initiation of second-line therapy [10]. Results of a more recent study suggested that an ALP level of 1.9 × ULN at 6 months of UCDA treatment is an indicator for initiating second-line therapy, introducing a higher ALP threshold as well as an earlier time point for treatment modification [11]. These studies reflect that treatment guidelines and clinical practice have largely depended on monitoring ALP to determine first-line treatment response in patients with PBC. Furthermore, they highlight the lack of uniform thresholds and timeframes for guiding treatment decisions [12,13].
Current clinical guidelines also focus on ALP thresholds as key indicators of negative clinical outcomes. The European Association for the Study of the Liver guidelines identified ALP >1.50 × ULN as the threshold for increased risk, while the American Association for the Study of Liver Diseases (AASLD) guidelines set the threshold at ALP ≥1.67 × ULN based on studies with a single baseline biochemistry measurement [12,13]. A growing body of literature suggests a continued risk of negative outcomes (disease progression, liver transplantation and death) even in patients meeting the various ALP criteria used to define biochemical treatment response, while also highlighting the potential predictive value of total bilirubin (TB), AST, alanine transaminase (ALT) and serum albumin [14–19]. While UDCA nonresponse and key predictors of negative clinical outcomes are defined biochemically, liver stiffness measurements offer complementary information that may indicate ongoing disease activity or incomplete disease control, even when biochemical response appears adequate [20].
Several risk prediction studies have extrapolated outcomes based on limited biomarker data (i.e., at baseline and after a short duration of first-line treatment, or by evaluating only a small set of biomarkers). The value of single-point-in-time or short-term biomarker levels is limited by multiple factors (e.g., ALP can be elevated following a bone fracture). Furthermore, biomarker levels at baseline do not reflect the effectiveness of long-term disease management over years to decades of follow-up. The association between clinical outcomes and a biomarker measurement outside the threshold may have a cumulative effect over time in this chronic disease. It is conceivable that persistent values beyond thresholds for multiple biochemical markers may be associated with a greater risk than a single occurrence of increased or decreased levels of a single biomarker.
The aim of this study is to expand on previous work examining the associations of longitudinal measurements of several liver biomarkers in risk assessment modeling in PBC, using real-world data from a large administrative claims database [16,17]. We analyzed repeated liver biochemistry measurements to explore the association between the degree and duration of time outside of normal limits for ALP, TB, AST, ALT and albumin with negative clinical outcomes, defined as a composite outcome of time to first occurrence of hospitalization for hepatic decompensation, liver transplantation or death among patients with PBC.
Materials & methods
Data source
This retrospective cohort study was conducted using Optum's de-identified Clinformatics® Data Mart Database (CDM), which is derived from a database of administrative health claims for members of large commercial and Medicare Advantage health plans. CDM also includes laboratory test results.
Study population
Patients aged ≥18 years, without cirrhosis or with compensated cirrhosis, and enrolled in the CDM database from 1 July 2007 to 31 March 2021, were included if they were diagnosed with PBC (index date) by either ≥2 outpatient claims with a PBC diagnosis (ICD-10-CM K74.3 or ICD-9-CM 571.6) on separate days or ≥1 inpatient claim with a diagnosis of PBC; had ≥6 months of continuous enrollment prior to PBC diagnosis, including the index date (baseline period); and had lab values during the baseline period or up to 14 days post index and ≥1 laboratory value in the post index period.
Patients were excluded if they had confounding comorbidities including autoimmune hepatitis (AIH), HIV infection, history of gastric bypass, any history of hepatitis C or active hepatitis B infection, primary sclerosing cholangitis, alcohol-associated liver disease, Gilbert syndrome, hepatocellular carcinoma, hepatorenal syndrome, Paget’s disease, recent bone fracture, portal hypertension or evidence of hepatic decompensation (diagnosis, procedure and drug codes in Supplementary Table 1). Patients were also excluded if they had received a liver transplant any time prior to index or had abnormally high baseline liver biochemistry values (ALP >1000 u/l, TB >3 mg/dl, AST >300 u/l, or ALT >300 u/l) in the 6 months prior to index. Patients who received any second-line therapies, either obeticholic acid (OCA) or off-label fenofibrate, at baseline were excluded to eliminate this as a potential confounder.
Time-dependent exposure variable
The primary analysis was a survival analysis using a Cox model with a time-dependent exposure variable, whereby predictor variables were measured repeatedly throughout the study period to estimate cumulative effects over time. We quantified exposure as the proportion of time a biomarker level exceeded a prespecified threshold [21]. For example, using a threshold for TB of ULN, a patient with TB > ULN for 12 months over 2 years would have a value beyond normal limits 50% of the time by the end of 2 years; if there were no further TB elevations, the patient would be elevated 33% of the time at 3 years and 20% of the time at 5 years. Thus, the percentage of time TB is elevated changes as a function of time under observation. The hazard ratio (HR) for an increase in the proportion of time outside of normal limits was expressed in 10% increments. Laboratory values were carried forward between observations.
The thresholds chosen for this analysis capture those used in common UDCA response criteria (e.g., Paris I, Paris II and Rotterdam) [8,22]. The thresholds for each biomarker were defined as multiples of ULN for ALP (1×, 1.2×, 1.5×, 1.67×, 2.0×), TB (0.6×, 0.8×, 1.0×, 2.0×), AST (1×, 1.5×, 2.0×) and ALT (1×, 1.5×, 2.0×) and multiples of the lower limits of normal (LLN) for albumin (1×, 1.09×, 1.14×). For TB, recent research has shown that levels above 0.6 × ULN are associated with incremental risk of liver transplantation and death in patients with PBC [18], so thresholds were examined at and above this level.
Baseline predictor variables
Baseline variables in the models included patient demographics (age and sex) and comorbidities (nonalcoholic steatohepatitis [NASH] and cirrhosis). Baseline comorbidities were coded as present if diagnosis or procedure codes were present in the 6 months before index (diagnosis, procedure, and drug codes in Supplementary Table 1).
Outcome variables
Negative clinical outcomes were defined as a composite of first occurrence of hospitalization for a decompensating event, liver transplantation, or all-cause death outcomes commonly utilized in PBC studies [23]. Decompensating events included ascites, esophageal or gastric varices with bleeding, or hepatic encephalopathy. The use of spironolactone, furosemide, lactulose, or rifaximin during an inpatient admission was also considered indicative of hepatic decompensation.
Statistical analysis
Baseline patient characteristics were reported using descriptive statistics. Frequency and timing of liver biochemistry testing during the follow-up period were also characterized. The number and percentage of subjects either censored or with outcomes were presented.
The primary modeling analyses employed a time-dependent Cox proportional hazards model with time-dependent covariates in survival analyses, assessing time to first occurrence hospitalization for hepatic decompensation, liver transplantation, or death. Time-invariant baseline covariates included age, sex, NASH and cirrhosis. The time-dependent exposure was the proportion of laboratory values outside prespecified thresholds at each time point (summary of thresholds in Table 2). Patients were censored at database disenrollment, initiation of either OCA or fenofibrate or the end of the study period.
| Baseline characteristic | Frequency/mean (n = 2402) |
|---|---|
| Sex, n (%) | |
| Female | 2049 (85.3) |
| Male | 353 (14.7) |
| Age, mean (SD), y | 63.3 (13.1) |
| NASH, n (%) | 169 (7.0) |
| Cirrhosis, n (%) | 265 (11.0) |
| Baseline UDCA, n (%) | 1637 (68.2) |
| UDCA use during follow-up, n (%) | 1697 (70.7) |
| Follow-up characteristic | |
| Follow-up time, median (IQR), y | 2.2 (1.1–3.9) |
| Censoring events, n (%) | |
| Follow-up OCA or fenofibrate | 87 (3.6) |
| End of enrollment | 1729 (72.0) |
| End of follow-up | 395 (16.4) |
| Outcomes, n (%) | |
| Composite | 191 (8.0) |
| First event† | |
| Hospitalization for hepatic decompensation | 99 (4.1) |
| Liver transplant | 5 (0.2) |
| Death | 87 (3.6) |
†
Events are not mutually exclusive; multiple events can occur on the same date.
IQR: Interquartile range; NASH: Nonalcoholic steatohepatitis; OCA: Obeticholic acid; SD: Standard deviation; UDCA: Ursodeoxycholic acid.
| Characteristic | Frequency/mean |
|---|---|
| ALP model (n = 2378) | |
| Follow-up time, median (IQR) | 2.2 (1.1–3.9) |
| Follow-up ALP labs, n, mean (SD) | 5.4 (5.2) |
| Patients with follow-up labs outside of specified threshold, n (%) | |
| ALP ≥ULN | 1635 (68.8) |
| ALP ≥1.2 × ULN | 1305 (54.9) |
| ALP ≥1.5 × ULN | 933 (39.2) |
| ALP ≥1.67 × ULN | 777 (32.7) |
| ALP ≥2 × ULN | 550 (23.1) |
| Proportion/percentage of follow-up time outside of normal limits, mean (SD) | |
| ALP ≥ULN | 52.5 (44.6) |
| ALP ≥1.2 × ULN | 38.3 (43.6) |
| ALP ≥1.5 × ULN | 23.9 (37.8) |
| ALP ≥1.67 × ULN | 18.4 (34.2) |
| ALP ≥2 × ULN | 12.3 (28.9) |
| Censoring events, n (%) | |
| Follow-up OCA or fenofibrate | 86 (3.6) |
| End of enrollment | 1710 (72.0) |
| End of follow-up | 394 (16.6) |
| Outcomes, n (%) | |
| Composite | 188 (7.9) |
| First event† | |
| Hospitalization for hepatic decompensation | 98 (4.1) |
| Liver transplant | 5 (0.2) |
| Death | 85 (3.6) |
| TB model (n = 2373) | |
| Follow-up time, median (IQR) | 2.2 (1.1–3.9) |
| Follow-up TB labs, n, mean (SD) | 5.4 (5.2) |
| Patients with follow-up labs outside of specified threshold, n (%) | |
| TB ≥0.6 × ULN | 1264 (53.3) |
| TB ≥0.8 × ULN | 675 (28.5) |
| TB ≥ULN | 425 (17.9) |
| TB ≥2 × ULN | 87 (3.7) |
| Proportion/percentage of follow-up time outside of normal limits, mean (SD) | |
| TB ≥0.6 × ULN | 31.5 (39.3) |
| TB ≥0.8 × ULN | 15.3 (30.9) |
| TB ≥ULN | 8.5 (23.6) |
| TB ≥2 × ULN | 1.1 (7.9) |
| Censoring events, n (%) | |
| Follow-up OCA or fenofibrate | 86 (3.6) |
| End of enrollment | 1708 (72.0) |
| End of follow-up | 391 (16.5) |
| Outcomes, n (%) | |
| Composite | 188 (7.9) |
| First event† | |
| Hospitalization for hepatic decompensation | 98 (4.1) |
| Liver transplant | 5 (0.2) |
| Death | 85 (3.6) |
| AST model (n = 2378) | |
| Follow-up time, median (IQR) | 2.2 (1.1–3.9) |
| Follow-up AST labs, n, mean (SD) | 5.4 (5.2) |
| Patients with follow-up labs outside of specified threshold, n (%) | |
| AST ≥ULN | 1489 (62.6) |
| AST ≥1.5 × ULN | 784 (33.0) |
| AST ≥2 × ULN | 478 (20.1) |
| AST ≥5 × ULN | 49 (2.1) |
| Proportion/percentage of follow-up time outside of normal limits, mean (SD) | |
| AST ≥ULN | 37.5 (40.9) |
| AST ≥1.5 × ULN | 14.6 (29.3) |
| AST ≥2 × ULN | 7.5 (21.5) |
| AST ≥5 × ULN | 0.3 (2.8) |
| Censoring events, n (%) | |
| Follow-up OCA or fenofibrate | 86 (3.6) |
| End of enrollment | 1711 (72.0) |
| End of follow-up | 393 (16.5) |
| Outcomes, n (%) | |
| Composite | 188 (7.9) |
| First event† | |
| Hospitalization for hepatic decompensation | 98 (4.1) |
| Liver transplant | 5 (0.2) |
| Death | 85 (3.6) |
| ALT model (n = 2385) | |
| Follow-up time, median (IQR) | 2.2 (1.1–3.9) |
| Follow-up ALT labs, n, mean (SD) | 5.4 (5.2) |
| Patients with follow-up labs outside of specified threshold, n (%) | |
| ALT ≥ULN | 1020 (42.8) |
| ALT ≥1.5 × ULN | 555 (23.3) |
| ALT ≥2 × ULN | 337 (14.1) |
| ALT ≥5 × ULN | 29 (1.2) |
| Proportion/percentage of follow-up time outside of normal limits, mean (SD) | |
| ALT ≥ULN | 20.7 (33.5) |
| ALT ≥1.5 × ULN | 9.0 (23.0) |
| ALT ≥2 × ULN | 4.8 (17.1) |
| ALT ≥5 × ULN | 0.2 (3.6) |
| Censoring events, n (%) | |
| Follow-up OCA or fenofibrate | 86 (3.6) |
| End of enrollment | 1717 (72.0) |
| End of follow-up | 392 (16.4) |
| Outcomes, n (%) | |
| Composite | 190 (8.0) |
| First event† | |
| Hospitalization for hepatic decompensation | 99 (4.2) |
| Liver transplant | 5 (0.2) |
| Death | 86 (3.6) |
| Albumin model (n = 2383) | |
| Follow-up time, median (IQR) | 2.2 (1.1–3.9) |
| Follow-up ALB labs, n, mean (SD) | 5.5 (5.3) |
| Patients with follow-up labs outside of specified threshold, n (%) | |
| ALB ≤1.14 × LLN | 1149 (48.2) |
| ALB ≤1.09 × LLN | 926 (38.9) |
| ALB ≤1.0 × LLN | 436 (18.3) |
| Proportion/percentage of follow-up time outside of normal limits, mean (SD) | |
| ALB ≤1.14 × LLN | 26.3 (36.7) |
| ALB ≤1.09 × LLN | 19.2 (32.7) |
| ALB ≤1.0 × LLN | 7.2 (21.2) |
| Censoring events, n (%) | |
| Follow-up OCA or fenofibrate | 86 (3.6) |
| End of enrollment | 1716 (72.0) |
| End of follow-up | 391 (16.4) |
| Outcomes, n (%) | |
| Composite | 190 (8.0) |
| First event† | |
| Hospitalization for hepatic decompensation | 98 (4.1) |
| Liver transplant | 5 (0.2) |
| Death | 87 (3.7) |
†
Events are not mutually exclusive; multiple events can occur on the same date.
Follow-up time, censoring events, negative clinical outcomes, and proportion of follow-up time with laboratory values outside of evaluated thresholds are shown for each model.
ALB: Albumin; ALP: Alkaline phosphatase; ALT: Alanine transaminase; AST: Aspartate aminotransferase; IQR: Interquartile range; OCA: Obeticholic acid; SD: Standard deviation; TB: Total bilirubin; ULN: Upper limit of normal.
Separate models were estimated for the proportion of time spent above thresholds for each biomarker. Another model including both ALP and TB, choosing the lowest threshold for each variable (ALP ≥ULN and TB ≥ 0.6 × ULN) was also estimated. The proportional hazards assumption was tested using a global chi-square test based on the scaled Schoenfeld residuals. HRs and 95% CIs for each covariate and proportion of time above thresholds (per 10% increment) were reported.
Two subgroup sensitivity analyses using Cox proportional models were performed. The first sensitivity analysis included only patients with a PBC diagnosis identified based on ICD-10 codes, and the second sensitivity analysis excluded patients with NASH or cirrhosis at baseline. HRs, lower and upper confidence levels (CLs), and p-values were reported.
All analyses were conducted in SAS v9.4 and R v4.0.0.
Results
Patient characteristics
Of 17,979 adult patients in the database with a diagnosis of PBC, 2402 fulfilled inclusion criteria (Figure 1). As shown in Table 1, 85.3% of patients were female. At baseline, mean patient age was 63.3 years (SD: 13.1); 11.0% had compensated cirrhosis, 7.0% had NASH and 68.2% were receiving UDCA therapy. During follow-up, 70.7% of patients received UDCA. Median follow-up time was 2.2 years (interquartile range: 1.1–3.9 years); 3.6% (n = 87) of patients were censored at the start of second-line treatment. Overall, 8.0% (n = 191) experienced ≥1 negative clinical outcome; the first event was hospitalization for hepatic decompensation in 4.1% of patients (n = 99), liver transplantation in 0.2% (n = 5), and death in 3.6% (n = 87) (Table 1).
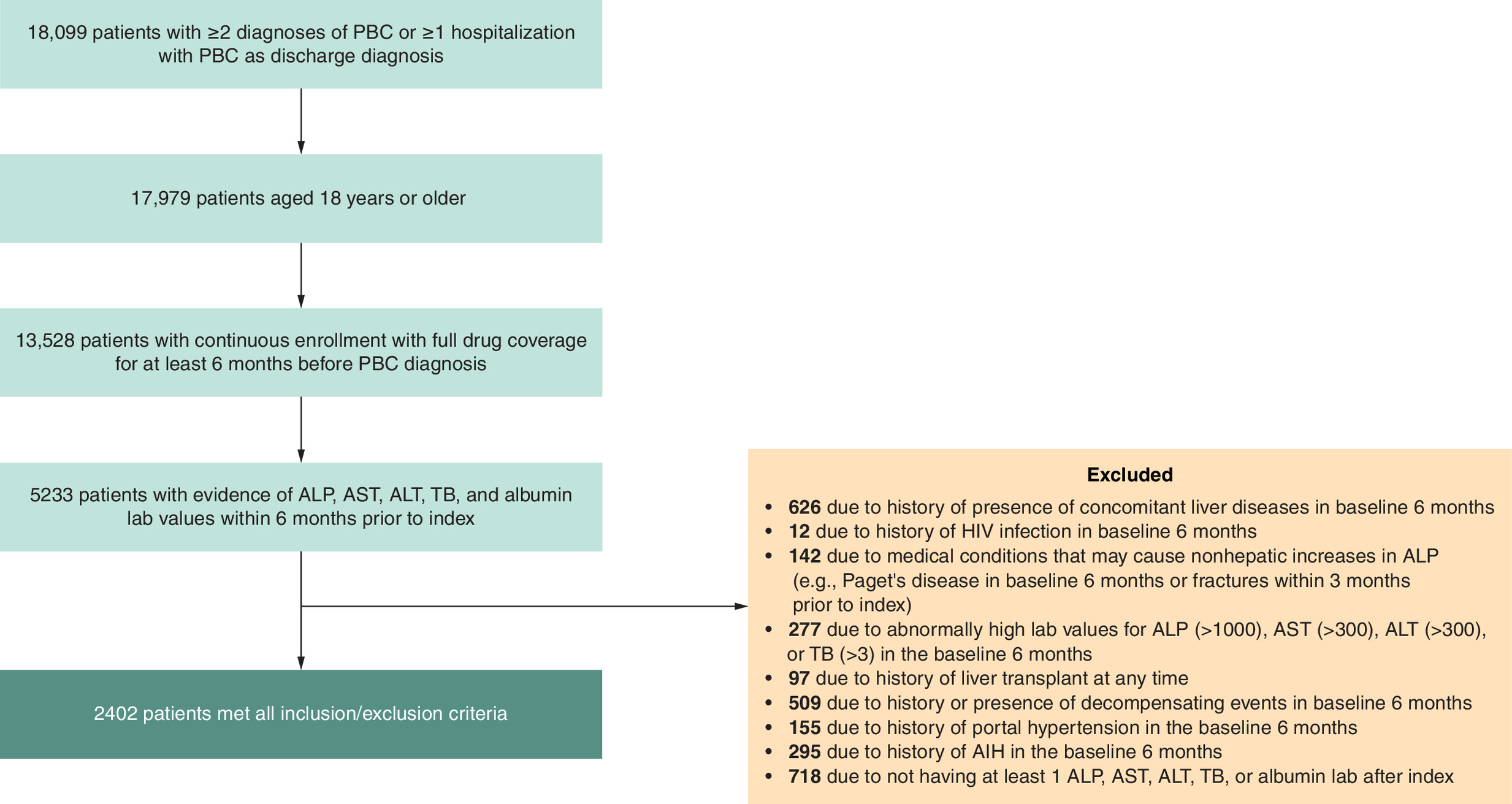
Figure 1. Flow diagram of patient selection.
AIH: Autoimmune hepatitis; ALP: Alkaline phosphatase; ALT: Alanine aminotransferase; AST: Aspartate aminotransferase; PBC: Primary biliary cholangitis; TB: Total bilirubin.
Among the 2402 patients identified, a total of 2378 patients met the criteria and were included in the ALP model; 2373 were included in the TB model, 2378 were included in the AST model, 2385 were included in the ALT model, and 2383 were included in the albumin model. The combined ALP and TB model included 2370 patients. Follow-up time, censoring, negative clinical outcomes and proportions of time outside of evaluated thresholds are presented in Table 2. On average, patients had approximately five measures of each biomarker prior to censoring or an event, whichever occurred first. Mean proportion of time above ULN was 52.5% for ALP, 8.5% for TB, 37.5% for AST and 20.7% for ALT; mean proportion of time below LLN was 7.2% for albumin.
Negative clinical outcomes
For each of the biomarkers assessed (ALP, TB, AST, ALT and albumin), a greater proportion of time spent outside of thresholds and greater divergence from normal limits were associated with an increased risk of hepatic decompensation, liver transplantation, or death (Figure 2). Using the 5-year modeled follow-up period as an example, a patient with TB > ULN for 12 months (20% of 5 years) was estimated to have a 34% increase in risk (HR = 1.34) of negative clinical outcomes (Figure 2B), while a patient with 36 months of TB > ULN over 5 years (60% of the time) would have a 140% (2.4-times greater) risk (HR = 2.40). For ALP (Figure 2A), AST (Figure 2C) and ALT (Figure 2D), each 10% increase in time above ULN was associated with a 6.5%, 9.9% and 7.3% increase in risk, respectively. For albumin, each 10% increase in time below LLN was associated with a 23.3% increase in risk (Figure 2E).
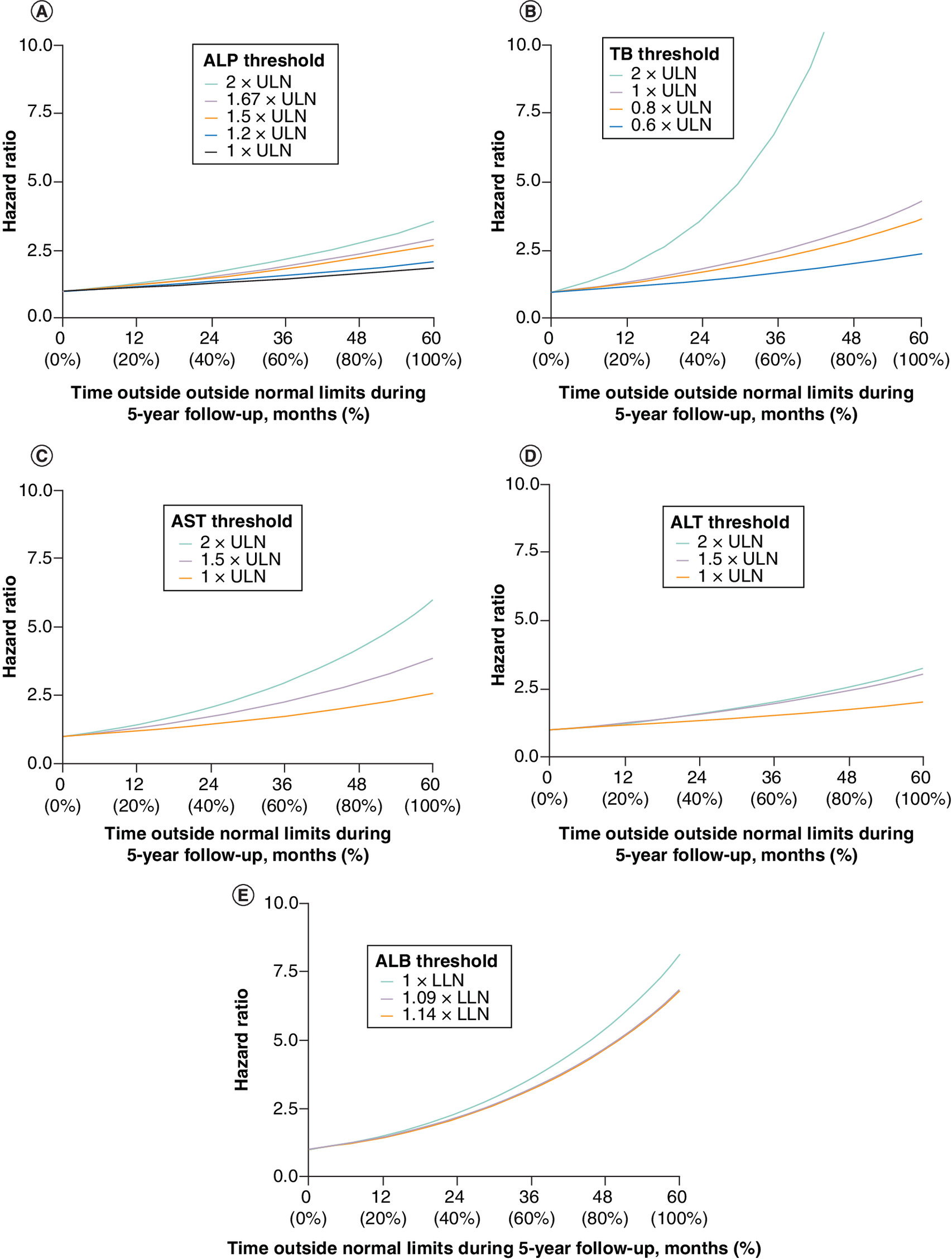
Figure 2. Hazard ratios for risk of hospitalization for hepatic decompensation, liver transplantation or death (composite) as a function of time above prespecified thresholds.
5-year follow-up example for: (A) ALP (n = 2379), (B) total bilirubin (n = 2374), (C) AST (n = 2379), (D) ALT (n = 2386) and (E) ALB (n = 2384).
ALB: Albumin; ALP: Alkaline phosphatase; ALT: Alanine aminotransferase; AST: Aspartate aminotransferase; LLN: Lower limit of normal; TB: Total bilirubin; ULN: Upper limit of normal.
The assumptions of proportional hazard, evaluated using a global chi-square test based on the scaled Schoenfeld residuals for each model, were supported by nonsignificant global tests for all thresholds with the exceptions of ALP ≥ 2 × ULN (p = 0.007) and TB ≥ 2 × ULN (p = 0.006).
Table 3 shows the Cox regression model with time-dependent covariates combining ALP and TB, with the lowest thresholds applied. All variables except NASH were associated with a significant increase in risk of a negative clinical outcome. As shown in Figure 3, there was a fourfold increase in the risk of an event in patients with consistent elevations (100% of observed time) of both ALP ≥ULN and TB ≥ 0.6 × ULN relative to patients with no time above these thresholds. Supplementary Table 2 demonstrates the significant increase in risk of a negative clinical outcome as ALP and TB deviate further from ULN.
| Parameter | Hazard ratio | 95% CI | p-value |
|---|---|---|---|
| Proportion of time ALP ≥ ULN (for a 10% increase) | 1.059 | 1.033–1.085 | <0.001 |
| Proportion of time TB ≥ 0.6 × ULN (for a 10% increase) | 1.091 | 1.063–1.119 | <0.001 |
| Age (per 10-year increase) | 1.568 | 1.415–1.737 | <0.001 |
| Sex (female vs male) | 0.609 | 0.472–0.785 | <0.001 |
| NASH (yes vs no) | 1.385 | 0.967–1.984 | 0.076 |
| Cirrhosis (yes vs no) | 1.470 | 1.098–1.68 | 0.010 |
n = 2370.
The primary analysis was a survival analysis using a Cox proportional hazards model with a time-dependent exposure variable. Predictor variables were measured repeatedly throughout the study period to estimate cumulative effects over time. The effects of age, sex, and the presence of NASH or cirrhosis were also evaluated.
ALP: Alkaline phosphatase; CI: Confidence interval; NASH: Nonalcoholic steatohepatitis; TB: Total bilirubin; ULN: Upper limit of normal.
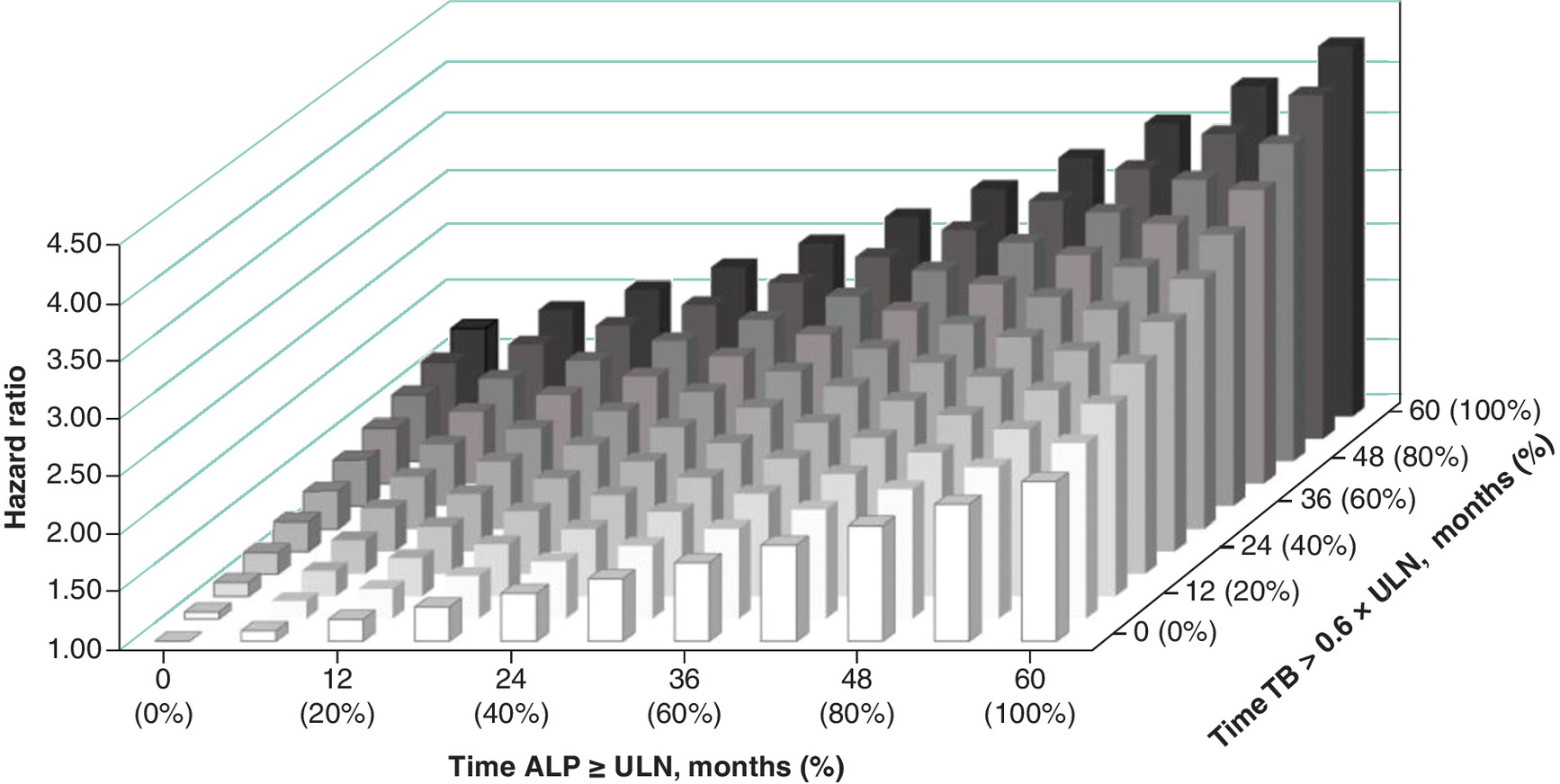
Figure 3. Hazard ratios for risk of hospitalization for hepatic decompensation, liver transplantation or death (composite) as a function of time above prespecified thresholds. Five-year follow-up example for ALP ≥ULN and total bilirubin ≥ 0.6 × ULN (n = 2370).
ALP: Alkaline phosphatase; TB: Total bilirubin; ULN: Upper limit of normal.
Subgroup sensitivity analyses
Results from a sensitivity analysis (Supplementary Tables 3 & 4) including only patients with a confirmed PBC diagnosis based on ICD-10 codes (n = 1532) and a separate sensitivity analysis (Supplementary Tables 5 & 6) excluding patients with NASH or cirrhosis at baseline (n = 1977) were similar to results from the original analyses.
Discussion
In this study, 8.0% of patients with PBC, either without cirrhosis or with compensated cirrhosis, experienced negative clinical outcomes, defined as a composite of the first occurrence of hospitalization for hepatic decompensation, liver transplantation or death. The most common first event of the composite outcome was hospitalization for hepatic decompensation (4.1%), indicative of meaningful disease progression during follow-up. Death was the first event for 3.6% of patients; the mortality component of the composite end point, defined as all-cause death, aligns with common reporting in PBC studies [23]. Liver transplantation was the least frequent first event (0.2%). ALP, TB, AST, ALT and albumin values beyond thresholds were each associated with an increased risk of negative clinical outcomes. Additionally, in line with previous reports [18], the risk of the negative clinical outcome was fourfold higher in patients with both ALP ≥ ULN and TB ≥ 0.6 × ULN during the follow-up period.
Current AASLD and European Association for the Study of the Liver guidelines are consistent with the seminal works of Lammers et al. [16] and Carbone et al. [17] in utilizing single measures of biomarkers to predict the risk of liver transplantation and death, whereby ALP values > 1.67 × ULN and >1.5 × ULN and TB > ULN were identified as thresholds triggering the need for second-line pharmaceutical intervention in PBC [12,13]. Although the GLOBE [24] and UK-PBC [17] scores are designed to predict transplant-free and liver-related outcomes, respectively, they are based on static measurements taken at baseline and 12 months after initiating UDCA treatment, rather than continuous monitoring over the treatment period. The findings of the current analysis build on this existing evidence, highlighting the clinical relevance of AST, ALT and albumin levels, while continuing to underscore the significance of elevated ALP and TB levels. Furthermore, these results emphasize the importance of continued biomarker monitoring throughout the disease course, given the observed increases in the composite outcome risk associated with not only the magnitude of out-of-range biomarker values but also with the duration of time spent outside the thresholds.
These findings suggest that clinicians and treatment guidelines should expand beyond monitoring only ALP and TB when assessing risk or determining the need to initiate first- or second-line therapy, by incorporating additional biomarkers such as ALT, AST and albumin. This work may support the evolution of biochemical criteria used in PBC disease monitoring. The importance of timely pharmacotherapeutic intervention in PBC is highlighted by the reduction in negative clinical outcomes demonstrated with first-line UDCA and second-line OCA treatment [25–32]. Additionally, PBC management may benefit from considering both the absolute levels of multiple biomarkers and the duration of time spent beyond thresholds when evaluating risk of disease progression and guiding treatment decisions for the appropriate patient populations. Future research is needed to expand on these findings to further validate and quantify the potential benefits of timely therapeutic intervention in PBC, including examining the cumulative effect of threshold deviations across multiple biomarkers and measures of inflammation and fibrosis.
Limitations
This was a retrospective analysis of administrative claims data, which has inherent limitations, including the possibility of miscoding, billing-related bias and missing information. To mitigate the risk of miscoding, we required at least two outpatient or one inpatient claims with a PBC diagnosis, as similar criterion has demonstrated a positive predictive value of 73% for confirmed PBC and 89% for confirmed or suspected PBC [33]. Prior to October 2015, when no PBC-specific ICD-9 diagnosis code existed, identification was based on the biliary cirrhosis code (571.6). However, our sensitivity analysis, which included only patients with an ICD-10 PBC-specific diagnosis code, confirmed the original study findings. Additionally, although we excluded patients with an AIH diagnosis code at baseline, it is possible that a small percentage of patients with a PBC/AIH overlap syndrome were included.
Patients receiving second-line treatments were excluded from this analysis in order to isolate outcomes under standard first-line therapy (i.e., UDCA). As a result, the study cohort may underrepresent individuals at higher risk for negative clinical outcomes. Although liver stiffness can also be used to show inadequate response to UDCA and progression of disease [13,20], liver stiffness measurements data are not readily available in claims data.
It should be noted that patients who met the study inclusion criteria entered the cohort at the time of their first qualifying PBC diagnosis during the prespecified study period. As a result, the patient population included both incident and prevalent PBC, likely with heterogeneous time since their initial diagnosis. Additionally, patients had varying lengths of follow-up due to changes in their insurance status. Our study also included patients with NASH and cirrhosis, conditions that, when combined with PBC, may lead to negative clinical outcome sooner than with PBC alone. However, a separate sensitivity analysis excluding individuals with NASH or cirrhosis at baseline demonstrated that our findings remained qualitatively unchanged. The significance and magnitude of the effect of increasing time outside biomarker thresholds in the subgroup were similar to those observed in the overall analyses.
Regarding the composite outcome, cause of death was not reported in this study, as this information is not readily available in claims data; however, patients with PBC often have a high comorbidity burden, which may have contributed to mortality [34]. Additionally, the biomarkers and thresholds of interest (ALP, AST, and ALT >ULN, TB >0.6 × ULN, and albumin <LLN) were based on laboratory test results. Extreme/implausible values were removed to avoid associations driven by outliers, and patients with no laboratory tests during the follow-up period were excluded, potentially introducing selection and measurement bias. Unlike clinical trial data, laboratory assessments in clinical practice are not collected at fixed intervals, and not all lab values were available in the dataset. As a result, laboratory values were carried forward between observations and may not capture potential changes that occurred during these intervals. Additionally, adjustments were not made for other key prognostic factors, such as UDCA response, fibrosis stage, comorbidities, sex or treatment adherence, potentially introducing residual confounding. Finally, as with any real-world study, unobserved factors and limitations in generalizability are potential concerns, as this study focused on patients with compensated PBC who had US insurance coverage. However, the use of a large US healthcare database, along with prespecified inclusion and exclusion criteria and replication of results across multiple sensitivity analyses, supports the robustness of the findings.
In conclusion, this research demonstrates that in patients living with PBC, whether untreated or receiving first-line therapy, elevations in ALP, TB, AST and ALT and reduction in albumin levels beyond guideline-recommended thresholds are predictive of negative clinical outcomes. A combination of ALP and TB above conservative thresholds was a robust predictor, while the aminotransferases AST and ALT yielded additional insight into the risk of negative outcomes. Our findings further suggest that longitudinal biomarker monitoring may offer additional value by enabling earlier risk stratification and identification of UDCA nonresponse prior to the 12-month time point used in existing prognostic scores and biochemical response criteria. Given evidence demonstrating the ability of current therapies to reduce these events [31,35–37], clinicians, and ultimately, treatment guidelines may consider more frequent monitoring of all available liver biomarkers and timely initiation of treatment to reduce the risk of negative clinical outcomes.
Summary points
•
Primary biliary cholangitis (PBC) is a rare chronic liver disease that, without effective treatment, may progress to cirrhosis and lead to negative clinical outcomes, including hepatic decompensation, liver transplantation, and death.
•
Current treatment guidelines recommend monitoring alkaline phosphatase (ALP) and total bilirubin (TB) to determine treatment response and predict the risk of negative clinical outcomes.
•
This retrospective cohort study used administrative health claims and laboratory test results from patients with PBC enrolled in Optum's de-identified Clinformatics® Data Mart Database to analyze repeated liver biochemistry measurements.
•
A time-dependent Cox proportional hazards model with time-dependent covariates assessed the time to first occurrence of hepatic decompensation, liver transplantation, or death.
•
Separate models evaluated the association between the degree and duration of time outside normal limits for ALP, TB, alanine aminotransferase (ALT), aspartate aminotransferase (AST) and albumin with negative clinical outcomes.
•
Between 2007 and 2021, 2402 patients met the inclusion criteria. Among these patients, 8.0% experienced a negative clinical outcome of hepatic decompensation, liver transplantation or death.
•
Each 10% increase in time outside thresholds was associated with a 6.5%, 9.2%, 9.9%, 7.3% and 23.3% increase in risk of negative outcomes for ALP, TB, AST, ALT and albumin, respectively.
•
For each biomarker, a greater proportion of time spent outside recommended thresholds and a greater divergence from normal limits correlated with an increased risk of negative clinical outcomes, suggesting that more frequent monitoring of all available liver biomarkers and timely treatment initiation may improve patient outcomes.
Author contributions
All authors conceived and designed the study; JP MacEwan, CS Parzynski and D Mercer performed the data analyses; all authors reviewed the data analyses; JP MacEwan and T Mayne wrote the manuscript; and all authors read, edited and approved the manuscript.
Financial disclosure
This study was supported by Intercept Pharmaceuticals, Inc., a wholly owned subsidiary of Alfasigma S.p.A.
Competing interests disclosure
TE Ritter participates in speaking panels for Takeda, Janssen, Pfizer, Bristol Myers Squibb and AbbVie; serves on the Data Adjudication Committee for Ferring/Rebiotix; is a member of the Advisory Board for AbbVie, Ardelyx, Arena, Boehringer Ingelheim, Bristol Myers Squibb/Celgene, Ferring, Genentech/Roche, Gilead, Intercept, Janssen, Lilly, Pfizer, Prometheus, Sanofi and Takeda; and is an Advisory Board member and shareholder for Iterative Scopes. CJ Hanson is a Speaker for Intercept and Salix; is a Consultant for Evoke, Intercept, Phathom and Salix. C Fernandes has nothing to disclose. JP MacEwan, X Zhao, CS Parzynski and D Mercer are employees of Genesis Research. E Ness, D Wheeler and T Mayne are former employees of Intercept Pharmaceuticals, Inc. KV Kowdley receives honoraria, fees, equity, research support and clinical trial grants from AbbVie, Corcept, CymaBay, Enanta, Genfit, Gilead, GSK, Hanmi, HighTide, Inipharm, Intercept, Madrigal, Mirum, Novo Nordisk, NGM Bio, Pfizer, Pliant, Terns, Viking and 89bio. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing disclosure
Medical writing support was provided by Shawn Vahabzadeh, PharmD, of Intercept Pharmaceuticals at the time of drafting. Editorial support was provided by Citrus Health Group, Inc. (IL, USA) and was funded by Intercept Pharmaceuticals, Inc., a wholly owned subsidiary of Alfasigma S.p.A.
Ethical conduct of research
This study utilized retrospective deidentified data and was considered to be of minimal or no risk to subjects.
Open access
This work is licensed under the Creative Commons Attribution 4.0 License. To view a copy of this license, visit https://creativecommons.org/licenses/by/4.0/
Supplementary Material
File (supplementary data.docx)
- Download
- 132.81 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Colapietro F, Bertazzoni A, Lleo A. Contemporary epidemiology of primary biliary cholangitis. Clin. Liver Dis. 26(4), 555–570 (2022).
2.
Lu M, Li J, Haller IV et al. Factors associated with prevalence and treatment of primary biliary cholangitis in United States health systems. Clin. Gastroenterol. Hepatol. 16(8), 1333–1341 (2018).
3.
Lv T, Chen S, Li M, Zhang D, Kong Y, Jia J. Regional variation and temporal trend of primary biliary cholangitis epidemiology: a systematic review and meta-analysis. J. Gastroenterol. Hepatol. 36(6), 1423–1434 (2021).
4.
Buchanan-Peart K-A, MAcEwan JP, Levine A et al. United States (US) prevalence of diagnosed primary biliary cholangitis: 41 per 100,000 adults with wide regional variability [abstract 4588-C]. Presented at: The Liver Meeting. MA, USA (12–14 November 2023).
5.
Hirschfield GM, Dyson JK, Alexander GJM et al. The British Society of Gastroenterology/UK-PBC primary biliary cholangitis treatment and management guidelines. Gut 67(9), 1568–1594 (2018).
6.
Lammers WJ, Kowdley KV, van Buuren HR. Predicting outcome in primary biliary cirrhosis. Ann. Hepatol. 13(4), 316–326 (2014).
7.
Corpechot C, Chazouilleres O, Poupon R. Early primary biliary cirrhosis: biochemical response to treatment and prediction of long-term outcome. J. Hepatol. 55(6), 1361–1367 (2011).
•• Defined biochemical response criteria for early-stage primary biliary cirrhosis, showing that patients achieving specific reductions in alkaline phosphatase and aspartate aminotransferase, alongside normal bilirubin, have a significantly lower risk of adverse outcomes, which can refine treatment monitoring and improve long-term patient management.
8.
Corpechot C, Abenavoli L, Rabahi N et al. Biochemical response to ursodeoxycholic acid and long-term prognosis in primary biliary cirrhosis. Hepatology 48(3), 871–877 (2008).
9.
Lammert C, Juran BD, Schlicht E et al. Biochemical response to ursodeoxycholic acid predicts survival in a North American cohort of primary biliary cirrhosis patients. J. Gastroenterol. 49(10), 1414–1420 (2014).
10.
Wilde AB, Lieb C, Leicht E et al. Real-world clinical management of patients with primary biliary cholangitis-a retrospective multicenter study from Germany. J. Clin. Med. 10(5), (2021).
11.
Murillo Perez CF, Ioannou S, Hassanally I et al. Optimizing therapy in primary biliary cholangitis: alkaline phosphatase at six months identifies one-year non-responders and predicts survival. Liver Int. 43(7), 1497–1506 (2023).
• Emphasizes the importance of early monitoring and intervention in primary biliary cholangitis (PBC) treatment to enhance prognosis and survival.
12.
Lindor KD, Bowlus CL, Boyer J, Levy C, Mayo M. Primary biliary cholangitis: 2018 practice guidance from the American Association for the Study of Liver Diseases. Hepatology 69(1), 394–419 (2019).
13.
European Association for the Study of the Liver. EASL clinical practice guidelines: the diagnosis and management of patients with primary biliary cholangitis. J. Hepatol. 67(1), 145–172 (2017).
14.
Corpechot C, Lemoinne S, Soret PA et al. Adequate versus deep response to ursodeoxycholic acid in primary biliary cholangitis: to what extent and under what conditions is normal alkaline phosphatase level associated with complication-free survival gain? Hepatology 79(1), 39–48 (2024).
15.
Gazda J, Drazilova S, Gazda M et al. Treatment response to ursodeoxycholic acid in primary biliary cholangitis: a systematic review and meta-analysis. Dig. Liver Dis. 55(10), 1318–1327 (2023).
16.
Lammers WJ, van Buurenzqz HR, Hirschfieldzqz GM et al. Levels of alkaline phosphatase and bilirubin are surrogate end points of outcomes of patients with primary biliary cirrhosis: an international follow-up study. Gastroenterology 147(6), 1338–1349 (2014).
• Seminal research demonstrating that alkaline phosphatase and bilirubin are reliable surrogate endpoints for predicting outcomes in patients with primary biliary cholangitis.
17.
Carbone M, Sharp SJ, Flack S et al. The UK-PBC risk scores: derivation and validation of a scoring system for long-term prediction of end-stage liver disease in primary biliary cholangitis. Hepatology 63(3), 930–950 (2016).
• Developed and validated the UK-PBC risk scores to assess the prognosis of patients with PBC using readily available laboratory measures, including platelet count, albumin, bilirubin, aminotransferases and alkaline phosphatase.
18.
Murillo Perez CF, Harms MH, Lindor KD et al. Goals of treatment for improved survival in primary biliary cholangitis: treatment target should be bilirubin within the normal range and normalization of alkaline phosphatase. Am. J. Gastroenterol. 115(7), 1066–1074 (2020).
• Demonstrated that maintaining bilirubin levels at or below 0.6 times the upper limit of normal and normalizing alkaline phosphatase are associated with improved survival outcomes in PBC, suggesting refined treatment targets to improve patient prognosis.
19.
Gatselis NK, Goet JC, Zachou K et al. Factors associated with progression and outcomes of early stage primary biliary cholangitis. Clin. Gastroenterol. Hepatol. 18(3), 684–692 (2020).
20.
Corpechot C, Carrat F, Gaouar F et al. Liver stiffness measurement by vibration-controlled transient elastography improves outcome prediction in primary biliary cholangitis. J. Hepatol. 77(6), 1545–1553 (2022).
21.
Mayne TJ, Vittinghoff E, Chesney MA, Barrett DC, Coates TJ. Depressive affect and survival among gay and bisexual men infected with HIV. Arch. Intern. Med. 156(19), 2233–2238 (1996).
22.
Kuiper EM, Hansen BE, de Vries RA et al. Improved prognosis of patients with primary biliary cirrhosis that have a biochemical response to ursodeoxycholic acid. Gastroenterology 136(4), 1281–1287 (2009).
23.
Tanaka A. Current understanding of primary biliary cholangitis. Clin. Mol. Hepatol. 27(1), 1–21 (2021).
24.
Lammers WJ, Hirschfield GM, Corpechot C et al. Development and validation of a scoring system to predict outcomes of patients with primary biliary cirrhosis receiving ursodeoxycholic acid therapy. Gastroenterology 149(7), 1804–1812; e1804 (2015).
25.
Poupon RE, Lindor KD, Cauch-Dudek K, Dickson ER, Poupon R, Heathcote EJ. Combined analysis of randomized controlled trials of ursodeoxycholic acid in primary biliary cirrhosis. Gastroenterology 113(3), 884–890 (1997).
26.
Poupon RE, Poupon R, Balkau B. The UDCA-PBC Study Group. Ursodiol for the long-term treatment of primary biliary cirrhosis. N. Engl. J. Med. 330(19), 1342–1347 (1994).
27.
Poupon RE, Balkau B, Eschwege E, Poupon R. UDCA-PBC Study Group. A multicenter, controlled trial of ursodiol for the treatment of primary biliary cirrhosis. N. Engl. J. Med. 324(22), 1548–1554 (1991).
28.
Pares A, Caballeria L, Rodes J. Excellent long-term survival in patients with primary biliary cirrhosis and biochemical response to ursodeoxycholic acid. Gastroenterology 130(3), 715–720 (2006).
29.
Lindor KD, Therneau TM, Jorgensen RA, Malinchoc M, Dickson ER. Effects of ursodeoxycholic acid on survival in patients with primary biliary cirrhosis. Gastroenterology 110(5), 1515–1518 (1996).
30.
Heathcote EJ, Cauch-Dudek K, Walker V et al. The Canadian multicenter double-blind randomized controlled trial of ursodeoxycholic acid in primary biliary cirrhosis. Hepatology 19(5), 1149–1156 (1994).
31.
Murillo Perez CF, Fisher H, Hiu S et al. Greater transplant-free survival in patients receiving obeticholic acid for primary biliary cholangitis in a clinical trial setting compared to real-world external controls. Gastroenterology 163(6), 1630–1642 (2022).
• Used real-world data to demonstrate that obeticholic acid treatment is associated not only with a reduction in surrogate markers but also improved transplant-free survival in patients with PBC, highlighting the importance of using surrogate markers and real-world evidence in assessing long-term efficacy in PBC.
32.
Khakoo NS, Sultan S, Reynolds JM, Levy C. Efficacy and safety of bezafibrate alone or in combination with ursodeoxycholic acid in primary biliary cholangitis: systematic review and meta-analysis. Dig. Dis. Sci. 68(4), 1559–1573 (2022).
33.
Myers RP, Shaheen AA, Fong A et al. Validation of coding algorithms for the identification of patients with primary biliary cirrhosis using administrative data. Can. J. Gastroenterol. 24(3), 175–182 (2010).
34.
Gish RG, MacEwan JP, Nair R et al. Burden of illness for patients with primary biliary cholangitis in the United States. Presented at: Gastroenterology & Hepatology Advanced Practice Providers Annual Conference. National Harbor, MD (7–9 September 2023).
35.
Brookhart A, Coombs C, Breskin A et al. Results of the HEROES Study: treatment efficacy of obeticholic acid on hepatic real-world outcomes in patients with primary biliary cholangitis [abstract 223]. Hepatology 76(Suppl. 1), S195–S196 (2022).
36.
Kowdley KV, Brookhart MA, Hirschfield G et al. Efficacy of obeticholic acid (OCA) vs placebo and external control (EC) on clinical outcomes in primary biliary cholangitis (PBC) [abstract 5032]. Hepatology 77(5), E144–E146 (2023).
37.
Kowdley KV, Hirschfield G, Mayne T et al. Clinical trial and real-world outcomes in patients with primary biliary cholangitis treated with obeticholic acid per current US label [abstract 4538-C]. Presented at: The Liver Meeting. Boston, MA (12–14 November 2023).
Information & Authors
Information
Published In
Copyright
© 2025 Intercept Pharmaceuticals, Inc. This work is licensed under the Creative Commons Attribution 4.0 License
History
Received: 15 November 2024
Accepted: 17 October 2025
Published online: 18 November 2025
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Association of liver biomarker values beyond current thresholds and negative clinical outcomes in primary biliary cholangitis: analysis of a real-world healthcare claims database. (2025) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2024-0198
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Devi Manoharan, Neural Network-Driven Optimization of Quality Engineering Metrics for High-Volume Healthcare Claims and EDI Transaction Performance, 2026 9th International Conference on Trends in Electronics and Informatics (ICOEI), 10.1109/ICOEI68323.2026.11541655, (2194-2203), (2026).