Acceptability and consumers' willingness to pay for comprehensive medication management services in Brazil
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Comprehensive medication management (CMM) is a clinical service that aims to optimize the therapeutic results of patients at the individual level. Studies carried out in Brazil and in several parts of the world have found a positive impact of the service, mainly in the resolution of drug therapy problems and in improving clinical outcomes and patients' quality of life. This service is not widespread and its acceptability and willingness to pay were not defined by the population yet. Objective: This work aims to conduct a study with users of private health services to determine the acceptability and willingness to pay for CMM services. Methods: This is a cross-sectional survey conducted through face-to-face interviews, among residents over 18 years of age of the metropolitan region of Belo Horizonte, capital of Minas Gerais State, Brazil. Results: For this study, 563 individuals were interviewed. Most respondents were female (55.1%), had completed high school (46.8%) and were employed (62.5%). The acceptability for the service was 93,25%, and among all respondents, 37 would not accept the service even if it was free. The amount of consumers' willingness to pay for the CMM service was estimated at $17.75 (40.00 BRL). Conclusion: The research results show that most people are willing to pay for the CMM service. This study can contribute to the decision-making regarding the implementation and pricing of the service in Brazil.
Tweetable abstract
Study examines willingness to pay for comprehensive medication management (CMM) services in Brazil, with findings that may assist healthcare administrators and insurers in implementing and pricing CMM services.
Plain language summary
What is this article about?
This article discusses a medical service called comprehensive medication management (CMM), which aims to make sure patients get the best results from their medications. Studies from different parts of the world, including Brazil, have shown that this service can solve problems related to medications and improve the health and quality of life of patients. However, not many people use this service, and it is not clear if people would be interested in using it or how much they would be willing to pay for it. So, researchers did a study in Belo Horizonte, Brazil, where they asked over 18-year-old residents about their thoughts on CMM.
What were the results?
They found that most of the 563 people they interviewed were okay with using this service, with about 93% of them saying they would be interested. Only 37 people out of all respondents said they would not want the service, even if it was free. The study also estimated that on average, people would be willing to pay about $17.75 (which is around 40.00 Brazilian Reals) for the CMM service.
What do the results of the study mean?
The study suggests that a lot of people are open to using the CMM service and are willing to pay for it. These findings could help health authorities in Brazil decide how to offer and price this service to benefit more people.
Comprehensive medication management (CMM) services are healthcare services that aim to evaluate not only the patient's medication list but the individual as a whole, focusing on how each medication is utilized and experienced by the patient in his daily life. The service's goal is to guarantee that each medication in use is appropriately indicated, the most effective and the safest considering all the patient's medical conditions, and that the patient can and should use the treatment as recommended [1]. The CMM service follows the theoretical and methodological framework of pharmaceutical care practice [1,2]. Pharmaceutical care practice provides a rational and standardized decision-making process that makes the work of clinical pharmacists comprehensive, reproducible and applicable to any healthcare context [1–3]. Besides the technical part, the framework of pharmaceutical care practice also describes the philosophy of practice that should be the foundation of the clinical work of the pharmacist, which includes a patient-centered, holistic and interdisciplinary approach to patient care [2].
In a private consultation, the pharmacist practitioner collects patient information, identifies drug-related problems, develops care plans to prevent and resolve drug-related problems and follows up with the patient to reach the best possible health outcomes. This work happens in collaboration with the healthcare team [1,2].
It is important to mention that CMM is the term first utilized in the PCPCC document, in accordance with the work of Cipolle et al. [2]. Before that, the service that follows the framework of pharmaceutical care practice was called medication therapy management (MTM). However, it should be highlighted that not all the published work that uses the term MTM refers to pharmaceutical care practice. However, all the cited studies in this manuscript that use the term MTM follow the theoretical framework of pharmaceutical care practice.
Many studies around the world and in Brazil have shown positive clinical, economic and humanistic outcomes of CMM services, which might justify their implementation and expansion in the healthcare system [4–16].
CMM is still not widespread, especially in developing countries like Brazil, despite the aggregate benefits already known [6–8,10,11,13,14]. Considering its low diffusion, the willingness to pay (WTP) for the service is a factor to be taken into account in its implementation within the health system. In these countries, the professional acts, for the most part, in dispensing and control of drug inventory, and the clinical performance still needs to be recognized and disseminated [11,13,14].
Currently, in Brazil, the CMM service is not incorporated in the list of procedures of the National Agency of Supplementary Health (ANS) in the scope of health plans [17]. Thus, in situations where it is necessary to define the price to be charged for a service that is not yet available on the market, it is possible to use the contingent valuation method to ascertain the monetary value that a consumer would pay for the benefit. In this type of situation, a hypothetical market situation is developed and questionnaires are used asking individuals the maximum amount they would pay for the service, thus discovering the WTP. Economists consider contingent valuation to be a method with a solid theoretical basis and is considered today as the standard method in the process of economic valuation of environmental and health resources [18–20].
Faced with a scenario in which resources are limited, economic assessments become essential to assist in decision-making for the sustainability and efficiency of health systems, whether they are public or not. Among these evaluations, WTP stands out, which aims to estimate the maximum value that an individual is willing to allocate to a health service or technology that will bring benefits to the individual in a hypothetical scenario [21,22]. The motivation for the elaboration of this study was to foster the discussion on the offering of CMM in Brazil since there is a scarcity of production on this topic, bibliography to define the price to be practiced and implementation of the service in the country. Thus, this study aimed to estimate the consumer's WTP for the CMM service in Brazil through questionnaires prepared using the contingent valuation method.
Methods
Design of study
This is a contingent valuation method used to determine the WTP for CMM services [23]. To determine the anchor price to be used in the questionnaire, the perspective of users who have health insurance was considered [24]. In this hypothetical scenario, the CMM service would be available by health insurers, so, as a basis for calculation, the average price of $31.06 (70.00 BRL) paid by insurers for outpatient medical care in 2017 was used [25,26]. The calculation of the average percentage incidence that the beneficiary would pay in case of using the service was based on an ANS publication, suggesting that the co-payment charge should not be greater than 40.0% of the monetary value of the service paid by the health insurance to the health providers [25,26]. Thus, two initial amounts of $9.32 (21.00 BRL) and $15.53 (35.00 BRL) were established as an additional fee for the CMM service in the hypothetical scenario created for the questionnaire. The questionnaires with even identifier codes contained the value of $15.53 (35.00 BRL) and the odd $9.32 (21.00 BRL) (Supplementary Materials). The use of two values aimed to reduce the impact of the anchor effect caused by bidding game techniques [27].
Study location
The research was conducted in the metropolitan region of Belo Horizonte, the capital of the state of Minas Gerais, Brazil. According to the demographic census conducted by the Brazilian Institute of Geography and Statistics (IBGE), the estimated population of Belo Horizonte was approximately 2,521,564 inhabitants and the municipal human development index (MHDI) was 0.810, whereas in Brazil, in the same reference period, the human development index (HDI) was 0.726 [28,29]. According to the National Supplementary Health Agency (ANS), which regulates private health insurance in Brazil, the coverage of private health insurance across the country in September 2023 includes 50,837,633 beneficiaries. In the state of Minas Gerais, 5,667,165 beneficiaries are covered, with 1,262,327 based in the metropolitan region of Belo Horizonte [30]. Brazil has a public and private health system. The private system is paid by companies or individuals, which pay, most of the time, a fixed and variable part, depending on the use of the services [31].
Respondents answered a questionnaire prepared by the research group according to other studies previously published [22,32–34]. The interviews were conducted from April to July 2019, by previously trained undergraduate students of Pharmacy from the Faculty of Pharmacy of the Federal University of Minas Gerais.
Data collection instrument
The methodology for estimating the WTP involved the application of a questionnaire [32,33,35] (Supplementary Materials) including the presentation to the respondent of all technical and clinical aspects of the CMM service. Previously, all interviewers were trained to ensure that the interviewees received the same information regardless of the interviewer. Before starting the data collection of the structured interview, all the interviewees' doubts about the research topic were elucidated [21,22,36].
The questionnaire (Supplementary Materials) was divided into six sections [36]. In section I, the questions were designed in a way to identify what was the participants' knowledge about the CMM service and if they understood the functioning of co-payment in a health insurance plan. In section II, there were questions to ascertain whether the participant understood the context and the information provided. In item III, the questions deal with the acceptability of including the CMM service through co-payment. If the participant accepted the inclusion of the service through co-payment (IV.A), the interviewer would proceed with questions consisting of discrete choice, a bidding game and an open question. If the participant did not accept the service using co-payment (IV.B), the following questions would ask if the participant would accept the service free of charge and, if the participant did not accept it, what the reasons are for declining. In item V, the participants were asked whether they would accept to pay the service for some family member and if so, for which family member. Finally, in part VI, a self-reported socioeconomic questionnaire was conducted [35].
In section IV, respondents answered a discrete choice question about their WTP of $9.32 (21.00 BRL) or $15.53 (35.00 BRL) for co-payment in an appointment of the CMM with a healthcare professional. Section IV.A1 and IV.A2 were questions involving higher or lower amounts compared with $9.32 (21.00 BRL) or $15.53 (35.00 BRL), depending on the WTP for CMM service of section IV.A (Supplementary Materials). At the end of item IV.A, respondents answered an open question about the maximum amount associated with their willingness to pay. All information relevant to the CMM including its objectives, benefits, and functions was included in the questionnaire.
Sampling & selection criteria
To perform the sample calculation, a margin of error of 5% was considered in a 95% confidence interval in estimating the percentage of acceptance of the service. Considering the scenario of greatest uncertainty, in which this percentage would be around 50%, the sample size was calculated as 400 respondents. To participate in the research, the interviewers approached people on the main circulation routes, markets and fairs in the metropolitan region of Belo Horizonte. The participation of all individuals in the research was voluntary.
As inclusion criteria for participants in the research, it was necessary to declare to be aged ≥18 years and to have health insurance. The latter is assumed so that the scenario would be more realistic. The reliability of WTP depends on how real the situation is for respondents. In line with previous publications, participants who demonstrated a WTP more than twice the amount of their declared monthly income were excluded from the analysis [21,32,33].
Data analysis
The median of WTP values was estimated only among respondents who declared willing to pay any amount greater than zero. Thus, respondents who did not accept the inclusion of the service through co-payment were excluded from the analysis of WTP but continued in the sensitivity analysis to verify the possible variables correlated with non-acceptance. Median values are generally used in the analysis of WTP to reduce the influence of lower and higher values obtained during data collection (outliers) [21].
Non-parametric tests (Mann-Whitney or Kruskal-Wallis) were used to compare the median values between the groups defined by qualitative covariates, considering a significance level of 5%. Scatter plot and Spearman coefficient were used to analyze the correlation between WTP and quantitative covariates.
Results
Characteristics of the population
The study was carried out with 563 individuals, aged between 18 and 84 years, who agreed to answer the questionnaire. The average age of the interviewees was 40 years (SD = 17), 54.9% were women, 62.5% were employed at the time of the interview, 46.9% had completed high school, and 51.3% had a corporate health plan (Table 1).
| Variable | n | % |
|---|---|---|
| Age in years, mean (SD) | 40 | (17) |
| Sex | ||
| Male | 251 | 44.6 |
| Female | 309 | 54.9 |
| Not answered | 3 | 0.5 |
| Education level | ||
| Had never attended school | 6 | 1.1 |
| Completed primary education | 56 | 9.9 |
| Completed high school | 264 | 46.9 |
| Completed bachelor's degree | 148 | 26.3 |
| Completed postgraduate degree | 88 | 15.6 |
| Not answered | 1 | 0.2 |
| Employment status | ||
| Employee | 350 | 62.2 |
| Not working | 139 | 24.7 |
| Retired | 71 | 12.6 |
| Not answered | 3 | 0.5 |
| Health insurance type of plan | ||
| Employer-sponsored health insurance | 289 | 51.3 |
| Individual health insurance | 241 | 42.8 |
| Not answered | 33 | 5.9 |
| Family income (number of minimal wages)† | ||
| ≤1 | 168 | 29.8 |
| >1 to ≤2 | 168 | 29.8 |
| >2 to ≤3 | 54 | 9.6 |
| >3 to ≤5 | 56 | 9.9 |
| >5 to ≤10 | 42 | 7.5 |
| >10 to ≤20 | 11 | 2.0 |
| Not answered | 64 | 11.4 |
| Noncommunicable diseases | ||
| Yes | 164 | 29.1 |
| No | 388 | 68.9 |
| Not answered | 11 | 2.0 |
†
Brazilian minimum wage in 2019: $442.88 (998.00 BRL).
SD: Standard deviation.
Willingness to pay for comprehensive medication management
Of the 563 respondents, 371 (65.9%) were eligible for the analysis of WTP. They would accept the CMM service through co-payment whereas 192 were not included in the WTP analysis because they were not willing to pay for the service. Respondents who accepted the service through co-payment were aged between 18 and 84 years (mean = 39, SD = 16), 198 (53.4%) were women, 171 (46.1%) had completed high school, 246 (66.3%) were employed and 195 (52.6%) had a corporate health plan, and 278 (74.9%) received more than twice the minimum wage.
Using the discrete choice technique, it was found that 314 (84.6%) WTP $12.43 (28.00 BRL) for the CMM service. In the bidding game, the interviewees were WTP from $0.29 (0.66 BRL) to $497.02 (1,120.00 BRL). In the open question, it was demonstrated that the value associated with WTP for the CMM service ranged from $0.29 (0.66 BRL) to $221.88 (500.00 BRL), thus presenting a median of $17.75 (Figure 1). Survey participants reported paying an additional fee (co-payment) for medical consultation in their health plan, mostly between $8.88 (20.00 BRL) and $15.98 (36.00 BRL), in which $14.64 (33.00 BRL) was the average rate disbursed.
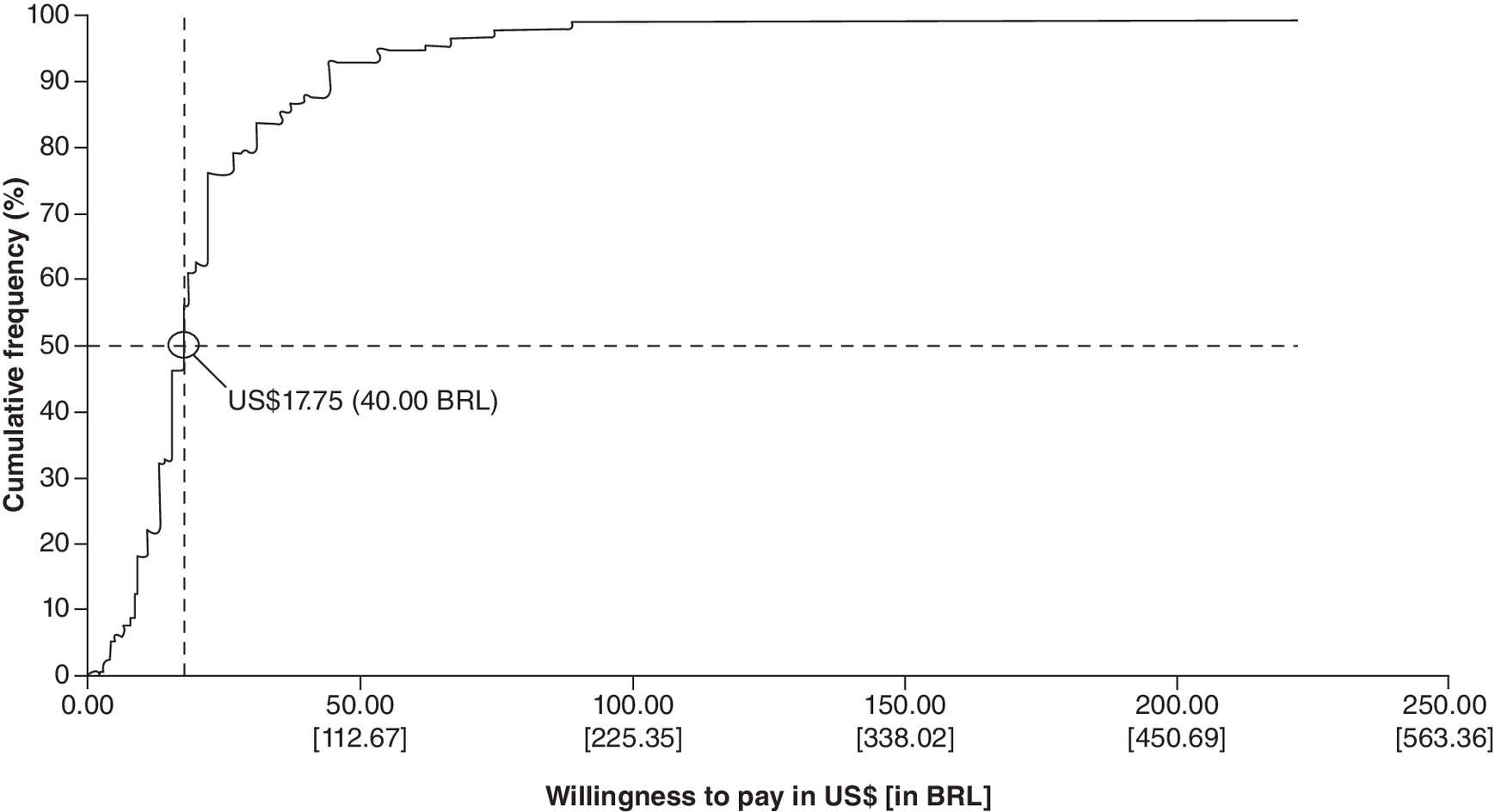
Figure 1. Cumulative percentage of willingness to pay by Brazilian consumers of private health services for the comprehensive medication management services according to maximum values reported.
BRL: Brazilian real.
There was statistical significance when comparing the amount paid for CMM service of those “working” with “not working” (p = 0.0087) and those “not working” with “retired” (p = 0.0211). The amount of co-participation paid by the respondents in a medical consultation compared with the maximum amount they would be WTP for CMM service has a positive linear relationship between the variables (Spearman's coefficient s = 0.3614; p = 0.0002) (Figure 2).
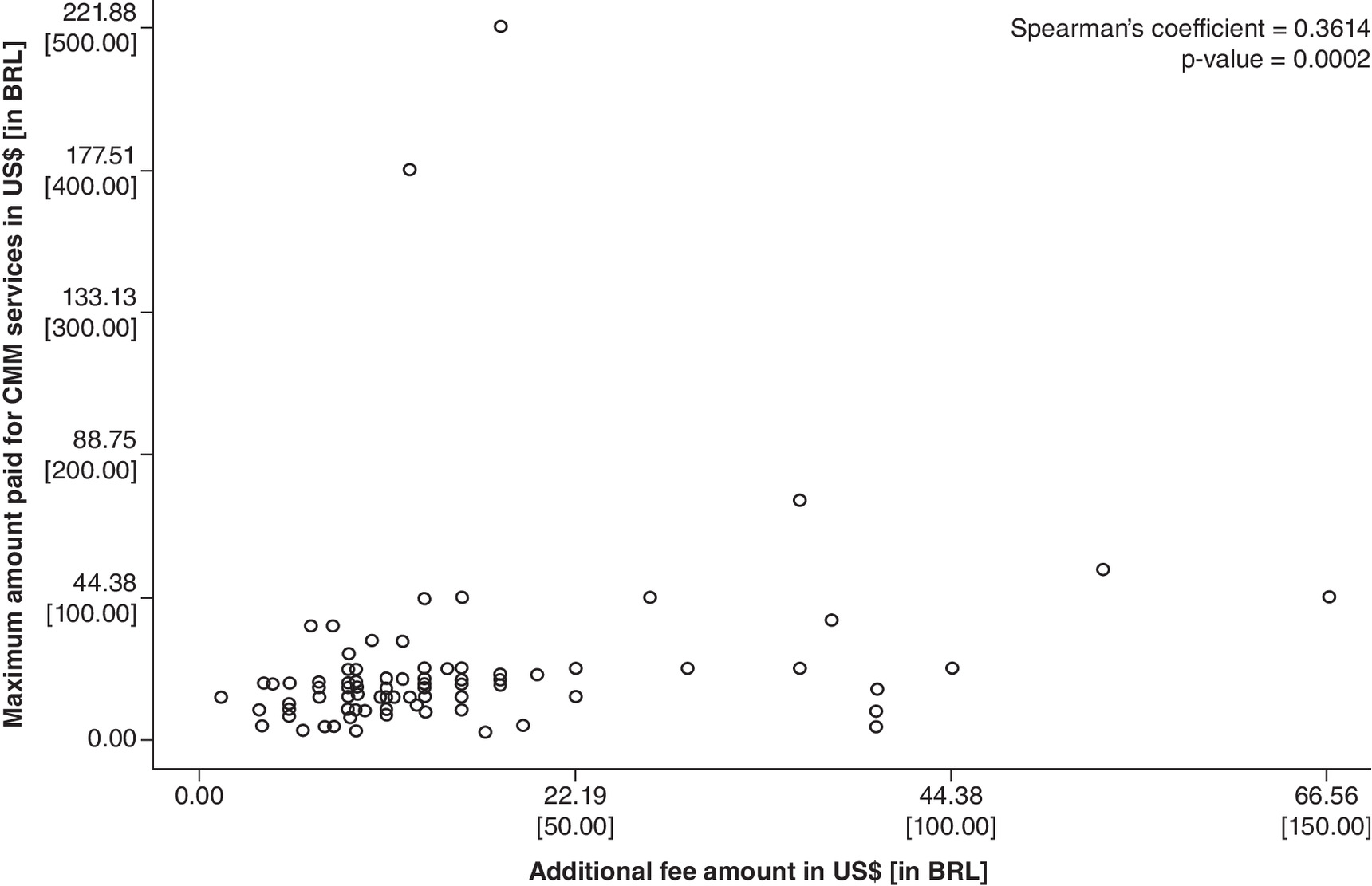
Figure 2. Scatter plot of additional fee versus maximum fee paid by Brazilian consumers for the comprehensive medication management services in a private health context.
BRL: Brazilian real; CMM: Comprehensive medication management.
The age of the interviewees correlates with the variable of the maximum amount they would pay for the service, showing a negative linear relationship between the variables (Spearman coefficient s = -0.206, p = 0.0001) (Figure 3).
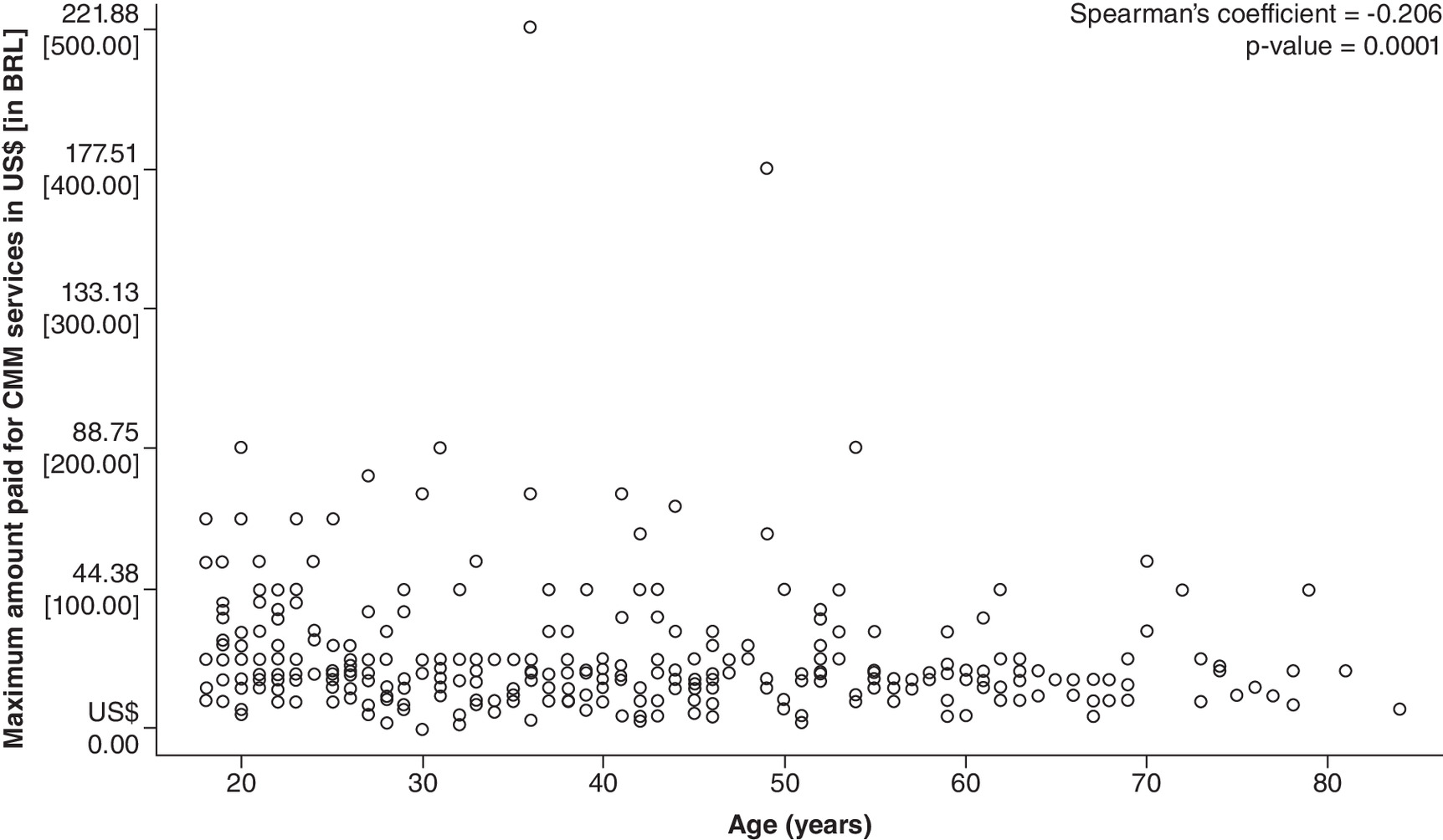
Figure 3. Dispersion graph of the age of Brazilian consumers of private health services who would accept the comprehensive medication management service versus the maximum amount they would pay for services.
BRL: Brazilian real; CMM: Comprehensive medication management.
There are possible values that can be considered outliers about the amount of WTP for the CMM service, as these values compromise a large part of the interviewees' per capita income. Furthermore, the data is asymmetric, with the majority of people compromising low values of per capita income. The average percentage that individuals are willing to commit to their income is 4.8%. Most individuals compromise values between 1.0% and 6.5%, but some individuals are willing to compromise values close to 0.1% or very high values reaching 80.0% (Figure 4).
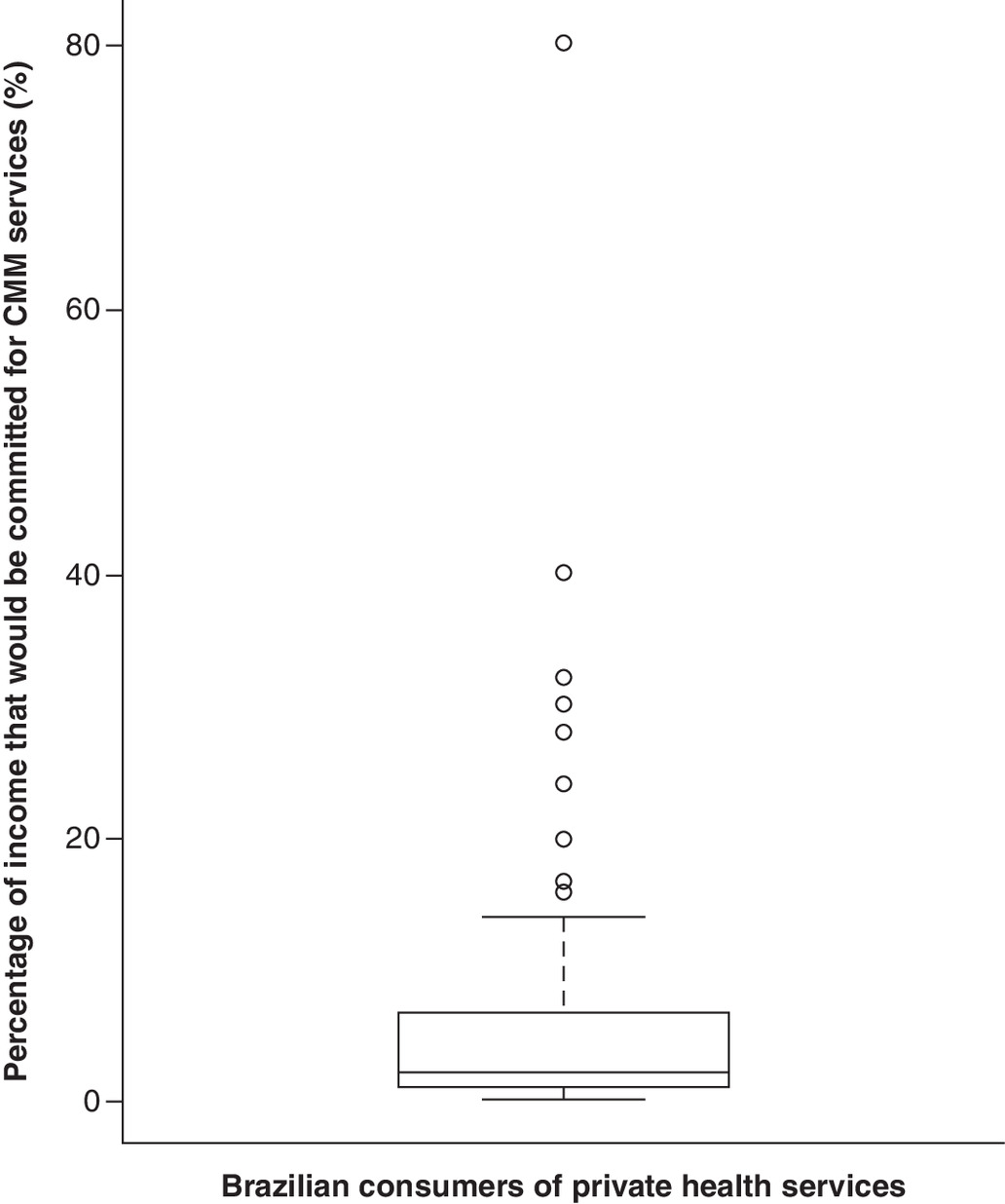
Figure 4. Percentage that Brazilian consumers of private health services would commit to their income to have access to the comprehensive medication management service.
CMM: Comprehensive medication management.
There was a statistical difference in the median between the amount willing to pay for CMM service and the per capita income of different age groups (p = 0.0011). The other variables and their respective p values were: “elementary school” with “high school” (p = 0.0001); “higher education” with “high school” (p < 0.001); types of occupation (p = 0.0026); “works” with “does not work” (p = 0.0016) and “does not work” with “retired” (p = 0.0052). Men are willing to commit from 0.093 to 40.0% of their per capita income, while women are willing to commit from 0.1 to 80.0%. Most male individuals chose to allocate from 1.0 to 6.0% of income to the additional fee for therapy, whereas female individuals chose to allocate from 1.4 to 7.0%. The median of the commitment to income impairment related to CMM service between women and men is significantly different (p = 0.0074).
Acceptability of the comprehensive medication management service through co-payment
Of the 563 participants who answered the questionnaire, 370 (65.9%) would accept the service through co-payment and 192 (34.1%) would not accept the service through co-payment. Statistical tests were carried out to verify the probability of acceptance or not of the CMM service and there were statistically significant differences between educational levels (elementary school, high school and higher education) regarding the acceptance of the co-payment of therapy (p = 0.0073), occupations (working, not working and retired) in relation to the acceptance of the co-payment management of drug therapy (p = 0.0086), and participants who believe that the pharmacist is responsible for the service with respondents who think that another professional is responsible for providing the service (p = 0.0217).
Additionally, from the 192 (34.1%) respondents would not accept the service through co-payment 155 (80.7%) would accept the service if it had no cost. However, 37 (19.3%) would not accept it even if there was no cost and the main reasons for non-acceptance include not seeing the service's usefulness (40.5%), preference to be accompanied by the doctor (29.7%), not believing that someone would do it free of charge (2.7%), lack of time for other consultations (2.7%), not using medication (2.7%), would only use it in extreme cases (2.7%), do not see a need in the service (2.7%), and for other reasons (16.2%). Comparing the 155 respondents who would accept the service for free versus the 32 who don't, were found differences in proportions between the different age groups (p = 0.0030), levels of education (elementary school, high school, and complete higher education) (p = 0.0242), types of occupation (working, not working and retiring) (p = 0.0001) and whether or not they have family members with chronic illness (p = 0.0080).
Discussion
To our knowledge, this is the first Brazilian study that evaluates the acceptability, sociodemographic predictors, and the WTP users of private health plans for CMM service. This data is essential for managers and administrators of hospitals and health insurers due to the importance that this type of service has, not only because of the benefits in the quality of life of the patients who use it but also in the financial advantages for hospitals, health plans and for patients [39]. With the reduction of problems related to medication use, faced in other studies, is possible to have a decrease in the number and length of hospital stays [39] – which is an important hospital problem due to the reduced number of hospital beds [40].
The study estimated the WTP of Brazilian consumers by the CMM service to foster the discussion about CMM in Brazil. There are still no studies published from the perspective of the Brazilian population to compare the results obtained by this study regarding the willingness of Brazilian individuals to use, for a fee, the CMM service performed by health professionals. However, in line with previous studies [41], the results of this research demonstrate that most participants are willing to pay for CMM services.
Most participants (65.9%) eligible for WTP analysis were willing to pay for the CMM service. The median value of $17.75 (40.00 BRL) that the participants were willing to pay is promising and higher than the estimate reported by another study from Jordan ($3.95), an upper middle-income country like Brazil [41,42], but less than the median value estimated in a study conducted in high-income countries [43,44]. These differences in the median values that the population is willing to pay for CMM service may reflect the greater economic power of the population and/or demonstrate that the participant's understanding of the benefits that these services can bring, for example, a greater understanding of treatments, greater knowledge about the medications used and, consequently, greater adherence to medications and improved quality of life directly impacts the WTP for these services [45,46].
Undoubtedly, many factors can influence the participants' WTP. This study demonstrated that women compared with men are willing to commit different percentages of their income for the CMM service (p = 0.0074). This can be justified by the fact that women use health services more and are associated with higher charges than men [47]. Age also proved to be an important factor, given that the higher the age of the interviewees, the lower the maximum amount paid for the service (p = 0.0001). Thus, more studies may be needed to investigate the factors associated with lower WTP in older people. Education is another variable that affected the maximum amount paid since the participants with higher education have a greater willingness to accept the CMM service (p = 0.0073). In contrast, a study that evaluated the acceptability of the CMM service in USA found that individuals with higher education had a lower rate of acceptability of the service [12]. Such results should be explored in future research, as the social and economic differences between countries may influence the largest WTP found in the present research. The results also demonstrated that the per capita income of the different age groups (p = 0.0011) influenced WTP, which is not surprising since it is expected that individuals who have a higher family income are more willing to commit a higher value for service than those with less purchasing power. Additionally, if per capita income is a factor influencing WTP, a more even distribution of purchasing power in a country like Brazil might impact the accessibility and acceptance of CMM services. If the price is not attractive to the majority of the population, the service could become highly segmented.
Among the people who would pay for the service, the median value of $17.75 (40.00 BRL) paid for CMM service is above the average value of $14.64 (33.00 BRL) that participants already pay as an additional fee (co-payment) for a medical consultation at their health plan. It was found that the higher the amount of co-payment paid by respondents in a medical consultation, the higher the maximum amount they would be willing to pay for the CMM service (p = 0.0002). This can be justified by the anchor effect, in which users who are exposed to higher prices of co-participation tend to pay higher amounts at this rate. In addition, as the CMM service is implemented and users learn more about the benefits of the service and the risks arising from problems related to medication use, the WTP for these users could increase.
Although approximately 34% of respondents would not pay for the service, most of them (80.7%) would use the service if it was offered free of charge. However, 19.3% would not accept the service even if it was free. These non-acceptance results are crucial to exploring ways to improve understanding and discussions about the CMM service. In a study conducted by Schumacher et al. [48]. it was demonstrated that previous experience with the CMM service increases the likelihood of using the service again. Therefore, action by health insurers to implement a limited number of free CMM consultations would possibly have a positive impact on adherence to the service, thus generating a new perception of value among users who are not interested in initially paying for the service.
As previously reported, a semi-Markov [49] model showed that CMM service is cost-effective in managing hypertension from the perspective of the US payer. Furthermore, it is estimated that the implementation of CMM will result in cost savings by reducing expenses resulting from non-optimized pharmacotherapy and there will be resolution of drug therapy problems, which can bring better therapeutic results to the patient due to the high-quality care process CMM services can offer [50]. Therefore, the WTP found in the present study can contribute to setting the price of the service by health insurers, aiming to foster the performance of health professionals in the provision of CMM services, and can contribute to possible economic modeling, aiming to assess the cost–effectiveness of the service.
Limitations & strengths
The main limitations of the work are inherent to the WTP methodology. One of these limitations is related to the anchor effect, which despite the attempt to minimize it using two initial values, can still have effects on the estimate of WTP. Another limitation is related to the likely overestimation of respondents when declaring WTP in declared preference surveys compared with the results of revealed preference surveys (real-world situations). This overestimation is recognized by some authors as budget constraint bias, in which, when considering the same intervention about other options, there is a different WTP than that found when evaluating a product or service in isolation [51].
In this study, the distribution of income from the respondents in the metropolitan region of Belo Horizonte ranges differ from the results presented by the IBGE, whose data indicates that the highest proportion of people who have health insurance are in the income range of more than five minimum wages, with the highest proportion of people with health insurance was in the income range of less than one minimum wage up to two minimum wages [52]. Therefore, the WTP may be underestimated, due to the predominance of a lower income range than the Brazilian population and this study may vary if applied to other scenarios in Brazil. However, this study demonstrates high methodological rigor, employing robust statistical analyses and featuring a substantial sample size of 563 individuals. The cross-sectional survey, with detailed demographic information, enhances analytical depth, ensuring reliability and validity in understanding acceptability and willingness to pay for CMM services among private health service users in Brazil.
Conclusion
Most participants were willing to accept and pay the median value of $17.75 (40.00 BRL) for the CMM service. The WTP varies in age, educational level, occupation, sex, and amount of co-participation paid by the respondents to a health insurance. Given the clinical and economic benefits that the service has presented over time, there is a need to consider expanding its use, so that more individuals could benefit. While our study underscores current acceptance and willingness to pay among insured individuals, future research is crucial to assess CMM's real-world impact on long-term patient well-being, healthcare utilization and economic outcomes. This unprecedented study can guide decision-makers in implementing and pricing CMM services effectively.
Summary points
•
The study examines the willingness to pay (WTP) for Comprehensive Medication Management (CMM) services in Brazil.
•
The majority of participants (65.9%) were willing to pay for CMM, with a median WTP of $17.75 (40.00 BRL).
•
Factors influencing WTP included age, education level, occupation, sex and the amount of co-payment for medical consultations.
•
The findings can assist healthcare administrators and insurers in implementing and pricing CMM services.
Author contributions
LL Tôrres, D Ramalho-de-Oliveira, EA Reis, IPD Godói, AA Guerra Júnior and CM Ruas were responsible for study conception and design; LL Tôrres was responsible for acquisition of data; LL Tôrres and EA Reis were responsible for data analysis; LL Tôrres, D Ramalho-de-Oliveira, EA Reis, IPD Godói, AA Guerra Júnior, PS Azevedo, TTR Sarmento and CM Ruas were responsible for drafting and final revision of the manuscript.
Acknowledgments
The authors thank all the 29 volunteer interviewers for their enthusiasm and the 563 respondents for their contribution to this research.
Financial disclosure
Resources were indirectly received from the Collaborating Center of the SUS for Technology Assessment and Excellence in Health (Ccates), Coordination of Superior Level Staff Improvement (Capes) and National Council for Scientific and Technological Development (CNPq). The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Competing interests disclosure
The authors have no financial and/or nonfinancial competing interests or relevant affiliations with any organization/entity to declare that are relevant to the subject matter or materials discussed in this manuscript. This includes employment, grants or research funding, consultancies, membership on scientific or other advisory boards, honoraria, stock ownership or options, paid expert testimony, patents received or pending, or royalties.
Writing disclosure
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
Participants were approached by the interviewers and invited to participate in the research after reading the informed consent form (ICF). Participants who agreed to participate signed two copies of the ICF. The study was approved by the research ethics committee of the Federal University of Minas Gerais (COEP/UFMG) under the certificate of presentation for ethical appreciation (CPEA) no. 66860617.8.0000.5149.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary material.docx)
- Download
- 7.07 MB
References
Papers of special note have been highlighted as: • of interest
1.
Patient-Centered Primary Care Collaborative. The Patient-Centered Medical Home: Integrating Comprehensive Medication Management to Optimize Patient Outcomes (2012). https://thepcc.org/sites/default/files/media/medmanagement.pdf
2.
Cipolle R, Strand L, Morley P. Pharmaceutical Care Practice: The Patient-Centered Approach to Medication Management (3rd Edition). McGraw-Hill Education, NY, USA (2012).
3.
Hepler CD, Strand LM. Opportunities and responsibilities in pharmaceutical care. Am. J. Heal. Pharm. 47(3), 533–543 (1990).
4.
Isetts BJ, Schondelmeyer SW, Artz MB et al. Clinical and economic outcomes of medication therapy management services: the Minnesota experience. J. Am. Pharm. Assoc. 48(2), 203–214 (2008).
5.
Ramalho de Oliveira D, Brummel AR, Miller DB. Medication therapy management: 10 years of experience in a large integrated health care system. J. Manag. Care Pharm. 16(3), 185–195 (2010).
6.
Sá-Borges AP, Guidoni CM, Freitas O, Pereira LRL. Economic evaluation of outpatients with Type 2 diabetes mellitus assisted by a pharmaceutical care service. Arq. Bras. Endocrinol. Metab. 55(9), 686–691 (2011).
7.
Balisa-Rocha BJ, Guimarães VG, Mesquita AR, Aguiar PM, Krass I, de Lyra Júnior DP. Enhancing health care for type 2 diabetes in Northern Brazil: a pilot study of pharmaceutical care in community pharmacy. African J. Pharm. Pharmacol. 6(35), 2584–2591 (2012).
8.
Mourão AOM, Ferreira WR, Martins MAP et al. Pharmaceutical care program for Type 2 diabetes patients in Brazil: a randomized controlled trial. Int. J. Clin. Pharm. 35, 79–86 (2013).
9.
Viswanathan M, Kahwati LC, Golin CE et al. Medication therapy management interventions in outpatient settings. JAMA Intern. Med. 175(1), 76–87 (2015).
10.
Santos BD, Nascimento MMGD, de Oliveira GCB et al. Clinical impact of a comprehensive medication management service in primary health care. J. Pharm. Pract. 34(2), 265–271 (2021).
11.
Neto PRO, Marusic S, de Lyra Júnior DP et al. Effect of a 36-month pharmaceutical care program on the coronary heart disease risk in elderly diabetic and hypertensive patients. J. Pharm. Pharm. Sci. 14(2), 249–263 (2011).
12.
Brown LM, Rashrash ME, Schommer JC. The certainty in consumers' willingness to accept pharmacist-provided medication therapy management services. J. Am. Pharm. Assoc. 57(2), 211–216 (2017).
• Focuses on consumers' willingness to accept pharmacist-provided medication therapy management services.
13.
Mendonça S de AM, Melo AC, Pereira GCC et al. Clinical outcomes of medication therapy management services in primary health care. Brazilian J. Pharm. Sci. 52(3), 365–373 (2016).
14.
Detoni KB, Oliveira IV, Nascimento MMG, Caux TR, Alves MR, Ramalho-de-Oliveira D. Impact of a medication therapy management service on the clinical status of patients with chronic obstructive pulmonary disease. Int. J. Clin. Pharm. 39(1), 95–103 (2017).
15.
Brajković A, Bićanić LA, Strgačić M, Orehovački H, Ramalho-de-Oliveira D, Mucalo I. The impact of pharmacist-led medication management services on the quality of life and adverse drug reaction occurrence. Pharmacy (Basel) 10(5), 102 (2022).
16.
Brajkovíc A, Bosnar L, Nascimento MMG et al. Healthcare utilization and clinical outcomes in older cardiovascular patients receiving comprehensive medication management services: a nonrandomised clinical study. Int. J. Environ. Res. Public Health 19(5), 2781 (2022).
17.
Agência Nacional de Saúde Suplementar. Rol de Procedimentos e Eventos em Saúde (2018). http://www.ans.gov.br/images/stories/Plano_de_saude_e_Operadoras/Area_do_consumidor/rol/2020/anexo-i-rol-2018-alterado-pelas-rns-453-457-revogacao-458-460-2020-crn.pdf
18.
Mitchell R, Carson R. Using Surveys to Value Public Goods: The Contingent Valuation Method (1st Edition). Resources for the Future (RFF) Press, USA (1989).
19.
Johannesson M, Johansson P-O, Jönsson B. Economic evaluation of drug therapy: a review of the contingent valuation method. Pharmacoeconomics 1(5), 325–337 (1992).
20.
Painter JT, Gressler L, Kathe N, Slabaugh SL, Blumenschein K. Consumer willingness to pay for pharmacy services: an updated review of the literature. Res. Soc. Adm Pharm. 14(12), 1091–1105 (2018).
• A review of consumers' willingness to pay for pharmacy services, providing an updated analysis of the literature.
21.
Haab T, McConnell K. Valuing Environmental and Natural Resources: The Econometrics of Non-Market Valuation. Edward Elgar Publishing, UK (2002).
22.
Drummond M, Sculpher M, Claxton K, Stoddart G, Torrance G. Methods for the Economic Evaluation of Health Care Programmes (4th Edition). Oxford University Press, York, UK (2015).
23.
Wang J, Hong SH. Contingent valuation and pharmacists' acceptable levels of compensation for medication therapy management services. Res. Soc. Adm Pharm. 11(3), e121–e132 (2015).
• Focuses on pharmacists' acceptable levels of compensation for medication therapy management services using the contingent valuation method.
24.
Simonson I, Drolet A. Anchoring effects on consumers' willingness-to-pay and willingness-to-accept. J. Consum. Res. 31(3), 681–690 (2004).
25.
Agência Nacional de Saúde Suplementar. ANS define regras para cobrança de coparticipação e franquia em planos de saúde (2018). http://www.ans.gov.br/aans/noticias-ans/consumidor/4499-ans-define-regras-para-cobranca-de-coparticipacao-e-franquia-em-planos-de-saude
26.
Agência Nacional de Saúde Suplementar. Painel de Precificação: Planos de Saúde. Agência Nacional de Saúde Suplementar, Rio de Janeiro (2018). https://www.gov.br/ans/pt-br/arquivos/assuntos/consumidor/reajustes-de-mensalidade/reajuste-anual-de-planos-individuais-familiares/painel_de_precificacao_planos_de_saude_2017.pdf
27.
Furnham A, Boo HC. A literature review of the anchoring effect. J. Socio. Econ. 40(1), 35–42 (2011).
28.
Instituto Brasileiro de Geografia e Estatística (2021). https://cidades.ibge.gov.br/brasil/mg/belo-horizonte/panorama
29.
United Nations Development Programme. Human Development Report 2020 (2020). http://hdr.undp.org/sites/default/files/hdr2020.pdf
30.
Ministério da Saúde. Departamento de Informática do Sistema Único de Saúde (DATASUS). TabNet ANS (2023). https://datasus.saude.gov.br/home/tabnet/
31.
Paim J, Travassos C, Almeida C et al. The Brazilian health system: history, advances, and challenges. Lancet 377(9779), 1778–1797 (2011).
32.
Godói IP, Santos AS, Reis EA et al. Consumer Willingness to Pay for Dengue Vaccine (CYD-TDV, Dengvaxia®) in Brazil; Implications for Future Pricing Considerations. Front Pharmacol. 8, 41 (2017).
• Analyzes consumers' willingness to pay for a dengue vaccine in Brazil. It was the first study using the CV method in the health analysis in Brazil.
33.
Muniz Júnior RL, Godói IP, Reis EA et al. Consumer willingness to pay for a hypothetical Zika vaccine in Brazil and the implications. Expert Rev. Pharmacoecon. Outcomes Res. 19(4), 473–482 (2019).
34.
Sarmento TTR, Godói IP, Reis EA, Godman B, Ruas CM. Consumer willingness to pay for a hypothetical chikungunya vaccine in Brazil and the implications. Expert Rev. Pharmacoecon. Outcomes Res. 22(3), 513–520 (2022).
35.
Johnston RJ, Boyle KJ, Adamowicz W (Vic) et al. Contemporary guidance for stated preference studies. J. Assoc. Environ. Resour. Econ. 4(2), 319–405 (2017).
36.
Bryman A. Integrating quantitative and qualitative research: how is it done? Qual. Res. 6(1), 97–113 (2006).
37.
The World Bank. PPP conversion factor (2019). https://data.worldbank.org/indicator/PA.NUS.PPP?locations=BR
38.
Truong HA, Groves CN, Congdon HB, Dang DT, Botchway R, Thomas J. Potential cost savings of medication therapy management in safety-net clinics. J. Am. Pharm. Assoc. 55(3), 269–272 (2015).
39.
Winterstein AG, Sauer BC, Hepler CD, Poole C. Preventable drug-related hospital admissions. Ann. Pharmacother. 36(7–8), 1238–1248 (2002).
40.
O'Dwyer G, Konder MT, Machado CV, Alves CP, Alves RP. The current scenario of emergency care policies in Brazil. BMC Health Serv. Res. 13, 70 (2013).
41.
Jaber D, Aburuz S, Hammad EA, El-Refae H, Basheti IA. Patients' attitude and willingness to pay for pharmaceutical care: an international message from a developing country. Res. Soc. Adm Pharm. 15(9), 1177–1182 (2019).
• Investigates patients' attitudes and willingness to pay for pharmaceutical care, focusing on a developing country.
42.
World Population Review. Country Rankings. Middle-Income Countries 2023. https://worldpopulationreview.com/country-rankings/middle-income-countries
43.
Hanna A, White L, Yanamandram V. Patients' willingness to pay for diabetes disease state management services in Australian community pharmacies. Int. J. Pharm. Healthc. Mark. 4(4), 339–354 (2010).
44.
Woelfel JA, Carr-Lopez SM, Santos MD et al. Assessing Medicare beneficiaries' willingness-to-pay for medication therapy management services. Consult. Pharm. 29(2), 104–109 (2014).
• Examines Medicare beneficiaries' willingness to pay for medication therapy management services.
45.
Chisholm-Burns MA, Lee JK, Spivey CA et al. US pharmacists' effect as team members on patient care. Med. Care 48(10), 923–933 (2010).
46.
Tilton JJ, Edakkunnathu MG, Moran KM et al. Impact of a medication therapy management clinic on glycosylated hemoglobin, blood pressure, and resource utilization. Ann. Pharmacother. 53(1), 13–20 (2019).
47.
Bertakis KD, Azari R, Helms LJ, Callahan EJ, Robbins JA. Gender differences in the utilization of health care services. J. Fam. Pract. United States 49(2), 147–152 (2000).
48.
Schumacher L, Coe AB, Lester CA, Rothermal M, Dorsch MP. Factors that influence patient acceptance of clinical pharmacy services: a nationwide survey. J. Am. Pharm. Assoc. 60(6), 1058–1067; e4 (2020).
• Investigates factors that influence patients' acceptance of clinical pharmacy services.
49.
Schultz BG, Tilton J, Jun J, Scott-Horton T, Quach D, Touchette DR. Cost-effectiveness analysis of a pharmacist-led medication therapy management program: hypertension management. Value Health 24(4), 522–529 (2021).
50.
do Amaral PA, Mendonça S de AM, de Oliveira DR, Peloso LJ, Pedroso R dos S, Ribeiro MÂ. Impact of a medication therapy management service offered to patients in treatment of breast cancer. Brazilian J. Pharm. Sci. 54(2), e00221 (2018).
51.
Cookson R. Willingness to pay methods in health care: a sceptical view. Health Econ. 12(11), 891–894 (2003).
52.
Instituto Brasileiro de Geografia e Estatística. Pesquisa Nacional de Saúde 2019 (2020). https://biblioteca.ibge.gov.br/visualizacao/livros/liv101748.pdf
Information & Authors
Information
Published In
Copyright
© 2024 The Authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 2 August 2023
Accepted: 18 January 2024
Published online: 8 February 2024
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Acceptability and consumers' willingness to pay for comprehensive medication management services in Brazil. (2024) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2023-0127
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Vinícius Gonçalves Nogueira, Edna Afonso Reis, Brian Godman, Antony Paul Martin, Isabella Piassi Dias Godói, Acceptability and willingness to pay for a hypothetical HIV vaccine in Brazil and the implications: a cross-sectional study, Expert Review of Pharmacoeconomics & Outcomes Research, 10.1080/14737167.2024.2384543, 25, 1, (91-100), (2024).
- Jhoyce S. Souza, Edna A. Reis, Brian Godman, Stephen M. Campbell, Johanna C. Meyer, Luann W. P. Sena, Isabella P. D. Godói, Users’ Perceptions of Access to and Quality of Unified Health System Services in Brazil: A Cross-Sectional Study and Implications to Healthcare Management Challenges, International Journal of Environmental Research and Public Health, 10.3390/ijerph21060721, 21, 6, (721), (2024).
- Xinyue Zhang, Zhijia Tang, Yanxia Zhang, Wai Kei Tong, Qian Xia, Bing Han, Nan Guo, Knowledge, attitudes, and practices of primary healthcare practitioners regarding pharmacist clinics: a cross-sectional study in Shanghai, BMC Health Services Research, 10.1186/s12913-024-11136-3, 24, 1, (2024).