Use of interrupted time-series analyses in evaluating health economic outcomes following implementation of multilayer water-tight wound closure in a primary total joint arthroplasty population
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Total joint arthroplasty (TJA) with multi-layer, watertight closure (MLWC) using knotless barbed suture and 2-octyl cyanoacrylate plus polymer mesh tape was compared with conventional closure (CC) using Vicryl™ sutures and staples. Patients & methods: Electronic medical records of patients undergoing TJA (1574: total knee arthroplasty; 580: total hip arthroplasty; 13: unknown) from a single surgeon at a US hospital (CC 2011 to 2013; MLWC 2015 to 2020) were reviewed. Outcomes were length of stay (LOS), discharge to skilled nursing facility (SNF), 90-day surgical site infection (SSI) and 90-day readmission. Logistic regression controlled for baseline characteristics. Adjusted interrupted time series (ITS) analyses accounted for decreasing trends in LOS and SNF discharge over time. Results: Among 2167 TJA cases (mean [standard deviation] age 66.0 [9.7] years, 53.3% female), 906 received CC and 1261 received MLWC. Bivariate analysis showed no statistically significant differences in 90-day SSI rates; however, MLWC patients had 60% lower 90-day readmission rates (1.5 vs 3.8%, p < 0.05), 44% lower LOS (1.4 vs 2.5 days, p < 0.05) and 40% lower discharge rates to a skilled care facility (8.5 vs 14.1%, p < 0.05). Multivariable analyses showed CC patients were 2.45-times more likely to be readmitted within 90 days, 1.88-times more likely to be discharged to SNF and had 1.67-times longer LOS compared with MLWC. ITS analyses showed a sharp decline in LOS (0.9 days) and discharge to SNF (5.6% incidence) after implementation of MLWC, followed by no further changes for the remainder of the study period. Conclusion: MLWC was associated with ≥40% reduction in 90-day readmission, LOS and SNF discharge compared with TJA CC. LOS and discharge rate to SNF declined sharply after the implementation of MLWC.
Tweetable abstract
Study shows that advanced multi-layer, watertight closure (MLWC) in total joint replacement improved health economic outcomes.
Plain language summary
What is this article about?
Research evaluating the clinical and economic value of advanced multi-layer, watertight closure (MLWC) in total joint replacement is needed. This study compared the clinical and economic outcomes with advanced MLWC versus conventional closure (CC) for patients undergoing total joint replacement.
What were the results?
Patients who received CC had 1.67-times longer hospital length of stay, were 1.88-times more likely to be discharged from the hospital to a skilled nursing facility and 2.45-times more likely to be readmitted to the hospital within 90 days compared with patients who received MLWC. There was a sharp decline in hospital length of stay (0.9 days per patient) and discharge from the hospital to skilled nursing facilities (5.6% fewer patients) with the implementation of MLWC.
What do the results of the study mean?
Multiple quality of care and cost containment initiatives have been implemented for total joint replacement in recent years. Adoption of advanced MLWC rather than CC may result in improved health economic outcomes with total joint replacement.
Total hip arthroplasty (THA) and total knee arthroplasty (TKA) are valuable surgical treatments that improve motion and function, offer pain relief and enhance quality of life in patients with arthritis [1,2]. THA and TKA are among the most frequently performed surgical procedures in the US, and utilization is expected to increase in the coming decades [3–6]. While THA and TKA are typically very effective in improving pain and function with high survivorship and low morbidity and mortality, surgical site infection (SSI) is an important complication of total joint arthroplasty (TJA) as SSIs can increase morbidity, decrease patient satisfaction and increase hospital readmissions and healthcare costs [7,8].
It is estimated that approximately half of SSIs could be preventable if current evidence-based prevention strategies were employed [9]. US policymakers have attempted to improve quality of care and control healthcare costs by penalizing hospitals for readmissions and shifting risk to providers through consolidating payments in order to place limits on payment for specific treatments or periods. The Centers for Medicare and Medicaid Services' (CMS) Hospital Readmissions Reduction Program (HRRP) expanded its readmission penalties to include elective THA and TKA procedures in 2013. The Comprehensive Care for Joint Replacement (CJR) bundled payment model was implemented in April 2016 for Medicare beneficiaries undergoing hip or knee replacements. Evidence has shown that its implementation improved value, reflected in lower costs, decreased readmissions and complications, decreased hospital length of stay (LOS) and less discharge to post-acute facilities [10].
The occurrence of SSI has been shown to be affected by wound closure techniques and technologies [11–13]. While conventional sutures and staples are most commonly used for TJA procedures, integrated pathways incorporating multi-layer, watertight closure (MLWC) could increase the preventative effectiveness against joint prosthetic adverse events [14]. Among the barbed sutures that are available today, the Stratafix™ Knotless Tissue Control Devices (Ethicon, Inc., NJ, USA; henceforth ‘SFX KTCD’) comprise a portfolio of knotless barbed suture devices which can be used at various tissue layers, most of which are treated with IRGACARE® MP (triclosan) which inhibits bacterial colonization of the devices [15,16]. For superficial skin closure, 2-octyl cyanoacrylate adhesive combined with a polyester mesh (Dermabond® Prineo®, Ethicon, Inc.; henceforth ‘2OPM’) has been introduced to reinforce and share tension across a surgical incision [17]. Wounds dressed with mesh have shown decreased drainage compared with controls [18]. Wound drainage has been shown to contribute to delayed wound healing, decreased patient satisfaction, increased cost and increased risk of infection in TKA [17,19].
Research is needed to evaluate the clinical and economic value of advanced MLWC more thoroughly in THA and TKA. Given that multiple quality of care and cost containment initiatives have been implemented for THA and TKA in recent years, it is important to be able to differentiate whether observed changes in outcomes are due to the new technologies or interventions (e.g., MLWC) or due to background quality of care improvements. Interrupted time series (ITS) analysis is increasingly being advocated as a more robust design for evaluating healthcare quality improvement given its ability to control for biases [20–22]. ITS is a valuable study design for helping establish causality as it controls for pre-existing underlying short- and long-term trends by longitudinally tracking the outcome before and after an intervention [23,24]. Hence, the objective of this study was to use ITS analysis to compare health economic outcomes after THA and TKA when implementing MLWC using SFX KTCD and 2OPM compared with conventional closure (CC) using Vicryl™ sutures and staples.
Methods
Study population
This retrospective observational registry study identified consecutive patients undergoing THA or TKA from a single surgeon at TriHealth's Good Samaritan Hospital (OH, USA) (CC group: 2011 to 2013; MLWC group: 2015 to 2020). This study was reviewed and approved by the TriHealth Institutional Review Board (IRB number 19-032). Electronic medical records (EMRs) were reviewed to evaluate the outcomes of patients receiving THA and TKA.
Subjects were included in the study if they had undergone THA or TKA as elective, primary procedures during an inpatient admission between 1 January 2011 and 31 March 2020. Subjects were required to be aged ≥18 years and to have a minimum of 30 days of follow-up information from index (surgery date). Subjects were excluded if their records were found to be missing key data elements required for the pre-planned analyses, including patient demographics and all outcomes of interest.
Surgical procedures
The procedures were performed by a single surgeon who began adopting MLWC in 2014. Data for patients who received MLWC were collected from 2015 to 2020. From 2011 to 2013, conventional closure (CC) was the primary approach by the same surgeon. THA and TKA surgical preparation and technique prior to closure remained unchanged from 2011 to 2020.
For CC, the joint capsule was sutured using multiple #0 ETHIBOND interrupted sutures for both THA and TKA. Subcutaneous closure was achieved using 2-0 Vicryl sutures for THA and 0 Vicryl sutures for TKA. For both THA and TKA, subcuticular closure was performed with 2-0 Vicryl sutures and skin closure was performed with staples.
The wound closure approaches used for MLWC were as described in Snyder et al. [14]. In order to achieve optimal MLWC following THA, the joint capsule was sutured using ETHIBOND interrupted sutures (size 0). The hip bursa was closed with #1 bidirectional STRATAFIX™ Spiral. The iliotibial band was then sutured using #1 PDS STRATAFIX Symmetric and several #0 Ethibond interrupted sutures. #1 Spiral PDO bidirectional STRATAFIX suture was used for subcutaneous closure, followed by 2-0 PGA Spiral bidirectional STRATAFIX suture for the subcuticular layer and the DERMABOND™ PRINEO™ Wound Closure System for skin closure.
For TKA MLWC, the surgical team began by suturing the fat pad with 2-0 running Vicryl. This was followed by closure of the joint capsule, using #1 PDS STRATAFIX Symmetric, and several #0 Ethibond interrupted sutures positioned around the medial patella femoral ligament. Subcutaneous closure was performed using bidirectional #1 PDO STRATAFIX Spiral. 2-0 PGA Spiral bidirectional STRATAFIX was used subcuticularly, followed by the self-adhering mesh of the Dermabond Prineo carefully applied to approximate the skin tissue and 2-octyl cyanoacrylate was used to coat gently on top of the adhesive mesh.
Outcome measures
Baseline patient characteristics that were evaluated included age, sex, race/ethnicity, American Society of Anesthesiology (ASA) score, presence of urinary tract infection (UTI), obesity or dementia and year of surgery. The primary outcome of interest was the rate of 90-day readmission. Secondary outcomes included hospital LOS, discharge status (i.e., home or skilled care), operating room (OR) time, 90-day rate of emergency department (ED) visits and complications including death, periprosthetic infection, venous thromboembolism (VTE), wound dehiscence and wound infection.
Statistical analysis
All cases from 2014 were excluded since it was a transitioning period from CC to MLWC. A mix of both wound closure approaches were used during this time period and the dataset did not capture specifically which product was used for a procedure. In 2015, however, every patient received MLWC approach. Descriptive analyses were performed comparing the MLWC and CC cohorts on baseline characteristics as well as on the clinical outcomes of interest. Continuous variables were examined using Student's t-tests and categorical variables were evaluated using Fisher's Exact and chi-squared tests. Following bivariate analyses, separate logistic regression models controlled for differences in baseline characteristics were used to evaluate the association of CC versus MLWC with readmission, ED visits, discharge status, LOS and OR time. Sensitivity analyses were performed accordingly using age as the benchmark covariate to evaluate the potential impact of unobserved confounders.
Adjusted ITS analyses were then conducted to account for decreasing trends in LOS and shift in discharge status over the study period. ITS analysis, also known as segmented regression analysis [25], enabled assessment of whether MLWC had an effect significantly greater than the underlying time trend [26]. The monthly mean of adjusted LOS and discharge rate to skilled care facilities were calculated for CC and MLWC cohorts, respectively, and then were fitted into linear regression models to show the level and slope changes before and after the introduction of MLWC. To test for changes in LOS and discharge status over time, the slopes of the linear splines over time were calculated and compared before and after the change in wound care.
Power calculations were performed to ensure the sample size of this study are sufficient to detect significant differences. Attempts to find representative literature in total hip and knee readmission rates within 90 days proved to be challenging so several articles were considered in calculating a power analysis. The literature [3–5] demonstrated an average 90-day readmission rate of 8% with a maximum of 11.7% and a minimum of 4.2%. Assuming an effect size between 3.8 and 7.5%, an alpha of 0.05 with 80% power, a sample size between 204 and 622 in each group, respectively, would be sufficient.
Results
Baseline patient demographic & clinical characteristics
The study included 2167 distinct patients receiving at least one TJA procedure (1574 TKA; 580 THA; 13 unknown) between 1 January 2011 and 31 December 2020 (Table 1). Of these, 1261 (58.2%) patients received procedures in which MLWC was used and 906 (41.8%) received conventional closure (CC). Patients were distributed somewhat evenly across the 10 years of the study. The surgeon began using MLWC during 2014, hence, data for CC patients were derived from 2011–2013 and data for MLWC patients were derived from 2015 to 2020.
| Characteristic | CC (n = 906) | MLWC (n = 1261) | Total (n = 2167) | p-value | |
|---|---|---|---|---|---|
| Age (years) | Mean (standard deviation) | 65.4 (10.3) | 66.5 (9.3) | 66.0 (9.7) | <0.05 |
| Median | 65.0 | 66.0 | 66.0 | ||
| Sex | Female | 487 (53.8%) | 669 (53.1%) | 1156 (53.3%) | 0.75 |
| Male | 419 (46.2%) | 592 (46.9%) | 1011 (46.7%) | ||
| Race/ethnicity | Black | 18 (3.0%) | 47 (3.7%) | 65 (3.5%) | <0.05 |
| Other | 7 (1.2%) | 80 (6.4%) | 87 (4.7%) | ||
| White | 580 (95.9%) | 1129 (89.9%) | 1709 (91.8%) | ||
| Missing | 301 | 5 | 306 | ||
| American Society of Anesthesiology score | Healthy | 25 (4.2%) | 31 (2.6%) | 56 (3.1%) | 0.23 |
| Incapacitating disease | 10 (1.7%) | 16 (1.3%) | 26 (1.5%) | ||
| Mild systemic disease | 305 (51.8%) | 649 (54.3%) | 954 (53.5%) | ||
| Severe systemic disease | 249 (42.3%) | 499 (41.8%) | 748 (41.9%) | ||
| Missing | 317 | 66 | 383 | ||
| Intercurrent urinary tract infection | No | 596 (98.0%) | 1252 (99.3%) | 1848 (98.9%) | <0.05 |
| Yes | 12 (2.0%) | 9 (0.7%) | 21 (1.1%) | ||
| Missing | 298 | 0 | 298 | ||
| Obesity diagnosis | No | 494 (81.2%) | 945 (74.9%) | 1439 (77.0%) | <0.05 |
| Yes | 114 (18.8%) | 316 (25.1%) | 430 (23.0%) | ||
| Missing | 298 | 0 | 298 | ||
| Dementia | No | 603 (99.2%) | 1258 (99.8%) | 1861 (99.6%) | <0.05 |
| Yes | 5 (0.8%) | 3 (0.2%) | 8 (0.4%) | ||
| Missing | 298 | 0 | 298 |
Bolded values denote statistically significant differences at p < 0.05.
CC: Conservative closure; MLWC: Multi-layered watertight closure.
The mean (standard deviation) age of all patients in the study at baseline was 66.0 (9.7) years and a slightly greater proportion of the patients were female (53.3%). Most patients were White (91.8%), 3.5% were Black and 4.7% were other race/ethnicity. According to ASA scores, most patients had mild systemic disease (53.5%) or severe systemic disease (41.9%), and few were categorized as healthy (3.1%) or having incapacitating disease (1.5%). Obesity was present among 23.0% of patients, intercurrent UTI among 1.1%, and dementia among 0.4%. Compared with patients who received CC, patients who received MLWC were older (66.5 vs 65.4 years; p < 0.05), a smaller proportion were white (89.9 vs 95.9%; p < 0.05), a greater proportion had obesity (25.1 vs 18.8%), and a smaller proportion had intercurrent UTI (0.7 vs 2.0%; both p < 0.05).
Unadjusted (bivariate) analyses
Unadjusted bivariate analyses demonstrated that, compared with patients with MLWC, a greater proportion of patients with CC had a 90-day readmission (3.8 vs 1.5%; p < 0.05; Table 2). Mean LOS was longer among patients with CC (2.5 vs 1.4 days; p < 0.05) and a smaller proportion of patients with CC were discharged to home following their total hip or total knee procedures (85.9 vs 91.5%; p < 0.05). OR time (MLWC 80.7 min, CC 79.9 min) and the proportion of patients with 90-day ER visits (MLWC 99.4%, CC 99.6% min) did not differ between patients with MLWC and CC. The proportions of patients with complications were similar for MLWC and CC, with the exception of venous thromboembolism (VTE) as a slightly greater proportion of patients with MLWC had VTE (1.1 vs 0.3%; p = 0.04; Table 2).
| CC (n = 906) | MLWC (n = 1261) | Total (n = 2167) | p-value | ||
|---|---|---|---|---|---|
| Primary outcome | |||||
| 90-day readmission rate | No | 872 (96.2%) | 1242 (98.5%) | 2114 (97.6%) | <0.05 |
| Yes | 34 (3.8%) | 19 (1.5%) | 53 (2.4%) | ||
| Missing | 0 | 0 | 0 | ||
| Secondary outcomes | |||||
|---|---|---|---|---|---|
| Length of stay | Mean | 2.5 (0.9) | 1.4 (0.9) | 1.8 (1.0) | <0.05 |
| Median | 2.0 | 1.0 | 2.0 | ||
| Missing | 0 | 0 | 0 | ||
| Discharge status | Home | 778 (85.9%) | 1152 (91.5%) | 1930 (89.1%) | <0.05 |
| Skilled Care | 128 (14.1%) | 107 (8.5%) | 235 (10.9%) | ||
| Missing | 0 | 2 | 2 | ||
| Operating room time (min) | Mean | 79.9 (25.1) | 80.7 (16.8) | 80.5 (19.9) | 0.44 |
| Median | 76.0 | 78.0 | 78.0 | ||
| Missing | 299 | 2 | 301 | ||
| 90-day emergency department visit rate | No | 902 (99.6%) | 1254 (99.4%) | 2156 (99.5%) | 0.71 |
| Yes | 4 (0.4%) | 7 (0.6%) | 11 (0.5%) | ||
| Missing | 0 | 0 | 0 | ||
| 90-day complications | |||||
|---|---|---|---|---|---|
| Death | Yes | 0 (0.0%) | 1 (0.1%) | 1 (0.0%) | 0.40 |
| No | 906 (100.0%) | 1260 (99.9%) | 2166 (100.0%) | ||
| Periprosthetic infection | Yes | 8 (0.9%) | 15 (1.2%) | 23 (1.1%) | 0.49 |
| No | 898 (99.1%) | 1246 (98.8%) | 2144 (98.9%) | ||
| Venous thromboembolism | Yes | 3 (0.3%) | 14 (1.1%) | 17 (0.8%) | 0.04 |
| No | 903 (99.7%) | 1247 (98.9%) | 2150 (99.2%) | ||
| Wound dehiscence | Yes | 2 (0.2%) | 4 (0.3%) | 6 (0.3%) | 0.67 |
| No | 904 (99.8%) | 1257 (99.7%) | 2161 (99.7%) | ||
| Wound infection | Yes | 11 (1.2%) | 20 (1.6%) | 31 (1.4%) | 0.47 |
| No | 895 (98.8%) | 1241 (98.4%) | 2136 (98.6%) | ||
Bolded values denote statistically significant differences at p < 0.05.
CC: Conservative closure; MLWC: Multi-layered watertight closure.
Adjusted (multivariate) analyses
After adjustment for differences in baseline characteristics, patients with CC were shown to be 2.45-times more likely to be readmitted within 90 days and 1.88-times more likely to be discharged to skilled care facilities compared with patients with MLWC (Table 3). Patients with CC also had 1.67-times longer LOS compared with patients with MLWC. The likelihood of ER visits and OR time did not significantly differ between patients with MLWC and CC (Table 3). Sensitivity analyses were performed on readmission rate, discharge rate to skilled care facilities, and LOS. In all three cases, the bounds on confounding as strong as age, R2Y∼Z|X,D and R2D∼Z|X, were below the robustness value (RV), meaning that unobserved confounders as strong as age were not sufficient to explain away the observed difference between MLWC and CC (Table 4).
| Outcomes | CC (n) | MLWC (n) | CC | MLWC | Odds ratio (CC vs MLWC) | -95% CI | 95% CI | p-value |
|---|---|---|---|---|---|---|---|---|
| 90-day readmission | 586 | 1190 | 0.01 | 0.00 | 2.45 | 1.29 | 4.68 | 0.01 |
| LOS (days) | 581 | 1122 | 2.41 | 1.45 | 1.67 | 1.59 | 1.75 | <0.0005 |
| Skilled care discharge status | 586 | 1188 | 0.08 | 0.05 | 1.88 | 1.34 | 2.65 | <0.0005 |
| OR time (min) | 584 | 1188 | 79.44 | 80.97 | 0.98 | 0.96 | 1.01 | 0.12 |
| 90-day ED visits | 586 | 1190 | 0.00 | 0.00 | 0.95 | 0.23 | 3.92 | 0.94 |
Bolded values denote statistically significant differences at p < 0.05.
CC: Conservative closure; CI: Confidence interval; ED: Emergency department; LOS: Length of stay; MLWC: Multi-layered watertight closure; OR: Operating room.
| Outcome | Treatment | Coef. estimate | R2Y∼D|X | RVq = 1 | Benchmark covariate; age |
|---|---|---|---|---|---|
| Readmission rate | WC | -0.0223 | 0.45% | 6.53% | R2Y∼Z|X,D = 0.32%, R2D∼Z|X = 0.37% |
| Discharge rate to SNF | WC | -0.0588 | 0.88% | 8.97% | R2Y∼Z|X,D = 6.33%, R2D∼Z|X = 0.36% |
| LOS | WC | -0.9724 | 22.89% | 41.63% | R2Y∼Z|X,D = 2.76%, R2D∼Z|X = 0.41% |
R2Y∼D|X: the partial R2 of the treatment with the outcome. RVq = 1: robustness value for bringing the point estimate of WC exactly to zero. R2Y∼Z|X,D and R2D∼Z|X: bounds on confounding (Benchmark covariate: Age).
LOS: Length of stay; RV: Robustness value; WC: Watertight closure.
ITS analysis
Differences in LOS and discharge status were statistically significant based on the ITS analyses. For LOS, unadjusted and adjusted ITS analysis showed a sharp decline of 0.2 days and 0.9 days, respectively (Figure 1). Similarly, there was a sharp decline in incidence of discharge to a skilled care facility (5.6% incidence) immediately after implementation of the MLWC approach, while the unadjusted ITS showed less than 0.2% increase in this rate (Figure 2). Levelling of the data with no further changes in LOS or discharge status was observed for the remainder of the study period.
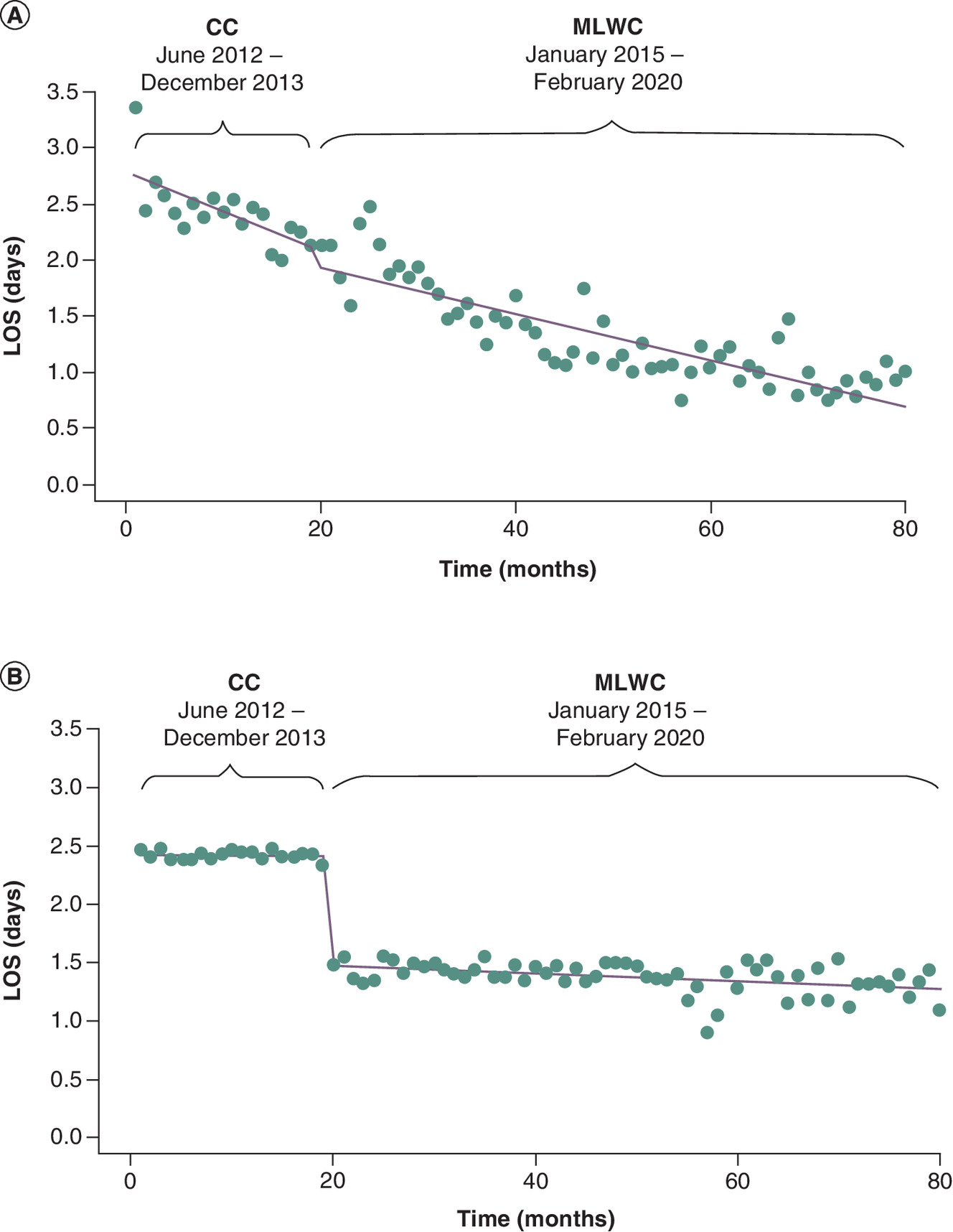
Figure 1. Interrupted time series analysis, length of stay (by month).
(A) Unadjusted. (B) Adjusted.
CC: Conservative closure; LOS: Length of stay; MLWC: Multi-layered watertight closure.
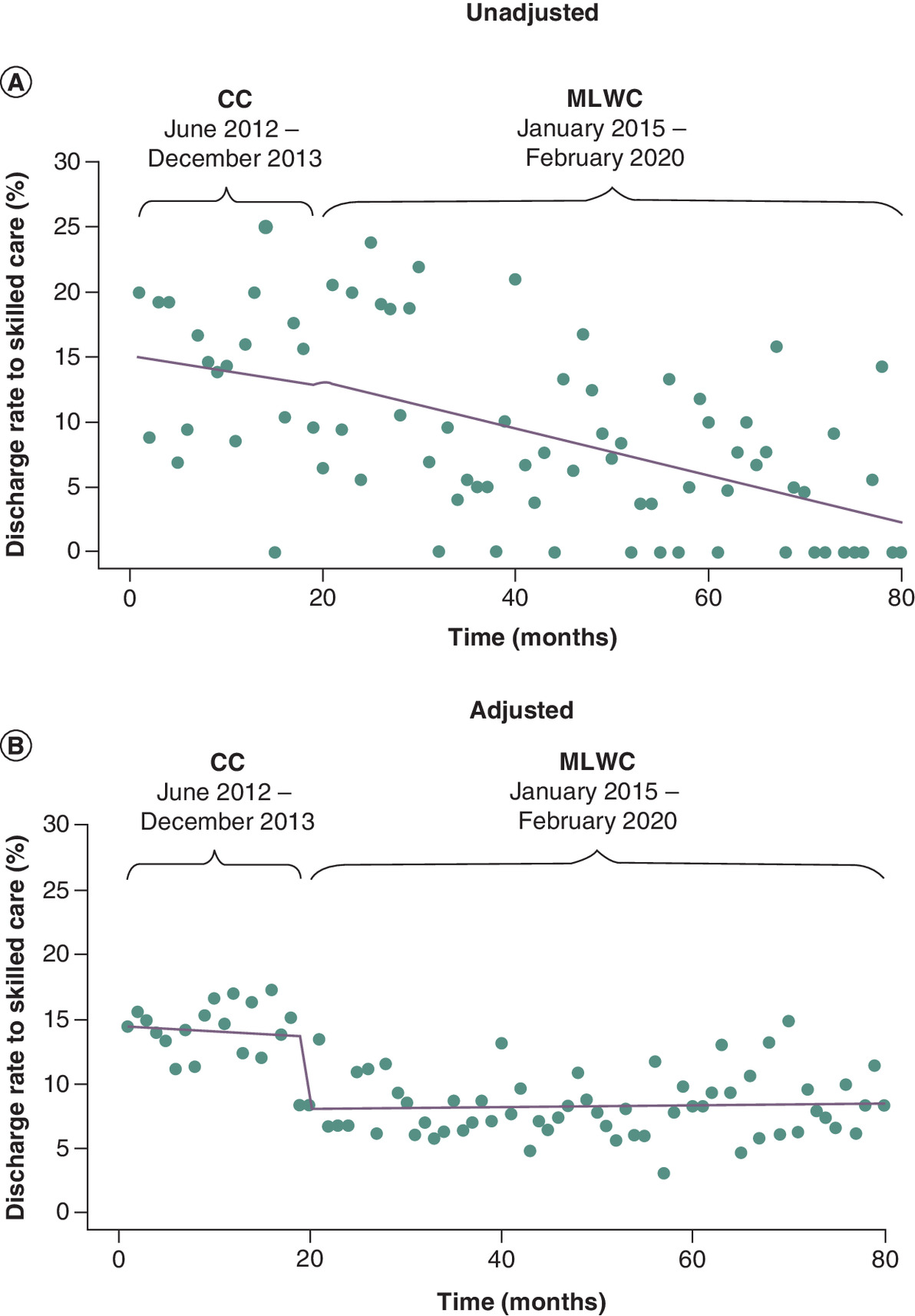
Figure 2. Interrupted time series analyses, discharge rate to a skilled care facility (by month).
(A) Unadjusted. (B) Adjusted.
CC: Conservative closure; MLWC: Multi-layered watertight closure.
Discussion
To our knowledge, this is the first study to employ adjusted ITS techniques to evaluate the clinical and economic outcomes associated with advanced MLWC among patients undergoing TJA. Among 2167 patients under a single surgeon at a single center, unadjusted analyses showed that there were no significant differences in 90-day SSI rates; however, patients with MLWC had 44% lower LOS (1.4 days vs 2.5 days, p < 0.05), 40% lower discharge rates to a skilled care facility (8.5% patients vs 14.1%, p < 0.05), and 60% lower 90-day readmission rates (1.5 vs 3.8%, p < 0.05) compared with patients with CC. Multivariate analyses confirmed that CC was associated with longer LOS, discharge to skilled care, and 90-day readmission. To account for time-dependent factors, e.g., decreasing trends in LOS and shift in discharge status over the study period, ITS analyses were performed to isolate any of these effects and evaluated the direct impact of using MLWC. The adjusted ITS analyses were also performed to account for the difference in patient cohorts of MLWC and CC. The results of the adjusted ITS analyses confirmed the impact of introducing MLWC, showing a sharp decline in LOS (0.9 days) and discharge status to a skilled care facility (5.6% incidence) immediately after implementation of the MLWC approach. The sensitivity analyses showed that the unobserved confounders in this study were not sufficient to explain away the concluded difference between MLWC and CC.
Efforts to improve quality of care and control healthcare costs for THA and TKA have included penalizing hospitals for THA or TKA readmissions and consolidating THA and TKA payments. CMS’ HRRP expansion to THA and TKA was finalized in 2013 and was implemented in 2014. Then, in 2016, comprehensive care with the CJR was implemented for Medicare beneficiaries. Given that MLWC in the current study was implemented by the surgeon in 2014, it was important to elucidate whether the change in outcomes was due to the change in wound care or to other concomitant quality of care changes. ITS analysis is a valuable study design for establishing causality as it controls for pre-existing underlying short- and long-term trends by longitudinally tracking the outcome before and after an intervention [23,24]. ITS analyses showed a consistent downward trend in LOS and discharge to a skilled facility, and then a sharp decline immediately after implementation of the MLWC approach. This confirmed the important impact of introducing MLWC despite shifting trends in LOS and discharge status.
Some studies have shown mixed results when evaluating the impact of THA and TKA quality of care and cost containment strategies [27,28]. It has been suggested that readmissions for patients after elective surgery are more likely a consequence of procedure-related complications rather than failure of care coordination. Hence, systems-level interventions that have proved effective at reducing readmissions for patients with chronic medical diseases (e.g., discharge navigators, care transition programs and medication reconciliation by pharmacists) may not be generalizable to those recovering from elective surgery. Thus, in order to reduce SSI, readmission, LOS and skilled care facility discharge with THA and TKA, providers and payers may need to focus on procedure-related changes that impact complications, such as improved wound care.
The 90-day readmission rate in the current study was significantly lower for MLWC patients (1.5 vs 3.8%; p < 0.05). In 2012, the Hospital Readmissions Reduction Program was introduced by Medicare in the US to reduce the frequency of readmissions. Hospitals with above average readmissions were financially penalized. Furthermore, the Comprehensive Care for Joint Replacement bundled payment model was introduced in 2016 as a mechanism to restrain healthcare spending for total hip and knee arthroplasty (the study hospital participated in this program). Hospitals were provided a single lump-sum payment from Medicare to manage the entire episode of care for a period of 90 days. Hospitals that spent more than the target price or performed below a quality threshold were required to repay Medicare a portion of the episode spending. Therefore these findings are highly economically relevant from payer and provider perspectives. A driver of the observed differences in readmission rates could be the shorter hospital LOS in the MLWC group. A study from 2017 reported that among Medicare patients undergoing knee or hip arthroplasty, increased hospital LOS was a significant risk factor for 90-day readmission because of the increased adverse outcomes associated with increased LOS such as hospital-acquired infections [29]. However, reasons for readmission were not available in the dataset and therefore could not be examined. Regardless, readmissions represent not only an undesirable circumstance for patients, but are also an important quality target for hospitals, and viewed as an important driver of costs to the overall healthcare system.
The reduced LOS and discharge rate to SNF could be attributed to SFX KTCD which has numerous clinical advantages compared with traditional interrupted sutures including the ability to achieve better watertight closure of the wound. Furthermore, 2OPM for skin closure may also promote quicker transition to a home setting, given that it allows patients to shower immediately after procedures and obviates the need for wound dressing changes in the hospital [29–32]. The watertight closure across multiple tissue layers with SFX KTCD and comparatively greater strength as well as unique antimicrobial barrier of 2OPM represent a potential solution to wound complications such as dehiscence and drainage, which can be a retrograde infection pathway [30]. Nevertheless, further research to corroborate and identify the specific underlying causes of these findings related to hospital LOS and discharge to SNF rate would be beneficial.
Some previous studies have also shown the benefits of advanced MLWC with the innovative combination of barbed sutures and a skin closure system. Anderson et al. [33] and Herndon et al. [34] found that use of barbed sutures used in deep layers with 2OPM was associated with fewer episodes of delayed wound healing and reoperations than the standard wound dressing. The authors suggested that the possible mechanism may be that 2OPM distributes wound tension more evenly. In addition, since it remains in place longer during the immediate postoperative period, it may provide prolonged wound-edge support. Snyder and colleagues [14] described their implementation of evidence-based integrated clinical pathways incorporating watertight MLWC and suggested that the integrated clinical pathways and MLWC could synergistically improve the preventative effectiveness against joint prosthetic adverse events such as SSIs [14]. Similarly, Vendittoli and colleagues [35] used an enhanced recovery after surgery (ERAS) protocol along with MLWC that resulted in reduced hospital LOS, improved patient care, and reduced direct healthcare costs. Finally, Flener and colleagues [36] conducted a retrospective EMR review to evaluate the outcomes of 1828 patients receiving MWLC or CC for total hip or knee arthroplasties. Similar to the current study, MLWC was associated with significantly shorter inpatient LOS and increased likelihood of being discharged to home compared with CC. Adjusted mean hospital LOS was a half-day shorter for MLWC (1.10 vs 1.65 days; p < 0.001) and MLWC patients were more likely to be discharged home (odds ratio 4.61; p = 0.002). Our study findings support those of previous authors and build upon them given that ITS analysis is considered a more robust technique for evaluating healthcare quality improvement because of its ability to control for biases [20–22]. ITS controls for pre-existing underlying short- and long-term trends by longitudinally tracking the outcome before and after an intervention [23,24], enabling assessment of whether MLWC had an effect significantly greater than the underlying time trend [26].
Although not perfect in capturing all relevant data, the availability of EMR data presents an opportunity to efficiently evaluate quality of care for individuals in the real-world clinical setting. EMR datasets capture a variety of patient-level data that represent integral components of care that may not necessarily be available through other retrospective database sources such as administrative claims databases or patient registries (e.g., information on the specific type of endoprosthesis used) [37,38]. EMRs also provide efficient access to detailed, longitudinal data that would otherwise be difficult to collect [39,40]. However, limitations of EMR data include coding errors or incomplete information for clinical visits and subsequent follow-up. Also, the patients selected for this study represent a convenience sample from a single site, and patients, treatment methods, and institutional policies may differ in other settings of care, therefore limiting the generalizability of results. Finally, although the present study carefully applied statistical analysis techniques (i.e., logistic regression and ITS) to improve causal inference of comparative treatment effects, the study was still retrospective and observational in design and causality cannot be established for the observed relationships. Despite these limitations, the study utilized ITS analysis to contribute to the evidence for the potential clinical and economic benefits of MLWC in THA and TKA.
Conclusion
Among patients undergoing THA or TKA, MLWC was associated with at least 40% reduction in 90-day readmission rates, LOS, and discharge to a skilled facility compared with CC. ITS confirmed the impact of introducing the MLWC approach despite shifting trends in LOS and discharge status. MLWC may facilitate shorter LOS and the ability to discharge to home and may result in fewer readmission after THA and TKA. Further studies with larger cohorts of patients at multiple sites are warranted.
Summary points
•
Research evaluating the clinical and economic value of advanced multi-layer, watertight closure (MLWC) in total joint arthroplasty (TJA) is needed.
•
Interrupted time series (ITS) analysis is a valuable study design for evaluating healthcare quality improvement as it controls for pre-existing underlying short- and long-term trends.
•
To our knowledge, this is the first study to employ adjusted ITS techniques to evaluate clinical and economic outcomes of advanced MLWC versus conventional care (CC) among patients undergoing THA and TKA.
•
MLWC was associated with ≥40% reduction in 90-day readmission, length of stay (LOS), and skilled nursing facility (SNF) discharge compared with TJA CC.
•
Multivariable analyses showed CC patients were 2.45-times more likely to be readmitted within 90 days, 1.88-times more likely to be discharged to SNF and had 1.67-times longer LOS compared with MLWC.
•
ITS analyses showed a sharp decline in LOS (0.9 days) and discharge to SNF (5.6% incidence) with MLWC.
•
Given that multiple quality of care and cost containment initiatives have been implemented for TJA in recent years, it is important to differentiate whether observed changes in outcomes are due to the new technologies or interventions (e.g., MLWC) or due to background quality of care improvements.
•
ITS confirmed the impact of introducing the MLWC approach despite shifting trends in LOS and discharge status.
•
Adoption of advanced MLWC may result in improved clinical and economic outcomes.
Author contributions
Z Tan, K Etter, J Tomaszewski and B Po-Han Chen and WJ were involved in the study design, implementation of clinical research data analysis, data interpretation, and manuscript review; NJ Gunja was involved in the study design, data interpretation, and manuscript writing and review.
Acknowledgments
The authos acknowledge the entire TriHealth team who contributed to this study. The authors also thank the late MA Snyder for shaping the study design and whose patient cohort was examined in this research. Thanks also go to S Wurzelbacher for providing details on the surgical approach for wound closure and to L Leibel for assisting with data extraction. The authors also thank Natalie Edwards of Health Services Consulting Corporation, Boxborough, MA, USA for editorial assistance with the manuscript.
Financial disclosure
This study was funded by the Dr Mark A Snyder Musculoskeletal Research Fund and Ethicon. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Competing interests disclosure
The authors are employees of Johnson & Johnson (J&J). The authors had full control of the manuscript and provided their final approval of all content. Publication of the study results was not contingent on the sponsor's approval or censorship of the manuscript. The authors have no other competing interests or relevant affiliations with any organization/entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing disclosure
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The study was reviewed and approved by the TriHealth Institutional Review Board (IRB number 19-032).
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
References
Papers of special note have been highlighted as: • of interest
1.
Liu X-W, Zi Y, Xiang L-B, Wang Y. Total hip arthroplasty: a review of advances, advantages and limitations. Int. J. Clin. Experim. Med. 8(1), 27–36 (2015).
2.
Marsh M, Newman S. Trends and developments in hip and knee arthroplasty technology. J Rehabil. Assist. Technol. Eng. 8, 2055668320952043 (2021).
3.
Fingar KR, Stocks C, Weiss AJ, Steiner CA. Statistical Brief #186: most frequent operating room procedures performed in U.S. hospitals, 2003–2012. Healthcare Cost and Utilization Project (HCUP) Statistical Briefs. Agency for Healthcare Research and Quality, MD, USA (2006).
4.
Kurtz S, Mowat F, Ong K et al. Prevalence of primary and revision total hip and knee arthroplasty in the United States from 1990 through 2002. J. Bone Joint Surg. Am. 87(7), 1487–1497 (2005).
5.
Kurtz S, Ong K, Lau E, Mowat F, Halpern M. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J. Bone Joint Surg. Am. 89(4), 780–785 (2007).
6.
Schwartz AM, Farley KX, Guild GN, Bradbury TL Jr. Projections and epidemiology of revision hip and knee arthroplasty in the United States to 2030. J. Arthroplasty. 35(6S), S79–S85 (2020).
7.
Bernatz JT, Tueting JL, Anderson PA. Thirty-day readmission rates in orthopedics: a systematic review and meta-analysis. PLOS. ONE. 10(4), e0123593 (2015).
8.
Saleh A, Faour M, Sultan AA et al. Emergency department visits within thirty days of discharge after primary total hip arthroplasty: a hidden quality measure. J. Arthroplasty. 34(1), 20–26 (2019).
9.
Umscheid CA, Mitchell MD, Doshi JA et al. Estimating the proportion of healthcare-associated infections that are reasonably preventable and the related mortality and costs. Infect. Control Hosp. Epidemiol. 32(2), 101–114 (2011).
10.
Gray CF, Prieto HA, Duncan AT, Parvataneni HK. Arthroplasty care redesign related to the Comprehensive Care for Joint Replacement model: results at a tertiary academic medical center. Arthroplasty. Today. 4(2), 221–226 (2018).
• Presents evidence that the implementation of the Comprehensive Care for Joint Replacement bundled payment model improved value, reflected in lower costs, decreased readmissions and complications, decreased hospital length of stay (LOS), and less discharge to post-acute facilities.
11.
Li T, Zhang H, Chan PK et al. Risk factors associated with surgical site infections following joint replacement surgery: a narrative review. Arthroplasty. 4(1), 11 (2022).
12.
Alexander JW, Solomkin JS, Edwards MJ. Updated recommendations for control of surgical site infections. Ann. Surg. 253(6), 1082–1093 (2011).
13.
Berríos-Torres SI, Umscheid CA, Bratzler DW et al. Centers for Disease Control and Prevention Guideline for the Prevention of Surgical Site Infection, 2017. JAMA. Surg. 152(8), 784–791 (2017).
14.
Snyder MA, Sympson AN, Wurzelbacher SJ, Brian Chen PH, Ernst FR. Integrated clinical pathways with watertight, multi-layer closure to improve patient outcomes in total hip and knee joint arthroplasty. J. Orthop. 18, 191–196 (2020).
• This literature review summarized evidence for wound closure techniques and found that higher quality comparative evidence for multi-layer, watertight closure (MLWC) vs. conventional care was needed.
15.
Ming X, Rothenburger S, Yang D. In vitro antibacterial efficacy of MONOCRYL plus antibacterial suture (Poliglecaprone 25 with triclosan). Surg. Infect. (Larchmt). 8(2), 201–208 (2007).
16.
Ethicon Inc. STRATAFIX™ Symmetric PDS™ Plus Knotless Tissue Control Device (2023). https://www.jnjmedtech.com/en-US/product/stratafix-symmetric-pds-plus-knotless-tissue-control-device/barbed-suture
17.
Ethicon Inc. DERMABOND® PRINEO® Skin Closure System (2023). https://www.jnjmedtech.com/en-US/product/dermabond-prineo-skin-closure-system
18.
El-Gazzar Y, Smith DC, Kim SJ et al. The use of dermabond® as an adjunct to wound closure after total knee arthroplasty: examining immediate post-operative wound drainage. J. Arthroplasty. 28(4), 553–556 (2013).
19.
Parvizi J, Ghanem E, Joshi A et al. Does “excessive“ anticoagulation predispose to periprosthetic infection? J. Arthroplasty. 22(2 Suppl. 6), 24–28 (2007).
20.
Penfold RB, Zhang F. Use of interrupted time series analysis in evaluating health care quality improvements. Acad. Pediatr. 13(Suppl. 6), S38–S44 (2013).
21.
Fretheim A, Tomic O. Statistical process control and interrupted time series: a golden opportunity for impact evaluation in quality improvement. BMJ. Qual. Saf. 24(12), 748–752 (2015).
22.
Ogrinc G, Mooney S, Estrada C et al. The SQUIRE (Standards for QUality Improvement Reporting Excellence) guidelines for quality improvement reporting: explanation and elaboration. BMJ. Qual. Saf. 17(Suppl. 1), i13–i32 (2008).
23.
Soumerai SB, Starr D, Majumdar SR. How do you know which health care effectiveness research you can trust? A guide to study design for the perplexed. Prev. Chron. Dis. 12, E101 (2015).
24.
Schaffer AL, Dobbins TA, Pearson S-A. Interrupted time series analysis using autoregressive integrated moving average (ARIMA) models: a guide for evaluating large-scale health interventions. BMC. Med. Res. Methodol. 21(1), 58 (2021).
• Presents evidence that ITS is a valuable study design for helping establish causality by controling for pre-existing underlying short- and long-term trends by longitudinally tracking the outcome before and after an intervention.
25.
Kontopantelis E, Doran T, Springate DA, Buchan I, Reeves D. Regression based quasi-experimental approach when randomisation is not an option: interrupted time series analysis. BMJ. 350, h2750 (2015).
26.
Bernal JL, Cummins S, Gasparrini A. Interrupted time series regression for the evaluation of public health interventions: a tutorial. Int. J. Epidemiol. 46(1), 348–355 (2017).
27.
Borza T, Oreline MK, Skolarus TA et al. Association of the Hospital Readmissions Reduction Program With Surgical Readmissions. JAMA. Surg. 153(3), 243–250 (2018).
28.
Thirukumaran CP, McGarry BE, Glance LG et al. Impact of hospital readmissions reduction program penalties on hip and knee replacement readmissions: comparison of hospitals at risk of varying penalty Amounts. J. Bone Joint Surg. Am. 102(1), 60–67 (2020).
29.
Williams J, Kester BS, Bosco JA, Slover JD, Iorio R, Schwarzkopf R. The association between hospital length of stay and 90-day readmission risk within a total joint arthroplasty bundled payment initiative. The Journal of arthroplasty 32(3), 714–718 (2017).
30.
Weiss AP, Krackow KA. Persistent wound drainage after primary total knee arthroplasty. J. Arthroplasty. 8(3), 285–289 (1993).
31.
Vakil JJ, O'Reilly MP, Sutter EG, Mears SC, Belkoff SM, Khanuja HS. Knee arthrotomy repair with a continuous barbed suture: a biomechanical study. J Arthroplasty 26(5), 710 (2011).
32.
Nett M, Avelar R, Sheehan M, Cushner F. Water-tight knee arthrotomy closure: comparison of a novel single bidirectional barbed self-retaining running suture versus conventional interrupted sutures. J Knee Surg 24(1), 55 (2011).
33.
Anderson FL, Herndon CL, Lakra A et al. Polyester mesh dressings reduce delayed wound healing and reoperations compared with silver-impregnated occlusive dressings after knee arthroplasty. Arthroplasty. Today. 6(3), 350–353 (2020).
• Findings from this study showed that Mesh dressings were associated with fewer episodes of delayed wound healing and reoperations than the standard dressing.
34.
Herndon CL, Coury JR, Sarpong NO et al. Polyester mesh dressings reduce delayed wound healing rates after total hip arthroplasty compared with silver-impregnated occlusive dressings. Arthroplasty. Today. 6(2), 158–162 (2020).
• In this retrospective series, the authors showed that Mesh dressings were a safe and reliable dressing type for THA and were associated with a decrease in early wound healing complications when compared with standard, silver-impregnated occlusive dressings.
35.
Vendittoli PA, Pellei K, Desmeules F et al. Enhanced recovery short-stay hip and knee joint replacement program improves patients outcomes while reducing hospital costs. Orthop. Traumatol. Surg. Res. 105(7), 1237–1243 (2019).
36.
Flener JL, Po-Han Chen B, Ernst FR, Libolt A, Barrett WS. Advanced Multi-Layer Watertight Closure Versus Conventional Closure in Total Hip and Knee Replacement Surgery: A Retrospective Observational Study. International Society for Pharmacoeconomics and Outcomes Research (ISPOR) EU, Vienna, Austria (2022).
• This retrospective EHR review showed that MLWC was associated with significantly shorter inpatient LOS and increased likelihood of being discharged to home compared to CC; however, pre-existing underlying short- and long-term longitudinal trends were not controlled for.
37.
Häyrinen K, Saranto K, Nykänen P. Definition, structure, content, use and impacts of electronic health records: a review of the research literature. Int. J. Med. Inform. 77(5), 291–304 (2008).
38.
Emir B, Masters ET, Mardekian J et al. Identification of a potential fibromyalgia diagnosis using random forest modeling applied to electronic medical records. J. Pain. Res. 8, 277–288 (2015).
39.
Pathak J, Kho AN, Denny JC. Electronic health records-driven phenotyping: challenges, recent advances, and perspectives. J. Am. Med. Inform. Assoc. 20(e2), e206–e211 (2013).
40.
Weng C, Appelbaum P, Hripcsak G et al. Using EHRs to integrate research with patient care: promises and challenges. J. Am. Med. Inform. Assoc. 19(5), 684–687 (2012).
Information & Authors
Information
Published In
Copyright
© 2024 Ethicon Endo Inc. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 28 June 2023
Accepted: 19 January 2024
Published online: 28 February 2024
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Use of interrupted time-series analyses in evaluating health economic outcomes following implementation of multilayer water-tight wound closure in a primary total joint arthroplasty population. (2024) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2023-0110
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Andrea Baldini, Damiano Ardiri, Lorenzo Benvenuti, Mattia Chirico, Enrico Fiorilli, Alessandro Singlitico, Filippo Leggieri, What Are the Game Changers in Total Knee Arthroplasty? A Narrative Review, Journal of Personalized Medicine, 10.3390/jpm15080389, 15, 8, (389), (2025).
- Jana Flener, Brian Chen, Frank Ernst, Aaron Libolt, Najmuddin Gunja, William Barrett, Advanced Multi-Layer Watertight Closure versus Conventional Closure in Total Hip and Knee Replacement Surgery, Pragmatic and Observational Research, 10.2147/POR.S450183, Volume 15, (93-102), (2024).