Adjusting for treatment crossover in the MAVORIC trial: survival in advanced mycosis fungoides and Sézary syndrome
Publication: Journal of Comparative Effectiveness Research
Abstract
Background: Relative overall survival (OS) estimates reported in the MAVORIC trial are potentially confounded by a high proportion of patients randomized to vorinostat switching to mogamulizumab; furthermore, vorinostat is not used in clinical practice in the UK. Methods: Three methods were considered for crossover adjustment. Survival post-crossover adjustment was compared with data from the Hospital Episode Statistics (HES) to contextualize estimates. Results: Following adjustment, the OS hazard ratio for mogamulizumab versus vorinostat was 0.42 (95% CI: 0.18, 0.98) using the method considered most appropriate based on an assessment of assumptions and comparison with HES. Conclusions: OS of mogamulizumab relative to vorinostat may be underestimated in MAVORIC due to the presence of crossover. The HES database was used to validate this adjustment.
Cutaneous T-cell lymphoma (CTCL) is a very rare form of non-Hodgkin lymphoma that can substantially impact morbidity and mortality. CTCL is largely incurable, and median survival varies between 1 and 6 years, depending on stage and typology, with early-stage CTCL having a better prognosis [1–5].
In the UK, 55% of CTCLs are mycosis fungoides (MF), which are characterized by skin lesions all over the body, such as patches in early stages and tumors, systemic involvement and death in later stages [6,7]. Sézary syndrome (SS) is clinically closely related to MF but rare (2.5% of cases), with more aggressive leukemic involvement and the occurrence of erythroderma and lymphadenopathy.
Treatment options depend on presentation and severity, and they range from skin-directed therapies to systemic treatment with biologics, chemotherapies or allogeneic stem cell transplant [8]. In advanced MF or SS, treatment options include systemic treatment. From second line in the relapsed or refractory MF/SS population there is no standard of care and treatments are often limited to off-label chemotherapies and recycled treatment options.
Mogamulizumab (Poteligeo®), a first-in-class defucosylated humanized IgG1 κ monoclonal antibody, was compared with vorinostat in MAVORIC, an open-label, international, phase III, randomized, controlled trial in people with relapsed or refractory MF/SS (NCT01728805) [9]. Vorinostat was the comparator approved by the US FDA. Although not approved by the European Medicines Agency (EMA), vorinostat was selected as the comparator for the MAVORIC trial, as the majority of European patients were likely to have received at least one of the other currently available treatments, and re-challenge in a clinical trial setting would have been both unethical for the patients and inappropriate by introducing selection bias into the study. Vorinostat was considered reflective of chemotherapies used later in the treatment pathway. Furthermore, vorinostat is the only drug with evidence in patients with SS, and it would have been unethical to use a treatment with no evidence of efficacy in this patient population [10–12]. The EMA approved mogamulizumab based on the MAVORIC trial design [13]. Investigator-assessed progression-free survival (PFS; primary end point) was statistically significantly (p < 0.05) better with mogamulizumab than vorinostat (hazard ratio [HR]: 0.53; 95% CI: 0.41, 0.69). Conversely, the difference in overall survival (OS; exploratory end point) between mogamulizumab and vorinostat was not significant. The testing for an effect on OS was confounded by a high proportion (72.6%) of subjects switching from vorinostat to mogamulizumab, so the effect of mogamulizumab on OS may have been underestimated.
This ‘non-administrative crossover’ [14] is common in oncology trials and permits participants to switch from the control to experimental treatment after disease progression, so that they can benefit from the new experimental treatment [15]. However, for economic models and UK Health Technology Assessment (HTA) decision-making purposes, comparison with current clinical practice is required without confounding from treatment switching.
It is therefore necessary to estimate the adjusted OS benefit of mogamulizumab compared with vorinostat, without treatment crossover. The aim of this study was to identify the most reasonable and credible approach to adjust for crossover, using real-world evidence (RWE) reflecting clinical practice in the UK.
Methods
Data
This is a secondary analysis of the MAVORIC trial, details of which have been published elsewhere [9], using a data cut from 2 March 2019. Participants were randomized (1:1) to mogamulizumab 1 mg/kg or vorinostat 400 mg. The protocol allowed people randomized to vorinostat to receive mogamulizumab if they had confirmed disease progression after at least two cycles of vorinostat or had intolerable toxicity (grade ≥3 adverse events, excluding inadequately treated nausea, vomiting, diarrhea and alopecia) despite dose reduction and side effect management [16]. Switching to non-trial treatments was not adjusted for, as it reflected current clinical practice (‘systematic’ crossover [14]).
In MAVORIC, eligible participants had stage IB-IVB, histologically confirmed relapsed or refractory MF/SS and failed (for progression or toxicity, assessed by principal investigator) at least one systemic therapy [9]. However, due to their limited treatment options and high unmet need, the primary focus was the advanced population (n = 243 [65%], defined as any stage SS and stage ≥IIB MF at diagnosis). The secondary population was the intention-to-treat (ITT) MAVORIC population (n = 372).
Statistical analysis
National Institute for Health and Care Excellence (NICE) offers guidance on ‘simple’ and ‘complex’ approaches to adjust for crossover [17]. As simple methods may introduce bias into the analysis, three complex methods from the NICE guidance were considered: rank preserving structural failure time models (RPSFTM), inverse probability of censoring weights (IPCW) and two-stage estimation (TSE). Detailed methodology is well described elsewhere [17].
RPSFTM assumes that mogamulizumab multiplies survival time by a given factor once a participant starts receiving it. It requires the randomization assumption, where participants in each treatment arm are comparable, and the common treatment effect assumption, where participants who switch (‘switchers’) from vorinostat to mogamulizumab following progression have the same treatment effect on the accelerated time scale compared with participants randomized to mogamulizumab.
The IPCW method weights control participants according to their probability of switching treatment. Weights are increased for participants who did not switch, but had a high estimated propensity for crossover, relative to participants with a low estimated propensity for crossover. Weights are obtained using logistic regression, which estimates the likelihood of a participant switching treatments. A key assumption is that all material baseline or time-dependent prognostic factors for mortality are accounted for (‘no unmeasured confounders’).
The TSE method adjusts for crossover after a specific disease-related time-point (the ‘secondary baseline’). Analysis time can be reset to zero at this point. The secondary baseline for this analysis was disease progression, as most participants switched treatments at this time-point. The effect of the new treatment on extending survival can be estimated from the point of disease progression to death, specifically for control group switchers. This comparison is not randomized, so variables are included to account for differences in participant characteristics between switchers and non-switchers. Key assumptions include no unmeasured confounders and no time-dependent confounding after disease progression.
For IPCW and TSE, baseline characteristics and time-dependent confounders were considered for inclusion in each model. A list of variables considered in the analysis is included in the Supplementary Material. The best-fitting model was selected based on the Akaike information criterion (AIC). Model fitting was performed on the overall ITT population. Calculated weights were assumed to be exchangeable between the ITT and advanced populations.
Kaplan–Meier (KM) curves and Cox hazard ratios (HRs) with 95% CIs are presented for each method and population (advanced and ITT). Stratification factors were not included in the calculation of Cox HRs. Analyses were performed in R [18].
Selecting the most appropriate method
Following the NICE guidelines, the most appropriate method was selected based on the applicability of the underlying assumptions and the clinical/biological plausibility of the results [17]. The latter was assessed comparing results from each statistically appropriate method to external data, including RWE from the UK, published observational studies and clinical expert experience.
RWE was from the Hospital Episode Statistics (HES) database, which includes all patients with MF/SS treated in UK National Health Service (NHS) secondary care in England over the last 10-year period. This is considered one of the best sources of RWE for analyses supporting HTA in the UK. It was hypothesized that the adjusted vorinostat estimate that most closely matches the RWE would provide an accurate OS estimate of current clinical practice outcomes without crossover. MF/SS patients treated with second line systemic treatment in secondary care (n = 198) were assumed to represent the advanced patient population. For this step, survival curves were fitted to the crossover-adjusted data and the HES data, and a naive comparison was made between the curves. See the Supplementary Material for the methodology on the survival analysis.
Survival for the ITT population was also elicited from UK clinical experts (one clinical oncology consultant, two dermatology consultants) with long-term experience in treating MF/SS patients [19] through a short survey in 2019.
Results
Patient population
Baseline characteristics for the vorinostat arm were similar between non-switchers and switchers for the advanced and ITT populations (Table 1). In the advanced population, 78.5% (n = 95) of vorinostat participants switched to mogamulizumab.
| Advanced | Intention-to-treat | ||||||
|---|---|---|---|---|---|---|---|
| Vorinostat, non-switchers | Vorinostat, switchers | Mogamulizumab | Vorinostat, non-switchers | Vorinostat, switchers | Mogamulizumab | ||
| n | 26 | 95 | 122 | 51 | 135 | 186 | |
| Mean (SD) age, years | 63.73 (11.07) | 66.78 (11.48) | 64.20 (13.37) | 61.55 (12.48) | 63.90 (12.60) | 62.82 (13.34) | |
| n (%) | |||||||
| Age >65 years | 11 (42%) | 60 (63%) | 62 (51%) | 19 (37%) | 73 (54%) | 84 (45%) | |
| CTCL type | MF | 8 (31%) | 26 (27%) | 41 (34%) | 33 (65%) | 66 (49%) | 105 (56%) |
| SS | 18 (69%) | 69 (73%) | 81 (66%) | 18 (35%) | 69 (51%) | 81 (44%) | |
| Stage | IA/IB | 2 (8%) | 7 (7%) | 9 (7%) | 21 (41%) | 33 (24%) | 46 (25%) |
| IIA/IIB | 7 (27%) | 13 (14%) | 15 (12%) | 8 (16%) | 16 (12%) | 23 (12%) | |
| IIIA/IIIB | 4 (15%) | 18 (19%) | 35 (29%) | 4 (8%) | 18 (13%) | 35 (19%) | |
| IVA1/IVA2/IVB | 10 (38%) | 48 (51%) | 57 (47%) | 10 (20%) | 48 (36%) | 57 (31%) | |
| UN | 3 (12%) | 9 (9%) | 6 (5%) | 8 (16%) | 20 (15%) | 25 (13%) | |
| Region | USA | 10 (38%) | 60 (63%) | 69 (57%) | 22 (43%) | 81 (60%) | 98 (53%) |
| Europe | 14 (54%) | 31 (33%) | 44 (36%) | 22 (43%) | 48 (36%) | 70 (38%) | |
| Rest of world | 2 (8%) | 4 (4%) | 9 (7%) | 7 (14%) | 6 (4%) | 18 (10%) | |
| ECOG | 0 | 11 (42%) | 51 (54%) | 67 (55%) | 28 (55%) | 76 (56%) | 106 (57%) |
| 1 | 15 (58%) | 44 (46%) | 53 (43%) | 23 (45%) | 59 (44%) | 78 (42%) | |
| 2 | 0 (0%) | 0 (0%) | 2 (2%) | 0 (0%) | 0 (0%) | 2 (1%) | |
CTCL: Cutaneous T-cell lymphoma; ECOG: Eastern Cooperative Oncology Group; MF: Mycosis fungoides; SD: Standard deviation; SS: Sézary syndrome; UN: Unstaged.
Crossover adjustment
Results for the advanced population are presented here. The ITT population results are in the Supplementary Material. Table 2 presents the HR and median survival for the unadjusted, IPCW- and TSE-adjusted analysis.
| Analysis | Median overall survival for mogamulizumab (months) | Median overall survival for vorinostat (months) | Hazard ratio for mogamulizumab vs vorinostat (95% CI) |
|---|---|---|---|
| Unadjusted | 57.17 | Not reached | 1.17 (95% CI: 0.78, 1.76) |
| IPCW | 7.43 | 0.42 (95% CI: 0.18, 0.98) | |
| TSE | 41.93 | 0.76 (95% CI: 0.50, 1.16) |
IPCW: Inverse probability of censoring weights; TSE: Two-stage estimation.
The OS HR for mogamulizumab compared with vorinostat without adjustment for crossover was 1.17 (95% CI: 0.78, 1.76).
For the RPSFTM method (Figure 1A), the common treatment effect assumption was not satisfied. PFS significantly differed between the two trial arms [9], and it was not considered clinically plausible that participants who started mogamulizumab after progression on vorinostat would have the same OS treatment effect on the accelerated time scale as participants originally randomized to mogamulizumab. Therefore, it was not considered further.
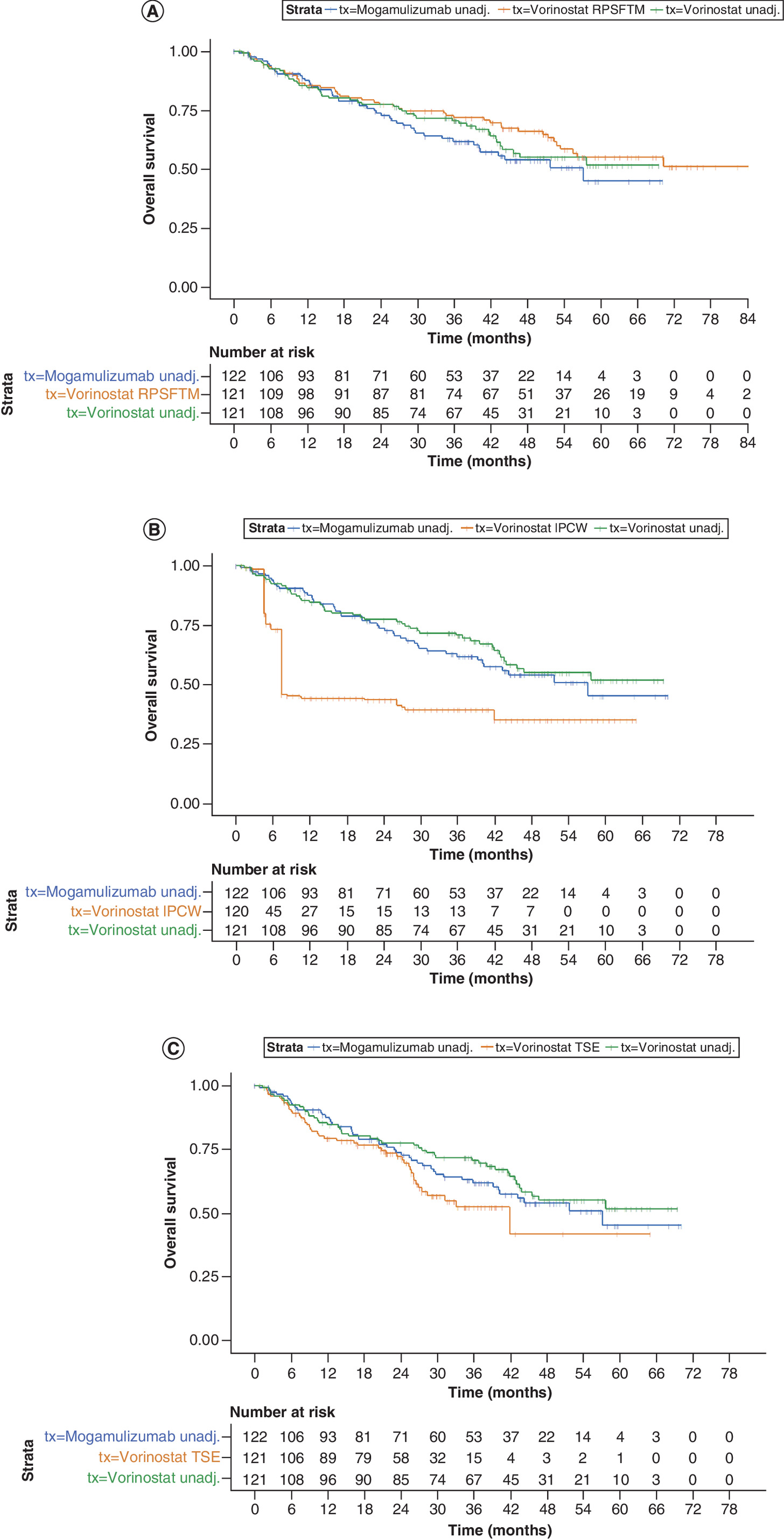
Figure 1. Kaplan–Meier curves advanced population.
(A) Adjusted for crossover with rank preserving structural failure time models, (B) adjusted for crossover with inverse probability of censoring weights and (C) adjusted for crossover with two-stage estimation.
IPCW: Inverse probability of censoring weights; RPSFTM: Rank preserving structural failure time model; TSE: Two-stage estimation; Unadj: Unadjusted.
For IPCW, the best-fitting logistic regression used to calculate the weights in the analysis included the following patient characteristics: histology (MF/SS), disease stage, adverse events (yes/no), region, progression status, Eastern Cooperative Oncology Group (ECOG) status and age >65 years (see Supplementary Material for more details on variables and weights).
The HR was 0.42 (0.18, 0.98) for mogamulizumab compared with vorinostat. The visible ‘drop’ in number-at-risk in the adjusted vorinostat arm at 6 months (Figure 1B) is due to the MAVORIC trial design, which allowed participants to cross over only after two full cycles of treatment and an additional minimum 2 weeks' waiting period. The IPCW approach censors participants at point of switch and upweights the remaining participants, so switchers were effectively removed from the KM curve, resulting in a drop in the curve.
For TSE, the best-fitting model included the following characteristics: histology (MF/SS), disease stage, adverse events, region, progression status, ECOG status and age >65 years. The HR was 0.76 (0.50, 1.16) for mogamulizumab compared with vorinostat (Figure 1C).
The assumptions associated with the IPCW and TSE were considered reasonable although difficult to prove. Both methods have uncertainty; the IPCW is informed by 45 patients and the TSE by even fewer (29 patients who were randomized to vorinostat and progressed but did not switch to mogamulizumab). Therefore, it was imperative to use external data and clinical opinion to choose the most appropriate approach.
Clinical plausibility
To compare the adjusted vorinostat curves to current UK clinical practice from the HES data, independent parametric models were fitted to the adjusted vorinostat treatment arm for the IPCW, TSE and HES data. An exponential model provided the best fit in all three cases, based on goodness-of-fit statistics and visual inspection of the goodness-of-fit to observed KM data and diagnostic plots.
The TSE-adjusted vorinostat arm was substantially higher than the HES arm, suggesting that it overestimates OS for current UK clinical practice. The IPCW-adjusted curve was close to the HES arm and, therefore, was a better reflection of OS for UK clinical practice (Figure 2A & B).
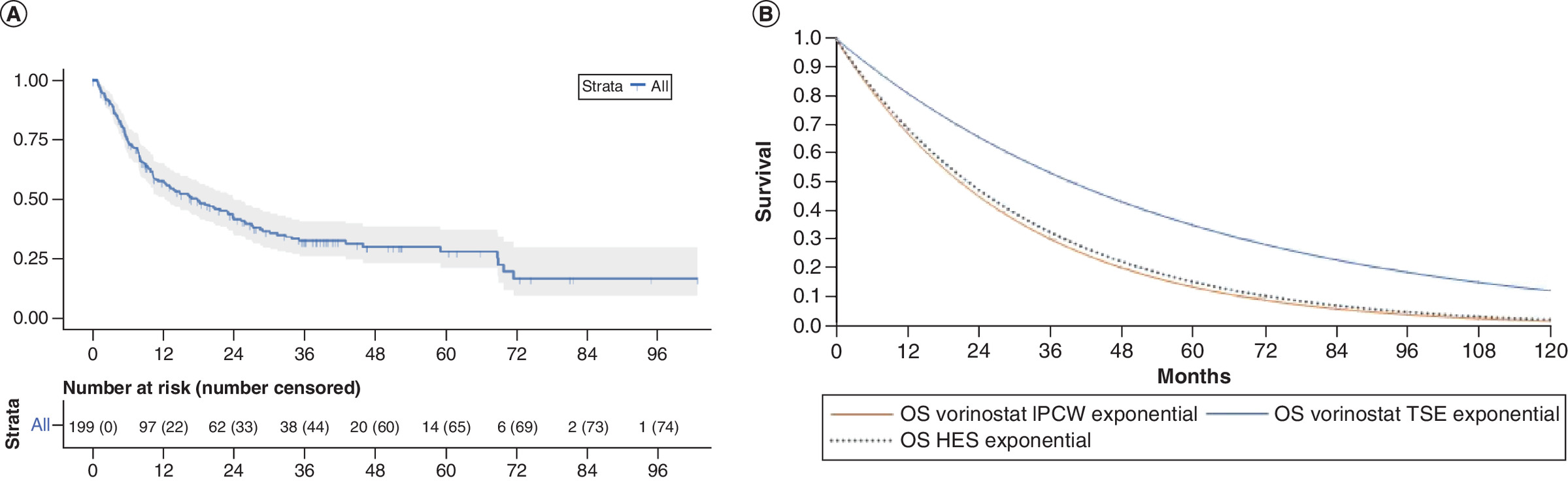
Figure 2. Overall survival compared to real world data.
(A) Hospital Episode Statistics overall survival for mycosis fungoides/Sézary syndrome participants and (B) comparison with adjusted vorinostat arm.
HES: Hospital Episode Statistics; IPCW: Inverse probability of censoring weights; OS: Overall survival; TSE: Two-stage estimation.
Median survival in the HES data was around 6 years from diagnosis and 1.5 years from initiation of second line systemic treatment for advanced MF/SS patients. Additionally, four large observational studies reported median OS from diagnosis in advanced MF/SS patients to be around 5 years from diagnosis, reducing to 1.5 years for stage IV patients (Table 3) [1–3,20]. These estimates are for a population with better life expectancy than in the MAVORIC trial due to a lower proportion (7–15%) of SS patients than in MAVORIC (47%) and a lower proportion of stage IV patients.
| Median survival for advanced patients | Source | Median survival | Details | Comments | Ref. |
|---|---|---|---|---|---|
| From diagnosis | Kim et al. 2003 | 1.5–4.0 years | 93% MF, 7% SS 94% stage IA-IIIB, median survival: 4 years 6% stage IVA1-IVB, median survival: 1.5 years | With lower proportion of stage IV patients, less heavily pre-treated, smaller proportion of SS than MAVORIC trial population | [2] |
| Agar et al. 2010 | 1.4–4.7 years | 93% MF, 7% SS 71% stage IA-IIA 18% stage IIB-IIIA, median survival: 4.7 years 4% stage IIIB, median survival: 3.4 years 4% stage IVA1, median survival: 3.8 years 2% stage IVA2, median survival: 2.1 years 1% stage IVB, median survival: 1.4 years | [1] | ||
| Talpur et al. 2012 | ∼5 years | 85% MF, 15% SS Stages not reported Estimated from Kaplan–Meier graphs | [3] | ||
| Scarisbrick et al. 2015 | 5.3 years | 36% stage IIB, median survival: 68 months 25% stage III, median survival: not reached 36% stage IVA, median survival: 47.5 months 3% stage IVB, median survival: 33 months | [20] | ||
| HES database | ∼6 years | 85% MF, 15% SS Stages not reported SS: 2.6 years; MF: not reached, 58% surviving at 6 years | Less heavily pre-treated, smaller proportion of SS than MAVORIC trial population | ||
| From the start of second-line systemic treatment | HES database | 1.5 years | – | With smaller proportion of SS than MAVORIC trial population | |
| From the start of second-line systemic treatment | For vorinostat arm from MAVORIC adjusted with IPCW | 1.8 years† | Advanced, non-switchers (detail in Table 1): 31% MF, 69% SS Stage IA-IIA: 12% Stage IIB: 23% Stage IIIA-IIIB: 15% Stage IVA1-IVB: 38% Unreported: 12% | Compared with HES and other observational datasets, higher proportion of SS and higher proportion of stage IVA+ patients | |
| For vorinostat arm from MAVORIC adjusted with TSE | 3.4 years† |
†
Once an exponential survival model has been fit to the data, see Figure 2B and detail in the Supplementary Material.
HES: Hospital Episode Statistics; IPCW: Inverse probability of censoring weights; MF: Mycosis fungoides; SS: Sézary syndrome; TSE: Two-stage estimation.
This is consistent with the IPCW results for advanced MF/SS patients from second line systemic treatment, while the TSE-adjusted results substantially exceed those for people receiving second line systemic treatment and is closer to the survival seen from diagnosis.
Clinical experts confirmed that the survival predictions for advanced MF/SS patients from second line systemic treatment by the TSE is not realistic.
Discussion
The treatment effect of mogamulizumab may be underestimated if crossover from vorinostat to mogamulizumab is not adjusted for. Extensive crossover reported for individuals randomized to vorinostat in MAVORIC possibly indicates poor disease control with vorinostat, reflected by a low response rate and rapid progression [9]. Adjusting for crossover is important for HTA decision making because decisions on treatment reimbursement should be made comparing the new experimental treatment with existing clinical practice where non-systematic crossover does not occur.
Adjusting for crossover resulted in a reduction of the OS HR for mogamulizumab compared with vorinostat, using both statistically appropriate methods (IPCW and TSE). However, there were uncertainties associated with both. The IPCW method may be biased in situations where there is a high proportion of switchers [21], such as the MAVORIC trial, whereas the TSE method relied on a very small number of patients (n = 28). The direction of the results for both crossover adjustment methods was the same. The choice between the two approaches required external validation.
Clinical plausibility using external data from UK RWE (HES database of all MF/SS patients treated in NHS England secondary care in the last 10-year period) and published observational data suggests that the TSE method overestimates survival from second line systemic treatment in advanced MF/SS. IPCW-adjusted vorinostat curves appeared to reflect the expected survival of advanced MF/SS participants in England. Therefore, external validation with real-world data supported the use of IPCW to adjust for treatment switching for the advanced MF/SS population in England. This results in an HR of 0.42 (95% CI: 0.18, 0.98) for mogamulizumab compared with vorinostat.
The strengths of this study are that it explored all NICE Decision Support Unit ‘complex’ methods to adjust for crossover. Extensive external validation was conducted using both RWE and published observational studies, which helped select the optimal approach.
Alternative methods may be more appropriate for obtaining an accurate estimate of the mogamulizumab treatment effect in the advanced MF/SS population. For example, an indirect comparison that adjusts for differences in patient populations between the mogamulizumab arm in MAVORIC and the observational arm from the HES database could be performed. Alternatively, trial protocols could pre-plan a synthetic control for situations where there is a high likelihood that crossover would occur.
Future research could consider how best to use RWE to select the optimal crossover approach. Further exploration of methods is particularly pertinent when more than one approach appear reasonable yet provide different estimates.
Conclusion
Non-systematic crossover should be adjusted for, particularly when the trial data are being used in HTA decision making. In the crossover adjustment of the MAVORIC trial, the two methods (IPCW and TSE) that were statistically appropriate demonstrated that mogamulizumab could improve OS once crossover had been adjusted for, which provides an important treatment option in a care setting where options are limited. External validation using RWE and published observational data supported the use of IPCW in this analysis, resulting in an HR of 0.42 (95% CI: 0.18, 0.98) for mogamulizumab compared with vorinostat.
The choice of crossover adjustment method should include both a statistical assessment of the approaches and external validation for clinical/biological plausibility. Choosing the best adjustment approach can be challenging, and it may not be clear which approach provides the best estimate of adjusted treatment effect. The use of external data can reduce uncertainties and has helped select not only a reasonable methodological approach for MAVORIC but also the most credible, considering local clinical practice.
•
There is an unmet need in second and subsequent line advanced mycosis fungoides and Sézary syndrome.
•
The MAVORIC trial compared mogamulizumab with vorinostat in patients with mycosis fungoides/Sézary syndrome and reported that patients treated with mogamulizumab had a progression-free survival benefit versus vorinostat.
•
Overall survival was confounded by 73% of vorinostat patients switching to mogamulizumab.
•
After adjusting for switching, the results suggested mogamulizumab improved overall survival.
•
This finding was supported using comparisons to real-world evidence.
Author contributions
N Hawkins performed the conceptualization and design of the research study, conducted the formal analysis of the data and reviewed the manuscript. N Muszbek performed the conceptualization and design of the research study and reviewed the manuscript. R Evans conducted the formal analysis of the data and wrote the manuscript. P Dequen-O'Byrne supervised the project and reviewed the manuscript. T Jones supervised the project and reviewed the manuscript. L McNamara supervised the project and reviewed the manuscript.
Financial & competing interests disclosure
N Hawkins, R Evans, P Dequen-O'Byrne and N Muszbek: advisory/consultancy for Kyowa Kirin, and are employees or directors of Visible Analytics L McNamara and T Jones: employees of Kyowa Kirin. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed. Editing and proofreading were provided by D H Bodicoat of Simplified Data. Development of this manuscript was supported by Kyowa Kirin. The authors have no other relevant affiliations or financialinvolvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
Supplementary Material
File (supplementary material.docx)
- Download
- 2.40 MB
References
Papers of special note have been highlighted as: • of interest
1.
Agar NS, Wedgeworth E, Crichton S et al. Survival outcomes and prognostic factors in mycosis fungoides/Sézary syndrome: validation of the revised International Society for Cutaneous Lymphomas/European Organisation for Research and Treatment of Cancer staging proposal. J. Clin. Oncol. 28(31), 4730–4739 (2010).
• Provides key observations on long-term real-world outcomes for patients with advanced mycosis fungoides and Sézary syndrome.
2.
Kim YH, Liu HL, Mraz-Gernhard S, Varghese A, Hoppe RT. Long-term outcome of 525 patients with mycosis fungoides and Sezary syndrome: clinical prognostic factors and risk for disease progression. Arch. Dermatol. 139(7), 857–866 (2003).
• Provides key observations on long-term real-world outcomes for patients with advanced mycosis fungoides and Sézary syndrome.
3.
Talpur R, Singh L, Daulat S et al. Long-term outcomes of 1,263 patients with mycosis fungoides and Sézary syndrome from 1982 to 2009. Clin. Cancer Res. 18(18), 5051–5060 (2012).
• Provides key observations on long-term real-world outcomes for patients with advanced mycosis fungoides and Sézary syndrome.
4.
Scarisbrick JJ, Whittaker S, Evans AV et al. Prognostic significance of tumor burden in the blood of patients with erythrodermic primary cutaneous T-cell lymphoma. Blood 97(3), 624–630 (2001).
5.
NHS Digital. Hospital Episode Statistics (HES) (2019). https://digital.nhs.uk/data-and-information/data-tools-and-services/data-services/hospital-episode-statistics
• Provides key observations on long-term real-world outcomes for patients with advanced mycosis fungoides and Sézary syndrome.
6.
Public Health England. National cancer registration and analysis services. Registration of cutaneous t-cell lymphoma (CTCL) in England (2016). www.ncin.org.uk/view?rid=3275
7.
Trautinger F, Eder J, Assaf C et al. European Organisation for Research and Treatment of Cancer consensus recommendations for the treatment of mycosis fungoides/Sézary syndrome – update 2017. Eur. J. Cancer 77, 57–74 (2017).
8.
Gilson D, Whittaker SJ, Child FJ et al. British Association of Dermatologists and U.K. Cutaneous Lymphoma Group guidelines for the management of primary cutaneous lymphomas 2018. Br. J. Dermatol. 180(3), 496–526 (2019).
9.
Kim YH, Bagot M, Pinter-Brown L et al. Mogamulizumab versus vorinostat in previously treated cutaneous T-cell lymphoma (MAVORIC): an international, open-label, randomised, controlled phase 3 trial. Lancet Oncol. 19(9), 1192–1204 (2018).
• The primary publication of the MAVORIC trial results.
10.
Duvic M, Hymes K, Heald P et al. Bexarotene is effective and safe for treatment of refractory advanced-stage cutaneous T-cell lymphoma: multinational phase II-III trial results. J. Clin. Oncol. 19(9), 2456–2471 (2001).
11.
Olsen EA, Kim YH, Kuzel TM et al. Phase IIb multicenter trial of vorinostat in patients with persistent, progressive, or treatment refractory cutaneous T-cell lymphoma. J. Clin. Oncol. 25(21), 3109–3115 (2007).
12.
European Medicines Agency. Poteligeo: European public assessment report (EPAR) (2019). www.ema.europa.eu/en/medicines/human/EPAR/poteligeo
13.
European Medicines Agency. Summary of product characteristics. Poteligeo® (mogamulizumab) (2019). www.ema.europa.eu/en/medicines/human/EPAR/poteligeo
14.
European Medicines Agency (EMA). Question and answer on adjustment for cross-over in estimating effects in oncology trials (2018). www.ema.europa.eu/en/documents/scientific-guideline/question-answer-adjustment-cross-over-estimating-effects-oncology-trials_en.pdf
15.
Sullivan TR, Latimer NR, Gray J, Sorich MJ, Salter AB, Karnon J. Adjusting for treatment switching in oncology trials: a systematic review and recommendations for reporting. Value Health 23(3), 388–396 (2020).
16.
Kyowa Kirin Pharmaceutical Development, Inc. Open-label, multi-center, randomized study of anti-CCR4 monoclonal antibody KW-0761 (mogamulizumab) versus vorinostat in subjects with previously treated cutaneous T-cell lymphoma (2012). https://clinicaltrials.gov/ct2/show/NCT01728805
17.
Latimer NR, Abrams KR. NICE DSU technical support document 16: adjusting survival time estimates in the presence of treatment switching. Decision Support Unit, ScHARR 57 (2014).
• A key publication for guidance on treatment switching adjustment methodologies.
18.
R Core Team. R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing, Vienna, Austria (2020). www.R-project.org/
19.
National Institute for Health and Care Excellence (NICE). Mogamulizumab for previously treated mycosis fungoides and Sézary syndrome [ID1405] – committee papers (2020). www.nice.org.uk/guidance/gid-ta10305/documents/committee-papers
20.
Scarisbrick JJ, Prince HM, Vermeer MH et al. Cutaneous lymphoma international consortium study of outcome in advanced stages of mycosis fungoides and Sézary syndrome: effect of specific prognostic markers on survival and development of a prognostic model. J. Clin. Oncol. 33(32), 3766–3773 (2015).
• Provides key observations on long-term real-world outcomes for patients with advanced mycosis fungoides and Sézary syndrome.
21.
Latimer NR, Abrams KR, Lambert PC et al. Adjusting for treatment switching in randomised controlled trials – a simulation study and a simplified two-stage method. Stat. Methods Med. Res 26(2), 724–751 (2017).
Information & Authors
Information
Published In
Pages: 805 - 813
PubMed: 35678206
Copyright
© 2022 The Authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 6 April 2022
Accepted: 20 May 2022
Published online: 9 June 2022
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Adjusting for treatment crossover in the MAVORIC trial: survival in advanced mycosis fungoides and Sézary syndrome. (2022) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2022-0070
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Harlan Campbell, Nicholas Latimer, Jeroen P Jansen, Shannon Cope, Augmented two-stage estimation for treatment switching in oncology trials: Leveraging external data for improved precision, Statistical Methods in Medical Research, 10.1177/09622802251374838, 34, 12, (2249-2269), (2025).
- Corrado Zengarini, Alba Guglielmo, Martina Mussi, Giovanna Motta, Claudio Agostinelli, Elena Sabattini, Bianca Maria Piraccini, Alessandro Pileri, A Narrative Review of the State of the Art of CCR4-Based Therapies in Cutaneous T-Cell Lymphomas: Focus on Mogamulizumab and Future Treatments, Antibodies, 10.3390/antib13020032, 13, 2, (32), (2024).
- Neil Hawkins, Noemi Muszbek, Rachel Evans, Linda McNamara, Trefor Jones, Overall survival in the UK in mycosis fungoides or Sézary syndrome cutaneous T-cell lymphoma: comparative effectiveness of mogamulizumab versus current standard of care, Journal of Comparative Effectiveness Research, 10.57264/cer-2023-0017, 12, 10, (2023).
- Noemi Muszbek, Edit Remak, Qian Xin, Linda McNamara, Trefor Jones, Cost–utility analysis of mogamulizumab in advanced mycosis fungoides and Sézary syndrome cutaneous T-cell lymphoma, Journal of Comparative Effectiveness Research, 10.57264/cer-2023-0028, 12, 7, (2023).