The impact of lower limb chronic venous disease on quality of life: patient and physician perspectives
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: This research compared patient and physician perceptions of quality of life (QoL) in C0–4 chronic venous disease (CVD). Methods: Qualitative standardized phone interviews were conducted with 100 patients and 60 specialists from Brazil, China, the Czech Republic, Italy and Russia. Results: In addition to the impact of physical symptoms on QoL, patient interviews revealed a high aesthetic and emotional burden of C0–4 CVD that contributes to social isolation and affects relationships. Physicians were aware of the physical impact but underestimated the other implications of CVD on their patients' QoL. Conclusion: Healthcare professional awareness of the overall impact of CVD on QoL needs improvement. All aspects of QoL should be assessed in order to manage CVD effectively.
Plain language summary
Chronic venous disease (CVD) is a progressive condition that occurs when the functioning of the veins, which are blood vessels that move blood back to the heart, is compromised, leading to swelling and other physical changes in the legs. CVD can be debilitating to those who suffer from it, so the authors surveyed 100 people with CVD as well as 60 physicians who treat them to understand more about the impact of this disease. The authors found that CVD affects people not only physically but also aesthetically and emotionally, which impacts on relationships and leads to social isolation. Physicians are aware of the physical impact of CVD but often underestimate other burdens their patients might experience, so the authors suggest that physicians consult their patients on these aspects when treating them.
Chronic venous disease (CVD) is a progressive condition characterized by long-standing morphological and functional venous abnormalities that primarily affect the lower limbs irrespective of whether they produce symptoms [1–3]. The spectrum of CVD physical symptoms and signs may comprise heaviness, pain, night cramps, itching, telangiectasias, varicosities, edema, skin hyperpigmentation, lipodermatosclerosis and (in severe cases) venous ulcers, all of which negatively affect patients' quality of life (QoL) [2,4,5].
CVD is usually described according to the Clinical–Etiological–Anatomical–Pathophysiological (CEAP) classification, which ranges from stage C0 (no visible or palpable signs of venous disease) to C6 (active venous ulcer), with each clinical class further characterized as symptomatic (s) or asymptomatic (a) [6]. According to global estimates, 19% of adults (or almost one person in five) have C2 CVD (varicose veins) [7]. When all C classes are included, the worldwide prevalence of CVD is high, with C0s–6 CVD occurring in 83.6% of the adult population consulting general practitioners in the international Vein Consult Program [8]. The majority (81.5%) of the population in the Vein Consult Program had C0s–4 CVD, whereas individuals with C5–6 disease (healed or active ulcers) represented only 2.1%. A more recent international web-based survey conducted in a representative sample of the general adult population from eight countries in Europe and South America demonstrated that 22% of respondents had symptoms of CVD [9]. Even individuals showing no clinical or diagnostic signs of lower limb CVD commonly experience CVD-like symptoms that can be attributed to venous hypertension during prolonged standing. This observation highlights the role of microcirculatory involvement in physiological venous insufficiency and further demonstrates the prevalence and importance of venous symptoms, including C0s CVD, in the general population [10,11].
CVD has an increasingly negative impact on QoL as the disease progresses [1,3,5,12–14]. Thus, QoL of CVD patients can become very poor, to the extent that QoL in individuals with venous ulceration is comparable with that of patients with congestive heart failure or chronic lung disease [4,15]. Several scales can be used to assess QoL of patients with CVD, including the Chronic Venous Insufficiency Questionnaire (CIVIQ), a validated, self-administered questionnaire that was specifically developed for patients with venous leg symptoms or signs but without active or healed ulceration (C0s–4) [16–18]. There is, however, limited information on the extent to which C0–4 CVD affects patients' QoL. The present international survey was conducted to further our understanding of the overall impact of C0s–4 CVD on patients' QoL and to identify any gaps between patient and physician perceptions of the impact of CVD on QoL, thereby pinpointing opportunities to improve management of the disease in patients without venous ulceration.
Methods
Research design & participants
This cross-sectional survey was conducted in Brazil, China, the Czech Republic, Italy and Russia. CVD specialists (vascular surgeons, angiologists and phlebologists) and patients aged ≥18 years with lower limb CEAP C0–4 CVD based on patients' perception were eligible to participate in the survey. In each country, patients and physicians were identified by local recruiters of the fieldwork agency (Research Partnership Ltd.) and from their local databases. A recruitment plan was predefined with a target number of 100 patients and 60 physicians (all CVD specialists). Patients participating in physician–patient paired interviews were recruited via physician referral (at least two patients from every participating physician were interviewed). Paired interviews accounted for a point of reference between the two sets of respondents.
Qualitative 60-min phone interviews were conducted separately with patients and physicians using standardized patient and physician discussion guides (Supplementary Appendices A & B) translated into all relevant languages. Interviews were conducted between 22 September and 26 October 2020. Before their phone interview, patients were asked to complete the 14-item CIVIQ (CIVIQ-14) [19,20], which has been validated in several international linguistic versions, including the five languages covered in this research (www.civiq-20.com/getting-copy/linguistic-versions-civiq-14/). CIVIQ-14 items were scored on a scale from 1 (no problems) to 5 (very high frequency/intensity).
Patient interviews
Patients were asked to quantify the impact of CVD on QoL on a scale of 1 (very low impact) to 5 (very high impact) across four dimensions: physical symptoms, aesthetics/appearance, emotional effects and relationships. Patients were also asked to use a scale of 1 (dissatisfied) to 5 (very highly satisfied) to quantify how satisfied they were with the way their physicians managed their QoL. Key qualitative questions posed to patients included the following: “How do these [CVD] symptoms impact your QoL? Please give me some examples in your daily life”; “Considering both night and day, which aspects of your daily life do they affect?”; and “Did they [the doctor] ask anything about your QoL? What did they say? How did they measure it?”. Patients completed the CIVIQ-14 before the interviews and were also asked qualitative questions about the questionnaire, including to what extent CIVIQ-14 covered significant problems impacting their QoL; whether anything that impacted their QoL was not included in the questionnaire; and what, if anything, could be done to improve the questionnaire.
Physician interviews
Physicians were asked to quantify their perception of the impact of CVD on their patients' QoL on a scale of 1 (very small impact) to 5 (very high impact) in relation to physical symptoms, aesthetics/appearance, emotional effects and relationships. They were also asked to use a scale of 1 (dissatisfied) to 5 (very highly satisfied) to quantify how satisfied they thought their patients were with how they were managing their QoL.
Key open-ended questions posed to physicians included the following: “Do you ask anything about QoL?”; “What do you say?”; and “How do you measure it?”. In addition, physicians were asked qualitative questions about CIVIQ-14. After being asked if they were aware of scores and scales used to measure QoL, physicians were asked to what extent they used CIVIQ-14 in practice. Physicians were then asked about the benefits, challenges, disadvantages and shortcomings of CIVIQ-14 and what, if anything, would need to change for them to use CIVIQ-14 in all patients.
Statistical methods
Research Partnership Ltd analyzed the results of this survey. Relevant numerical data were aggregated in Excel (Microsoft Corporation, WA, USA), and statistical testing was run via data tables and MERLIN 10 (Merlinco Ltd, London, UK) for means and Excel for proportions.
Potential sources of bias were addressed through a carefully designed screener and the geographical spread of the sample and via a double-blind approach. The sample size of n = 100 patients and n = 60 healthcare providers was selected so that two to three subgroups could be compared at a global level (e.g., male vs female, age categories and specialty type).
Descriptive statistics were calculated for rating scores obtained from phone interview questions and CIVIQ-14 scores. In addition to mean ± standard deviation (SD) values, results were expressed as proportions of patients with scores of 4 or 5. Differences between patient/physician subgroups as well as between patients and physicians were assessed using Pearson's chi-square (for proportions) or Z-tests (for means). The data met the assumptions of the tests. A difference with a two-sided p < 0.05 was considered significant. Responses to general qualitative questions were summarized according to emergent themes – namely, the number of times certain words, such as ‘anxious’, ‘embarrassed’, ‘scared’ or ‘worried’, were mentioned.
Research ethics
All participants gave their informed consent for the collection and use of medical and health information in an aggregated and pseudonymized manner for the purposes of this research only. Participants were paid an honorarium for participating in the survey.
The survey complied with UK data protection law, the British Healthcare Business Intelligence Association's legal and ethical guidelines and Association of the British Pharmaceutical Industry and Market Research Society codes of practice. As this was not an investigation of clinical outcomes with any particular intervention, neither ethics committee approval nor clinical trial registration was required in any of the countries involved in the survey. The research was conducted by Research Partnership Ltd (London, UK) and funded by Servier.
Results
Patient & physician characteristics
In total, 100 patients (20 from each participating country) and 60 physicians (12 from each participating country) were recruited. Overall, there were 31 physician–patient study pairs: 14 from Italy, eight from China, four from Russia, three from Brazil and two from the Czech Republic.
As shown in Table 1, most (69%) patients were female, 57% were aged 41–60 years, 25% were aged 18–40 years and 18% were aged >60 years. The mean age was 48.7 years (range: 21–79). BMI mean ± SD was 26.2 ± 7.2 kg/m2, and BMI was <40 kg/m2 in 93% of patients. BMI was >30, 25–30 and <25 kg/m2 in 53, 18 and 23% of C4 patients, respectively. Most patients either worked full-time or were retired. A total of 28% of patients had a job in which they were rarely standing, 28% had a job in which they were occasionally standing and 44% had a job in which they were frequently standing. The majority had been diagnosed 2–5 years previously and had started treatment within 3 months after diagnosis. CVD was C2–3 in 56% of patients, 75% of patients were taking a venoactive drug and most (64%) patients felt that CVD had a high impact on their QoL. In contrast, 28% of patients felt that CVD had a moderate impact on their QoL and 8% felt it had a low impact.
| Characteristic | Patients (n = 100) |
|---|---|
| Sex, n (%) | |
| Female | 69 (69.0) |
| Male | 31 (31.0) |
| Age, years, mean ± SD | 48.7 ± 11.5 |
| Age, years, n (%) | |
| 18–40 | 25 (25.0) |
| 41–60 | 57 (57.0) |
| ≥61 | 18 (18.0) |
| BMI, kg/m2, mean ± SD | 26.2 ± 7.2 |
| BMI, kg/m2, n (%) | |
| <25 | 57 (57.0) |
| 25–30 | 28 (28.0) |
| 31–40 | 8 (8.0) |
| >40 | 7 (7.0) |
| Frequency of standing, n (%) | |
| Frequent | 44 (44.0) |
| Occasional | 28 (28.0) |
| Rare | 28 (28.0) |
| CEAP classification, n (%) | |
| C0–1 | 18 (18.0) |
| Female† | 14 (20.3) |
| Male‡ | 4 (12.9) |
| C2–3 | 56 (56.0) |
| Female† | 36 (52.2) |
| Male‡ | 20 (64.5) |
| C4 | 26 (26.0) |
| Female† | 19 (27.5) |
| Male‡ | 7 (22.6) |
| Using VAD, n (%) | 75 (75.0) |
| Impact of CVD on QoL, n (%) | |
| High | 64 (64.0) |
| Low | 36 (36.0) |
†
Percentage calculated using all female patients (n = 69) as the denominator.
‡
Percentage calculated using all male patients (n = 31) as the denominator.
BMI: Body mass index; CEAP: Clinical–Etiological–Anatomical–Pathophysiological; CVD: Chronic venous disease; QoL: Quality of life; SD: Standard deviation; VAD: Venoactive drug.
Most (80%) physicians were male, >50% were vascular surgeons, 48% had >14 years experience managing patients with CVD and 53% had a CVD caseload of >90 patients per month (Table 2). There was a high level of venoactive drug prescribing (>55 per month in 52% of physicians), and 80% of physicians felt that CVD had a high impact on their patients' QoL.
| Characteristic | Physicians (n = 60) |
|---|---|
| Sex, n (%) | |
| Female | 12 (20.0) |
| Male | 48 (80.0) |
| Specialty, n (%) | |
| Angiologist | 14 (23.3) |
| Angiologist/phlebologist | 1 (1.7) |
| Phlebologist | 11 (18.3) |
| Vascular surgeon | 34 (56.7) |
| Years in practice, mean ± SD | 15.6 ± 8.8 |
| Years in practice, n (%) | |
| ≤14 | 31 (51.7) |
| >14 | 29 (48.3) |
| CVD caseload per month, mean ± SD | 119.9 ± 112.7 |
| CVD caseload per month, n (%) | |
| ≤90 | 28 (46.7) |
| >90 | 32 (53.3) |
| VAD prescriptions per month, mean ± SD | 79.4 ± 85.3 |
| VAD prescriptions per month, n (%) | |
| >55 | 31 (51.7) |
| ≤55 | 29 (48.3) |
| Impact of CVD on patients' QoL, n (%) | |
| High | 48 (80.0) |
| Low | 12 (20.0) |
CVD: Chronic venous disease; QoL: Quality of life; SD: Standard deviation; VAD: Venoactive drug.
Impact of CVD on QoL
Patient perspectives
The impact of CVD on QoL, as perceived by patients, increased with CEAP clinical class progression (Table 3). Compared with C0–1 and C2–3 patients, mean QoL scores for all dimensions of CVD (physical symptoms, aesthetics/appearance, effect on relationships and emotional burden) were significantly higher for C4 patients (p < 0.05). Significantly more patients with C4 disease than C0–1 or C2–3 disease rated the emotional burden of CVD and effect of CVD on relationships as having a high or very high impact on their QoL (p < 0.05) (Figure 1). There was also a trend toward a higher proportion of C4 versus C0–1 and C2–3 patients rating physical symptoms and aesthetics/appearance as having a high to very high impact on their QoL (46–69% of C4 patients vs 30–48% of C2–3 patients and 22–39% of C0–1 patients).
| Characteristic | Mean ± SD† | |||
|---|---|---|---|---|
| Physical symptoms | Aesthetics/appearance | Effect on relationships | Emotional burden | |
| Disease stage | ||||
| C0–1 (n = 18) | 2.8 ± 1.2 | 3.0 ± 1.5 | 1.8 ± 0.9 | 2.2 ± 1.0 |
| C2–3 (n = 56) | 3.0 ± 1.1 | 3.1 ± 1.3 | 2.0 ± 1.1 | 2.6 ± 1.2 |
| C4 (n = 26) | 3.5 ± 0.9‡ | 4.0 ± 1.2§ | 3.0 ± 1.3¶ | 3.4 ± 1.1# |
| Age, years | ||||
| 18–40 (n = 25) | 3.1 ± 1.0 | 3.3 ± 1.1 | 2.3 ± 1.2 | 3.0 ± 1.1 |
| 41–60 (n = 57) | 3.0 ± 1.1 | 3.4 ± 1.4 | 2.1 ± 1.2 | 2.6 ± 1.3 |
| >60 (n = 18) | 3.1 ± 1.0 | 3.3 ± 1.6 | 2.7 ± 1.4 | 2.8 ± 1.2 |
| Sex | ||||
| Male (n = 31) | 3.2 ± 0.9 | 3.0 ± 1.4 | 2.2 ± 1.3 | 2.7 ± 1.3 |
| Female (n = 69) | 3.0 ± 1.1 | 3.5 ± 1.3 | 2.3 ± 1.2 | 2.7 ± 1.2 |
| Country | ||||
| All (n = 100) | 3.1 ± 1.1 | 3.3 ± 1.4 | 2.3 ± 1.2 | 2.7 ± 1.2 |
| Brazil (n = 20) | 3.5 ± 1.3†† | 3.6 ± 1.4 | 2.6 ± 1.3‡‡ | 3.2 ± 1.4§§ |
| China (n = 20) | 3.2 ± 0.9 | 3.4 ± 1.4 | 2.0 ± 1.1 | 2.7 ± 0.9 |
| Czech Republic (n = 20) | 2.7 ± 1.1 | 3.1 ± 1.4 | 1.8 ± 0.9 | 2.1 ± 1.2 |
| Italy (n = 20) | 2.8 ± 1.0 | 3.1 ± 1.4 | 2.6 ± 1.4¶¶ | 2.6 ± 1.2 |
| Russia (n = 20) | 3.2 ± 0.8 | 3.6 ± 1.3 | 2.4 ± 1.3 | 3.1 ± 1.2## |
†
Impact scale of 1 (very low impact) to 5 (very high impact).
‡
p < 0.0358 versus C0–1 and p < 0.0295 versus C2–3 disease.
§
p < 0.0185 versus C0–1 and p < 0.0021 versus C2–3 disease.
¶
p < 0.0003 versus C0–1 and p < 0.0007 versus C2–3 disease.
#
p < 0.0002 versus C0–1 and p < 0.0029 versus C2–3 disease.
††
p < 0.0357 versus Czech Republic and p < 0.0409 versus Italy.
‡‡
p < 0.0236 versus Czech Republic.
§§
p < 0.0076 versus Czech Republic.
¶¶
p < 0.0316 versus Czech Republic.
##
p < 0.0085 versus Czech Republic.
SD: Standard deviation.
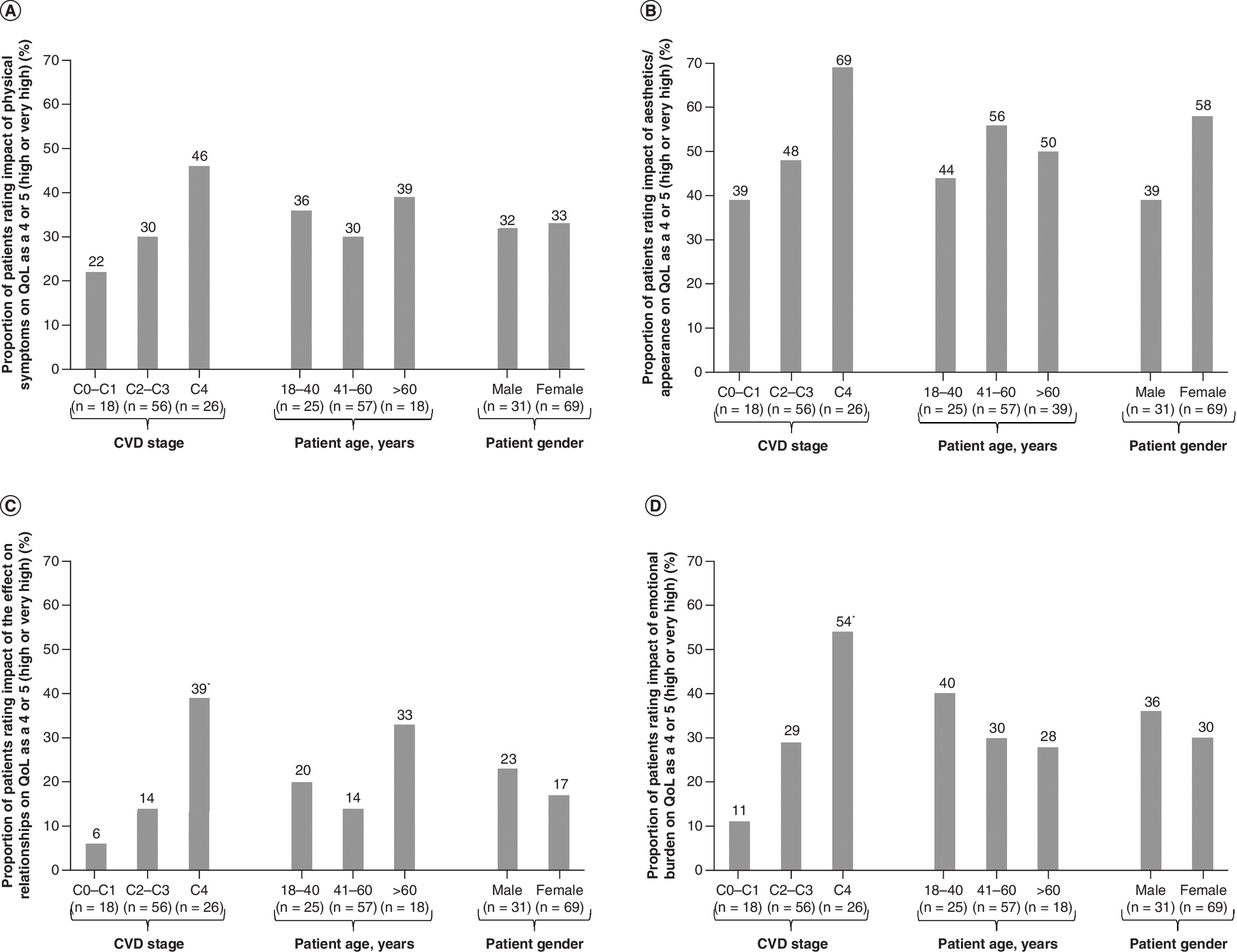
Figure 1. Proportions of patients who rated the impact of chronic venous disease on quality of life as a 4 or 5 on a scale of 1 (very low impact) to 5 (very high impact).
Ratings in relation to (A) physical symptoms, (B) aesthetics/appearance, (C) effect on relationships and (D) emotional burden according to disease stage, patient age and patient sex.
*p < 0.05 versus C0–1 and C2–3.
CVD: Chronic venous disease; QoL: Quality of life.
Younger patients (aged 18–40 years) and men tended to struggle more with the emotional burden of CVD compared with older patients and women, with 40% of younger patients and 36% of men rating the emotional burden of CVD as having a high or very high impact on their QoL versus ≤30% of older patients and women. The impact of CVD on relationships also tended to have a greater effect on the QoL of men than women, with a high or very high impact in 23% of men versus 17% of women. Subgroups of patients aged 18–60 years tended to fare better than older patients in this regard, with a high or very high impact in 14–20% of patients aged 18–60 years versus 33% of older patients. Leg aesthetics/appearance tended to affect the QoL of female patients to a greater extent than male patients, with a high or very high impact in 58% of female patients versus 39% of male patients.
Physician perspectives
In all countries, physician responses to survey questions indicated that they tend to focus on and overestimate the impact of physical symptoms. Globally, the mean QoL score was 3.7 ± 0.9 for the impact of physical symptoms compared with 3.4 ± 1.0 for aesthetic impact, 2.7 ± 1.1 for the effect of CVD on relationships and 3.3 ± 1.0 for emotional burden (Table 4).
| Characteristic | Mean ± SD† | |||
|---|---|---|---|---|
| Physical symptoms | Aesthetics/appearance | Effect on relationships | Emotional burden | |
| Sex | ||||
| Male (n = 48) | 3.7 ± 0.9 | 3.4 ± 1.1 | 2.7 ± 1.2 | 3.3 ± 1.0 |
| Female (n = 12) | 3.8 ± 0.9 | 3.3 ± 0.6 | 3.0 ± 1.0 | 3.3 ± 1.1 |
| Years in practice | ||||
| ≤14 (n = 31) | 3.8 ± 0.8 | 3.2 ± 1.0 | 2.9 ± 1.2 | 3.6 ± 1.2 |
| >14 (n = 29) | 3.6 ± 1.0 | 3.6 ± 1.0 | 2.5 ± 1.0 | 3.0 ± 0.7‡ |
| CVD caseload per month | ||||
| ≤90 (n = 28) | 3.7 ± 0.8 | 3.3 ± 1.1 | 2.5 ± 1.2 | 3.2 ± 1.2 |
| >90 (n = 32) | 3.8 ± 1.0 | 3.5 ± 0.8 | 2.9 ± 1.1 | 3.4 ± 0.9 |
| Country | ||||
| All (n = 60) | 3.7 ± 0.9§ | 3.4 ± 1.0 | 2.7 ± 1.1¶ | 3.3 ± 1.0# |
| Brazil (n = 12) | 3.8 ± 1.0 | 3.5 ± 0.8 | 3.1 ± 1.2 | 3.6 ± 1.1 |
| China (n = 12) | 3.6 ± 0.8 | 2.7 ± 1.2 | 2.3 ± 1.3 | 3.1 ± 1.2 |
| Czech Republic (n = 12) | 3.5 ± 0.9 | 3.1 ± 0.6 | 2.5 ± 0.8 | 3.0 ± 0.6 |
| Italy (n = 12) | 3.5 ± 0.5 | 4.1 ± 0.5††,‡‡,§§ | 3.0 ± 0.7 | 3.6 ± 0.7¶¶ |
| Russia (n = 12) | 4.2 ± 1.0 | 3.7 ± 1.1 | 2.7 ± 1.4 | 3.3 ± 1.3 |
†
Impact scale of 1 (very low impact) to 5 (very high impact).
‡
p < 0.0002 versus ≤14 years in practice.
§
p < 0.005 versus patient mean for physical symptoms.
¶
p < 0.026 versus patient mean for effect on relationships.
#
p < 0.0007 versus patient mean for emotional burden.
††
p < 0.0212 versus Brazil.
‡‡
p < 0.0001 versus China.
§§
p ≤ 0.0001 versus Czech Republic.
¶¶
p < 0.0030 versus patient mean for emotional burden.
CVD: Chronic venous disease; SD: Standard deviation.
When the results were analyzed according to years of practice (more experienced physicians with >14 years' practice versus less experienced physicians with ≤14 years' practice), some statistically significant differences were observed. Compared with physicians with ≤14 years' practice, a significantly higher proportion of more experienced physicians believed that the impact of CVD aesthetics on QoL was high (36 vs 69%; p < 0.0096). By contrast, a significantly lower proportion of more experienced versus less experienced physicians believed that the effect of CVD on patients' relationships had a high impact on QoL (14 vs 39%; p < 0.0292). This was also observed for the emotional burden of CVD, with 31% of physicians with >14 years' practice rating this as having a high impact on QoL versus 61% of less experienced doctors (p < 0.0189). The mean emotional burden score was also significantly higher when assessed by physicians with ≤14 years' practice rather than those with more experience (3.6 vs 3.0; p = 0.0171) (Table 4).
Physician versus patient perspectives
Overall, a significantly higher proportion of physicians (58%) than patients (33%) rated physical symptoms as having a high or very high impact on QoL (p < 0.0017) (Figure 2). The aesthetic impact of CVD on QoL was rated as high or very high by 52% of physicians and patients overall but tended to be underestimated by physicians in Brazil, Russia and China and overestimated by physicians in Italy. In most countries, and in the overall sample, a higher proportion of physicians than patients felt that the emotional burden and effect of CVD on relationships had a high or very high impact on patients' QoL (emotional burden: 47% of physicians vs 32% of patients; effect on relationships: 27% of physicians vs 19% of patients).
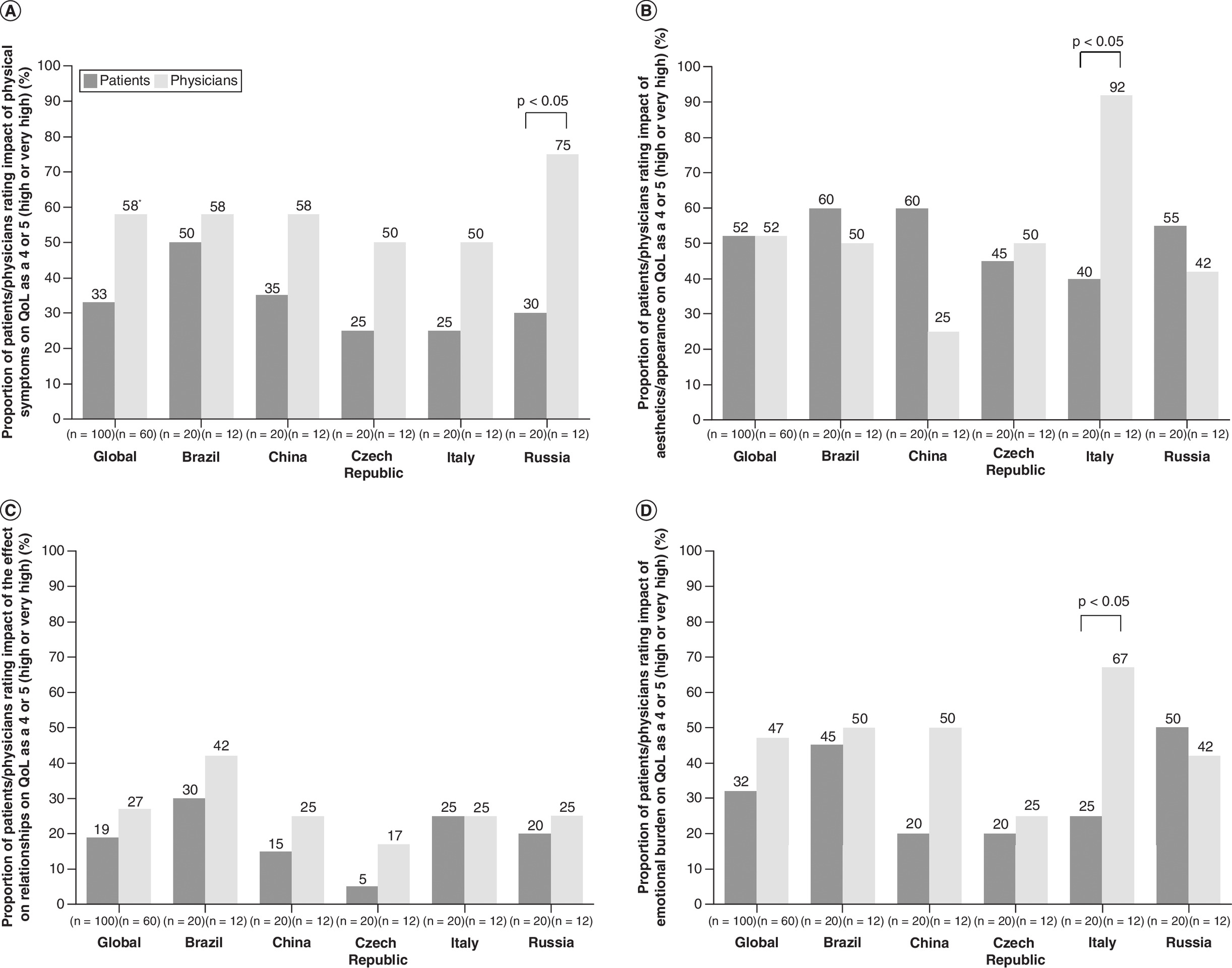
Figure 2. Proportions of patients and physicians† who rated the impact of chronic venous disease on quality of life as a 4 or 5 on a scale of 1 (very low impact) to 5 (very high impact).
Ratings in relation to (A) physical symptoms, (B) aesthetics/appearance, (C) effect on relationships and (D) emotional burden according to country.
*p < 0.05 versus physicians.
†Some physicians based their response on potential maximum impact in patients with the most severe disease.
QoL: Quality of life.
Management of QoL
In all countries, patients were significantly less satisfied with the management of their QoL than physicians perceived them to be, although the difference between physician and patient perceptions in Italy was minimal (Figure 3). Globally, the mean ± SD score was 4.1 ± 0.7 for physician-perceived patient satisfaction with physician management of QoL and 3.5 ± 1.4 for patient satisfaction with physician management of QoL (p < 0.0004). The mean ± SD physician-perceived patient satisfaction score was 4.4 ± 0.6 among more experienced physicians (>14 years' practice), which was significantly higher than that of less experienced physicians (3.8 ± 0.7; p < 0.0004). Both C4 and C2–3 patients were significantly less satisfied with their physicians than C0–1 patients were, with mean ± SD physician satisfaction scores of 3.0 ± 1.5 versus 4.2 ± 1.1 for C4 versus C0–1 patients (p < 0.0022) and 3.5 ± 1.3 versus 4.2 ± 1.1 for C2–3 versus C0–1 patients (p < 0.0249).
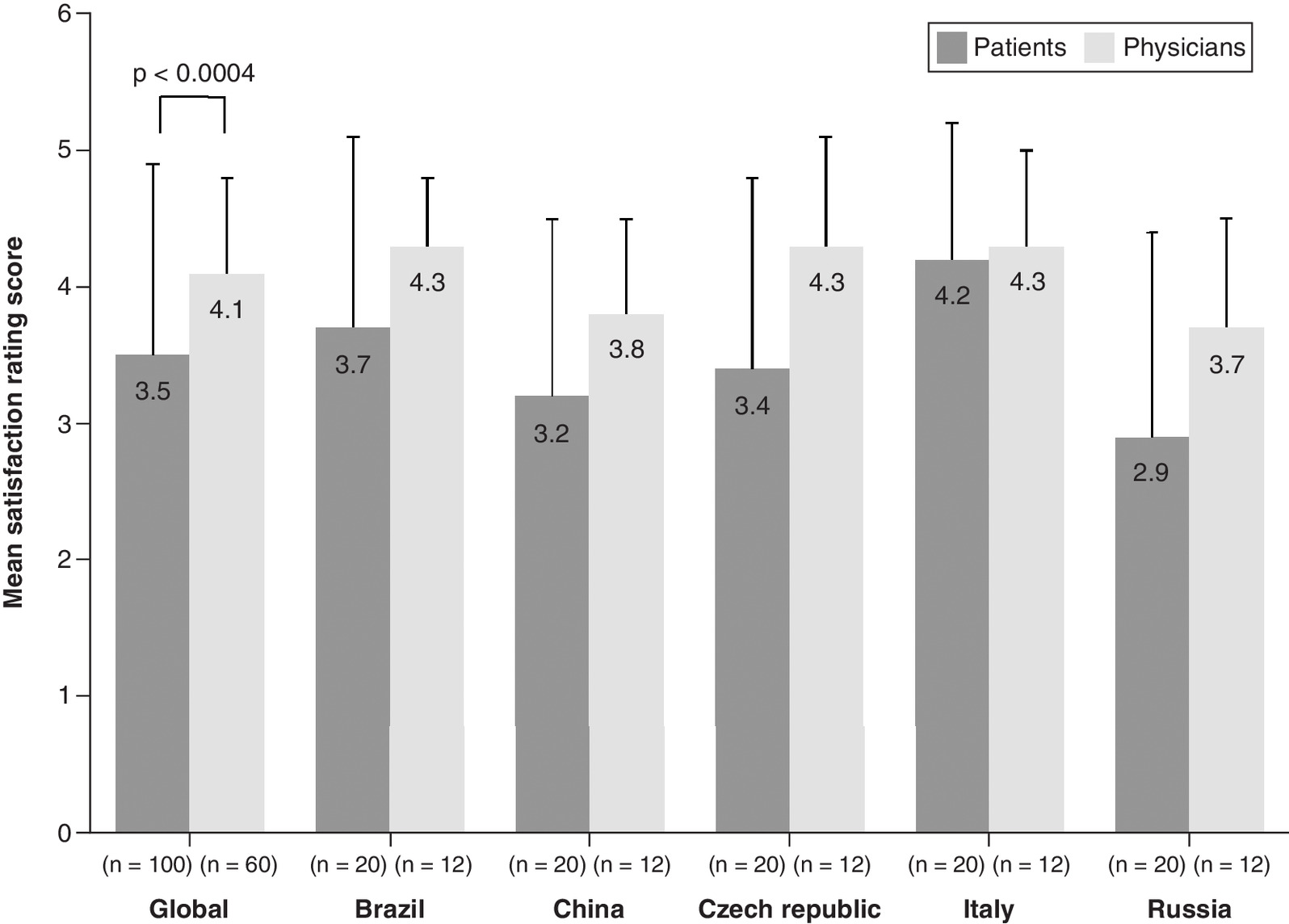
Figure 3. Mean scores for patient satisfaction with physician management of quality of life and physician perception of patient satisfaction with their quality of life management on a scale of 1 (dissatisfied) to 5 (very highly satisfied).
Error bars represent standard deviation.
CIVIQ-14 patient responses & physician use
The responses of patients to CIVIQ-14 questions showed that the emotional burden of CVD was as high as the physical burden (Figure 4). The most prominent emotional element of CVD was patient embarrassment about showing their legs (39% scored this item as a 4 or 5) followed by a tendency to feel nervous/tense and become easily irritated (18–20% scored these items as a 4 or 5). The mean ± SD score for the CIVIQ-14 embarrassment item in patients with C4 disease (3.6 ± 1.3) was significantly higher than that observed in C0–1 and C2–3 patients (2.4 ± 1.4 and 2.8 ± 1.3, respectively; C4 vs C0–1; p < 0.00034; C4 vs C2–3; p < 0.0143). Patients with C4 CVD also felt significantly more nervous/tense than patients with C0–1 CVD (mean ± SD score: 2.8 ± 1.1 vs 2.1 ± 1.1; p < 0.0383).
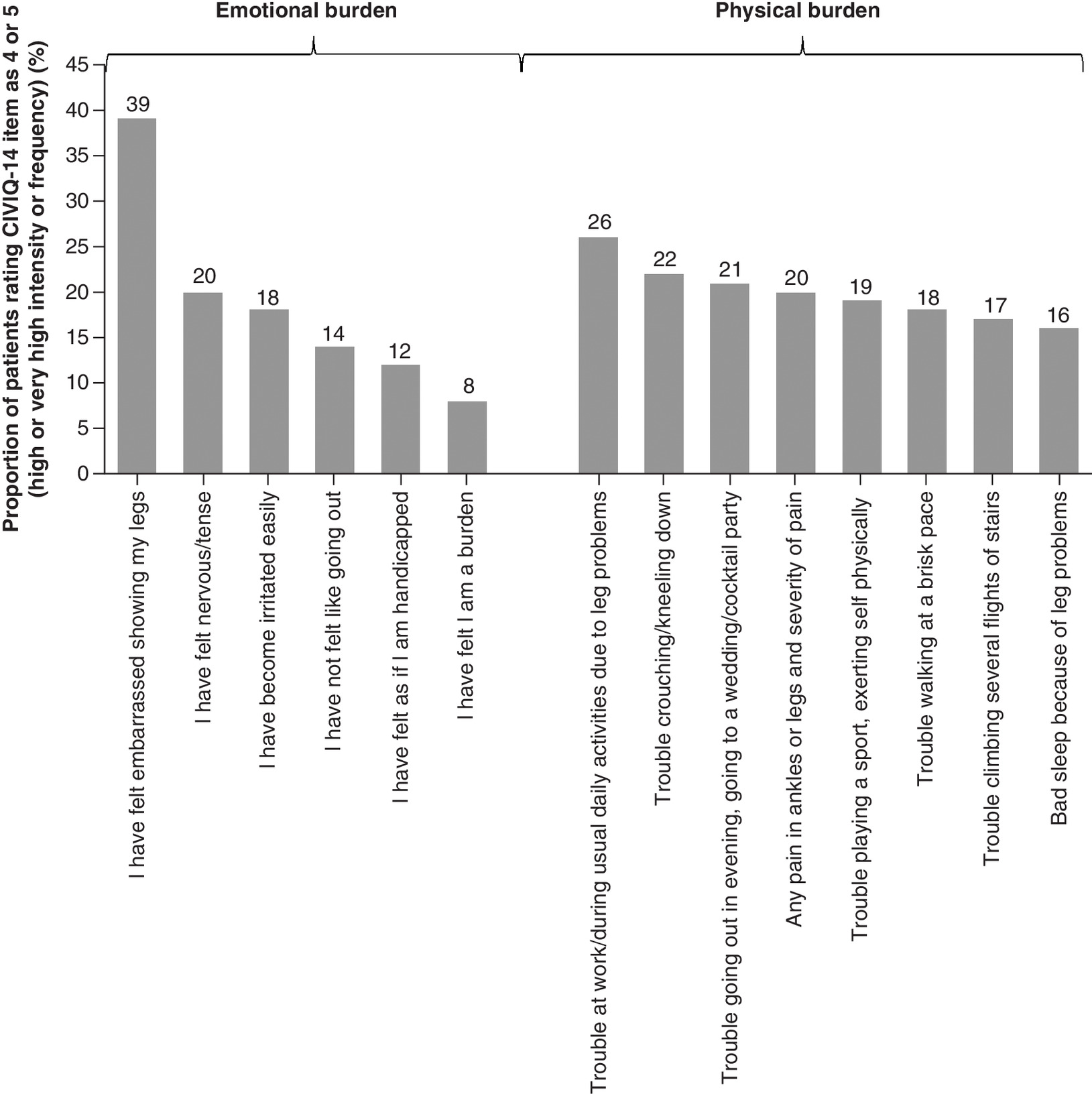
Figure 4. Proportions of patients who rated 14-item Chronic Venous Insufficiency Questionnaire items as a 4 or 5 on a scale of 1 (no symptom, pain or trouble) to 5 (highest intensity or frequency).
CIVIQ-14: 14-item Chronic Venous Insufficiency Questionnaire.
In relation to the physical burden of CVD, patients had trouble at work/undertaking daily activities due to leg problems (26% scored this item as a 4 or 5). Patients also had difficulty crouching/kneeling, going to social events and exerting themselves physically (19–22% scored these items as a 4 or 5). In addition, ankle and leg pain was highly or very highly problematic in 20% of patients and could have a profound impact on sleep (16% rated the CIVIQ-14 sleep item as a 4 or 5). Mean ± SD scores for CIVIQ-14 items showed that patients with C4 disease experienced a significantly greater burden than those with C0–1 disease in relation to the following items: trouble going out (2.6 ± 1.2 vs 1.8 ± 1.0; p < 0.0127), trouble at work (3.1 ± 1.0 vs 2.4 ± 1.0; p < 0.0224), trouble playing sports (2.9 ± 1.1 vs 2.0 ± 0.8; p < 0.0017) and ankle/leg pain (3.2 ± 0.8 vs 2.3 ± 0.6; p < 0.05). In C2–3 patients, the mean ± SD ankle/leg pain score (2.8 ± 1.0; p < 0.0272) was significantly lower than that observed in C4 patients, and the mean ± SD trouble going out score (2.5 ± 1.2; p < 0.0115) was significantly higher than that observed in those with C0–1 CVD.
When asked about CIVIQ-14, 80% of patients said they felt the questionnaire covers most of the important elements of CVD that affect QoL, including social impact, daily activities, pain, work, treatment and sleep. However, they also felt that CIVIQ-14 focuses on the functional aspects of CVD and does not adequately address the psychological impact of the disease. Other areas left unaddressed by CIVIQ-14 but essential from the perspective of patients included the aesthetic impact of CVD (especially for younger women), the impact of CVD on clothing choices and the financial burden of CVD (i.e., out-of-pocket expenses, such as compression stockings).
There was very low awareness of CIVIQ-14 and other CVD QoL scales among physicians. Physicians considered CIVIQ-14 useful in theory but more suited to academic research and generally would not use it to measure QoL in routine practice because of consultation time constraints. However, physicians specified that they would most likely use CIVIQ-14 when assessing treatment response in patients with C4–6 disease.
General findings
Aspects of CVD that affect relationships and contribute to the physical, aesthetic and emotional burden of the disease, as highlighted by patients, are summarized in Supplementary Box 1. The signs and symptoms of CVD mentioned in interviews with patients typically included varicose veins, leg pain and swollen or heavy legs, all of which contribute to the physical burden of the disease. Trends were observed for increased severity of varicose veins in women versus men and patients with C4 versus C0–3 CVD and increased severity of leg pain in patients with C4 versus C0–3 CVD. The aesthetic burden of the disease was highlighted, particularly in female patients and those with higher-stage disease. It was also evident that CVD contributes to a high emotional burden and directly affects patients' relationships.
Physicians typically considered the emotional impact of CVD to be high only in female patients with C3–4 disease, and they often did not recognize that male patients and those with early-stage disease also struggle emotionally and may require additional support. Patients tended to recall being asked about exercise and their daily routine, noting that emotions and feelings have not been a key focus of discussions with their physicians.
Disturbed sleep was a problem for around 25% of patients (Supplementary Box 2) and has a major impact on their lives and relationships. Disturbed sleep tended to be most problematic for patients with C3–4 CVD. Unless a patient raised the issue themselves, physicians acknowledged that they do not routinely ask patients about their sleep function, especially in patients with C0–2 disease.
Only about 50% of patients across all disease severities recalled being specifically asked about their QoL by their physician. Physicians typically considered that the emotional burden and effect of CVD on relationships had a high or very high impact on QoL in patients with more severe CVD. In general, patients highlighted a lack of holistic information (i.e., advice on diet/nutrition and exercise to help manage CVD) during consultations with their physician and reported leaving these consultations feeling uninformed, worried and anxious.
Discussion
The authors' study is one of the first to simultaneously assess patients' and physicians' perspectives on the impact of CEAP C0–4 CVD on all dimensions of QoL, including physical, emotional, relational and aesthetic aspects. The results of the survey show that physicians tend to place a heavy emphasis on physical symptoms when assessing patients with C0–4 CVD and do not always have time to comprehensively assess the impact of CVD on their patients' QoL. From the perspective of patients, the aesthetic impact of CVD and the effects of the disease on their emotional well-being and relationships were identified as important issues for which additional support may be required.
Irrespective of age or sex, the authors' results indicate that CEAP class C0s–4 CVD can negatively impact patients' QoL, with symptoms such as pain and swelling limiting their ability to carry out daily tasks, participate in work or leisure activities, socialize and sleep well. In addition to the negative impact of physical symptoms on QoL, the authors found that C0–4 CVD has a high emotional burden, instilling anxiety and fear about the future, particularly for younger patients (aged 18–40 years). Furthermore, a high proportion of patients participating in the authors' survey found the appearance of varicose veins and other aesthetic problems upsetting. This was particularly, but not exclusively, the case for female patients, who may be more concerned than men about their appearance [21,22]. Anxiety, embarrassment, low self-esteem and social isolation associated with aesthetic problems contributed to the emotional burden of CVD in the authors' patients and had a detrimental effect on their relationships.
Consistent with what is already known about CVD [1,3–5,12,13], the authors' questioning showed that the negative impact of CVD on QoL increases as the clinical class of the disease progresses to CEAP C4. However, although a relatively high proportion of patients with C4 disease (39–69%) rated CVD physical symptoms, aesthetics/appearance, effect on relationships and emotional burden as having a high or very high impact on their QoL, these aspects of CVD also had a high or very high impact on the QoL of a substantial proportion of patients with earlier-stage disease (14–48% with C2–3 CVD and 6–39% with C0–1 CVD).
It has previously been shown that compared with the general population, QoL is significantly worse in patients with varicose veins (C2 CVD) [23,24], and that even very early-stage CVD (C0s) can have a negative effect on QoL [12]. The authors' findings add to the small body of literature showing that QoL can be affected in patients with early-stage CVD disease. In addition to the burden of physical symptoms (22–30% of patients with C0–3 disease rated this as having a high or very high impact on QoL), the authors' patient interviews revealed that early-stage CVD could be associated with a high emotional burden (11% of patients with C0–1 disease and 29% of patients with C2–3 disease rated the emotions associated with CVD as having a high or very high impact on QoL). Aesthetics/appearance may also be bothersome at an early stage, with 39% of patients with C0–1 disease and 48% of patients with C2–3 disease rating the impact of aesthetics/appearance on QoL as high or very high.
Patient responses to CIVIQ-14 indicated that the emotional burden of CVD is as high as the physical burden. Physician interviews revealed that although physicians have a good understanding of the physical impact of CVD, most mistakenly believe that emotional problems primarily occur only in the later stages of the disease and in female patients. Therefore, physicians tend to underestimate the emotional impact of CVD, particularly in patients with early-stage disease and in male patients. Although more experienced physicians (>14 years' practice) were most aware of the aesthetic impact of CVD on patients' QoL, less experienced physicians seemed be more aware of the potentially high emotional burden of CVD.
Physicians acknowledged that they often assess QoL solely by asking general questions about symptoms and functionality without broaching the emotional impact of CVD. It was also apparent that physicians may not be fully aware of the extent to which sleep disturbances can affect the QoL of patients with C0–4 disease and seldom asked their patients questions addressing sleep disturbances. As has been reported for patients with venous ulceration [13], the more informed the patient is, the more empowered and accepting of the disease they are likely to feel. However, patients in the authors' survey pointed out that they have often felt poorly informed about their disease after consultations with their physicians.
With the exception of Italy, patient interviews revealed wide gaps between patient satisfaction with the management of their QoL and physician perception of patient satisfaction. Physician-referred patients (physician–patient study pairs) tended to be more satisfied than non-paired patients (mean satisfaction rating score: 4.0 vs 3.25). The high number of Italian physicians paired with patients (14 vs two to eight in other countries) may therefore have resulted in a response bias that influenced the Italian patient satisfaction rating scores.
To ensure that all CVD patients receive appropriate treatment that provides symptom relief, slows disease progression and improves QoL, physicians must be proactive and ask targeted questions rather than waiting for patients to raise problems that they may think the physician will consider unimportant or untreatable [25]. For example, the qualitative portion of the authors' study highlighted the major impact that sleep disturbance has on the lives of patients with C0–4 CVD, and physicians should therefore consider asking all patients how their sleep may be affected.
Although treatment guidelines acknowledge that assessment of QoL in patients with CVD is integral to a complete and thorough evaluation of their disease status and list disease-specific scales that are available to assist with this [26,27], such scales were not being used in clinical practice by the physicians participating in the authors' research. Although physicians acknowledged that CIVIQ-14 could be useful for tracking patient progress and symptoms, they reported that a major drawback to its use in clinical practice is its perceived incompatibility with short consultation times. Patient interviews also indicated that although CIVIQ-14 questions cover important elements of CVD affecting QoL, including sleep disturbances and some of the emotional aspects of the disease that physicians tend to neglect, there is a need for further customization to incorporate other important items, including the aesthetic and psychological impact of CVD; the impact of CVD on specific exercises/activities, clothing and diet; and the financial burden of the disease.
The findings of the authors' study are limited by the small sample size and reliance on respondents to provide accurate information. In addition, the authors' research may be subject to participation bias because participants were financially remunerated for completing the survey. Compared with general populations, differences in working habits and conditions, lifestyles, BMI, salary and educational levels might also have introduced bias. Furthermore, compared with the Vein Consult Program population [8], a relatively high proportion of patients participating in the authors' survey had C2–4 CVD (40.1 vs 82%), which may have accentuated some of the trends observed in the survey. Although the authors did assess QoL across a number of countries, the results may not be generalizable to other populations. In addition, as previously mentioned, there was an imbalance of physician–patient paired interviews in different countries, which increased the potential for response bias in countries with the highest numbers of physician–patient pairs. The non-validated nature of the phone interview questions may also limit the relevance of the authors' findings.
Conclusion
CEAP class C0s–4 CVD can negatively impact patients' QoL irrespective of age or sex, increasingly affecting not only physical but also emotional, relational and aesthetic aspects of patients' lives as the clinical class of the disease progresses to C4. Physicians and patients perceive the impact of C0–4 CVD on QoL differently. Although physicians are aware that patients with C0–4 CVD are impacted physically, they may underestimate the emotional, aesthetic and relational impacts of the disease in these patients. Greater physician awareness of the importance of assessing and supporting the emotional well-being of their patients would help to serve the needs of patients with C0–4 CVD. Development and widespread implementation of a simple CVD QoL scale that assesses all aspects of QoL, including physical, emotional and social well-being, and could be quickly completed by patients before their appointments would help to achieve this.
•
Chronic venous disease (CVD) has an increasingly negative impact on quality of life (QoL) as the Clinical–Etiological–Anatomical–Pathophysiological clinical class progresses, but compared with patients with Clinical–Etiological–Anatomical–Pathophysiological class C5–6 disease (healed or active ulcers), little is known about QoL in patients without venous ulceration (Clinical–Etiological–Anatomical–Pathophysiological class C0s–4 disease).
•
A qualitative phone survey of 100 patients with C0–4 CVD and 60 specialist physicians (vascular surgeons, angiologists and phlebologists) was conducted in Brazil, China, the Czech Republic, Italy and Russia.
•
A high proportion of patients with C4 disease (up to 69%) rated CVD physical symptoms, aesthetics/appearance, effect on relationships and emotional burden as having a high or very high impact on their QoL.
•
CVD physical symptoms, aesthetics/appearance, effect on relationships and emotional burden also had a high or very high impact on the QoL of a substantial proportion of patients with C0–3 disease (up to 48% with C2–3 CVD and up to 39% with C0–1 CVD).
•
Patients perceived the emotional burden of CVD to be as high as the physical burden, but physicians tended to overestimate the impact of physical symptoms on QoL or underestimate the emotional burden.
•
Patients indicated that painful legs lead to disturbed sleep, and this tended to be most problematic for patients with C2–3 or C4 CVD.
•
Physicians often assessed QoL by asking only general questions about symptoms and functionality. Patients tended to be less satisfied with the management of their QoL than physicians perceived them to be.
•
Although physicians acknowledged that the 14-item Chronic Venous Insufficiency Questionnaire, which includes questions on some of the emotional elements of CVD, could be useful for tracking QoL in C0–4 patients, they would not use such a tool in clinical practice because of perceived incompatibility with short consultation times.
Author contributions
E Braund and C Fradet-Aubignat contributed to study design; enrolled respondents via fieldwork partners; performed analyses, including statistical analysis; prepared the study report; and read and approved drafts of the manuscript. C Regnier and T Peudon contributed to study design, read and revised the study report and manuscript drafts and approved the final versions. FR Santiago, J Ulloa and S Gianesini contributed to study design; analysis; interpretation of results; and manuscript drafts, including critical revision and approval of the final version. All authors have access to all anonymized data. The decision to submit this research for publication was made by C Régnier and T Peudon.
Financial & competing interests disclosure
This research was funded by Servier. C Régnier and T Peudon are employees of Servier. E Braund and C Fradet-Aubignat are employees of Research Partnership Ltd. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Medical writing assistance was provided by J Dalton, who wrote the first draft on behalf of Springer Healthcare Communications. This medical writing assistance was funded by Servier.
Ethical conduct of research
Before participating in the research, all physicians and patients were asked to provide permission to share medical and health information and were informed that they would be paid an honorarium for participating in the survey. Participants' data were used in a general and anonymized manner for the purposes of this research only and were not provided to any third party. The research complied with UK data protection law, the British Healthcare Business Intelligence Association's legal and ethical guidelines and Association of the British Pharmaceutical Industry and Market Research Society codes of practice. As this was not an investigation of clinical outcomes with any particular intervention, neither ethics committee approval nor clinical trial registration was required.
Data sharing statement
The anonymized data that support the findings of this study are available on reasonable request from the corresponding author.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary materials.docx)
- Download
- 54.01 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Bergan JJ, Schmid-Schonbein GW, Smith PD, Nicolaides AN, Boisseau MR, Eklof B. Chronic venous disease. N. Engl. J. Med. 355(5), 488–498 (2006).
2.
Eklof B, Perrin M, Delis KT et al. Updated terminology of chronic venous disorders: the VEIN-TERM transatlantic interdisciplinary consensus document. J. Vasc. Surg. 49(2), 498–501 (2009).
3.
Onida S, Davies AH. Predicted burden of venous disease. Phlebology 31(Suppl. 1), 74–79 (2016).
4.
Davies AH. The seriousness of chronic venous disease: a review of real-world evidence. Adv. Ther. 36(Suppl. 1), 5–12 (2019).
5.
Nicolaides AN, Labropoulos N. Burden and suffering in chronic venous disease. Adv. Ther. 36(Suppl. 1), 1–4 (2019).
6.
Lurie F, Passman M, Meisner M et al. The 2020 update of the CEAP classification system and reporting standards. J. Vasc. Surg. Venous Lymphat. Disord. 8(3), 342–352 (2020).
•• Provides the most recent update of the Clinical–Etiological–Anatomical–Pathophysiological classification system.
7.
Salim S, Machin M, Patterson BO, Onida S, Davies AH. Global epidemiology of chronic venous disease: a systematic review with pooled prevalence analysis. Ann. Surg. 274(6), 971–976 (2021).
8.
Rabe E, Guex JJ, Puskas A, Scuderi A, Fernandez Quesada F. Epidemiology of chronic venous disorders in geographically diverse populations: results from the Vein Consult Program. Int. Angiol. 31(2), 105–115 (2012).
•• Provides real-world data on the epidemiology of chronic venous disorders.
9.
Rabe E, Regnier C, Goron F, Salmat G, Pannier F. The prevalence, disease characteristics and treatment of chronic venous disease: an international web-based survey. J. Comp. Eff. Res. 9(17), 1205–1218 (2020).
• Provides real-world data on chronic venous disease (CVD).
10.
Blättler W, Thomae HJ, Amsler F. Venous leg symptoms in healthy subjects assessed during prolonged standing. J. Vasc. Surg. Venous Lymphat. Disord. 4(4), 455–462 (2016).
11.
Rabe E, Pannier F. What have we learned from the Bonn Vein Study? Phlebolymphology 13(4), 188–193 (2006).
• Reviews the Bonn Vein Study.
12.
Branisteanu DE, Feodor T, Baila S, Mitea IA, Vittos O. Impact of chronic venous disease on quality of life: results of vein alarm study. Exp. Ther. Med. 17(2), 1091–1096 (2019).
13.
Wellborn J, Moceri JT. The lived experiences of persons with chronic venous insufficiency and lower extremity ulcers. J. Wound Ostomy Continence Nurs. 41(2), 122–126 (2014).
14.
Kahn SR, M'lan CE, Lamping DL et al. Relationship between clinical classification of chronic venous disease and patient-reported quality of life: results from an international cohort study. J. Vasc. Surg. 39(4), 823–828 (2004).
• Compares clinical classification and quality of life in CVD.
15.
Carradice D, Mazari FA, Samuel N, Allgar V, Hatfield J, Chetter IC. Modelling the effect of venous disease on quality of life. Br. J. Surg. 98(8), 1089–1098 (2011).
16.
Kuet ML, Lane TR, Anwar MA, Davies AH. Comparison of disease-specific quality of life tools in patients with chronic venous disease. Phlebology 29(10), 648–653 (2014).
17.
Launois R. Health-related quality-of-life scales specific for chronic venous disorders of the lower limbs. J. Vasc. Surg. Venous Lymphat. Disord. 3(2), 219–227.e1-3 (2015).
18.
Wu Z, Ma Y. A narrative review of the quality of life scales specific for chronic venous diseases. Medicine (Baltimore) 100(20), e25921 (2021).
19.
Launois R, Le Moine JG, Lozano FS, Mansilha A. Construction and international validation of CIVIQ-14 (a short form of CIVIQ-20), a new questionnaire with a stable factorial structure. Qual. Life Res. 21(6), 1051–1058 (2012).
•• Describes the 14-item Chronic Venous Insufficiency Questionnaire (CIVIQ-14).
20.
Le Moine JG, Fiestas-Navarrete L, Katumba K, Launois R. Psychometric validation of the 14 items ChronIc Venous Insufficiency Quality of Life Questionnaire (CIVIQ-14): confirmatory factor analysis. Eur. J. Vasc. Endovasc. Surg. 51(2), 268–274 (2016).
21.
Amsler F, Rabe E, Blattler W. Leg symptoms of somatic, psychic, and unexplained origin in the population-based Bonn Vein Study. Eur. J. Vasc. Endovasc. Surg. 46(2), 255–262 (2013).
22.
Martinez-Gonzalez MC, Martinez-Gonzalez RA, Guerra-Tapia A. Esthetic dermatology and emotional well-being according to gender. J. Cosmet. Dermatol. 17(3), 410–416 (2018).
23.
Smith JJ, Garratt AM, Guest M, Greenhalgh RM, Davies AH. Evaluating and improving health-related quality of life in patients with varicose veins. J. Vasc. Surg. 30(4), 710–719 (1999).
24.
Sritharan K, Lane TR, Davies AH. The burden of depression in patients with symptomatic varicose veins. Eur. J. Vasc. Endovasc. Surg. 43(4), 480–484 (2012).
25.
Sheikh P. The patient experience in venous disease. J. Comp. Eff. Res. 9(17), 1167–1169 (2020).
26.
Nicolaides A, Kakkos S, Baekgaard N et al. Management of chronic venous disorders of the lower limbs. Guidelines according to scientific evidence. Part II. Int. Angiol. 39(3), 175–240 (2020).
•• Provides 2020 guidelines on chronic venous disorders.
27.
De Maeseneer MG, Kakkos SK, Aherne T et al. European Society for Vascular Surgery (ESVS) 2022 clinical practice guidelines on the management of chronic venous disease of the lower limbs. Eur. J. Vasc. Endovasc. Surg. 63(2), 184–267 (2022).
•• Provides 2022 guidelines on chronic venous disorders.
Information & Authors
Information
Published In
Pages: 789 - 803
PubMed: 35642553
Copyright
© 2022 Fabricio Rodrigues Santiago. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 16 March 2022
Accepted: 5 May 2022
Published online: 1 June 2022
Keywords:
Topics
Authors
Funding Information
Servier
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
The impact of lower limb chronic venous disease on quality of life: patient and physician perspectives. (2022) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2022-0054
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Efthymios D. Avgerinos, Spyros N. Vasdekis, Dimitrios G. Kardoulas, Garyfallia Stefanou, Georgia Kourlaba, Antonios Papageorgiou, Prevalence of Chronic Venous Disease and Quality of Life in the Adult Greek Population: Results from the VeinProtect Study, European Journal of Vascular and Endovascular Surgery, 10.1016/j.ejvs.2025.09.016, 71, 4, (661-670), (2026).
- undefined Paweł Grzesikowski, undefined Jakub Kubiak, undefined Paulina Klich, undefined Kinga Bekier, undefined Hanna Nowicka, IMPACT OF PHYSICAL ACTIVITY ON SYMPTOM SEVERITY AND QUALITY OF LIFE IN CHRONIC VENOUS DISEASE: A SYSTEMATIC REVIEW, International Journal of Innovative Technologies in Social Science, 10.31435/ijitss.1(49).2026.4924, 1(49), (2026).
- Olena O. Dyadyk, Valentyn A. Khodos, Hlib O. Melnychuk, Mykhailo S. Myroshnychenko, Kateryna I. Popova, Morphological features of the great saphenous vein in patients with chronic venous disease of the lower extremities undergoing the most common endovenous treatment techniques, Polski Merkuriusz Lekarski, 10.36740/Merkur202504111, 53, 4, (509), (2025).
- Yunjiao Wang, Rui Li, Liping Bai, Zhuanfang Zou, Chunyan Zheng, Feijin Peng, Shuzhen Wang, Yujin Yang, A study of social isolation in patients with varicose veins of the lower extremities: A scoping review, Journal of Tissue Viability, 10.1016/j.jtv.2024.09.012, 33, 4, (930-937), (2024).
- Vitória Estéfani Almeida Silva, Estefane Theophilo de Freitas Pereira, Juliana Alves Ferreira, Andrew Magno Teixeira, Ricardo Moreira Borges, Luiz Cláudio Rodrigues Pereira da Silva, Bioactive Compounds in Citrus Species with Potential for the Treatment of Chronic Venous Disease: A Review, Current Pharmaceutical Design, 10.2174/0113816128314974240724045220, 30, 36, (2835-2849), (2024).
- K.V. Lobastov, V.V. Kozlova, A.V. Kovalchuk, A.B. Bargandzhiya, L.A. Laberko, Place and role of compression therapy in modern minimally invasive treatment of varicose veins, Journal of Venous Disorders, 10.17116/flebo202418031246, 18, 3, (246), (2024).
- Binoy Kumaran, Darren Targett, Tim Watson, Benefits of home-based foot neuromuscular electrical stimulation on self-reported function, leg pain and other leg symptoms among community-dwelling older adults: a sham-controlled randomised clinical trial, BMC Geriatrics, 10.1186/s12877-024-05271-z, 24, 1, (2024).
- Peter R. Corridon, Zehara M. Ali, Meklit G. Shibru, Jovana Paunovic, Igor V. Pantic, Shaun H. Preston, Sustainable varicose vein therapy using functionalized hydrogels derived solely from livestock waste, Frontiers in Sustainable Food Systems, 10.3389/fsufs.2024.1434977, 8, (2024).
- Jorge H. ULLOA, Fedor LURIE, Fabricio R. SANTIAGO, Sergio GIANESINI, Lourdes REINA, Jinsong WANG, Ravul JINDAL, Wassila TAHA, Mamuka BOKUCHAVA, Armando MANSILHA, Systematic literature review and expert meeting report on health-related quality of life in chronic venous disease, International Angiology, 10.23736/S0392-9590.23.05108-8, 42, 6, (2024).
- Zoubida Tazi Mezalek, Toni Feodor, Larisa Chernukha, Zhong Chen, Ana Rueda, Ignacio Escotto Sánchez, Alejandro José González Ochoa, Joanna Chirol, Vanessa Blanc-Guillemaud, Caroline Lohier-Durel, Jorge Hernando Ulloa, VEIN STEP: A Prospective, Observational, International Study to Assess Effectiveness of Conservative Treatments in Chronic Venous Disease, Advances in Therapy, 10.1007/s12325-023-02643-6, 40, 11, (5016-5036), (2023).