Palbociclib versus abemaciclib in HR+/HER2- advanced breast cancer: an indirect comparison of patient-reported end points
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To assess the relative impact of palbociclib plus fulvestrant (PAL + FUL) and abemaciclib plus fulvestrant (ABEM + FUL) on patient-reported outcomes in patients with hormone receptor-positive, HER2-negative (HR+/HER2-) advanced breast cancer. Patients & methods: Anchored matching-adjusted indirect comparisons were conducted using individual patient data from PALOMA-3 (PAL + FUL) and summary-level data from MONARCH-2 (ABEM + FUL). Outcomes included the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 items (EORTC QLQ-C30) and its breast cancer-specific module (QLQ-BR23). Results: Significantly different changes from baseline favoring PAL + FUL compared with ABEM + FUL were observed in global quality of life (6.95 [95% CI: 2.19–11.71]; p = 0.004) and several functional/symptom scales, including emotional functioning, nausea/vomiting, appetite loss, diarrhea and systemic therapy side effects. Conclusion: PAL + FUL was associated with more favorable patient-reported outcomes than ABEM + FUL in patients with HR+/HER2- advanced breast cancer.
Palbociclib was the first CDK4/6 inhibitor approved by the US FDA in combination with letrozole for the treatment of women with hormone receptor positive (HR+), HER2-negative (HER2-) advanced breast cancer (ABC) in February 2015 [1]. In February 2016, the indication was extended to include combination therapy with palbociclib and fulvestrant (PAL + FUL) [1]. The approval of PAL + FUL was supported by findings from the Phase III PALOMA-3 trial, which showed significantly improved progression-free survival (PFS) compared with placebo in combination with fulvestrant (PBO + FUL) [2].
In March 2017, ribociclib was approved in combination with an aromatase inhibitor (AI), and the indication was extended to include combination therapy with fulvestrant in July 2018 [3,4]. Abemaciclib became the third CDK4/6 inhibitor to receive FDA approval in combination with fulvestrant (ABEM + FUL) in September 2017 [5] based on findings of improved PFS compared with PBO + FUL in the Phase III MONARCH-2 trial [6].
Although improvements in PFS and overall survival (OS) compared with PBO + FUL have been demonstrated with each of the available CDK4/6 inhibitors [2,4,6,7], these therapies have not been directly compared in head-to-head randomized controlled trials (RCTs) in patients with HR+/HER2- ABC. In the absence of data from RCTs, indirect treatment comparisons (ITCs) can be conducted to control for differences in patient populations between studies, allowing for meaningful comparisons of treatment effects. When individual patient data (IPD) are available for one study and summary-level data are available for a comparator study, matching-adjusted indirect comparison (MAIC) methods can be used to reduce differences between trials by matching and adjusting the IPD to the summary-level data of the comparator trial. If a common comparator is available, an anchored MAIC can be conducted to further adjust for differences in prognostic factors across trials by anchoring through the control arm.
A previous ITC showed similar relative PFS between palbociclib, ribociclib and abemaciclib [8]. A recently published anchored MAIC compared OS between palbociclib and each of the other CDK4/6 inhibitors using IPD from PALOMA-3 and summary-level data from MONALEESA-3 and MONARCH-2 to account for differences between trials [9]. The results of this study showed that relative improvements in OS are similar between CDK4/6 inhibitors despite considerably different median survival times reported across studies, highlighting the importance of adjusting for cross-trial differences when comparing treatment effects.
In addition to improving survival outcomes, maintaining health-related quality of life (HRQoL) is a core goal of therapy for patients with HR+/HER2- ABC [10–13]. However, HRQoL may be impacted by treatment-related toxicity and disease burden [11,13–15]; therefore, patient-reported outcomes (PROs) that assess HRQoL are critical to inform treatment decisions [16]. Safety profiles of the CDK4/6 inhibitors used in the treatment of patients with HR+/HER2- ABC are well characterized. Hematologic adverse events (primarily neutropenia) are common with all of these therapies; however, abemaciclib is also associated with a high risk of diarrhea [6,13,17,18], and ribociclib requires regular monitoring for potential prolongation of the QT interval [3,18].
To the best of our knowledge, no ITCs have been conducted to compare HRQoL outcomes between any CDK4/6 inhibitors in this patient population. The objective of the present study was to conduct an anchored MAIC analysis by leveraging IPD from the PALOMA-3 study and summary-level data from the MONARCH-2 study to compare PRO scores between PAL + FUL and ABEM + FUL among patients with HR+/HER2- ABC. Comparisons with ribociclib were not conducted in this study due to limited reporting of change from baseline (CFB) in scores for several PRO scales of interest in publications for MONALEESA-3 [19].
Patients & methods
Patient-reported outcome assessment
PROs used in the present analysis included the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 items (EORTC QLQ-C30) and its breast cancer-specific module (EORTC QLQ-BR23). The QLQ-C30 is a 15-scale, 30-item questionnaire that includes one global health status (GHS)/QoL scale, five functional scales (physical, role, emotional, cognitive and social functioning), and nine symptom scales (fatigue, nausea/vomiting, pain, dyspnea, insomnia, appetite loss, constipation, diarrhea and financial difficulties). The QLQ-BR23 is a 23-item breast cancer-specific questionnaire that includes four functional scales (body image, sexual functioning, sexual enjoyment and future perspectives) and four symptom scales (systemic therapy side effects, breast symptoms, arm symptoms and upset by hair loss) [11]. Data for the sexual enjoyment and upset by hair loss scales were not available from MONARCH-2; therefore, these scales were not included in the present analysis. For global QoL and functional scales, higher scores indicate better QoL/functioning than lower scores. For symptom scales, higher scores indicate increased symptom severity [11].
Anchored matching-adjusted indirect comparisons
PALOMA-3 compared PAL + FUL to PBO + FUL and MONARCH-2 compared ABEM + FUL to PBO + FUL in the treatment of women with HR+/HER2- ABC. IPD were available for the PALOMA-3 trial and published summary-level data were available for the MONARCH-2 trial. Since PBO + FUL is a common comparator between the two trials and there are known cross-trial differences [9], an anchored MAIC was deemed an appropriate method for comparing results of PROs for PAL + FUL and ABEM + FUL.
The methods used for the MAICs were consistent with those presented by the National Institute for Health and Care Excellence (NICE) [20]. Patients in the PALOMA-3 [2] IPD were matched with those in MONARCH-2 [6] based on inclusion/exclusion criteria to ensure that patients who would not have been eligible for MONARCH-2 did not contribute to effect estimates. To match the trial populations, patients who had prior chemotherapy for metastatic breast cancer (MBC) or who had ≥2 prior lines of endocrine therapy (ET) for MBC were removed from the PALOMA-3 IPD. After matching, the IPD were adjusted (i.e., reweighed) to align with the means and variances of baseline characteristics reported in the MONARCH-2 trial; this step estimates how PAL + FUL would have performed in the MONARCH-2 population. Patient-level weights were computed via a propensity score model, where patients from PALOMA-3 were weighted using the inverse odds of being in PALOMA-3 compared with MONARCH-2 based on baseline characteristics. An overview of the matching and adjusting steps used in this analysis is presented in Figure 1.
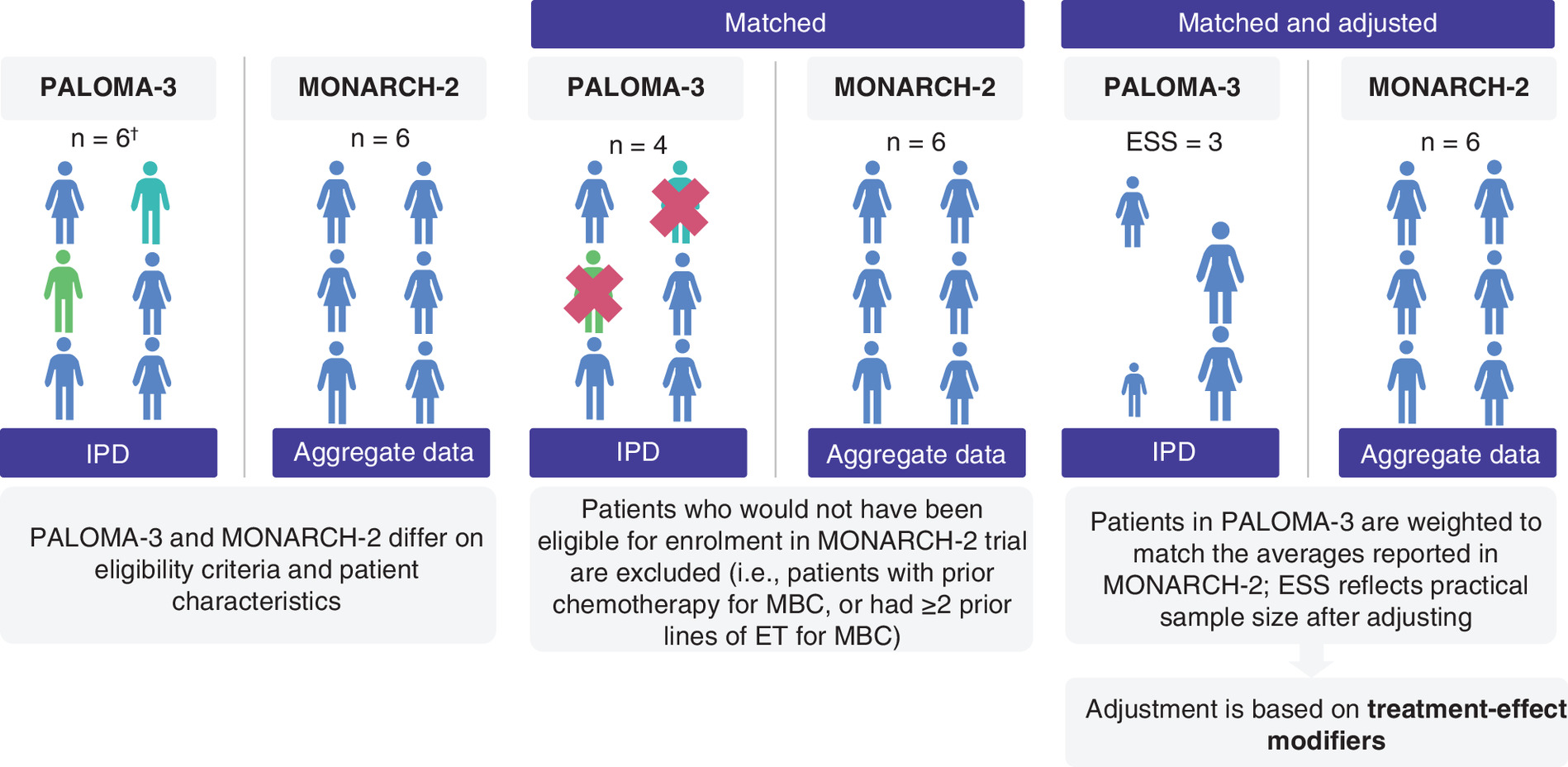
Figure 1. Overview of matching & adjusting steps in a matching-adjusted indirect treatment comparison.
†Note that the n’s presented in this figure are for illustrative purposes only.
ESS: Effective sample size; ET: Endocrine therapy; IPD: Individual patient data; MBC: Metastatic breast cancer.
The MAICs performed for the comparison of PAL + FUL and ABEM + FUL were anchored with PBO + FUL as the common comparator; therefore, differences in prognostic characteristics across the PALOMA-3 and MONARCH-2 trials were controlled for when comparing relative treatment effects. Anchored MAICs only rely on the assumption that trials are similar with respect to treatment-effect modifiers; therefore, the MAICs performed in this analysis exclusively relied on balancing baseline characteristics that may alter the treatment effects between PALOMA-3 and MONARCH-2.
Treatment-effect modifiers
Although matching based on inclusion/exclusion criteria results in similar patients being included between trials, baseline characteristics may still vary between study populations. For example, a smaller proportion of patients had no previous lines of therapy for MBC in the PALOMA-3 PRO set (25%) than in MONARCH-2 (61%). Table 1 presents the differences in baseline characteristics for the PALOMA-3 and MONARCH-2 populations used in the MAICs. Since anchored MAICs are not affected by known or unknown prognostic variables, the IPD for PALOMA-3 only had to be adjusted to align with the means and variances of the treatment-effect modifiers from MONARCH-2.
| Characteristic | Category | PALOMA-3† (n = 501), n (%) | MONARCH-2 (n = 669), n (%) | SMD |
|---|---|---|---|---|
| Age‡, years, estimated mean (SD) | – | 58.0 (11.5) | 58.8 (10.4) | 0.073 |
| Race | White Asian Other | 369 (74) 103 (21) 27 (5) | 373 (59) 214 (34) 42 (7) | 0.322 0.294 0.084 |
| Region | North America Europe Asia | 231 (46) 160 (32) 110 (22) | 178 (27) 279 (42) 212 (31) | 0.403 0.208 0.205 |
| ECOG PS | 1 0 | 189 (38) 311 (62) | 264 (40) 400 (60) | 0.041 |
| Metastatic site | Visceral Bone only Visceral and bone only Other | 297 (59) 113 (23) 3 (1) 88 (17) | 373 (56) 180 (27) 0 (0) 113 (17) | 0.061 0.092 0.142 0 |
| Organs involved (n) | 1 2 ≥3 | 166 (33) 145 (29) 190 (38) | 263 (40) 200 (30) 203 (30) | 0.146 0.022 0.169 |
| Prior AI | Yes No | 432 (86) 69 (14) | 465 (70) 204 (30) | 0.394 |
| Prior chemotherapy | Neoadjuvant or adjuvant Metastatic None | 212 (42) 161 (32) 128 (26) | 401 (60) 0 (0) 268 (40) | 0.366 0.970 0.301 |
| Sensitivity to prior ET | Yes No | 396 (79) 105 (21) | 488 (74)§ 172 (26)¶ | 0.118 |
| Previous lines of therapy for MBC | 0 1 ≥2 | 124 (25) 194 (39) 183 (36) | 396 (61) 256 (39) 0 (0) | 0.781 0 1.061 |
| Menopausal status | Pre-/perimenopausal Postmenopausal | 102 (20) 399 (80) | 114 (17) 551 (83) | 0.077 |
Percentages reflect the total number of patients with available data for the specified variable.
†
Values for PALOMA-3 were calculated using IPD.
‡
The estimated mean and SD for each variable in MONARCH-2 was calculated by first calculating the sample mean and SD for the treatment and placebo arms, and then using those values to calculate the pooled mean and SD.
§
Secondary ET resistance used to identify sensitivity to prior ET.
¶
Primary ET resistance used to identify no sensitivity to prior ET.
AI: Aromatase inhibitor; ECOG PS: Eastern Cooperative Oncology Group performance status; ET: Endocrine therapy; IPD: Individual patient data; MBC: Metastatic breast cancer; SD: Standard deviation; SMD: Standardized mean difference.
The impact of treatment-effect modifiers on the results of MAICs can vary. In general, treatment-effect modifiers that greatly impact treatment effects and significantly differ between trials have a large impact on MAIC results, whereas those that only slightly impact treatment effects and are similar between trials have a lesser impact on MAIC results. Including unnecessary covariates can increase variance of the estimated treatment effects but omitting an important covariate can result in bias. Therefore, it was necessary to leverage both clinical and statistical expertise to select covariates to balance while reweighing the PALOMA-3 IPD.
A previous MAIC was conducted using IPD from PALOMA-3 and published summary-level data from MONARCH-2 to investigate OS [9]. The MAIC selected treatment-effect modifiers that were deemed important based on assessment of the literature and clinical opinion, extent of treatment modifications, differences in characteristics between trials and impact on effective sample size (ESS) [9]. The same rank-ordered treatment-effect modifiers were used in the present analysis; however, measurable disease was not included, as this variable had a strong negative linear correlation with metastatic site.
Accounting for the longitudinal structure of the data
The IPD from the PALOMA-3 trial were longitudinal (i.e., outcomes for patients were measured at several time points). However, the anchored MAICs did not consider the longitudinal structure of the data; therefore, patient-level weights were extracted from the MAIC. The weights were then incorporated into a repeated measures mixed-effect model with a binary treatment indicator (i.e., PAL + FUL vs ABEM + FUL) for each outcome (i.e., each QLQ-C30 or QLQ-BR23 subscale). The covariates of the repeated measures mixed-effect model were treatment, treatment by time and baseline scores for the outcome of interest. This approach used a restricted maximum likelihood method with an unstructured covariance matrix [11]. Outputs from the repeated measures mixed-effect model were then used in conjunction with the summary-level data from MONARCH-2 in least-square (LS) mean calculations to determine the mean estimate and find the mean difference (MD) between PAL + FUL and ABEM + FUL and the related 95% CI.
A histogram of the patient level weights extracted from the MAICs of PAL + FUL to ABEM + FUL is shown in Supplementary Figure 1.
Traditional ITC methods
Similar to MAICs, traditional (Bucher) ITCs compare the relative effects between two treatments anchored through a common comparator. However unlike MAICs, traditional ITC methods only require summary-level data from both trials in the comparison [20,22]. In this study, the MAICs represented the primary analysis and the traditional ITCs were only conducted to validate the results of the MAICs.
Adjusting for multiplicity
Due to the large number of outcomes being considered in the comparison of PAL + FUL to ABEM + FUL, there was a risk of Type I error. To adjust for multiplicity, the Bonferroni correction was applied to the 15 scales of the QLQ-C30 and the six scales of the QLQ-BR23, separately.
Results
Matching the PALOMA-3 IPD to the MONARCH-2 population
In total, 501 patients were included in the PALOMA-3 PRO IPD. After removing any patients with missing values for baseline characteristics of interest, 495 patients remained. After matching, a total of 270 patients remained. In terms of reasons for removal from the PALOMA-3 IPD, 43 patients had chemotherapy in the metastatic setting, 65 patients had ≥2 previous lines of therapy for MBC and 117 patients met both exclusion criteria (Supplementary Figure 2). Out of the 270 patients remaining in the PALOMA-3 IPD, 180 patients received PAL + FUL and 90 patients received PBO + FUL.
Global QoL & functional scales (QLQ-C30)
Results of the MAICs for global QoL (MD: 6.95 [95% CI: 2.19–11.71]; p = 0.004; Figure 2) and emotional functioning (MD: 5.40 [95% CI: 0.78–10.02]; p = 0.022) showed statistically significant differences in favor of PAL + FUL compared with ABEM + FUL.
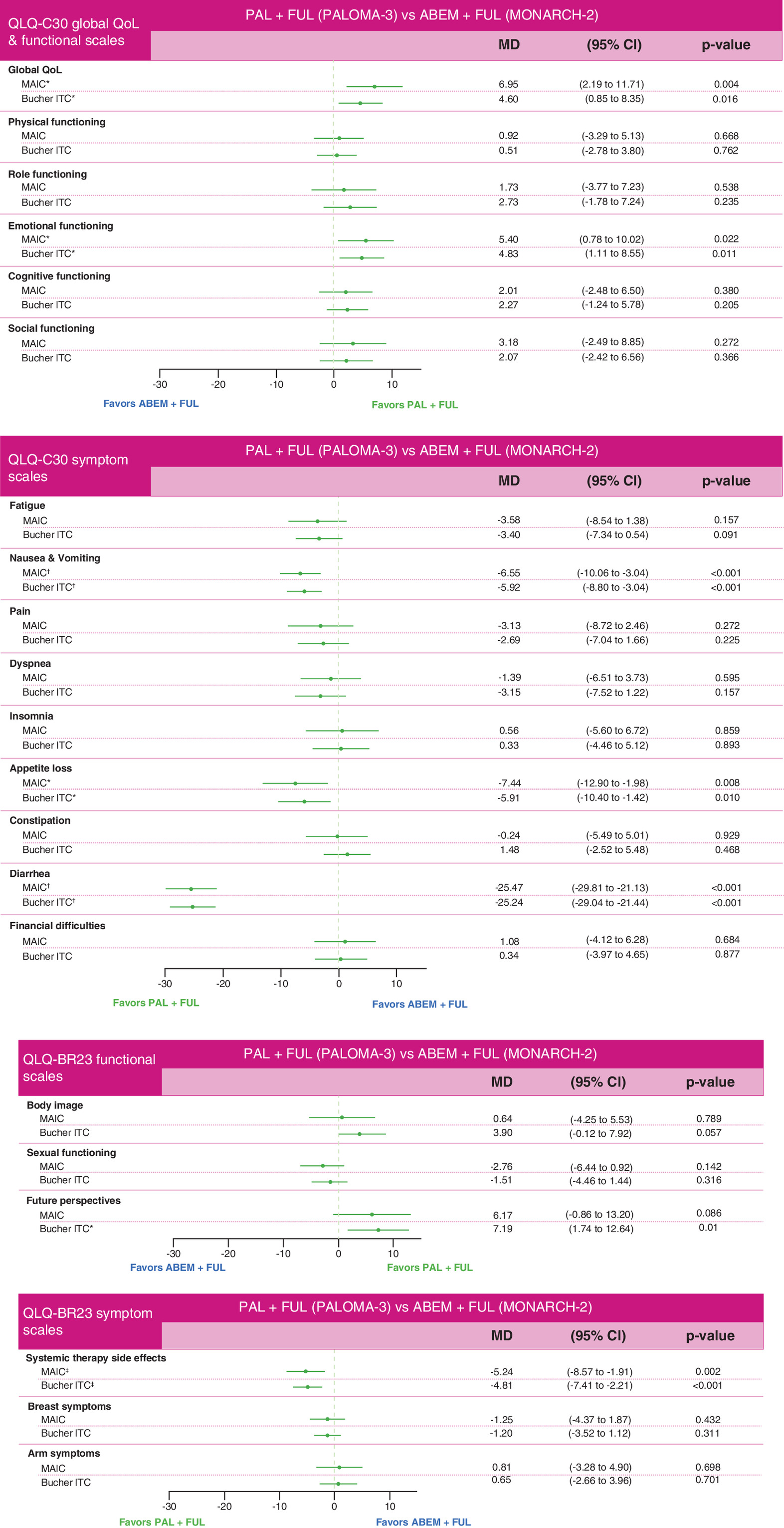
Figure 2. Matching-adjusted indirect comparison results and traditional indirect treatment comparison results comparing palbociclib + fulvestrant to abemaciclib + fulvestrant for the EORTC QLQ-C30 and QLQ-BR23 global quality of life, functional, and symptom scales.
For global QoL and functional scales, MD >0 indicates direction of improved outcome for PAL+FUL. For symptom scales, MD >0 indicates direction of improved outcome for ABEM+FUL. The following treatment-effect modifiers are adjusted for in the MAIC of PAL+FUL to ABEM+FUL: race, previous lines of therapy for MBC, number of organs involved, region, metastatic site, age, prior chemotherapy, sensitivity to prior ET, baseline ECOG PS, prior AI, and menopausal status.
*p < 0.05.
†Statistical significance according to the Bonferonni correction for the EORTC QLQ-C30 scales (p < 0.003).
‡Statistical significance according to the Bonferonni correction for the EORTC QLQ-BR23 scales (p < 0.008).
ABEM: Abemaciclib; AI: Aromatase inhibitor; ECOG PS: Eastern Cooperative Oncology Group performance status; EORTC QLQ-BR23: European Organisation for Research and Treatment of Cancer Breast Cancer Module; EORTC QLQ-C30: European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire-Core 30 items. ET: Endocrine therapy; FUL: Fulvestrant; MAIC: Matching-adjusted indirect comparison; MBC: Metastatic breast cancer; MD: Mean difference; PAL: Palbociclib; QoL: Quality of life.
The MAIC results for the remaining functional scales of the QLQ-C30 were numerically in favor of PAL + FUL compared with ABEM + FUL (Figure 2), including physical functioning (MD: 0.92 [95% CI: -3.29 to 5.13]; p = 0.668), role functioning (MD: 1.73 [95% CI: -3.77 to 7.23]; p = 0.538), cognitive functioning (MD: 2.01 [95% CI: -2.48 to 6.50]; p = 0.380) and social functioning (MD: 3.18 [95% CI: -2.49 to 8.85] p = 0.272); however, none of these results reached statistical significance.
Traditional ITC results based on summary-level data only for the QLQ-C30 global QoL and functional scales were consistent with the MAIC results (Figure 2). A visualization of the LS mean CFB for PAL + FUL (unmatched and unadjusted, matched and adjusted) and ABEM + FUL (summary-level data) for the QLQ-C30 global QoL and functional scales are shown in Figure 3.
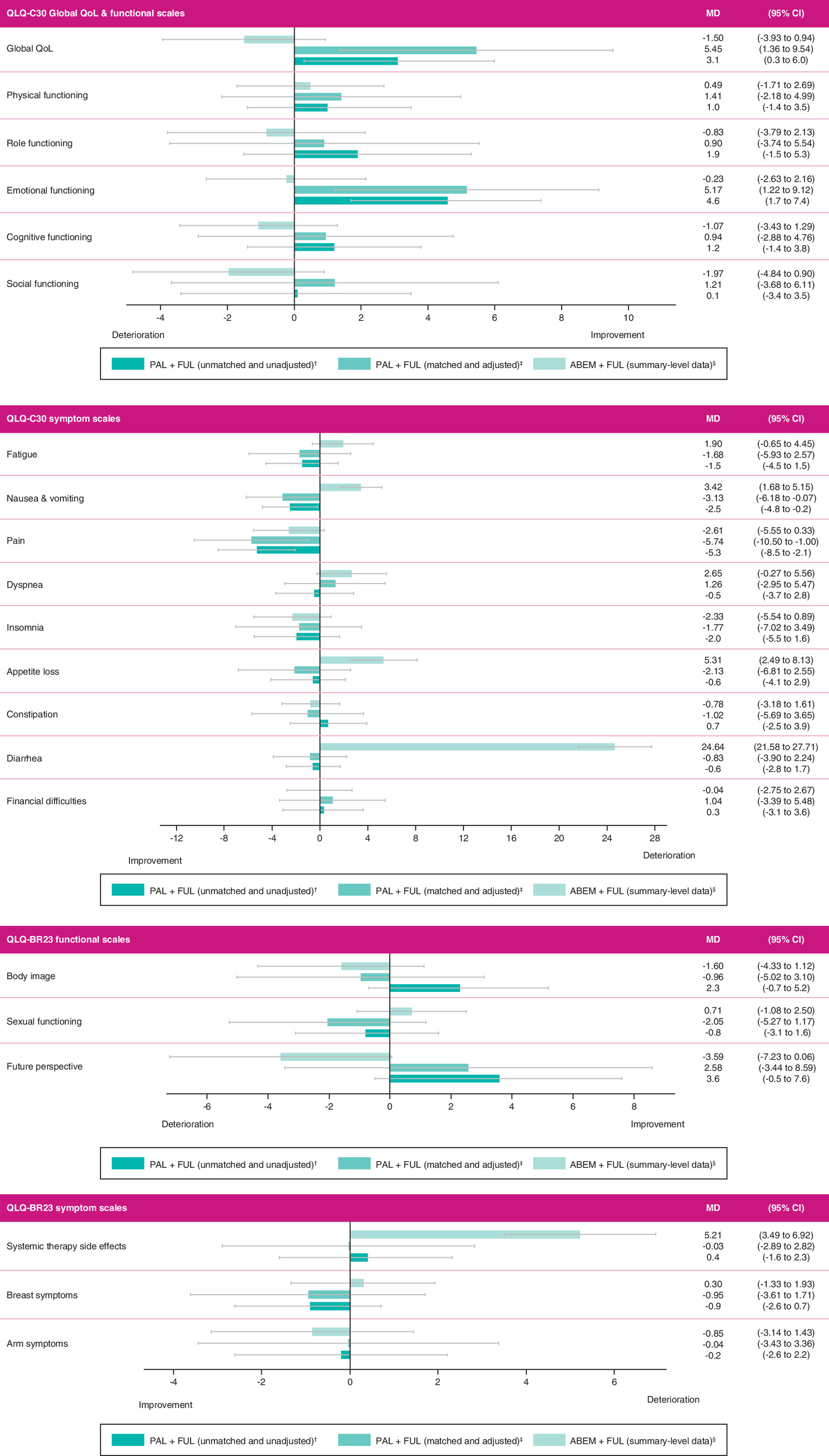
Figure 3. Overall least squares means change from baseline for the EORTC QLQ-C30 and QLQ-BR23 global quality of life, functional, and symptom scales.
For global QoL and functional scales, MD >0 indicate improved QoL/functioning. For symptom scales, MD >0 indicate increased symptom severity. The grey bars represent the CIs for each mean difference.
†LS mean CFB from the unmatched and unadjusted population in PALOMA-3 for PAL+FUL vs PBO+FUL.
‡LS mean CFB from the matched and adjusted population in PALOMA-3 for PAL+FUL vs PBO+FUL.
§LS mean CFB from MONARCH-2 for ABEM+FUL vs PBO+FUL.
ABEM: Abemaciclib; CFB: Change from baseline; EORTC QLQ-BR23: European Organisation for Research and Treatment of Cancer Breast Cancer Module; EORTC QLQ-C30: European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire-Core 30 items; FUL: Fulvestrant; LS: Least-squares; MD: Mean difference; PAL: Palbociclib; PBO: Placebo; QoL: Quality of life.
Symptom scales (QLQ-C30)
Results of the MAICs for the QLQ-C30 symptom scales showed statistically significant differences in favor of PAL + FUL compared with ABEM + FUL for nausea/vomiting (MD: -6.55 [95% CI: -10.06 to -3.04]; p < 0.001; Figure 2), appetite loss (MD: -7.44 [95% CI: -12.90 to -1.98]; p = 0.008) and diarrhea (MD: -25.47 [95% CI: -29.81 to -21.13]; p < 0.001).
No statistically significant differences were found for the other QLQ-C30 symptom scales. The MAIC results for fatigue (MD: -3.58 [95% CI: -8.54 to 1.38]; p = 0.157; Figure 2), pain (MD: -3.13 [95% CI: -8.72 to 2.46]; p = 0.272), dyspnea (MD: -1.39 [95% CI: -6.51 to 3.73]; p = 0.595) and constipation (MD: -0.24 [95% CI: -5.49 to 5.01]; p = 0.929) were numerically in favor of PAL + FUL, whereas MAIC results for insomnia (MD: 0.56 [95% CI: -5.60 to 6.72]; p = 0.859) and financial difficulties (MD: 1.08 [95% CI: -4.12 to 6.28]; p = 0.684) were numerically in favor of ABEM + FUL.
Traditional ITC results based on summary-level data only for the QLQ-C30 symptom scales were generally consistent with the MAIC results, with the exception of constipation (Figure 2). However, neither the traditional ITC nor the MAIC results for constipation were statistically significant. Figure 3 shows LS mean CFB for PAL + FUL (unmatched and unadjusted, matched and adjusted) and ABEM + FUL (summary-level data) for the QLQ-C30 symptom scales.
Functional scales (QLQ-BR23)
None of the MAIC results for the QLQ-BR23 functional scales were statistically significant. The MAIC results for body image (MD: 0.64 [95% CI: -4.25 to 5.53]; p = 0.798; Figure 2) and future perspective (MD: 6.17 [95% CI: -0.86 to 13.20]; p = 0.086) were numerically in favor of PAL + FUL compared with ABEM + FUL; and MAIC results for sexual functioning (MD: -2.76 [95% CI: -6.44 to 0.92]; p = 0.142) were numerically in favor of ABEM + FUL compared with PAL + FUL.
The results of traditional ITCs based on summary-level data from both trials for the QLQ-BR23 functional scales were generally consistent with the MAIC results (Figure 2). The LS mean CFB for PAL + FUL (unmatched and unadjusted, matched and adjusted) and ABEM + FUL (summary-level data) for the QLQ-BR23 functional scales are shown in Figure 3.
Symptom scales (QLQ-BR23)
Results of the MAIC for systemic therapy side effects (MD: -5.24 [95% CI: -8.57 to -1.91]; p = 0.002; Figure 2) were statistically significant in favor of PAL + FUL compared with ABEM + FUL.
The MAIC results for the other QLQ-BR23 symptom scales did not show statistically significant differences between treatment arms. The results for breast symptoms (MD: -1.25 [95% CI: -4.37 to 1.87]; p = 0.432; Figure 2) were numerically in favor of PAL + FUL, and results for arm symptoms (MD: 0.81 [95% CI: -3.28 to 4.90]; p = 0.698) were numerically in favor of ABEM + FUL.
Traditional ITC results based on summary-level data only for the QLQ-BR23 symptom scales were consistent with the MAIC results (Figure 2). A visualization of the LS mean CFB for PAL + FUL (unmatched and unadjusted, matched and adjusted) and ABEM + FUL (summary-level data) for the QLQ-BR23 symptom scales is shown in Figure 3.
Discussion
After matching study populations based on inclusion/exclusion criteria and adjusting for differences in baseline characteristics between trials, several statistically significant differences in favor of PAL + FUL compared with ABEM + FUL were observed. Other results were not statistically significant, although most were numerically in favor of PAL + FUL compared with ABEM + FUL. No HRQoL/PRO end points were shown to favor ABEM + FUL compared with PAL + FUL. Overall, these results indicate that PAL + FUL may better improve or maintain HRQoL among patients with HR+/HER2- ABC than ABEM + FUL.
To the best of our knowledge, no RCTs have been conducted to directly compare the safety and efficacy of PAL + FUL and ABEM + FUL, as well as their relative impact on HRQoL. Recent ITCs have shown similar relative PFS [8] and OS [9] between PAL + FUL and ABEM + FUL; however, no comparative evidence is available for the relative impact of these therapies on PROs, despite maintenance of HRQoL being an important goal of therapy for patients with HR+/HER2- ABC [10–13]. The present study is the first to use MAIC methods to compare the effect of PAL + FUL and ABEM + FUL on PROs assessing HRQoL. Individually reported results from the PALOMA-3 trial showed significant differences in favor of PAL + FUL compared with PBO + FUL in EORTC QLQ-C30 global QoL scores and CFB in pain and nausea/vomiting [11]. However, a significantly greater deterioration from baseline in QLQ-BR23 ‘upset by hair loss’ score was observed with PAL + FUL than with PBO + FUL. No other significant differences between groups were observed. In contrast, in MONARCH-2, the results were similar between groups for most functional and symptom scores, although there were significant differences in favor of PBO + FUL compared with ABEM + FUL in appetite loss, nausea/vomiting, diarrhea and systemic therapy side effects [13]. The results of the present study are consistent with the individually reported trial results of HRQoL for PAL + FUL and ABEM + FUL and inform our understanding of the relative impact of these agents on patient-reported experiences.
The EORTC QLQ-C30 is among the most commonly used measures of HRQoL in oncology studies; however, there are challenges with clinical interpretation of results using this tool [23]. The use of minimally important differences (MIDs) can help enhance clinical interpretation of HRQoL outcomes [23,24]. Cocks et al. have published evidence-based guidelines that provide MIDs to aid in interpretation of results using the QLQ-C30 [23]. Applying these guidelines to the MAIC results in the present study indicates that statistically significant and clinically relevant differences in favor of PAL + FUL compared with ABEM + FUL were observed for global QoL, nausea/vomiting, appetite loss and diarrhea. According to the guidelines, all other differences between groups were of trivial clinical significance. The statistically significant and clinically meaningful difference between groups for global QoL may be particularly important, as this measure represents the totality of a patient’s experience; this supports greater improvements in QoL with PAL + FUL than with ABEM + FUL. Guidelines providing MIDs for the QLQ-BR23 scales were not identified; therefore, we are unable to comment on the clinical significance of the findings for these outcomes.
The finding of a statistically significant, clinically relevant difference in diarrhea scores between PAL + FUL and ABEM + FUL is noteworthy. Diarrhea is a common adverse event of treatment with abemaciclib [6,13,17], and a recent indirect analysis of RCTs found that palbociclib was associated with a reduced risk of diarrhea compared with abemaciclib (relative risk: 0.13 [95% CI: 0.02–0.92]; p = 0.04). Risk of diarrhea is also an important consideration in terms of therapy choice among patients and their physicians. A recent study used a discrete choice experiment and a best-worst scaling exercise to understand preferences regarding attributes of treatment-related toxicity among patients with MBC and oncologists in the USA [18]. Avoiding the risk of diarrhea was rated as one of the most important attributes for choice of CDK4/6 inhibitor among both patients and physicians. Consequently, the profile of palbociclib was deemed preferable to that of abemaciclib (both in combination with an AI). Furthermore, in the present study, both statistically significant and clinically meaningful differences in favor of PAL + FUL were also found in nausea/vomiting and appetite loss scores, suggesting that patients are more likely to perceive improvements across multiple gastrointestinal symptoms with PAL + FUL than with ABEM + FUL.
In addition to impacting treatment decisions among patients and clinicians, HRQoL data are widely considered in value assessment frameworks and in evaluations by health technology assessment (HTA) agencies. In the USA, value assessment frameworks inform how resources should be allocated to achieve the best clinical health and HRQoL outcomes while also providing a tool to assist payers with coverage, formulary and reimbursement decisions [25]. Notably, these frameworks consistently emphasize the importance of the patient perspective and HRQoL data. For example, the Institute for Clinical and Economic Review value assessment framework considers HRQoL as a critical health outcome in clinical effectiveness evaluations and gives greater weight to changes that impact quantity or quality of life than to intermediate clinical outcomes [26]. In terms of clinical organizations, the American Society of Clinical Oncology Value Framework includes bonus points in their net health benefit calculations if a product improves HRQoL or symptom palliation; however, the American Society of Clinical Oncology also recognizes that deficient consideration is currently given to PROs because of the lack of consistent reporting of such outcomes in clinical trials [27]. Similarly, although the European Society for Medical Oncology Magnitude of Clinical Benefit Scale considers credit adjustments based on results of PROs for HRQoL in clinical trials, the most recent version highlights the need for further consultation with patients and patient advocacy organizations regarding the validity of HRQoL credit allocation or deduction [28].
In Canada, the pan-Canadian Oncology Drug Review includes HRQoL as part of the effectiveness assessment in their deliberative framework [29]. However, in a study that assessed the frequency at which HRQoL data were included in submissions to the the pan-Canadian Oncology Drug Review between 2015 and 2018, 56% of submissions did not have original data on HRQoL [30]. Similar findings were reported in a study that evaluated data from six European HTA agencies from England/Wales, France, Germany, the Netherlands, Poland and Scotland [31]. Although all agencies considered HRQoL a relevant end point, only 54% of publicly available relative effectiveness assessments for anticancer drugs approved by the EMA between 2011 and 2013 included original data for HRQoL [31]. Of the reports that included HRQoL data, the results of these outcomes impacted the recommendation in 74% of relative effectiveness assessments, including in 100% of the assessments in France, Germany and the Netherlands [31]. Furthermore, HRQoL data had a negative impact on only 7% of recommendations across all jurisdictions, highlighting the limited potential downside of including such outcomes from the HTA perspective [31]. These findings highlight that, despite the recognized importance of HRQoL to healthcare decision makers, comparative evidence for such outcomes is often lacking. The present study helps to address this need in the HR+/HER2- ABC setting. Overall, PROs are important tools for value-based care, and capturing the patient perspective with such outcomes may ultimately improve the patient experience, increase the length of time on treatment and improve survival [32–35].
There are several strengths of the present study. This is the first analysis to use MAIC methods to compare HRQoL outcomes between treatments in patients with breast cancer, leveraging IPD from PALOMA-3 to reduce differences in patient populations between trials by adjusting for treatment-effect modifiers and anchoring through a common comparator. The comparison was largely made possible because of the fully disaggregated reporting of CFB in EORTC QLQ-C30 and QLQ-BR23 scales in the MONARCH-2 publication [13]. In addition, the methods used in the analysis were consistent with guidance issued by NICE [20] and leveraged rank-ordered clinically relevant treatment-effect modifiers from a previous MAIC [9]. Furthermore, the MAIC results for the EORTC QLQ-C30 were compared with MIDs from evidence-based guidelines [23] to aid in clinical interpretation of the findings. Overall, these MAICs allowed for a robust comparison of HRQoL outcomes between PAL + FUL and ABEM + FUL.
This study has some limitations that should be considered. MAIC methodology assumes that all treatment-effect modifiers are balanced between trials, and anchored analyses preserve randomization and are not affected by known or unknown prognostic variables [20,36]; however, differences in characteristics included in the analysis were limited by summary-level data reported in the publications for MONARCH-2. Furthermore, the analysis was unable to account for differences in the management of adverse events (and associated tolerability of the drugs based on adherence, dose modification/titration and discontinuation data) that may have impacted the comparison because access to IPD was only available for the PALOMA-3 trial. As the primary outcomes of this analysis included 21 scales across the EORTC QLQ-C30 and the QLQ-BR23, there was a risk of Type I error due to multiplicity. To account for this, the Bonferroni correction was applied to the 15 scales of the QLQ-C30 and the six scales of the QLQ-BR23 separately. The analysis did not include the upset by hair loss or sexual enjoyment QLQ-BR23 scales as data for these outcomes were not available from MONARCH-2. Since the patient population of PALOMA-3 was matched and adjusted to that of MONARCH-2, ESS was reduced. Furthermore, given the longitudinal aspect of the data, an accurate ESS could not be obtained for the MAICs. However, since several statistically significant differences were found even after the Bonferroni correction was applied and given the concordance between the traditional ITC and MAIC results, decreased and/or inaccurate ESS likely did not impact the conclusions.
Conclusion
This is the first published MAIC analysis of HRQoL outcomes among patients with breast cancer. The results of this study suggest that PAL + FUL is associated with favorable outcomes on several cancer-specific PRO end points compared with ABEM + FUL in terms of both statistical and clinical significance. Therefore, PAL + FUL may be the preferred treatment choice to maintain HRQoL and improve patient experience compared with ABEM + FUL. These findings may help to inform shared treatment decisions for patients with HR+/HER2- ABC and clinicians, and system-level decision-making among payers and HTA agencies.
•
Palbociclib (PAL) and abemaciclib (ABEM) are CDK4/6 inhibitors approved, in combination with fulvestrant (FUL), for the treatment of hormone receptor-positive, HER2-negative advanced breast cancer (HR+/HER2- ABC).
•
No head-to-head randomized controlled trials have been conducted to directly compare PAL + FUL and ABEM + FUL.
•
In addition to improving survival outcomes, maintaining health-related quality of life (HRQoL) while on treatment is an important consideration for patients with HR+/HER2- ABC; however, comparative data for CDK4/6 inhibitors are unavailable.
•
The present study used anchored matching-adjusted indirect comparison (MAIC) methods leveraging individual patient data from the PALOMA-3 study and summary-level data from the MONARCH-2 study to compare patient-reported outcomes between PAL + FUL and ABEM + FUL among patients with HR+/HER2- ABC.
•
The MAIC results showed that PAL + FUL was associated with significant improvements compared with ABEM + FUL across several functional and symptom subscales, including global QoL, emotional functioning, nausea/vomiting, appetite loss, diarrhea and systemic therapy side effects.
•
The MAIC results for the EORTC QLQ-C30 were compared with minimally important differences from evidence-based guidelines to aid in clinical interpretation of the findings.
•
Clinically meaningful differences in favor of PAL + FUL compared with ABEM + FUL were found for global QoL, nausea/vomiting, appetite loss and diarrhea.
•
The results of this study suggest that PAL + FUL is associated with favorable outcomes on several cancer-specific patient-reported outcome end points compared with ABEM + FUL in terms of both statistical and clinical significance.
•
To the best of our knowledge, this is the first published MAIC analysis of HRQoL outcomes among patients with breast cancer and these findings may help to inform shared treatment decisions for patients with HR+/HER2- ABC, clinicians and payer/health technology assessment agencies.
Author contributions
E Law, A Haltner, R McTavish and C Cameron were responsible for the study conception and design. R Gavanji, S Walsh, E Law, A Haltner, R McTavish and C Cameron were responsible for the acquisition, analysis and interpretation of data. S Walsh was responsible for the drafting the manuscript, and all the authors were responsible for critically revising/reviewing the manuscript and for providing final approval. All the authors agree to be held accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part are appropriately investigated and resolved.
Financial & competing interests disclosure
This study was funded by Pfizer, Inc. E Law is an employee of and stockholder in Pfizer, Inc. C Cameron is an employee and shareholder of EVERSANA™. R Gavanji, S Walsh, A Haltner and R McTavish are employees of EVERSANA who were paid consultants to Pfizer in connection with the development of this manuscript. EVERSANA receives consultancy fees from major pharmaceutical and medical device companies, including Pfizer. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Medical writing and editorial support was provided by Ari L Mendell of EVERSANA and was funded by Pfizer.
Data-sharing statement
Upon request, and subject to review, Pfizer will provide the data that support the findings of this study. Subject to certain criteria, conditions and exceptions, Pfizer may also provide access to the related individual anonymized participant data. See https://www.pfizer.com/science/clinical-trials/trial-data-and-results for more information.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
United States Food & Drug Administration. Drugs@FDA: FDA-approved drugs - palbociclib (IBRANCE) (2019). http://www.accessdata.fda.gov/scripts/cder/daf/index.cfm?event=overview.process&var ApplNo=207103
2.
Turner NC, Ro J, André F et al. Palbociclib in hormone-receptor-positive advanced breast cancer. N. Engl. J. Med. 373(3), 209–219 (2015).
• Presents results for the primary outcome (progression-free survival) and baseline patient characteristics from the PALOMA-3 trial.
3.
United States Food & Drug Administration. Drugs@FDA: FDA-approved drugs - ribociclib (KISQALI) (2020). http://www.accessdata.fda.gov/scripts/cder/daf/index.cfm?event=overview.process&varApplNo=209092
4.
Slamon DJ, Neven P, Chia S et al. Phase III randomized study of ribociclib and fulvestrant in hormone receptor-positive, human epidermal growth factor receptor 2-negative advanced breast cancer: MONALEESA-3. J. Clin. Oncol. 36(24), 2465–2472 (2018).
5.
United States Food & Drug Administration. Drugs@FDA: FDA-approved drugs - abemaciclib (VERZENIO) (2020). http://www.accessdata.fda.gov/scripts/cder/daf/index.cfm?event=overview.process&varApplNo=208716
6.
Sledge GW Jr, Toi M, Neven P et al. MONARCH 2: abemaciclib in combination with fulvestrant in women With HR+/HER2- advanced breast cancer who had progressed while receiving endocrine therapy. J. Clin. Oncol. 35(25), 2875–2884 (2017).
• Presents results for the primary outcome (progression-free survival) and baseline patient characteristics from the MONARCH 2 trial.
7.
Cristofanilli M, Rugo HS, Im S-A et al. Overall survival (OS) with palbociclib (PAL) + fulvestrant (FUL) in women with hormone receptor–positive (HR+), human epidermal growth factor receptor 2–negative (HER2–) advanced breast cancer (ABC): Updated analyses from PALOMA-3. J. Clin. Oncol. 39(Suppl. 15), 1000–1000 (2021).
8.
Petrelli F, Ghidini A, Pedersini R et al. Comparative efficacy of palbociclib, ribociclib and abemaciclib for ER+ metastatic breast cancer: an adjusted indirect analysis of randomized controlled trials. Breast Cancer Res. Treat. 174(3), 597–604 (2019).
9.
Rugo HS, Haltner A, Zhan L et al. Matching-adjusted indirect comparison of palbociclib versus ribociclib and abemaciclib in hormone receptor-positive/HER2-negative advanced breast cancer. J. Comp. Eff. Res. 10(6), 457–467 (2021).
•• Presents results of matching-adjusted indirect comparisons assessing relative overall survival with palbociclib compared with abemaciclib and ribociclib.
10.
De Mello Ramirez Medina J, De Araujo Trugilho I, Mendes GNB et al. Advanced clinical stage at diagnosis of breast cancer is associated with poorer health-related quality of life: a cross-sectional study. Eur. J. Breast Health 15(1), 26–31 (2019).
11.
Harbeck N, Iyer S, Turner N et al. Quality of life with palbociclib plus fulvestrant in previously treated hormone receptor-positive, HER2-negative metastatic breast cancer: patient-reported outcomes from the PALOMA-3 trial. Ann. Oncol. 27(6), 1047–1054 (2016).
•• Presents results for patient-reported outcomes from the PALOMA-3 trial.
12.
Marandino L, La Salvia A, Sonetto C et al. Deficiencies in health-related quality-of-life assessment and reporting: a systematic review of oncology randomized Phase III trials published between 2012 and 2016. Ann. Oncol. 29(12), 2288–2295 (2018).
13.
Kaufman PA, Toi M, Neven P et al. Health-related quality of life in MONARCH 2: abemaciclib plus fulvestrant in hormone receptor-positive, HER2-negative advanced breast cancer after endocrine therapy. Oncologist 25(2), e243–e251 (2020).
•• Presents results for patient-reported outcomes from the MONARCH 2 trial.
14.
Miles D, Von Minckwitz G, Seidman AD. Combination versus sequential single-agent therapy in metastatic breast cancer. Oncologist 7(Suppl. 6), 13–19 (2002).
15.
Dear RF, Mcgeechan K, Jenkins MC, Barratt A, Tattersall MH, Wilcken N. Combination versus sequential single agent chemotherapy for metastatic breast cancer. Cochrane Database Syst. Rev. 2013(12), Cd008792 (2013).
16.
Cardoso F, Costa A, Senkus E et al. 3rd ESO-ESMO International Consensus guidelines for advanced breast cancer (ABC 3). Ann. Oncol. 28(1), 16–33 (2017).
17.
Rugo HS, Huober J, García-Sáenz JA et al. Management of abemaciclib-associated adverse events in patients with hormone receptor-positive, human epidermal growth factor receptor 2-negative advanced breast cancer: safety analysis of MONARCH 2 and MONARCH 3. Oncologist 26(1), e53–e65 (2021).
18.
Maculaitis MC, Liu X, Will O et al. Oncologist and patient preferences for attributes of CDK4/6 inhibitor regimens for the treatment of advanced/metastatic HR Positive/HER2 negative breast cancer: discrete choice experiment and best-worst scaling. Patient Prefer. Adherence 14, 2201–2214 (2020).
• Describes a discrete choice experiment/best-worst scaling study of patient and oncologist preferences for properties of CDK4/6is used to treat HR+/HER2- advanced breast cancer.
19.
Fasching PA, Beck JT, Chan A et al. Ribociclib plus fulvestrant for advanced breast cancer: health-related quality-of-life analyses from the MONALEESA-3 study. Breast 54, 148–154 (2020).
20.
NICE. NICE DSU Technical Support Document 18: methods for population-adjusted indirect comparisons in submission to NICE. (2021). http://nicedsu.org.uk/wp-content/uploads/2018/08/Population-adjustment-TSD-FINAL-ref-rerun.pdf
21.
Sledge GW Jr, Toi M, Neven P et al. The effect of abemaciclib plus fulvestrant on overall survival in hormone receptor-positive, ERBB2-negative breast cancer that progressed on endocrine therapy-MONARCH 2: a randomized clinical trial. JAMA Oncol. 6(1), 116–124 (2020).
22.
Bucher HC, Guyatt GH, Griffith LE, Walter SD. The results of direct and indirect treatment comparisons in meta-analysis of randomized controlled trials. J. Clin. Epidemiol. 50(6), 683–691 (1997).
23.
Cocks K, King MT, Velikova G et al. Evidence-based guidelines for interpreting change scores for the European Organisation for the Research and Treatment of Cancer Quality of Life Questionnaire Core 30. Eur. J. Cancer 48(11), 1713–1721 (2012).
24.
Musoro JZ, Coens C, Fiteni F et al. Minimally important differences for interpreting EORTC QLQ-C30 scores in patients with advanced breast cancer. JNCI Cancer Spectr. 3(3), 1–7 (2019).
25.
National Pharmaceutical Council. Guiding practices for patient-centered value assessment (2021). https://www.npcnow.org/sites/default/files/2021-04/npc-guiding-practices-for-patient-centered-value-assessment.pdf
26.
Institute for Clinical and Economic Review (ICER). 2020–2023 value assessment framework (2020). https://34eyj51jerf417itp82ufdoe-wpengine.netdna-ssl.com/wp-content/uploads/2021/03/ICER_2020_2023_VAF_013120-4-2.pdf
27.
Schnipper LE, Davidson NE, Wollins DS et al. Updating the American Society of Clinical Oncology Value Framework: revisions and reflections in response to comments received. J. Clin. Oncol. 34(24), 2925–2934 (2016).
28.
Cherny NI, Dafni U, Bogaerts J et al. ESMO-magnitude of clinical benefit scale version 1.1. Ann. Oncol. 28(10), 2340–2366 (2017).
29.
Canadian Agency for Drugs and Technologies in Health: pan-Canadian Oncology Drug Review (pCODR) expert review committee deliberative framework (2016). https://www.cadth.ca/sites/default/files/pcodr/The%20pCODR%20Expert%20Review%20Committee%20%28pERC%29/pcodr_perc_deliberative_frame.pdf
30.
Raymakers AJN, Regier DA, Peacock SJ. Health-related quality of life in oncology drug reimbursement submissions in Canada: a review of submissions to the pan-Canadian Oncology Drug Review. Cancer 126(1), 148–155 (2020).
31.
Kleijnen S, Leonardo Alves T, Meijboom K et al. The impact of quality-of-life data in relative effectiveness assessments of new anti-cancer drugs in European countries. Qual. Life Res. 26(9), 2479–2488 (2017).
32.
Kotronoulas G, Kearney N, Maguire R et al. What is the value of the routine use of patient-reported outcome measures toward improvement of patient outcomes, processes of care, and health service outcomes in cancer care? A systematic review of controlled trials. J. Clin. Oncol. 32(14), 1480–1501 (2014).
33.
Velikova G, Booth L, Smith AB et al. Measuring quality of life in routine oncology practice improves communication and patient well-being: a randomized controlled trial. J. Clin. Oncol. 22(4), 714–724 (2004).
34.
Basch E, Deal AM, Dueck AC et al. Overall survival results of a trial assessing patient-reported outcomes for symptom monitoring during routine cancer treatment. JAMA 318(2), 197–198 (2017).
35.
Denis F, Basch E, Septans AL et al. Two-year survival comparing web-based symptom monitoring vs routine surveillance following treatment for lung cancer. JAMA 321(3), 306–307 (2019).
36.
Song F, Loke YK, Walsh T, Glenny A-M, Eastwood AJ, Altman DG. Methodological problems in the use of indirect comparisons for evaluating healthcare interventions: survey of published systematic reviews. BMJ 338, 1–7 (2009).
Information & Authors
Information
Published In
Pages: 109 - 120
PubMed: 34751591
Copyright
© 2021 Chris Cameron. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 17 September 2021
Accepted: 21 October 2021
Published online: 9 November 2021
Keywords:
Topics
Authors
Funding Information
Pfizer, Inc.
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Palbociclib versus abemaciclib in HR+/HER2- advanced breast cancer: an indirect comparison of patient-reported end points. (2021) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2021-0221
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Diana Lüftner, Maggie Banys-Paluchowski, Andreas D. Hartkopf, Manuel Hörner, Wolfgang Janni, Dagmar Langanke, Volkmar Müller, Andreas Schneeweiss, Marcus Schmidt, Marc Thill, Michael Untch, Achim Wöckel, Lukas Höllrich, Julia Kreuzeder, Almuth Marx, Julia Meinzinger, Hanna Regus-Leidig, Christian Roos, Hien Wohlgemuth, Stephanie Sussmann, Peter A. Fasching, Indirect Treatment Comparison between Ribociclib Combined with Non-Steroidal Aromatase Inhibitors and Ovarian Function Suppression vs. Tamoxifen in Premenopausal Women with Early Breast Cancer, Senologie - Zeitschrift für Mammadiagnostik und -therapie, 10.1055/a-2784-6305, 23, 01, (63-74), (2026).
- Benlong Yang, Zhengkui Sun, Quchang Ouyang, Zhongsheng Tong, Shu Wang, Hongyuan Li, Zhaofeng Niu, Yiding Chen, Lin-xiaoxi Ma, Haoqi Wang, Mu Tang, Zheyu Hu, Xueqiang Gao, Xu Wang, Fei Xie, Qiao Cheng, Yong Shen, Cuizhi Geng, Haibo Wang, Jiong Wu, Safety and quality of life of CDK4/6 inhibitors therapy for hormone receptor-positive, human epidermal growth factor receptor 2-negative advanced breast cancer: a multicenter cross-sectional survey in China, BMC Cancer, 10.1186/s12885-025-14223-8, 25, 1, (2025).
- Cecília Menezes Farinasso, Vinícius Lins Ferreira, Flávia Cordeiro Medeiros, Aline Pereira da Rocha, Patrícia do Carmo Silva Parreira, Layssa Andrade Oliveira, Lays Pires Marra, Rosa Camila Lucchetta, Haliton Alves de Oliveira, Matching-Adjusted Indirect Comparison Studies in Oncology: A Scoping Review Focused on Reporting Quality, Value in Health Regional Issues, 10.1016/j.vhri.2025.101088, 47, (101088), (2025).
- Diana Lüftner, Maggie Banys-Paluchowski, Andreas D. Hartkopf, Manuel Hörner, Wolfgang Janni, Dagmar Langanke, Volkmar Müller, Andreas Schneeweiss, Marcus Schmidt, Marc Thill, Michael Untch, Achim Wöckel, Lukas Höllrich, Julia Kreuzeder, Almuth Marx, Julia Meinzinger, Hanna Regus-Leidig, Christian Roos, Hien Wohlgemuth, Stephanie Sussmann, Peter A. Fasching, Indirect Treatment Comparison between Ribociclib Combined with Non-Steroidal Aromatase Inhibitors and Ovarian Function Suppression vs. Tamoxifen in Premenopausal Women with Early Breast Cancer, Geburtshilfe und Frauenheilkunde, 10.1055/a-2561-6640, 85, 06, (599-610), (2025).
- Shogo Nakamoto, Tadahiko Shien, Takayuki Iwamoto, Shinichiro Kubo, Mari Yamamoto, Tetsumasa Yamashita, Chihiro Kuwahara, Masahiko Ikeda, Absolute lymphocyte count and neutrophil-to-lymphocyte ratio as predictors of CDK 4/6 inhibitor efficacy in advanced breast cancer, Scientific Reports, 10.1038/s41598-024-60101-x, 14, 1, (2024).
- Fatima Cardoso, Julie Rihani, Victoria Harmer, Nadia Harbeck, Ana Casas, Hope S Rugo, Peter A Fasching, Adam Moore, Joanna de Courcy, Purnima Pathak, Sina Haftchenary, Dawn Aubel, Eva Schumacher-Wulf, Quality of Life and Treatment-Related Side Effects in Patients With HR+/HER2− Advanced Breast Cancer: Findings From a Multicountry Survey, The Oncologist, 10.1093/oncolo/oyad207, 28, 10, (856-865), (2023).
- Ernest H Law, Chris Cameron, Letter in Reply: indirect comparison of quality-of-life scores between patients with advanced breast cancer receiving palbociclib and abemaciclib in combination with fulvestrant, Journal of Comparative Effectiveness Research, 10.57264/cer-2023-0009, 12, 6, (2023).
- Vittorio Gebbia, Maria Rosaria Valerio, Federica Martorana, Maria Vita Sanò, Paolo Vigneri, Letter to the Editor: statistics and clinical perception of patients’ reported outcomes for palbociclib and abemaciclib: a sliding doors story, Journal of Comparative Effectiveness Research, 10.57264/cer-2022-0212, 12, 6, (2023).
- Erilaine de F Corpes, Romel J V Yanez, Denise M da Silva, Kauane M Leite, Milena C T Martins, Milena M Vieira, Cristina P R S dos Santos, Ana F C Fernandes, Régia C M B Castro, Health-related quality of life of women with breast cancer being treated with hormone therapy: A scoping review, Journal of Oncology Pharmacy Practice, 10.1177/10781552231168071, 29, 4, (944-955), (2023).
- Laura Dormer, Journal of Comparative Effectiveness Research: 2022 year in review, Journal of Comparative Effectiveness Research, 10.57264/cer-2023-0026, 12, 4, (2023).