Comparative effectiveness of catheter ablation devices in the treatment of atrial fibrillation: a network meta-analysis
Publication: Journal of Comparative Effectiveness Research
Abstract
Atrial fibrillation (AF) ablation is most commonly performed using radiofrequency (RF) and cryoballoon (CB) catheters. Ablation Index is a novel lesion-quality marker associated with improved outcomes in RF ablation. Due to lack of direct comparative evidence between the latest generations of technologies, there is uncertainty regarding the best treatment option. Aim: To conduct a network meta-analysis to evaluate the comparative effectiveness of RF with Ablation Index to other catheter ablation devices in the treatment of AF. Methods: Searches for randomized and nonrandomized prospective comparative studies of ablation catheters were conducted in multiple databases. The outcome of interest was 12-month freedom from atrial arrhythmias after a single ablation procedure. Studies were grouped as high-, low- and unclear-quality based on study design and balanced baseline patient characteristics. Bayesian hierarchical network meta-analysis was conducted and results presented as relative risk ratios with 95% credible intervals (CrIs). Results: 12 studies evaluating five different catheter ablation devices were included. Radiofrequency ablation with Ablation Index was associated with statistically significantly greater probability of 12-month freedom from atrial arrhythmias than Arctic Front (relative risk: 1.77; 95% CrI: 1.21–2.87), Arctic Front Advance™ (1.41; 1.06–2.47), THERMOCOOL™ (1.34; 1.17–1.48) and THERMOCOOL SMARTTOUCH™ (1.09; 1–1.3). Results were robust in multiple sensitivity analyses. Conclusion: Radiofrequency catheter with Ablation Index is superior to currently available options for 12-month freedom from atrial arrhythmias after AF ablation. This study provides decision-makers with robust, pooled, comparative evidence of the latest ablation technologies.
Catheter ablation is a minimally invasive option for the treatment of atrial fibrillation (AF) [1–3]. Ablation is routinely performed using radiofrequency (RF) and cryoballoon (CB) catheters, with RF catheters being the most widely used technology [1,4]. Radiofrequency catheters have evolved since their introduction to include contact force (CF) technology, which provides real-time feedback on the contact between the catheter tip and cardiac tissue during ablation. Ablation with CF catheters has improved freedom from atrial arrhythmia compared with non-CF catheters and has reduced complications, procedure time and fluoroscopy time [5–12].
More recently, use of a novel lesion-quality marker, Ablation Index (also referred to as VISITAG SURPOINT™), with CF catheters has been associated with improved outcomes of RF ablation. A recent meta-analysis reported a significant 57% reduction in the odds of acute pulmonary vein (PV) reconnection and significant 65% reduction in recurrence of atrial arrhythmias 12 months after an Ablation Index-guided procedure compared with use of CF catheters alone [13].
For CB catheters, three successive generations have followed the first-generation CB. The second-generation CB included a redesigned balloon that allowed for more uniform cooling across the surface, which led to improved effectiveness and safety when compared with first-generation CB [14,15]. Third and fourth generations of the CB catheter have been developed to include shorter tips to help improve assessment of time to PV isolation. Emerging evidence on these devices has shown similar effectiveness and safety as the second-generation device [16,17].
Direct comparative data between the advanced catheter ablation technologies are lacking, making assessments of the different ablation technologies challenging. Randomized trials have compared the effectiveness and safety of RF and CB catheters [18–23]; however, of these published studies, few have included advanced catheter ablation technologies [18,22]. To date, no studies comparing CF catheters with Ablation Index to CB have been published.
Although several meta-analyses have been published that compare RF and CB technologies, it is difficult to understand the comparative effectiveness of specific devices because analyses often combine catheters with different technologies (e.g., combine first- and second-generation devices and different CF technologies), include a broad range of patients (i.e., combine paroxysmal and persistent AF, drug-naive and drug-refractory), and do not have a clear follow-up period (i.e., combine studies that report outcomes at various follow-up periods). Network meta-analysis (NMA) enables the indirect comparison of treatments that have not been directly compared in clinical trials [24]. Network meta-analyses are robust and well established for the use of guideline development and decision-making at national (e.g., NICE, Canadian Agency for Drugs and Technologies in Health [CADTH]) and international (e.g., WHO) levels. The objective of this study was to conduct an NMA that considers the totality of prospective comparative evidence to evaluate the pooled clinical effectiveness of the THERMOCOOL SMARTTOUCH™ Catheter with Ablation Index compared with other available catheter ablation devices, including second-generation CB, in the treatment of AF.
Methods
A Bayesian statistical model was used to conduct the NMAs. The study protocol was registered on PROSPERO (registration number CRD42018093077, available online at: www.crd.york.ac.uk/PROSPERO/display_record.php?ID=CRD42018093077). Reporting of the analysis follows the Preferred Reporting Items of Systematic Reviews and Meta-analyses (PRISMA) Extension Statement for Reporting of Systematic Reviews Incorporating Network Meta-analyses of Health Care Interventions (Supplementary Material 1) [25].
Search strategy
A comprehensive search strategy was developed to search PubMed to identify relevant studies (Supplementary Material 2). Searches of relevant grey literature and key study bibliographies were also conducted. Only English-language articles published from 2008 onward were reviewed.
Eligibility criteria & study selection
Studies that included adult patients (≥18 years old) with paroxysmal AF (PAF) refractory and/or intolerant to antiarrhythmic drugs undergoing first-time catheter ablation were considered if they compared the use of one catheter ablation device of interest to another (Supplementary Material 3). The primary interventions of interest included the THERMOCOOL SMARTTOUCH SF Catheter with Ablation Index. Relevant comparators included THERMOCOOL SMARTTOUCH Catheter/THERMOCOOL SMARTTOUCH SF Catheter, THERMOCOOL™ Catheter/THERMOCOOL SF Catheter, Arctic Front Cryoballoon, Arctic Front Advance™ Cryoballoon, Arctic Front Advance-Short Tip and Arctic Front Advance Pro™. Studies must have reported on the outcome of interest: 12-month freedom from atrial arrhythmias, defined as AF, atrial tachycardia (AT) or atrial flutter (AFL) after a single procedure, excluding events that occurred during a 3-month blanking period, and without touch-up using a focal catheter. Randomized controlled trials (RCTs) and prospective observational studies were considered. Studies were excluded if they were retrospective or single arm in design or did not report freedom from or recurrence of atrial arrhythmias disaggregated by device. Study screening was conducted by a single reviewer K Eaton (KE) and validated by a second reviewer L Patel (LP). Conflicts were resolved by consensus through discussion or a third party D Grima (DG).
Data extraction
Data extracted included: study design, sample size, patient baseline characteristics, interventions and key outcomes. Some data were extracted by digitizing data (DigitizeIt version 2.2.2 digitizing software) for outcomes at 12 months, when available. No data imputation was required, and no attempt was made to contact study authors for clarification of results or to obtain missing data. Data were extracted by a single reviewer (KE) and verified for accuracy by a second reviewer K Dawkins (KD). Conflicts were resolved by consensus or a third party (LP).
Quality assessment & study hierarchy
Risk of bias of randomized and nonrandomized studies was assessed separately using two independent tools. For studies in which patients were randomized to device-level interventions, the Cochrane Risk of Bias Tool for Randomized Controlled Trials was used [26]. For nonrandomized studies or randomized studies that did not randomize for device-level comparisons, the Cochrane Risk of Bias in Nonrandomized Studies of Interventions (ROBINS-I) was used [27]. One reviewer (KE) scored studies according to the respective tool’s grading scheme, and a second reviewer A Dineen (AD) confirmed scores; discrepancies were resolved by consensus or a third party (LP).
A single comprehensive classification scheme was developed to assess the overall hierarchy of studies, including studies for which subgroup data were extracted. The classification scheme assessed study design, adjustment for baseline differences between treatment groups, and balance in baseline characteristics between treatment groups, where balance was identified as the absence of significant differences. Studies were grouped as high-, low- or unclear-quality according to the following definitions: high-quality studies were RCTs or prospective observational studies that reported balanced baseline characteristics or adjusted to balance baseline characteristics between treatment groups; low-quality studies were those that reported unbalanced, unadjusted baseline characteristics; and unclear-quality studies were those that did not report baseline characteristics (i.e., for a treatment or patient subgroup).
Data synthesis & analysis
Devices were represented as individual nodes within the network to best reflect their variability in design, functionality and use in practice. Network meta-analyses were performed using methods as outlined in NICE Decision Support Unit Technical Support Series [28] with extensions to account for evidence from multiple study designs as described by Efthimiou et al. [29]. Specifically, analyses were conducted using a three-level Bayesian hierarchical model to incorporate both randomized and nonrandomized evidence (additional detail in Supplementary Material 4). The Bayesian hierarchical model provides estimates of treatment effect in each of the three subnetworks (i.e., high-, unclear- and low-quality), as well as an overall average across designs. Estimates for the primary analysis were taken from the high-quality subnetwork, which allows them to primarily be based on high-quality evidence while being influenced (i.e., borrowing strength) from the unclear- and low-quality subnetworks. Furthermore, low- and unclear-quality studies were weighted 50% compared with high-quality studies. The Bayesian hierarchical NMA was conducted using R Statistical Software version 3.5.3 and JAGS version 4.3.0. All analyses were conducted using a random-effects model with vague priors. Outcomes were modeled on the log-odds scale and converted to relative risk (RR) ratios with 95% credible intervals (CrIs) using the model-estimated average baseline event rate as described by NICE [28]. Absolute rates and 95% CrIs were calculated by adding the estimated treatment effect for each technology to the pooled reference treatment response estimated by the NMA.
Risk ratios <1 or >1 favor one of the catheter ablation devices over the other. CrIs can be interpreted as the Bayesian equivalent to confidence intervals, with CrIs excluding 1 indicating the Bayesian-equivalent of statistical significance. An advantage of Bayesian analyses is that they allow for calculation of the probability that a treatment is the best, second best – among others. These ranks are summarized using medians and their uncertainty is captured by the surface under the cumulative ranking curve area (SUCRA) statistic [30]. SUCRA is expressed as a percentage such that a treatment with a SUCRA of 100% is the best treatment with zero uncertainty. Available study and patient characteristics were assessed for similarity and to investigate the potential effect of heterogeneity. Inconsistency models for hierarchical NMAs have not been developed and tested, therefore an inconsistency analysis was not performed. In addition, NMA results were qualitatively compared with those from direct comparisons generated from traditional meta-analyses using R Statistical Software version 3.6.1. Detailed methods are included in Supplementary Material 4.
Secondary & sensitivity analyses
A secondary analysis was conducted to assess the overall average estimate from the hierarchical NMA, as this estimate would be relevant for decision-makers interested in the average effect across the populations included in each design.
Sensitivity analyses were conducted to assess the robustness of the primary analysis. To assess the influence of the evidence weighting (i.e., low- and unclear-quality studies) on results, sensitivity analyses where low- and unclear-quality studies were not downweighted and where low- and unclear-quality studies were downweighted 80% compared with high-quality studies were conducted. To assess the impact of variance in the subnetworks for low- and unclear-quality studies on primary analysis results, a sensitivity analysis using equivalent standard deviations across all three levels of the Bayesian hierarchical NMA was conducted, where the between-study heterogeneity was assumed to be equivalent in high-, unclear- and low-quality studies.
Results
Literature search & study characteristics
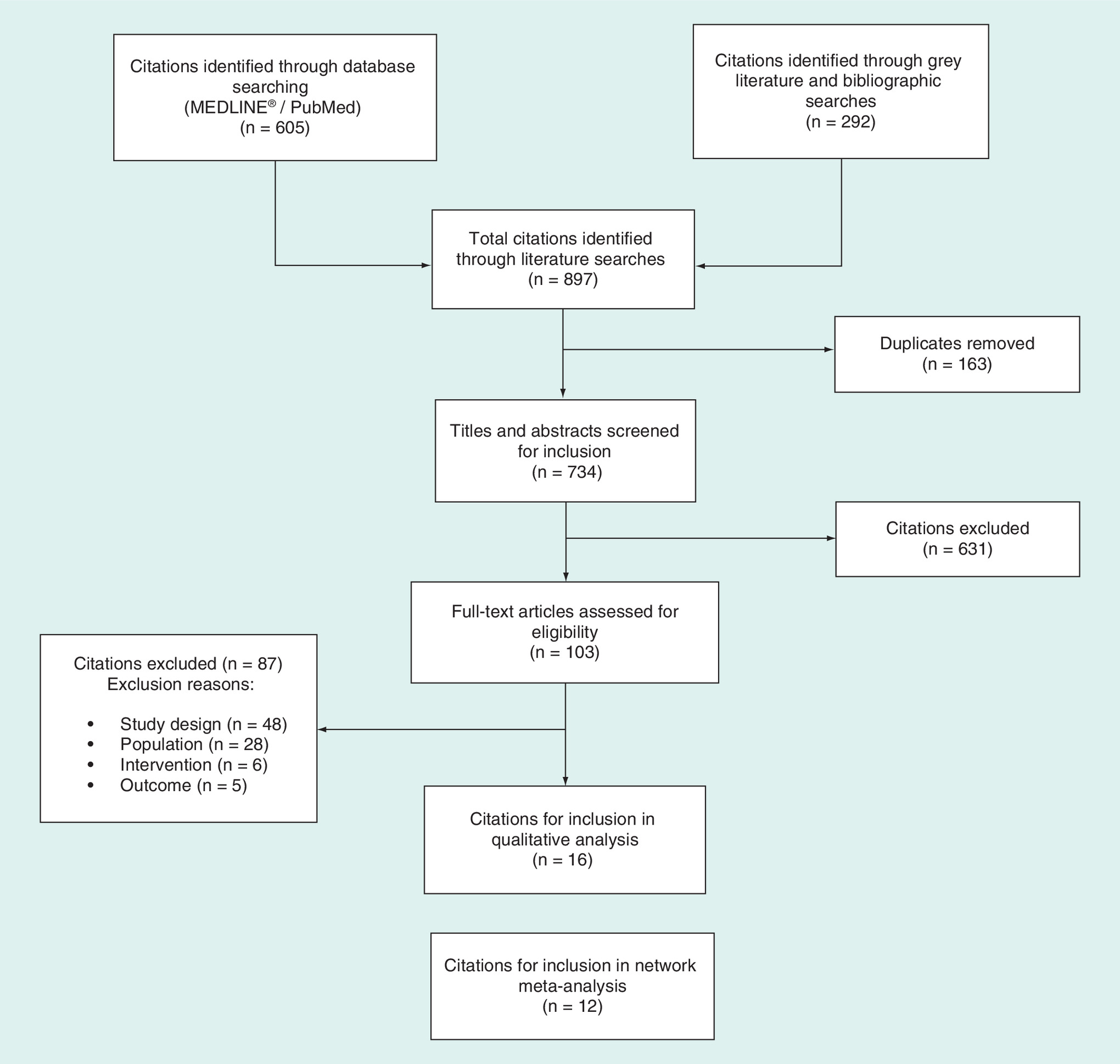
The literature search identified 897 potentially relevant studies, of which 631 were subsequently excluded during the title and abstract review process (Figure 1). Of the 103 eligible full-text articles assessed, 16 were identified for potential inclusion in the quantitative analysis [5–7,15,18,21–23,31–38]. Overall, 12 studies met the criteria for inclusion in the quantitative analyses [5–7,15,18,21,23,32–34,37,38].
Catheters examined in the 12 selected studies included: THERMOCOOL, THERMOCOOL SMARTTOUCH SF, THERMOCOOL SMARTTOUCH SF with Ablation Index, Arctic Front and Arctic Front Advance (Table 1). Males comprised 43–88% of patients, and mean patient age ranged from 56 to 65 years. Presence of paroxysmal AF was 48–100%, and mean duration of AF ranged from 45.6 to 56.4 months. Left atrial diameter, left ventricular ejection fraction and CHA2DS2-VASc score were similar across studies. History of coronary artery disease, stroke or transient ischemic attack, hypertension and diabetes varied broadly across studies. Two studies did not report patient baseline characteristics disaggregated by subgroup [18,34]. The definition of effectiveness used in included studies varied, including the type of recurrent arrhythmia measured (e.g., AF, AT and AFL) (Supplementary Material 5).
| Study (year) | Treatment device | N | Age (years) | PAF (%) | Males (%) | Duration of AF (months) | LAD (mm) | LVEF (%) | CHA2DS2-VASc score | CHADS2 score | BMI | Stroke or TIA (%) | HT (%) | Diabetes (%) | Ref. |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Andrade et al. (2014) | THERMOCOOL™ | 50 | 58.6 | 100 | 86 | – | 39.2 | 59.9† | – | – | – | – | – | – | [5] |
| THERMOCOOL SMARTTOUCH™ | 25 | 58.8 | 100 | 76 | – | 32.4 | 63.3† | – | – | – | – | – | – | ||
| Davtyan et al. (2018) | Arctic Front Advance™ | 44 | 57.6 | 100 | 48.9 | – | 41 | – | 1.3 | – | 29.9 | 11.1 | 77.8 | 4.4 | [23] |
| THERMOCOOL SMARTTOUCH | 45 | 55.6 | 100 | 43.2 | – | 40 | – | 1.3 | – | 29.8 | 9.1 | 77.3 | 13.6 | ||
| Dhillon et al. (2018) | THERMOCOOL SMARTTOUCH | 50 | 59.9 | 100 | 48† | Median: 42 | 38.7 | – | 1.68 | – | – | – | 34 | 6 | [33] |
| THERMOCOOL SMARTTOUCH + AI | 50 | 60.1 | 100 | 70† | Median: 24 | 37.6 | – | 1.3 | – | – | – | 38 | 12 | ||
| Hussein et al. (2017) | THERMOCOOL SMARTTOUCH | 89 | 62 | 48 | 73 | – | 41 | – | – | 0.65 | 29 | 9 | 30 | 9 | [34] |
| THERMOCOOL SMARTTOUCH + AI | 89 | 62 | 50 | 75 | – | 42 | – | – | 0.65 | 29 | 3 | 34 | 15 | ||
| Itoh et al. (2016)‡ | THERMOCOOL | 50 | 61 | 100 | 62 | – | 38 | 65 | 1.8 | 1.0 | – | 8 | 52 | 16 | [7] |
| THERMOCOOL SMARTTOUCH | 50 | 65 | 100 | 60 | – | 37 | 65 | 2.3 | 1.3 | – | 14 | 64 | 10 | ||
| Jourda et al. (2015)‡ | Arctic Front Advance | 75 | 59.9 | 100 | 73.3 | 45.6 | – | 64.4 | 1.3 | 0.7 | 28.2† | 4 | 34.7 | 8.0 | [32] |
| THERMOCOOL SMARTTOUCH | 75 | 62.5 | 100 | 76.0 | 52.8 | – | 65.5 | 1.5 | 0.9 | 26.5† | 10.7 | 48.0 | 4.0 | ||
| Koektuerk et al. (2017) | Arctic Front | 21 | 62 | 100 | 71.4 | – | – | 58.7 | 1.8 | – | – | – | 52.4 | 9.5 | [15] |
| Arctic Front Advance | 93 | 61 | 100 | 60.2 | – | – | 59.9 | 1.8 | – | – | – | 58.1 | 5.4 | ||
| Kuck et al. (2016) | Radiofrequency | 376 | 60.1 | 100 | 63 | 56.4 | 40.6 | – | 1.8 | – | 27.8 | – | 58.8 | 5.9 | [18] |
| Cryoballoon | 374 | 59.9 | 100 | 59 | 55.2 | 40.8 | – | 1.9 | – | 28.0 | – | 57.5 | 9.9 | ||
| Marijon et al. (2014) | THERMOCOOL | 30 | 61.0 | 100 | 73.3 | – | – | 65.4 | 0.58 | – | – | – | – | – | [6] |
| THERMOCOOL SMARTTOUCH | 30 | 59.9 | 100 | 70.0 | – | – | 64.7 | 0.86 | – | – | – | – | – | ||
| Perez-Castellano et al. (2014) | THERMOCOOL | 25 | Median: 56 | 100 | 88 | – | Median: 42 | – | – | – | – | – | 32 | 8 | [21] |
| Arctic Front | 25 | Median: 58 | 100 | 68 | – | Median: 42 | – | – | – | – | – | 24 | 16 | ||
| Phlips et al. (2018) | THERMOCOOL SMARTTOUCH | 50 | 62 | 100 | 62 | Median: 24 | 40.4 | – | – | – | 26.6 | – | 40 | 0 | [38] |
| THERMOCOOL SMARTTOUCH + AI | 50 | 61 | 100 | 72 | Median: 24 | 39.9 | – | – | – | 27.0 | – | 30 | 4 | ||
| Zhao et al. (2017) | Arctic Front | 50 | 60.9 | 100 | 72 | 47.5 | – | 62.4 | 0.89 | – | – | – | 38 | 12 | [37] |
| Arctic Front Advance | 50 | 60.4 | 100 | 80 | 51.3 | – | 61 | 0.82 | – | – | – | 36 | 14 |
Data are expressed as means or proportion of patients (%) except where otherwise noted. Blank cells represent unreported data.
†
Differences between baseline characteristics within in each treatment group are significant (p < 0.05).
‡
Data were reported for vascular disease.
AF: Atrial fibrillation; AI: Ablation Index; BMI: Body mass index; HT: Hypertension; LAD: Left atrial diameter; LVEF: Left ventricular ejection fraction; PAF: Paroxysmal atrial fibrillation; TIA: Transient ischemic attack.
Risk of bias assessment & study hierarchy
Risk of bias assessment for studies in which patients were randomized to device-level interventions revealed that one RCT had high risk of performance bias [21] and one had low risk of attrition and reporting bias (Supplementary Material 6) [23]. The ROBINS-I tool revealed all nonrandomized studies to have a moderate overall risk of bias for the outcome of freedom from atrial arrhythmias at 12-month follow-up (Supplementary Material 7).
Primary analysis
A total of 12 studies and 1722 patients were included in the primary analysis (Figure 2). The evidence network consisted primarily of multiple-study connections of two to four studies; single-study connections informed comparisons across device generations and ablation technologies (e.g., one study connecting the Arctic Front and THERMOCOOL SMARTTOUCH nodes and one study connecting the THERMOCOOL and Arctic Front Advance nodes). Evidence plots for each subnetwork (i.e., high-, unclear- and low-quality) are presented in Supplementary Material 9.

Figure 2. Evidence network of studies included in the primary analysis.
In the evidence network, the width of the lines for each connection is proportional to the number of studies comparing each pair of treatments. The size of each treatment node is proportional to the number of participants.
AI: THERMOCOOL SMARTTOUCH™ with Ablation Index; CB1: Arctic Front; CB2: Arctic Front Advance™; ST: THERMOCOOL SMARTTOUCH™; TC: THERMOCOOL™.
THERMOCOOL SMARTTOUCH with Ablation Index was associated the highest absolute probability (95.8%) of 12-month freedom from atrial arrhythmias, followed by THERMOCOOL SMARTTOUCH (87.5%), THERMOCOOL (71.5%), Arctic Front Advance (66.3%) and Arctic Front (54.0%). When compared with all other catheter ablation devices, results favored THERMOCOOL SMARTTOUCH with Ablation Index for the probability of 12-month freedom from atrial arrhythmias (Figure 3; Supplementary Material 10). THERMOCOOL SMARTTOUCH with Ablation Index was associated with a significantly greater (77%) likelihood of freedom from atrial arrhythmias than Arctic Front (RR: 1.77, 95% CrI: 1.21–2.87).
Similarly, THERMOCOOL SMARTTOUCH with Ablation Index was associated with a statistically significantly greater (41%) likelihood of 12-month freedom from atrial arrhythmias than Arctic Front Advance (RR: 1.41; 95% CrI: 1.06–2.47). Additionally, THERMOCOOL SMARTTOUCH with Ablation Index was associated with a significantly greater (34%) likelihood of freedom from atrial arrhythmias than THERMOCOOL (RR: 1.34; 95% CrI: 1.17–1.48) and a significantly greater (9%) likelihood of freedom from atrial arrhythmias than THERMOCOOL SMARTTOUCH (RR: 1.09; 95% CrI: 1–1.3). THERMOCOOL SMARTTOUCH with Ablation Index was ranked first among treatments (median rank 1; 95% CI: 1–2), followed by THERMOCOOL SMARTTOUCH (median rank 2; 95% CI: 2–3), THERMOCOOL (median rank 3; 95% CI: 3–5), Arctic Front Advance (median rank 4; 95% CI: 2–5) and Arctic Front (median rank 5; 95% CI: 4–5) (Supplementary Material 11). Furthermore, THERMOCOOL SMARTTOUCH with Ablation Index had the highest SUCRA (99.2%), followed by THERMOCOOL SMARTTOUCH (73.0%), THERMOCOOL (39.5%), Arctic Front Advance (33.6%) and Arctic Front (4.7%) (Supplementary Material 12).
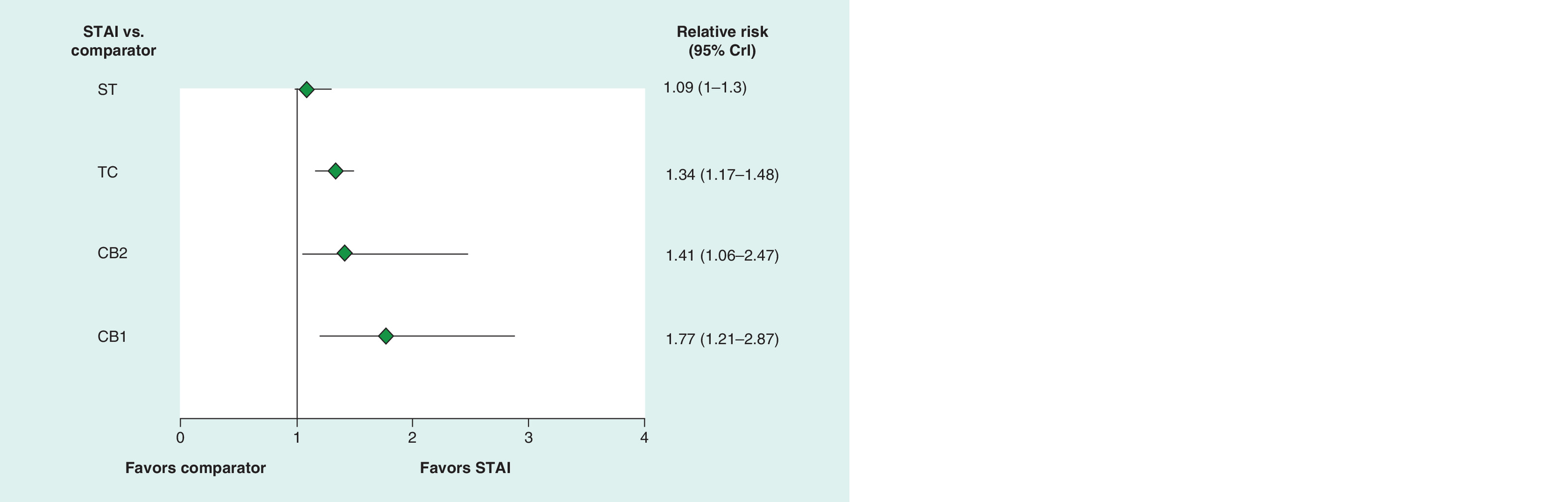
Figure 3. Forest plot summarizing results of the primary analysis for THERMOCOOL SMARTTOUCH™ with Ablation Index vs comparators.
CB1: Arctic Front; CB2: Arctic Front Advance™; CrI: Credible interval; ST: THERMOCOOL SMARTTOUCH™; STAI: THERMOCOOL SMARTTOUCH™ with Ablation Index; TC: THERMOCOOL™.
Secondary & sensitivity analyses
Secondary and sensitivity analyses included all studies from the primary analysis. The overall average effect across populations was similar to the results of the primary analysis (Figure 4; Supplementary Material 13). THERMOCOOL SMARTTOUCH with Ablation Index continued to have a statistically significantly greater likelihood of freedom from atrial arrhythmias than all catheter ablation devices except THERMOCOOL SMARTTOUCH, as well as the highest median rank and SUCRA (Supplementary Appendices 11 & 12).
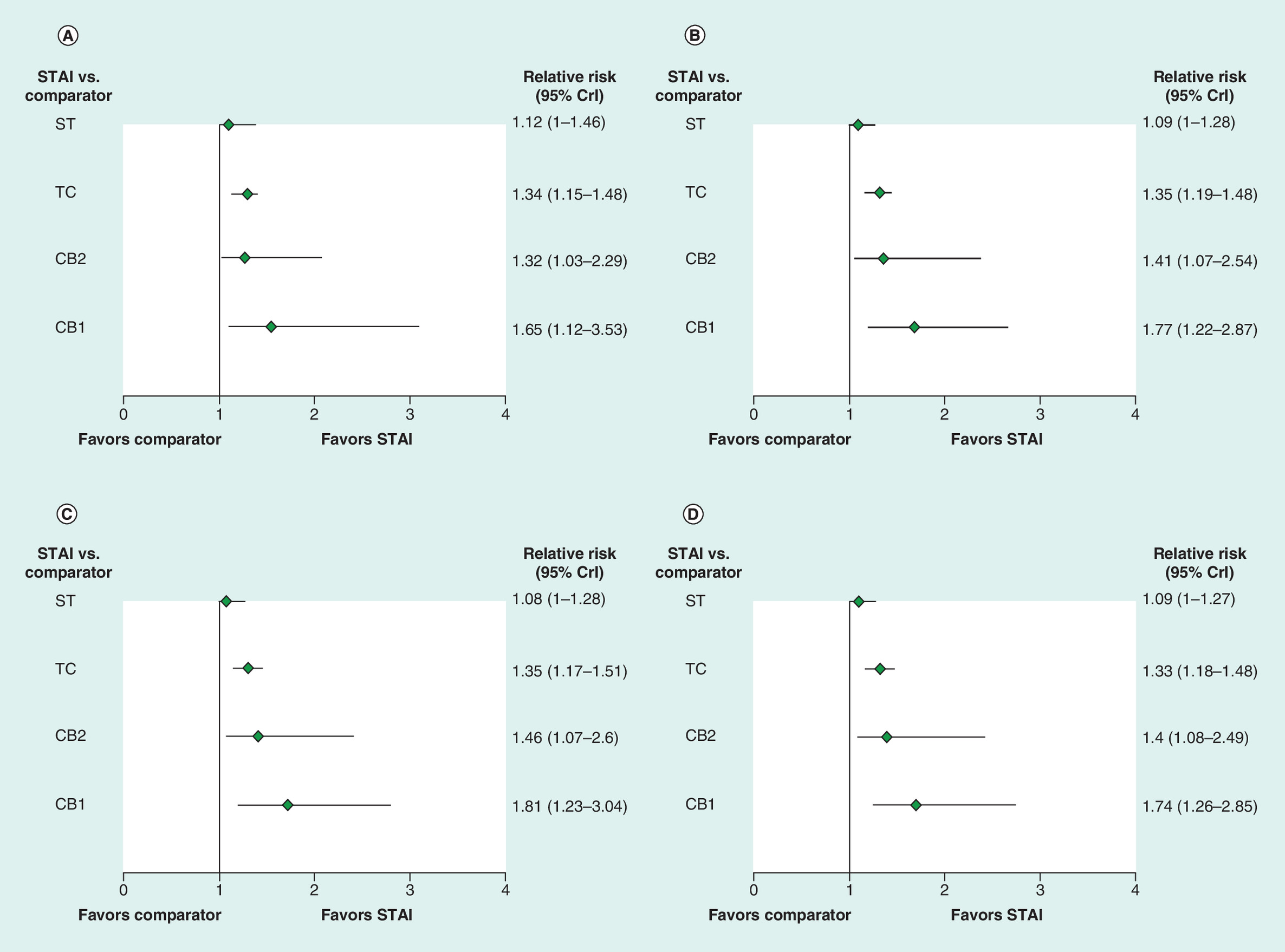
Figure 4. Summary of results from the secondary and sensitivity analyses for THERMOCOOL SMARTTOUCH™ with Ablation Index vs comparators.
(A) Bayesian hierarchical model with 50% downweighting (overall average effect); (B) Bayesian hierarchical model without downweighting (high quality); (C) Bayesian hierarchical model with 80% downweighting (high quality); (D) Bayesian hierarchical model where all three levels shared standard deviation and low- and unclear-quality studies are weighted by 50% of high-quality studies (high quality).
CB1: Arctic Front; CB2: Arctic Front Advance™; CrI: Credible interval; ST: THERMOCOOL SMARTTOUCH™; STAI: THERMOCOOL SMARTTOUCH™ with Ablation Index; TC: THERMOCOOL™.
Results of the primary analysis were reasonable and robust to changes in downweighting of low- and unclear-quality studies and the uncertainty in the low- and unclear-quality study levels due to low number of studies (Figure 4; Supplementary Material 13). When low- and unclear-quality studies were not downweighted or were downweighted 80%, THERMOCOOL SMARTTOUCH with Ablation Index continued to have a statistically significantly greater probability of freedom from atrial arrhythmias than all other catheter ablation devices. Additionally, results were consistent when an equivalent standard deviation was used across all three levels of the Bayesian hierarchical model. In all sensitivity analyses, THERMOCOOL SMARTTOUCH with Ablation Index continued to have the highest median rank and SUCRA (Supplementary Materiales 11 & 12).
Discussion
Advancements to catheter ablation technology are continually emerging; however, contemporary, high-quality evidence comparing these advanced technologies such as the THERMOCOOL SMARTTOUCH with Ablation Index are lacking. The objective of this study was to evaluate the comparative effectiveness of THERMOCOOL SMARTTOUCH with Ablation Index using the totality of currently available prospective comparative evidence for RF and CB ablation.
Overall, results from this analysis showed that THERMOCOOL SMARTTOUCH with Ablation Index provides significantly greater likelihood of freedom from recurrent atrial arrhythmias at 12-month follow-up than other catheter ablation devices. Additionally, THERMOCOOL SMARTTOUCH with Ablation Index was ranked first among all treatments and was associated with the highest probability of being ranked among the best treatments (SUCRA) for freedom from atrial arrhythmias at 12 months. Results of the primary analysis were robust in sensitivity analyses. Our results are consistent with those of a meta-analysis that compared THERMOCOOL SMARTTOUCH with Ablation Index to THERMOCOOL SMARTTOUCH, which found use of Ablation Index was associated with significant reductions in acute PV reconnection and arrhythmia recurrence at 12-month follow-up [13]. However, studies directly comparing CB to advanced RF technology are lacking; specifically, no studies directly compare CB to RF technology with the use of Ablation Index.
The lack of direct comparative data between alternative treatments makes assessments of various technologies challenging. This analysis provides decision-makers with robust, pooled, comparative evidence for the latest generations of catheter ablation devices used in the treatment of AF, namely THERMOCOOL SMARTTOUCH with Ablation Index and Arctic Front Advance, that reflects the totality of published evidence.
One limitation of this study is that results may be biased due to inclusion of poor-quality studies (i.e., low- or unclear-quality). Although the aim of a Bayesian hierarchical model is to incorporate the additional uncertainty related to biases introduced by pooling different study designs, the ability to estimate the true effect may be limited by an immature network and/or a lack of high-quality studies. Methods have been developed to manually adjust potentially biased studies based on the results of meta-epidemiological literature, but their application to this problem would be inappropriate owing to the lack of such studies specific to medical devices [29]. Another limitation was the lack of homogeneity across studies. The conduct of an NMA assumes there is homogeneity between studies being compared; however, heterogeneity was unavoidably introduced, for example, through differences in patient baseline characteristics, in the type of recurrent arrhythmia measured (i.e., AF, AT and AFL), and in the method used to monitor arrhythmias (Supplemental Material 16). This may affect the generalizability and applicability of results.
A major strength of the present study is that it is the first NMA to compare the effectiveness of AF ablation across several catheter ablation devices, with a focus on the most current technologies of Ablation Index and second-generation CB. Furthermore, the results of this analysis are highly comprehensive, including 12 prospective comparative studies. The majority of NMAs are conducted using RCTs; however, nonrandomized studies may be considered if RCT data are limited [39]. Specifically, conduct of a Bayesian hierarchical NMA is a rigorous statistical approach used to incorporate randomized and nonrandomized studies [40]. Incorporation of both randomized and nonrandomized studies helps to improve the generalizability and applicability of results to real-world scenarios important in clinical and health economic decision-making [41].
Conclusion
Overall, catheter ablation using the THERMOCOOL SMARTTOUCH Catheter with Ablation Index is statistically significantly more favorable for freedom from atrial arrhythmias at 12 months than first- and second-generation RF and CB catheters. This is the first study to provide decision-makers with robust, pooled, comparative evidence of the latest ablation technologies that reflects the totality of evidence available, particularly contemporary, high-quality studies.
•
Ablation Index is a novel lesion-quality marker associated with improved outcomes in radiofrequency ablation; however, there is a lack of direct comparative evidence between the latest generations of catheter ablation devices and uncertainty regarding the best treatment option.
•
We conducted a Bayesian hierarchical network meta-analysis of 12 prospective studies to evaluate the comparative effectiveness of radiofrequency ablation with Ablation Index to other catheter ablation devices in the treatment of atrial fibrillation (AF).
•
Radiofrequency ablation using the THERMOCOOL SMARTTOUCH™ Catheter with Ablation Index was associated the highest absolute probability (95.8%) of 12-month freedom from atrial arrhythmias, followed by THERMOCOOL SMARTTOUCH (87.5%), THERMOCOOL™ (71.5%), Arctic Front Advance™ (66.3%) and Arctic Front (54.0%).
•
THERMOCOOL SMARTTOUCH with Ablation Index was associated with statistically significantly greater probability of 12-month freedom from atrial arrhythmias than Arctic Front (relative risk: 1.77; 95% credible interval: 1.21–2.87), Arctic Front Advance (1.41; 1.06–2.47), THERMOCOOL (1.34; 1.17–1.48) and THERMOCOOL SMARTTOUCH (1.09; 1–1.3).
•
THERMOCOOL SMARTTOUCH with Ablation Index was ranked first among all treatments and was associated with the highest probability of being ranked among the best treatments (SUCRA) for freedom from atrial arrhythmias at 12 months.
•
In secondary and sensitivity analyses, the overall average effect across populations was similar to the results of the primary analysis.
•
The present study conducted a Bayesian hierarchical network meta-analysis, which is a rigorous statistical approach used to incorporate randomized and nonrandomized studies and improves the generalizability and applicability of results to real-world scenarios.
•
This analysis provides decision-makers with robust, pooled, comparative evidence for the latest generations of catheter ablation devices used in the treatment of atrial fibrillation.
Supplementary data
To view the supplementary data that accompany this paper please visit the journal website at: Supplementary Material
Author contributions
L Goldstein, M Velleca and G Costa contributed to the conception and design of the research and provided critical revisions and intellectual content to the manuscript. D Gupta and T De Potter provided substantial intellectual content, and revisions to the manuscript. T Disher, L Patel, D Grima and K Eaton conducted analyses, discussed the results, drafted the manuscript and contributed to the final version of the manuscript. All authors provided critical and intellectual feedback of the research, analysis and manuscript.
Acknowledgments
The authors would like to thank A Dineen for general support and K Dawkins (employees of Cornerstone Research Group, Inc.) for general and medical writing support.
Financial & competing interests disclosure
This work was funded by Biosense Webster, Inc. D Gupta and T De Potter are consultants to BioSense Webster, Inc. T Disher, L Patel, D Grima, and K Eaton are employees of Cornerstone Research Group, Inc. Cornerstone Research Group, Inc. receives consultancy fees from major pharmaceutical and device companies, including Biosense Webster, Inc. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Medical writing assistance was provided by Cornerstone Research Group.
Ethical conduct of research
This article is based on previously conducted studies and does not contain any studies with human participants or animals performed by any of the authors.
Data sharing statement
The datasets analyzed during the current study are available from the corresponding author on reasonable request.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary_appendicies.docx)
- Download
- 820.13 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Calkins H, Hindricks G, Cappato R et al. 2017 HRS/EHRA/ECAS/APHRS/SOLAECE expert consensus statement on catheter and surgical ablation of atrial fibrillation. Heart Rhythm 14(10), e275–e444 (2017).
• An expert consensus statement on catheter and surgical ablation of atrial fibrillation (AF). Ablation is routinely performed using radiofrequency (RF) and cryoballoon (CB) catheters, with RF catheters being the most widely used technology.
2.
January CT, Wann LS, Alpert JS et al. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society. J. Am. Coll. Cardiol. 64(21), e1–e76 (2014).
3.
Kirchhof P, Benussi S, Kotecha D et al. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur. J. Cardiothorac. Surg. 50(5), e1–e88 (2016).
4.
Chen J, Dagres N, Hocini M et al. Catheter ablation for atrial fibrillation: results from the first European Snapshot Survey on Procedural Routines for Atrial Fibrillation Ablation (ESS-PRAFA) Part II. Europace 17(11), 1727–1732 (2015).
5.
Andrade JG, Monir G, Pollak SJ et al. Pulmonary vein isolation using ‘contact force’ ablation: the effect on dormant conduction and long-term freedom from recurrent atrial fibrillation – a prospective study. Heart Rhythm 11(11), 1919–1924 (2014).
6.
Marijon E, Fazaa S, Narayanan K et al. Real-time contact force sensing for pulmonary vein isolation in the setting of paroxysmal atrial fibrillation: procedural and 1-year results. J. Cardiovasc. Electrophysiol. 25(2), 130–137 (2014).
7.
Itoh T, Kimura M, Tomita H et al. Reduced residual conduction gaps and favourable outcome in contact force-guided circumferential pulmonary vein isolation. Europace 18(4), 531–537 (2016).
8.
Nair GM, Yeo C, MacDonald Z et al. Three-year outcomes and reconnection patterns after initial contact force guided pulmonary vein isolation for paroxysmal atrial fibrillation. J. Cardiovasc. Electrophysiol. 28(9), 984–993 (2017).
9.
Lee G, Hunter RJ, Lovell MJ et al. Use of a contact force-sensing ablation catheter with advanced catheter location significantly reduces fluoroscopy time and radiation dose in catheter ablation of atrial fibrillation. Europace 18(2), 211–218 (2016).
10.
Sciarra L, Golia P, Natalizia A et al. Which is the best catheter to perform atrial fibrillation ablation? A comparison between standard ThermoCool, SmartTouch, and Surround Flow catheters. J. Interv. Cardiac Electrophysiol. 39(3), 193–200 (2014).
11.
Martinek M, Lemes C, Sigmund E et al. Clinical impact of an open-irrigated radiofrequency catheter with direct force measurement on atrial fibrillation ablation. Pacing Clin. Electrophysiol. 35(11), 1312–1318 (2012).
12.
Zhou X, Lv W, Zhang W et al. Impact of contact force technology on reducing the recurrence and major complications of atrial fibrillation ablation: a systematic review and meta-analysis. Anatol. J. Cardiol. 17(2), 82–91 (2017).
13.
Pranata R, Vania R, Huang I. Ablation-index guided versus conventional contact-force guided ablation in pulmonary vein isolation – systematic review and meta-analysis. Indian Pacing Electrophysiol. J. 19(4), 155–160 (2019).
•• A systematic review and meta-analysis showing significantly lower 12-month incidence of AF, atrial tachycardia (AT) and atrial flutter and significantly shorter fluoroscopy time and total ablation time with an ablation index-guided procedure than a conventional RF ablation procedure.
14.
Fürnkranz A, Bordignon S, Schmidt B et al. Improved procedural efficacy of pulmonary vein isolation using the novel second-generation cryoballoon. J. Cardiovasc. Electrophysiol. 24(5), 492–497 (2013).
15.
Koektuerk B, Yorgun H, Koch A et al. Pulmonary vein isolation in patients with paroxysmal atrial fibrillation: long-term clinical outcomes with first- and second-generation cryoballoons. Herz 42(1), 91–97 (2017).
16.
Heeger CH, Schuette C, Seitelberger V et al. Time-to-effect guided pulmonary vein isolation utilizing the third-generation versus second generation cryoballoon: one year clinical success. Cardiol. J. (2018). (Epub ahead of print).
17.
Aryana A, Kowalski M, O’Neill PG et al. Catheter ablation using the third-generation cryoballoon provides an enhanced ability to assess time to pulmonary vein isolation facilitating the ablation strategy: short- and long-term results of a multicenter study. Heart Rhythm 13(12), 2306–2313 (2016).
18.
Kuck KH, Brugada J, Furnkranz A et al. Cryoballoon or radiofrequency ablation for paroxysmal atrial fibrillation. N. Engl. J. Med. 374(23), 2235–2245 (2016).
• A randomized trial found the efficacy for the treatment of paroxysmal AF with CB ablation was noninferior to RF ablation and found no significant difference in overall safety between the two groups. Notably, the study did not randomize patients to advanced technologies within the CB and RF groups and was not sufficiently powered to compare advanced technologies.
19.
Hunter RJ, Baker V, Finlay MC et al. Point-by-point radiofrequency ablation versus the cryoballoon or a novel combined approach: a randomized trial comparing 3 methods of pulmonary vein isolation for paroxysmal atrial fibrillation (the cryo versus RF trial). J. Cardiovasc. Electrophysiol. 26(12), 1307–1314 (2015).
20.
Luik A, Radzewitz A, Kieser M et al. Cryoballoon versus open irrigated radiofrequency ablation in patients with paroxysmal atrial fibrillation: the prospective, randomized, controlled, noninferiority freeze AF study. Circulation 132(14), 1311–1319 (2015).
21.
Perez-Castellano N, Fernandez-Cavazos R, Moreno J et al. The COR trial: a randomized study with continuous rhythm monitoring to compare the efficacy of cryoenergy and radiofrequency for pulmonary vein isolation. Heart Rhythm 11(1), 8–14 (2014).
22.
Gunawardene MA, Hoffmann BA, Schaeffer B et al. Influence of energy source on early atrial fibrillation recurrences: a comparison of cryoballoon vs. radiofrequency current energy ablation with the endpoint of unexcitability in pulmonary vein isolation. Europace 20(1), 43–49 (2018).
23.
Davtyan K, Shatakhtsyan V, Poghosyan H et al. Radiofrequency versus cryoballoon ablation of atrial fibrillation: an evaluation using ECG, holter monitoring, and implantable loop recorders to monitor absolute and clinical effectiveness. BioMed Res. Int. 2018, 3629384, 1–7 (2018).
24.
Tonin FS, Rotta I, Mendes AM, Pontarolo R. Network meta-analysis: a technique to gather evidence from direct and indirect comparisons. Pharm. Pract. (Granada) 15(1), 943 (2017).
25.
Hutton B, Salanti G, Caldwell DM et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: checklist and explanations. Ann. Intern. Med. 162(11), 777–784 (2015).
26.
Higgins JP, Altman DG, Gotzsche PC et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 343, d5928 (2011).
27.
Sterne JA, Hernan MA, Reeves BC et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ 355, i4919 (2016).
28.
Dias S, Welton NJ, Sutton AJ, Ades AE. NICE DSU technical support document 2: a generalised linear framework for pairwise and network meta-analysis of randomized controlled trials. 1–98 (2011). http://www.nicedsu.org.uk
29.
Efthimiou O, Mavridis D, Debray TP et al. Combining randomized and non-randomized evidence in network meta-analysis. Stat. Med. 36(8), 1210–1226 (2017).
30.
Dias S, Welton NJ, Sutton AJ, Caldwell DM, Lu G, Ades AE. Evidence synthesis for decision making 4: inconsistency in networks of evidence based on randomized controlled trials. Med. Decis. Making 33(5), 641–656 (2013).
31.
Buist TJ, Adiyaman A, Smit JJJ, Ramdat Misier AR, Elvan A. Arrhythmia-free survival and pulmonary vein reconnection patterns after second-generation cryoballoon and contact-force radiofrequency pulmonary vein isolation. Clin. Res. Cardiol. 107(6), 498–506 (2018).
32.
Jourda F, Providencia R, Marijon E et al. Contact-force guided radiofrequency vs. second-generation balloon cryotherapy for pulmonary vein isolation in patients with paroxysmal atrial fibrillation-a prospective evaluation. Europace 17(2), 225–231 (2015).
33.
Dhillon G, Ahsan S, Honarbakhsh S et al. A multicentered evaluation of ablation at higher power guided by Ablation Index: establishing ablation targets for pulmonary vein isolation. J. Cardiovasc. Electrophysiol. 30(3), 357–365 (2019).
• A comparative study showing the rate of acute pulmonary vein (PV) reconnection was significantly lower and the rate of freedom from atrial arrhythmia at 12-month follow-up was higher in patients who received the Ablation Index-guided procedure than in patients who received a conventional contact force (CF)-guided procedure.
34.
Hussein A, Das M, Chaturvedi V et al. Prospective use of Ablation Index targets improves clinical outcomes following ablation for atrial fibrillation. J. Cardiovasc. Electrophysiol. 28(9), 1037–1047 (2017).
• A comparative study showing that Ablation Index-guided procedure was associated with a significantly improved rate of PV isolation success, and a significantly lower rate of acute PV reconnection and AT recurrence at 12-month follow-up than a group of propensity-matched controls who underwent CF-guided ablation.
35.
Sciarra L, Iacopino S, Palama Z et al. Impact of the third generation cryoballoon on atrial fibrillation ablation: an useful tool? Indian Pacing Electrophysiol. J. 18(4), 127–132 (2018).
36.
Solimene F, Schillaci V, Shopova G et al. Safety and efficacy of atrial fibrillation ablation guided by Ablation Index module. J. Interv. Cardiac Electrophysiol. 54(1), 9–15 (2019).
• A prospective, single-arm registry showing Ablation Index-guided ablation is feasible (i.e., high rate of PV isolation success), safe (i.e., low rate of complications) and effective (i.e., high single-procedure arrhythmia-free survival).
37.
Zhao A, Squara F, Marijon E, Thomas O. Two-year clinical outcome after a single cryoballoon ablation procedure: a comparison of first- and second-generation cryoballoons. Arch. Cardiovasc. Dis. 110(10), 543–549 (2017).
38.
Phlips T, Taghji P, El Haddad M et al. Improving procedural and one-year outcome after contact force-guided pulmonary vein isolation: the role of interlesion distance, Ablation Index, and contact force variability in the ‘CLOSE’-protocol. Europace 20(Fi_3), f419–f427 (2018).
• A comparative study showing 12-month freedom from AF, atrial flutter and AT was significantly higher in patients who received the Ablation Index-guided procedure than patients who received the conventional CF procedure. Additionally, procedure time and total RF time were significantly shorter in patients who received the Ablation Index-guided procedure.
39.
Schnell-Inderst P, Hunger T, Conrads-Frank A, Arvandi M, Siebert U. Ten recommendations for assessing the comparative effectiveness of therapeutic medical devices: a targeted review and adaptation. J. Clin. Epidemiol. 94, 97–113 (2018).
40.
Cameron C, Fireman B, Hutton B et al. Network meta-analysis incorporating randomized controlled trials and non-randomized comparative cohort studies for assessing the safety and effectiveness of medical treatments: challenges and opportunities. Syst. Rev. 4, 147–147 (2015).
41.
Husereau D. Real-world evidence: what role can it play in real-world decision-making? Summary report of the IHE Roundtable. Edmonton (AB). Institute of Health Economics, 1–12 (2017).
Information & Authors
Information
Published In
Pages: 115 - 126
PubMed: 31913063
Copyright
© 2020 Laura Goldstein. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 5 November 2019
Accepted: 27 November 2019
Published online: 8 January 2020
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Comparative effectiveness of catheter ablation devices in the treatment of atrial fibrillation: a network meta-analysis. (2020) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2019-0165
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Chukwuka Elendu, Nkechi P. Ogwu, Alexander U. Okatta, Eunice K. Omeludike, Emmanuel C. Ogelle, Babajide T. Obidigbo, Mary C. Joseph, Emmanuella I Osamuyi, Afeez O. Ogidan, Klein A. Jingwa, Abdul-Rahaman A Ottun, Mariam M.F. Eldorghamy, Tuvakbibi Gurbanova, Fathy E.A.E. Soltan, Umesh Bhadana, Vaibhav S. Nasre, Cyrus P. Yadav, Rishabh Jaiswal, Global Research Progress on Radiofrequency Ablation in Cardiology, Annals of Medicine & Surgery, 10.1097/MS9.0000000000002858, 87, 2, (725-747), (2025).
- Tom De Potter, Cindy Tong, Sonia Maccioni, Maria Velleca, Thibaut Galvain, Cost‐utility of VISITAG SURPOINT in catheter ablation of atrial fibrillation, Pacing and Clinical Electrophysiology, 10.1111/pace.14931, 47, 4, (568-576), (2024).
- Biqi Zhang, Jie Han, Dongchen Zhou, Jiajia Jiang, Jiawei Zhong, Yunlong Lu, Chenyu Zuo, Xingwei Lu, Jianwei Xuan, Aohan Zu, Yuxian He, Xingang Sun, Lu Chen, Liangrong Zheng, Radiofrequency ablation using the ThermoCool SmartTouch Catheter guided by ablation index versus antiarrhythmic drugs in atrial fibrillation treatment in China: a cost-consequence analysis, Journal of Comparative Effectiveness Research, 10.57264/cer-2023-0035, 13, 2, (2024).
- Qin-Dan Yan, Ke-Zeng Gong, Xue-Hai Chen, Jian-Hua Chen, Zhe Xu, Wei-Wei Wang, Fei-Long Zhang, Comparison of Second-Generation Cryoballoon Ablation and Quantitative Radiofrequency Ablation Guided by Ablation Index for Atrial Fibrillation, Angiology, 10.1177/00033197231159254, 75, 5, (462-471), (2023).
- Dong-Sung Won, Yubeen Park, Jinsu An, Dae Sung Ryu, Jeon Min Kang, Ji Won Kim, Song Hee Kim, Chu Hui Zeng, Hongbae Kim, Hyung-Sik Kim, Jung-Hoon Park, Sang Soo Lee, Stent-based electrode for radiofrequency ablation in the rat esophagus: a preliminary study, Scientific Reports, 10.1038/s41598-022-23472-7, 12, 1, (2022).
- Min Hu, Yi Han, Wangyang Zhao, Wen Chen, Long-Term Cost-Effectiveness Comparison of Catheter Ablation and Antiarrhythmic Drugs in Atrial Fibrillation Treatment Using Discrete Event Simulation, Value in Health, 10.1016/j.jval.2021.10.014, 25, 6, (975-983), (2022).
- Emmanouil Charitakis, Silvia Metelli, Lars O. Karlsson, Antonios P. Antoniadis, Konstantinos D. Rizas, Ioan Liuba, Henrik Almroth, Anders Hassel Jönsson, Jonas Schwieler, Dimitrios Tsartsalis, Skevos Sideris, Elena Dragioti, Nikolaos Fragakis, Anna Chaimani, Comparing efficacy and safety in catheter ablation strategies for atrial fibrillation: a network meta-analysis, BMC Medicine, 10.1186/s12916-022-02385-2, 20, 1, (2022).
- Adam E Berman, Sonia Maccioni, Rahul Khanna, Atrial fibrillation ablation with advanced radiofrequency catheter versus second-generation cryoballoon catheter, Journal of Comparative Effectiveness Research, 10.2217/cer-2021-0170, 11, 9, (659-668), (2022).
- Emmanouil Charitakis, Silvia Metelli, Lars O. Karlsson, Antonios P. Antoniadis, Ioan Liuba, Henrik Almroth, Anders Hassel Jönsson, Jonas Schwieler, Skevos Sideris, Dimitrios Tsartsalis, Elena Dragioti, Nikolaos Fragakis, Anna Chaimani, Comparing Efficacy and Safety in Catheter Ablation Strategies for Paroxysmal Atrial Fibrillation: A Network Meta-Analysis of Randomized Controlled Trials, Diagnostics, 10.3390/diagnostics12020433, 12, 2, (433), (2022).
- Chenxia Wu, Xinyi Li, Zhengtian Lv, Qian Chen, Yang Lou, Wei Mao, Xinbin Zhou, Second-generation cryoballoon versus contact force radiofrequency ablation for atrial fibrillation: an updated meta-analysis of evidence from randomized controlled trials, Scientific Reports, 10.1038/s41598-021-96820-8, 11, 1, (2021).