Atrial fibrillation ablation with advanced radiofrequency catheter versus second-generation cryoballoon catheter
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To compare cost and readmissions among atrial fibrillation (AF) patients undergoing ablation using the THERMOCOOL SMARTTOUCH™ SF (STSF) radiofrequency catheter versus the Arctic Front Advance™ (AFA) cryoballoon catheter. Patients & methods: The Premier Healthcare Database was used for the study purposes. Propensity score matching was used to match patients in the two groups. Costs and readmissions were assessed. A regression model was used for outcome assessment. Results: After propensity matching, 2767 patients were identified in each of the STSF and AFA cohorts. In the matched cohort, STSF patients had significantly lower supply costs than AFA patients. STSF patients had significantly lower 4–12-month AF-related inpatient readmissions compared with AFA patients (2.58% vs 3.99%; p = 0.0402). Costs of care summing index procedure and readmission costs were also lower for the STSF patients versus AFA patients. Conclusions: Patients who underwent AF ablation using the STSF catheter versus the AFA catheter had lower cost and AF-related readmissions.
Atrial fibrillation (AF) is the most common form of arrhythmia among adults in the USA [1]; more than 3 million people in the USA are diagnosed annually with AF, and this number is expected to increase to 7.5 million by 2050 [2]. AF is associated with considerable morbidity and mortality and imposes a substantial healthcare burden on patients, providers and payers [3,4]. The annual total direct medical costs among patients with AF are five times that of patients without AF, and the annual total direct medical and indirect costs (i.e., medically-related work-lost costs) are ∼US$14,000 higher among patients with AF compared with patients without AF [3]. The total annual healthcare cost of AF is estimated to be ∼US$6.7 billion, with AF-related hospitalizations accounting for 44% of those costs [5].
For patients with AF who do not tolerate or are unresponsive to antiarrhythmic drugs (AADs), catheter ablation is indicated as a second-line therapy [6–9]. In the Catheter Ablation Versus Antiarrhythmic Drug Therapy for Atrial Fibrillation (CABANA) trial, a multicenter, prospective, randomized trial comparing ablation treatment with drug therapy (AADs or rate control) among untreated or incompletely treated AF patients, recurrence of any (symptomatic or asymptomatic) AF was reduced by 48% (HR: 0.52; 95% CI: 0.45–0.60; p < 0.0001) and recurrence of symptomatic AF was reduced by 51% (HR: 0.49; 95% CI: 0.39–0.61; p < 0.001) over a 60-month follow-up period [10,11]. However, no significant differences in primary end point occurrence (a composite of death, disabling stroke, serious bleeding or cardiac arrest) were observed between the two study arms (ablation vs drug therapy) over a 48.5-month median follow-up period (8.0% vs 9.2%; HR: 0.86; 95% CI: 0.65–1.15; p = 0.30) [12]. Studies have reported radiofrequency (RF) ablation (with or without AADs) to be reasonably cost-effective as compared with AAD treatment alone for symptomatic, drug-refractory paroxysmal AF [13].
Various technological developments have improved the performance of catheters used for ablation; RF catheters with advanced porous tip technology allow for uniform cooling and reduced fluid delivery, while catheters with contact force technology significantly improve the ability to create durable lesions by providing real-time, catheter-to-tissue interaction information [14,15]. The THERMOCOOL SMARTTOUCH™ SF catheter (STSF; Biosense Webster, CA, USA) is a contact force catheter with 56-hole advanced porous tip technology that received premarket approval from the US FDA in 2016. Cryoballoon catheters, such as the Arctic Front Advance™ catheter (AFA; Medtronic, Dublin, Ireland), use cryoenergy for lesion formation as an alternate treatment approach for ablation.
There are very few studies comparing outcomes among patients with AF undergoing ablation procedures using the STSF versus AFA catheter. In one such study, labeled the CIRCA-DOSE study, which was a multicenter, randomized trial, outcomes among patients with paroxysmal AF were compared among those treated with contact force sensing RF catheters (STSF or THERMOCOOL SMARTTOUCH™ [ST] catheter) versus cryoballoon catheter (AFA; four-minute or two-minute approach) [16]. No significant difference in one-year efficacy outcome was observed between the study groups (53.9% for the RF group, 52.2% for the four-minute AFA approach and 51.7% for the two-minute AFA approach; p = 0.87). It should be noted that the RF approach included both the STSF and prior-generation ST catheter. Though the ST catheter is contact force sensing (similar to the STSF catheter), it is a standard irrigated 6-hole catheter and does not have 56-hole advanced porous tip irrigation as the STSF catheter. In a study comparing outcomes among patients with AF treated with STSF versus ST catheter, a significant reduction (51.7%; p < 0.01) in total irrigation fluid delivery was observed with the advanced irrigation STSF catheter compared with the standard irrigation ST catheter [17]. As also noted by the study authors, advanced fluid delivery with the STSF catheter could be critical when treating patients with ventricular function impairments. A recent study by Costea et al. compared outcomes among AF patients who underwent ablation using the STSF versus the AFA using real-world hospital data [18]. Results showed that AF patients treated with STSF had lower total ablation procedure costs and supply costs versus AFA. Additionally, patients who underwent ablation using the STSF catheter were less likely to experience cardiovascular (CV)-related readmissions compared with AFA patients 4–6 months postprocedure (excluding the blanking period, 0–3 months postprocedure). Though the study provided useful information regarding improved patient outcomes associated with the STSF versus the AFA, the follow-up period for key readmission outcomes was limited to 6 months. This study compared cost and 12-month readmissions following catheter ablation with STSF versus AFA for patients with AF using a nationwide hospital billing database.
Methods
Data source
This was a retrospective, observational cohort study using the Premier Healthcare Database (PHD), which contains complete clinical coding, hospital cost and patient billing data from more than 700 hospitals throughout the USA. Although the database excludes federally-funded hospitals (e.g., Veterans Affairs), the hospitals included are nationally representative, based on hospital size (i.e., number of beds), geographic region, location (urban and rural) and teaching hospital status. The database contains a date-stamped log of all billed items by the cost-accounting departments including laboratory, diagnostic and therapeutic services, primary and secondary diagnoses for each patient's hospitalization and medications. Detailed, service-level information for each hospital day is recorded, including details on medication and devices received.
Study sample
Patients aged 18 years and above with a primary diagnosis of AF who underwent an elective catheter ablation procedure in an inpatient or outpatient setting between 1 September 2016, and 31 March 2020, were identified in the PHD, with the first such ablation considered the index ablation/index admission. Patients who had an index ablation in a hospital that continuously contributed inpatient and outpatient data to the PHD in the 12-month preindex ablation period were identified. Patients who had catheter ablation or surgical ablation, valvular procedure, atrioventricular (AV) node ablation or left atrial appendage occlusion procedures in the 12-month preindex ablation period were excluded. Further, patients who had US$0 for their total index admission cost, supply cost and/or room and board cost were excluded. Patients were identified as being treated by STSF only if STSF was listed for the procedure, or as being treated by AFA if AFA was listed for the procedure (with or without additional point-to-point catheter), according to hospital charge descriptors. A text search strategy using fuzzy logic that incorporated a combination of device name, model number and/or catalog number was used to identify relevant study devices in the database. As per Title 45 Code of Federal Regulations, Part 46 of the USA, 45 CFR 46.101(b)(4) (www.hhs.gov/ohrp/humansubjects/guidance/45cfr46.html), the retrospective analysis of data from the PHD conducted in this study was exempt from Institutional Review Board (IRB) oversight.
Study outcomes
Primary outcomes included procedure cost, CV-related readmissions through 12 months (i.e., inpatient readmissions with a primary diagnosis of CV disease including AF) and AF-related readmissions through 12 months (i.e., inpatient readmissions with a primary diagnosis of AF). All readmission outcomes were assessed with and without a blanking period of 0–3 months post procedure. Cost outcomes included total cost for the index procedure (including supply/device costs, pharmacy costs, radiology costs and other costs associated with hospital admission), supply cost alone, sum of total index procedure cost plus 12-month CV-related (including AF) inpatient readmission cost and sum of total index procedure cost plus 12-month AF-related inpatient readmission cost. Costs were viewed from a hospital's perspective and were adjusted for medical inflation and reported in 2020 USD. Supplementary Appendix I lists the diagnosis and procedure codes associated with study inclusion/exclusion criteria and outcomes of interest.
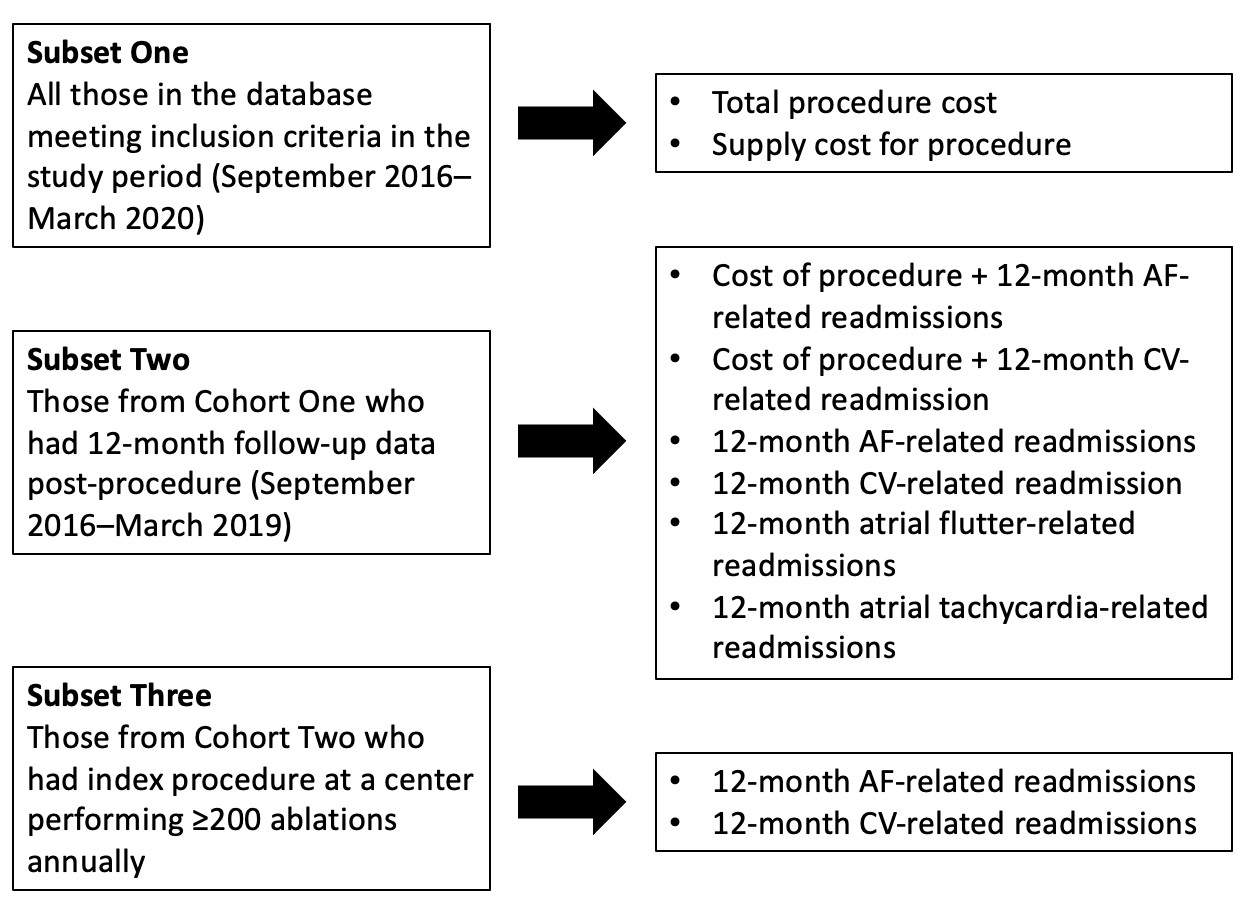
Study outcomes were necessarily examined in different subsets of the total eligible population; namely, total index procedure cost and supply cost were studied in the total study sample, whereas outcomes that involved 12-month CV-related and AF-related readmissions were restricted to those patients who had 12-month follow-up data available. Additionally, because the volume of ablations performed at a center may affect AF outcomes [12], 12-month readmission outcomes in the subset of the 12-month follow-up study sample who had procedures performed in high-volume centers were compared. For this sensitivity analysis, the sample was restricted to patients who had their index ablation procedure in a hospital that performed ≥200 AF ablations in the 12-month pre-index ablation period. Propensity matching was performed for each successive subset of patients; the three sample subsets and relevant outcomes investigated in each subset are shown in Supplementary Figure 1.
Study covariates
Patient demographics were collected, including age, sex, race and insurance type. Clinical characteristics assessed at index admission were hypertension, valvular heart disease, Elixhauser comorbidity score [19] and CHA2DS2-VASc score (which assesses for congestive heart failure, hypertension, age ≥75 years, diabetes mellitus, stroke or transient ischemic attack, vascular disease, age 65–74 years and sex category) [20]. The year and setting of the procedure (inpatient/outpatient) were also assessed. Hospital and provider characteristics collected included hospital size, geographic region (southern, western, etc.), teaching status and total hospital ablation volume in the 12-month pre-index ablation period (classified based on median cutoff).
Statistical analysis
A 1:1 propensity score matching (greedy match algorithm with 0.10 caliper) was used to match patients in the STSF and AFA groups. Three sets of propensity models were run for the study based on the three subsets of patients identified for analysis. The standardized difference was used to assess the postmatch balance of the covariates included in the propensity score model, with any covariate having a standardized mean difference (SMD) absolute value >0.25 or <-0.25 considered significant. Bivariate comparisons of outcomes in the matched cohorts were performed using t-test (for cost) and chi-square (for readmissions) analyses. Generalized estimating equation (GEE) models were used for outcome assessment, controlling for the clustering effect of hospitals and any significant covariate based on SMDs. For cost outcomes, a GEE model with log link and gamma distribution function was used. For CV- and AF-related readmissions, GEE with logit link and binomial distribution was used. In all analyses, a two-sided p < 0.05 was the threshold for statistically significant differences. Exponentiated ratios (ERs) and 95% CIs were calculated. All analyses were conducted using SAS for Windows, Version 9.4 (SAS Institute Inc., NC, USA).
Results
A total of 11,519 patients were identified, with 7758 patients (mean age: 64.96 ± 10.16 years; 62.68% [4863/7758] male) treated exclusively with STSF and 3761 patients (mean age: 64.93 ± 10.25; 59.61% [2242/3761] male) treated with AFA (with or without an additional point-to-point catheter). Figure 1 describes the patient attrition based on study criteria.
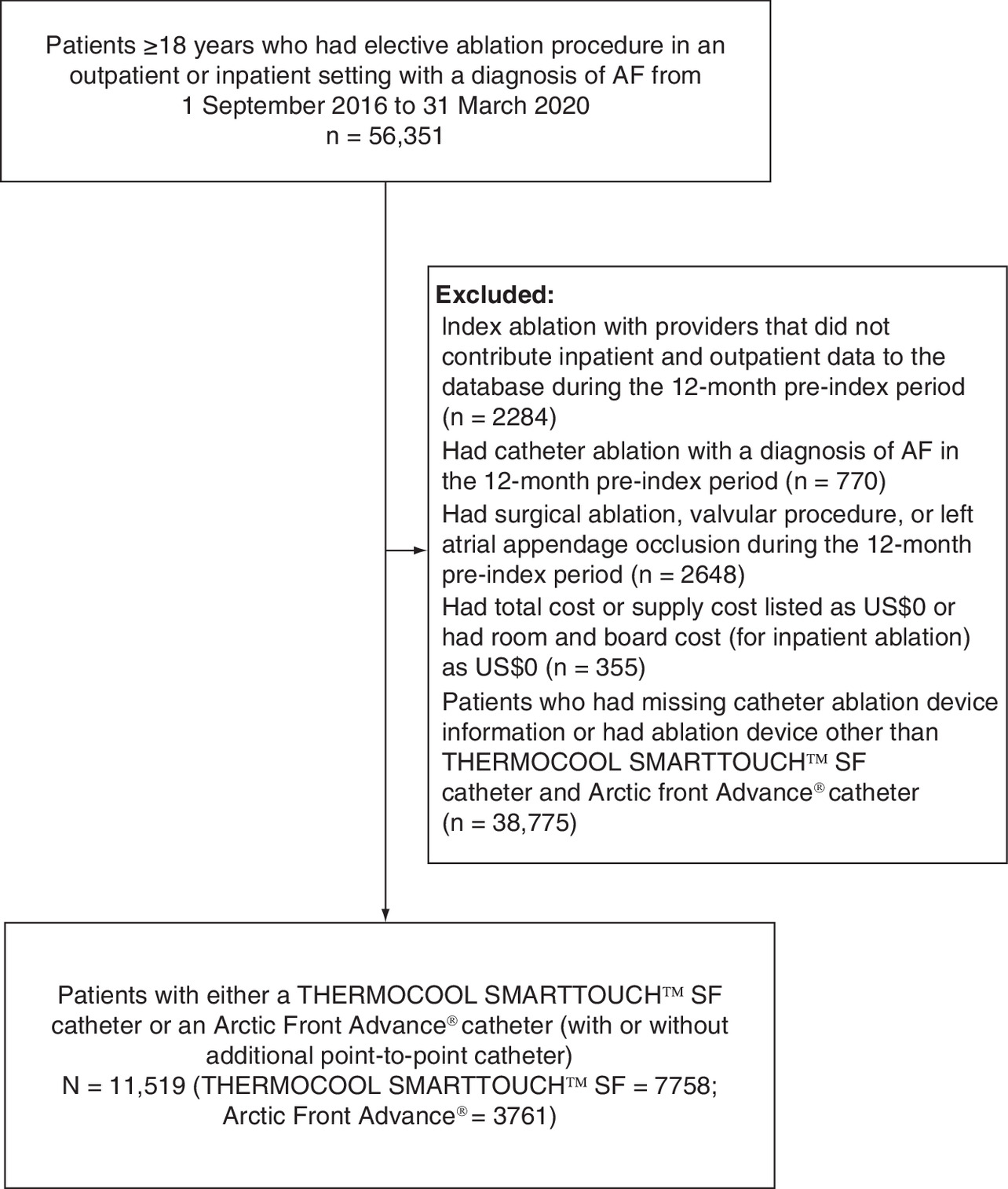
Figure 1. Patient attrition during database inclusion/exclusion criteria searches.
AF: Atrial fibrillation; AV: Atrioventricular.
Patient and provider characteristics for the sample identified for assessment of total index admission cost and supply cost are presented in Supplementary Table 1. In the prematch sample of 11,519 patients, there were significant differences between the STSF and AFA groups for ablation year, hospital region and hospital size. After matching, 2767 patients were identified for both STSF and AFA (mean age: 63.98 vs 65.14 years; 62.27% [1723/2767] vs 60.21% [1666/2767] male, respectively).
Cost outcomes are reported in Table 1. There were no significant differences in total index admission cost for STSF versus AFA (US$24,801 versus $25,914; ER: 0.9570, 95% CI: 0.8633–1.0610; p = 0.4040). However, supply costs were significantly lower for STSF patients compared with AFA patients (US$10,539 vs $13,416; ER: 0.7855, 95% CI: 0.7118–0.8669; p < 0.0001), amounting to a 21.45% lower cost for STSF.
| Exponentiated cost (STSF [2767] vs AFA [2767]) | Exponentiated ratio (GEE model) | 95% CI | p-value† | |
|---|---|---|---|---|
| Total index procedure admission cost | $24,801 (SE: $941.34) vs $25,914 (SE: $995.47) | 0.9570 | 0.8633–1.0610 | 0.4040 |
| Supply cost for index procedure | $10,539 (SE: $448.24) vs $13,416 (SE: $694.10) | 0.7855 | 0.7118–0.8669 | <0.0001 |
| Index procedure admission cost + 12-month total CV-related inpatient readmission cost | $26,155 (SE: $1153.47) vs $29,190 (SE: $1228.50) | 0.8960 | 0.8031–0.9997 | 0.0494 |
| Index procedure admission cost + 12-month AF-related inpatient readmission cost | $25,099 (SE: $1087.85) vs $27,893 (SE: $1057.40) | 0.8998 | 0.8104–0.9992 | 0.0482 |
†
Based on p-value from GEE model (empirical based standard error estimate) accounting for hospital clustering in the matched cohort.
AF: Atrial fibrillation; AFA: Arctic Front Advance™; CV: Cardiovascular; GEE: Generalized estimating equation; SE: Standard error; STSF: THERMOCOOL SMARTTOUCH™ SF.
When restricting the pre-match sample to patients with available follow-up data in the 12-month post procedure period, 6527 patients remained, with 4089 patients in the STSF group and 2438 patients in the AFA group. After propensity matching, 1781 patients were identified for the STSF (mean age: 64.26 years; 62.55% [1114/1781] male) and AFA (mean age: 64.59; 61.20% [1090/1781] male) groups, respectively (Supplementary Table 2). In this matched cohort, STSF patients had a lower cost of procedure plus 12-month CV-related inpatient readmission cost compared with AFA patients (US$26,155 vs $29,190; ER: 0.8960, 95% CI: 0.8031–0.9997; p = 0.0494). STSF patients were also observed to have a lower cost of procedure plus 12-month AF-related inpatient readmission cost compared with AFA patients (US$25,099 vs $27,893; ER: 0.8998, 95% CI: 0.8104–0.9992; p = 0.0492).
When examining readmissions (Table 2), no significant differences were observed between STSF and AFA patients for 12-month CV-related inpatient readmissions (with or without a blanking period). For AF-related inpatient readmissions including the blanking period (0–12 months), STSF patients had a significantly lower rate compared with AFA patients on bivariate analysis (4.83% vs 6.4; p = 0.0416); however, results from the GEE analysis suggested no difference in the two devices (ER: 0.7794, 95% CI: 0.5349–1.1357; p = 0.1945). For AF-related inpatient readmissions excluding the blanking period (4–12 months), STSF patients were observed to have a significantly lower rate compared with AFA patients (2.58% vs 3.99%; p = 0.0188). GEE analysis showed that STSF patients had 33.84% lower odds of AF-related inpatient admissions than AFA patients in the postindex ablation 4–12-month period (ER: 0.6616, 95% CI: 0.4458–0.9817; p = 0.0402).
| Bivariate comparison (STSF [n = 1781] vs AFA [n = 1781]) | p-value† | Odds ratio (GEE model) | 95% CI | p-value‡ | |
|---|---|---|---|---|---|
| Inpatient admissions among STSF vs AFA patients | |||||
| CV-related readmission | |||||
| 0–12 months | 9.55% vs 10.56% | 0.3158 | 0.9146 | 0.6909–1.2108 | 0.5329 |
| 4–12 months | 5.22% vs 6.06% | 0.2761 | 0.8770 | 0.6370–1.2076 | 0.4214 |
| AF-related readmission | |||||
| 0–12 months | 4.83% vs 6.40% | 0.0416 | 0.7794 | 0.5349–1.1357 | 0.1945 |
| 4–12 months | 2.58% vs 3.99% | 0.0188 | 0.6616 | 0.4458–0.9817 | 0.0402 |
| Inpatient admissions in STSF vs AFA patients in high-volume centers | |||||
| CV-related readmission | |||||
| 0–12 months | 68 (9.08%) vs 82 (10.95%) | 0.2282 | 0.8982 | 0.5850–1.3792 | 0.6237 |
| 4–12 months | 36 (4.81%) vs 50 (6.68%) | 0.1200 | 0.7079 | 0.4520–1.1087 | 0.1313 |
| AF-related readmission | |||||
| 0–12 months | 28 (3.74%) vs 51 (6.81%) | 0.0078 | 0.5864 | 0.3379–1.0176 | 0.0577 |
| 4–12 months | 14 (1.87%) vs 31 (4.14%) | 0.0101 | 0.4751 | 0.2290–0.9857 | 0.0456 |
†
Based on p-value from student t-test comparing outcome in the matched cohort.
‡
Based on p-value from GEE model (empirical based standard error estimate) accounting for hospital clustering in the matched cohort.
AF: Atrial fibrillation; AFA: Arctic Front Advance™; CV: Cardiovascular; GEE: Generalized estimating equation; STSF: THERMOCOOL SMARTTOUCH™ SF.
For sensitivity analysis of readmissions outcomes, 2357 STSF patients and 1509 AFA patients were identified in the pre-match sample as having index procedures at centers performing ≥200 ablations annually. After propensity matching, 749 patients each were identified for the STSF (mean age: 63.64 years; 62.75% [470/749] male) and AFA (mean age: 64.59 years; 62.35% [467/749] male) groups (Supplementary Table 3). Patients who underwent ablation using STSF had significantly lower AF-related inpatient admissions 4–12 months post procedure compared with those who had ablation with the AFA (1.87% vs 4.14%; p = 0.0101). Results from GEE analysis suggested that STSF patients had 52.49% lower odds (ER: 0.4751, 95% CI: 0.229–0.986; p = 0.0456) of AF-related inpatient admissions in the 4–12-month post-index admission period compared with AFA patients. There were no significant differences in GEE analyses between groups for AF-related inpatient admissions in the 0–12-month post ablation period or for CV-related inpatient admissions (with or without a blanking period; Table 2).
Discussion
This real-world analysis of a nationwide database examining catheter ablation for AF demonstrated that STSF use was associated with significantly lower supply costs and overall costs (when including the cost of 12-month readmissions) compared with the AFA catheter. Further, patients who underwent ablation using the STSF catheter had lower odds of AF-related inpatient readmissions in the post-blanking 4–12-month period compared with those who had ablation using the AFA catheter. There were no significant differences observed between groups for procedure cost alone or 12-month CV-related inpatient readmissions. Thus, compared with AFA, STSF may be a more cost-effective option for patients undergoing catheter ablation.
There is limited information in the literature comparing procedural and other costs for STSF and AFA patients. Costea et al. compared six-month outcomes among STSF and AFA patients and showed that patients treated with STSF had lower total ablation procedure costs and lower supply costs versus AFA [18]. The authors found that roughly half of the savings were attributable to the use of an additional point-to-point catheter in the AFA group. Though not specific to the device under investigation in this study, prior research has suggested RF ablation is less costly than cryoballoon ablation [21,22]. Similar to the current analysis, an older study using the PHD database examined the cost differential between RF and cryoballoon ablation and determined the inpatient cost to be 30% higher and outpatient cost to be 19.5% higher for the cryoballoon group as compared with RF-treated patients [21]. In a single-center study comparing procedural cost, safety and efficacy outcomes among symptomatic AF patients treated with RF versus cryoballoon ablation, cryoballoon utilization was associated with an incremental US$7482 hospital cost per procedure (US$24,392 vs $31,874; p < 0.0001) [22]. Though total procedural cost appeared to be lower ($1113) among STSF patients in the present study, the difference was not significant.
Ming et al. performed a cost-effectiveness analysis of cryoballoon versus RF ablation technologies for the treatment of AF [23]. Their modeling analysis included data from a single large tertiary care medical center in China. The total number of patients included in their outcome analyses was 340 and first-generation cryoballoon technology was used in all patients included in the analysis. Unlike the current study, which included second-generation cryoballoon-treated patients, these authors did not comment on the type of RF ablation catheters used in the RF arm of their analysis. They found cryoballoon technology to be cost-effective when compared with RF (ICER = $16,590 per quality-adjusted life-year gained). When comparing this analysis to ours, we feel that the inclusion of newer cryoballoon and RF technologies, in conjunction with a significantly larger sample size derived from multicenter diverse clinical data provides a more contemporary and accurate representation of the downstream costs and benefits associated with AF ablation. Finally, the ongoing COVID-19 pandemic has strained healthcare systems as they reduce elective procedures and galvanize resources needed for COVID-19 response efforts [24]. As hospitals navigate these economic challenges, cost savings could be accrued during AF ablation procedures through the use of the STSF catheter versus the AFA catheter.
Though no differences were observed in CV-related readmissions in the current study, STSF patients were observed to have a lower rate of 12-month AF-related readmissions (both with and without the blanking period). These results were consistent when analyses were restricted to high-volume centers. In their study examining six-month outcomes, Costea et al. observed a lower likelihood of CV-related readmissions in the post-blanking 4–6-month period for STSF patients compared with AFA patients (odds ratio [OR]: 0.460, 95% CI: 0.220–0.959) [18]. Though the authors did not observe a significant difference in 4–6-month AF-related readmissions, AF was considered the main driver of CV-related readmissions. More recently, results from the RACE-AF trial, which is a single-center, prospective, randomized clinical trial comparing contact force (CF), irrigated RF catheter and second-generation cryoballoon catheter, suggested no difference between the two catheters in durable isolation of pulmonary veins when assessed at 4–6 months post ablation (76% vs 81%; p = 0.32) [25]. The study further reported a 99.95% reduction in AF burden in the post-blanking period in the RF group and 99.34% in the cryoballoon group (p = 0.36). Both Costea et al. [18] and the RACE-AF trial [25] had a short-term follow-up period (post-blanking 4–6 months). The current results suggest that the benefits and efficacy profile of CF irrigated STSF catheter as compared with second-generation cryoballoon catheter are accrued over a longer-term follow-up period. Further research is needed to examine the difference in readmission and cost outcomes between the STSF and AFA catheters beyond the 12-month post ablation window.
More recent advancements in RF ablation include the development and clinical implementation of a novel lesion-quality marker, the Ablation Index (AI). This indicator of the quality of an RF ablation lesion has led to considerable improvements in clinical outcomes among AF ablation patients [26,27]. In their meta-analysis of studies involving AI-guided procedures versus conventional ablation procedures, Pranata et al. found a significantly lower incidence of 12-month AF/AT/atrial flutter (AFL) in AI-guided procedures (OR: 0.35, 95% CI: 0.17–0.73; p = 0.005; I2: 58%) compared with procedures that did not use AI [27]. When comparing 12-month recurrence in atrial arrhythmias between RF ablation (ST/STSF) with AI and cryoballoon (AFA) using matching-adjusted indirect comparison, Hussein et al. observed a 70% reduction in 12-month atrial arrhythmia recurrence (HR: 0.30, 95% CI: 0.13–0.71) with the RF with AI group versus the cryoballoon group [28]. A network meta-analysis comparing 12-month atrial arrhythmia recurrence between ST with AI versus first- and second-generation RF and cryoballoon catheters found that the former was associated with a significantly higher probability of 12-month freedom from atrial arrhythmias compared with AFA catheter (relative risk [RR]: 1.41; 95% CI: 1.06–2.47) [29]. AI utilization in study cases in the current study could not be assessed, as this information is not available in the PHD. However, it is very likely that AI use would have occurred for some (if not all) of the STSF procedures in this study. Further research using alternative data sources and settings comparing STSF use with AI versus AFA could shed more light on the clinical benefit accrued with the use of AI with RF ablation.
In the current study, the lower likelihood of readmissions among STSF patients is very likely the main driver behind the lower cost of index procedure plus the cost of inpatient readmissions. In this way, STSF use contributed to lowering the total cost of AF management up to 12 months post procedure. As healthcare dollars become scarce, the lower total cost of care for AF patients undergoing ablation associated with STSF use versus AFA use may offer economic savings for patients, payers and providers.
This study has several limitations. Unique device identifiers (UDIs) are not fully adopted, so devices were identified using fuzzy logic algorithms relying on device names and catalog identifiers; these imperfect search strategies may lead to misidentification. Some clinical and procedural parameters, such as AF severity, ablation technique and procedure time, are not listed in the PHD, although these factors could affect outcomes. Additionally, readmission was only registered in the PHD if the patient returned to the same hospital where the index procedure was performed; therefore, it is possible that some readmissions were not captured, making the observed rate of readmission potentially lower than the true rate of readmission. It is fair to assume that this would have led to nondifferential bias (i.e., the same rate of readmissions not being captured in both STSF and AFA groups), and thus would have equally affected the two study cohorts. This study involved observational retrospective database analysis, and as such, causal inferences cannot be assumed. When examining the distribution of the patients, around 89% were white and 62% were male. As such, nonwhites and females were underrepresented in our study, which is reflective of ablation treatment. Studies have reported nonwhites and females to be less likely to receive ablation treatment for AF [30–32], which would explain the underrepresentation in this study. Further, the clinical success rates of AF ablation procedures could vary by demographic factors including race and sex [33]. If feasible, future comparative studies at the specific device level should consider a more representative demographic distribution. Finally, any errors that occurred during billing or hospital coding could have influenced the study results.
Conclusion
For patients undergoing AF ablation, operative use of the STSF catheter was associated with lower supply cost and a lower rate of 12-month postoperative AF-related inpatient admissions. STSF catheter use was also associated with a lower total cost of AF management (cost of index procedure plus 12-month inpatient readmissions costs). As CV healthcare resources become increasingly strained due to increasing AF prevalence and incidence within the emerging post-COVID-19 pandemic care delivery environment, these results suggest that both financial savings and improved patient outcomes may be accrued with the use of the STSF catheter compared with the AFA catheter during routine catheter ablation of AF.
•
Limited information is currently available on differences in cost and inpatient readmission burden among atrial fibrillation (AF) patients who underwent ablation using a 56-hole advanced porous tip contact force radiofrequency catheter (THERMOCOOL SMARTTOUCH™ SF) versus a second-generation cryoballoon catheter (Arctic Front Advance™ catheter).
•
Using a nationwide hospital billing database, this study found lower supply costs during ablation procedures, lower inpatient readmission costs (including procedure cost) and lower AF-related inpatient readmission rate for radiofrequency catheter patients compared with second-generation cryoballoon patients.
•
No differences were observed in procedure cost and cardiovascular-related inpatient readmissions between the study cohorts.
•
As healthcare resources are constrained, a trend further accentuated by the COVID-19 pandemic, the use of an advanced radiofrequency catheter for AF ablation offers economic savings and improved clinical benefit (from a readmission perspective) compared with second-generation cryoballoon catheters.
Author contributions
Conception and design: all authors. Collection and assembly of data: S Maccioni and R Khanna. Data analysis and interpretation: S Maccionid R Khanna. Manuscript writing: all authors. Final approval of manuscript: all authors.
Financial & competing interests disclosure
This study was funded by Johnson & Johnson. A Berman has served as a consultant to Biosense Webster. S Maccioni and R Khanna are Johnson & Johnson employees. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
The authors acknowledge Superior Medical Experts for their assistance with drafting and editing.
Ethical conduct of research
In the USA, retrospective analyses of the Premier Healthcare Database data are considered exempt from institutional review board (IRB) oversight as dictated by Title 45 Code of Federal Regulations, Part 46 of the USA, specifically 45 CFR 46.101(b)(4) (www.hhs.gov/ohrp/humansubjects/guidance/45cfr46.html).
Data sharing statement
Data may be obtained from a third party and are not publicly available.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
Supplementary Material
{kind=link}
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Wyndham CR. Atrial fibrillation: the most common arrhythmia. Tex. Heart Inst. J. 27(3), 257–267 (2000).
2.
Naccarelli GV, Varker H, Lin J, Schulman KL. Increasing prevalence of atrial fibrillation and flutter in the United States. Am. J. Cardiol. 104(11), 1534–1539 (2009).
3.
Wu EQ, Birnbaum HG, Mareva M et al. Economic burden and co-morbidities of atrial fibrillation in a privately insured population. Curr. Med. Res. Opin. 21(10), 1693–1699 (2005).
4.
Benjamin EJ, Wolf PA, D'agostino RB, Silbershatz H, Kannel WB, Levy D. Impact of atrial fibrillation on the risk of death: the Framingham Heart Study. Circulation 98(10), 946–952 (1998).
5.
Coyne KS, Paramore C, Grandy S, Mercader M, Reynolds M, Zimetbaum P. Assessing the direct costs of treating nonvalvular atrial fibrillation in the United States. Value Health 9(5), 348–356 (2006).
6.
Calkins H, Hindricks G, Cappato R et al. 2017 HRS/EHRA/ECAS/APHRS/SOLAECE expert consensus statement on catheter and surgical ablation of atrial fibrillation: executive summary. Europace 20(1), 157–208 (2018).
7.
January CT, Wann LS, Calkins H et al. 2019 AHA/ACC/HRS Focused Update of the 2014 AHA/ACC/HRS Guideline for the Management of Patients With Atrial Fibrillation: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. J. Am. Coll. Cardiol. 74(1), 104–132 (2019).
8.
Kirchhof P, Benussi S, Kotecha D et al. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Europace 18(11), 1609–1678 (2016).
9.
Senoo K, Lau YC, Lip GY. Updated NICE guideline: management of atrial fibrillation (2014). Expert Rev. Cardiovasc. Ther. 12(9), 1037–1040 (2014).
10.
Poole JE, Bahnson TD, Monahan KH et al. Recurrence of atrial fibrillation after catheter ablation or antiarrhythmic drug therapy in the CABANA trial. J. Am. Coll. Cardiol. 75(25), 3105–3118 (2020).
11.
Packer DL, Mark DB, Robb RA et al. Catheter ablation versus antiarrhythmic drug therapy for atrial fibrillation (CABANA) trial: study rationale and design. Am. Heart J. 199, 192–199 (2018).
12.
Packer DL, Mark DB, Robb RA et al. Effect of catheter ablation vs antiarrhythmic drug therapy on mortality, stroke, bleeding, and cardiac arrest among patients with atrial fibrillation: The CABANA randomized clinical trial. JAMA 321(13), 1261–1274 (2019).
13.
Reynolds MR, Zimetbaum P, Josephson ME, Ellis E, Danilov T, Cohen DJ. Cost-effectiveness of radiofrequency catheter ablation compared with antiarrhythmic drug therapy for paroxysmal atrial fibrillation. Circ. Arrhythm. Electrophysiol. 2(4), 362–369 (2009).
14.
Peichl P, Kautzner J. Advances in irrigated tip catheter technology for treatment of cardiac arrhythmias. Recent Pat. Cardiovasc. Drug Discov. 8(1), 10–16 (2013).
15.
Plenge T, Van Den Bruck JH, Lüker J, Sultan A, Steven D. Porous tip contact force-sensing catheters for pulmonary vein isolation: performance in a clinical routine setting. J. Interv. Card Electrophysiol. 57(2), 251–259 (2020).
• Demonstrated shorter ablation time and lower irrigation fluid delivery with the SMARTTOUCH™ SF catheter versus the SmartTouch catheter.
16.
Andrade JG, Champagne J, Dubuc M et al. Cryoballoon or radiofrequency ablation for atrial fibrillation assessed by continuous monitoring: a randomized clinical trial. Circulation 140(22), 1779–1788 (2019).
17.
Maurer T, Rottner L, Makimoto H, Reissmann B et al. The best of two worlds? Pulmonary vein isolation using a novel radiofrequency ablation catheter incorporating contact force sensing technology and 56-hole porous tip irrigation. Clinical Research in Cardiology 107(11), 1003–1012 (2018).
• Total irrigation fluid delivery was shown to reduce by 51.7% with the use of the SMARTTOUCH™ SF catheter as compared to the ST catheter among patients with drug-refractory atrial fibrillation.
18.
Costea A, Goldstein L, Maccioni S, Kalsekar I, Khanna R. Real-world outcomes comparison among adults with atrial fibrillation undergoing catheter ablation with a contact force porous tip catheter versus a second-generation cryoballoon catheter: a retrospective analysis of multihospital US database. BMJ Open 10(8), e035499 (2020).
•• Significantly lower procedure cost and supply cost were observed for patients with atrial fibrillation treated with the SMARTTOUCH™ SF catheter versus the Arctic Front Advance™ catheter.
19.
Elixhauser A, Steiner C, Harris DR, Coffey RM. Comorbidity measures for use with administrative data. Med. Care 36(1), 8–27 (1998).
20.
Lip GY, Nieuwlaat R, Pisters R, Lane DA, Crijns HJ. Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: the euro heart survey on atrial fibrillation. Chest 137(2), 263–272 (2010).
21.
Hunter TD, Palli SR, Rizzo JA. Cost comparison of radiofrequency catheter ablation versus cryoablation for atrial fibrillation in hospitals using both technologies. J. Med. Econ. 19(10), 959–964 (2016).
•• Inpatient and outpatient costs were reported to be higher for patients with atrial fibrillation undergoing cryoablation versus radiofrequency ablation.
22.
Mandell J, Amico F, Parekh S, Snow J, Germano J, Cohen TJ. Early experience with the cryoablation balloon procedure for the treatment of atrial fibrillation by an experienced radiofrequency catheter ablation center. J. Invasive Cardiol. 25(6), 288–292 (2013).
23.
Ming J, Wei Y, Sun H et al. Cost-effectiveness of cryoballoon ablation versus radiofrequency ablation for paroxysmal atrial fibrillation in China: results based on real-world data. Value Health 22(8), 863–870 (2019).
24.
Khullar D, Bond AM, Schpero WL. COVID-19 and the financial health of US hospitals. JAMA 323(21), 2127 (2020).
25.
Sorensen SK, Johannessen A, Worck R, Hansen ML, Hansen J. Radiofrequency Versus cryoballoon catheter ablation for paroxysmal atrial fibrillation: durability of pulmonary vein isolation and effect on atrial fibrillation burden: The RACE-AF randomized controlled trial. Circ. Arrhythm. Electrophysiol. 14(5), e009573 (2021).
26.
Hussein A, Das M, Riva S et al. Use of ablation index-guided ablation results in high rates of durable pulmonary vein isolation and freedom from arrhythmia in persistent atrial fibrillation patients: The PRAISE Study results. Circ. Arrhythm. Electrophysiol. 11(9), e006576 (2018).
27.
Pranata R, Vania R, Huang I. Ablation-index guided versus conventional contact-force guided ablation in pulmonary vein isolation - systematic review and meta-analysis. Indian Pacing Electrophysiol. J. 19(4), 155–160 (2019).
• Radiofrequency ablation guided by the Ablation Index resulted in a significantly lower incidence of atrial fibrillation/atrial tachycardia/atrial flutter, shorter fluoroscopy time and total ablation time compared with conventional ablation.
28.
Hussein A, Gupta D, De Potter T et al. Treatment of atrial fibrillation using ablation index-guided contact force ablation: a matching-adjusted indirect comparison to cryoballoon ablation. Adv. Ther. 37(2), 785–799 (2020).
29.
Gupta D, Potter T, Disher T et al. Comparative effectiveness of catheter ablation devices in the treatment of atrial fibrillation: a network meta-analysis. J. Comp. Eff Res. 9(2), 115–126 (2020).
30.
Nanda A, Kabra R. Racial differences in atrial fibrillation epidemiology, management, and outcomes. Curr. Treat. Options Cardiovasc. Med. 21(12), 85 (2019).
31.
Eberly LA, Garg L, Yang L et al. Racial/ethnic and socioeconomic disparities in management of incident paroxysmal atrial fibrillation. JAMA Netw. Open 4(2), e210247 (2021).
32.
Patel N, Deshmukh A, Thakkar B et al. Gender, race, and health insurance status in patients undergoing catheter ablation for atrial fibrillation. Am. J. Cardiol. 117(7), 1117–1126 (2016).
33.
Shah RU, Freeman JV, Shilane D, Wang PJ, Go AS, Hlatky MA. Procedural complications, rehospitalizations, and repeat procedures after catheter ablation for atrial fibrillation. J. Am. Coll. Cardiol. 59(2), 143–149 (2012).
Information & Authors
Information
Published In
Pages: 659 - 668
PubMed: 35535654
Copyright
© 2022 Johnson & Johnson. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 15 July 2021
Accepted: 19 April 2022
Published online: 10 May 2022
Keywords:
Topics
Authors
Funding Information
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Atrial fibrillation ablation with advanced radiofrequency catheter versus second-generation cryoballoon catheter. (2022) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2021-0170
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Pengcheng Zhao, Jie Yuan, Zhongyi Jin, Yuhan Zhao, Ting Zhang, Comparison of 3C4L and 2C3L radiofrequency ablation strategies for persistent atrial fibrillation: procedural profile and 2-year outcomes, Frontiers in Cardiovascular Medicine, 10.3389/fcvm.2025.1591569, 12, (2026).
- Alexandru I Costea, Rahul Khanna, Maximiliano Iglesias, Yiran Rong, Hospital readmissions following catheter ablation for atrial fibrillation with THERMOCOOL™ STSF/ THERMOCOOL™ ST catheter with CARTO™ 3 system versus TactiCath™ catheter with EnSite™ system, Journal of Comparative Effectiveness Research, 10.57264/cer-2024-0075, 14, 1, (2024).