Ospemifene versus local estrogen: adherence and costs in postmenopausal dyspareunia
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Objective was to compare adherence and persistence, as well as direct healthcare costs and utilization, of ospemifene to available local estrogen therapies (LETs). Patients & methods: This retrospective database study used integrated medical and pharmacy claims data from the IQVIA Real-World Data Adjudicated Claims – US Database. Results: Ospemifene patients had significantly greater adherence and persistence compared with the other nonring LETs. Ospemifene had the lowest mean outpatient costs of any of the LET cohorts, including the estradiol vaginal ring. Total all-cause healthcare costs were also significantly less for ospemifene patients compared with all other LETs.
In the USA, the average age of menopause is 51 years and it can begin in women during their 40s [1,2]. With the onset of menopause comes a reduction in estrogen levels, which can result in genitourinary syndrome of menopause exhibiting a variety of symptoms including vulvar and vaginal atrophy (VVA) [3–5]. In the USA, there are approximately 64 million postmenopausal women and up to 50% may suffer from VVA symptoms [6]. VVA is sustained, continuous and does not resolve with time or without treatment. Without medical care, VVA symptoms adversely influence women’s quality of life, including sexual relations and emotional health [7]. VVA is distinguished by a range of specific patient complaints including vaginal dryness, inflammation, discomfort, sharp pain and discharge, recurrent urinary tract infections, dysuria and dyspareunia [3–5]. Dyspareunia, a condition characterized by persistent or frequent genital pain associated with sex, is a widespread concern in postmenopausal women. Symptoms of VVA can be severe enough to interfere with a woman’s ability to have pain-free sexual activity [6]. A recent survey of postmenopausal women found that 59% reported painful intercourse [8]. Contributing to decreased quality of life, women with dyspareunia describe frustration, worry, anguish and reduced disposition [9,10].
A number of options are available for the treatment of VVA symptoms including dyspareunia. These range from OTC lubricant and moisturizers to prescription medications including vaginal estrogens (cream, tablets and ring), as well as ospemifene, an oral selective estrogen receptor modulator (SERM) [6]. However, despite the availability of these various treatment options, treatment adherence remains an issue as this condition may necessitate long-term therapy [8,11,12]. Adherence barriers for available medications include lack of immediate symptom improvement, confusion over proper dosage administration and inconvenience (e.g., messiness and leakiness), which may lead to suboptimal adherence and potential over or underdosing of the medication [12,13]. Also specific to vaginal rings, difficulty with insertion and removal has been reported [5,14]. Consistent with these reports, a 2017 survey of postmenopausal women (n = 1858) found adherence with the vaginal ring was not ideal as 57% reported using the ring only ‘as needed’ when labeling indicated the ring should be used for 90 days [8]. In an earlier 2013 survey of postmenopausal women (n = 3046), up to 44% stopped using at least one dyspareunia treatment due to dissatisfaction [15]. Furthermore, patients had concerns about treatment with local estrogen therapies (LETs) related to safety which was a reason either not to initiate treatment or to discontinue it. Finally, the cost of therapy was considered by physicians as presenting a barrier to treatment or cause of discontinuation [16].
In order to increase compliance to treatment, many providers include the patient in the decision-making process for selecting an appropriate therapy. Additionally, women may fail one or more of the treatments for VVA requiring consideration of another option by the healthcare provider. Thus, treatment modality selection depends on various factors including the severity of the symptoms, the effectiveness of therapy for the individual patient and patient preference. Since every patient is unique and responds to available treatment options differently with different side effects, treatment of dyspareunia and other VVA symptoms need be tailored to the specific patient’s needs [6].
Ospemifene is a third-generation SERM which was approved by the FDA in 2013 as an oral treatment for dyspareunia and in January 2019 for the treatment of moderate to severe vaginal dryness due to menopause [17]. Ospemifene can provide women relief from dyspareunia and vaginal dryness in as soon as 12 weeks [18–20]. The efficacy and safety of ospemifene on moderate to severe symptoms of VVA, specifically dyspareunia and vaginal dryness, were examined in four placebo-controlled clinical trials (three 12-week efficacy trials and one 52-week long-term safety trial). In the four placebo-controlled trials, a total of 1100 women received placebo and 1416 women received 60 mg ospemifene [17]. In the first and second clinical trial, the modified intent-to-treat population of women treated with ospemifene, when compared with placebo, demonstrated a statistically significant improvement in the moderate to severe most bothersome symptom (MBS) of dyspareunia (trial I, p = 0.0012 and trial II, p < 0.0001) [21,22]. The trials that evaluated the MBS of vaginal dryness, demonstrated a statistically significant improvement in the moderate to severe MBS of vaginal dryness (trial I, p = 0.0136 and trial III, p < 0.0001) [20]. Ospemifene has been evaluated in ten Phase II and III trials (N = 2209) with 847 subjects who had up to 52 weeks of exposure. The adverse reactions reported more commonly in the ospemifene treatment group (60 mg once daily) and at frequency ≥1.0% were, hot flush (12.2%) and vaginal discharge (6%), muscle spasms (4.5%), headaches (2.8%), hyperhidrosis (2.5%), vaginal hemorrhage (1.3%), night sweats (1.2%) [20].
Prior to the availability of ospemifene, only LETs were available and frequently used to treat symptoms of VVA, including dyspareunia. However, not all LETs are specifically approved for dyspareunia. In addition to ospemifene, conjugated estrogen cream [23] and estradiol vaginal inserts [24] are specifically indicated for dyspareunia, whereas estradiol cream [25] and the estradiol vaginal ring [26] are not. This study is the first to examine healthcare costs, treatment adherence and persistence using real-world treatment data for VVA based on common treatments administered (e.g., ospemifene, available LETs), regardless of FDA labeling.
Patients & methods
Data source
This study used integrated medical and pharmacy claims data from the IQVIA Real-World Data Adjudicated Claims – US Database. The data are representative of the national, commercially insured population in terms of age and gender. The database includes both inpatient and outpatient diagnoses and procedures, in addition to both retail and mail order prescription records. Available data on prescription records include the National Drug Code and the Generic Product Identification code, as well as the quantity of the medication dispensed. Amounts charged by providers and amounts allowed and paid by health plans are available for all services rendered, including the dates of service for all claims. Additional data elements include demographic variables (e.g., age, gender and geographic region), product type (e.g., health maintenance organization, preferred provider organization), payer type (e.g., commercial, self-pay), provider specialty, and start and stop dates for plan enrollment.
Patient selection & inclusion criteria
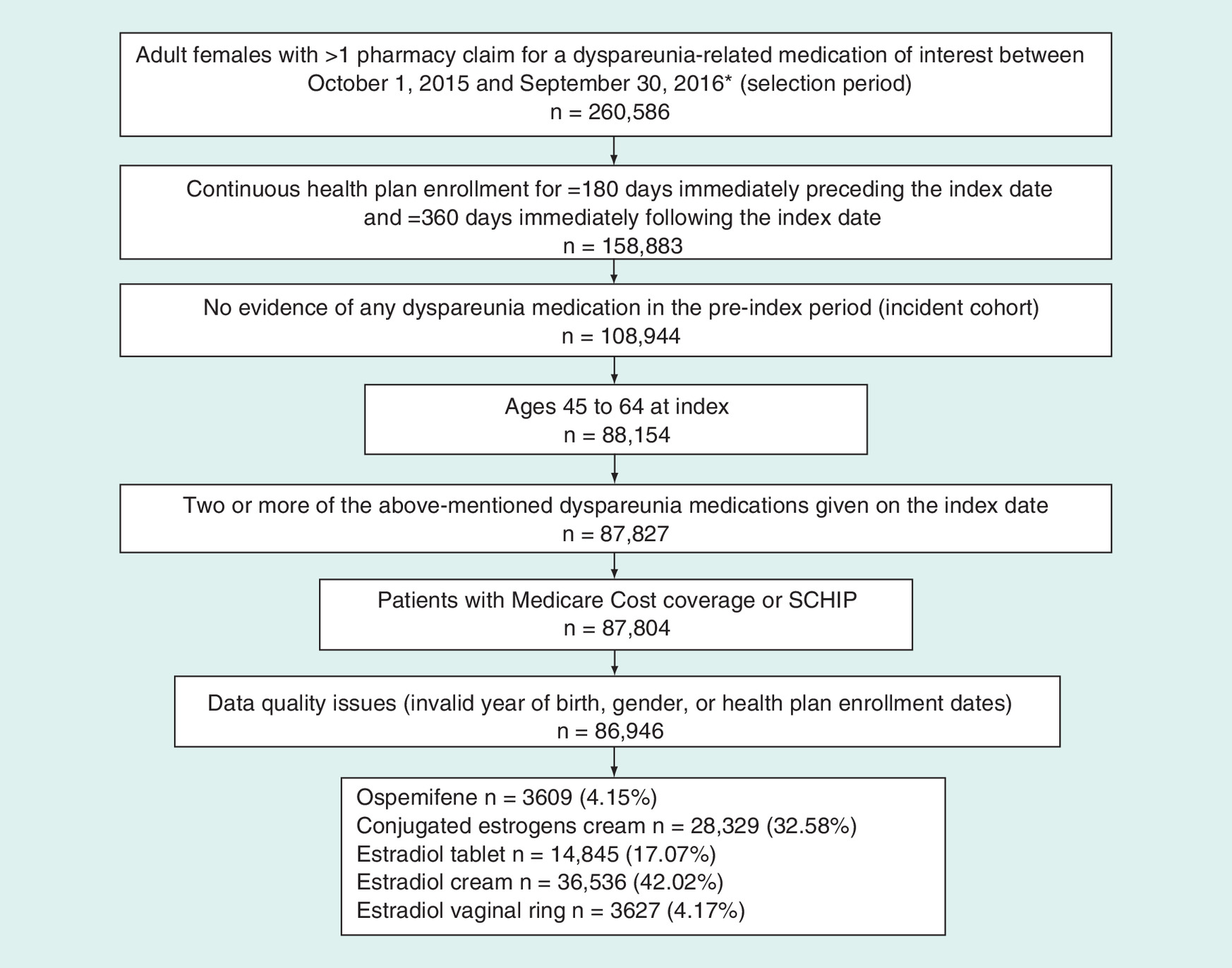
A cohort of patients between 1 October 2015 and 30 September 2016 (selection window) were identified for analysis applying the following criteria: ≥1 pharmacy claim for a dyspareunia-related medication of interest (e.g., ospemifene, conjugated estrogens and estradiol); continuous health plan enrollment for ≥180 days immediately preceding the index date (preindex period, used to report baseline demographic and clinical characteristics) and ≥360 days immediately following the index date (postindex period, used for outcome measurement); at least one medical claim with a diagnosis code of menopause or vulvovaginal atrophy during the preindex period; no evidence of any dyspareunia medication in the preindex period (incident cohort) and aged 45–64 at index. Patients were excluded from the study sample if: at least two of the earlier-mentioned dyspareunia medications of interest were given on the index date (n = 327); patients had Medicare cost coverage or state children’s health insurance program (n = 23); or data quality issues were found, such as invalid year of birth, gender or health plan enrollment dates (n = 858) (Figure 1).
Cohorts of interest
For patients meeting the above-mentioned inclusion/exclusion criteria, five medication-based cohorts were identified for outcomes comparison based on FDA approval for the same/similar indication at the time of the sampling:
•
Ospemifene tablet
•
Conjugated estrogen cream
•
Estradiol vaginal insert
•
Estradiol cream
•
Estradiol vaginal ring
Adherence & persistence
Adherence was calculated using the proportion of days covered (PDC) over the fixed 12-month postindex period, capped at 100%. The numerator was the total number of days supplied for a patient’s index dyspareunia therapy, while the denominator was 360 days, the total number of days in the required follow-up period. Claims extending beyond day 360 were prorated to include only the portion of days’ supply captured within this 12-month window. Additionally, if a patient refilled a prescription early, any days ‘double counting’, or overlapping, from the early refill were counted only once. The number and proportion of patients considered adherent for the full follow-up period (PDC ≥80%) were collected and reported. Clinical evidence supports the use of the 80% threshold to measure adherence [27].
Persistence was calculated based on the time from index dyspareunia therapy initiation until: the first observed gap (measured using a default refill grace period equal to 1.5-times the days’ supply of the previous prescription) in medication possession during the follow-up period (discontinuation); therapy switch (defined as evidence of a prescription fill for another dyspareunia-related medication, other than the index therapy, within 30 days before or after the discontinuation of the index therapy) or the end of patient follow-up at 12 months.
Healthcare resource utilization & costs
For each of the medication cohorts, both all-cause and dyspareunia-related healthcare resource utilization were measured and reported over the 12-month postindex period dyspareunia-related utilization was defined as all medical claims with a diagnosis code of dyspareunia, as well as all pharmacy claims for any dyspareunia-related medication.
Total preindex costs were calculated, combining both medical and pharmacy costs. For all medication cohorts, total all-cause healthcare costs, including pharmacy, outpatient and inpatient costs, were captured and reported over the 12-month postindex period. Pharmacy component costs included costs associated with the index medications. Costs were calculated on a per-patient basis and averaged across the cohort. Only direct healthcare costs for services covered by the patient’s insurance benefit were reported, using the allowed amount on the claim, representing the contracted reimbursable amount for covered medical services or supplies that the health plan agrees to pay to service providers. Costs were converted to 2017 US dollars using the medical component of the Consumer Price Index. Similarly, dyspareunia-related healthcare costs were analyzed and reported over the 12-month postindex period.
Comorbidities
Statistical analysis
For all univariate measures reported, p values using Pearson’s χ2 test (for categorical variables) and the Wilcoxon rank-sum test (for continuous variables) were generated to evaluate differences in outcomes between the index medication cohorts. Two logistic regression models were constructed to identify predictors of both persistence and adherence to the index therapy. A generalized linear model (GLM) was used to evaluate differences in total all-cause costs over the postindex period among patients in ospemifene cohort compared with patients in the LET cohorts. Results for the GLM model were presented in terms of cost ratios (exponentiated β-coefficients) along with corresponding 95% CIs. Independent variables in the models included all baseline demographic and clinical characteristics that were found to be significantly different between cohorts, as well as a stepwise model-building approach (p < 0.10 for inclusion and retention). Collinearity among the variables of interest was evaluated during model development.
Results
Sample size
Following the application of the inclusion and exclusion criteria, the sample included 86,946 patients. The categorization by cohort was ospemifene (n = 3609; 4.15%), conjugated estrogens cream (n = 28,329; 32.58%), estradiol vaginal insert (n = 14,845; 17.07%), estradiol cream (n = 36,536; 42.02%) and estradiol vaginal ring (n = 3627; 4.17%). The median age across the five cohorts was 57 years.
Baseline patient characteristics
The majority of patients had insurance coverage via a preferred provider organization, ranging from a low of 75.44% in the estrogens cream cohort to 89.53% in the ospemifene cohort (p < 0.0001). Most of the patients across the sample (>74%) had a Charlson Comorbidity Index score of 0 (p < 0.0001), though the average Charlson Comorbidity Index was different among the cohorts. The comorbidities of interest were statistically different across all cohorts for depression, sexual dysfunction, cardiovascular disease, stroke, cancer, vasomotor symptoms and sleep disturbances. Across the five cohorts, an average of 30.50% were taking antidepressants and 29.80% were on an antihypertensive medication; the proportions between cohorts were different (both p < 0.0001). Total mean preindex costs were lowest for ospemifene ($4794.12) compared with the other cohorts ($5636.10; $5743.59; $5637.52; $5575.46 for conjugated estrogens cream, estradiol vaginal insert, estradiol cream and estradiol vaginal ring, respectively [p = 0.0071]) (Table 1).
| Characteristics | Ospemifene | Conjugated estrogens cream | Estradiol vaginal insert | Estradiol cream | Estradiol vaginal ring | p-value | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| (N = 3609) | % | (N = 28,329) | % | (N = 14,845) | % | (N = 36,536) | % | (N = 3627) | % | ||
| Age | |||||||||||
| – Mean | 56.42 | 56.74 | 56.89 | 56.65 | 56.82 | <0.0001 | |||||
| – SD | 4.43 | 4.66 | 4.56 | 4.67 | 4.52 | ||||||
| – Median | 57 | 57 | 57 | 57 | 57 | <0.0001 | |||||
| Age group (n, %) | <0.0001 | ||||||||||
| – 45–49 | 267 | 7.40 | 2284 | 8.06 | 1049 | 7.07 | 3078 | 8.42 | 251 | 6.92 | |
| – 50–54 | 907 | 25.13 | 6534 | 23.06 | 3341 | 22.51 | 8446 | 23.12 | 825 | 22.75 | |
| – 55–59 | 1437 | 39.82 | 10,274 | 36.27 | 5540 | 37.32 | 13,434 | 36.77 | 1411 | 38.90 | |
| – 60–64 | 998 | 27.65 | 9237 | 32.61 | 4915 | 33.11 | 11,578 | 31.69 | 1140 | 31.43 | |
| Health plan type (n, %) | <0.0001 | ||||||||||
| – Consumer-directed healthcare | 0 | 0.00 | 47 | 0.17 | 34 | 0.23 | 81 | 0.22 | 9 | 0.25 | |
| – Health maintenance organization | 138 | 3.82 | 3430 | 12.11 | 1562 | 10.52 | 3666 | 10.03 | 327 | 9.02 | |
| – Indemnity | 140 | 3.88 | 1805 | 6.37 | 462 | 3.11 | 882 | 2.41 | 158 | 4.36 | |
| – Point of service | 87 | 2.41 | 1521 | 5.37 | 668 | 4.50 | 1388 | 3.80 | 187 | 5.16 | |
| – Preferred provider organization | 3231 | 89.53 | 21,372 | 75.44 | 11,988 | 80.75 | 30,275 | 82.86 | 2898 | 79.90 | |
| – Other/unknown | 13 | 0.36 | 154 | 0.54 | 131 | 0.88 | 244 | 0.67 | 48 | 1.32 | |
| Payer type (n, %) | <0.0001 | ||||||||||
| – Commercial | 2158 | 59.79 | 16,538 | 58.38 | 9241 | 62.25 | 22,908 | 62.70 | 2458 | 67.77 | |
| – Medicaid | 4 | 0.11 | 1407 | 4.97 | 147 | 0.99 | 768 | 2.10 | 13 | 0.36 | |
| – Medicare risk | 0 | 0.00 | 62 | 0.22 | 20 | 0.13 | 75 | 0.21 | 3 | 0.08 | |
| – Self-insured | 1434 | 39.73 | 10,150 | 35.83 | 5294 | 35.66 | 12,504 | 34.22 | 1103 | 30.41 | |
| – Unknown | 13 | 0.36 | 172 | 0.61 | 143 | 0.96 | 281 | 0.77 | 50 | 1.38 | |
| Charlson comorbidity index (n, %) | |||||||||||
| – Mean | 0.38 | 0.43 | 0.42 | 0.41 | 0.37 | 0.0002 | |||||
| – SD | 0.81 | 0.93 | 0.93 | 0.91 | 0.87 | ||||||
| – Median | 0 | 0 | 0 | 0 | 0 | ||||||
| – 0 | 2759 | 76.45 | 21,123 | 74.56 | 11,264 | 75.88 | 27,533 | 75.36 | 2830 | 78.03 | <0.0001 |
| – 1 | 504 | 13.97 | 4175 | 14.74 | 1914 | 12.89 | 5148 | 14.09 | 423 | 11.66 | |
| – 2 | 250 | 6.93 | 2045 | 7.22 | 1176 | 7.92 | 2697 | 7.38 | 282 | 7.78 | |
| – 3+ | 96 | 2.66 | 986 | 3.48 | 491 | 3.31 | 1158 | 3.17 | 92 | 2.54 | |
| Total preindex costs | |||||||||||
| – Mean | 4794.12 | 5636.10 | 57,43.58 | 5637.52 | 5575.46 | 0.0071 | |||||
| – SD | 10,587.07 | 14,097.88 | 15,643.05 | 13,361.08 | 12,912.07 | ||||||
| – Median | 1754.60 | 1902.36 | 1975.10 | 1977.06 | 2006.87 | <0.0001 | |||||
| Specific comorbidities of interest (n, %) | |||||||||||
| – Depression (including major depressive disorder) | 399.00 | 11.06 | 3179.00 | 11.22 | 1676.00 | 11.29 | 3903.00 | 10.68 | 461.00 | 12.71 | 0.002 |
| – Sexual dysfunction | 76.00 | 2.11 | 356.00 | 1.26 | 268.00 | 1.81 | 610.00 | 1.67 | 85.00 | 2.34 | <0.0001 |
| – Cardiovascular disease | 108.00 | 2.99 | 931.00 | 3.29 | 385.00 | 2.59 | 1052.00 | 2.88 | 63.00 | 1.74 | <0.0001 |
| – Stroke | 18.00 | 0.50 | 269.00 | 0.95 | 129.00 | 0.87 | 324.00 | 0.89 | 24.00 | 0.66 | 0.0474 |
| – Deep vein thrombosis | 6.00 | 0.17 | 88.00 | 0.31 | 34.00 | 0.23 | 119.00 | 0.33 | 9.00 | 0.25 | 0.2054 |
| – Cancer | 168.00 | 4.66 | 1418.00 | 5.01 | 1047.00 | 7.05 | 2121.00 | 5.81 | 262.00 | 7.22 | <0.0001 |
| – Dementia | 3.00 | 0.08 | 20.00 | 0.07 | 6.00 | 0.04 | 27.00 | 0.07 | 3.00 | 0.08 | 0.714 |
| – Vasomotor symptoms/hot flashes | 330.00 | 9.14 | 1950.00 | 6.88 | 1253.00 | 8.44 | 3178.00 | 8.70 | 397.00 | 10.95 | <0.0001 |
| – Sleep disturbances | 304.00 | 8.42 | 2678.00 | 9.45 | 1310.00 | 8.82 | 3380.00 | 9.25 | 386.00 | 10.64 | 0.0032 |
| – Migraine | 177.00 | 4.90 | 1238.00 | 4.37 | 669.00 | 4.51 | 1677.00 | 4.59 | 181.00 | 4.99 | 0.2937 |
| – Anxiety | 376.00 | 10.42 | 3225.00 | 11.38 | 1592.00 | 10.72 | 4045.00 | 11.07 | 393.00 | 10.84 | 0.1716 |
| Specific medications of interest (n, %) | |||||||||||
| – Antidepressants | 1210.00 | 33.53 | 8292.00 | 29.27 | 4297.00 | 28.95 | 10,294.00 | 28.17 | 1181.00 | 32.56 | <0.0001 |
| – Antihypertensives | 1153.00 | 31.95 | 9474.00 | 33.44 | 4209.00 | 28.35 | 11,088.00 | 30.35 | 903.00 | 24.90 | <0.0001 |
SD: Standard deviation.
Adherence & persistence
Over the 12-month postindex period, ospemifene patients exhibited the highest adherence among nonring medications, with a mean PDC of 0.392 compared with the other cohorts (0.201, 0.321, 0.217, 0.527 for conjugated estrogen cream, estradiol vaginal insert, estradiol cream, estradiol vaginal ring, respectively; p < 0.0001). Similarly, persistence for ospemifene patients was greater than that for the other cohorts, except for the estradiol vaginal ring (22.83% for ospemifene compared with 4.99, 16.40, 6.27 and 43.56% for conjugated estrogen cream, estradiol vaginal insert, estradiol cream, estradiol ring, respectively; p < 0.0001). While rates of discontinuation were high, ospemifene had the lowest rate of discontinuation among the nonring treatments (77.1% for ospemifene vs 95.01, 83.6, 93.73 and 56.44%; (conjugated estrogen cream, estradiol vaginal insert, estradiol cream, estradiol ring, respectively; p < 0.0001) (Table 2).
| Ospemifene | Conjugated estrogens cream | Estradiol vaginal insert | Estradiol cream | Estradiol vaginal ring | p-value | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Measure | (N = 3609) | % | (N = 28,329) | % | (N = 14,845) | % | (N = 36,536) | % | (N = 3627) | % | |
| PDC (100% max) | |||||||||||
| – <20% | 1281 | 35.49 | 18,018 | 63.60 | 6233 | 41.99 | 21,243 | 58.14 | 104 | 2.87 | <0.0001 |
| – 20–39% | 829 | 22.97 | 7027 | 24.80 | 3984 | 26.84 | 10,240 | 28.03 | 1437 | 39.62 | <0.0001 |
| – 40–59% | 563 | 15.60 | 2199 | 7.76 | 2051 | 13.82 | 3198 | 8.75 | 665 | 18.33 | <0.0001 |
| – 60–79% | 397 | 11.00 | 722 | 2.55 | 1399 | 9.42 | 1115 | 3.05 | 536 | 14.78 | <0.0001 |
| – >80% | 539 | 14.93 | 363 | 1.28 | 1178 | 7.94 | 740 | 2.03 | 885 | 24.40 | <0.0001 |
| – Mean | 0.392 | 0.201 | 0.321 | 0.217 | 0.527 | <0.0001 | |||||
| – SD | 0.294 | 0.168 | 0.260 | 0.182 | 0.285 | ||||||
| – Median | 0.250 | 0.167 | 0.233 | 0.167 | 0.500 | <0.0001 | |||||
| Total days’ supply | |||||||||||
| – Mean | 141 | 72 | 115 | 78 | 190 | <0.0001 | |||||
| – SD | 106 | 60 | 94 | 65 | 103 | ||||||
| – Median | 90 | 60 | 84 | 60 | 180 | <0.0001 | |||||
| Total patients completely persistent during follow-up period (n, %) | 824 | 22.83 | 1413 | 4.99 | 2435 | 16.40 | 2291 | 6.27 | 1580 | 43.56 | <0.0001 |
| Persistent days for all patients | |||||||||||
| – Mean | 151 | 67 | 115 | 73 | 213 | <0.0001 | |||||
| – SD | 130 | 78 | 120 | 85 | 133 | ||||||
| – Median | 90 | 30 | 64 | 30 | 177 | <0.0001 | |||||
| Number of prescriptions per patient (n, %) | |||||||||||
| – 1 | 1490 | 41.29 | 22,916 | 80.89 | 8468 | 57.04 | 29,289 | 80.16 | 1663 | 45.85 | <0.0001 |
| – 2 | 526 | 14.57 | 3278 | 11.57 | 2334 | 15.72 | 4147 | 11.35 | 508 | 14.01 | |
| – 3+ | 1593 | 44.14 | 2135 | 7.54 | 4043 | 27.23 | 3100 | 8.48 | 1456 | 40.14 | |
PDC: Proportion of days covered; SD: Standard deviation.
Healthcare utilization & costs
All-cause total mean pharmacy utilization (number of pharmacy prescriptions) was highest for the ospemifene cohort (32.12), compared with conjugated estrogens cream (31.85), estradiol vaginal insert (28.79), estradiol cream (29.81) and estradiol vaginal ring (27.76; p < 0.0001). The ospemifene cohort had the lowest total mean outpatient services (number of visits) (38.04), compared with the other cohorts (41.57, 42.19, 42.48, 40.06, conjugated estrogen cream, estradiol vaginal insert, estradiol cream, estradiol ring, respectively (p < 0.0001). Mean hospital admissions were different for all cohorts, ranging from a low of 0.05 in the estradiol vaginal ring to a high of 0.07 for conjugated estrogens cream (median = 0 for all cohorts; p = 0.0084).
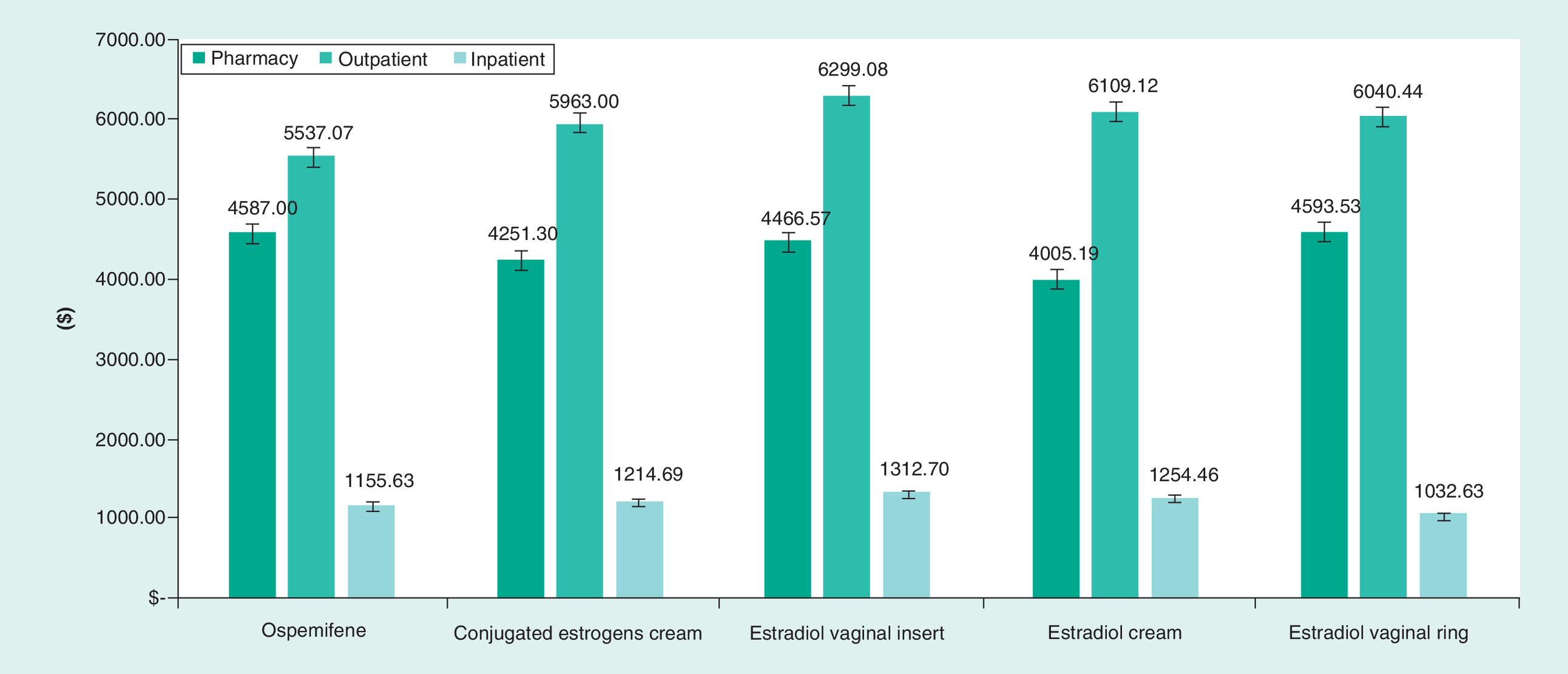
Total all-cause mean pharmacy costs (not limited to pharmacy costs associated with postmenopausal symptoms) were greatest for the estradiol vaginal ring ($4593.53) compared with the other cohorts (ospemifene $4587.17, estradiol vaginal insert $4466.57, conjugated estrogen cream $4251.30, estradiol cream $4005.19; p = 0.0003). All other medications accounted for the highest pharmacy costs in all cohorts (no statistical difference detected). Ospemifene had the lowest total mean outpatient costs ($5537.07) while estradiol vaginal inserts had the highest ($6299.08; p = 0.0011). All-cause total outpatient costs were lowest in the ospemifene cohort ($5537.07) when measured against the other cohorts (conjugated estrogens cream [$5963.00], estradiol vaginal insert [$6299.08], estradiol cream [$6109.12] and estradiol vaginal ring [$6040.44]; p < 0.0011). Consequently, total all-cause healthcare costs were significantly less for ospemifene patients ($11,745.15) compared with all other LETs (p = 0.0098) (Figure 2).
Predictors of persistence & adherence
In addition to the index medication, both patient age and payer type were significant predictors of persistence and adherence in the results of logistic regression modeling. Compared with the ospemifene cohort (reference group), only the estradiol vaginal ring demonstrated significantly higher persistence and adherence. The following odds ratios (ORs) and 95% CIs were reported for persistence: conjugated estrogens cream (OR: 0.170, 95% CI: 0.155–0.187), estradiol vaginal insert (OR: 0.628, 95% CI: 0.573–0.687), estradiol cream (OR: 0.217, 95% CI: 0.199–0.238) and estradiol vaginal ring (OR: 2.446, 95% CI: 2.205–2.713; p < 0.0001) (Table 3). When predicting adherence, the following ORs and 95% CIs were reported: conjugated estrogens cream (0.069, 95% CI: 0.060–0.079), estradiol vaginal insert (OR: 0.462, 95% CI: 0.414–0.517), estradiol cream (OR: 0.113, 95% CI: 0.100–0.127) and estradiol vaginal ring (OR: 1.710, 95% CI: 1.514–1.933; p < 0.0001) (Table 4).
| Variable | Odds ratio | Lower limit (95% CI) | Upper limit (95% CI) | p-value |
|---|---|---|---|---|
| Cohort (reference: ospemifene) | ||||
| – Conjugated estrogens cream | 0.170 | 0.155 | 0.187 | <0.0001 |
| – Estradiol vaginal insert | 0.628 | 0.573 | 0.687 | <0.0001 |
| – Estradiol cream | 0.217 | 0.199 | 0.238 | <0.0001 |
| – Estradiol vaginal ring | 2.446 | 2.205 | 2.713 | <0.0001 |
| Age group (reference: 60–64) | ||||
| – 45–49 | 0.623 | 0.561 | 0.691 | <0.0001 |
| – 50–54 | 0.764 | 0.716 | 0.815 | <0.0001 |
| – 55–59 | 0.909 | 0.861 | 0.960 | 0.0007 |
| Payer type: (reference: commercial) | ||||
| – Medicaid | 0.761 | 0.629 | 0.922 | 0.0052 |
| – Medicare risk | 2.252 | 1.464 | 3.465 | 0.0002 |
| – Self-insured | 0.944 | 0.898 | 0.992 | 0.0233 |
| – Unknown | 1.178 | 0.924 | 1.503 | 0.1859 |
| Specific comorbidities of interest (reference: no) | ||||
| – Cardiovascular disease | 0.874 | 0.752 | 1.015 | 0.0778 |
| Variable | Odds ratio | Lower limit (95% CI) | Upper limit (95% CI) | p-value |
|---|---|---|---|---|
| Cohort (reference: ospemifene) | ||||
| – Conjugated estrogens cream | 0.069 | 0.060 | 0.079 | <0.0001 |
| – Estradiol vaginal insert | 0.462 | 0.414 | 0.517 | <0.0001 |
| – Estradiol cream | 0.113 | 0.100 | 0.127 | <0.0001 |
| – Estradiol vaginal ring | 1.710 | 1.514 | 1.933 | <0.0001 |
| Age group (reference: 60–64) | ||||
| – 45–49 | 0.811 | 0.700 | 0.940 | 0.0054 |
| – 50–54 | 0.902 | 0.821 | 0.992 | 0.0338 |
| – 55–59 | 0.965 | 0.889 | 1.047 | 0.3907 |
| Payer type: (reference: commercial) | ||||
| – Medicaid | 1.508 | 1.176 | 1.933 | 0.0012 |
| – Medicare risk | 2.635 | 1.420 | 4.891 | 0.0021 |
| – Self-insured | 0.966 | 0.898 | 1.039 | 0.3558 |
| – Unknown | 1.002 | 0.703 | 1.428 | 0.9910 |
| Specific medications of interest (reference: no) | ||||
| – Antihypertensives | 1.083 | 1.005 | 1.168 | 0.0370 |
Adjusted cost estimate
After adjusting for differences in baseline characteristics, results of the GLM model indicated that patients in the estradiol tablet cohort had significantly higher total costs compared with patients in the ospemifene cohort (cost ratio 1.048; 95% CI: 1.008–1.090; p = 0.0175). Compared with the ospemifene cohort (reference group), no other medication demonstrated significantly different total costs.
Discussion
This study is the first to examine persistence, adherence and costs of ospemifene compared with other available LETs in the USA. Overall healthcare utilization and costs were lower for ospemifene than all other available LET treatments, while adherence and persistence with ospemifene was highest among the nonring cohorts.
A number of over-the-counter and government-approved prescription therapies available in the USA demonstrate effectiveness, depending on the severity of VVA symptoms. Suggested initial therapy is local, nonhormonal and includes vaginal lubricants and moisturizers [30]. However, few clinical studies have been conducted on the efficacy and safety of these products, some of which containing flavors, solvents or preservatives, and have warming properties [6]. For women who do not respond to these local, nonhormonal therapies, low dose local vaginal estrogen treatments are available in the form of cream, tablet or ring, and have exhibited efficacy for VVA symptoms with minimal systemic absorption [6]. While local delivery of estrogen is preferred, women with complaints additional to VVA, such as vasomotor symptoms, systemic hormone therapy is an effective treatment with the risk/benefit individualized for every patient [31]. Among women using oral estrogen therapy, 75% report favorable response for relief of VVA symptoms [6]. The only oral nonhormonal therapy approved for women with vaginal dyspareunia and/or dryness is the SERM, ospemifene [6,17]. This study identifies five medication-based cohorts which were chosen based on FDA approval for the same/similar indication at the time of the sampling. Of note, in 2003, the FDA changed the approval process for this category of medication; the current ‘Estrogen and Estrogen/Progestin Drug Products to Treat Vasomotor Symptoms and VVA Symptom’ include the MBS of VVA which was not the case before 2003 [30]. Therefore, at the time of this sampling, the included medication cohorts of interest do not have the exact same indications, some include general symptoms of VVA, others such as ospemifene, were only indicated for dyspareunia, a symptom of VVA.
In 2002, after many years of popularity of HRT usage, the clinical landscape shifted with the first results from the randomized comparison of estrogen and progestin with placebo in the Women's Health Initiative (WHI) data which showed that HRT was actually associated with increasing rates of cardiovascular disease, dementia and hormone dependent cancer such endometrial cancer and breast cancer [32]. Physicians were conflicted about the WHI results and its implications. Current LET formulations include vaginal creams, vaginal rings and vaginally administered tablets. Of note, neither LET regimens nor SERMs were studied in the WHI [33], and there is no evidence to support a risk for LET or ospemifene similar to that for systemic estrogen therapy [32,34].
Based on the study’s findings, ospemifene patients demonstrated significantly greater adherence and persistence when compared with other nonring LETs (p < 0.0001). Ospemifene also had significantly lower mean outpatient costs of any of the LET cohorts, including the estradiol vaginal ring (p = 0.0011). Total healthcare costs were lower for ospemifene patients compared with all other LETs, including the estradiol vaginal ring, though after adjusting for baseline characteristics the effect is limited to ospemifene compared with estradiol tablets. Given the delivery method of estradiol via the vaginal ring, higher persistence and adherence is expected (e.g., longer period of time between required refills, no requirement for oral dosing/administration); a comparison of healthcare utilization and costs among all available LETs provides an additional assessment of the available dyspareunia treatment options. It should be noted that total healthcare costs for the ospemifene cohort were lower compared with other cohorts both before and after initial treatment, indicating that there may be inherent differences in the medication cohorts not measured in this analysis such as income or coverage differences.
Patient preference plays a significant role in the management of dyspareunia and adherence to treatment [6,35]. When a patient is not satisfied with their medication, their adherence to that medication is lower. Patient preference is also directly linked to the method of administration [12]. In the recent EMPOWER survey of postmenopausal women, the most satisfied patients were users of an oral medication (67%), while the least satisfied were utilizers of the vaginal ring (33%) [8]. Via a survey, Minkin et al. found that postmenopausal women using vaginal rings delayed refilling their prescription for several reasons: difficult insertion and removal, they and/or their sexual partner could feel the ring, concerns about infection including hygiene and cleanliness, or because the ring does not contain the lowest effective dose of estrogen available [22]. Among women who expressed a preference for treatment administration, the REVIVE (REal Women’s VIews of Treatment Options for Menopausal Vaginal ChangEs) survey found that 55% preferred an oral formulation for relief of their postmenopausal symptoms before an oral treatment was available in the USA [14]. These results are consistent with the findings of this study regarding nonring treatments.
Limitations
There are several limitations inherent in using administrative claims data for real-world studies, which should be considered when evaluating this study’s findings. As with any such analyses, it needs to be stated that claims are collected for the purposes of payment resolution rather than for research. In addition, any claims analysis is limited by the reported codes, which can include coding mistakes such as undercoding [36]. The adherence data only capture whether patients filled their prescription, not whether they actually took the prescription. The prevalence and availability of novel therapies within the selected study inclusion period could bias categorization of patients into specific medication cohorts, given that the first prescription of interest was selected as index date. The impact of patients’ out-of-pocket expenses for specific medications of interest was not studied. The data and the chosen payer perspective limited the cost analysis portion of this study to direct cost estimation. As dyspareunia is associated with considerable indirect costs [37,38], the total healthcare costs presented here inherently underestimate the overall cost of treatment. Claims data permit focus on commercial managed care patients, but the results may not be generalizable to patients with other types of healthcare plans, such as traditional Medicare.
Conclusion
This study reflects real world use of treatments of dyspareunia a symptom of VVA in postmenopausal women. Ospemifene patients had significantly greater adherence and persistence compared with the other nonring LETs: conjugated estrogen cream, estradiol vaginal insert and estradiol cream (p < 0.0001). The once every 3 months estradiol vaginal ring group exhibited higher adherence and persistence compared with daily use products. Future studies on adherence and persistence will provide further understanding on how to improve individualization of treatment of VVA symptoms.
•
This study is the first to examine persistence, adherence and healthcare utilization and costs of ospemifene compared with other available local estrogen therapies (LETs) in the USA.
•
Ospemifene patients demonstrated significantly greater adherence and persistence when compared with other nonring LETs (p < 0.0001).
•
Ospemifene also had significantly lower mean outpatient costs of any of the LET cohorts, including the estradiol vaginal ring (p = 0.0011).
•
Total healthcare costs were lower for ospemifene patients compared with all other LETs, including the estradiol vaginal ring.
•
Given the delivery method of estradiol via the vaginal ring, higher persistence and adherence is likely expected (e.g., longer period of time between required refills, no requirement for oral dosing/administration); a comparison of healthcare utilization and costs among all available LETs provides an additional assessment of the available dyspareunia treatment options.
Financial & competing interests disclosure
This study was funded by Duchesnay. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Medical writing support was funded by Duchesnay.
References
1.
The North American Menopause Society. Menopause 101: a primer for the perimenopausal (2018). https://www.menopause.org/for-women/menopauseflashes/menopause-symptoms-and-treatments/menopause-101-a-primer-for-the-perimenopausal
2.
Mayo Clinic. Menopause (2018). https://www.mayoclinic.org/diseases-conditions/menopause/symptoms-causes/syc-20353397
3.
Mac Bride MB, Rhodes DJ, Shuster LT. Vulvovaginal atrophy. Mayo Clin. Proc. 85(1), 87–94 (2010).
4.
Lev-Sagie A. Vulvar and vaginal atrophy: physiology, clinical presentation, and treatment considerations. Clin. Obstet. Gynecol. 58(3), 476–491 (2015).
5.
Kingsberg SA, Kroll R, Goldstein I et al. Patient acceptability and satisfaction with a low-dose solubilized vaginal estradiol softgel capsule, TX-004HR. Menopause 24(8), 894–899 (2017).
6.
Management of symptomatic vulvovaginal atrophy: 2013 position statement of The North American Menopause Society. Menopause 20(9), 888–902 (2013).
7.
Wysocki S, Kingsberg S, Krychman M. Management of vaginal atrophy: implications from the REVIVE survey. Clin. Med. Insights Reprod. Health 8, 23–30 (2014).
8.
Kingsberg SA, Krychman M, Graham S, Bernick B, Mirkin S. The Women’s EMPOWER Survey: identifying women’s perceptions on vulvar and vaginal atrophy and its treatment. J. Sex. Med. 14(3), 413–424 (2017).
9.
Sadownik LA, Smith KB, Hui A, Brotto LA. The impact of a woman’s dyspareunia and its treatment on her intimate partner: a qualitative analysis. J. Sex Marital Ther. 43(6), 529–542 (2017).
10.
Parish SJ, Nappi RE, Krychman ML et al. Impact of vulvovaginal health on postmenopausal women: a review of surveys on symptoms of vulvovaginal atrophy. Int. J. Womens Health 5, 437–447 (2013).
11.
Faubion SS, Rullo JE. Sexual dysfunction in women: a practical approach. Am. Fam. Physician 92(4), 281–288 (2015).
12.
Mattsson LA, Ericsson A, Bogelund M, Maamari R. Women’s preferences toward attributes of local estrogen therapy for the treatment of vaginal atrophy. Maturitas 74(3), 259–263 (2013).
13.
Portman D, Shulman L, Yeaw J et al. One-year treatment persistence with local estrogen therapy in postmenopausal women diagnosed as having vaginal atrophy. Menopause 22(11), 1197–1203 (2015).
14.
LePage K, Selk A. What do patients want? A needs assessment of vulvodynia patients attending a vulvar diseases clinic. Sex. Med. 4(4), e242–e248 (2016).
15.
Kingsberg SA, Wysocki S, Magnus L, Krychman ML. Vulvar and vaginal atrophy in postmenopausal women: findings from the REVIVE (REal Women's VIews of Treatment Options for Menopausal Vaginal ChangEs) survey. J. Sex. Med. 10(7), 1790–1799 (2013).
16.
Kingsberg SA, Larkin L, Krychman M, Parish SJ, Bernick B, Mirkin S. WISDOM survey: attitudes and behaviors of physicians toward vulvar and vaginal atrophy (VVA) treatment in women including those with breast cancer history. Menopause 26(2), 124–131 (2019).
17.
Duchesnay. Ospemifene full prescribing information (2019). https://files.duchesnay.com/duchesnay-usa/osphena/osphena-prescribing-information.pdf
18.
Shin JJ, Kim SK, Lee JR, Suh CS. Ospemifene: a novel option for the treatment of vulvovaginal atrophy. J. Menopausal Med. 23(2), 79–84 (2017).
19.
Nappi RE, Panay N, Bruyniks N, Castelo-Branco C, De Villiers TJ, Simon JA. The clinical relevance of the effect of ospemifene on symptoms of vulvar and vaginal atrophy. Climacteric 18(2), 233–240 (2015).
20.
Archer D, Goldstein S, Simon JA et al. Efficacy and safety of ospemifene in postmenopausal women with moderate-to-severe vaginal dryness: a Phase III, randomized, double-blind, placebo-controlled, multicenter trial. Menopause 26(6), 611–621 (2019).
21.
Bachmann GA, Komi JO. Ospemifene effectively treats vulvovaginal atrophy in postmenopausal women: results from a pivotal Phase III study. Menopause 17(3), 480–486 (2010).
22.
Portman DJ, Bachmann GA, Simon JA. Ospemifene, a novel selective estrogen receptor modulator for treating dyspareunia associated with postmenopausal vulvar and vaginal atrophy. Menopause 20(6), 623–630 (2013).
23.
Premarin Prescribing Information (2018). https://www.premarinvaginalcream.com/about
24.
Imvexxy Prescribing Information (2018). https://www.imvexxy.com/pi.pdf
25.
Estrace Prescribing Information (2018). https://www.estracecream.com/
26.
Estring Prescribing Information (2018). http://labeling.pfizer.com/ShowLabeling.aspx?id=567
27.
Alliance PQ. PQA adherence measures (2019). https://www.pqaalliance.org/adherence-measures
28.
Shook LL. An update on hormone replacement therapy: health and medicine for women: a multidisciplinary, evidence-based review of mid-life health concerns. Yale J. Biol. Med. 84(1), 39–42 (2011).
29.
Simon JA, Nappi RE, Kingsberg SA, Maamari R, Brown V. Clarifying Vaginal Atrophy’s Impact on Sex and Relationships (CLOSER) survey: emotional and physical impact of vaginal discomfort on North American postmenopausal women and their partners. Menopause 21(2), 137–142 (2014).
30.
Shifren JL, Gass ML. The North American Menopause Society recommendations for clinical care of midlife women. Menopause 21(10), 1038–1062 (2014).
31.
The NAMS 2017 Hormone Therapy Position Statement Advisory Panel. The 2017 hormone therapy position statement of The North American Menopause Society. Menopause 24(7), 728–753 (2017).
32.
Crandall CJ, Hovey KM, Andrews CA et al. Breast cancer, endometrial cancer, and cardiovascular events in participants who used vaginal estrogen in the Women’s Health Initiative Observational Study. Menopause 25(1), 11–20 (2018).
33.
Manson JE, Aragaki AK, Rossouw JE et al. Menopausal hormone therapy and long-term all-cause and cause-specific mortality: the Women’s Health Initiative Randomized Trials. JAMA 318(10), 927–938 (2017).
34.
Simon JA, Altomare C, Cort S, Jiang W, Pinkerton JV. Overall safety of ospemifene in postmenopausal women from placebo-controlled Phase II and III trials. J. Womens Health 27(1), 14–23 (2018).
35.
Minkin MJ, Maamari R, Reiter S. Improved compliance and patient satisfaction with estradiol vaginal tablets in postmenopausal women previously treated with another local estrogen therapy. Int. J. Womens Health 5, 133–139 (2013).
36.
Donga P, DeKoven M, Kaplan T et al. Costs of Clostridium histolyticum and fasciectomy for Dupuytren’s contracture. Am. J. Pharm. Benefits 7(1), 7–12 (2015).
37.
Kleinman NL, Rohrbacker NJ, Bushmakin AG, Whiteley J, Lynch WD, Shah SN. Direct and indirect costs of women diagnosed with menopause symptoms. J. Occup. Environ. Med. 55(4), 465–470 (2013).
38.
Soliman AM, Yang H, Du EX, Kelley C, Winkel C. The direct and indirect costs associated with endometriosis: a systematic literature review. Hum. Reprod. 31(4), 712–722 (2016).
Information & Authors
Information
Published In
Pages: 1111 - 1123
PubMed: 31432687
Copyright
© 2019 Future Medicine Ltd.
History
Received: 10 July 2019
Accepted: 6 August 2019
Published online: 21 August 2019
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Ospemifene versus local estrogen: adherence and costs in postmenopausal dyspareunia. (2019) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2019-0091
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Maria Cristina Meriggiola, Paola Villa, Angelo Cagnacci, Stefano Luisi, Tommaso Simoncini, Massimo Stomati, Alessandra Lami, Tiziana Di Paolantonio, Silvia Marsini, Antonio Nicolucci, Cristina Puglielli, Rossella E. Nappi, Treatment of vulvovaginal atrophy is associated with high levels of satisfaction and improves symptom severity and patient-reported outcomes: 12-month results of the PatieEnt satisfactiON studY (PEONY), Menopause, 10.1097/GME.0000000000002737, 33, 7, (799-809), (2026).
- Costantino Di Carlo, Angelo Cagnacci, Filippo Murina, Silvia Maffei, Angelamaria Becorpi, Stefano Lello, Ospemifene and vulvovaginal atrophy: an update of the clinical profile for post-menopausal women, Expert Opinion on Pharmacotherapy, 10.1080/14656566.2024.2391009, 25, 11, (1541-1554), (2024).
- Jill Dreyfus, Swapna Munnangi, Camilla Bengtsson, Bárbara Correia, Rejane Figueiredo, James H. Stark, Michele Zawora, Mark S. Riddle, Jason D. Maguire, Qin Jiang, Claudia Ianos, Juan Naredo Turrado, Henrik Svanström, Steven Bailey, Mitchell DeKoven, Background incidence rates of health outcomes in populations at risk for Lyme disease using US administrative claims data, Vaccine, 10.1016/j.vaccine.2024.01.037, 42, 5, (1094-1107), (2024).
- María J. Cancelo, Rafael Sánchez Borrego, Santiago Palacios, Laura Baquedano, Tanit Corbacho Garza, Noelia Fernández Aller, Carmen García Ferreiro, Juan José Quijano Martín, A. Javier González Calvo, Vulvovaginal atrophy in the CRETA study: the healthcare professionals’ perception, Gynecological Endocrinology, 10.1080/09513590.2023.2264405, 39, 1, (2023).
- Haixiao Wen, Chong Lu, Meng Zhang, Xingling Qi, A real-world disproportionality analysis of ospemifene: data mining of the public version of FDA adverse event reporting system, Expert Opinion on Drug Safety, 10.1080/14740338.2023.2247971, 22, 11, (1133-1142), (2023).
- James A. Simon, Alex Ferenczy, Denise Black, Alex Castonguay, Catherine Royer, Rafik Marouf, Catherine Beauchemin, Efficacy, tolerability, and endometrial safety of ospemifene compared with current therapies for the treatment of vulvovaginal atrophy: a systematic literature review and network meta-analysis, Menopause, 10.1097/GME.0000000000002211, 30, 8, (855-866), (2023).
- Santiago Palacios, Rafael Sánchez-Borrego, Beatriz Suárez Álvarez, Félix Lugo Salcedo, A. Javier González Calvo, Juan José Quijano Martín, María J. Cancelo, María Fasero, Impact of vulvovaginal atrophy therapies on postmenopausal women's quality of life in the CRETA study measured by the Cervantes scale, Maturitas, 10.1016/j.maturitas.2023.03.007, 172, (46-51), (2023).
- S. Palacios, R. E. Nappi, M. J. Cancelo, S. Sánchez, T. Simoncini, Expert opinion on the treatment of vulvovaginal atrophy with ospemifene based on new evidence, Climacteric, 10.1080/13697137.2023.2190881, 26, 4, (388-391), (2023).
- R. Sánchez-Borrego, M. V. de Diego Pérez de Zabalza, M. J. Alfageme Gullón, M. L. Alija Castrillo, M. Sánchez Prieto, S. Palacios, A. J. González Calvo, J. J. Quijano Martín, M. J. Cancelo, Satisfaction and medication adherence in women with vulvovaginal atrophy: the CRETA, Climacteric, 10.1080/13697137.2023.2190508, 26, 5, (437-444), (2023).
- Kathleen Ridgeway, Elizabeth T. Montgomery, Kevin Smith, Kristine Torjesen, Ariane van der Straten, Sharon L. Achilles, Jennifer B. Griffin, Vaginal ring acceptability: A systematic review and meta-analysis of vaginal ring experiences from around the world, Contraception, 10.1016/j.contraception.2021.10.001, 106, (16-33), (2022).