Cost–effectiveness of tacrolimus for the treatment of moderate-to-severe lupus nephritis in China
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Therapy for lupus nephritis (LN) requires treatment with immunosuppressive regimens, often including intravenous cyclophosphamide (IVCY), mycophenolate mofetil (MMF) or azathioprine. Additionally, tacrolimus (original form or generic) is recommended to treat LN patients in Asia, including China. However, the cost–effectiveness of tacrolimus therapy has not previously been assessed. We aimed to estimate the cost–effectiveness of tacrolimus in the treatment of moderate-to-severe LN versus standard therapies in China. Materials & methods: This cost–effectiveness model combined a decision-tree/Markov-model structure to map transitions between health states during induction and maintenance treatment phases. Induction with tacrolimus, IVCY or MMF, was followed by tacrolimus, MMF or azathioprine maintenance. Results: According to the model, during induction, complete remission rates were higher with tacrolimus versus IVCY (relative risk 1.40 vs IVCY [deterministic sensitivity analysis minimum 0.92, maximum 2.13]) and time to response was shorter. Relapse rates were lower with tacrolimus versus azathioprine or MMF during maintenance. Tacrolimus induction and maintenance was the most cost-effective regimen, incurring the lowest total costs (CN¥180,448) with the highest quality-adjusted life-years. Conclusion: The model demonstrated that tacrolimus use in both induction and maintenance therapy may be an efficacious and cost-effective treatment for LN in China.
Systemic lupus erythematosus (SLE) is an autoimmune disease characterized by a loss of self-tolerance and the development of autoantibodies to self-antigens [1]. One of the major complications of SLE is lupus nephritis (LN), the renal manifestation of SLE. LN significantly increases the morbidity and mortality of SLE patients [2,3], and people of Asian origin have a greater likelihood of presenting with more severe LN compared with other racial or ethnic groups [4]. Furthermore, LN is an important cause of chronic renal failure in Asia [3,5], and can lead to end-stage renal disease (ESRD) [6]. Effective treatment of LN at an early stage reduces the number of patients who progress to ESRD. Given the high costs associated with dialysis and kidney transplantation [7], the low transplantation rate in Asia, and the high morbidity and mortality rates associated with prolonged dialysis [8], the prevention of ESRD in LN patients is not only life-saving but likely to be a cost-saving intervention. Selecting an appropriate therapy early in the disease course thus has important implications on saving long-term healthcare costs [9–11].
Therapy for LN requires treatment with aggressive immunosuppressive regimens [6,12], which aim to halt deterioration of renal function and prevent the need for dialysis and transplantation [6]. While high-dose oral corticosteroids are generally the mainstay of therapy [6,12,13], they are associated with potentially severe side effects [14,15]. Decreasing reliance on steroids is now a pertinent issue, and immunosuppressive agents are often added to therapy to minimize adverse reactions and increase treatment efficacy. In this regard, intravenous cyclophosphamide (IVCY) and mycophenolate mofetil (MMF) are typically used in the induction treatment phase, while MMF and azathioprine (AZA) are used in the maintenance phase, including in China [6,12,13,16,17]. The calcineurin inhibitor, tacrolimus, is also recommended for the treatment of LN [6,13,16,17], and in Asia, tacrolimus induction and maintenance therapy is suggested for the treatment of Class III–V disease [18]. For example, in China, combined use of corticosteroid given together with cyclophosphamide or MMF, with or without tacrolimus, is often used as induction therapy, and low-dose corticosteroid with MMF or AZA, or tacrolimus is adopted as maintenance therapy for LN [19].
In a network meta-analysis, calcineurin inhibitors more effectively induced disease remission compared with IVCY [20]. Tacrolimus has been demonstrated to be steroid-sparing [21,22], and a pilot study reported that approximately 90% of patients achieved a complete or partial response to tacrolimus induction therapy at 6 months [23]. Response rates after 12 and 24 months of add-on tacrolimus treatment were 66.7 and 80.0%, respectively, in patients with Class V LN and nephrotic syndrome [24]. Furthermore, a 6-month induction regimen with tacrolimus in patients with active LN achieved a numerically higher cumulative probability of complete remission and response rate compared with IVCY treatment [25]. In a systematic literature review including 65 studies, tacrolimus was superior to low-dose cyclophosphamide in achieving renal remission/response [26]. Tacrolimus was shown to be non-inferior to MMF in the treatment of LN [27], and was associated with more rapid proteinuria reduction compared with standard therapy [22,25]. Importantly, maintenance treatment with tacrolimus was effective in preventing flares in LN, potentially preventing long-term renal damage and reducing dependence on steroid treatment [21,22,28,29].
The decision to treat patients with tacrolimus is affected by multiple factors, including its availability and affordability, and the use of tacrolimus varies regionally within China. Nevertheless, the use of tacrolimus for LN is relatively higher in China compared with other countries in Asia, and it is thought that the original form (Prograf) and generics are used to treat approximately 15% of LN patients in China. In order to ascertain the clinical and cost–effectiveness of tacrolimus versus standard therapies, China's payers, regulators and physicians require a network meta-analysis and cost–effectiveness model. There are a plethora of publications from China that report treatment strategies with tacrolimus, as single or multitherapy with steroids for both induction and maintenance therapy for LN, which supports the development of such a model. However, while evidence suggests that tacrolimus can achieve and maintain remission, thereby reducing the likelihood of expensive late-stage events such as ESRD and kidney transplantation [30], there has been no cost–effectiveness analysis. We, therefore, developed a model of the cost–effectiveness of tacrolimus in the treatment of moderate-to-severe LN versus standard therapies in China.
Materials & methods
Amaris Consulting UK, a consultancy company that provides services for evidence generation, market access and statistical or health economic assessment of new health technologies and health policies, was contracted to conduct the literature review, develop the model specifications, perform statistical analyses, develop and test the model, and produce the subsequent technical report.
Patient population
This model focused on patients with focal or diffuse proliferative LN, as defined by Class III, IV, with or without concomitant Class V of the International Society of Nephrology-Renal Pathology Society classification [31]. In the model, mean patient age at baseline was arbitrarily selected as 18 years. Mean weight was 60 kg and mean body surface area was 1.63 m2, based on feedback from an expert advisory board that these values would be relevant to LN patients in China.
Treatment pathways
The model included nine treatment pathways, with three possible induction treatments (tacrolimus [3 mg/day, which is the standard protocol in China], IVCY [0.75 g/m2/month for 6 months] or MMF [2 g/day]) and three possible maintenance treatments (tacrolimus [0.05 mg/kg/day], AZA [2 mg/kg/day] or MMF [2 g/day]) [13,18,32]. Throughout the manuscript, immunosuppressive regimens are reported in the format ‘induction followed by maintenance’ therapy. Second-line induction therapies included in the model were IVCY for patients who had received first-line tacrolimus, MMF for first-line IVCY, and IVCY for first-line MMF. All the induction and maintenance regimens modeled also included corticosteroid therapy (10 mg/day prednisolone) [6,12,13,18].
Outcomes
The outcomes of the study were rate of complete remission, a composite of complete and partial remission, time to response (complete remission, or a composite of complete and partial remission) and cost–effectiveness of the treatment regimens over a 20-year horizon from a Chinese payer perspective. The payer refers to national reimbursement drug list and provincial reimbursement drug list stakeholders (e.g., health economists, health policy makers and national reimbursement drug list/provincial reimbursement drug list reviewers).
Systematic literature review & network meta-analysis
A systematic literature review was carried out that evaluated clinical, economic and quality of life (QoL) outcomes in patients with LN, to inform the cost–effectiveness model structure and to provide data for input (i.e., remission and relapse rates, incidence of adverse events [AEs], etc.). The selection criteria for the systematic literature review were prespecified, and based on the Population, Intervention, Comparator, Outcome and Study type (PICOS) framework (Supplementary Material 1). Tacrolimus was initially licensed for the treatment of LN in Japan in 2007, with the pivotal clinical study completed in 2006. EMBASE and the Cochrane Library were, therefore, searched to identify relevant articles published between 2006 and 2016 (the model was completed in early 2017). MEDLINE and MEDLINE In-Process were searched to find articles published from database initiation until 2016. In addition, manual searches were undertaken to identify relevant conference abstracts and posters presented between 2013 and 2016 at key scientific conferences. Websites considered for the manual search included those for the American College of Rheumatology, European League Against Rheumatism, British Society for Rheumatology, Asia Pacific League of Associations for Rheumatology and Clinicaltrials.gov. Search terms used to identify relevant publications (and also to perform manual searches) are outlined in Supplementary Material 1.
Overall, 1927 records were identified and, upon initial screening, 106 studies were considered to be of interest. Following a full-text review of these publications, 43 were identified as meeting the selection criteria and 34 were clinical studies. The clinical studies were carried out in a variety of countries, including China (n = 9), USA (n = 4), Japan (n = 2), Czech Republic (and Slovakia) (n = 2), the Netherlands (n = 2), Italy (n = 1), Canada (n = 1), India (n = 1), Thailand (n = 1) and Egypt (n = 1). Four studies were multinational, and six studies did not state the location. The PRISMA diagram is presented in Supplementary Material 1. While no formal heterogeneity assessment was conducted, the included clinical trials were considered comparable for study duration, dosing, number of treatment cycles, concomitant steroid use, class of LN, study location, end points and relevant patient characteristics when reported (e.g., age, sex, treatment history, baseline serum creatinine, urine protein/creatinine ratio and proteinuria).
As none of the studies included in the systematic literature review were head-to-head trials of all interventions included in the model, two network meta-analyses were performed in order to estimate the complete and partial response rates and health state transition probabilities (described in the transition probabilities and clinical inputs section).
Data were sought from Chinese or Asian populations wherever possible, particularly for economic aspects of the model. Where necessary, clinical data were taken from other patient populations.
Expert advisory board
An expert advisory board comprising 14 members, including rheumatologists and nephrologists, was provided with a draft of the model structure and proposed assessment of effectiveness, as well as treatment protocols. The panel then provided feedback regarding adjustments to the model structure, treatment duration and model cycles, which were implemented in the final model.
Model structure
Three cost-utility analyses in patients with LN were identified from the systematic literature review, and assessed:
Of the three identified economic models, two were Markov models with analyses conducted over a lifetime horizon [33,34] and one was a patient-level simulation to analyze only the induction phase [35]. Markov models use disease states to represent all possible consequences of an intervention. The disease states are mutually exclusive, but patients can transition between states. Time spent in each disease state and transitions between states are associated with a cost and a health outcome, which are then aggregated for a modeled cohort of patients over successive cycles. As the goals of LN treatment differ between the induction and maintenance phases – the former to induce a state of disease quiescence, the latter to consolidate remission and prevent relapse – modelling these two phases separately was considered valid.
Across the models, differentiating disease progression over time by response status was pertinent in both the induction and maintenance phases. The health states included in the previously published models were active disease, complete remission and partial remission [33,35], ESRD and death [33,34], and LN relapse [34]. As such, our cost–effectiveness model consisted of an induction phase and a maintenance phase, each containing three health states: active disease, partial remission and complete remission. The maintenance phase outcomes also included the health states of ESRD, kidney transplantation, post-kidney transplantation and death. Complete remission was defined as the return of serum creatinine to the patient's previous baseline level, plus a decline in the urine protein-to-creatinine ratio to <500 mg/g [13]. Partial remission was the stabilization (±25%) or improvement of serum creatinine, but not to the patient's previous baseline level, plus a ≥50% decrease in urine protein-to-creatinine ratio [13].
Both the induction and maintenance phases assessed patient transitions between health states using 3-month cycles, and patients could transition to the health state of death at any point during treatment. Feedback from an expert advisory board was that treatment efficacy would be evaluated approximately every 3 months. Therefore, as transitions were measured every 3 months in the induction phase, this was carried through to the maintenance phase.
Patients entered our model in the induction phase in a state of active disease. The induction phase utilized a decision tree model structure, as presented in Figure 1A, and patients could remain in the induction phase up to 18 months, depending on response to treatment. Patients entered the maintenance phase in the health state in which they left the induction phase – either in complete remission, partial remission, or with active disease. If patients had not achieved complete remission by 18 months, they transitioned to the maintenance phase. Given the time-dependent outcomes associated with LN and the chronic nature of the disease, the maintenance phase utilized a Markov model structure (Figure 1B) [33,34], within which patients could transition back to active disease and then transition to ESRD. From ESRD patients could temporarily enter a 3-month tunnel state that included kidney transplantation followed by post-kidney transplantation.
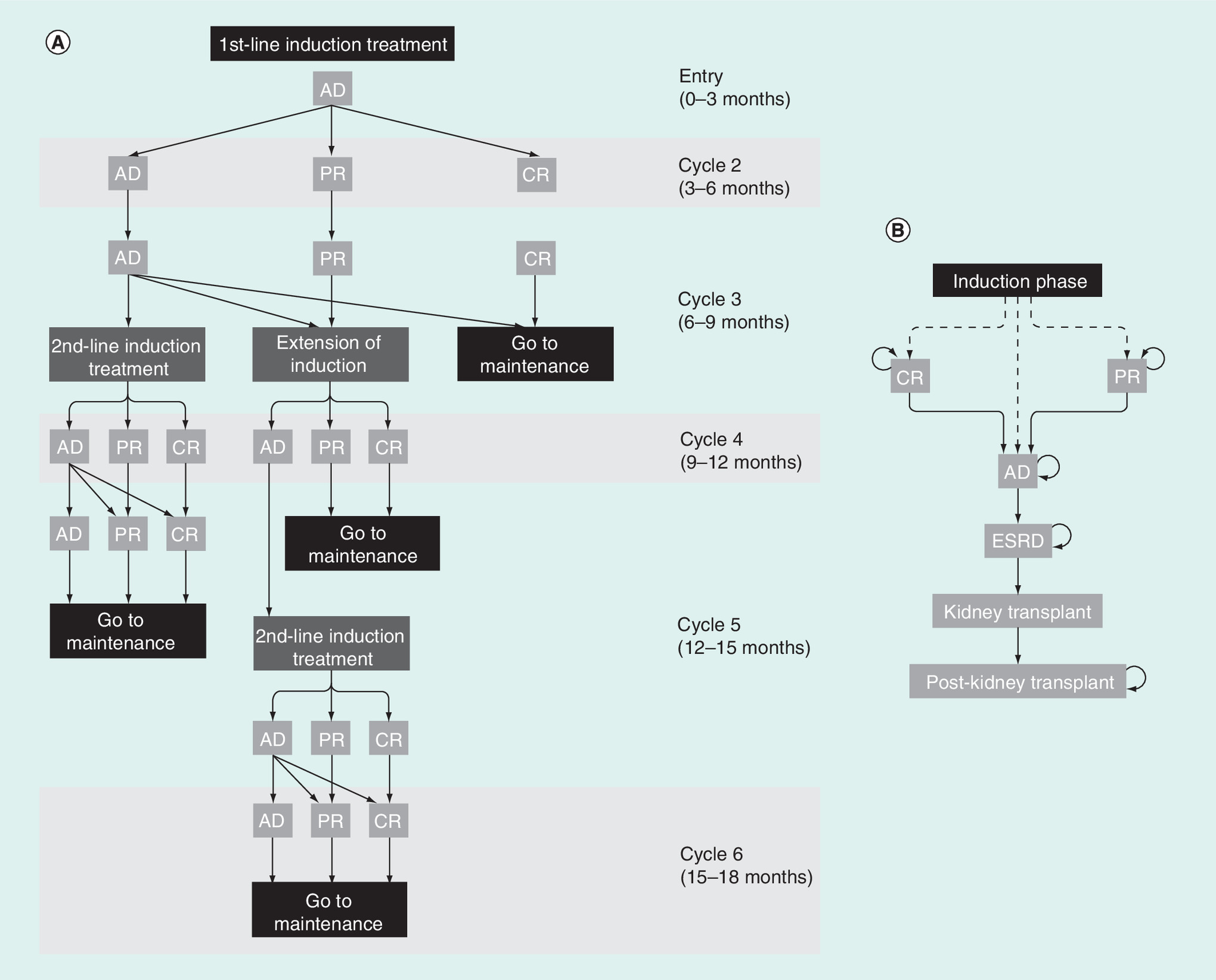
Figure 1. Structure of the induction phase decision-tree (A) and maintenance phase Markov (B) models.
(A) Patients entered the induction phase in an AD state. At cycle 3, patients still with AD received second-line induction therapy (MMF or IVCY) or an extension of first-line induction treatment, patients with PR received an extension of the first-line induction treatment, and patients in CR transitioned to the maintenance phase. Patients with AD receiving second-line induction therapy could transition to PR or CR at cycles 4 and 5, subsequently moving to the maintenance phase. Patients with PR receiving an extension of first-line induction therapy may transition to PR or CR in cycle 4, and then transition to the maintenance phase in cycle 5. Patients with PR transitioning to the AD state following an extension received second-line induction therapy in cycle 5. These patients may then transition to AD, PR or CR over cycles 5 and 6, and transition to the maintenance phase at cycle 6. (B) In all health states during the maintenance phase, there is the risk of death due to other causes (background mortality), as well an increased risk of death in patients post transplantation.
AD: Active disease; CR: Complete remission; ESRD: End-stage renal disease; IVCY: Intravenous cyclophosphamide; MMF: Mycophenolate mofetil; PR: Partial remission.
Patients accumulated costs and benefits in the form of quality-adjusted life years (QALYs) with the different health states over time.
Transition probabilities & clinical inputs
In order to determine the rates of remission and transitions between health states in the model, the event rates and probability of their occurrence were obtained from studies identified in the systematic literature review and, where possible, a network meta-analysis was conducted to compare treatments (see Supplementary Material 2 for a summary of data sources).
For the induction phase, across the studies, complete remission rates ranged from 1 to 50% for IVCY, 9 to 59% for MMF and 4 to 62% for tacrolimus [25,27,36–43]. Partial remission rates during induction ranged from 20 to 70% for IVCY, 21 to 48% for MMF and 27 to 38% for tacrolimus [25,27,36–39,41,42,44,45]. A direct comparison of IVCY treatment effect versus all other therapies was possible using data obtained from randomized clinical studies identified in the literature review. As such, a network meta-analysis (Bucher's method) was conducted on the rates of complete/partial remission by the end of 6 months of induction therapy in order to indirectly compare the other treatments included in the model [46]. Given that only pairwise comparisons were included (with IVCY as the primary comparator), results were not expected to differ between pairwise and network meta-analyses. Figure 2 presents the publications in the network meta-analysis for complete and partial remission in the induction phase. Random effects models were employed for calculating the mixed treatment comparison for complete and partial remission in the network meta-analysis (Table 1).
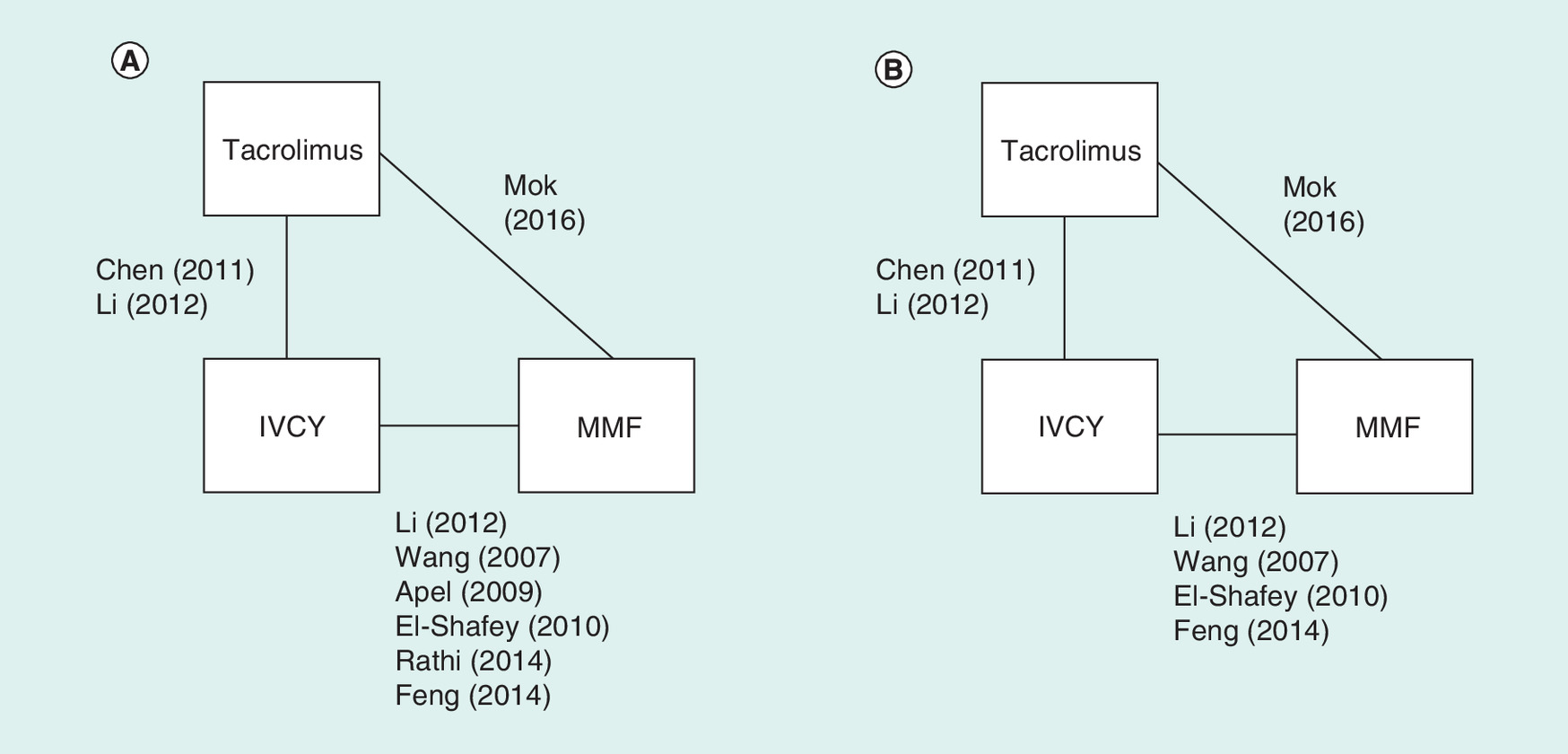
Figure 2. Publications included in the network meta-analysis for complete remission (A) and partial remission (B) in the induction phase.
AZA: Azathioprine; IVCY: Intravenous cyclophosphamide; MMF: Mycophenolate mofetil.
| Efficacy measure | IVCY | MMF | Tacrolimus |
|---|---|---|---|
| Pooled RR complete remission | Reference† | 1.12 (0.85, 1.47) | 1.40 (0.92, 2.13) |
| Pooled RR partial remission | Reference† | 0.98 (0.67, 1.45) | 0.90 (0.57, 1.43) |
| Baseline probability of complete remission at 6 months (%) | 22.4 (13.8, 31.0) | 25.0 (19.0, 32.9) | 31.2 (20.5, 47.7) |
| Baseline probability of partial remission at 6 months (%) | 28.9 (19.0, 38.7) | 28.4 (19.3, 41.8) | 26.1 (16.5, 41.3) |
†
IVCY is the reference treatment. Numbers in brackets are 95% CI.
IVCY: Intravenous cyclophosphamide; MMF: Mycophenolate mofetil; RR: Relative risk.
Due to a lack of head-to-head evidence, a mixed treatment comparison of therapy efficacy could not be conducted for the maintenance phase. Therefore, efficacy in the maintenance phase was determined by relapse rates using data extracted from existing trials identified in the literature review and, where required, extrapolating across the 20-year horizon [47–49]. An estimate on the rate of relapse for patients receiving AZA was obtained from Chan et al. and for patients who received MMF, a hazard ratio from Dooley et al. was applied to this [47,48]. No comparative evidence was found for tacrolimus, and so absolute relapse rates from Takeuchi et al. were used [49].
Health state transition probabilities for the movement between active disease, partial remission and complete remission were derived from the published literature identified in the systematic literature review and, for the induction phase, following a network meta-analysis [47–50]; the probabilities are presented in Table 2. The initial probabilities were calculated based on remission rates in the trials for IVCY. Transition probabilities were adjusted using an exponential function to obtain per-cycle probabilities. As no efficacy estimates were available for the use of second-line induction therapies, it was assumed that a treatment used as a second-line therapy was just as effective in inducing remission as it would be when used as a first-line therapy.
| Treatment | Transition | Probability (3-month cycle), % | 95% CI | Source |
|---|---|---|---|---|
| Transition probabilities: induction phase | ||||
| Tacrolimus | AD to CR | 17.1 | 10.8–27.6 | Network meta-analysis (using a mixed treatment comparison) |
| Tacrolimus | AD to PR | 14.0 | 8.6–23.4 | |
| IVCY | AD to CR | 11.9 | 7.1–16.9 | |
| IVCY | AD to PR | 15.7 | 10.0–21.7 | |
| MMF | AD to CR | 13.4 | 10.0–18.1 | |
| MMF | AD to PR | 15.4 | 10.2–23.7 | |
| Transition probabilities: maintenance phase | ||||
| Tacrolimus | CR to AD | 0.2 | 0.0–0.6 | Takeuchi et al. (2015) |
| Tacrolimus | PR to AD | 1.7 | 0.3–3.8 | Takeuchi et al. (2015) |
| AZA | CR to AD | 1.7 | 0.2–5.7 | Chan et al. (2005) |
| AZA | PR to AD | 8.9 | 0.1–36.5 | Chan et al. (2005) |
| MMF | CR to AD | 0.7 | 0.0–4.5 | Dooley et al. (2011) |
| MMF | PR to AD | 4.0 | 0.0–30.1 | Dooley et al. (2011) |
| All | AD to ESRD | 0.1 | 0.0–0.5 | Chan et al. (2005) |
| All | ESRD to kidney transplantation | 0.3 | 0.3–0.3 | Zhang et al. (2016) |
| All | Kidney transplantation to post transplantation | 100 | NA | Assumption |
| All | Post transplantation to death | 0.2 | 0.1–0.4 | Zhang et al. (2016) |
Health state transition probabilities for the movement between AD, PR and CR were derived from the published literature identified in the systematic literature review and from a network meta-analysis of the identified studies where applicable. Where data were derived from a single study, the reference has been cited. All CIs and probabilistic values utilized the beta distribution in their calculation.
AD: Active disease; AZA: Azathioprine; CR: Complete remission; ESRD: End-stage renal disease; IVCY: Intravenous cyclophosphamide; MMF: Mycophenolate mofetil; NA: Not applicable; PR: Partial remission.
For late-stage events, the probabilities of transition were derived from published literature [47,50] and adjusted using exponential functions to obtain per-cycle probabilities (Table 2). Patient death unrelated to LN was included in the model using all-cause mortality probabilities from the WHO China Life Tables 2015–2016 [51].
Health state utility values
Quality-adjusted life years
Only AEs with a significant impact on cost or health outcomes were included in the model. The incidence of AEs occurring during treatment with each of the included interventions, and utility decrements as a result of AEs, was extracted from the literature (see Supplementary Material 2 for a summary): amenorrhea (utility decrement -0.039), menstrual abnormality (-0.039), leukopenia (-0.090), alopecia (-0.045), infection (-0.310), gastrointestinal AE (-0.006), herpes zoster (-0.280) and tremor (-0.074) [34,35,53–57]. Most disutility values were not sourced from patients with SLE or LN, as data were not available. To calculate an overall loss in QALYs as the result of AEs, the individual disutility was multiplied by the intervention and treatment phase-specific incidence of events (i.e., decrement of 0.05 in 10% of patients = -0.005 QALYs). The overall disutility associated with AEs per drug per treatment phase was calculated as the sum of all utility decrements for all AEs and then applied as a one-off decrement in QoL.
Cost inputs & resource use
Costs are presented as Chinese Yuan (CN¥), which is the local currency. Only direct medical costs (drugs and visits) were included in the cost–effectiveness model. Drug costs were calculated for the induction and maintenance phases based on the recommended dosing schedules and on the Chinese National Reimbursement Drug List. In the model, the cost of maintenance treatment was applied until the patient relapsed (i.e., transitioned to the active disease health state in the maintenance phase of the model). Dialysis costs were applied to all patients in the ESRD health state (CN¥20,047 per cycle [58]). Costs associated with patients in the kidney transplant state included inpatient accommodation (CN¥2557 per transplant), medication (CN¥47,819), surgical procedures (CN¥9122), examination fees (CN¥7878), nursing care (CN¥346) and miscellaneous (CN¥1382) [7]. Post-transplantation care was costed at CN¥13,520 per 3-month cycle [59].
Uncertainty analyses
A deterministic sensitivity analysis (DSA) and a probabilistic sensitivity analysis (PSA) was performed (Table 3). For the DSA, parameters were varied using the 95% confidence intervals generated from conventionally used distributions (i.e., beta distribution for transition probabilities and utilities). For parameters with unknown standard errors, these were assumed to be 20% of the mean. For the PSA, a Monte Carlo simulation was performed using 5000 iterations of randomly sampled values from the defined distributions. All parameters, except drug costs and discount rates, were included in the sensitivity analyses.
| Parameter | Baseline value | Standard error | DSA min value | DSA max value | PSA distribution |
|---|---|---|---|---|---|
| CR rates at 6 months | |||||
| – IVCY | 22.4% | 0.044 | 13.8% | 31.0% | Beta– |
| – MMF | 25.0% | 0.036 | 19.0%† | 32.9%† | Beta |
| – Tacrolimus | 31.2% | 0.069 | 20.5%† | 47.7%† | Beta |
| – AZA | 23.6% | 0.117 | 9.9%† | 55.8%† | Beta |
| PR rates at 6 months | |||||
| – IVCY | 28.9% | 0.050 | 19.0% | 38.7% | Beta |
| – MMF | 28.4% | 0.057 | 19.3%† | 41.8% | Beta |
| – Tacrolimus | 26.1% | 0.063 | 16.5%† | 41.3% | Beta |
| – AZA | 34.2% | 0.041 | 27.1%† | 43.2% | Beta |
| Utility values | |||||
| – AD | 0.764 | ±20% | 0.069 | 1.000 | Beta |
| – CR | 0.940 | ±20% | 0.106 | 1.000 | Beta |
| – PR | 0.850 | ±20% | 0.087 | 1.000 | Beta |
| –ESRD | 0.689 | ±20% | 0.054 | 1.000 | Beta |
| – Post transplantation | 0.870 | ±20% | 0.092 | 1.000 | Beta |
| Non-drug costs | |||||
| – Cost of dialysis | CN¥20,047 | ±20% | CN¥12,189 | CN¥27,905 | Normal |
| – Inpatient stay | CN¥2557 | ±20% | CN¥1555 | CN¥3559 | Normal |
| – Medications | CN¥47,819 | ±20% | CN¥29,075 | CN¥66,564 | Normal |
| – Surgical procedures | CN¥9122 | ±20% | CN¥5546 | CN¥12,697 | Normal |
| – Examination fee | CN¥7878 | ±20% | CN¥4790 | CN¥10,966 | Normal |
| – Nursing care | CN¥346 | ±20% | CN¥210 | CN¥481 | Normal |
| – Miscellaneous | CN¥1382 | ±20% | CN¥840 | CN¥1924 | Normal |
| – Post-transplantation care | CN¥13,520 | ±20% | CN¥8220 | CN¥18,819 | Normal |
| AE costs (one-off cost per treatment) | |||||
| – Tacrolimus: induction | CN¥16 | ±20% | CN¥10 | CN¥22 | Normal |
| – MMF: induction | CN¥31 | ±20% | CN¥19 | CN¥43 | Normal |
| – IVCY: induction | CN¥35 | ±20% | CN¥21 | CN¥29 | Normal |
| – Tacrolimus: maintenance | CN¥5 | ±20% | CN¥3 | CN¥6 | Normal |
| – MMF: maintenance | CN¥28 | ±20% | CN¥17 | CN¥39 | Normal |
| – AZA: maintenance | CN¥33 | ±20% | CN¥20 | CN¥46 | Normal |
| AE disutilities (applied once per treatment) | |||||
| – Tacrolimus: induction | -0.111 | ±20% | -0.071 | -0.157 | Beta |
| – MMF: induction | -0.161 | ±20% | -0.104 | -0.229 | Beta |
| – IVCY: induction | -0.208 | ±20% | -0.133 | -0.294 | Beta |
| – Tacrolimus: maintenance | -0.008 | ±20% | -0.005 | -0.011 | Beta |
| – MMF: maintenance | -0.195 | ±20% | -0.125 | -0.276 | Beta |
| – AZA: maintenance | -0.129 | ±20% | -0.083 | -0.183 | Beta |
†
DSA values calculated as a function of IVCY remission rate and relative risks. The DSA minimum and maximum values for each parameter were based on the baseline value, standard error and the distribution applied. This was used to create 95% CIs on the point estimate. Using macros coded in Visual Basic for Applications in the Excel model, the analysis was rerun, sampling the minimum and maximum values for each point estimate in turn to see how the incremental cost-effectiveness ratio and net monetary benefit changed.
AD: Active disease; AE: Adverse event; AZA: Azathioprine; CR: Complete remission; DSA: Deterministic sensitivity analysis; ESRD: End-stage renal disease; IVCY: Intravenous cyclophosphamide; MMF: Mycophenolate mofetil; PR: Partial remission; PSA: Probabilistic sensitivity analysis.
Results
Remission
Based on the studies included, in modelling of the induction phase, tacrolimus was associated with a higher rate of complete remission versus IVCY and MMF (relative risk 1.40 vs IVCY [DSA minimum 0.92, maximum 2.13]; relative risk vs MMF 1.120 [DSA minimum 0.85, maximum 1.47]), and rate of composite complete or partial remission, and a shorter time to response (Figure 3A). The relative risks of achieving partial remission with tacrolimus or MMF compared with IVCY were 0.90 (DSA minimum 0.57, maximum 1.43) and 0.98 (DSA minimum 0.67, maximum 1.45), respectively (Table 1). In modelling of maintenance therapy, the rate of loss of remission (complete remission and composite complete or partial remission) was predicted to be lower with tacrolimus than with MMF or AZA over 20 years of treatment (Figure 3B). However, without formal assessment of the overall quality of the evidence upon which these results are based – for example by using the Grading of Recommendations, Assessment, Development and Evaluations framework – the findings should be interpreted with caution.
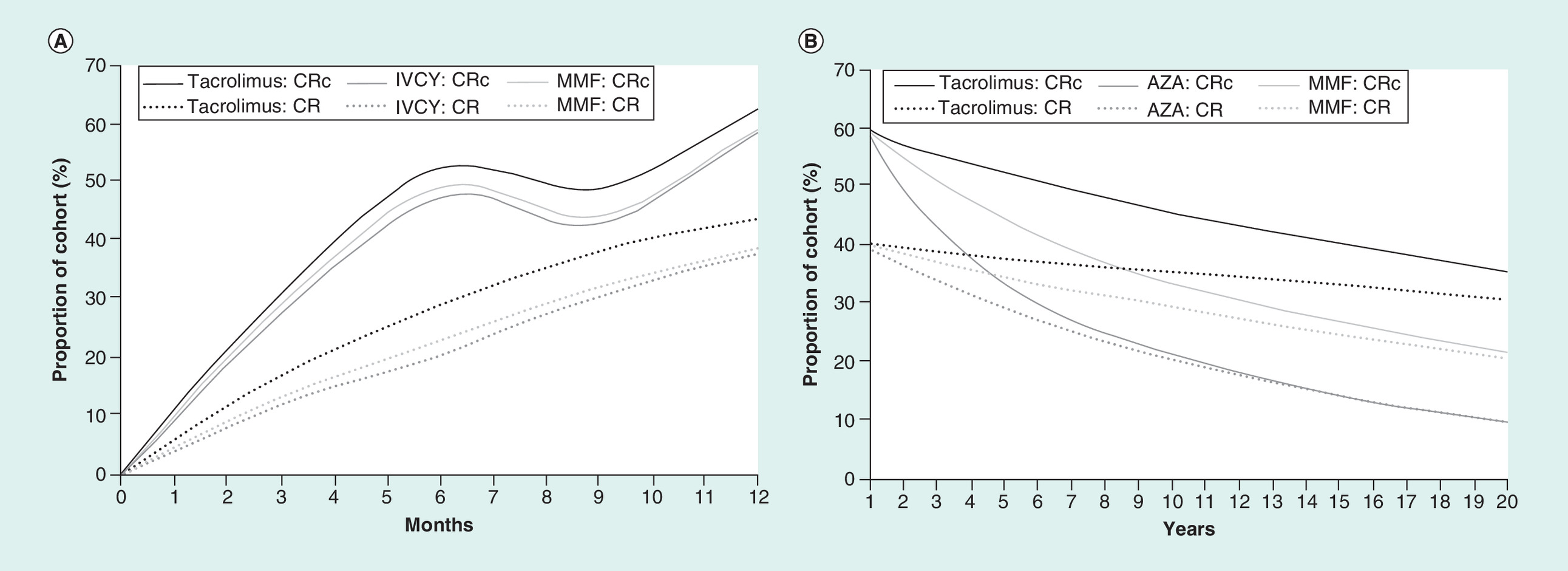
Figure 3. Percentage of the cohort in remission during the first 12 months, stratified by induction therapy (A) and in remission in years 2–20 stratified by maintenance therapy (B).
CRc refers to a composite of complete and partial remission. The curves are averaged across the nine treatment pathways by (A) the three initial induction treatments and (B) maintenance. Therefore, graph A contains solely patients in the induction phase in months 0–6, and both patients undergoing induction therapy and those in maintenance therapy in months 6–12.
AZA: Azathioprine; CR: Complete remission; CRc: Complete remission composite; IVCY: Intravenous cyclophosphamide; MMF: Mycophenolate mofetil.
Cost–effectiveness
The treatment regimens predicted to have the highest QALY gain versus all other comparators were tacrolimus induction + tacrolimus maintenance, and IVCY induction + tacrolimus maintenance (11.9 QALYs for both). Estimates of the 20-year expected medical costs associated with these two regimens were CN¥180,448 and CN¥292,085, respectively, with tacrolimus + tacrolimus incurring the lowest total costs with the highest total QALYs of the regimens analyzed (Table 4). At all reasonable willingness-to-pay thresholds, tacrolimus + tacrolimus was also predicted to be associated with the highest net monetary benefit, followed by IVCY + tacrolimus and MMF + tacrolimus (Table 4). Plotting incremental QALYs against incremental costs for each treatment regimen showed that tacrolimus + tacrolimus was likely to be more cost-effective than the other treatment regimens modeled (Figure 4).
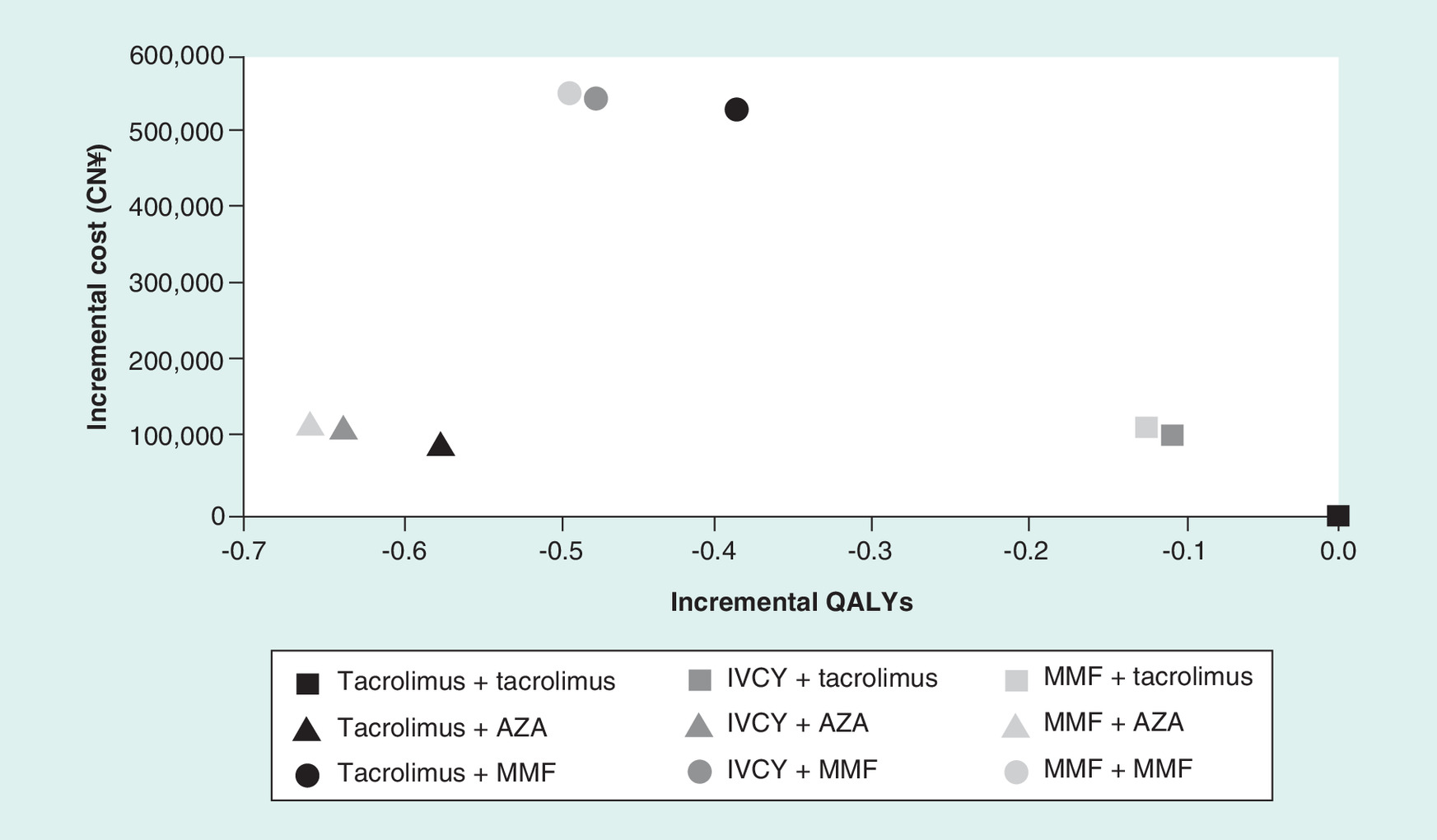
Figure 4. Base case cost–effectiveness plane stratified by treatment regimen, with tacrolimus + tacrolimus as the comparator regimen.
AZA: Azathioprine; IVCY: Intravenous cyclophosphamide; MMF: Mycophenolate mofetil; QALY: Quality-adjusted life year.
| Regimen | Costs (CN¥) | QALYs | Life years† | Net monetary benefit (CN¥)‡ |
|---|---|---|---|---|
| Tacrolimus + tacrolimus | 180,448 | 11.9 | 14.9 | 2,205,074 |
| Tacrolimus + AZA | 272,007 | 11.4 | 14.9 | 1,998,662 |
| Tacrolimus + MMF | 704,959 | 11.5 | 14.9 | 1,603,571 |
| IVCY + tacrolimus | 292,085 | 11.9 | 14.9 | 2,072,360 |
| IVCY + AZA | 291,206 | 11.3 | 14.9 | 1,966,955 |
| IVCY + MMF | 721,084 | 11.5 | 14.9 | 1,569,600 |
| MMF + tacrolimus | 298,252 | 11.8 | 14.9 | 2,063,254 |
| MMF + AZA | 297,568 | 11.3 | 14.9 | 1,956,421 |
| MMF + MMF | 728,080 | 11.4 | 14.9 | 1,559,197 |
†
Life years are the same because most deaths were not related to the treatment pathway. All-cause mortality is the main cause of death, with death following kidney transplantation being a minor secondary risk.
‡
Net monetary benefit was calculated at a willingness-to-pay threshold of CN¥200,000.
AZA: Azathioprine; IVCY: Intravenous cyclophosphamide; MMF: Mycophenolate mofetil; QALY: Quality-adjusted life year.
Deterministic sensitivity analysis
Results of the DSA for tacrolimus + tacrolimus versus other regimens using tacrolimus as the induction drug showed that base case results were most sensitive to utility values and the rate of complete remission during the induction phase.
For tacrolimus + tacrolimus versus regimens using IVCY induction therapy, complete remission with tacrolimus during the induction phase impacted net monetary benefit (Figure 5). Sensitivity was also demonstrated to the efficacy of the secondary induction therapy and utility values. When comparing tacrolimus with IVCY secondary induction + tacrolimus with other regimens using MMF induction, the greatest sensitivity was induction of remission and the utility values of the regimen.
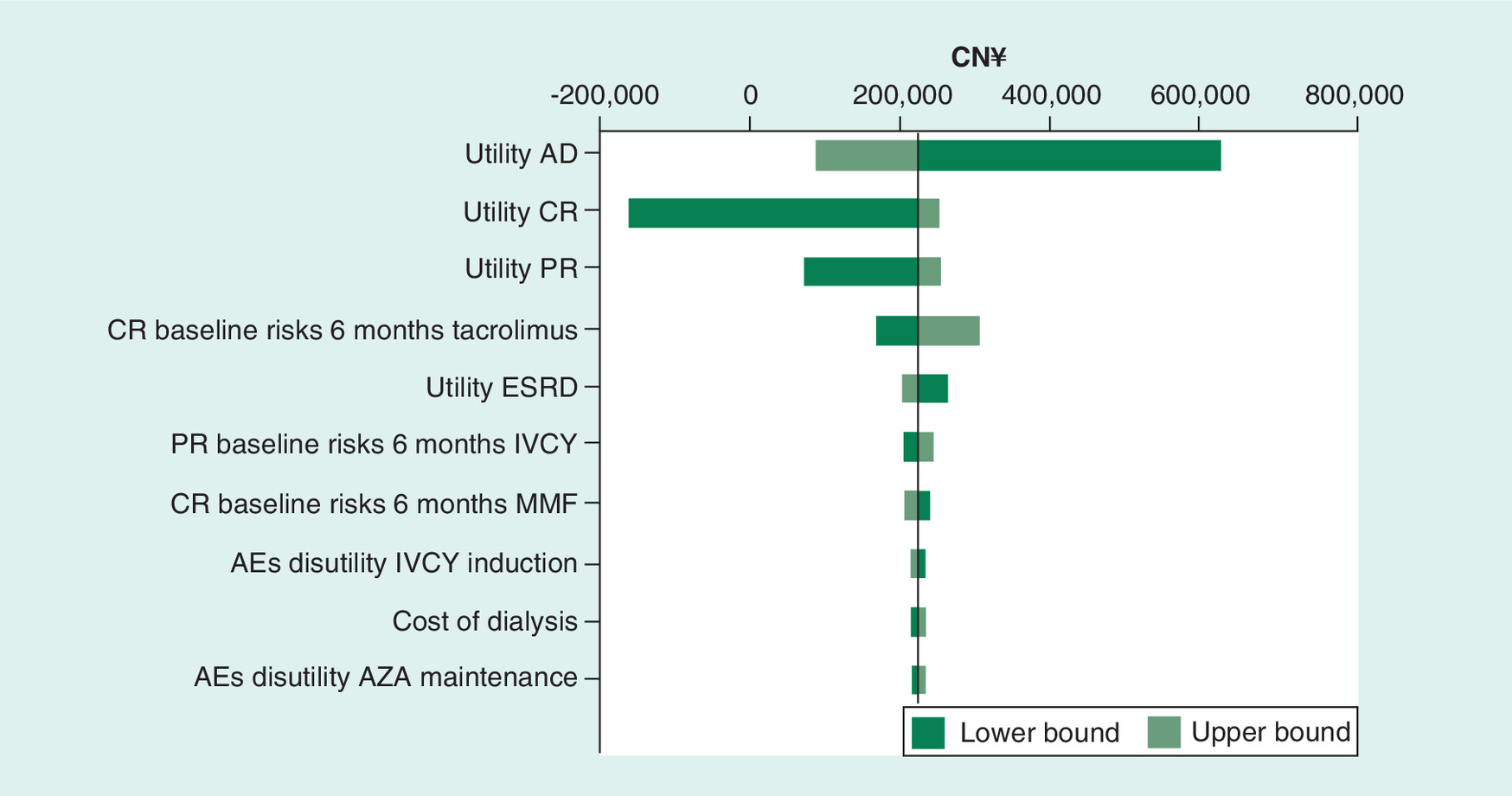
Figure 5. Sensitivity of the net monetary benefit at a willingness-to-pay threshold of CN¥200,000 between tacrolimus + tacrolimus, and IVCY + AZA regimens.
Upper and lower bounds refer to the confidence intervals of the parameter underlying the value, not the upper and lower bounds of the results. For example, the graph shows that by increasing the utility associated with AD, the net monetary benefit decreases, whereas increasing the baseline risk of CR with tacrolimus increases the net monetary benefit.
AD: Active disease; AE: Adverse event; AZA: Azathioprine; CR: Complete remission; ESRD: End-stage renal disease; IVCY: Intravenous cyclophosphamide; MMF: Mycophenolate mofetil; PR: Partial remission.
Probabilistic sensitivity analysis
Across all willingness-to-pay thresholds up to CN¥200,000, tacrolimus + tacrolimus had the highest probability of being cost effective compared with the other treatment regimens (Figure 6). Assuming a willingness-to-pay threshold of between one- and three-times the nominal gross domestic product (GDP) per capita in China (CN¥54,000–168,000), the probability that tacrolimus + tacrolimus was the most cost-effective treatment for LN was between 96 and 72%, compared with the next most likely regimen (tacrolimus + AZA; between 1.7 and 10.4%). The three treatment regimens using MMF as the maintenance therapy had a probability of being cost-effective of less than 0.001 across all explored willingness-to-pay thresholds.
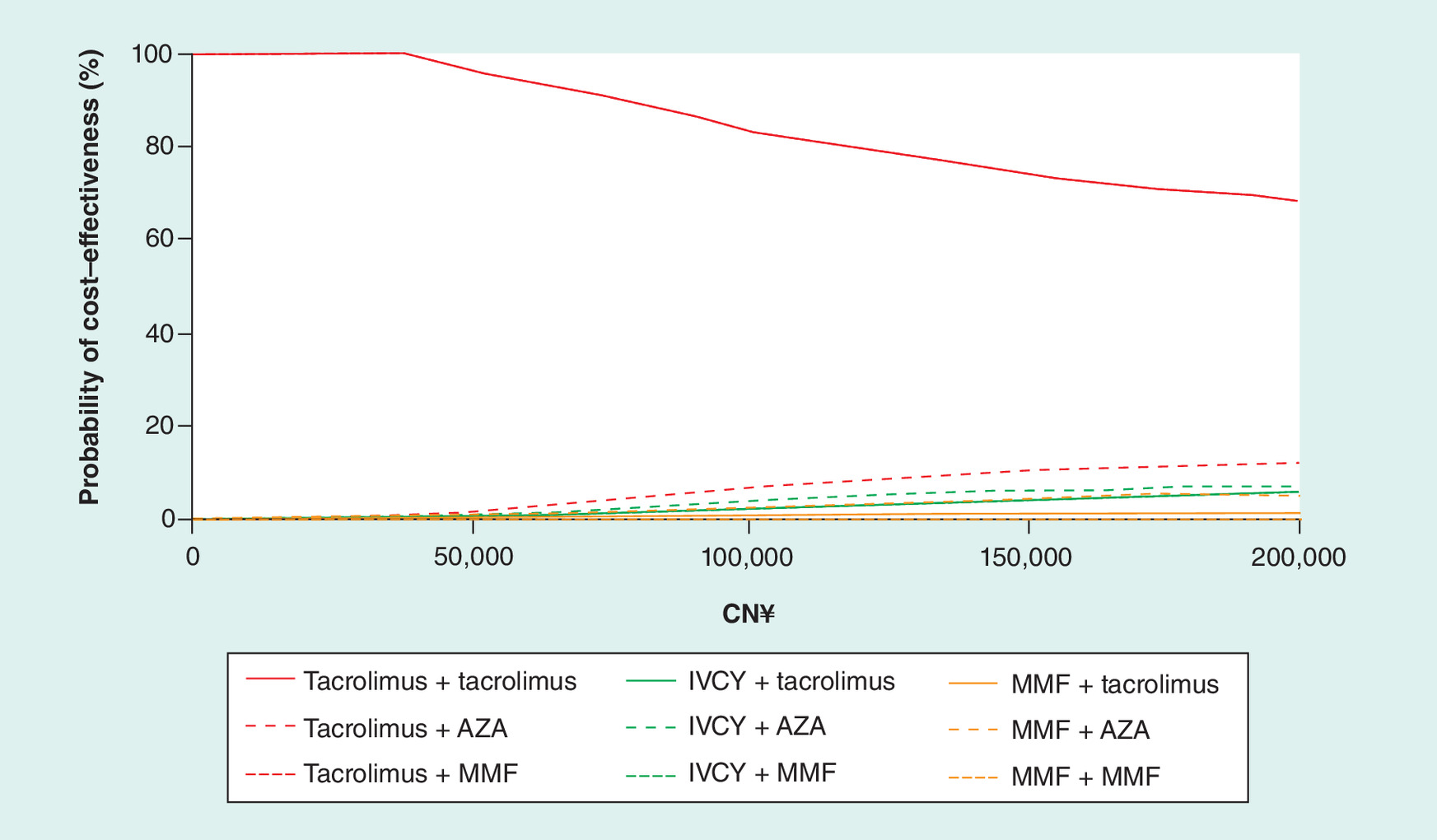
Figure 6. Cost–effectiveness acceptability curve identifying the treatment with the highest net monetary benefit at varying values of willingness-to-pay for a quality-adjusted life year.
AZA: Azathioprine; IVCY: Intravenous cyclophosphamide; MMF: Mycophenolate mofetil; QALY: Quality-adjusted life year.
Discussion
This is the first economic model to assess the lifetime impact of treatment with tacrolimus on moderate-to-severe LN. With the parameters included in this model, rates of complete remission and composite of complete or partial remission, and time to response during induction were predicted to be better with tacrolimus than with IVCY and MMF. Lower relapse rates with tacrolimus than AZA and MMF were also predicted during the maintenance phase. Furthermore, tacrolimus-based induction and maintenance regimens were the most cost-effective of those tested in deterministic and probabilistic analyses. Across a range of willingness-to-pay thresholds, tacrolimus-based induction and maintenance therapy had the greatest probability of being the most cost-effective treatment for moderate-to-severe LN in China versus the comparator regimens.
Our economic model is the first to use a combined decision-tree and Markov model structure to capture the differences between health transitions in the induction and maintenance phases, respectively, for LN treatment. The induction phase of treatment for LN has previously been modeled in two studies. While Mohara et al. used a Markov model with 6-month treatment cycles to assess the value of four treatment regimens for LN in the first year, Wilson et al. used a patient-level simulation with 3-month cycles [33,35]. A decision-tree structure with 3-month cycle length was considered the most appropriate method for representing the transitions in induction therapy in China, in line with feedback from an advisory board comprising a panel of experts in LN from across Asia [unpublished observations]. However, while Wilson et al. applied a time horizon of only 6 months [35], we extended the induction phase up to 18 months to better capture complex transitions between health states and transitions to second-line therapies.
Compared with the induction phase, a Markov structure was chosen to model transitions in the maintenance phase, which is consistent with Mohara et al. and Nee et al. [33,34]. This approach was preferable over a static decision-tree model as it was considered to better represent the time-dependent outcomes associated with LN, and the long time horizon. Due to the structure of the model, most modeled patients were in complete remission when they entered the maintenance phase of treatment. However, patients transitioned to the maintenance phase after 18 months, even if they had not achieved complete remission; although this is not usual in clinical practice, the simplification captures the key outcomes of induction trials.
Our model incorporated similar health states to those previously reported [33–35]. However, other models were limited by only including infection (generally only major infection) as an AE [33–35]. Given that, for example, MMF treatment is associated with a lower incidence of major infection than IVCY, this could skew the outcomes from the models toward lower costs associated with treating AEs, lesser impact of AEs on patient QoL and greater QALYs gained with MMF compared with IVCY regimens [35]. By contrast, our model included infection as well as other AEs that have a significant impact on cost or health outcomes, thereby providing greater reliability in identifying the most cost-effective treatment strategy. Additionally, the tacrolimus efficacy findings with this model are potentially pertinent, as evidence suggests that early disease remission in the induction phase correlates with reduced risk of progression to ESRD [9–11]. While tacrolimus has been associated with more rapid proteinuria reduction compared with standard therapy [22,25], this may be via non-immune mechanisms, such as by reducing glomerular perfusion pressure and stabilizing the podocyte skeleton [62]. The resulting rapid attenuation of proteinuria may impact the complete remission rates reported in clinical trials, and subsequently in this model.
Tacrolimus-based induction and maintenance therapy accrued the lowest total cost and highest QALY gain versus all other comparators. This was supported by the probabilistic analysis, which demonstrated that tacrolimus as induction and maintenance therapy was the most cost-effective regimen at willingness-to-pay thresholds of CN¥54,000–168,000. A higher remission rate during induction was predicted with the tacrolimus-based regimen versus standard treatments for LN; therefore, it may not be surprising that lifetime costs were lower and QALYs gained were higher with tacrolimus-based therapy. Furthermore, sensitivity analyses demonstrated that the rates of remission, as well as the utility values associated with health states, were key drivers of cost–effectiveness, in line with previous reports [33,34]. From a Chinese payer's perspective, these results are encouraging as they suggest that tacrolimus may be effective and the most cost-effective treatment for patients in China with moderate-to-severe LN.
Comparing the results of the current model with those previously developed in LN, some conflicting results were observed. For example, Mohara et al. found that regimens with IVCY as induction and AZA as maintenance therapy were likely to be more effective than MMF as induction and maintenance treatment [33]. Although the results of the current model found the MMF + MMF regimen to be considerably more expensive than IVCY + AZA (ΔCN¥436,873), the health benefits were also greater (Δ0.1 QALYs). This may be due to the hazard ratio of relapse with MMF compared with AZA utilized in this model being lower than the estimates used in the Mohara model (0.44 vs 0.75, respectively) [48,63]. The authors stand by their decision to use this estimate, as it was obtained from a large-scale, longitudinal study into LN with a high proportion of patients of Asian race in the sample [38]. The results of the current model are more aligned with findings from Wilson et al., whose model generally predicted MMF to result in improved QoL compared with IVCY [35].
In general, published treatment guidelines are in agreement with the Kidney Disease: Improving Global Outcomes recommendations, with IVCY or MMF being recommended for patients with class III or IV LN and MMF for the higher classes of disease, with the opportunity to switch to the other induction therapy after treatment failure [6,12,13]. The Chinese Nephrotic Syndrome Immunosuppression Treatment Committee additionally commented that tacrolimus + steroid induction therapy is as effective or superior to an IVCY + steroid regimen [16]. Therefore, the final number of treatment pathways included in the model was deemed to be appropriate to an Asian setting, with this being the first cost–effectiveness model to include tacrolimus as induction and maintenance therapy [33–35].
This study had a number of limitations, most of which were similar to those associated with other cost–effectiveness models. Our approach may be associated with imprecision, the risk of publication bias, inconsistency between studies included in the model, and the need for indirect comparisons between treatments – all of which could impact the output from our model. However, these are common issues in cost–effectiveness studies where database searches/literature analyses are performed. Furthermore, without an assessment of the overall quality of the included studies – for example, by using the Grading of Recommendations, Assessment, Development and Evaluations framework – or an assessment of the heterogeneity between included studies, it is possible that findings regarding relapse and remission rates could be overstated. Reliance on baseline data from randomized clinical trials for predicting clinical outcomes may be insufficient. Clinical trials generally include a selective population, which may not be representative of the entire LN population. Due to lack of reliable, long-term (real world) data for each of the regimens included in the model, we also assumed that clinical effects were time-homogenous (i.e., remission and relapse rates were constant over time). The sensitivity analyses were, therefore, valuable in determining the cost–effectiveness of tacrolimus.
Using an economic model is not as robust as analyzing data from randomized clinical trials and any findings regarding effectiveness should be considered as predictions only. Furthermore, accessing data in Asian countries is complex and limited data are available. Indeed, there were a paucity of data to estimate the relative risk of remission and of long-term data for Asian populations, as well a lack of data and experience in healthcare settings other than China. Our intention is to continue to monitor the literature with a view to updating the literature search (which was performed in 2016) and rerunning the analysis for a future publication. A further limitation was that transition probabilities in the second line of the induction therapy were assumed to be equal to the induction phase, due to a lack of information available to incorporate in the network meta-analysis. Additional research is, therefore, needed on the clinical impact of tacrolimus in the maintenance phase.
The estimates of cost–effectiveness may be conservative with the tacrolimus-based regimens, given that recent evidence suggests a reduced dependence on corticosteroids under tacrolimus therapy [21,22]. As well as the obvious reduction in costs this would incur, the additional benefit of a reduced AE burden by eliminating high-dose steroid use could impact effectiveness estimates compared with the concomitant corticosteroid therapy approach [unpublished findings from the TRUST study, a post-marketing surveillance study of the long-term efficacy and safety of tacrolimus in steroid-resistant LN patients in Japan. However, there was a paucity of available information regarding the effect of chronic tacrolimus maintenance therapy in LN, which should be addressed in prospective long-term clinical trials.
In China, the willingness-to-pay threshold is not well defined. As a proxy for this, the commonly cited one- to three-times nominal GDP per capita was used to estimate net monetary benefit at various thresholds. It should be noted that there is considerable uncertainty in using GDP as a proxy for willingness to pay, both from a theoretical perspective (as has been discussed previously [64,65]) and due to the wide variation in GDP per capita between cities in China. For example, Beijing, Shanghai and Guangzhou have a higher GDP compared with smaller cities. Willingness-to-pay thresholds should, therefore, be interpreted with a degree of caution. The results of this study may also only be generalized to patient populations and settings comparable with those in China, as the structure of healthcare delivery and ethnicity may impact their applicability in other settings. Indeed, the severity of LN affects the choice of treatment regimen and, therefore, the cost of treatment. As this model focused on patients with Class III and IV LN, with or without concomitant Class V disease [31], the findings may not be applicable to patients with other classes of LN where alternative treatment options might be more appropriate.
Conclusion
In the model utilized for this study, tacrolimus appeared to induce complete remission more frequently than current standard therapies, and was associated with a lower rate of loss of composite complete or partial remission than MMF. Tacrolimus as both induction and maintenance therapy versus as the induction drug showed that base case results were most sensitive to utility values and the rate of complete remission during the induction phase. Across all included willingness-to-pay thresholds (up to CN¥200,000), tacrolimus as both induction and maintenance therapy had the highest probability of being cost effective. While results should be interpreted with caution due to a paucity of available evidence for some health state transitions, tacrolimus as both induction and maintenance therapy was found to be the most cost-effective for LN treatment in China.
Future perspective
Demonstrating the steroid-sparing effect of tacrolimus in a large-scale clinical trial could serve to improve the cost–effectiveness of tacrolimus by reducing the drug acquisition costs by approximately CN¥10,000 over the 20-year time horizon, assuming that there is no impact on efficacy.
•
This cost–effectiveness model compared immunosuppressive regimens for moderate-to-severe lupus nephritis (LN) from a Chinese-payer perspective over a 20-year horizon.
•
The model combined a decision-tree/Markov-model structure to map transitions between health states during induction and maintenance treatment phases, respectively.
•
Nine treatment pathways were included, with three possible induction treatments (tacrolimus, intravenous cyclophosphamide or mycophenolate mofetil [MMF]) and three possible maintenance treatments (tacrolimus, azathioprine or MMF).
•
Complete remission rate, composite of complete and partial remission, and time to response in the induction phase predicted with the model were better with tacrolimus than with intravenous cyclophosphamide or MMF.
•
In this model, tacrolimus was associated with lower relapse rates than azathioprine and MMF in the maintenance phase.
•
Regimens including tacrolimus as induction and maintenance therapy incurred the lowest total costs (CN¥180,448) with the highest quality-adjusted life years (11.9) versus the other treatment regimens modeled.
•
Across a range of willingness-to-pay thresholds, tacrolimus as induction and maintenance therapy had the greatest probability of being the most cost-effective treatment for moderate-to-severe LN in China versus the comparator regimens.
•
The model demonstrated that tacrolimus use in both induction and maintenance therapy may be an efficacious and cost-effective treatment for LN in China.
Author contributions
All authors substantially contributed to the conception and design of the work, and the analysis, or interpretation of data for the work. In addition, all authors revised the manuscript critically for important intellectual content.
Acknowledgments
The authors would like to acknowledge TM Chan (Division of Nephrology, Department of Medicine, Queen Mary Hospital, University of Hong Kong) for the advice he has provided regarding this project, and his kind review of the manuscript. The authors would also like to thank T Jiang (David Geffen School of Medicine at University of California, Los Angeles) for his helpful literature search, discussion and review of the manuscript.
Financial & competing interests disclosure
All authors report nonfinancial support from Astellas Pharma, Inc. in the development of this manuscript. This involved assistance from a Medical Writer, funded by Astellas Pharma, Inc., in drafting the initial version of the manuscript under the direction of the authors, and providing editorial support throughout its development. H Jiang, S Kim and AYR Ooi are employees of Astellas. The development of this model was sponsored by Astellas Pharma Singapore. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
DT Draper, PhD, CMPP and A MacLucas, PhD from Cello Health MedErgy assisted in drafting the initial version of the manuscript under the direction of the authors, and provided editorial support throughout its development. Editorial support in the development of this manuscript was funded by Astellas Pharma, Inc.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (suppl_file.docx)
- Download
- 87.29 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
La Paglia GMC, Leone MC, Lepri G et al. One year in review 2017: systemic lupus erythematosus. Clin. Exp. Rheumatol. 35, 551–561 (2017).
2.
Bernatsky S, Boivin J-F, Joseph L et al. Mortality in systemic lupus erythematosus. Arthritis Rheum. 54, 2550–2557 (2006).
3.
Saxena R, Mahajan T, Mohan C. Lupus nephritis: current update. Arthritis Res. Ther. 13, 240 (2011).
4.
Yap DYH, Chan TM. Treatment of lupus nephritis: practical issues in Asian countries. Int. J. Rheum. Dis. 18, 138–145 (2015).
5.
Mok CC. Epidemiology and survival of systemic lupus erythematosus in Hong Kong Chinese. Lupus. 20, 767–771 (2011).
6.
Bertsias GK, Tektonidou M, Amoura Z et al. Joint European League Against Rheumatism and European Renal Association-European Dialysis and Transplant Association (EULAR/ERA-EDTA) recommendations for the management of adult and paediatric lupus nephritis. Ann. Rheum. Dis. 71, 1771–1782 (2012).
7.
Zhao W, Zhang L, Han S et al. Cost analysis of living donor kidney transplantation in China: a single-center experience. Ann. Transplant. 17, 5–10 (2012).
8.
Yap DYH, Tang CSO, Ma MKM, Lam MF, Chan TM. Survival analysis and causes of mortality in patients with lupus nephritis. Nephrol. Dial. Transplant. 27, 3248–3254 (2012).
9.
Fiehn C, Hajjar Y, Mueller K, Waldherr R, Ho AD, Andrassy K. Improved clinical outcome of lupus nephritis during the past decade: importance of early diagnosis and treatment. Ann. Rheum. Dis. 62, 435–439 (2003).
10.
Fiehn C. Early diagnosis and treatment in lupus nephritis: how we can influence the risk for terminal renal failure. J. Rheumatol. 33, 1464–1466 (2006).
11.
Houssiau FA, Vasconcelos C, D'Cruz D et al. Early response to immunosuppressive therapy predicts good renal outcome in lupus nephritis: lessons from long-term followup of patients in the Euro-Lupus Nephritis Trial. Arthritis Rheum. 50, 3934–3940 (2004).
12.
Hahn BH, McMahon MA, Wilkinson A et al. American College of Rheumatology guidelines for screening, treatment, and management of lupus nephritis. Arthritis Care Res. 64, 797–808 (2012).
13.
Kidney Disease: Improving Global Outcomes (KDIGO). KDIGO clinical practice guideline for glomerulonephritis. Kidney Int. Suppl. 2, 139–274 (2012).
14.
Moya FB, Pineda Galindo LF, García de la Peña M. Impact of chronic glucocorticoid treatment on cardiovascular risk profile in patients with systemic lupus erythematosus. J. Clin. Rheumatol. 22, 8–12 (2016).
15.
Lightstone L, Doria A, Wilson H, Ward FL, Larosa M, Bargman JM. Can we manage lupus nephritis without chronic corticosteroids administration? Autoimmun. Rev. 17, 4–10 (2018).
• Review article highlighting that the side effects associated with corticosteroid treatment for lupus nephritis might be minimized by tapering corticosteroids in patients achieving a stable renal remission.
16.
Chinese Nephrotic Syndrome Immunosuppression Treatment Committee. Expert consensus on adult nephrotic syndrome immunosuppressive therapy. Chin. J. Nephrol. 30, 467–474 (2014).
17.
Chan TM. Treatment of severe lupus nephritis: the new horizon. Nat. Rev. Nephrol. 11, 46–61 (2015).
•• Review of evidence supporting the standard of care immunosuppressive treatments, including the use of calcineurin inhibitors, and emerging therapies for the treatment of severe lupus nephritis.
18.
Mok CC, Yap DY, Navarra SV et al. Overview of lupus nephritis management guidelines and perspective from Asia. Nephrology 19, 11–20 (2014).
19.
Chen Y, Sun J, Zou K, Yang Y, Liu G. Treatment for lupus nephritis: an overview of systematic reviews and meta-analyses. Rheumatol. Int. 37, 1089–1099 (2017).
•• Systematic review of the treatment options for lupus nephritis, including the role of tacrolimus as induction therapy.
20.
Palmer SC, Tunnicliffe DJ, Singh-Grewal D et al. Induction and maintenance immunosuppression treatment of proliferative lupus nephritis: a network meta-analysis of randomized trials. Am. J. Kidney Dis. 70, 324–336 (2017).
21.
Borrows R, Loucaidou M, Van Tromp J et al. Steroid sparing with tacrolimus and mycophenolate mofetil in renal transplantation. Am. J. Transplant. 4, 1845–1851 (2004).
22.
Li X, Li H, Chen J et al. Tacrolimus as a steroid-sparing agent for adults with steroid-dependent minimal change nephrotic syndrome. Nephrol. Dial. Transplant. 23, 1919–1925 (2008).
• Prospective, open-label cohort study demonstrating that 24 weeks of tacrolimus therapy was effective and steroid-sparing for Chinese adults with steroid dependent minimal change nephrotic syndrome.
23.
Mok CC, Tong KH, To CH, Siu YP, Au TC. Tacrolimus for induction therapy of diffuse proliferative lupus nephritis: an open-labeled pilot study. Kidney Int. 68, 813–817 (2005).
24.
Yap DYH, Ma MKM, Mok MMY, Kwan LPY, Chan GCW, Chan TM. Long-term data on tacrolimus treatment in lupus nephritis. Rheumatology 53, 2232–2237 (2014).
25.
Chen W, Tang X, Liu Q et al. Short-term outcomes of induction therapy with tacrolimus versus cyclophosphamide for active lupus nephritis: a multicenter randomized clinical trial. Am. J. Kidney Dis. 57, 235–244 (2011).
26.
Singh JA, Hossain A, Kotb A, Wells GA. Comparative effectiveness of immunosuppressive drugs and corticosteroids for lupus nephritis: a systematic review and network meta-analysis. Syst. Rev. 5, 155 (2016).
• Systematic review and network meta-analysis of trials of immunosuppressive drugs and corticosteroids in patients with lupus nephritis.
27.
Mok CC, Ying KY, Yim CW et al. Tacrolimus versus mycophenolate mofetil for induction therapy of lupus nephritis: a randomised controlled trial and long-term follow-up. Ann. Rheum. Dis. 75, 30–36 (2016).
•• Randomized, controlled, parallel-group study demonstrating non-inferiority of tacrolimus to mycophenolate mofetil, when combined with prednisolone, for induction therapy of active lupus nephritis.
28.
Webster P, Wardle A, Bramham K, Webster L, Nelson-Piercy C, Lightstone L. Tacrolimus is an effective treatment for lupus nephritis in pregnancy. Lupus. 23, 1192–1196 (2014).
29.
Kraaij T, Bredewold OW, Trompet S et al. TAC-TIC use of tacrolimus-based regimens in lupus nephritis. Lupus Sci. Med. 3, e000169 (2016).
30.
Clarke AE, Panopalis P, Petri M et al. SLE patients with renal damage incur higher health care costs. Rheumatology 47, 329–333 (2008).
31.
Weening JJ, D'Agati VD, Schwartz MM et al. The classification of glomerulonephritis in systemic lupus erythematosus revisited. Kidney Int. 65, 521–530 (2004).
32.
Chen W, Liu Q, Chen W et al. Outcomes of maintenance therapy with tacrolimus versus azathioprine for active lupus nephritis: a multicenter randomized clinical trial. Lupus. 21, 944–952 (2012).
33.
Mohara A, Pérez Velasco R, Praditsitthikorn N, Avihingsanon Y, Teerawattananon Y. A cost-utility analysis of alternative drug regimens for newly diagnosed severe lupus nephritis patients in Thailand. Rheumatology 53, 138–144 (2014).
34.
Nee R, Rivera I, Little DJ, Yuan CM, Abbott KC. Cost-utility analysis of mycophenolate mofetil versus azathioprine based regimens for maintenance therapy of proliferative lupus nephritis. Int. J. Nephrol. 2015, 917567 (2015).
35.
Wilson ECF, Jayne DRW, Dellow E, Fordham RJ. The cost–effectiveness of mycophenolate mofetil as firstline therapy in active lupus nephritis. Rheumatology 46, 1096–1101 (2007).
36.
Li X, Ren H, Zhang Q et al. Mycophenolate mofetil or tacrolimus compared with intravenous cyclophosphamide in the induction treatment for active lupus nephritis. Nephrol. Dial. Transplant. 27, 1467–1472 (2012).
37.
Liu Z, Zhang H, Liu Z et al. Multitarget therapy for induction treatment of lupus nephritis: a randomized trial. Ann. Intern. Med. 162, 18–26 (2015).
38.
Wang J, Hu W, Xie H et al. Induction therapies for class IV lupus nephritis with non-inflammatory necrotizing vasculopathy: mycophenolate mofetil or intravenous cyclophosphamide. Lupus. 16, 707–712 (2007).
39.
Bao H, Liu Z-H, Xie H-L, Hu W-X, Zhang H-T, Li L-S. Successful treatment of class V+IV lupus nephritis with multitarget therapy. J. Am. Soc. Nephrol. 19, 2001–2010 (2008).
40.
Appel GB, Contreras G, Dooley MA et al. Mycophenolate mofetil versus cyclophosphamide for induction treatment of lupus nephritis. J. Am. Soc. Nephrol. 20, 1103–1112 (2009).
41.
El-Shafey EM, Abdou SH, Shareef MM. Is mycophenolate mofetil superior to pulse intravenous cyclophosphamide for induction therapy of proliferative lupus nephritis in Egyptian patients? Clin. Exp. Nephrol. 14, 214–221 (2010).
42.
Feng X, Gu F, Chen W et al. Mizoribine versus mycophenolate mofetil or intravenous cyclophosphamide for induction treatment of active lupus nephritis. Chin. Med. J. 127, 3718–3723 (2014).
43.
Rathi M, Goyal A, Jaryal A et al. Comparison of low-dose intravenous cyclophosphamide with oral mycophenolate mofetil in the treatment of lupus nephritis. Kidney Int. 89, 235–242 (2016).
44.
Grootscholten C, Ligtenberg G, Hagen EC et al. Azathioprine/methylprednisolone versus cyclophosphamide in proliferative lupus nephritis. A randomized controlled trial. Kidney Int. 70, 732–742 (2006).
45.
Austin HA, Illei GG, Braun MJ, Balow JE. Randomized, controlled trial of prednisone, cyclophosphamide, and cyclosporine in lupus membranous nephropathy. J. Am. Soc. Nephrol. 20, 901–911 (2009).
46.
Kiefer C, Sturtz S, Bender R. Indirect comparisons and network meta-analyses estimation of effects in the absence of head-to-head trials – part 22 of a series on evaluation of scientific publications. Dtsch. Arztebl. Int. 112, 803–808 (2015).
47.
Chan TM, Tse KC, Tang CSO, Lai KN, Li FK. Long-term outcome of patients with diffuse proliferative lupus nephritis treated with prednisolone and oral cyclophosphamide followed by azathioprine. Lupus 14, 265–272 (2005).
48.
Dooley MA, Jayne D, Ginzler EM et al. Mycophenolate versus azathioprine as maintenance therapy for lupus nephritis. N. Engl. J. Med. 365, 1886–1895 (2011).
49.
Takeuchi T, Wakasugi N. Long-term safety and efficacy of tacrolimus for lupus nephritis patients in real-world setting – results from 5 year interim analysis of post marketing surveillance of 1376 patients in Japan [presentation]. In: American College of Rheumatology/Association of Rheumatology Health Professionals annual meeting, (2015). Abstract 1795.
•• Five-year interim analysis of post-marketing surveillance data demonstrating that tacrolimus therapy was generally tolerable and effective for the treatment of lupus nephritis in Japan.
50.
Zhang X, Liu S, Li Y, Wang Y, Tian M, Liu G. Long-term effectiveness and cost–effectiveness of metformin combined with liraglutide or exenatide for type 2 diabetes mellitus based on the CORE diabetes model study. PLoS ONE 11, e0156393 (2016).
51.
WHO. Global Health Observatory data repository. Life tables by country China. http://apps.who.int/gho/data/?theme=main&vid=60340
52.
Bavanandan S, Yap Y-C, Ahmad G, Wong H-S, Azmi S, Goh A. The cost and utility of renal transplantation in Malaysia. Transplant. Direct. 1, e45 (2015).
53.
Lenert LA, Sturley AP, Rapaport MH, Chavez S, Mohr PE, Rupnow M. Public preferences for health states with schizophrenia and a mapping function to estimate utilities from positive and negative symptom scale scores. Schizophr. Res. 71, 155–165 (2004).
54.
Chau D, Becker DL, Coombes ME, Ioannidis G, Adachi JD, Goeree R. Cost–effectiveness of denosumab in the treatment of postmenopausal osteoporosis in Canada. J. Med. Econ. 15(Suppl. 1), 3–14 (2012).
55.
Nafees B, Stafford M, Gavriel S, Bhalla S, Watkins J. Health state utilities for non small cell lung cancer. Health Qual. Life Outcomes. 6, 84 (2008).
56.
Tsuchiya T, Fukuda T, Furuiye M, Kawabuchi K. Pharmacoeconomic analysis of consolidation therapy with pemetrexed after first-line chemotherapy for non-small cell lung cancer. Lung Cancer 74, 521–528 (2011).
57.
Sonnenberg FA, Burkman RT, Hagerty CG, Speroff L, Speroff T. Costs and net health effects of contraceptive methods. Contraception 69, 447–459 (2004).
58.
Kidney Service China. Kidney dialysis in China (2019). http://www.kidneyservicechina.com/dialysis-kidney-disease/2686.html
59.
Xiaoming P, Heli X, Chenguang D, Hua L, Guozhen C, Tianci B. Cost of two different therapies for end-stage renal disease in northwest China. J. Med. Coll. PLA 27, 80–86 (2012).
60.
Mo X, Gai Tobe R, Wang L et al. Cost–effectiveness analysis of different types of human papillomavirus vaccination combined with a cervical cancer screening program in mainland China. BMC Infect. Dis. 17, 502 (2017).
61.
Shao H, Zhai S, Zou D et al. Cost–effectiveness analysis of dapagliflozin versus glimepiride as monotherapy in a Chinese population with type 2 diabetes mellitus. Curr. Med. Res. Opin. 33, 359–369 (2017).
62.
Ayoub I, Nelson J, Rovin BH. Induction therapy for lupus nephritis: the highlights. Curr. Rheumatol. Rep. 20, 60 (2018).
63.
Houssiau FA, D'Cruz D, Sangle S et al. Azathioprine versus mycophenolate mofetil for long-term immunosuppression in lupus nephritis: results from the MAINTAIN Nephritis Trial. Ann. Rheum. Dis. 69, 2083–2089 (2010).
64.
Marseille E, Larson B, Kazi DS, Kahn JG, Rosen S. Thresholds for the cost–effectiveness of interventions: alternative approaches. Bull. World Health Organ. 93, 118–124 (2015).
65.
Bertram MY, Lauer JA, De Joncheere K et al. Cost–effectiveness thresholds: pros and cons. Bull. World Health Organ. 94, 925–930 (2016).
Information & Authors
Information
Published In
Pages: 1125 - 1141
PubMed: 31580156
Copyright
© 2019 Hongsi Jiang. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 16 October 2018
Accepted: 8 August 2019
Published online: 3 October 2019
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Cost–effectiveness of tacrolimus for the treatment of moderate-to-severe lupus nephritis in China. (2019) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2018-0111
Export citation
Select the citation format you wish to export for this article or chapter.