Commonly used definitions in real-world studies may underestimate the prevalence of renal disease among nonvalvular atrial fibrillation patients
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To describe comorbidities among treated nonvalvular atrial fibrillation (NVAF) patients and assess the impact of using different time (‘look back’ windows) on the prevalence estimates. Patients & methods: We included all adult nonvalvular atrial fibrillation patients newly initiating treatment in the Clinical Practice Research Datalink. Comorbidities included in the Charlson Comorbidity Index were defined using an all available, 3- and 1-year look back window before the start of treatment. Results: The prevalence of comorbidities was high and increased when using longer look back windows; the largest difference was observed for renal disease (+15.6%). Conclusion: Our findings emphasize the importance of using all available data when characterizing chronic conditions and highlights the high comorbidity burden in this population.
Atrial fibrillation (AF) is the most common sustained cardiac arrhythmia and is characterized by uncoordinated atria activation with a resulting decline of atrial mechanical function [1]. Patients with AF have an approximately five-times increased risk of experiencing ischemic stroke compared with patients without the condition [1,2], and all-cause mortality is around twice as high [3]. In Europe, the estimated prevalence of AF is between 1.5 and 2.0% [4]; this increases to 10–17% in those 80 years of age or older [5].
As the AF population tends to be elderly, they often present with multiple comorbidities [6–8]. Comorbidities that are particularly common in patients with AF include cardiovascular conditions such as hypertension, which is considered an important modifiable risk factor for AF [5] and heart failure, which coexists in 13–25% of AF patients [9–13]. There is also a strong association between AF and chronic kidney disease (CKD), with the prevalence of AF estimated to be as high as 13–27% in patients on hemodialysis [14]. Patients with incident AF have been estimated to have a 67% increased risk of developing end-stage renal disease compared with those without AF [15], highlighting that renal disease is both a cause and consequence of AF [16].
A high comorbidity burden may make it more challenging to achieve adequate anticoagulation control [17]. A recent study using data from the UK Biobank reported increasing mortality rates among patients with AF with an increasing number of comorbidities, and suggested that the restricted number of comorbidities included in the CHADS2VASC score may mean that these patients are not treated effectively [7].
Because of these challenges, accurate descriptions of the comorbidity prevalence among patients receiving oral anticoagulants (OACs) are important. However, when using so called ‘real-world’ data sources, there are a number of methodological choices which can greatly impact the estimated burden of comorbidities. These include the diagnostic codes used to define the conditions, but also the time window during which comorbidities are assessed. Many studies specify a minimum of 1-year time window, a so called ‘look back window’, during which the presence of a diagnostic codes for the condition is taken to indicate presence of the disease. However, depending on the nature of the specific chronic condition, patients may not necessarily have a healthcare encounter recorded in this time frame. This is a particular concern for patients with chronic conditions who may not interact regularly with a healthcare provider, and the application of a short look back window may in these instances lead to an underestimate of disease prevalence [18–21].
We aimed to assess the prevalence of common comorbidities among treated nonvalvular atrial fibrillation (NVAF) patients in the UK using a range of different look back windows. We restricted our analyses to NVAF patients as the recently developed direct oral anticoagulants are approved for use in this population specifically. This has resulted in an increased number of publications focusing on real-world evaluations of comparative effectiveness specifically in the NVAF population, and these studies rely on accurate assessments of comorbidities. Our objectives were twofold; first, to accurately describe the comorbidity burden among treated NVAF patients in the UK, and second, to describe the impact of using short look back windows on disease prevalence in this population.
Patients & methods
Data source
Data were obtained from a UK primary care database, the Clinical Practice Research Datalink (CPRD), which includes longitudinal data from general practices that are representative of the UK population [22]. These data were linked to secondary care data from the Inpatient and Outpatient Hospital Episode Statistics (HES) database and mortality data from the Office for National Statistics (ONS).
Inclusion & exclusion criteria
This was a retrospective cohort study that included patients with a diagnosis of AF who initiated treatment between 1 December 2012 and 1 July 2017. The index date was defined as the date of first the OAC prescription. Patients were identified as nonvalvular if they had no prior diagnosis of mitral stenosis or a procedural code for mechanical heart valve replacement. Patients were also required to be 18 years or older at index date and have at least 1 year of baseline data (available time-period prior to index date). In addition, patients were required to have no diagnosis of venous thromboembolism in the 3 months prior. The selection of the cohort has been described in detail elsewhere [23].
Comorbidities of interest
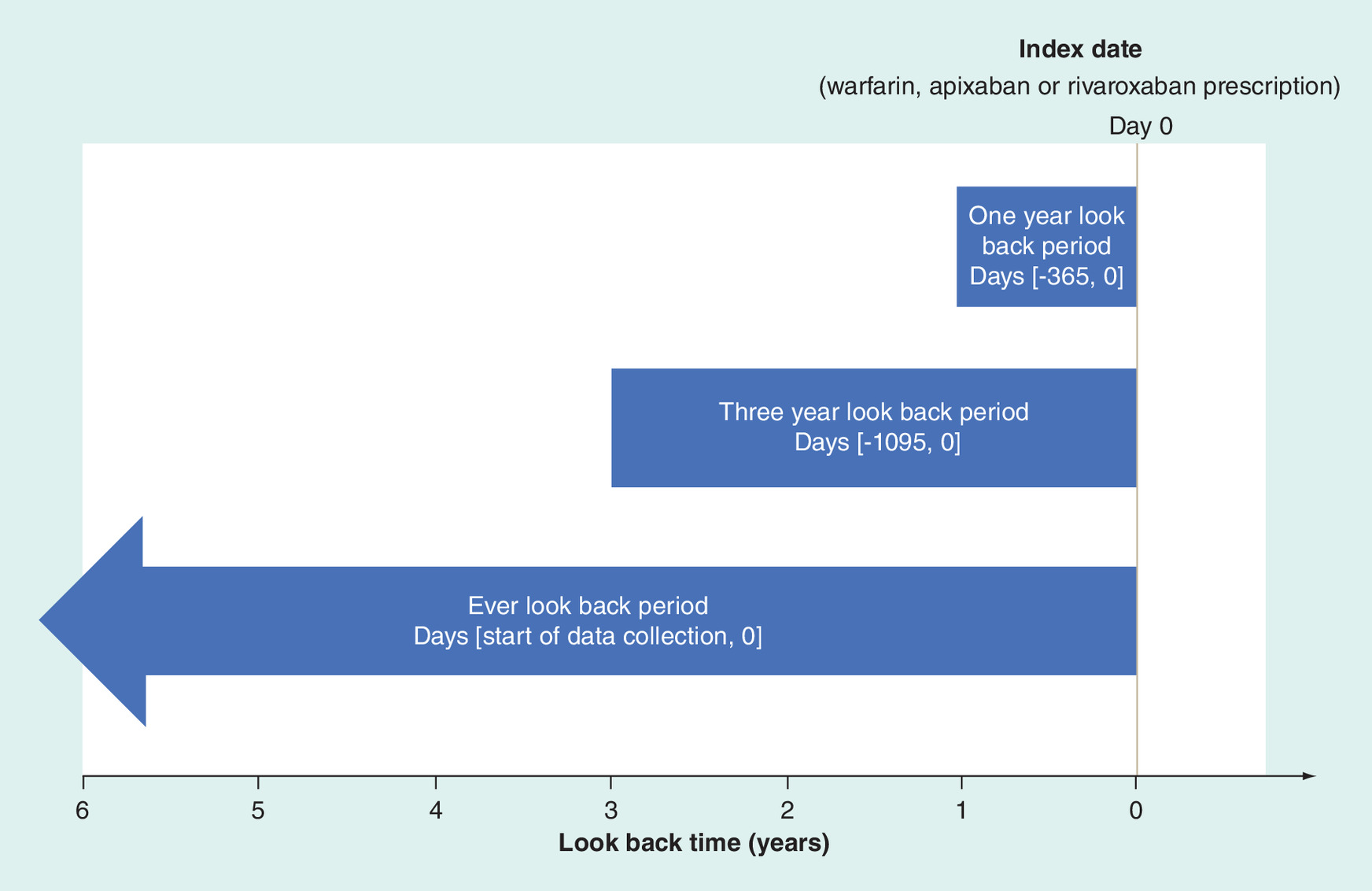
For the purposes of describing comorbidities, we focused on the comorbidities included in the Charlson Comorbidity Index (CCI), a commonly used score which summarizes the comorbidity burden in a population. All conditions were identified using READ and/or ICD-10 diagnoses codes. The comorbidities included in the CCI are myocardial infarction, congestive heart failure, peripheral vascular disease, dementia, chronic pulmonary disease, rheumatic disease, peptic ulcer disease, mild liver disease, diabetes with chronic complications, diabetes without chronic complications, hemiplegia and paraplegia, renal disease, any malignancy, moderate or severe liver disease, metastatic solid tumor and acquired AIDS/HIV. These were identified in three different look back windows including an ever (all available data), 3- and 1-year look back, as illustrated in Figure 1.
CCI scores were estimated using weights applied in the updated and validated methods described by Quan et al. 2011 [24].
Analytical methods
The prevalence of comorbidities was presented as number and percentages. CCI was described using median, interquartile range (IQR), and minimum-maximum for the continuous score, and as number and percentages for each category (0, 1, 2, 3, 4+). The analyses were descriptive in nature and no statistical tests were performed. All analyses were conducted using SAS v9.4 and Stata 11.
Results
In total, 15,860 patients were included. The median age was 77 years (IQR: 14) and 7134 (45.0%) of the patients were female. A detailed description of the demographic characteristics of the apixaban and warfarin patients in this population have been previously published [23]. The cumulative prevalence of the comorbidities can be seen in Figure 2.
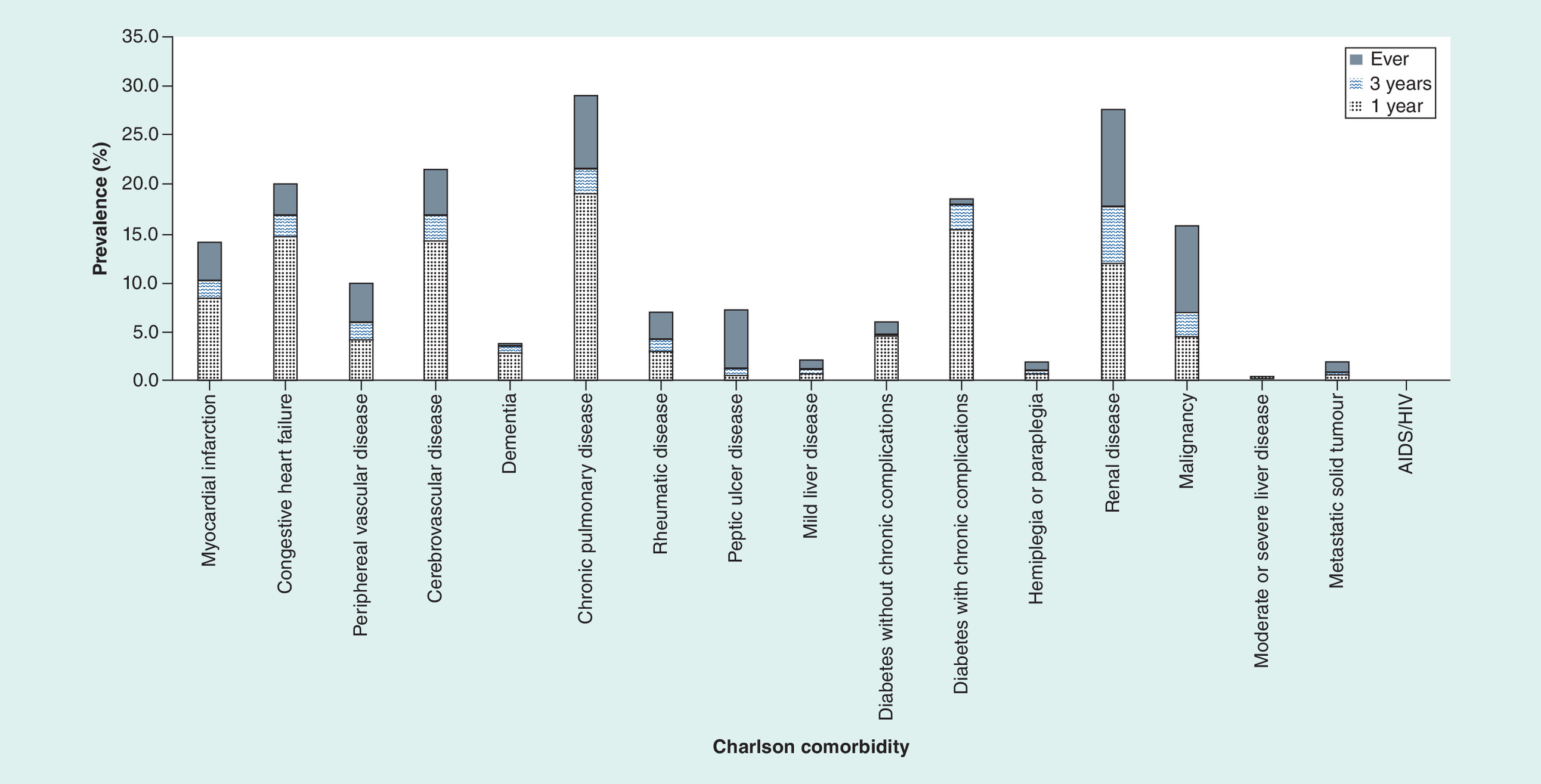
Using a 1-year look back window, the three most common comorbidities were chronic pulmonary disease (19.2%), diabetes with chronic complications (15.5%) and congestive heart failure (14.7%). When applying a 3-year look back, chronic pulmonary disease and diabetes with chronic complications were still the most common conditions, at 21.7 and 18.0% respectively. However, the third most common condition changed to renal disease (17.9%), which increased in prevalence by a relatively large amount when applying the longer look back window (+5.9%). Using an ever look back window, the most common comorbidity was still chronic pulmonary disease (29.1%), followed by renal disease (27.6%). The third most common comorbidity was now cerebrovascular disease with at 21.7%.
The prevalence of all comorbidities was, as expected given the definitions, higher when using an ever look back window compared with one and 3-year periods (Figure 2). One exception to this was observed for diabetes without complications; the prevalence of this condition decreased slightly between the 1- and 3-year periods (-1.2%). The largest absolute increases in prevalence when applying the longer look back windows were observed for renal disease (+5.9 and +15.6% using a 3-year and ever look back, respectively), followed by malignancy (+2.5% and +11.4% for 3-year and ever look backs). The third largest increase was observed for cerebrovascular disease (+2.7%) when using a 3-year look back, and for chronic pulmonary disease (+9.9%) when using an ever look back window.
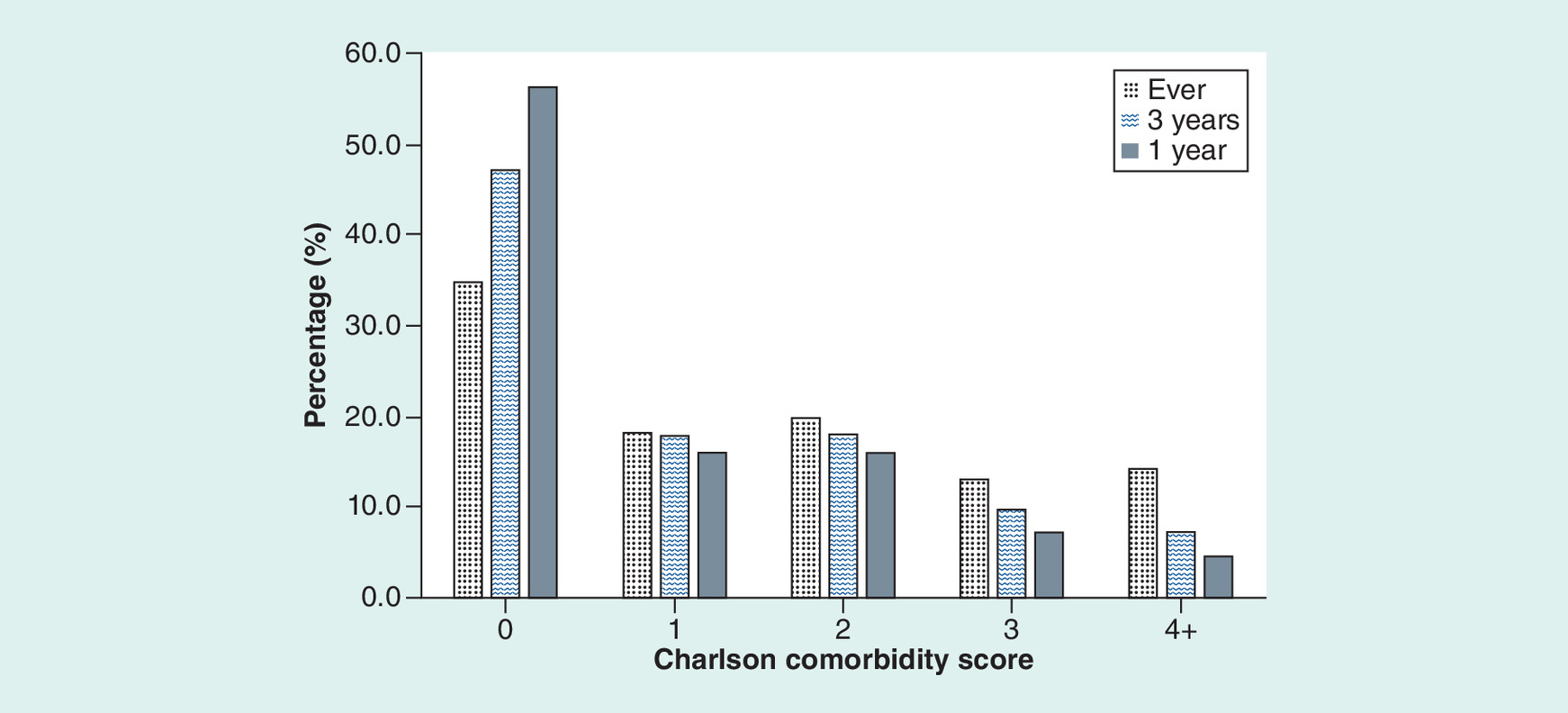
Median CCI scores did not vary markedly using different look back windows, increasing slightly from 0 (IQR = 0–2) to 1 (IQR = 0–2) and 1 (IQR = 0–3) using a 1 year compared with a 3 year and ever look back. The percentage of patients that had a CCI score >0 increased from 46.3% using a 1-year look back window to 69.0% using an ever look back (Figure 3).
Discussion
In this study of treated NVAF patients in the UK, the burden of different comorbidities was high. The most common comorbidities varied depending on the look back window applied; when using an ever look back period chronic pulmonary disease was most common, followed by renal disease and cerebrovascular disease. The prevalence of all comorbidities apart from diabetes without complications increased with longer look back windows, with the largest increases observed for renal disease, malignancies, cerebrovascular disease and chronic pulmonary disease. In real-world data, short look back windows are often applied, either out of necessity or study design choice. They are particularly common in US insurance claims databases, where the rate of patient disenrollment can be high [25]. Our findings emphasize that when a shorter look back window is used, the prevalence of some chronic conditions may be underestimated. In our population of NVAF patients using UK CPRD/HES linked data; this was particularly marked for renal disease; as well as for malignancies, cerebrovascular disease and chronic pulmonary disease.
There are several possible explanations for the increase in prevalence of chronic conditions we observed when extending the look back window. In CPRD, diagnostic Read codes tend to be entered only once upon the initial diagnosis. It is possible that the extension of the look back window allows us to capture more initial instances of a diagnosis, particularly if follow-up visits are entered using less specific codes. This would have less of an impact for more severe patients treated in secondary care, as the relevant ICD-10 codes are re-entered in HES. For renal disease, it is also feasible that the patients with mild disease are seen relatively infrequently, as current guidelines only recommend frequent monitoring for more severe patients [26]. Other comorbidities, which were particularly affected by the increased look back window, were malignancies, cerebrovascular disease and chronic pulmonary disease. All of these conditions showed relatively modest increases in prevalence with the extension of the look back window from 1 to 3 year, at just under a 3% increase, but larger increases when extending the look back further to all available data. It is feasible that we are capturing some historical diagnoses from which patient may no longer require frequent care due to having completed treatment. The appropriateness of including these diagnoses when describing patient characteristics at a particular time point will depend on the study aim. Regarding the decrease in prevalence observed for diabetes without complications, this is likely due to the fact that more patients are characterized has having complications with the extension of the look back window, and consequently recategorized from diabetes without complication to diabetes with complications.
We are not alone in describing the impact of the look back period on prevalence estimates in pharmacoepidemiological studies [18,20,27–29]. Rassen et al. recently investigated the impact of varying look back windows on incidence and prevalence estimates in a UK (CPRD) and US (MarketScan) database, and described increased prevalence of 4.3- to 8.3- times higher in CPRD depending on the disease, and an 1.8- to 2.4-times higher prevalence in MarketScan [20]. This is in line with findings reported by Ekstrom and colleagues, who found marked increases in the estimated prevalence, coupled with decreased incidence estimates, of different diseases when expanding the look back periods using Swedish registry data [30]. Although the impact of using a short look back window on absolute risk estimates is marked and consistently reported across the literature, the consequent impact of this on relative effect estimates appears more varied [21,27–29,31]. This is likely due to multiple factors, including the strength of any potential confounding path and whether the look back windows are differential or nondifferential between treatment groups [28].
Our study has a number of limitations. First, the comorbidities estimated in this study are only reflective of NVAF patients treated with OACs. However, the majority of NVAF patients are expected to be treated with OACs in the UK, and this number is increasing over time. A UK study estimated in 2015–2016 that 73.9% of NVAF patients initiated anticoagulation therapy at diagnosis [32]. Nonetheless, by restricting the population to treated NVAF patients certain patient groups may be under represented; specifically patients who are slightly younger, and those with fewer comorbidities [32]. This should be borne in mind as a limitation regarding the generalizability of our results.
Second, prevalence estimates using administrative data are sensitive to the coding practices within the relevant healthcare system, which may change over time. Although the validity of the CPRD is considered to be high [33], here are examples of diagnoses being under recorded in both CPRD and HES for certain conditions [34,35]. In the UK, the Quality and Outcomes Framework (QOF) has incentivized recording of CKD in primary care based on two estimated glomerular filtration rate (eGFR) measurements <60 ml/min/1.73 m2 [36]. However, prior studies have found that a relatively large proportion of patients meeting biochemical criteria for CKD could lack appropriate Read Codes. A recent analysis of data from the National Chronic Kidney Disease Audit found that 30% of patients with biochemical CKD, as defined by creatinine measures, lacked a Read Code for Stage 3–5 CKD; however, this varied between 4 and 100% on a practice level [36]. Nonetheless, the percentage of patients who had codes for other renal disorders, dialysis or a kidney transplant was higher. The prevalence of renal disease in the ever look back period in our study (27.6%) is comparable with the range of renal disease prevalence in the NVAF population in the literature; including studies utilizing biochemical criteria (22.2–35.5%) [37–39]. This implies that the prevalence of renal disease may be more accurately estimated in CPRD/HES data when an ever look back is applied and codes indicating unspecific renal disease, as opposed to staged CKD, are used. To increase the accuracy of prevalence estimates of renal disease in this data, it might have been appropriate to identify renal disease using estimated glomerular filtration rate (eGFR) results tests, as adopted in previous real-world studies [37–39]. This is because eGFR tests are expected to be frequently recorded in the data, as physicians are recommended to conduct a test if patients experience a change in treatment or development of a comorbidity [40]. Recently published data [23] indicate that the use of diagnostic codes and a short look back window in isolation could underestimate the prevalence of renal dysfunction, compared with additionally using laboratory test results
Using treatments to identify conditions in addition to diagnostic codes might also have mitigated the impact of varying the look back window for some conditions, for example diabetes. However, for those conditions where the largest increases in prevalences were observed – renal disease and malignancies – treatment information would be difficult to utilize. For renal disease, this is because the relevant prescription drugs such as ACE-inhibitors have multiple indications, and chemotherapy treatments which could be used to indicate active treatment for a malignancy are not recorded within either CPRD or HES. Other limitations of our study include the potentially reduced generalizability due to HES linkage only being available for English practices and the potential for erroneous recording of data. We also acknowledge that the accuracy of the prevalence estimates is a direct reflection of the accuracy of the code lists, which, although based on a publication [24], have not been specifically validated within CPRD. Strengths of our study includes the large sample size and the primary and secondary care linkage, which allowed us to capture diagnoses in multiple settings.
Conclusion
Our study describes a high comorbidity burden among NVAF patients newly initiating treatment in England, with chronic pulmonary disease present among almost one in three patients and renal disease in more than one in four. The estimated prevalence of several conditions, most notably renal disease and malignancies, increased markedly when using an all available compared with a 1-year look back window. Our findings highlight the importance of utilizing longer look back windows when estimating the prevalence of chronic conditions in the NVAF population and emphasizes the high comorbidity burden among these patients.
•
Characterizing comorbidities among nonvalvular atrial fibrillation patients is important, as a high comorbidity burden may negatively impact anticoagulation control and has been linked to increase mortality.
•
Real-world studies aiming to describe comorbidity burdens face numerous methodological choices when defining comorbidities. One of these involves the specification of a so called ‘look back window’. This is the amount of time before the start of follow-up used to define the presence or absence of a disease. Most studies specify a minimum of a 1-year look back window.
•
We used data from the Clinical Practice Research Datalink linked to Hospital Episode Statistics to describe the comorbidity burden among treated NVAF patients in the UK using different look back windows.
•
The prevalence of comorbidities was high, and comorbidity prevalence increased when using longer look back windows. The largest difference was observed for renal disease (+15.6%), followed by malignancies (+11.4%).
•
Although the impact of extending look back windows on prevalence estimates has been shown in previous studies, our findings highlights the impact this can have within RW studies in the NVAF population and emphasizes the high comorbidity burden in this population.
Author contributions
All authors met the four standards for Authorship Credit as published in the Future Science Group Author Disclosure Form, and contributed sufficiently to the work to take responsibility for the article content.
Acknowledgments
We would like to acknowledge the contribution of Robert Donaldson of Evidera, who assisted with the creation of the analytical files.
Financial & competing interests disclosure
This study was sponsored by Bristol Myers-Squibb. S Ramagopalan and F Mehmud are employees of Bristol Myers-Squibb and hold stock options in Bristol Myers-Squibb. A Schultze, S Graham and B Nordstrom are salaried employees of Evidera and are prohibited from accepting remuneration of any sort from clients of Evidera. Evidera received funding from Bristol Myers-Squibb to conduct this study. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The authors state that the study was conducted in accordance with the ethical principles that have their origin in the Declaration of Helsinki, that are consistent with the current guidelines for International Society for Pharmacoepidemiology (ISPE) Good Pharmacoepidemiology Practices (GPP), and in accordance with local applicable laws and regulations. The protocol and proposed conduct of cohort study were approved by the Independent Scientific Advisory Committee (ISAC; 17_188).
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
References
1.
European Society of Cardiology (Esc). Atrial Fibrillation 2016 (Management of). ESC Clinical Practice Guidelines. 2019 (12 April), (2016). https://www.escardio.org/Guidelines/Clinical-Practice-Guidelines/Atrial-Fibrillation-Management
2.
Stewart S, Hart CL, Hole DJ, Mcmurray JJ. A population-based study of the long-term risks associated with atrial fibrillation: 20-year follow-up of the Renfrew/Paisley study. Am. J. Med. 113(5), 359–364 (2002).
3.
Wolf PA, Abbott RD, Kannel WB. Atrial fibrillation as an independent risk factor for stroke: the Framingham Study. Stroke 22(8), 983–988 (1991).
4.
Ruddox V, Sandven I, Munkhaugen J, Skattebu J, Edvardsen T, Otterstad JE. Atrial fibrillation and the risk for myocardial infarction, all-cause mortality and heart failure: a systematic review and meta-analysis. Eur. J. Prev. Cardiol. 24(14), 1555–1566 (2017).
5.
Friberg L, Bergfeldt L. Atrial fibrillation prevalence revisited. J. Intern. Med. 274(5), 461–468 (2013).
6.
Zoni-Berisso M, Lercari F, Carazza T, Domenicucci S. Epidemiology of atrial fibrillation: European perspective. Clin. Epidemiol. 6, 213–220 (2014).
7.
Ahlsson A, Manolis AS, Casadei B et al. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur. Heart J. 37(38), 2893–2962 (2016).
8.
Nicholl BI, Jani BD, Gallacher KI et al. Multimorbidity and co-morbidity in atrial fibrillation and effects on survival: findings from UK Biobank cohort. EP Europace 20(FI_3), f329–f336 (2017).
9.
Vanbeselaere V, Truyers C, Elli S et al. Association between atrial fibrillation, anticoagulation, risk of cerebrovascular events and multimorbidity in general practice: a registry-based study. BMC Cardiovasc. Disord. 16, 61 (2016).
10.
Carson PE, Johnson GR, Dunkman WB, Fletcher RD, Farrell L, Cohn JN. The influence of atrial fibrillation on prognosis in mild to moderate heart failure. The V-HeFT Studies. The V-HeFT VA Cooperative Studies Group. Circulation 87(6 Suppl.), VI102–VI110 (1993).
11.
Deedwania PC, Singh BN, Ellenbogen K, Fisher S, Fletcher R, Singh SN. Spontaneous conversion and maintenance of sinus rhythm by amiodarone in patients with heart failure and atrial fibrillation: observations from the Veterans Affairs Congestive Heart Failure Survival Trial of Antiarrhythmic Therapy (CHF-STAT). The Department of Veterans Affairs CHF-STAT Investigators. Circulation 98(23), 2574–2579 (1998).
12.
Mahoney P, Kimmel S, Denofrio D, Wahl P, Loh E. Prognostic significance of atrial fibrillation in patients at a tertiary medical center referred for heart transplantation because of severe heart failure. Am. J. Cardiol. 83(11), 1544–1547 (1999).
13.
Seiler J, Stevenson WG. Atrial fibrillation in congestive heart failure. Cardiol. Rev. 18(1), 38–50 (2010).
14.
Senni M, Tribouilloy CM, Rodeheffer RJ et al. Congestive heart failure in the community: a study of all incident cases in Olmsted County, Minnesota, in 1991. Circulation 98(21), 2282–2289 (1998).
15.
Reinecke H, Brand E, Mesters R et al. Dilemmas in the management of atrial fibrillation in chronic kidney disease. J. Am. Soc. Nephrol. 20(4), 705–711 (2009).
16.
Bansal N, Fan D, Hsu CY, Ordonez JD, Marcus GM, Go AS. Incident atrial fibrillation and risk of end-stage renal disease in adults with chronic kidney disease. Circulation 127(5), 569–574 (2013).
17.
Olesen JB, Lip GYH, Kamper A-L et al. Stroke and bleeding in atrial fibrillation with chronic kidney disease. N. Engl. J. Med. 367(7), 625–635 (2012).
18.
Choi J, Damaraju C, Mills R et al. Impact of comorbidities on time in therapeutic range in patients with nonvalvular atrial fibrillation. J. Am. Coll. Cardiol. 59(13 Supplement), E1855 (2012).
19.
Chen G, Lix L, Tu K et al. Influence of using different databases and ‘look back’ intervals to define comorbidity profiles for patients with newly diagnosed hypertension: implications for health services researchers. PLoS ONE 11(9), e0162074 (2016).
20.
Fortin Y, Crispo JaG, Cohen D, Mcnair DS, Mattison DR, Krewski D. Optimal look back period and summary method for Elixhauser comorbidity measures in a US population-based electronic health record database. Open Access Med. Stat. 7, 1–13 (2017).
21.
Rassen JA, Bartels DB, Schneeweiss S, Patrick AR, Murk W. Measuring prevalence and incidence of chronic conditions in claims and electronic health record databases. Clin. Epidemiol. 11, 1–15 (2019).
22.
Zhang JX, Iwashyna TJ, Christakis NA. The performance of different lookback periods and sources of information for Charlson Comorbidity adjustment in Medicare claims. Med. Care 37(11), 1128–1139 (1999).
23.
Herrett E, Gallagher AM, Bhaskaran K et al. Data Resource Profile: Clinical Practice Research Datalink (CPRD). Int. J. Epidemiol. 44(3), 827–836 (2015).
24.
Ramagopalan SV, Graham S, Carroll R et al. Discontinuation and primary care visits in nonvalvular atrial fibrillation patients treated with apixaban or warfarin. J. Comp. Eff. Res. 8(6), 371–379 (2019).
25.
Li B, Couris CM, Januel J-M et al. Updating and validating the Charlson Comorbidity Index and Score for Risk Adjustment in hospital discharge abstracts using data from 6 countries. Am. J. Epidemiol. 173(6), 676–682 (2011).
26.
Butler AM, Todd JV, Sahrmann JM, Lesko CR, Brookhart MA. Informative censoring by health plan disenrollment among commercially insured adults. Pharmacoepidemiol. Drug Saf. 28(5), 640–648 (2019).
27.
National Institute for Health and Care Excellence (Nice). Chronic kidney disease in adults: assessment and management. Clinical guideline [CG182]. Recommendations. Frequency of monitoring (2019).
28.
Brunelli SM, Gagne JJ, Huybrechts KF et al. Estimation using all available covariate information versus a fixed look-back window for dichotomous covariates. Pharmacoepidemiol. Drug Saf. 22(5), 542–550 (2013).
29.
Connolly JG, Schneeweiss S, Glynn RJ, Gagne JJ. Quantifying bias reduction with fixed-duration versus all-available covariate assessment periods. Pharmacoepidemiol. Drug Saf. 28(5), 665–670 (2019).
30.
Conover MM, Sturmer T, Poole C et al. Classifying medical histories in US Medicare beneficiaries using fixed vs all-available look-back approaches. Pharmacoepidemiol. Drug Saf. 27(7), 771–780 (2018).
31.
Ekström N, Törnblom M, Titievsky L, Wintzell V, Stark J, Rosenlund M. Assessment of misclassification bias due to short look-back periods in epidemiological studies of chronic disease incidence. Presented at: 34th International Conference on Pharmacoepidemiology & Therapeutic Risk Management. Prague, Czech Republic (2018).
32.
Nakasian SS, Rassen JA, Franklin JM. Effects of expanding the look-back period to all available data in the assessment of covariates. Pharmacoepidemiol. Drug Saf. 26(8), 890–899 (2017).
33.
Apenteng PN, Gao H, Hobbs R, Fitzmaurice DA, On Behalf of Uk Garfield-Af Investigators and Garfield-Af Steering Committee. Temporal trends in antithrombotic treatment of real-world UK patients with newly diagnosed atrial fibrillation: findings from the GARFIELD-AF registry. BMJ Open 13;8(1), e018905 (2017).
34.
Herrett E, Thomas SL, Schoonen WM, Smeeth L, Hall AJ. Validation and validity of diagnoses in the General Practice Research Database: a systematic review. Br. J. Clin. Pharmacol. 69(1), 4–14 (2010).
35.
Herrett E, Dinesh Shah A, Boggon R, Denaxas S, Al E. Completeness and diagnostic validity of recording acute myocardial infarction events in primary care, hospital care, disease registry, and national mortality records: cohort study. BMJ 346 (2013).
36.
Mcdonald L, Sammon CJ, Samnaliev M, Ramagopalan S. Under-recording of hospital bleeding events in UK primary care: a linked Clinical Practice Research Datalink and Hospital Episode Statistics study. Clin. Epidemiol. 10, 1155–1168 (2018).
37.
Kim LG, Cleary F, Wheeler DC et al. How do primary care doctors in England and Wales code and manage people with chronic kidney disease? Results from the National Chronic Kidney Disease Audit. Nephrol. Dial. Transplant. 33(8), 1373–1379 (2018).
38.
Mert KU, Mert GO, Basaran O et al. Real-world stroke prevention strategies in nonvalvular atrial fibrillation in patients with renal impairment. Eur. J. Clin. Invest. 47(6), 428–438 (2017).
39.
Go AS, Fang MC, Udaltsova N et al. Impact of proteinuria and glomerular filtration rate on risk of thromboembolism in atrial fibrillation: the anticoagulation and risk factors in atrial fibrillation (ATRIA) study. Circulation 119(10), 1363–1369 (2009).
40.
Reinecke H, Nabauer M, Gerth A et al. Morbidity and treatment in patients with atrial fibrillation and chronic kidney disease. Kidney Int. 87(1), 200–209 (2015).
41.
National Institute for Health and Care Excellence. Assessment and monitoring of chronic kidney disease (2019). https://www.nice.org.uk/guidance/cg182/
Information & Authors
Information
Published In
Pages: 961 - 968
PubMed: 31317772
Copyright
© 2019 Sreeram V Ramagopalan et al.
History
Received: 5 June 2019
Accepted: 27 June 2019
Published online: 18 July 2019
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Commonly used definitions in real-world studies may underestimate the prevalence of renal disease among nonvalvular atrial fibrillation patients. (2019) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2019-0070
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Miriam Chisholm, Sricharan Navuluri, Moronke Ogundolie, Matthew Boykin, Sakshi Chopra, Sirajbir Sodhi, Samantha Kaplan, Alexandra Gaviser, Tonia Poteat, Whitney R Robinson, Nrupen Bhavsar, Length of look-back periods in studies using administrative data: a scoping review, Epidemiologic Reviews, 10.1093/epirev/mxaf019, 48, 1, (2026).