Putting patients first: an inventive service delivering cancer treatment at home
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: This study evaluated the patient experience of receiving subcutaneous chemotherapy at home via a unique ‘Cancer Treatment at Home’ outreach service adapted by the UK Clatterbridge Cancer Centre NHS Foundation Trust. Patients & methods: The service involved using highly trained nurses to deliver cancer treatments to patients in their own homes. Patient outcomes were monitored over 12 months via the Systemic Anti-Cancer Therapy at Home (SACT) survey using handheld electronic devices. Results: Of the 56 participating cancer patients, 53 provided responses. Patients received subcutaneous trastuzumab, denosumab, pembrolizumab, fulvestrant and goserelin. Overall, 96% of respondents were ‘very satisfied’ and 4% ‘satisfied’ with the service. All respondents would recommend the service to others. Conclusion: The ‘Cancer Treatment at Home’ service has improved the patient experience for cancer care and has been recognized nationally for its achievements.
At present, systemic anti-cancer therapy (SACT) plays a significant part in a cancer treatment pathway. However, patients undergoing SACT face numerous challenges, posing a great social and financial burden and significantly impacting on their quality of life (QoL) [1,2].
The costs related to cancer can largely be categorized as direct, indirect and psychosocial. Previous studies have reported that patients encounter substantial direct costs, including those related to the day-to-day living [3–5] and ‘out-of-pocket’ costs related to treatment, such as travel expenses, parking charges and prescription medication [6–9]. The economic burden of cancer also comprises significant indirect costs, including loss of time dedicated to usual activities, for example, the decision to work or retire and the impact on savings and/or holidays [7,10,11]. In addition, the psychosocial impact of the disease is high, with data from patient-reported outcome assessments showing high levels of depression, anxiety, worry, fear, anger and guilt [4,12]. As a result, QoL is increasingly being used as an outcome measure in studies to evaluate the effectiveness of cancer treatments [13–15], in addition to survival benefit.
While traditionally SACT is administered in a hospital or ambulatory setting as outpatient treatment, this approach places a high economic burden on the healthcare system. The rising overall costs of delivering high-quality cancer care are becoming increasingly apparent [16–18], and innovative ways of providing more cost-effective therapy are required. Home-based chemotherapy has been proposed as an alternative solution to support the growing number of patients requiring cancer treatment [19]. In addition, it may also be less stressful for the patient, and thus, have a positive psychological impact [20,21]. In the UK, private providers exist that offer chemotherapy treatment in a home setting [22]; however, this may lead to the breakdown of coordinated care with specialist oncology centers. In addition, such outsourcing of homecare with private providers has historically resulted in challenges around the consistency of service provision [23].
The Clatterbridge Cancer Centre NHS Foundation Trust (CCC) is one of the largest networked cancer centers in the UK, providing nonsurgical oncology services to a population of over 2.3 million people in Merseyside, Cheshire and the Isle of Man. The center has adapted a unique, outreach model to enable the provision of cost-effective cancer treatment at home (as an extension of the hub-and-spoke model); thereby, providing home-based care while addressing the possible challenges with coordinated, consistent service provision. Here, we describe our approach and evaluate the experience of delivering chemotherapy at home from a patient’s perspective.
Patients & methods
‘Cancer Treatment at Home’ model
The ‘Cancer Treatment at Home’ service was developed based on the Royal Pharmaceutical Society’s ‘Professional Standards for Homecare Services in England’ [24] and ‘Handbook for Homecare Service in England’ [25].
The Clatterbridge Pharmacy Ltd (PharmaC; Bebington, UK), established in 2014, is a wholly owned subsidiary company of the Trust; this enables medicines to be supplied to patients for home-administration, ‘zero-rated’ for value-added tax (VAT). The implications of these VAT exemptions are that savings on some therapies can be used to offset higher-cost drugs, which has widened the treatment options available to the CCC and permitted delivery of treatment at home. This offers the possibility of extending the service to more patients by increasing the number of therapies on offer and consequently improving its long-term financial viability. The ‘Treatment at Home’ service is the only one of its type in the UK to be run in-house with support of a Trust-owned pharmacy.
The service in practice
The Clatterbridge in the Community Steering Group, consisting of nurses, pharmacists and governance team members, proposed that the implementation of the ‘Cancer Treatment at Home’ service (following an initial pilot) be undertaken in two phases (Table 1):
•
Phase 1: Administration of a broader list of identified treatments for a wider range of cancers, based on patient need, as per the CCC ‘Cancer Treatment at Home’ Policy
•
Phase 2: Administration of all intravenous treatments based on patient need, as per the CCC ‘Cancer Treatment at Home’ Policy
| Phase | Treatment administration | Regions covered |
|---|---|---|
| Phase 1 Breast Cancer | Administration of all identified subcutaneous treatments based on patient need, as per the CCC ‘Cancer Treatment at Home’ Policy: • Trastuzumab • Trastuzumab + denosumab + bloods • Trastuzumab + goserelin • Denosumab + bloods • Denosumab + fulvestrant + bloods • Denosumab + goserelin + bloods • Fulvestrant + goserelin + bloods • Goserelin | • Wirral (continuation of pilot) • Halton and Chester (April 2015) • Liverpool (September 2015) • St Helens and Southport (September 2015) |
| Phase 2 Melanoma | Administration of all intravenous treatments based on patient need, as per the CCC ‘Cancer Treatment at Home’ Policy: • Pembrolizumab | • Wirral (continuation of pilot) |
CCC: Clatterbridge Cancer Centre NHS Foundation Trust.
A pilot scheme was conducted to establish the model with one drug (trastuzumab), for a defined patient population, where the most experience of home treatment was available. In addition, trastuzumab administered at home was also able to generate the capacity-releasing and financial efficiencies necessary for the model to progress to Phases 1 and 2 of the project.
Patient enrolment
Clinicians were made aware of the service through individual communications, via the CCC nurses working throughout the network, various cancer network and site-specific clinical reference groups. The service was initially set up as an opt-in service so patients could continue to receive chemotherapy at the clinic if they preferred, but was subsequently amended to an opt-out service, to encourage patient recruitment into the scheme. At the time of survey collection, approximately two-thirds of patients referred into the CCC service were treated in the adjuvant setting and a third were treated in the palliative setting.
New patients opting to sign up to the service initially had a number of treatments at the clinic to ensure safe and effective therapy was possible. Each patient received either verbal or face-to-face risk assessment, including review of patients’ physical health, side effects and toxicities, local site reaction, risk of anaphylaxis and allergy and co-morbidities. Following satisfactory administration of treatment, patients were eligible to book in via a centralized referral system to have subsequent treatments delivered at home. All patients provided written informed consent to receive treatment at home; patients were asked to complete a Home Patient Survey.
Patients were monitored for treatment-related toxicities via the following surveillance process:
•
All patients are reviewed prior to or during each cycle of treatment, prior to drug administration
•
If the patient was presented with a toxicity, they would be given either a telephone consultation or face-to-face advice by the specialist nurse relating to that specific toxicity
•
If that toxicity could not be resolved, the patient would be referred to the CCC triage hotline/Clinical Decision Unit (CDU) for review
•
The patient may be asked to attend CCC/CDU or their local accident and emergency (A&E)/emergency department for further review
•
If attending the CDU, the patient would be reviewed by a doctor on the ward, and if necessary, may be admitted into the CCC. The same would apply at a local District General Hospital/accident and emergency department
•
If admitted to a District General Hospital, they would be reviewed by a doctor, and the acute oncology team would be notified of their admission
•
During these processes, the oncologist would be notified and the patient would be referred back to them for additional support, in other words, a clinic appointment with the oncologist
•
Treatment may be put on hold until this review has been completed
Treatment administration
All ‘Cancer Treatment at Home’ chemotherapy nurses were specially trained, including peer supervision to support the safe and effective use of homecare services by patients. In addition, due to the risk of carrying medical equipment and drugs in the community and in entering patients’ homes, all nurses were required to undertake appropriate safety training for lone workers. All nurses were signed off on successful completion of training and evidence of competency. In addition, the nurses were directly employed by the CCC and used the Trust’s networked clinics as a base. Controlling the service centrally provided the flexibility to respond to local demand and needs of patients, and use established systems and processes, for example, governance and staff training, logistics, distribution and information technology networks and insurance cover. A small fleet of CCC vehicles were used to facilitate at-home appointments; local geography and travel times were considered to ensure the service had the capacity to run successfully.
Implementation of patient pathways, detailed protocols for delivering quality cancer care [26], also guaranteed that important milestones such as treatment reviews, scans and blood tests, and physician consultations could continue to take place as per CCC protocols, and that clinical governance was consistently adhered to.
Outcome measures
The overall efficiency of the ‘Cancer Treatment at Home’ service was measured by the number of patients treated, length of treatment time and total length of additional time in patients’ homes.
Patient outcomes were monitored via a 12-month-duration SACT at Home Patient Survey (aligned with the National Cancer Patient Experience Survey), which was completed at home by their nurse, using a handheld electronic device [27]. The survey covered topics such as safety, respect and dignity, satisfaction with the service, perceived benefits and service improvement challenges.
Results
Patients
Fifty-six patients (median age: 46–65 years; age range: 20 to +76 years) with diagnosed cancer were enrolled to receive chemotherapy at home as part of the ‘Cancer Treatment at Home’ service and agreed to participate in the SACT patient survey. Three patients were excluded from the analysis as they did not provide responses to any questions from the survey beyond demographic information. In addition, not all patients provided a response to all questions in the survey. Consequently, data will be reported as n/N (%), where n is the number of same responses for the question asked, and N is the total number of responses provided for the question asked.
The treatments were administered between April 2015 and September 2016 in the Merseyside and Cheshire areas. In total, 46 patients received subcutaneous trastuzumab. Other treatments included single drugs or combinations of drugs including denosumab, pembrolizumab, fulvestrant and goserelin (Table 1; Figure 1). Patients were referred for treatment from across the region, with most coming from locations near to the CCC. The majority of patients in the ‘Treatment at Home’ study were aged 46–65 years (Figure 2A) with 26% of all patients receiving palliative treatment (Figure 2B). Two rounds of surveys were collected in two 4-week periods.
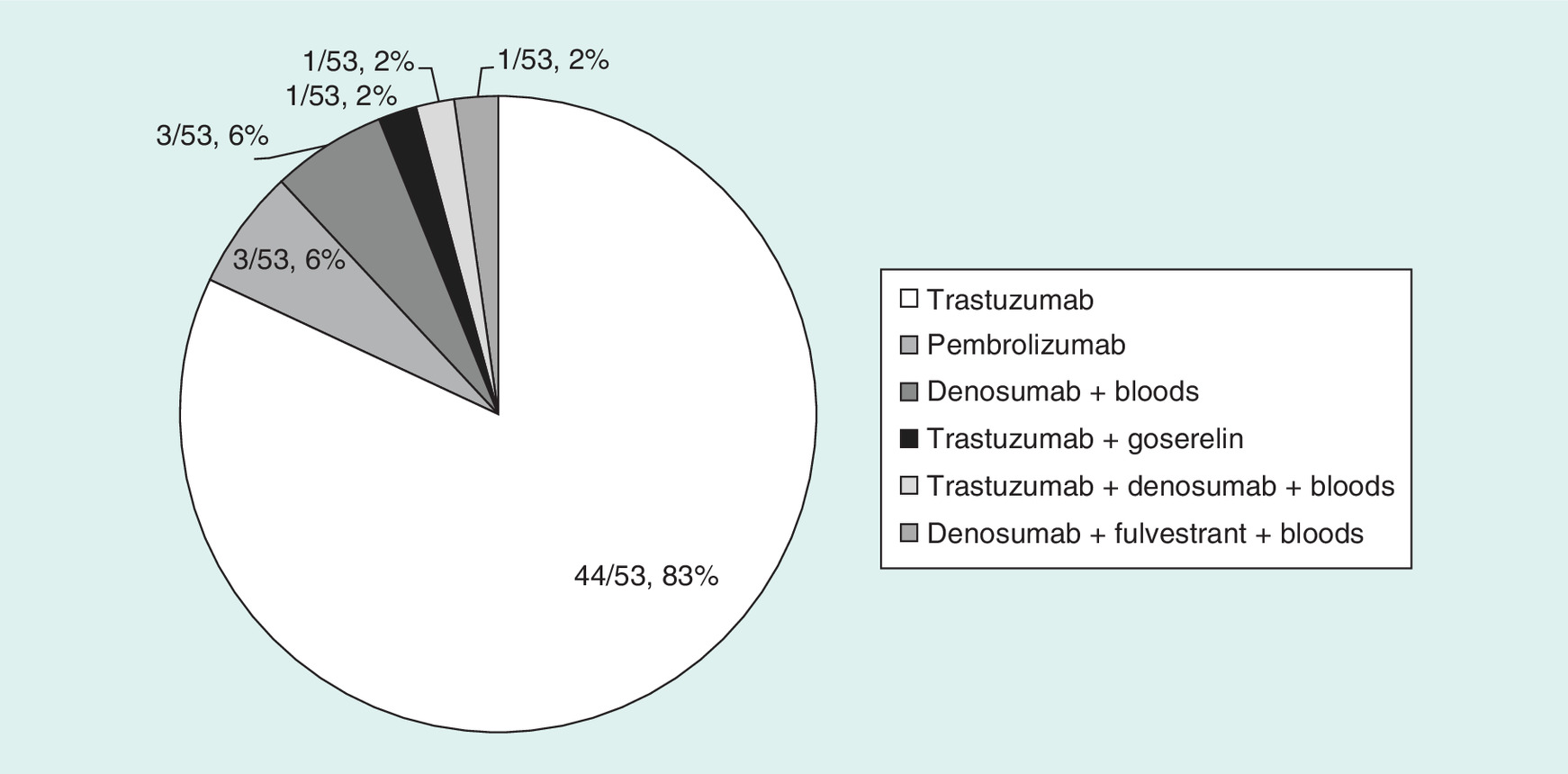
Figure 1. Breakdown of treatments received by patients enrolled in the ‘Cancer Treatment at Home’ service who participated in the systemic anti-cancer therapy patient survey.
Reported as n/N, %.
n: Subset of the total population; N: Total population.

Figure 2. Age and cycle of treatent for patients enrolled on the ‘Treatment at Home’ service who participated in the systemic anti-cancer therapy patient survey, reported as n/N, %.
(A) Distribution of age ranges, and (B) cycle of treatment given to patients.
n: Subset of the total population; N: Total population.
Service efficiency & appointments
Treatment delivery times ranged from 5 to >60 min, with most patients’ (39/46 [85%]) total length of treatment time taking 30–45 min (Figure 3A). In addition, nurses were in patients’ homes for an additional 0–30 min beyond the allocated time for treatment (anecdotally, this time was spent in staff–patient discussion around health needs and personalized treatment; Figure 3B).
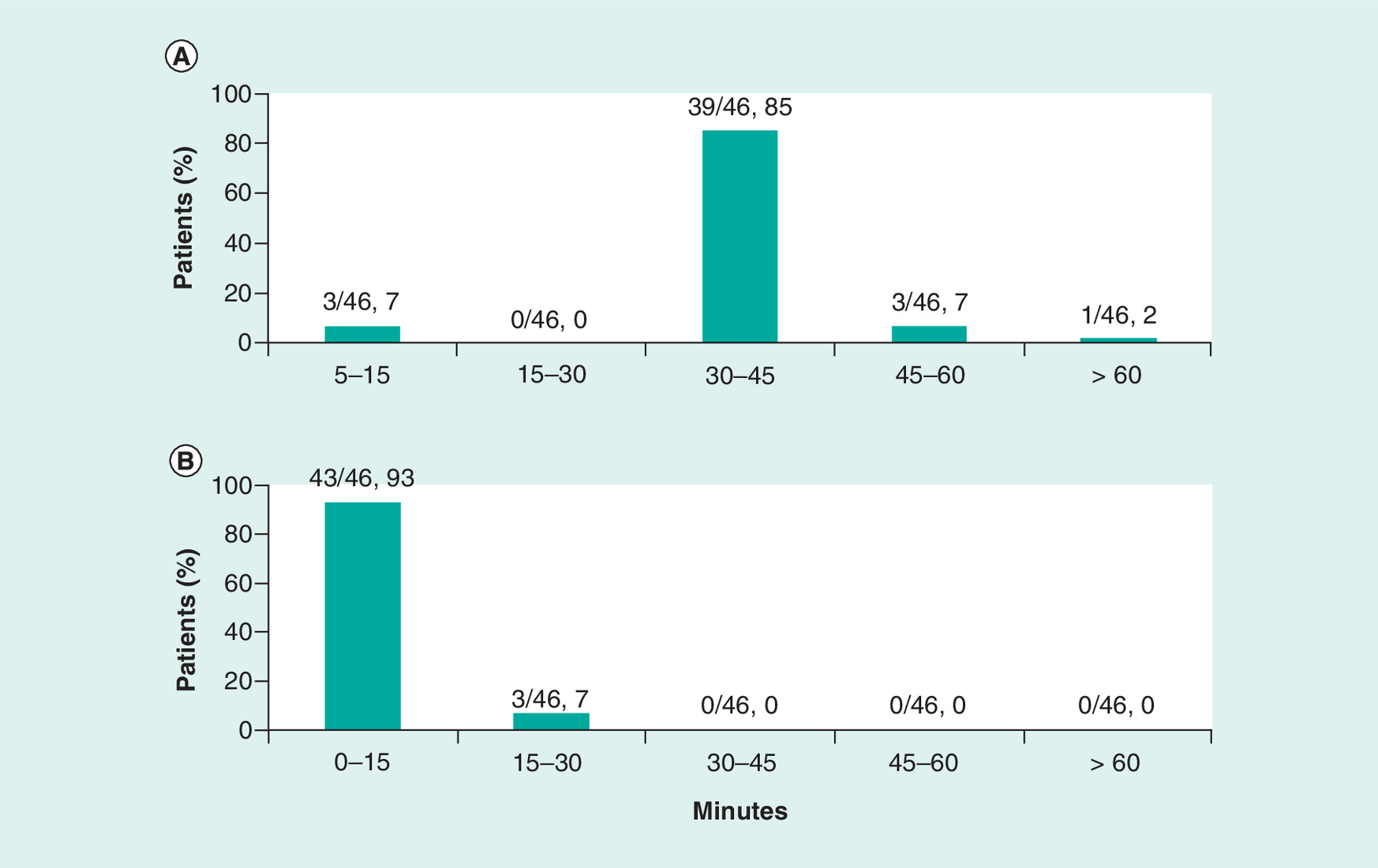
Figure 3. Efficiency of the ‘Treatment at Home’ service.
Efficiency was measured by (A) total length of treatment time, and (B) total length of additional time spent in patients’ homes, reported as n/N, %.
n: Subset of the total population; N: Total population.
All survey respondents indicated that nurses introduced themselves, all patients felt the majority of times and dates were convenient and all were informed of most delays in appointment times. Nurses were reported to be ‘always be on time’ by 40/51 (78%) of respondents and ‘usually on time’ by 11/51 (22%) of respondents.
Thirty-four out of 53 (64%) patients preferred treatment times between 9 am and 1 pm, 12/53 (23%) patients expressed a preference between 1 pm and 5 pm and 7/53 (13%) patients preferred times before 9 am.
Patient safety
All patients indicated they were asked to confirm their personal details, whether they were fit enough to proceed with the treatment, and whether they felt safe with the nurses in their homes, and felt confidence in the ability of their nurse. All nurses were confirmed to have washed their hands prior to treatment administration, and all patients were given information on who to contact with regard to any problems they may experience following the treatment. None of the patients needed to attend triage or seek subsequent emergency treatment in relation to the service or treatment given.
Overall patient satisfaction
Results of the survey demonstrated high satisfaction levels with the ‘Cancer Treatment at Home’ service (Figure 4). All respondents indicated they would recommend the service to others. Table 2 highlights the anecdotal patient-reported benefits of using the service, divided into three categories: driving/parking, waiting/convenience and continuity/QoL.
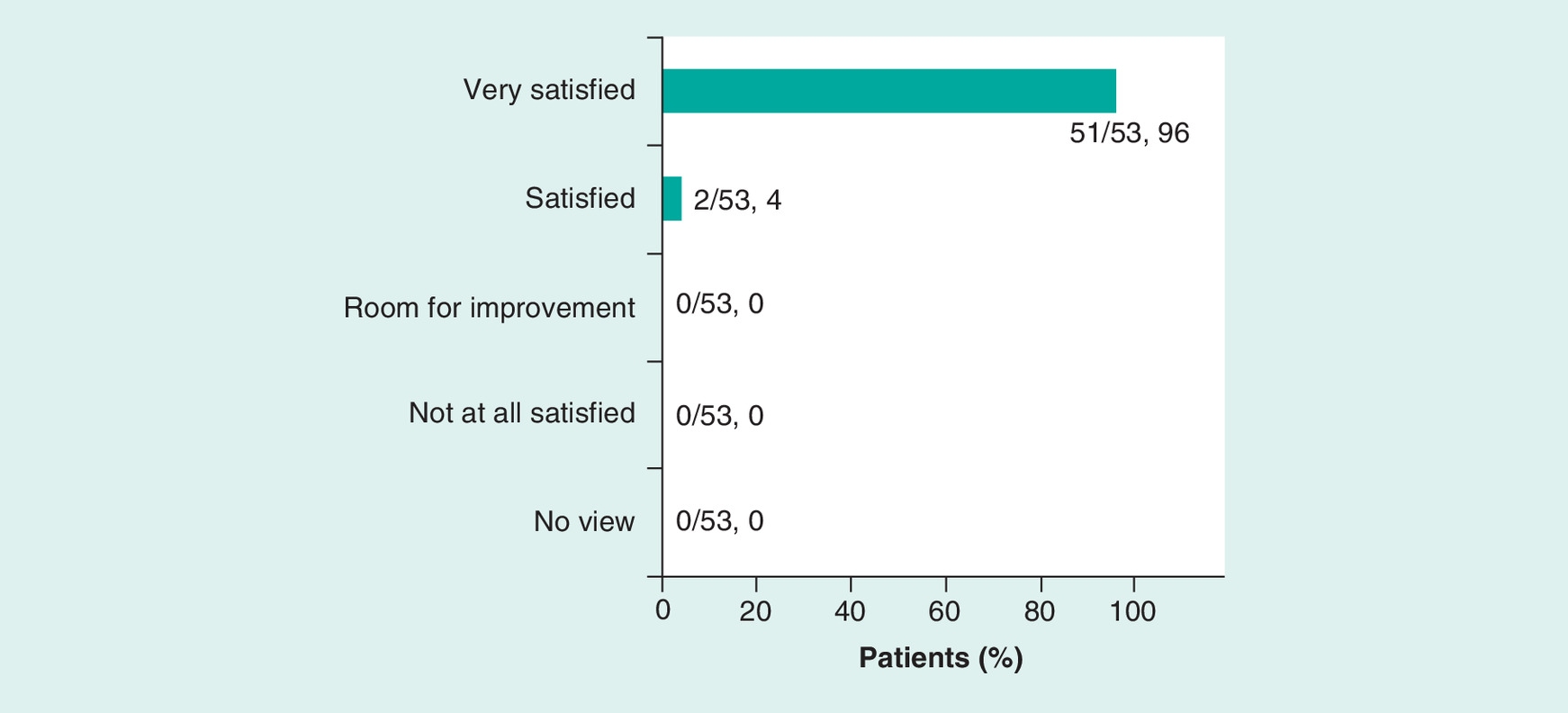
Figure 4. Responses to the question ‘How satisfied are you with the overall service?’.
Reported as n/N, %.
n: Subset of the total population; N: Total population.
| Travelling/parking | Waiting/convenience | Continuity/QoL |
|---|---|---|
| “Save hospital trips” “Time not wasted in car” “No stress finding parking” “Petrol cost reduced” “No parking costs” “No need for bus” “Saves on ambulance time” “Saves on long ambulance return” “Not relying on lifts” | “It is quick and easy” “Much better than waiting 2.5 h for an injection… as I once did” “No waiting times, I don't like waiting in hospital” “Waiting times in hospital can be long and I've been missed before” “Comfort at home with no stress” “More relaxed and informal, privacy, convenient” “Easier than setting up and transporting wheelchairs” “Convenient to me; basically, keeping me alive” “Do not have to go out when feeling poorly” | “Same nurse… better one to one” “A personal service” “I need confidence to go out, so better for me” “Get time to speak to nurse” “Reduced anxiety” “The ability to work from home” “Upsets me going to CCC, so better at home” “Puts my mind at ease having treatment at home” “Fits in with work-life” “Do not have to rely on others; more private” |
CCC: Clatterbridge Cancer Centre NHS Foundation Trust; QoL: Quality of life.
Patient feedback & areas for improvement of the service
Comments on the service and areas for improvement suggested by respondents included: not being able to obtain a morning slot on some occasions; request for future appointments to be linked to a scheduler, and thus, providing the option to be alerted ahead of appointment dates and times and prior to the arrival of the nurse; request for future treatments to be offered at their place of work or other locations and personal drawbacks including missing friends at CCC.
Discussion
Here, we aimed to describe our unique model of cancer treatment administered at home and to examine how patients perceive their experience of this. To our knowledge, the CCC ‘Cancer Treatment at Home’ service is the only one of its kind to be run in-house with the support of a Trust-owned pharmacy, and is one of the first centers in the UK using its own highly trained nurses to deliver cancer treatments to patients in their own homes. Patients undergoing chemotherapy at home reported high levels of satisfaction with the service. Home-based chemotherapy was highlighted by patients in the study as reducing the requirement for travelling, waiting times, and stress and anxiety, as well as increasing comfort levels, independence and providing a personalized service.
Recent feedback from an inspection performed by the UK Care Quality Commission (an external inspectorate that provides judgement on the quality of care based on a combination of findings at the time of inspection) judged that the ‘Treatment at Home’ service was ‘outstanding’ [28–30]. This evaluation was based upon a number of sources, which included information from the Intelligent Monitoring System and information provided by patients, the public and other organizations. The Care Quality Commission emphasized that the service ‘embodied the overall trust and service vision of providing the best cancer care to their patients’ [28].
While the service has demonstrated great success, there are many key aspects that need to be taken into consideration before attempting to implement the service in other locations. It is important that a multidisciplinary team, ideally from a center of excellence, is set up to provide structure and clear processes on how the project will be led. In addition, it is recommended that the service is initially started with the use of one drug, typically one with minimal emetic risk (<10% frequency of emesis) [31], and the patient profiles and geography are mapped as part of the initial project plan.
There are also a number of governance aspects that need to be considered prior to introducing the service including: patient pathways to ensure follow-up is consistent with protocols and clinical governance is adhered to; definition of patient eligibility criteria, including inclusion and exclusion criteria; development of comprehensive documentation to ensure procedures and support for all treatment eventualities; treatment scheduling and home treatment planning to fit in with the hospital rotas; insurance cover outside the hospital setting; provisions for storage and transportation of medication; performance of lone worker risk assessments, including requirements for training and how best to support and monitor lone workers; maintenance of patient confidentiality, particularly in relation to possible corporate branding as part of uniform and transport vehicle; ensuring prescription records are part of the Trust’s overall electronic prescribing system and the electronic patient record; management of anaphylaxis and other adverse events; the medical/nonmedical equipment required and its transportation; disposal of waste; clinical documentation and record-keeping; recruitment of nurses to meet demands; training and competency checks of employed nurses and business continuity arrangements.
Comparisons with other studies assessing home-based chemotherapy demonstrate similar results. A study by Borras et al., conducted in Spain, compared the experience of patients with colorectal cancer receiving chemotherapy at home with those patients receiving hospital treatment. While the results demonstrated no differences between the groups in terms of QoL, levels of patient satisfaction were higher in the home-treatment group, specifically regarding information received and nursing care. While a cost analysis was not performed, the authors highlighted the at-home service would require additional resources but could be considered as an economically realistic alternative, considering the indirect benefit to patients [21]. A study by Joo et al., conducted in South Korea, compared patient-reported and economic outcomes in patients with advanced colorectal cancer receiving chemotherapy at home or in hospital. Results demonstrated higher satisfaction and lower economic cost for home-based chemotherapy, although it should be noted that physicians played a major role in the decision for patients to opt for home-based chemotherapy [20]. An additional study by Bordonaro et al., conducted in Italy, assessed the effect of a home-based cancer treatment program on QoL and satisfaction in a cohort of patients with a range of cancers treated with oral chemotherapy. This multicenter study demonstrated significant improvements (p < 0.05) in symptom and physical-functioning scales and found patients expressed high satisfaction with oral chemotherapy [32]. While to our knowledge, the cost–effectiveness of home-based chemotherapy administration has not been studied in detail, all the studies discussed have demonstrated patients’ preference for home-based chemotherapy, highlighting the importance of providing this service as an option.
Our study had some limitations. First, not all patients were eligible for the service, thus a ‘fitter’ population of patients who cope better with treatment may have been selected, which may have provided more positive survey results. Second, not everyone who received treatment at home participated in the survey and satisfied patients may have been more likely to respond to the survey. Furthermore, surveys were completed by nurses based on patient responses, which could be complemented and further validated by independent surveys completed by patients themselves. In addition, the service was provided with a limited nursing capacity and an optimized staff level could have further improved patient services, and thereby, resulted in more positive patient feedback. Patients enrolled in the study received a limited number of simple chemotherapy regimens and this model may therefore not be applicable to complex combinations of drugs. Currently, these medicines are supplied as ‘zero-rated’ for VAT; thus, the model may not be sustainable if savings resulting from this privilege are removed. The service commenced Phase 3 in August 2016 to include the administration of parenteral immunotherapy for treatment of melanoma.
Conclusion
In summary, the findings support the provision of cancer treatment in a home setting to help relieve increasing pressure on hospital-based chemotherapy services and the program aligns with National Health Service’s Five Year Forward View, which describes the goal of supporting care availability much closer to people’s homes, wherever possible [33]. The ‘Cancer Treatment at Home’ service has been demonstrated to be very successful for the CCC and the patients that use the service, with 100% satisfaction, and it has been recognized nationally for its achievements. It is important to ensure that the service is appropriately resourced to achieve the projected activity before it can be extended further to other drugs and cancer pathways. While further studies are needed to confirm the feasibility and benefits of the model, the positive survey results observed in this study demonstrate this to be a viable model that can be implemented in other locations so more patients have the option to have treatment administered outside the hospital setting.
Future perspective
Future developments and improvements of the service that are being considered include: telehealth review of patients; patient-reported outcomes for the assessment of quality of care; an option to link home delivery of oral SACT; cost–benefit analysis of providing the service compared with traditional models of care and potential expansion of treatment locations, for example, work or school. Indeed, an extension into the workplace was initiated by the CCC in 2018, which involves the delivery of subcutaneous treatments in a safe and suitable area. Although in an early phase, the initiative has already received positive patient feedback, including that it minimizes disruption for patients returning to work.
•
Traditionally, systemic anti-cancer therapy (SACT) is administered in a hospital or ambulatory setting as outpatient treatment, but this approach places a high economic burden on the healthcare system; home-based chemotherapy has been proposed as an alternative solution.
•
The Clatterbridge Cancer Centre NHS Foundation Trust in the UK has adapted a unique, outreach model to enable the provision of cost-effective cancer treatment at home.
•
In this study we describe our ‘Cancer Treatment at Home’ service and evaluated the experience of delivering chemotherapy at home from a patient’s perspective.
•
The overall efficiency of the service was measured by the number of patients treated, length of treatment time and total length of additional time in patients’ homes; patient outcomes were monitored for 12 months via the SACT at Home Patient Survey, which was completed at home by their nurse, using a handheld electronic device.
•
Fifty-six patients (20 to +76 years of age) with diagnosed cancer were enrolled to receive chemotherapy at home as part of the service and agreed to participate in the SACT patient survey; 53 patients completed the survey.
•
Patients received subcutaneous trastuzumab, denosumab, pembrolizumab, fulvestrant and goserelin.
•
Treatment delivery times were 30–45 min for most (85%) patients; overall, 96% of respondents were ‘very satisfied’ and 4% ‘satisfied’ with the service.
•
Comments on the service and areas for improvement reported by the patients included: more morning time slots; pre-appointment alerts; offer treatments at place of work or other locations and personal drawbacks, such as missing friends that they would normally see in the clinic.
•
The ‘Cancer Treatment at Home’ service has improved the patient experience for cancer care and has been recognized nationally for its achievements.
Author contributions
All authors were responsible for the study conception and design; for the acquisition, analysis and interpretation of data and were involved in drafting and revising the manuscript. All authors have approved the submitted version to be published and agree to be accountable for aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Financial & competing interests disclosure
H Poulter-Clark declares a nonremunerative position of influence (Executive Director, Clatterbridge Pharmacy Ltd). The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Medical writing support was provided by S Grewal, of Helios Medical Communications (Alderley Edge, Cheshire, UK) and funded by Amgen (Europe) GmbH (Rotkreuz, Switzerland). Editorial support was provided by D Cutler, CMPP of Aspire Scientific (Bollington, UK) and funded by Amgen (Europe) GmbH.
Ethical conduct of research
All patients provided written informed consent to receive treatment at home; patients were asked to complete the Home Patient Survey.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Barbaret C, Brosse C, Rhondali W et al. Financial distress in patients with advanced cancer. PLoS ONE 12(5), e0176470 (2017).
2.
Oh PJ, Cho JR. Changes in fatigue, psychological distress, and quality of life after chemotherapy in women with breast cancer: a prospective study. Cancer Nurs. (2018) (Epub ahead of print).
3.
Azzani M, Roslani AC, Su TT. The perceived cancer-related financial hardship among patients and their families: a systematic review. Support. Care Cancer 23(3), 889–898 (2015).
4.
Delgado-Guay M, Ferrer J, Rieber AG et al. Financial distress and its associations with physical and emotional symptoms and quality of life among advanced cancer patients. Oncologist 20(9), 1092–1098 (2015).
5.
Sharp L, O'Leary E, O'Ceilleachair A et al. Financial impact of colorectal cancer and its consequences: associations between cancer-related financial stress and strain and health-related quality of life. Dis. Colon Rectum 61(1), 27–35 (2018).
6.
Ó Céilleachair A, Hanly P, Skally M et al. Counting the cost of cancer: out-of-pocket payments made by colorectal cancer survivors. Support. Care Cancer 25(9), 2733–2741 (2017).
7.
Zafar SY, Peppercorn JM, Schrag D. Barriers and facilitators for return to work in cancer survivors with job loss experience: a focus group study. Eur. J. Cancer Care 26(5), e12420 (2017).
8.
Sharp L, Timmons A. National Cancer Registry/Irish Cancer Society. The financial impact of a cancer diagnosis (2010). www.ncri.ie/sites/ncri/files/pubs/FinancialImpactofaCancerDiagnosis(SummaryReport).pdf
9.
Kidney Cancer Support Network. Cancer's hidden price tag: revealing the costs behind the illness (2017). www.kcsn.org.uk/opinion-pieces/cancers-hidden-price-tag-revealing-costs-behind-illness
10.
Altice CK, Banegas MP, Tucker-Seeley RD, Yabroff KR. Financial hardships experienced by cancer survivors: a systematic review. J. Natl Cancer Inst. 109(2), pii: djw205 (2017).
11.
NHS, Department of Health. Quality of life of cancer survivors in England – Report on a pilot survey using Patient Reported Outcome Measures (PROMS) (2012). www.gov.uk/government/uploads/system/uploads/attachment_data/file/267042/9284-TSO-2900701-PROMS-1.pdf
12.
Ominyi JN, Nwodom MU. Psychological impact of lung cancer on the newly diagnosed patients. Int. J. Sci. Res. 3(11), 522–528 (2014).
13.
Kirshbaum MN, Dent J, Stephenson J et al. Open access follow-up care for early breast cancer: a randomised controlled quality of life analysis. Eur. J. Cancer Care 26(4), e12577 (2017).
14.
Lloyd AJ, Kerr C, Penton J, Knerer G. Health-related quality of life and health utilities in metastatic castrate-resistant prostate cancer: a survey capturing experiences from a diverse sample of UK patients. Value Health 18(8), 1152–1157 (2015).
15.
Reijneveld JC, Taphoorn MJ, Coens C et al. Health-related quality of life in patients with high-risk low-grade glioma (EORTC 22033-26033): a randomised, open-label, Phase 3 intergroup study. Lancet Oncol. 17(11), 1533–1542 (2016).
16.
Vallejo-Torres L, Morris S, Kinge JM, Poirier V, Verne J. Measuring current and future cost of skin cancer in England. J. Public Health 36(1), 140–148 (2014).
17.
Aggarwal A, Sullivan R. Affordability of cancer care in the United Kingdom – is it time to introduce user charges? J. Cancer Policy 2(2), 31–39 (2014).
18.
Prager GW, Braga S, Bystricky B et al. Global cancer control: responding to the growing burden, rising costs and inequalities in access. ESMO Open 3(2), e000285 (2018).
19.
Larsen FO, Christiansen AB, Rishøj A et al. Safety and feasibility of home-based chemotherapy. Dan. Med. J. 65(5), pii: A5482 (2018).
• A randomized crossover study demonstrating that home-based chemotherapy is feasible and safe and might be a valuable alternative to treatment at an outpatient clinic.
20.
Lassalle A, Thomaré P, Fronteau C et al. Home administration of bortezomib in multiple myeloma is cost-effective and is preferred by patients compared with hospital administration: results of a prospective single-center study. Ann. Oncol. 27(2), 314–318 (2016).
21.
Borras JM, Sanchez-Hernandez A, Navarro M et al. Compliance, satisfaction, and quality of life of patients with colorectal cancer receiving home chemotherapy or outpatient treatment: a randomised controlled trial. BMJ 322(7290), 826 (2001).
22.
Corbett M, Heirs M, Rose M et al. The delivery of chemotherapy at home: an evidence synthesis. HS&DR 3(14), (2015).
• A systematic review of clinical effectiveness, qualitative and cost–effectiveness studies comparing the impact of delivering intravenous chemotherapy in different settings (home, community and hospital outpatient) on a range of outcomes, including quality of life, safety and costs.
23.
NHS England. Patient Safety Alert – Stage One: warning – minimising risks of omitted and delayed medicines for patients receiving homecare services (2014). www.england.nhs.uk/wp-content/uploads/2014/04/psa-omitted-delayed-meds.pdf
24.
Royal Pharmaceutical Society. Professional standards of homecare services in England (2013). www.rpharms.com/Portals/0/RPS%20document%20library/Open%20access/Professional%20standards/Professional%20standards%20for%20Homecare%20services/homecare-standards-final-sept-13.pdf
25.
Royal Pharmaceutical Society. Handbook for homecare services in England (2014). www.rpharms.com/Portals/0/RPS%20document%20library/Open%20access/Professional%20standards/Professional%20standards%20for%20Homecare%20services/homecare-services-handbook.pdf
•• Handbook to aid the implementation of the Royal Pharmaceutical Society Professional Standards for Homecare Services. The ‘Cancer Treatment at Home’ service was developed based on the best practices outlined in this handbook.
26.
Zon RT, Frame JN, Neuss MN et al. American Society of Clinical Oncology policy statement on clinical pathways in oncology. J. Oncol. Pract. 12(3), 261–266 (2016).
27.
Quality Health. National Cancer Patient Experience Survey guidance document (2014). www.quality-health.co.uk/resources/surveys/national-cancer-experience-survey/2014-national-cancer-patient-experience-survey/2014-national-cancer-patient-experience-survey-materials/687-2014-national-cancer-patient-experience-survey-guidance-manual/file
28.
Care Quality Commission. The Clatterbridge Cancer Centre NHS Foundation Trust Quality Report (2017). www.cqc.org.uk/sites/default/files/new_reports/AAAG0143.pdf
•• Report from the UK Care Quality Commission describing the quality of care at The Clatterbridge Cancer Centre NHS Foundation Trust. Based on an inspection, information from an ‘Intelligent Monitoring’ system and information from patients, the public and other organizations, the trust was rated ‘outstanding’.
29.
BBC News. Wirral's Clatterbridge Centre rated outstanding by health watchdog (2017). www.bbc.co.uk/news/uk-england-merseyside-38815659
30.
Liverpool Echo. Why patients cherish the ‘outstanding’ Clatterbridge Cancer Centre (2017). www.liverpoolecho.co.uk/news/liverpool-news/patients-cherish-outstanding-clatterbridge-cancer-12536203
31.
National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology™: Antiemesis (2019). www.nccn.org/professionals/physician_gls/pdf/antiemesis.pdf
32.
Bordonaro S, Romano F, Lanteri E et al. Effect of a structured, active, home-based cancer-treatment program for the management of patients on oral chemotherapy. Patient Prefer. Adherence 8, 917–923 (2014).
•• A multicenter observational study assessing home-based oral chemotherapy treatment. Home-based oral chemotherapy was associated with improvements in the quality of life of patients and caregivers, better adherence to treatment and the effective management of therapy and cancer-related symptoms.
33.
NHS England. Five Year Forward View (2014). www.england.nhs.uk/wp-content/uploads/2014/10/5yfv-web.pdf
•• A report representing the views of the NHS's national leadership, patient groups, clinicians and local communities outlining a vision for a better NHS and the changes required to achieve this. The report describes a goal of supporting cancer care availability much closer to people’s homes, wherever possible.
Information & Authors
Information
Published In
Pages: 951 - 960
PubMed: 31441319
Copyright
© 2019 Frances Yip, Burhan Zavery, Helen Poulter-Clark, Joan Spencer. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 21 March 2019
Accepted: 5 June 2019
Published online: 23 August 2019
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Putting patients first: an inventive service delivering cancer treatment at home. (2019) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2019-0038
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Chih-Hsien Li, Chuan-Wei Kuo, Ching-Hsiang Fan, Feasibility of using focused acoustic vortex for enhancing transdermal delivery, Ultrasonics, 10.1016/j.ultras.2025.107747, 156, (107747), (2025).
- Maria Francesca Furmenti, Gaia Bertarelli, Francesca Ferrè, Person-centred care in oncological home services: a scoping review of patients’ and caregivers’ experience and needs, BMC Health Services Research, 10.1186/s12913-024-12058-w, 25, 1, (2025).
- Hyoeun Jang, Sanghee Kim, DaeEun Kim, Mehee Park, Sunemee Rhue, Changmin Lee, Seulgee Kim, Byungmun Kang, Haeri Lee, “It's a part of the patient”: The experiences of patients with cancer undergoing home-based chemotherapy from patients' and nurses' perspectives, Asia-Pacific Journal of Oncology Nursing, 10.1016/j.apjon.2022.04.011, 9, 8, (100072), (2022).
- Marko Puzovic, Hana Morrissey, Patrick Anthony Ball, Intravenous Treatment in Home and Outpatient Settings: A Comprehensive Literature Review, International Journal of Social and Psychological Aspects of Healthcare, 10.51847/JMyEiUBztI, 2, 1, (8-22), (2022).
- Irene Lizano-Díez, Sonia Amaral-Rohter, Lucía Pérez-Carbonell, Susana Aceituno, Impact of Home Care Services on Patient and Economic Outcomes: A Targeted Review, Home Health Care Management & Practice, 10.1177/10848223211038305, 34, 2, (148-162), (2021).