Intravenous tranexamic acid reduces blood transfusions in revision total hip arthroplasty: a meta-analysis
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: We performed a meta-analysis to systematically assess the efficacy and safety of intravenous tranexamic acid in revision total hip arthroplasty. Method: Potential academic articles were identified from Cochrane Library, Medline, PubMed, EMBASE, ScienceDirect and other databases. The time range we retrieved from was that from the inception of electronic databases to February 2019. Gray studies were identified from the references of included literature reports. STATA version 11.0 was used to analyze the pooled data. Results: A total of eight articles were involved in our study. The overall participants of tranexamic acid (TXA) group were 3533, whereas it was 11,007 in the control group. Our meta-analysis showed that TXA is preferable for revision total hip arthroplasty because of its lower value of hemoglobin reduction (weighted mean difference = -1.277–1.405; 95% CI: -1.996 to -0.559; p < 0.001), the rate of blood transfusion (odds ratio: 0.233; 95% CI: 0.129–0.422; p < 0.001) and the number of red blood cell units transfused (weighted mean difference = -0.978; 95% CI = -1.631 to -0.324; p = 0.003). However, there was no difference in calculated blood loss (p = 0.075), operation duration (p = 0.569) and venous thromboembolism complications (p = 0.338). Conclusion: Based on available evidence, use of intravenous TXA for patients undergoing revision arthroplasty may reduce hemoglobin reduction, number of red blood cell units transfused and blood transfusion rate without increasing the risk of venous thromboembolism and length of operation duration. Given the relevant possible biases in our study, adequately powered and better-designed studies with long-term follow-up are required to reach a firmer conclusion.
Currently, patients with total hip arthroplasty (THA) for osteoarthritis, rheumatoid arthritis, femoral neck fracture and femoral head necrosis are increasing by years [1,2]. Similarly, there was an increase in the number of revision total hiparthroplasty (RHA) surgery due to infection, loose prosthesis and prosthetic wear [3–5]. It is estimated that RHA in 2030 may exceed 97,000 cases. The annual revision rate of the hip joint is about 19.05% and the rate of growth is 137% [6]. Perioperative hemorrhagic anemia is the main problem in orthopedic surgery, and the number of transfusions after total joint arthroplasty accounts for 40% of the total number of patients with orthopedic surgery [7–9]. The operation of the RHA still considered being operation with higher blood loss and blood transfusion rate during the perioperative period [10]. Though, surgeons and anesthesiologists have taken a number of steps to reduce perioperative blood loss and blood transfusion including controlled hypotension, local anesthesia, intraoperative blood recycling and erythropoietin [11,12]. Allogeneic blood transfusion could rapidly correct postoperative anemia, but there are obviously related complications: transfusion-related infectious diseases, intravascular hemolysis, transfusion-related acute lung loss and delayed recovery [7,13,14]. As an artificial synthesis of lysine analogs, tranexamic acid (TXA) could reduce calculated blood loss by blocking the antifibrinolysis of lysine binding sites [15]. Recently, some studies on primary THAs have suggested that a single or multiple uses of TXA (10 ∼ 20 mg/kg) could reduce postoperative bleeding without an increase of deep venous thrombosis (DVT) or pulmonary embolism [16–19]. Other studies have shown that intravenous TXA can reduce the bleeding of RHA [20]. Nevertheless, what is the effect of intravenous TXA reducing perioperative blood loss? Whether it will increase the risk of DVT and pulmonary embolism in patients will require further clinical study. Thus, we performed a meta-analysis pooling the relevant literature to definite the clinical effect in RHA.
Materials & methods
PRISMA [21], the abbreviation for Preferred Reporting Items for Systematic Reviews and Meta-Analyses, was used for the study guidelines.
Data sources & searches
Electronic databases including Cochrane Library, Medline (1966-2019.2), PubMed (1966-2019.2), EMBASE (1980-2019.2) and ScienceDirect (1985-2019.2) were searched for comparative studies involving intravenous TXA in patients undergoing revision THA. We retrieved the following keywords in combination with Boolean logic: total hip arthroplasty, total hip replacement, revision and intravenous TXA. Beyond that, the research of the appraisal reference list was manually checked to determine other potential qualification trials. The process iterates until no more articles could be determined.
Inclusion & exclusion criteria
The articles will be incorporated into the present meta-analysis if the literature meets the following preplanned criteria in accordance with PICOS: population: limited the comparison to patients undergoing RHA; intervention: used strictly intravenous TXA and placebo or nothing; comparison: compared the results about reducing blood loss and complications; outcome measures: the primary outcomes included transfusion requirements, hemoglobin (Hb) reduction, operation duration, calculated blood loss, venous thromboembolism (VTE) complications, number of RBC units transfused; and an official published full-text English-written randomized controlled trials (RCTs) or non-RCT. The exclusion criteria were as follows: conference or commentary articles and letters to the editor; animal trials; unclear patient characteristics and outcome data; case reports and case series; systematic reviews or meta-analyses.
Data extraction & outcome measures
Two of the reviewers respectively extracted data from the included studies. The following essential information was captured: first author names, publication year, samples size, study design, and outcomes and other relevant data. The extracted data (median, range and the size of the trial, and mean difference and standard deviation) are put into the designed standardized table according to the Cochrane Handbook. When there are differences of opinion, another authority author has the final decision. The outcome measurements were transfusion requirements, Hb reduction, operation duration, calculated blood loss, VTE complications and number of RBC units transfused.
Quality assessment & statistical analysis
We used the STATA version 11.0 (Stata Corporation, TX, USA) for statistical analyses. When I2 <25%, we considered the data have no obvious heterogeneity, and we conducted a meta-analysis using the fixed-effect model according to the Cochrane Handbook for Systematic Reviews of Interventions (version 5.1.0). Otherwise, the random-effect model was performed. The results of continuous outcomes (Hb reduction, operation duration, calculated blood loss and number of RBC units transfused) were expressed as weighted mean difference (WMD) with 95% CIs. For discontinuous various outcomes (transfusion requirements and VTE complications) odds ratio (OR) with 95% CIs was applied for the assessment.
Results
Search results
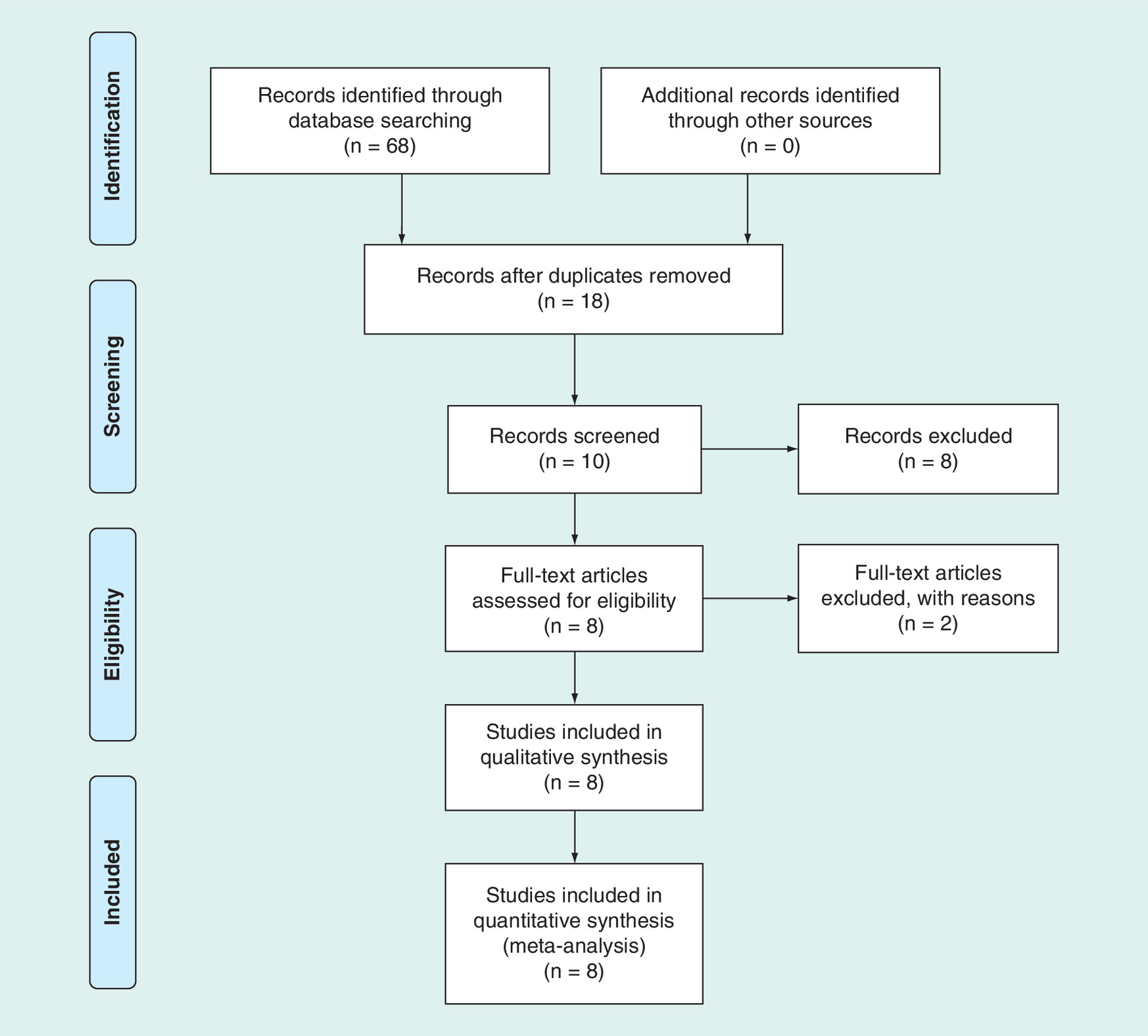
A total of 68 studies were identified as potentially relevant literature reports. Fifty reports were removed because of duplication. By scanning the title and abstract, eight reports were excluded according to the eligibility criteria. Eight reports are eliminated after browsing the full text. No additional studies were obtained after the reference review. Ultimately, eight studies were eligible for data extraction and meta-analysis. The searching process is shown in Figure 1.
Quality assessment
The literature quality evaluation was conducted separately by two reviewers. The study scores of RCT was assessed by Jadad scale. The study scores of all non-RCTs were assessed by Newcastle–Ottawa Scale, maximum of 9 points. The quality of most of the included publications was high, more details were shown Table 1.
| Study (year) | Design | Jadad scale | Total scores | ||
|---|---|---|---|---|---|
| Randomization | Blinding | Cohort | |||
| Gill et al. (2009) | Randomized controlled trial | 2 | 2 | 1 | 5 |
| NOS | |||||
| Selection | Comparability | Exposure | Total scores | ||
| Phillips et al. (2006) | Retrospective cohort study | 2 | 1 | 2 | 5 |
| Kazi et al. (2012) | Prospective cohort study | 3 | 1 | 2 | 6 |
| Duncan et al. (2015) | Retrospective cohort study | 3 | 1 | 2 | 7 |
| Park et al. (2016) | Retrospective cohort study | 4 | 1 | 2 | 7 |
| Mariani et al (2017) | Retrospective cohort study | 4 | 1 | 2 | 7 |
| Peck et al. (2018) | Retrospective cohort study | 3 | 1 | 2 | 6 |
| Reichel et al. (2018) | Retrospective cohort study | 4 | 1 | 3 | 8 |
NOS: Newcastle–Ottawa Scale.
Study characteristics
A total of eight articles (one RCTs [22] and seven non-RCTs [23–29]) were involved in our study. The overall participants of intravenous TXA group were 3533, whereas it was 11,007 in the control group. Demographic characteristics and details concerning the literature type of the included studies are shown in Table 2. Statistically similar baseline characteristics were observed between both the two groups. The methods of intravenous TXA use in RHA are shown in Table 3.
| Study | Year | Design | Recruitment | Sample | Mean age (years) | Gender (M/F) | VTE prophylaxis | |||
|---|---|---|---|---|---|---|---|---|---|---|
| TXA | Control | TXA | Control | TXA | Control | |||||
| Phillips et al. | 2006 | Non-RCT | 2003–2005 | 40 | 40 | Un | Un | Un | Un | LMWH |
| Gill et al. | 2009 | RCT | 2005–2007 | 5 | 5 | 61.4 | 66.6 | 1/4 | 2/3 | Warfarin + mechanical |
| Kazi et al. | 2012 | Non-RCT | 2008–2010 | 30 | 30 | 72 | 73 | 20/10 | 19/11 | LMWH |
| Duncan et al. | 2015 | Non-RCT | 2005–2010 | 2785 | 10,477 | 67 | 67 | Un | Un | Aspirin + LMWH |
| Park et al. | 2016 | Non-RCT | 2012–2014 | 114 | 56 | 63 | 69 | 61/48 | 30/22 | Unclear |
| Mariani et al. | 2017 | Non-RCT | 2011–2014 | 61 | 64 | 67.5 | 69.7 | 34/27 | 23/41 | LMWH |
| Peck et al. | 2018 | Non-RCT | 2008–2016 | 402 | 232 | Un | Un | 133/269 | 93/193 | Un |
| Reichel et al. | 2018 | Non-RCT | 2014–2016 | 96 | 103 | 66.1 | 68.6 | 39/57 | 47/56 | Enoxaparin |
F: Female; LMWH: Low-molecular-weight heparin; M: Male; non-RCT: Nonrandomized controlled trial; RCT: Randomized controlled trial; TXA: Tranexamic acid; VTE: Venous thromboembolism; Un: Unclear.
| Study | Year | Intervention of tranexamic acid |
|---|---|---|
| Phillips et al. | 2006 | TXA 10 mg/kg iv. 30 min before incision, then 10 mg/kg further dose after 6 h from operation |
| Gill et al. | 2009 | TXA 10 mg/kg iv. before induction of anesthesia, then 1 mg/kg/h infusion until wound closure |
| Kazi et al. | 2012 | TXA 10 mg/kg iv. 30 min before operation and 10 mg/kg iv. further dose after 3 h from operation |
| Duncan et al. | 2015 | TXA 1 g was infused before incision, then 1 g was infused immediately before closure |
| Park et al. | 2016 | TXA 1 g iv. at incision and TXA 1 g iv. further dose after 2 h from operation |
| Mariani et al. | 2017 | TXA 1 g iv. before skin incision and TXA 1 g iv. further dose until wound closure |
| Peck et al. | 2018 | TXA 20 mg/kg iv. before operative in all revision total hip arthroplasty cases |
| Reichel et al. | 2018 | TXA 10 mg/kg bodyweight was received by every patient suffering revision total hip arthroplasty and 1 mg/kg bodyweight/h further dose intraoperatively |
iv.: Intravenously; TXA: Tranexamic acid.
Outcomes of meta-analysis
Six outcomes were assessed with our meta-analysis: calculated blood loss, Hb reduction, transfusion requirements, number of RBC units transfused, operation duration and VTE complications (Table 4).
| Outcome | Studies | Groups | Overall effect | Heterogeneity | ||||
|---|---|---|---|---|---|---|---|---|
| TXA | Placebo | Effect estimate | 95% CI | p-value | I2 (%) | p-value | ||
| Calculated blood loss | 4 | 642 | 421 | -177.255 | -372.430 to 17.919 | 0.075 | 72.9 | 0.011 |
| Hemoglobin reduction | 2 | 144 | 86 | -1.405 | -1.810 to -0.999 | 0.000 | 42.5 | 0.187 |
| Transfusion requirements | 7 | 748 | 530 | 0.233 | 0.129 to 0.422 | 0.000 | 66.2 | 0.007 |
| RBC units transfused | 4 | 192 | 202 | -0.978 | -1.631 to -0.324 | 0.003 | 55.8 | 0.079 |
| Duration of operation | 2 | 210 | 159 | -6.037 | -26.775 to 14.702 | 0.568 | 51.2 | 0.152 |
| VTE complications | 5 | 3384 | 10,916 | 0.846 | 0.601 to 1.191 | 0.338 | 0.0 | 0.759 |
RBC: Red blood cell; TXA: Tranexamic acid; VTE: Venous thromboembolism.
Calculated blood loss
Four literatures provided the number of calculated blood loss. The results show 642 cases in the experimental group and 421 cases in the control group. Significant heterogeneity was observed, and a random effects model was used (I2 = 72.9%, p = 0.011). The calculated blood loss between the experimental and the control groups was not statistically significant (WMD = -177.255, 95% CI: -372.430, 17.919; p = 0.075; Figure 2).
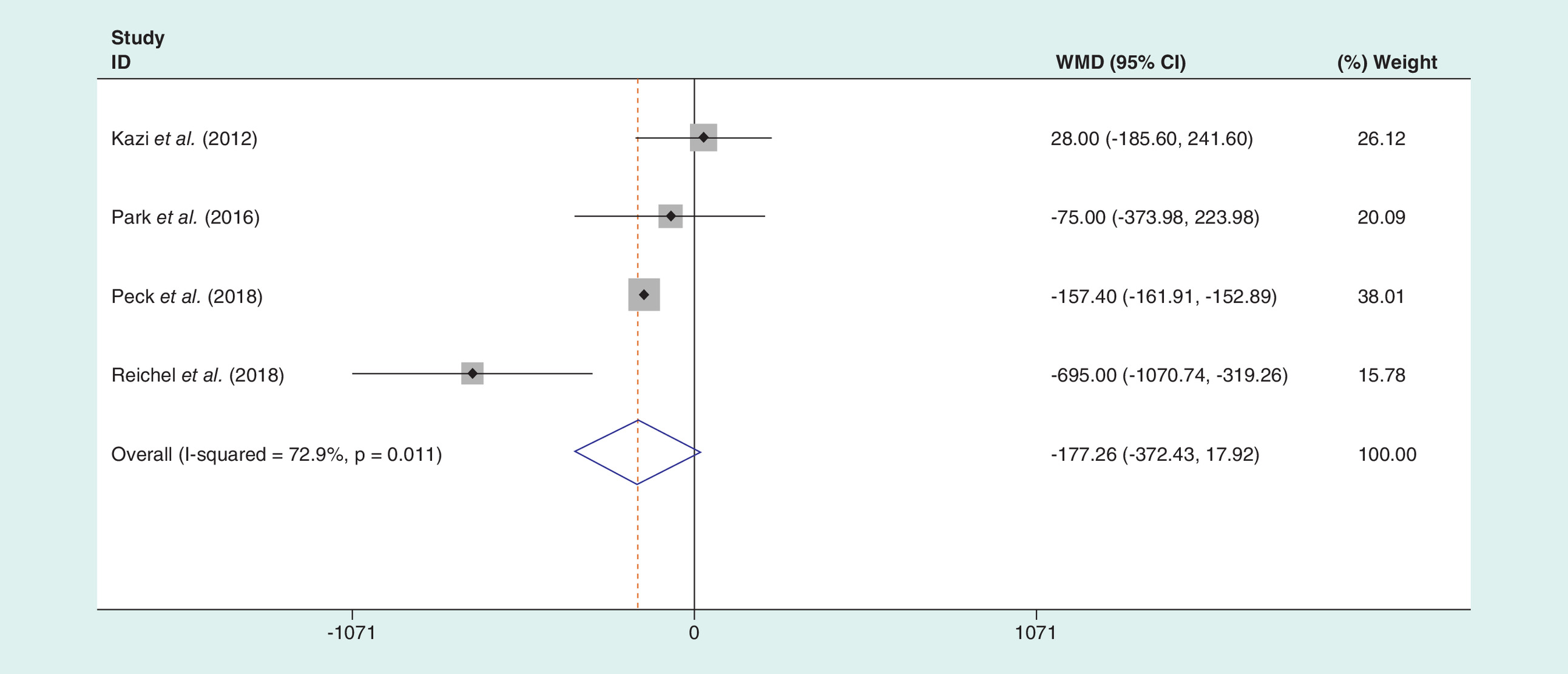
Figure 2. Forest plot on the assessment of the calculated blood loss.
WMD: Weighted mean difference.
Hemoglobin reduction
Two literatures provided the values of Hb reduction. A moderate heterogeneity was found (I2 = 42.5%, p = 0.187), we used random-effect model. The results show that there was a statistical difference between the experimental and the control groups (WMD = -1.277, 95% CI: -1.996, -0.559; p < 0.001; Figure 3). The present meta-analysis demonstrates intravenous TXA with a lower value of Hb reduction than placebo or nothing in RHA.
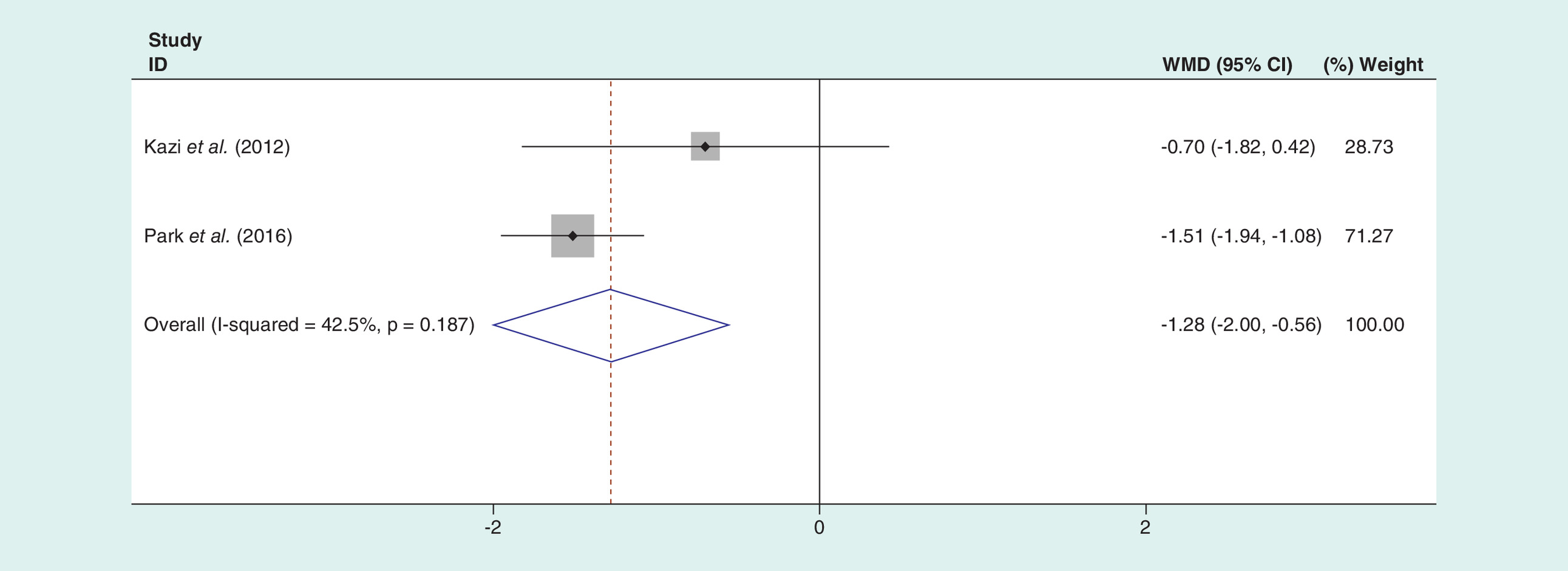
Figure 3. Forest plot on the assessment of the hemoglobin reduction.
WMD: Weighted mean difference.
Transfusion requirements
Seven literatures concentrated on the blood transfusion rate. Significant heterogeneity was found (I2 = 66.2%, p = 0.007), we used random model. The results show that there was a significant difference between experimental and control groups (OR: 0.233; 95% CI: 0.129, 0.422; p < 0.001; Figure 4). The present meta-analysis demonstrates intravenous TXA with a lower rate of blood transfusion than placebo or nothing in RHA.
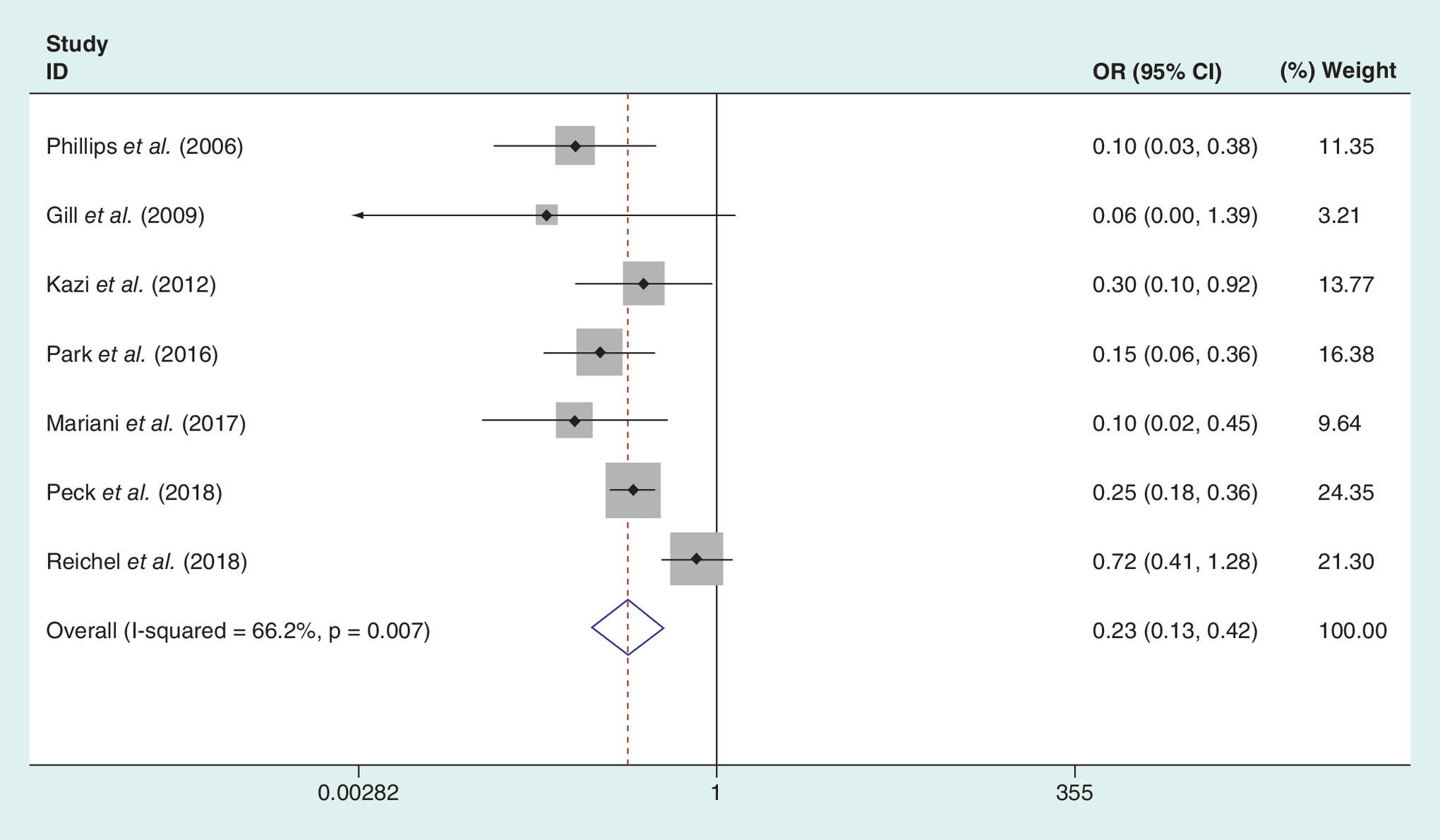
Figure 4. Forest plot on the assessment of the transfusion requirements.
OR: Odds ratio.
Number of RBC units transfused
Four articles mentioned the number of RBC units transfused and data pooled by a random effects model to reveal that there was a significant difference between the two groups (WMD = -0.978, 95% CI: -1.631 to -0.324; p = 0.003; Figure 5). The present meta-analysis demonstrates intravenous TXA with a lower number of RBC units transfused than placebo or nothing in RHA.
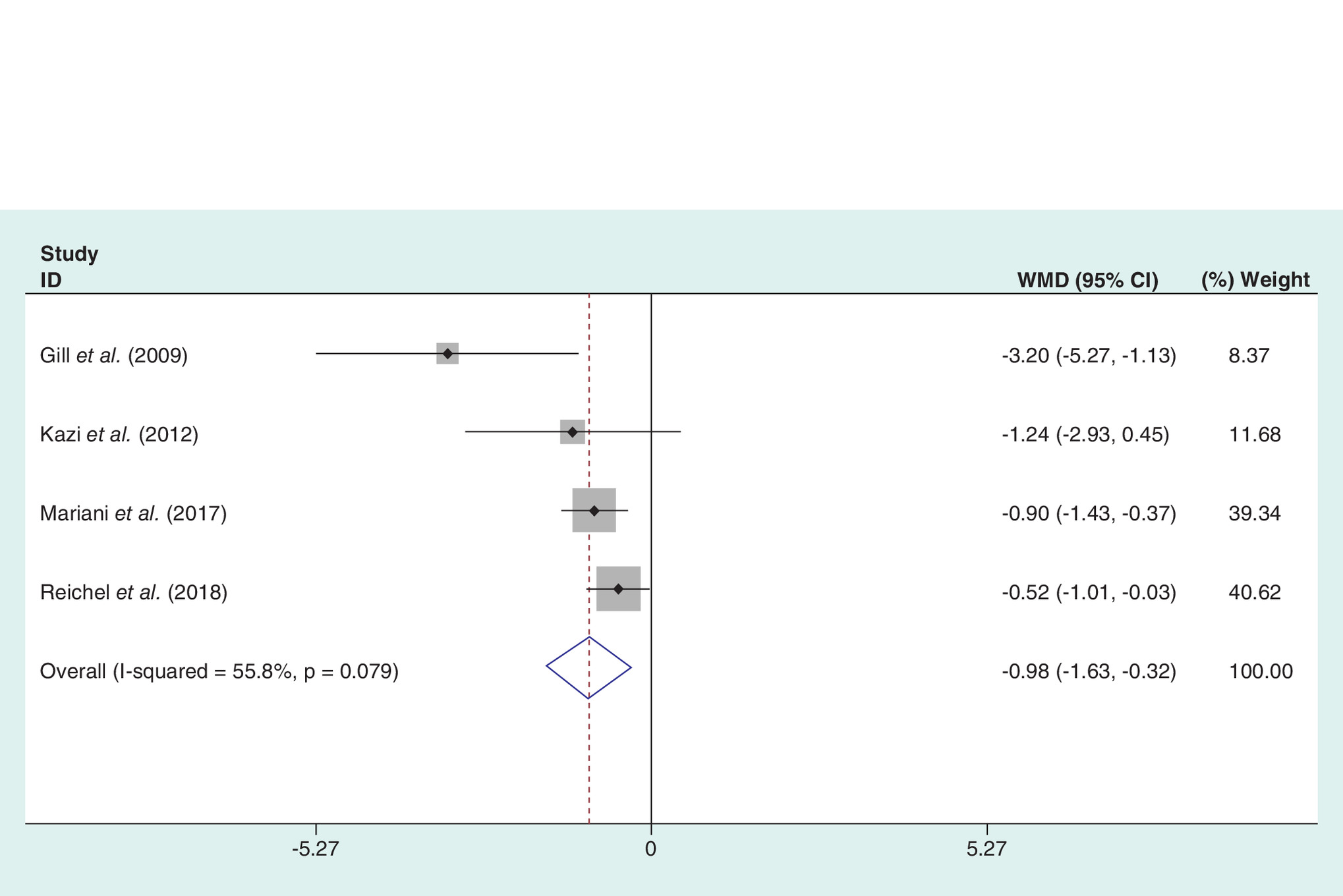
Figure 5. Forest plot on the assessment of the number of red blood cell units transfused.
WMD: Weighted mean difference.
Operation duration
Two articles mentioned the operation duration and data pooled by a random effects model to reveal that there was no significant difference between the two groups (WMD = -6.037, 95% CI: -26.775–14.702; p = 0.569; Figure 6).
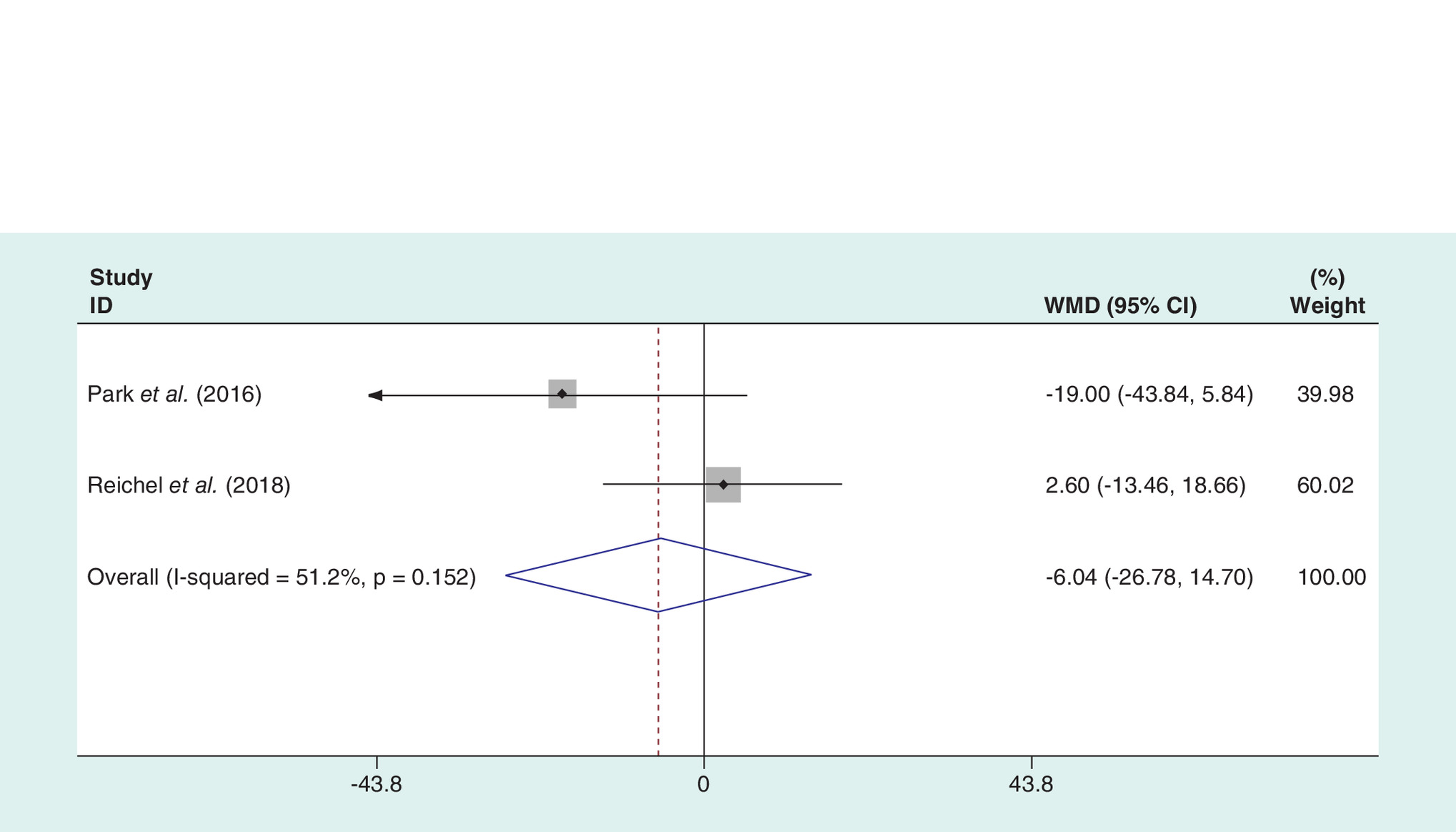
Figure 6. Forest plot on the assessment of the operation duration.
WMD: Weighted mean difference.
VTE complications
Five literatures provided the numbers of VTE in patients. No significant heterogeneity was found, fixed model was used (p = 0.759, I2 = 0.0%). The results show that there was no statistical difference between the experimental and the control groups (OR: 0.846; 95% CI: 0.601–1.191; p = 0. 338; Figure 7).
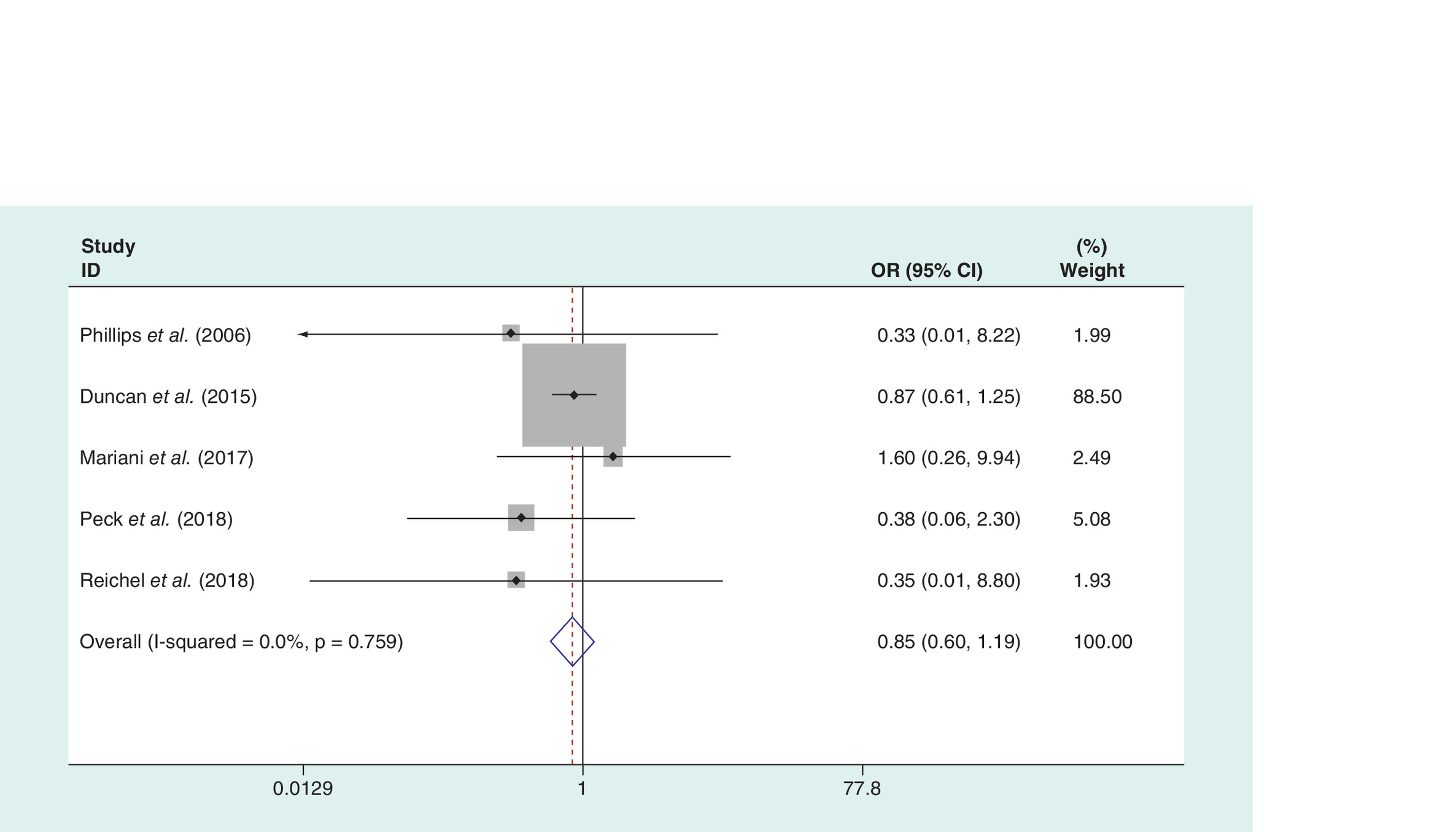
Figure 7. Forest plot on the assessment of the venous thromboembolism complications.
OR: Odds ratio.
Discussion
At present, most of the studies suggest that for patients with primary joint replacement, using small doses of intravenous TXA can effectively reduce the patients with perioperative blood loss, postoperative transfusion rate, the risk of surgery and hospitalization expenses and length of hospital stay [30–33]. Recently, intravenous TXA has applied in revision joint replacement. Extensive tissue damage and longer operation duration in the revision arthroplasty are usually associated with increased intraoperative and calculated blood loss [34]. The tissue damage caused by revision surgery could activate the fibrinolytic system, which is one of the reasons for the inevitable hemorrhage after surgery. As an artificial synthesis of lysine analogs, TXA could reduce perioperative blood loss by blocking the antifibrinolysis of lysine binding sites [15,35]. Yamasaki [36] found that the most bleeding time in 2 h after joint arthroplasty was followed by a gradual decrease in drainage volume per hour over time. Although TXA has been widely used to reduce blood loss and transfusion requirements in primary THA [37–40], little is known about the efficacy and safety of the use of TXA in RHA. This is the first meta-analysis, aimed to intravenous TXA, reduces blood transfusions in RHA and showed that intravenous TXA is preferable for RHA because of its lower value of Hb reduction, rate of blood transfusion and the number of RBC units transfused. However, there was no difference in calculated blood loss, operation duration and VTE complications.
As we all know, intravenous TXA has been effectively demonstrated to reduced Hb loss in THA [41,42]. One recent meta-analysis in THA patients showed that intravenous TXA was significantly associated with a lower reduction of Hb drop compared with control group (mean difference [MD] = -0.85; p < 0.001; 95% CI: -1.26 to -0.44) [42]. Intravenous TXA could reduce Hb loss up to 6.03 g/l compared with that in the control group in THA patients (p = 0.001; 95% CI: 3.90–8.15 g/l) [41]. Kzai et al. [24] use a large hospital database to assess the efficacy of intravenous TXA in patients undergoing RHA and found that the mean Hb reduction was 2.7 g/dl in the TXA group and 3.4 g/dl in the control group. There was a significant reduction in Hb reduction (TXA: 2.02 ± 1.27 g/l vs Control [CON]: 3.53 ± 1.40 g/l; p < 0.001) in the study of Park et al. [26]; the data of 144 participants in TXA group and 86 participants in the control group were extracted to make a further credible investigation. Similarly, the result of our meta-analysis (WMD = -1.405, 95% CI: -1.810, -0.999; p < 0.001) shows that intravenous TXA could significantly reduce the Hb reduction compared with the control group.
The seven included studies evaluate the effect of intravenous TXA on postoperative blood transfusion rate. Phillips et al. [20] found the application of TXA in RHA could effectively reduce the postoperative blood transfusion rate. The present meta-analysis shows that blood transfusion rate in the TXA group (40.37%) was significantly lower than that in control group (71.13%). Our pooled data demonstrated that intravenous TXA could effectively reduce the postoperative blood transfusion rate (OR: 0.233; 95% CI: 0.129–0.422; p < 0.001), which is in accordance with the research of Noordin et al. [43] and Kzai et al. [44]. At the same time, a reduction in the number of RBC unit transfused per patient is also a concern in RHA. In primary THA, one meta-analysis showed that reduction of the number of RBC units transfused per patient was not significantly in TXA group compared with the placebo group (WMD = 0.3, 95% CI: -0.49–1.09; p = 0.45) [41]. Our meta-analysis found that the number of RBC units transfused was significantly lower in the TXA group compared with the control group in RHA (WMD = -0.978, 95% CI: -1.631 to -0.324; p = 0.003). However, a high heterogeneity appeared in these results, we hypothesized that the transfusion trigger was the source of high heterogeneity.
Andreu et al. [45] measured blood loss in the drain at 24 h and found it is significantly differed in both groups, confirming more visible blood loss in the control group (TXA: 256.4 ± 266.6, CON: 594.6 ± 422.3, p = 0.009); they believes intravenous TXA administration appeared as an effective means of reducing blood loss in revision total knee arthroplasty operation. Based on the existing research results, Blanie et al. [46] believed that the fibrinolysis effect of the body will reach the peak around 6 h after surgery, and reduced to the preoperative level at 24 h after an operation. The optimal time for control and reduction of blood loss due to the activation of the fibrinolytic system during the perioperative period was from the beginning of surgery to 6 h after surgery [47–49]. The antifibrinolytic effect of TXA can last about 8 h, so it could limit the body’s hyperfibrinolysis to the maximum extent [47–49]. However, from our meta-analysis, four articles mentioned the number of calculated blood loss were pooled and showed that no statistically significant difference was found in the calculated blood loss between the experimental group and the control group. It may be due to the relatively small sample size of the included literatures. In our study, three articles measured calculated blood loss excluding the hidden blood loss while Reichel et al. [29] measured calculated blood loss according to the Brecher formula [50] that the hidden blood loss was included. Meanwhile, the heterogeneity reduced a lot when this article was excluded (I2 = 37.2; p = 0.204). The conclusion is still to be proved, more powered and better-designed studies are necessary to reach a firmer conclusion.
The security of antifibrinolytic agents in orthopedics major surgery has always been a topic of discussion, and whether the use of intravenous TXA will increase the risk of DVT after surgery is also a hot concern for surgeons. Although many scholars believe that the risk of VTE in Asian population is lower than that in the European and American populations, the literature reports that it still has a higher incidence of VTE [51,52]. Fargen et al. [53] showed that the preoperative TXA 10 mg/kg dose was widely believed to reduce blood loss and to prevent DVT, but several foreign studies [35,54–56] reported that the use of TXA in the perioperative period of primary joint arthroplasty surgery did not increase the incidence of VTE compared with the control group. The present meta-analysis demonstrated that intravenous TXA was not associated with an increased complication rate of VTE. At the same time, the results of our pooled data demonstrated that there was no statistic difference in length of operation duration (WMD = -6.037, 95% CI: -26.775–14.702; p = 0.569).
Our research also has some limitations that should be considered. First, the sample size of the included literature is too small. Second, different administrations of TXA, operation methods and study designs, especially in retrospective cohort study (RCSs), might have a biased impact on our results. Third, lacking long-term evaluation indexes such as Keen Society Score and range of motion. Fourth, the heterogeneity of hidden blood loss was still moderate due to no gold standard; more powered and better-designed studies are necessary to reach a firmer conclusion. Finally, the sample sizes of the included studies are relatively small in the present meta-analysis.
Conclusion
Based on available evidence, use of intravenous TXA for patients undergoing revision arthroplasty may reduce Hb reduction, number of RBC units transfused and blood transfusion rate without increasing the risk of VTE and length of operation duration. Given the relevant possible biases in our study, adequately powered and better-designed studies with long-term follow-up are required to reach a firmer conclusion.
•
We performed a meta-analysis pooling the relevant literature to define the clinical effect in revision total hiparthroplasty. Potential academic articles were identified from Cochrane Library, Medline, PubMed, EMBASE, ScienceDirect and other databases. STATA version 11.0 was used to analyze the pooled data.
•
The overall participants of tranexamic acid (TXA) group were 3533, whereas it was 11,007 in the control group.
•
Our meta-analysis showed that TXA is preferable for revision total hiparthroplasty because of its lower value of hemoglobin reduction, the rate of blood transfusion and the number of red blood cell units transfused.
•
However, there was no difference in calculated blood loss, operation duration and venous thromboembolism complications.
•
Based on available evidence, use of intravenous TXA for patients undergoing revision arthroplasty may reduce hemoglobin reduction, number of red blood cell units transfused, and blood transfusion rate without increasing the risk of venous thromboembolism and length of operation duration.
Financial & competing interests disclosure
This work was supported by funding from the National Natural Science Foundation of China (no. 81570507, XY Yang). The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Lehil MS, Bozic KJ. Trends in total hip arthroplasty implant utilization in the United States. J. Arthrop. 29(10), 1915–1918 (2014).
2.
Nguyen LC, Lehil MS, Bozic KJ. Trends in total knee arthroplasty implant utilization. J. Arthrop. 30(5), 739–742 (2015).
3.
Peersman G, Laskin R, Davis J, Peterson M. Infection in total knee replacement: a retrospective review of 6489 total knee replacements. Clin. Orthop. Rel. Res. (392), 15–23 (2001).
4.
Patel VP, Walsh M, Sehgal B, Preston C, Dewal H, Di Cesare PE. Factors associated with prolonged wound drainage after primary total hip and knee arthroplasty. J. Bone Joint Surg. Am. 89(1), 33–38 (2007).
• Shows that the number of revision total hiparthroplasty surgery increases a lot.
5.
Soohoo NF, Zingmond DS, Lieberman JR, Ko CY. Optimal timeframe for reporting short-term complication rates after total knee arthroplasty. J. Arthrop. 21(5), 705–711 (2006).
6.
Kurtz S, Ong K, Lau E, Mowat F, Halpern M. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J. Bone Joint Surg. Am. 89(4), 780–785 (2007).
7.
Oremus K. Tranexamic acid for the reduction of blood loss in total knee arthroplasty. Ann. Transl. Med. 3(Suppl. 1), S40 (2015).
8.
Ponnusamy KE, Kim TJ, Khanuja HS. Perioperative blood transfusions in orthopaedic surgery. J. Bone Joint Surg. Am. 96(21), 1836–1844 (2014).
9.
Ho KM, Ismail H. Use of intravenous tranexamic acid to reduce allogeneic blood transfusion in total hip and knee arthroplasty: a meta-analysis. Anaesthesiol. Int. Care 31(5), 529–537 (2003).
10.
Bridgens JP, Evans CR, Dobson PM, Hamer AJ. Intraoperative red blood-cell salvage in revision hip surgery. A case-matched study. J. Bone Joint Surg. Am. 89(2), 270–275 (2007).
11.
Cardone D, Klein AA. Perioperative blood conservation. Eur. J. Anaesthesiol. 26(9), 722–729 (2009).
12.
Zufferey P, Merquiol F, Laporte S et al. Do antifibrinolytics reduce allogeneic blood transfusion in orthopedic surgery? Anesthesiology 105(5), 1034–1046 (2006).
13.
Bierbaum BE, Callaghan JJ, Galante JO, Rubash HE, Tooms RE, Welch RB. An analysis of blood management in patients having a total hip or knee arthroplasty. J. Bone Joint Surg. Am. 81(1), 2–10 (1999).
14.
Carling MS, Jeppsson A, Eriksson BI, Brisby H. Transfusions and blood loss in total hip and knee arthroplasty: a prospective observational study. J. Orthop. Surg. Res. 10, 48 (2015).
15.
Struijk-Mulder MC, Horstmann WG, Verheyen CC, Ettema HB. Ten-year follow-up on Dutch orthopaedic blood management (DATA III survey). Arch. Orthop. Trauma Surg. 134(1), 15–20 (2014).
16.
Alshryda S, Sukeik M, Sarda P, Blenkinsopp J, Haddad FS, Mason JM. A systematic review and meta-analysis of the topical administration of tranexamic acid in total hip and knee replacement. Bone Joint J. 96-b(8), 1005–1015 (2014).
17.
Zhang H, Chen J, Chen F, Que W. The effect of tranexamic acid on blood loss and use of blood products in total knee arthroplasty: a meta-analysis. Knee Surg. Sports Traumatol. Arthrosc. 20(9), 1742–1752 (2012).
18.
Yang ZG, Chen WP, Wu LD. Effectiveness and safety of tranexamic acid in reducing blood loss in total knee arthroplasty: a meta-analysis. J. Bone Joint Surg. Am. 94(13), 1153–1159 (2012).
19.
Gillette BP, Desimone LJ, Trousdale RT, Pagnano MW, Sierra RJ. Low risk of thromboembolic complications with tranexamic acid after primary total hip and knee arthroplasty. Clin. Orthop. Rel. Res. 471(1), 150–154 (2013).
20.
Phillips SJ, Chavan R, Porter ML et al. Does salvage and tranexamic acid reduce the need for blood transfusion in revision hip surgery? J. Bone Joint Surg. Br. 88(9), 1141–1142 (2006).
21.
Akhigbe T, Zolnourian A, Bulters D. Compliance of systematic reviews articles in brain arteriovenous malformation with PRISMA statement guidelines: review of literature. J. Clin. Neurosci. 39, 45–48 (2017).
•• We performed a meta-analysis according to PRISMA statement guidelines, but issue number in this reference was undefined.
22.
Gill JB. The use of tranexamic acid in revision total hip arthroplasty: a pilot study. Curr. Opin. Orthop. 20(2), 152–156 (2009).
•• A high-quality randomized controlled trial.
23.
Phillips SJ, Chavan R, Porter ML et al. Does salvage and tranexamic acid reduce the need for blood transfusion in revision hip surgery? J. Bone Joint Surg. Br. 88(9), 1141–1142 (2006).
24.
Kazi HA, Fountain JR, Thomas TG, Carroll FA. The effect of bolus administration of tranexamic acid in revision hip arthroplasty. Hip Int. 22(6), 615–620 (2012).
25.
Duncan CM, Gillette BP, Jacob AK, Sierra RJ, Sanchez-Sotelo J, Smith HM. Venous thromboembolism and mortality associated with tranexamic acid use during total hip and knee arthroplasty. J. Arthrop. 30(2), 272–276 (2015).
26.
Park KJ, Couch CG, Edwards PK, Siegel ER, Mears SC, Barnes CL. Tranexamic acid reduces blood transfusions in revision total hip arthroplasty. J. Arthrop. 31(12), 2850–2855.e2851 (2016).
27.
Mariani P, Buttaro MA, Slullitel PA et al. Transfusion rate using intravenous tranexamic acid in hip revision surgery. Hip Int. 28(2), 194–199 (2018).
28.
Peck J, Kepecs DM, Mei B et al. The effect of preoperative administration of intravenous tranexamic acid during revision hip arthroplasty: a retrospective study. J. Bone Joint Surg. Am. 100(17), 1509–1516 (2018).
29.
Reichel F, Peter C, Ewerbeck V, Egermann M. Reducing blood loss in revision total hip and knee arthroplasty: tranexamic acid is effective in aseptic revisions and in second-stage reimplantations for periprosthetic infection. BioMed Res. Int. (2018) (Epub ahead of print).
30.
Imai N, Dohmae Y, Suda K, Miyasaka D, Ito T, Endo N. Tranexamic acid for reduction of blood loss during total hip arthroplasty. J. Arthrop. 27(10), 1838–1843 (2012).
31.
Mcconnell JS, Shewale S, Munro NA, Shah K, Deakin AH, Kinninmonth AW. Reduction of blood loss in primary hip arthroplasty with tranexamic acid or fibrin spray. Acta Orthopaed. 82(6), 660–663 (2011).
32.
Ralley FE, Berta D, Binns V, Howard J, Naudie DD. One intraoperative dose of tranexamic acid for patients having primary hip or knee arthroplasty. Clin. Orthop. Rel. Res. 468(7), 1905–1911 (2010).
33.
Kazemi SM, Mosaffa F, Eajazi A et al. The effect of tranexamic acid on reducing blood loss in cementless total hip arthroplasty under epidural anesthesia. Orthopedics 33(1), 17 (2010).
34.
Sehat KR, Evans RL, Newman JH. Hidden blood loss following hip and knee arthroplasty. Correct management of blood loss should take hidden loss into account. J. Bone Joint Surg. Br. 86(4), 561–565 (2004).
35.
Mccormack PL. Tranexamic acid: a review of its use in the treatment of hyperfibrinolysis. Drugs 72(5), 585–617 (2012).
36.
Yamasaki S, Masuhara K, Fuji T. Tranexamic acid reduces blood loss after cementless total hip arthroplasty-prospective randomized study in 40 cases. Int. Orthop. 28(2), 69–73 (2004).
37.
Moskal JT, Capps SG. Meta-analysis of intravenous tranexamic acid in primary total hip arthroplasty. Orthopedics 39(5), e883–892 (2016).
38.
Alshryda S, Sukeik M, Sarda P, Blenkinsopp J, Haddad FS, Mason JM. A systematic review and meta-analysis of the topical administration of tranexamic acid in total hip and knee replacement. Bone Joint J. 8, 1005–1015 (2014).
39.
Gandhi R, Evans HM, Mahomed SR, Mahomed NN. Tranexamic acid and the reduction of blood loss in total knee and hip arthroplasty: a meta-analysis. BMC Res. Notes 6, 184 (2013).
40.
Wang C, Xu GJ, Han Z et al. Topical application of tranexamic acid in primary total hip arthroplasty: a systemic review and meta-analysis. Int. J. Surg. 15, 134–139 (2015).
41.
Zhou XD, Tao LJ, Li J, Wu LD. Do we really need tranexamic acid in total hip arthroplasty? A meta-analysis of nineteen randomized controlled trials. Arch. Orthop. Trauma Surg. 133(7), 1017–1027 (2013).
42.
Wu Q, Zhang HA, Liu SL, Meng T, Zhou X, Wang P. Is tranexamic acid clinically effective and safe to prevent blood loss in total knee arthroplasty? A meta-analysis of 34 randomized controlled trials. Eur. J. Orthop. Surg. Traumatol. 25(3), 525–541 (2015).
• Tranexamic acid significantly reduced the leveal of hemoglobin in total hip arthroplasty.
43.
Noordin S, Waters TS, Garbuz DS, Duncan CP, Masri BA. Tranexamic acid reduces allogenic transfusion in revision hip arthroplasty. Clin. Orthop. Rel. Res. 469(2), 541–546 (2011).
44.
Kazi HA, Fountain JR, Thomas TG, Carroll FA. The effect of bolus administration of tranexamic acid in revision hip arthroplasty. Hip Int. 22(6), 615–620 (2012).
45.
Ortega-Andreu M, Talavera G, Padilla-Eguiluz NG et al. Tranexamic acid in a multimodal blood loss prevention protocol to decrease blood loss in revision total knee arthroplasty: a cohort study. Open Orthop. J. 10, 439–447 (2016).
46.
Blanie A, Bellamy L, Rhayem Y et al. Duration of postoperative fibrinolysis after total hip or knee replacement: a laboratory follow-up study. Thrombosis Res. 131(1), e6–e11 (2013).
47.
Burleson A, Guler N, Banos A et al. Perioperative factors and their effect on the fibrinolytic system in arthroplasty patients. Clin. Appl. Thromb. Hemost. 22(3), 274–279 (2016).
48.
Macaulay W, Westrich G, Sharrock N et al. Effect of pneumatic compression on fibrinolysis after total hip arthroplasty. Clin. Orthop. Rel. Res. (399), 168–176 (2002).
49.
Yoshida K, Wada H, Hasegawa M et al. Increased fibrinolysis increases bleeding in orthopedic patients receiving prophylactic fondaparinux. Int. J. Hematol. 95(2), 160–166 (2012).
50.
Brecher ME, Monk T, Goodnough LT. A standardized method for calculating blood loss. Transfusion 37(10), 1070–1074 (2010).
51.
Swayze OS, Nasser S, Roberson JR. Deep venous thrombosis in total hip arthroplasty. Orthop. Clin. N. Am. 23(2), 359–364 (1992).
52.
Stulberg BN, Insall JN, Williams GW, Ghelman B. Deep-vein thrombosis following total knee replacement. An analysis of six hundred and thirty-eight arthroplasties. J. Bone Joint Surg. Am. 66(2), 194–201 (1984).
53.
Fargen KM, Velat GJ, Lawson MF, Hoh BL, Mocco J. The stent anchor technique for distal access through a large or giant aneurysm. J. Neurointervent. Surg. 5(4), e24 (2013).
54.
Irisson E, Hemon Y, Pauly V, Parratte S, Argenson JN, Kerbaul F. Tranexamic acid reduces blood loss and financial cost in primary total hip and knee replacement surgery. Orthop. Traumatol. Surg. Res. 98(5), 477–483 (2012).
55.
Clave A, Fazilleau F, Dumser D, Lacroix J. Efficacy of tranexamic acid on blood loss after primary cementless total hip replacement with rivaroxaban thromboprophylaxis: a case–control study in 70 patients. Orthop. Traumatol. Surg. Res. 98(5), 484–490 (2012).
56.
Singh J, Ballal MS, Mitchell P, Denn PG. Effects of tranexamic acid on blood loss during total hip arthroplasty. J. Orthop. Surg. 18(3), 282–286 (2010).
Information & Authors
Information
Published In
Pages: 917 - 928
PubMed: 31436114
Copyright
© 2019 Future Medicine Ltd.
History
Received: 21 February 2019
Accepted: 17 May 2019
Published online: 22 August 2019
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Intravenous tranexamic acid reduces blood transfusions in revision total hip arthroplasty: a meta-analysis. (2019) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2019-0030
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Amir Human Hoveidaei, Reza Niakan, Amirhossein Salmannezhad, Alireza Pouramini, Ryan Palmer, Sagar Telang, Nathanael D. Heckmann, The Efficacy and Safety of Tranexamic Acid in Revision Total Knee and Total Hip Arthroplasty: A Systematic Review and Meta-Analysis, Arthroplasty Today, 10.1016/j.artd.2026.102054, 40, (102054), (2026).
- Niklas H. Koehne, Auston R. Locke, Samuel C. Frohlich, Kalyn Y. Dawes, Christoph A Schroen, Robert L. Parisien, The statistical fragility of tranexamic acid dosage and route of administration in total hip arthroplasty: A systematic review, Injury, 10.1016/j.injury.2025.112833, 56, 12, (112833), (2025).
- R. K. Gigengack, J. Slob, A. Meij-de Vries, E. Bosma, S. A. Loer, J. S. H. A. Koopman, C. H. van der Vlies, Efficacy of tranexamic acid versus placebo in reducing blood loss during burn excisional surgery: a multi-center, double-blind, parallel, randomized placebo-controlled clinical trial (TRANEX), Trials, 10.1186/s13063-024-08332-1, 25, 1, (2024).
- Mohammad Ghorbani, Seyed Hassan Sadrian, Rezvan Ghaderpanah, Colin C. Neitzke, Brian P. Chalmers, Saeid Esmaeilian, Elham Rahmanipour, Ali Parsa, Tranexamic acid in total hip arthroplasty: An umbrella review on efficacy and safety, Journal of Orthopaedics, 10.1016/j.jor.2024.03.010, 54, (90-102), (2024).
- Sibylle Kietaibl, Aamer Ahmed, Arash Afshari, Pierre Albaladejo, Cesar Aldecoa, Giedrius Barauskas, Edoardo De Robertis, David Faraoni, Daniela C. Filipescu, Dietmar Fries, Anne Godier, Thorsten Haas, Matthias Jacob, Marcus D. Lancé, Juan V. Llau, Jens Meier, Zsolt Molnar, Lidia Mora, Niels Rahe-Meyer, Charles M. Samama, Ecaterina Scarlatescu, Christoph Schlimp, Anne J. Wikkelsø, Kai Zacharowski, Management of severe peri-operative bleeding: Guidelines from the European Society of Anaesthesiology and Intensive Care, European Journal of Anaesthesiology, 10.1097/EJA.0000000000001803, 40, 4, (226-304), (2023).
- John R. Wickman, Breanna A. Polascik, Daniel Goltz, Taylor P. Stauffer, Jay Levin, Tally Lassiter, Christopher Klifto, Oke Anakwenze, The effect of intravenous tranexamic acid use on blood loss after revision shoulder arthroplasty, Seminars in Arthroplasty: JSES, 10.1053/j.sart.2022.07.011, 32, 4, (671-675), (2022).
- Chao Qin, Kai-li Du, Pei-yu Guo, Hong-da Gong, Chun-qiang Zhang, Tranexamic acid dosage for spinal surgery: a meta-analysis, European Spine Journal, 10.1007/s00586-022-07315-7, 31, 10, (2493-2501), (2022).