Persistence and adherence of biologics in US patients with psoriatic arthritis: analyses from a claims database
Abstract
Aim: To evaluate the persistence and adherence of subcutaneous biologics in patients with psoriatic arthritis (PsA). Patients & methods: Psoriatic arthritis patients who initiated adalimumab, certolizumab pegol, etanercept, golimumab or secukinumab between 15 January 2016 and 31 July 2017 were identified in the Truven Databases. Outcomes included discontinuation rate, persistence and adherence over 12 months. Results: Of 1558 patients included, the 12-month discontinuation rate was lowest with secukinumab (36.5%), followed by adalimumab, golimumab, etanercept and certolizumab pegol (42.6–51.6%). Mean persistence ranged from 240.7 (certolizumab pegol) to 282.8 days (secukinumab). The mean proportion of days covered was highest with secukinumab (0.67) and lowest with certolizumab pegol (0.49). Conclusion: Patients who initiated secukinumab had the lowest discontinuation rate and highest persistence and adherence over 12 months.
Psoriatic arthritis (PsA) is a chronic, progressive inflammatory condition of the skin and musculoskeletal system that affects 0.06–0.25% of the US population [1,2]. Manifestations of PsA include peripheral arthritis, enthesitis, dactylitis, axial involvement, and psoriatic skin and nail disease, which may occur alone or in combination [3]. PsA symptoms may range from mild to very severe, and may occur alone or in combination with each other, complicating disease management [4].
International guidelines developed by the Group for Research and Assessment of Psoriasis and Psoriatic Arthritis, and the European League Against Rheumatism recommend that first-line therapy include topicals, NSAIDs and/or corticosteroids [5,6]. However, for patients with moderate to severe PsA, or whose disease remains active despite conventional therapies, conventional synthetic disease-modifying antirheumatic drugs (DMARDs), targeted synthetic DMARDs or biologic therapies are recommended. Although TNF inhibitors (TNFis) were the only biologic options for many years [7–12], several newer biologic therapies have since been approved for the treatment of PsA, including the IL-12/23 inhibitor ustekinumab [13,14], the IL-17A inhibitors ixekizumab [15,16] and secukinumab [17,18], and the selective T-cell co-stimulatory modulator abatacept [19,20], providing patients and rheumatologists with the choice between a variety of biologics that have different mechanisms of action (MOAs), routes of administration and safety profiles.
The goals of treatment for patients with PsA are to achieve the lowest possible level of disease activity across all domains; to optimize functional status, improve quality of life and prevent structural damage; and to avoid or minimize complications, either from untreated active disease or from the therapy itself [5]. Better outcomes may be achieved with more frequent assessment of disease activity with dose escalations/changes, if needed [21]. Several studies have shown that switching biologics in clinical practice may lead to improved outcomes in some patients with PsA, while others would benefit from switching to a therapy with a different MOA; however, most of these studies examined only TNFis and/or were conducted outside the USA [22,23]. There is an unmet need to characterize persistence with and adherence to newer biologics with different MOAs in clinical practice, particularly in the USA, because high rates of discontinuation or switching and/or lower rates of adherence may suggest suboptimal treatment.
Secukinumab is a fully human anti-IL-17A monoclonal antibody approved for the treatment of PsA in the USA and was the first biologic approved for PsA targeting the IL-17 pathway [17,18]. Updated analyses of real-world data to examine treatment patterns with newly available biologic therapies in patients with PsA provide insight into their effectiveness in routine clinical practice. However, few real-world studies have been conducted on persistence and adherence of newer biologic therapies, particularly in the USA. The objective of this retrospective analysis of US administrative claims data was to assess 12-month discontinuation rates, persistence and adherence among patients with PsA who initiated secukinumab or a subcutaneous (sc.) TNFi.
Patients & methods
Study design & patient population
This retrospective cohort study was conducted using the Truven Analytics MarketScan® Commercial Claims and Encounters Database and the Medicare Supplemental Databases from 15 January 2015 to 31 July 2017. These databases contain information about cost, utilization and outcomes data for both inpatient and outpatient healthcare services provided for employees and their dependents covered under a variety of health plans, and the databases include all pharmacy fills with positive health plan payment or patient co-payment.
Patients with at least one outpatient pharmacy claim for a US FDA-approved sc. TNFi (adalimumab, certolizumab pegol, etanercept, golimumab) or an IL-17A inhibitor (secukinumab) for the treatment of PsA between 15 January 2016, and 31 July 2017, were identified in the Truven Health Analytics MarketScan Commercial and Medicare Supplemental Databases (Figure 1A). Eligible patients were aged ≥18 years at the time of biologic initiation (index date) and continuously enrolled with medical and pharmacy claims ≥12 months before the index date (baseline period from January 15, 2015) and ≥12 months after the index date (follow-up period through 31 July 2017). Patients had at least one PsA diagnosis (International Classification of Diseases, Ninth Revision, Clinical Modification [ICD-9-CM] 696.0 or ICD-10-CM L40.5x) and no pharmacy claims for the index biologic during the baseline period.

Figure 1. Study design.
(A) Schematic of study period; (B) Patient selection and attrition.
†Patients who have received one or more qualifying biologic by the index date will be placed into the index drug cohort of their first qualifying study biologic.
‡Defined as having no history of biologic use during the baseline period.
§Defined as having a history of biologic use during the baseline period.
PsA: Psoriatic arthritis.
All database records were de-identified and fully compliant with US patient confidentiality requirements, including the Health Insurance Portability and Accountability Act (HIPAA) of 1996. The databases have been evaluated and certified by an independent third party to satisfy the conditions set forth in Sections 164.514 (a)–(b)1ii of the HIPAA privacy rule regarding the determination and documentation of statistically de-identified data. Because the study used only de-identified patient records and did not involve the collection, use or transmittal of individually identifiable data, Institutional Review Board approval to conduct this study was not necessary.
Study variables & outcomes
Patients were assigned to mutually exclusive cohorts based on their index biologic. Patients who had received one or more qualifying biologic by the index date were placed into the index drug cohort of their first qualifying study biologic. Patient demographics (age, sex, geographic location and primary payer type) were assessed at the index date. Clinical characteristics measured during the baseline period included the history of psoriasis (based on ICD-9-CM diagnosis codes), the Deyo-Charlson Comorbidity Index (DCI) and binary (yes/no) flags for comorbidities relevant to patients with PsA based on previous studies and clinical expert opinion [24]. The DCI is an aggregate measure of comorbidity created using select diagnoses associated with chronic disease in the baseline period [25,26]; the DCI was based on both inpatient and outpatient diagnostic coding, using ICD-9-CM diagnosis and procedure codes. Comorbidities of interest included the following, based on ICD-9-CM diagnosis codes: major autoimmune disorders (Crohn disease, ulcerative colitis and irritable bowel disease), cardiovascular disease (hypertension, hyperlipidemia, coronary heart disease, cerebrovascular disease [stroke], peripheral vascular disease and carotid artery disease), malignancies, infectious diseases, diabetes, anxiety, depression, alcoholism, smoking and obesity. Prior use of medications during the 12-month baseline period was captured using National Drug Codes on pharmacy claims and procedure codes on outpatient claims. Medications included biologics (adalimumab, certolizumab pegol, etanercept, golimumab, infliximab, secukinumab and ustekinumab), systemic agents/conventional synthetic DAMARDs, oral corticosteroids, opioids, NSAIDS, targeted synthetic DMARDs (apremilast and tofacitinib) and topical agents. The number of unique biologics other than index medication was also captured during the 12-month baseline period.
Discontinuation rates with, persistence with, and adherence to the index biologic were evaluated descriptively during the 12-month follow-up period. Discontinuation was defined based on clinical expert opinion as no refill of the index biologic within 90 days after the previous days' supply was exhausted. Persistence was defined as the number of days from the index date to discontinuation of the index biologic (i.e., a treatment gap of ≥90 days) or to the end of follow-up if no gap was observed. Adherence was determined by the proportion of days covered (PDC), defined as the sum of the number of days in the follow-up period that the patient had the index biologic on hand divided by the total days in the follow-up period. Days with index medication on hand will be determined by the days' supply listed on pharmacy claims. For this analysis, patients with a PDC ≥0.80 during the follow-up period were considered adherent to their index biologic.
Data analysis
Primary analysis
For each index biologic cohort, descriptive analyses summarized patient demographics, clinical characteristics, comorbidity profile, treatment history and treatment patterns (i.e., discontinuation rates with, persistence with and adherence to index biologics). Categorical variables were summarized as the count and percentage of patients in each category. Continuous variables were summarized by means and standard deviations (SDs). The median time to discontinuation for each index biologic cohort during the 12-month follow-up period and the 95% CIs were assessed by Kaplan–Meier analysis. All analyses were performed using SAS 9.4 (Basic Edition).
Secondary analysis
All the primary analyses were also conducted in patients stratified by prior biologic use during the baseline period (i.e., biologic naive and biologic experienced) to determine whether treatment patterns were impacted by previous biologic experience.
Sensitivity analyses
Sensitivity analyses were performed using treatment gap cutoffs of ≥45 and ≥180 days as alternative definitions of discontinuation based on clinical expert opinion and previous studies of biologic treatment patterns. A 45-day gap has been used in previous studies based on the most common dosing regimen (≈30 days) plus 15 days to avoid misclassification of patients who briefly stopped treatment without discontinuation [27,28]. The 180-day gap is a conservative estimate chosen, based on expert opinion, to ensure that patients who stopped treatment did not restart treatment; it has been used in other studies of biologics in rheumatic and psoriatic disease [29–31].
Results
Of the 104,939 patients with PsA and one or more outpatient pharmacy claim for adalimumab, certolizumab pegol, etanercept, golimumab or secukinumab between 15 January 2016 and 31 July 2017, a total of 1558 were study eligible with ≥12 months of postindex follow-up time and were included in the analysis (Figure 1B). sc. biologic initiations included adalimumab (n = 720 [46.2%]), etanercept (n = 426 [27.3%]), certolizumab pegol (n = 93 [6.0%]), golimumab (n = 64 [4.1%]) and secukinumab (n = 255 [16.4%]). Of 1558 patients initiating sc. biologics, 1102 (70.7%) were biologic naive and 456 (29.3%) were biologic experienced.
Baseline characteristics
Demographics and clinical characteristics were similar across biologic treatment groups (Table 1). Overall, the mean age was approximately 50 years, and 56.0% (872/1558) of patients were female. The largest proportion of patients were in the southern region of the USA (47.9%, 744/1558), followed by the northeast (19.7%, 306/1558), the north central (19.3%, 300/1558) and the west (13.1%, 203/1558). Most patients (93.3% overall, 1454/1558) had commercial insurance. Overall, 66.9% (1042/1558) of patients across biologic groups had a history of psoriasis during the baseline period. The most common comorbidities across all biologic groups were hypertension (40.2%, 626/1558), hyperlipidemia (29.7%, 463/1558) and upper respiratory tract infections (25.9%, 403/1558). The proportion of biologic-experienced patients was highest among patients who initiated secukinumab (63.9%, 163/255), compared with that among patients initiating golimumab (56.3%, 36/64), certolizumab pegol (50.5%, 47/93), etanercept (23.0%, 98/426) and adalimumab (15.6%, 112/720).
| Characteristic | Index biologic | ||||
|---|---|---|---|---|---|
| ADA (n = 720) | CTZ (n = 93) | ETN (n = 426) | GOL (n = 64) | SEC (n = 255) | |
| Age, mean (SD), years | 48.6 (11.3) | 53.2 (12.1) | 49.7 (11.5) | 49.3 (10.0) | 51.0 (10.0) |
| Female, n (%) | 390 (54.2) | 68 (73.1) | 235 (55.2) | 45 (70.3) | 134 (52.5) |
| Geographic region, n (%) | |||||
| Northeast | 126 (17.5) | 17 (18.3) | 81 (19.0) | 18 (28.1) | 64 (25.1) |
| North central | 152 (21.1) | 12 (12.9) | 89 (20.9) | 5 (7.8) | 42 (16.5) |
| South | 347 (48.2) | 53 (57.0) | 191 (44.8) | 37 (57.8) | 116 (45.5) |
| West | 92 (12.8) | 9 (9.7) | 65 (15.3) | 4 (6.3) | 33 (12.9) |
| Primary payer, n (%) | |||||
| Commercial | 679 (94.3) | 78 (83.9) | 395 (92.7) | 62 (96.9) | 240 (94.1) |
| Medicare | 41 (5.7) | 15 (16.1) | 31 (7.3) | 2 (3.1) | 15 (5.9) |
| Length of follow-up, mean (SD), days | 461.0 (55.8) | 472.0 (52.0) | 463.8 (58.0) | 469.2 (52.2) | 447.0 (48.8) |
| History of psoriasis, n (%) | 494 (68.6) | 55 (59.1) | 269 (63.1) | 35 (54.7) | 189 (74.1) |
| Deyo–Charlson Comorbidity Index, mean (SD) | 0.6 (1.0) | 1.2 (1.5) | 0.8 (1.3) | 0.9 (1.1) | 1.0 (1.4) |
| Baseline comorbidities, n (%) | |||||
| Hypertension | 268 (37.2) | 49 (52.7) | 167 (39.2) | 22 (34.4) | 120 (47.1) |
| Hyperlipidemia | 208 (28.9) | 40 (43.0) | 121 (28.4) | 15 (23.4) | 79 (31.0) |
| Upper respiratory tract infection | 185 (25.7) | 33 (35.5) | 99 (23.2) | 21 (32.8) | 65 (25.5) |
| Obesity | 114 (15.8) | 20 (21.5) | 78 (18.3) | 13 (20.3) | 48 (18.8) |
| Diabetes | 117 (16.3) | 25 (26.9) | 65 (15.3) | 8 (12.5) | 52 (20.4) |
| Anxiety | 96 (13.3) | 15 (16.1) | 74 (17.4) | 10 (15.6) | 42 (16.5) |
| Depression | 93 (12.9) | 18 (19.4) | 71 (16.7) | 10 (15.6) | 38 (14.9) |
| Smoking | 47 (6.5) | 10 (10.8) | 28 (6.6) | 3 (4.7) | 17 (6.7) |
| Treatment history, n (%) | |||||
| NSAIDs | 387 (53.8) | 58 (62.4) | 230 (54.0) | 38 (59.4) | 131 (51.4) |
| – Opioids | 346 (48.1) | 63 (67.7) | 198 (46.5) | 40 (62.5) | 149 (58.4) |
| – Topical agents† | 663 (92.1) | 89 (95.7) | 378 (88.7) | 64 (100.0) | 244 (95.7) |
| Systemic agents/csDMARDs‡ | 504 (70.0) | 79 (84.9) | 307 (72.1) | 55 (85.9) | 171 (67.1) |
| tsDMARDs | 73 (10.1) | 19 (20.4) | 46 (10.8) | 13 (20.3) | 91 (35.7) |
| – Apremilast | 73 (10.1) | 18 (19.4) | 46 (10.8) | 11 (17.2) | 89 (34.9) |
| – Tofacitinib | 0 | 1 (1.1) | 0 | 2 (3.1) | 3 (1.2) |
| Biologics | 112 (15.6) | 47 (50.5) | 98 (23.0) | 36 (56.3) | 163 (63.9) |
| – Adalimumab | 0 | 21 (22.6) | 65 (15.3) | 10 (15.6) | 38 (14.9) |
| – Certolizumab pegol | 6 (0.8) | 0 | 5 (1.2) | 7 (10.9) | 10 (3.9) |
| – Etanercept | 66 (9.2) | 12 (12.9) | 0 | 12 (18.8) | 27 (10.6) |
| – Golimumab | 2 (0.3) | 3 (3.2) | 6 (1.4) | 0 | 14 (5.5) |
| – Infliximab | 17 (2.4) | 13 (14.0) | 16 (3.8) | 7 (10.9) | 28 (11.0) |
| – Secukinumab | 3 (0.4) | 0 | 3 (0.7) | 2 (3.1) | 0 |
| – Ustekinumab | 25 (3.5) | 9 (9.7) | 17 (4.0) | 9 (14.1) | 74 (29.0) |
| Number of unique biologics, mean (SD)§ | 0.2 (0.4) | 0.7 (0.8) | 0.3 (0.6) | 0.8 (0.8) | 0.8 (0.8) |
†Topical agents included coal tar, ketoconazole, salicylic acid, topical corticosteroids (alclometasone, amcinonide, betamethasone, clobetasol, desonide, desoximetasone, diflorasone, fluocinolone, flurandrenolide, fluticasone, halcinonide, halobetasol, hydrocortisone, pramoxine, prednicarbate and triamcinolone) and topical noncorticosteroids (anthralin, calcipotriene, calcitriol, pimecrolimus, tacrolimus and tazarotene).
‡Systemic agents/csDMARDs included acitretin, azathioprine, chloroquine/hydroxychloroquine, cyclosporine, hydroxyurea, isotretinoin, leflunomide, methotrexate, methoxsalen, mycophenolate mofetil, sulfasalazine, systemic corticosteroids (cortisone, dexamethasone, methylprednisolone, prednisolone, triamcinolone and hydrocortisone) and thioguanine.
§The number of unique biologic treatments excludes the index biologic treatment.
ADA: Adalimumab; csDMARD: Conventional synthetic disease-modifying antirheumatic drug; CTZ: Certolizumab pegol; ETN: Etanercept; GOL: Golimumab; SD: Standard deviation; SEC: Secukinumab; tsDMARD: Targeted synthetic disease-modifying antirheumatic drug.
Primary analysis: treatment gap ≥90 days
Overall, 680/1558 patients (43.6%) discontinued their index biologic therapy during 12-month follow-up when discontinuation was defined as a treatment gap ≥90 days. Patients who initiated secukinumab had the lowest 12-month discontinuation rate (36.5%, 93/255), followed by those initiating adalimumab (42.6%, 307/420), golimumab (45.3%, 29/64), etanercept (47.7%, 203/426) and certolizumab pegol (51.6%, 48/93) (Figure 2A). Persistence with the index biologic ranged from a mean (SD) of 240.7 (131.9) days (certolizumab pegol) to 282.8 (117.5) days (secukinumab). The median time to discontinuation could not be calculated in patients with treatment gaps ≥90 days due to low event rates and limited follow-up (Figure 2B).

Figure 2. Primary analysis: discontinuation with treatment gap ≥90 days.
(A) Discontinuation† rate and (B) time to discontinuation of index biologic during the 12-month follow-up period in patients with psoriatic arthritis who initiated a biologic using a treatment gap cutoff of ≥90 days (primary analysis).
†Discontinuation was defined as no refill of the index biologic within 90 days after the previous days' supply was exhausted.
‡Persistence was defined as the time from the first prescription fill of the index biologic to discontinuation of the index biologic (i.e., treatment gap ≥90 days), or the end of follow-up if no gap was observed.
The mean (SD) PDC with an index biologic was highest in patients who initiated secukinumab (0.67 [0.29]), compared with patients initiating adalimumab (0.65 [0.30]), etanercept (0.60 [0.31]), golimumab (0.59 [0.32]) and certolizumab pegol (0.49 [0.28]) (Figure 3). Overall, the proportion of patients adherent (PDC ≥0.80) to their index biologic across all biologics was 40.4% (629/1558). Adherence was highest with secukinumab (45.9%, 117/255), then adalimumab (43.5%, 313/720), golimumab (39.1%, 25/64), etanercept (36.9%, 157/426) and certolizumab pegol (18.3%, 17/93).
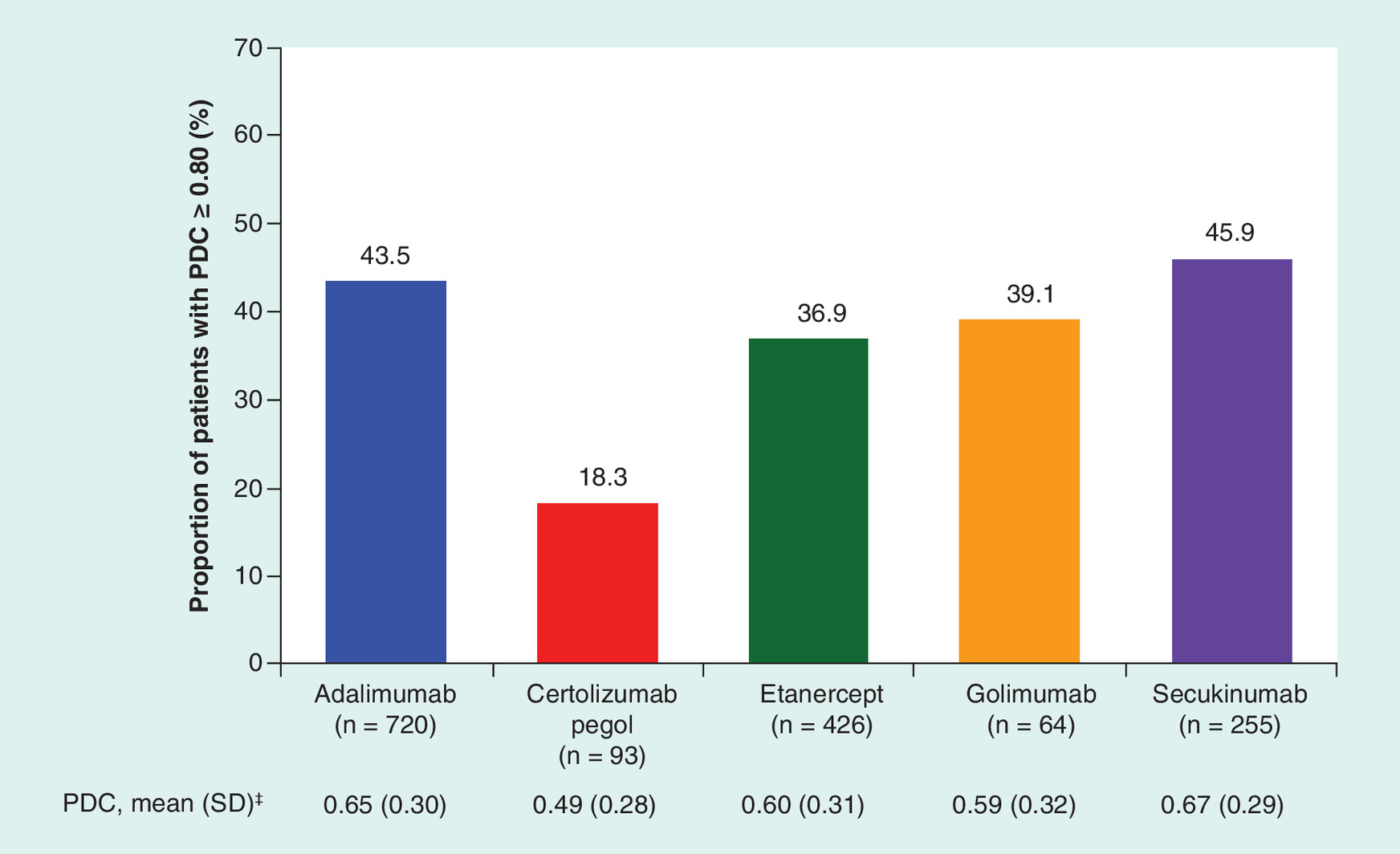
Figure 3. Adherence† to index biologic therapy during 12 months of follow-up among patients with psoriatic arthritis who initiated a biologic.
†Patients with a proportion of days covered ≥0.80 were considered adherent.
‡Proportion of days covered was defined as the sum of the number of days with the drug on hand divided by the number of days of follow-up.
PDC: Proportion of days covered.
Secondary analysis: biologic-naive & biologic-experienced cohorts
In the biologic-naive and biologic-experienced groups, respectively, the overall 12-month discontinuation rates across all biologics were 43.4% (478/1102) and 44.3% (202/456). Discontinuation rates were lowest, and persistence with index biologic was highest, with secukinumab versus other sc. biologics assessed (Figure 4). Biologic-naive patients who initiated secukinumab had the lowest 12-month discontinuation rate (32.6%, 30/92), followed by patients initiating golimumab (39.3%, 11/28), adalimumab (42.1%, 256/608), etanercept (47.6%, 156/328) and certolizumab pegol (54.3%, 25/46) (Figure 4A). Similarly, biologic-experienced patients who initiated secukinumab also had the lowest 12-month discontinuation rate (38.7%, 63/163), compared with patients initiating adalimumab (45.5%, 51/112), etanercept (48.0%, 47/98), certolizumab pegol (48.9%, 23/47) and golimumab (50.0%, 18/36) (Figure 4C). Persistence with the index biologic ranged from a mean (SD) of 228.2 (137.0) days with certolizumab pegol to 285.6 (122.8) days with secukinumab in biologic-naive patients (Figure 4A & B) and from 239.3 (138.2) days with golimumab to 281.3 (114.8) days with secukinumab in biologic-experienced patients (Figure 4C & D).
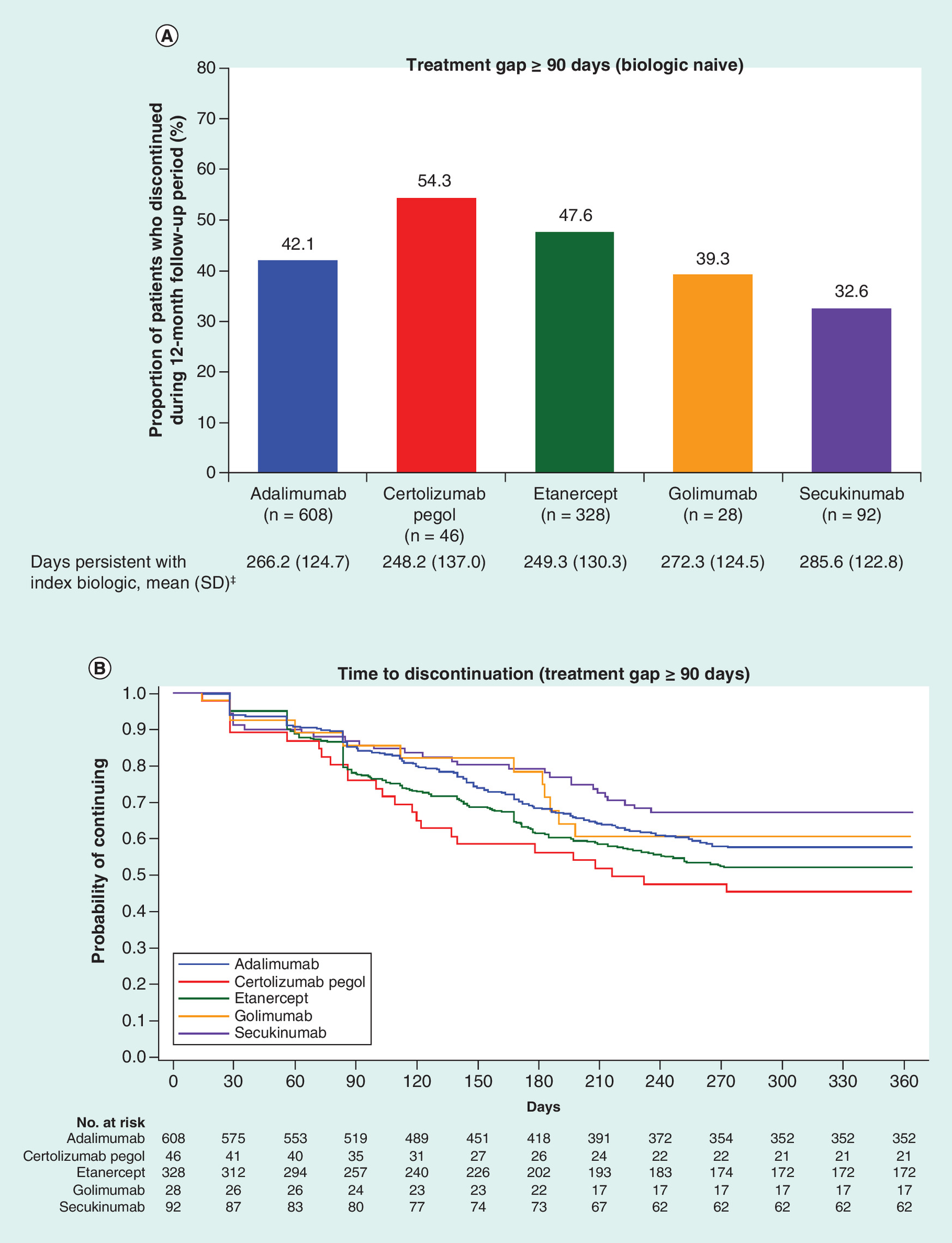
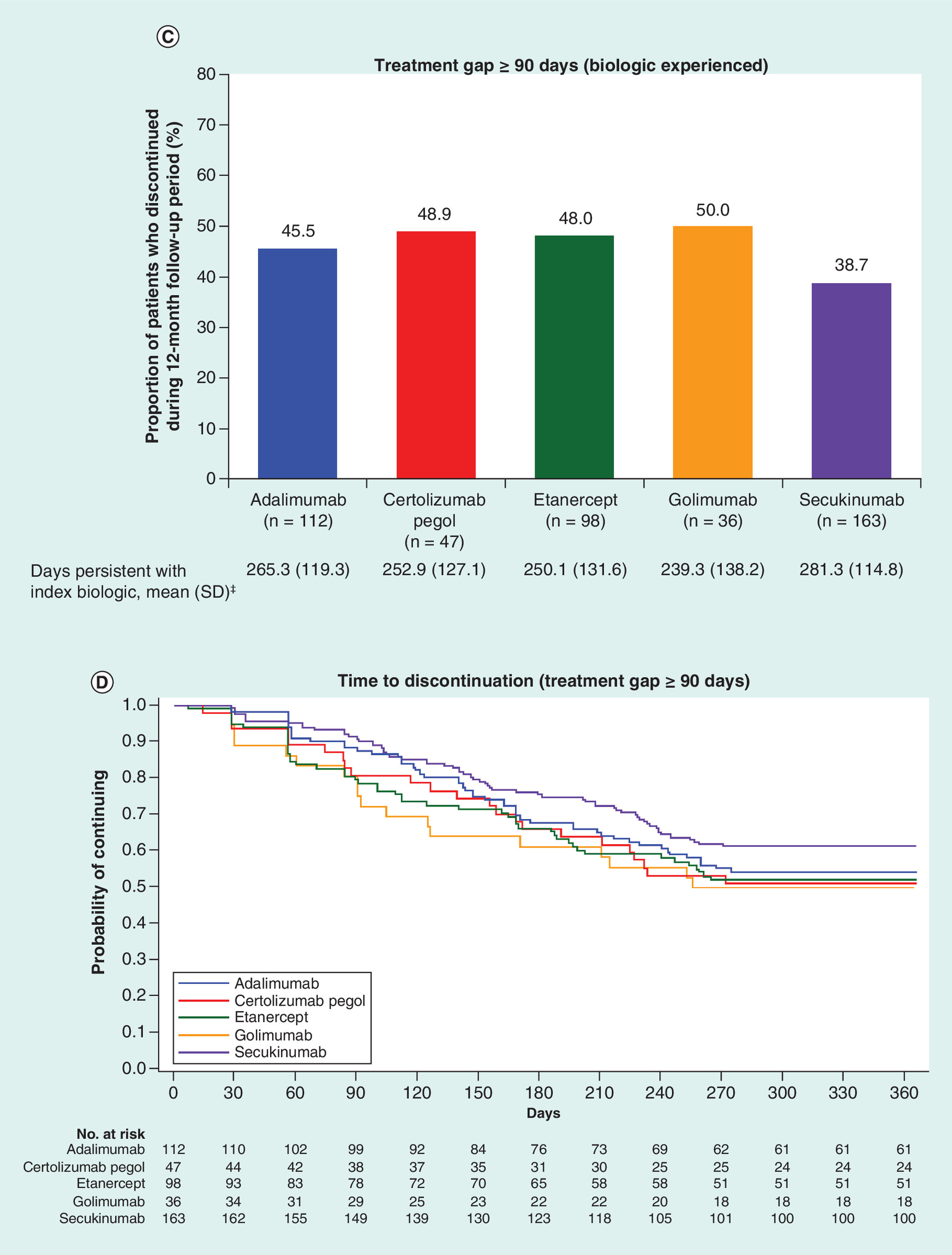
Figure 4. Discontinuation† rate and time to discontinuation of index biologic during the 12-month follow-up period.
(A & B) Biologic-naive and (C & D) biologic-experienced patients with psoriatic arthritis who initiated a biologic using a treatment gap cutoff of ≥90 days.
†Discontinuation was defined as no refill of the index biologic within 90 days after the previous days' supply was exhausted.
‡Persistence was defined as the time from the first prescription fill of the index biologic to discontinuation of the index biologic (i.e., treatment gap ≥90 days), or the end of follow-up if no gap was observed.
SD: Standard deviation.
The proportion of patients adherent (PDC ≥0.80) to their index biologic was 40.9% (451/1102) and 39.0% (178/456) in biologic-naive and -experienced groups, respectively. The proportion of adherent patients was lowest with certolizumab in both the biologic-naive (15.2%, 7/46; Figure 5A) and -experienced groups (21.3%, 10/47; Figure 5B). In both biologic-naive and -experienced patients, the mean (SD) PDC was highest with secukinumab (biologic naive: 0.69 [0.29]; biologic experienced: 0.66 [0.28]) and lowest with certolizumab pegol (biologic naive: 0.45 [0.27]; biologic experienced: 0.54 [0.29]). The proportion of biologic-naive patients who were adherent (PDC ≥0.80) to their index therapy was highest with secukinumab (53.3%, 49/92), while the proportion of biologic-experienced patients who were adherent to their index therapy was highest with adalimumab (44.6%, 50/112).

Figure 5. Adherence† to index biologic therapy during 12 months of follow-up.
(A) Biologic-naive and (B) biologic-experienced patients with psoriatic arthritis who initiated a biologic.
†Patients with a proportion of days covered ≥0.80 were considered adherent.
‡Proportion of days covered was defined as the sum of the number of days with the drug on hand divided by the number of days of follow-up.
PDC: Proportion of days covered.
Sensitivity analysis: treatment gaps ≥45 & ≥180 days
When discontinuation was defined using a shorter permissible treatment gap (≥45 days), the overall rate of discontinuation across all sc. biologics was 56.5% (881/1558), ranging from 51.8% (132/255; secukinumab) to 65.6% (61/93; certolizumab pegol). Patients initiating secukinumab had the highest mean (SD) persistence on index therapy (254.5 [123.8] days), while patients initiating certolizumab pegol had the lowest persistence (218.1 [127.1] days) (Supplementary Figure 1A). The median (95% CI) time to discontinuation was highest with secukinumab (308 [238 to >365] days) and lowest with certolizumab pegol (216 [155–274] days) (Supplementary Figure 1B). When discontinuation was defined using a longer permissible treatment gap (≥180 days), the overall rate of discontinuation decreased to 29.8% (464/1558), ranging from 21.6% (55/255; secukinumab) to 34.7% (148/426; etanercept). Patients initiating secukinumab had the highest mean (SD) persistence on index therapy (307.5 [112.2] days), while patients initiating etanercept, certolizumab pegol and golimumab, respectively, were comparable in having lowest persistence (270.7 [132.5] days, 272.1 [131.8] days and 273.0 [135.7] days) (Supplementary Figure 1C). The median time to discontinuation could not be estimated (Supplementary Figure 1D).
Discussion
In this retrospective analysis of US administrative claims data, patients who initiated secukinumab demonstrated lower discontinuation rates, higher persistence and greater adherence than patients initiating the other sc. biologics assessed, providing novel insight into patient outcomes with sc. biologic treatments. Overall, 43.6% of patients discontinued their index biologic therapy (≥90-day treatment gap) and 40.5% of patients remained adherent to their index biologic therapy (PDC ≥0.80) during 12-month follow-up. Patients who initiated secukinumab had the lowest 12-month discontinuation rate (36.5%) and highest mean (SD) number of days persistent on therapy (282.8 [117.5] days), while those initiating certolizumab pegol had the highest discontinuation rate (51.6%) and lowest mean (SD) number of days persistent on therapy (240.7 [131.9] days). Similar trends were observed in the sensitivity analyses when shorter (≥45 days) or longer (≥180 days) gaps in treatment were used as definitions for discontinuation. When stratified by prior biologic experience, discontinuation rates and the proportion of patients adherent to their index biologic among the biologic-naive and -experienced groups remained consistent with those of the overall population, with only minor differences between subgroups. Although the proportion of biologic-naive patients who were adherent (PDC ≥0.80) to their index therapy was highest with secukinumab, the proportion of biologic-experienced patients, who were adherent to their index therapy, was highest with adalimumab. For both groups, the proportion of adherent patients was lowest with certolizumab pegol.
Patient demographics and treatment histories were mostly similar across treatment groups; however, some characteristics could potentially explain differences in persistence and adherence. Notably, patients who initiated secukinumab were more likely to be biologic experienced at baseline (63.9%) and to have received a higher number of prior biologics than patients who initiated sc. TNFis, suggesting that secukinumab initiators may have more severe disease. This is not surprising because TNFis that have been available longer have traditionally been used as first-line biologic therapy due to lack of other agents with different MOAs, with an established safety and efficacy profile [32]. Because secukinumab demonstrated higher persistence and greater adherence than other sc. TNFis, guidance on treatment decisions may need to be re-examined for recommended first-line biologics. Although claims databases allowed only for limited assessment of disease activity, other studies have shown differences in disease severity between biologic-naive and -experienced patients [33]. There is evidence that switching biologics may be an effective strategy for some patients with PsA, but responses may be better for those patients who switch to a therapy with a different MOA [22,23]. Unlike many biologic-experienced TNFi initiators, who previously cycled between agents within the same class, all biologic-experienced patients who initiated secukinumab were switching to a therapy with a new MOA at baseline, which may have contributed to better overall persistence and adherence. As the biologic landscape in PsA continues to expand, additional analyses are needed to understand differences in treatment patterns and patient profiles in studies that include other newly approved biologic therapies.
There have been few studies in the USA that have used a ≥90-day gap to define discontinuation. Compared with our study, descriptive analyses from the Optum administrative claims database showed lower 12-month persistence rates with adalimumab (42.6 vs 57.6%), certolizumab pegol (32.0 vs 48.4%), etanercept (40.2 vs 52.3%) and golimumab (51.0 vs 54.7%) [34]. Differences between patient populations (i.e., higher prior biologic use and lower comorbidity burden in our study) may have contributed to differences in persistence. Other US claims-based studies of patients with PsA who initiated sc. biologics have used shorter treatment gaps (>45 or >60 days) to define discontinuation [27,35–39]. Although not every study examined individual biologics or used the same treatment gaps, complicating cross-study comparisons, the overall rate of discontinuation in our study using a >45-day gap (56.5%) was comparable to ranges of rates of nonpersistence (adalimumab, range: 41–63%; etanercept, 42–61%; biologics, 46–51%) observed in these studies. Unlike previous real-world studies that have shown shorter persistence with subsequent lines of biologic therapy in patients with PsA, in our study discontinuation rates and time to discontinuation were similar between biologic-naive and -experienced patients (43.4 and 44.3%, respectively), but additional adjusted analyses are needed to better understand factors associated with persistence [33,40]. The mean PDC with adalimumab (0.65), certolizumab pegol (0.49), etanercept (0.60) and golimumab (0.59) in our study was slightly lower than those previously reported among patients with PsA from the same database at 12-months of follow-up (mean PDC = 0.8 for adalimumab, etanercept and golimumab) [41], and comparable to analysis of another administrative claims database (adalimumab [0.56], certolizumab pegol [0.51], etanercept [0.57] and golimumab [0.61]) [34]. The overall proportion of patients adherent (PDC ≥0.8) to their index therapy is also similar to what was previously observed during the first year of therapy in patients with PsA, ankylosing spondylitis or rheumatoid arthritis who initiated an sc. TNFi (37%) [42]. These previous studies focused only on TNFis, whereas our study is among the first to include secukinumab, providing rheumatologists with valuable information about treatment patterns with a newer biologic in clinical practice.
These findings should be interpreted in context of the study's limitations, many of which are relevant to all studies involving administrative claims data. This was a retrospective analysis of US patients with mostly (>90%) commercial health coverage, with approximately 50% of patients located in the southern USA; therefore, the findings from this study may not be generalizable to all regions of the USA or other types of insurance coverage (i.e., Medicaid, Medicare or no insurance). Because the US healthcare system is different from other regions of the world, with a reimbursement structure potentially affecting treatment decisions, these data would not be generalizable outside of the USA. The sample sizes for some treatment groups were small, and the observed treatment patterns of the biologic therapies in this analysis were limited to the 12-month study period. Furthermore, patients who had a pharmacy claim for either secukinumab 300 or 150 mg were pooled together for this analysis. Longer-term studies with larger sample sizes that include newer biologics are needed. We did not capture reasons for treatment discontinuation nor clinical outcomes associated with treatment patterns – a general limitation of any claims-based study – but it is possible that some patients may have discontinued or de-escalated therapy because they were doing well on their index biologic. Additional analyses are needed to assess the long-term clinical impact of early discontinuation of and/or nonadherence to index therapy. Adjusted analyses to examine baseline predictors of early discontinuation and/or nonadherence, including potential pharmacogenetic factors that may impact response to treatment [43], would inform decision making for patients who may require more careful management of their disease. In addition, evidence of the prescription fill does not ensure actual use of the biologic therapy, potentially leading to further overestimation of persistence and/or adherence. The choice of biologic therapy and overall utilization rates may differ based on the formulary of each payer or employer group.
Conclusion
In this retrospective analysis of US administrative claims data, although patients who initiated secukinumab overall were most likely to be biologic experienced, they had lower discontinuation rates, higher persistence and greater adherence to their treatment over 12 months of follow-up than patients receiving the other sc. TNFis assessed. These findings address an unmet need by providing rheumatologists with insights about patients who initiate secukinumab and sc. TNFis in clinical settings.
Future perspective
While this study focused on secukinumab and currently approved sc. TNFis, there will be additional real-world data on treatment patterns of newer biologic therapies, including additional anti-IL-17A agents. Studies that provide updated information on characteristics and treatment patterns of patients treated with currently approved biologic therapies will be useful for payers and formulary decision makers. Additional studies should be regularly conducted as new biologics are approved to assess the long-term clinical and economic impact of early discontinuation of and/or nonadherence to existing treatments. Last, analyses that investigate reasons for discontinuation or switch of biologic treatment, as well as patient characteristics associated with nonpersistence, will help inform the shared decision-making process between rheumatologists and patients when choosing a new treatment.
Biologic treatments are available for patients with psoriatic arthritis (PsA), including TNF inhibitors (TNFis), as well as the newly approved IL-12/23 inhibitor ustekinumab, the IL-17A inhibitors ixekizumab and secukinumab, and the selective T-cell costimulatory modulator abatacept.
There is an unmet need to characterize persistence with and adherence to newer biologics with different mechanisms of action in clinical practice, particularly in the USA, because high rates of discontinuation or switching and/or lower rates of adherence may suggest suboptimal treatment.
The objective of this retrospective analysis of US administrative claims data was to assess 12-month discontinuation rates, persistence and adherence among patients with PsA who initiated secukinumab or a subcutaneous (sc.) TNFi (adalimumab, certolizumab pegol, etanercept or golimumab).
This US-based retrospective study used pharmacy claims data from 15 January 2016 to 31 July 31 2017, from the Truven Health Analytics MarketScan Commercial and Medicare Supplemental Databases.
Of 1558 patients with PsA included in the analysis, sc. biologic initiations included adalimumab (n = 720 [46.2%]) etanercept (n = 426 [27.3%]), certolizumab pegol (n = 93 [6.0%]), golimumab (n = 64 [4.1%]) and secukinumab (n = 255 [16.4%]); 1102 patients (70.7%) were biologic naive and 456 (29.3%) were biologic experienced.
Overall, 43.6% of patients discontinued their index biologic therapy (≥90-day treatment gap); discontinuation was lowest with secukinumab (36.5%), followed by adalimumab (42.6%), golimumab (45.3%), etanercept (47.7%) and certolizumab pegol (51.6%).
Persistence with the index biologic ranged from a mean of 240.7 days (certolizumab pegol) to 282.8 days (secukinumab).
Overall, 40.5% of patients remained adherent to their index biologic therapy (proportion of days covered ≥0.80) during 12-month follow-up; both the proportion of days covered and the percentage of patients who remained adherent were highest with secukinumab (0.67; 46%) and lowest with certolizumab pegol (0.49; 18%).
In this descriptive analysis, patients who initiated secukinumab were more likely to be biologic experienced and had a lower discontinuation rate, higher persistence and greater adherence over 12 months than those initiating the sc. TNFis assessed.
Supplementary data
To view the supplementary data that accompany this paper please visit the journal website at: www.futuremedicine.com/doi/full/10.2217/cer-2019-0023
Author contributions
All authors made substantial contributions to the conception or design of the work; or the acquisition, analysis or interpretation of data for the work; were involved in drafting the work or revising it critically for important intellectual content; provided final approval of the version to be published; and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Financial & competing interests disclosure
This study was sponsored by Novartis Pharmaceuticals Corporation, East Hanover, NJ, USA. KR Oelke has received speakers bureau fees from AbbVie, Amgen, Bristol-Meyers Squibb and Pfizer, and has received consulting fees from Novartis. O Chambenoit and P Hur are employees of Novartis. AQ Majjhoo has worked as an investigator, consultant and promotional speaker for Novartis. S Gray and K Higgins are employees of Truven Health Analytics. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Support for third-party writing assistance for this manuscript, furnished by E Deutsch, PhD, CMPP, of Health Interactions, Inc., was provided by Novartis Pharmaceuticals Corporation, East Hanover, NJ, USA.
Ethical conduct of research
All database records were de-identified and fully compliant with US patient confidentiality requirements, including the Health Insurance Portability and Accountability Act (HIPAA) of 1996. The databases have been evaluated and certified by an independent third party to satisfy the conditions set forth in Sections 164.514 (a)-(b)1ii of the HIPAA privacy rule regarding the determination and documentation of statistically de-identified data. Because the study used only de-identified patient records and did not involve the collection, use or transmittal of individually identifiable data, Institutional Review Board approval to conduct this study was not necessary.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
Supplementary Material
File (supplmaterial.docx)
- Download
- 307.65 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest.
1.
Mease PJ, Gladman DD, Papp KA et al. Prevalence of rheumatologist-diagnosed psoriatic arthritis in patients with psoriasis in European/North American dermatology clinics. J. Am. Acad. Dermatol. 69(5), 729–735 (2013).
2.
Ogdie A, Weiss P. The epidemiology of psoriatic arthritis. Rheum. Dis. Clin. North. Am. 41(4), 545–568 (2015).
3.
Gladman DD. Clinical features and diagnostic considerations in psoriatic arthritis. Rheum. Dis. Clin. North. Am. 41(4), 569–579 (2015).
4.
Gottlieb A, Korman NJ, Gordon KB et al. Guidelines of care for the management of psoriasis and psoriatic arthritis: section 2. Psoriatic arthritis: overview and guidelines of care for treatment with an emphasis on the biologics. J. Am. Acad. Dermatol. 58(5), 851–864 (2008).
5.
Coates LC, Kavanaugh A, Mease PJ et al. Group for Research and Assessment of Psoriasis and Psoriatic Arthritis 2015 treatment recommendations for psoriatic arthritis. Arthritis Rheumatol. 68(5), 1060–1071 (2016).
6.
Gossec L, Smolen JS, Ramiro S et al. European League Against Rheumatism (EULAR) recommendations for the management of psoriatic arthritis with pharmacological therapies: 2015 update. Ann. Rheum. Dis. 75(3), 499–510 (2016).
7.
Mease PJ, Gladman DD, Ritchlin CT et al. Adalimumab for the treatment of patients with moderately to severely active psoriatic arthritis: results of a double-blind, randomized, placebo-controlled trial. Arthritis Rheum. 52(10), 3279–3289 (2005).
8.
Mease PJ, Fleischmann R, Deodhar AA et al. Effect of certolizumab pegol on signs and symptoms in patients with psoriatic arthritis: 24-week results of a Phase III double-blind randomised placebo-controlled study (RAPID-PsA). Ann. Rheum. Dis. 73(1), 48–55 (2014).
9.
Mease PJ, Kivitz AJ, Burch FX et al. Etanercept treatment of psoriatic arthritis: safety, efficacy, and effect on disease progression. Arthritis Rheum. 50(7), 2264–2272 (2004).
10.
Kavanaugh A, McInnes I, Mease P et al. Golimumab, a new human tumor necrosis factor alpha antibody, administered every four weeks as a subcutaneous injection in psoriatic arthritis: twenty-four-week efficacy and safety results of a randomized, placebo-controlled study. Arthritis Rheum. 60(4), 976–986 (2009).
11.
Kavanaugh A, Husni ME, Harrison DD et al. Safety and efficacy of intravenous golimumab in patients with active psoriatic arthritis: results through week twenty-four of the GO-VIBRANT study. Arthritis Rheumatol. 69(11), 2151–2161 (2017).
12.
Antoni C, Krueger GG, de Vlam K et al. Infliximab improves signs and symptoms of psoriatic arthritis: results of the IMPACT 2 trial. Ann. Rheum. Dis. 64(8), 1150–1157 (2005).
13.
McInnes IB, Kavanaugh A, Gottlieb AB et al. Efficacy and safety of ustekinumab in patients with active psoriatic arthritis: 1 year results of the Phase III, multicentre, double-blind, placebo-controlled PSUMMIT 1 trial. Lancet 382(9894), 780–789 (2013).
14.
Ritchlin C, Rahman P, Kavanaugh A et al. Efficacy and safety of the anti-IL-12/23 p40 monoclonal antibody, ustekinumab, in patients with active psoriatic arthritis despite conventional non-biological and biological anti-tumour necrosis factor therapy: 6-month and 1-year results of the Phase 3, multicentre, double-blind, placebo-controlled, randomised PSUMMIT 2 trial. Ann. Rheum. Dis. 73(6), 990–999 (2014).
15.
Mease PJ, van der Heijde D, Ritchlin CT et al. Ixekizumab, an interleukin-17A specific monoclonal antibody, for the treatment of biologic-naive patients with active psoriatic arthritis: results from the 24-week randomised, double-blind, placebo-controlled and active (adalimumab)-controlled period of the Phase III trial SPIRIT-P1. Ann. Rheum. Dis. 76(1), 79–87 (2017).
16.
Nash P, Kirkham B, Okada M et al. Ixekizumab for the treatment of patients with active psoriatic arthritis and an inadequate response to tumour necrosis factor inhibitors: results from the 24-week randomised, double-blind, placebo-controlled period of the SPIRIT-P2 Phase 3 trial. Lancet 389(10086), 2317–2327 (2017).
17.
McInnes IB, Mease PJ, Kirkham B et al. Secukinumab, a human anti-interleukin-17A monoclonal antibody, in patients with psoriatic arthritis (FUTURE 2): a randomised, double-blind, placebo-controlled, Phase 3 trial. Lancet 386(9999), 1137–1146 (2015).
18.
Mease PJ, McInnes IB, Kirkham B et al. Secukinumab inhibition of interleukin-17A in patients with psoriatic arthritis. N. Engl. J. Med. 373(14), 1329–1339 (2015).
19.
Mease P, Genovese MC, Gladstein G et al. Abatacept in the treatment of patients with psoriatic arthritis: results of a six-month, multicenter, randomized, double-blind, placebo-controlled, Phase II trial. Arthritis Rheum. 63(4), 939–948 (2011).
20.
Mease PJ, Gottlieb AB, van der Heijde D et al. Efficacy and safety of abatacept, a T-cell modulator, in a randomised, double-blind, placebo-controlled, Phase III study in psoriatic arthritis. Ann. Rheum. Dis. 76(9), 1550–1558 (2017).
21.
Coates LC, Moverley AR, McParland L et al. Effect of tight control of inflammation in early psoriatic arthritis (TICOPA): a UK multicentre, open-label, randomised controlled trial. Lancet 386(10012), 2489–2498 (2015).
•• Tight control of disease activity using a treat-to-target approach in patients with early psoriatic arthritis significantly improved joint and skin outcomes.
22.
Reddy SM, Crean S, Martin AL, Burns MD, Palmer JB. Real-world effectiveness of anti-TNF switching in psoriatic arthritis: a systematic review of the literature. Clin. Rheumatol. 35(12), 2955–2966 (2016).
• A first-line TNF inhibitor (TNFi) had better outcomes compared with a subsequent TNFi, and significant differences were observed between second- and third-line TNFi.
23.
Merola JF, Lockshin B, Mody EA. Switching biologics in the treatment of psoriatic arthritis. Semin. Arthritis Rheum. 47(1), 29–37 (2017).
24.
Kaine J, Song X, Kim G, Hur P, Palmer JB. Higher incidence rates of comorbidities in patients with psoriatic arthritis compared with the general population using U.S. administrative claims data. J. Manag. Care Spec. Pharm. 25(1), 122–132 (2019).
25.
Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J. Chronic Dis. 40(5), 373–383 (1987).
26.
Deyo RA, Cherkin DC, Ciol MA. Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J. Clin. Epidemiol. 45(6), 613–619 (1992).
27.
Howe A, Eyck LT, Dufour R, Shah N, Harrison DJ. Treatment patterns and annual drug costs of biologic therapies across indications from the Humana commercial database. J. Manag. Care Spec. Pharm. 20(12), 1236–1244 (2014).
• Adalimumab, etanercept and infliximab were commonly used for the treatment of rheumatoid arthritis, psoriasis, psoriatic arthritis and ankylosing spondylitis; patients newly initiating treatment were less persistent than those continuing therapy.
28.
Gu T, Shah N, Deshpande G, Tang DH, Eisenberg DF. Comparing biologic cost per treated patient across indications among adult US managed care patients: a retrospective cohort study. Drugs Real World Outcomes 3(4), 369–381 (2016).
29.
Schwartzman S, Li Y, Zhou H, Herrera V, Palmer JB. Treatment patterns of subcutaneous biologic agent use among patients with ankylosing spondylitis [abstract]. Arthritis Rheumatol. 67(Suppl. 10), A2861 (2015).
30.
Harnett J, Wiederkehr D, Gerber R, Gruben D, Koenig A, Bourret J. Real-world evaluation of TNF-inhibitor utilization in rheumatoid arthritis. J. Med. Econ. 19(2), 91–102 (2016).
31.
Pogacsas L, Borsi A, Takacs P et al. Long-term drug survival and predictor analysis of the whole psoriatic patient population on biological therapy in Hungary. J. Dermatolog. Treat. 28(7), 635–641 (2017).
32.
Murdaca G, Colombo BM, Cagnati P, Gulli R, Spano F, Puppo F. Update upon efficacy and safety of TNF-α inhibitors. Expert. Opin. Drug Saf. 11(1), 1–5 (2012).
33.
Harrold LR, Stolshek BS, Rebello S et al. Impact of prior biologic use on persistence of treatment in patients with psoriatic arthritis enrolled in the US Corrona registry. Clin. Rheumatol. 36(4), 895–901 (2017).
•• The majority of patients with psoriatic arthritis were persistent with TNFi therapy; more biologic-naive than -experienced patients remained persistent over 4 years of follow-up.
34.
Walsh JA, Adejoro O, Chastek B, Palmer JB, Hur P. Treatment patterns among patients with psoriatic arthritis treated with a biologic in the United States: descriptive analyses from an administrative claims database. J. Manag. Care Spec. Pharm. 24(7), 623–631 (2018).
• Most patients with psoriatic arthritis who newly initiated a TNFi or anti-IL-12/23 inhibitor discontinued before 12 months.
35.
Chastek B, Fox KM, Watson C, Gandra SR. Etanercept and adalimumab treatment patterns in psoriatic arthritis patients enrolled in a commercial health plan. Adv. Ther. 29(8), 691–697 (2012).
36.
Bonafede M, Johnson BH, Fox KM, Watson C, Gandra SR. Treatment patterns with etanercept and adalimumab for psoriatic diseases in a real-world setting. J. Dermatolog. Treat. 24(5), 369–373 (2013).
37.
Bonafede M, Fox KM, Watson C, Princic N, Gandra SR. Treatment patterns in the first year after initiating tumor necrosis factor blockers in real-world settings. Adv. Ther. 29(8), 664–674 (2012).
38.
Zhang HF, Gauthier G, Hiscock R, Curtis JR. Treatment patterns in psoriatic arthritis patients newly initiated on oral nonbiologic or biologic disease-modifying antirheumatic drugs. Arthritis Res. Ther. 16(4), 420 (2014).
39.
Zhu B, Edson-Heredia E, Gatz JL, Guo J, Shuler CL. Treatment patterns and health care costs for patients with psoriatic arthritis on biologic therapy: a retrospective cohort study. Clin. Ther. 35(9), 1376–1385 (2013).
40.
Palmer JB, Li Y, Herrera V, Liao M, Tran M, Ozturk ZE. Treatment patterns and costs for anti-TNFα biologic therapy in patients with psoriatic arthritis. BMC Musculoskelet. Disord. 17, 261 (2016).
41.
Schwartzman S, Li Y, Zhou H, Palmer JB. Economic impact of biologic utilization patterns in patients with psoriatic arthritis. Clin. Rheumatol. 36(7), 1579–1588 (2017).
• Above-label dosing of TNFis resulted in significantly higher healthcare costs per patient.
42.
Calip GS, Adimadhyam S, Xing S, Rincon JC, Lee WJ, Anguiano RH. Medication adherence and persistence over time with self-administered TNF-α inhibitors among young adult, middle-aged, and older patients with rheumatologic conditions. Semin. Arthritis. Rheum. 47(2), 157–164 (2017).
43.
Murdaca G, Gulli R, Spano F et al. TNF-α gene polymorphisms: association with disease susceptibility and response to anti-TNF-α treatment in psoriatic arthritis. J. Invest. Dermatol. 134(10), 2503–2509 (2014).
Information & Authors
Information
Published In
Copyright
© 2019 Novartis Pharmaceuticals Organisation.
History
Received: 7 February 2019
Accepted: 11 March 2019
Published online: 26 March 2019
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Persistence and adherence of biologics in US patients with psoriatic arthritis: analyses from a claims database. (2019) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2019-0023
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Stephanie R. Harrison, George E. Fragoulis, Xabier Michelena, Cristina Macía-Villa, Louise Falzon, Stefan Siebert, Helena Marzo-Ortega, Alexandre Sepriano, Pedro M. Machado, Prevalence, outcomes, and predictive factors: a systematic literature review to inform the development of EULAR Points to Consider for the definition of Difficult-to-Manage and Treatment-Refractory psoriatic arthritis, EULAR Rheumatology Open, 10.1016/j.ero.2025.07.007, 2, 2, (100043), (2026).
- Laure Gossec, William Tillett, Laura C. Coates, Philip J. Mease, Maarten de Wit, Dafna D. Gladman, Ana‐Maria Orbai, Fabian Proft, Barbara Ink, Rajan Bajracharya, Jérémy Lambert, Patrick Healy, M. Elaine Husni, Control of Inflammation and Sustained Improvements in Patient‐Reported Outcomes in Patients With Psoriatic Arthritis: Bimekizumab Two‐Year Results From Two Phase 3 Studies, ACR Open Rheumatology, 10.1002/acr2.90053, 8, 5, (2026).
- Simone Parisi, Andrea Becciolini, Bernardo D’Onofrio, Alberto Lo Gullo, Olga Addimanda, Mirco Magnani, Massimo Reta, Romina Andracco, Natalia Mansueto, Patrizia Del Medico, Rosalba Caccavale, Marino Paroli, Maddalena Larosa, Gerolamo Bianchi, Dario Camellino, Bernd Raffeiner, Valeria Nucera, Aurora Ianniello, Cecilia Giampietro, Francesca Ometto, Marta Priora, Aldo Biagio Molica Colella, Elena Bravi, Ilaria Platè, Eugenio Arrigoni, Viviana Ravagnani, Alessandra Bezzi, Fabio Mascella, Maria Cristina Focherini, Alessia Fiorenza, Guido Rovera, Rosetta Vitetta, Palma Scolieri, Vincenzo Bruzzese, Alessandro Volpe, Riccardo Bixio, Antonio Marchetta, Federica Lumetti, Antonella Farina, Simone Bernardi, Francesco Girelli, Elisa Visalli, Giorgio Amato, Francesco De Lucia, Ylenia Dal Bosco, Roberta Foti, Rosario Foti, Francesca Serale, Francesco Cipollone, Myriam Di Penta, Emanuela Sabatini, Eleonora Celletti, Veronica Franchina, Francesco Molica Colella, Giulio Ferrero, Gilda Sandri, Dilia Giuggioli, Maria Chiara Ditto, Enrico Fusaro, Giuditta Adorni, Eleonora Di Donato, Daniele Santilli, Gianluca Lucchini, Alarico Ariani, Drug retention of TNF versus IL-23 inhibitors in psoriatic arthritis: a multicenter real-life cohort study, Therapeutic Advances in Musculoskeletal Disease, 10.1177/1759720X261436837, 18, (2026).
- Laure Gossec, Laura C Coates, Robert B M Landewé, Philip J Mease, Joseph F Merola, Christopher T Ritchlin, Yoshiya Tanaka, Akihiko Asahina, Fabian Proft, Nadine Goldammer, Myriam Manente, Barbara Ink, Rajan Bajracharya, Jason Coarse, Iain B McInnes, Bimekizumab safety and efficacy in patients with psoriatic arthritis: 3-year results from two phase 3 studies, Rheumatology, 10.1093/rheumatology/keag118, (2026).
- Yizhang Liu, Kun Hu, Yongfang Duan, Junchen Chen, Panpan Liu, Shuangyuan Zhou, Mi Zhang, Yehong Kuang, What is the optimal sequential therapy after secondary IL-17A inhibitor failure in psoriasis: switching to an IL-23 inhibitor or to another IL-17A inhibitor?, Journal of Dermatological Treatment, 10.1080/09546634.2025.2588072, 36, 1, (2025).
- Alarico Ariani, Maddalena Larosa, Alberto Lo Gullo, Olga Addimanda, Romina Andracco, Patrizia Del Medico, Marino Paroli, Maria Chiara Ditto, Bernd Raffeiner, Aurora Ianniello, Francesca Ometto, Marta Priora, Aldo Biagio Molica Colella, Elena Bravi, Viviana Ravagnani, Alessandra Bezzi, Rosetta Vitetta, Palma Scolieri, Alessandro Volpe, Federica Lumetti, Antonella Farina, Francesco Girelli, Elisa Visalli, Francesca Serale, Eleonora Celletti, Veronica Franchina, Francesco Molica Colella, Giulio Ferrero, Fabio Mascella, Maria Cristina Focherini, Alessia Fiorenza, Guido Rovera, Cecilia Giampietro, Simone Bernardi, Natalia Mansueto, Dario Camellino, Rosalba Caccavale, Valeria Nucera, Myriam Di Penta, Emanuela Sabatini, Ilaria Platè, Adorni Giuditta, Eleonora Di Donato, Daniele Santilli, Gianluca Lucchini, Mirco Magnani, Gianluca Smerilli, Giorgio Amato, Francesco De Lucia, Ylenia Dal Bosco, Roberta Foti, Francesco Cipollone, Gerolamo Bianchi, Rosario Foti, Eugenio Arrigoni, Antonio Marchetta, Vincenzo Bruzzese, Gilda Sandri, Enrico Fusaro, Massimo Reta, Dilia Giuggioli, Antonio Marchesoni, Simone Parisi, Andrea Becciolini, Comparative effectiveness of cycling versus swapping to IL-17 inhibitors after first TNF inhibitor failure in Psoriatic Arthritis: A real-world multicenter study, BMC Rheumatology, 10.1186/s41927-025-00587-8, 9, 1, (2025).
- Joseph F. Merola, Sarah Welby, Helena Roque, Jie Song, Olga Pilipczuk, Chao Lu, Jessica A. Walsh, Real-world use of biologic and targeted synthetic disease-modifying antirheumatic drugs in US patients with psoriatic arthritis: Persistence, patient characteristics associated with discontinuation, and dosing patterns, Journal of Managed Care & Specialty Pharmacy, 10.18553/jmcp.2025.31.8.808, 31, 8, (808-821), (2025).
- Hideto Kameda, Kentaro Ishii, Junna Kiriyama, Toshiaki Mikami, Hideya Uratsuji, Akimichi Morita, Secukinumab Persistence in Patients with Psoriatic Arthritis: An Adalimumab-Matched Retrospective Cohort Database Study (FLYWAY), Rheumatology and Therapy, 10.1007/s40744-025-00749-7, 12, 3, (493-511), (2025).
- Philip J. Mease, Shannon A. Ferrante, Natalie J. Shiff, Timothy P. Fitzgerald, Soumya D. Chakravarty, Jessica A. Walsh, Comparison of On-Label Treatment Persistence in Real-World Patients with Psoriatic Arthritis Receiving Guselkumab Versus Subcutaneous Interleukin-17A Inhibitors, Advances in Therapy, 10.1007/s12325-024-03042-1, 42, 2, (734-751), (2024).
- Magdalena Jasmen, Dominga García, Sebastián Ibáñez, Pamela Díaz, The Persistence of Biologic Therapies for Psoriatic Arthritis, JCR: Journal of Clinical Rheumatology, 10.1097/RHU.0000000000002159, 31, 3, (107-116), (2024).
- See more