Ongoing initiatives within the Scottish National Health Service to affect the prescribing of selective serotonin reuptake inhibitors and their influence
Abstract
Aim: Increasing use of selective serotonin-reuptake inhibitors (SSRIs) in Scotland, coupled with safety concerns with some SSRIs, and the increasing availability of generic SSRIs, have resulted in multiple initiatives to improve the quality and efficiency of their prescribing in Scotland. Our aim is to assess their influence to provide future direction. Materials & methods: The prescription costs analysis database was used to document utilization and expenditure on SSRIs between 2001 and 2017 alongside documenting the initiatives. Results: Multiple interventions over the years increased international nonproprietary name prescribing up to 99.9% lowering overall costs. This, coupled with initiatives to limit escitalopram prescribing due to concerns with its value, resulted in a 73.7% reduction in SSRI expenditure between 2001 and 2017 despite a 2.34-fold increase in utilization. Safety warnings resulted in a significant reduction in the prescribing of paroxetine, citalopram and escitalopram alongside a significant increase in sertraline Conclusion: Multiple initiatives have increased the quality and efficiency of SSRI prescribing in Scotland providing direction to others.
Across countries, there has been considerable growth in the use of medicines. In part, this has been driven by aging populations, an increase in primary prevention strategies, as well as single disease model guidelines and policies [1,2]. We have also seen the continual launch of new high-priced medicines [2,3]. These factors combined are adding to resource pressures within countries resulting in models and initiatives to address this [2–5]. Scotland is no exception, and during the last 20 years or more there have been multiple initiatives to enhance the quality and efficiency of prescribing to help improve patient outcomes within finite resources, providing direction to other countries.
Initiatives include encouraging high rates of international nonproprietary name (INN) prescribing with generics typically seen as similar to the originator in all but a minority of situations [6–8]. This is important as there are still concerns with generics across a number of countries [9–11]. Savings once generics become available in Scotland are enhanced by their reduced costs, which can be as low as 3% of prepatent loss originator prices [12,13]. INN prescribing is important in Scotland as pharmacists are not currently allowed to switch an originator or branded product to a generic if the physician prescribes the originator or branded product [7,14,15]. Alongside this, there have also been initiatives to increase the prescribing of multiple sourced products (generics) versus on-patent products in a class or related class where this does not compromise care to further save on costs. Classes include the proton pump inhibitors (PPIs), renin–angiotensin receptor blockers and statins [12,13,15].
Concomitant with this, there have also been multiple measures in Scotland to improve the quality of prescribing. These include encouraging physicians to prescribe higher doses of statins to improve long-term outcomes as well as initiatives to reduce the prescribing of lipid-lowering agents where there have been concerns with their effectiveness [12,15]. There have also been national and regional initiatives in Scotland to reduce the doses of PPIs prescribed, as well as encourage regular monitoring of patients on long-term PPIs, due to concerns with the consequences of their long-term use [16–19].
Depression and other mental health conditions, such as anxiety disorders, are prevalent in Scotland with 11.3% of the adult population in 2010–2011 prescribed antidepressants [20]. These high rates of prescribing are possibly influenced by westernized societies’ expectations of happiness, and consequential medicalization of unhappiness [21,22], as well as expansion of the indications for antidepressants. The selective serotonin-reuptake inhibitors (SSRIs) are the most frequently prescribed antidepressants in Scotland, accounting for over 50% of all antidepressants prescribed in recent years [20,23,24]. However, unlike the PPIs, renin–angiotensin blockers and statins, the situation with antidepressants is more challenging as they are not readily interchangeable, which limits the potential for therapeutic switching within a class [12,13,15,25,26]. This is because antidepressants such as the SSRIs exhibit subtle differences, which can affect both their efficacy and side effects [27–29]. Having said this, there have been activities among the Health Boards (regions) in Scotland to limit the prescribing of escitalopram versus other SSRIs, including fluoxetine and citalopram, where there have been considerable differences in costs but limited differences in patient outcomes [17,30–32]. Health Board activities included prescribing targets for escitalopram [33]. They also include switching suitable patients prescribed escitalopram prior to citalopram to now being prescribed citalopram (C Johnson, P.C.). Encouragingly, 90% of patients remained on citalopram after the switch at a 3-month review. Such activities are important from a health policy perspective as they help to conserve resources without compromising care.
We have also seen initiatives in other countries to influence the prescribing of antidepressants where there have been concerns. This includes instigating prescribing restrictions for duloxetine in the management of patients with depression in Sweden due to concerns with its effectiveness and costs versus other antidepressants [34], as well as education and other activities to limit the prescribing of vortioxetine again due to concerns with its cost–effectiveness [35,36]. Such activities are likely to continue.
We are also aware that there have been concerns with the increased risk of suicides with paroxetine as well as other SSRIs since the early 2000s [37–42]. In addition, paroxetine is associated with a higher incidence of discontinuation symptoms versus other SSRIs, which necessitates a longer period of dose reduction [43]. There have also been concerns with potential QTc interval prolongation and Torsade de Pointes with citalopram and escitalopram from 2011 onward [44], although the latter may be infrequently reported [45]. The concerns with possible QTc interval prolongation with citalopram and escitalopram resulted in the MHRA in the UK and Health Boards in Scotland providing guidance on their use [46–69]. This included recommending alternative SSRIs for new patients, as well as for patients where there were concerns with citalopram and escitalopram. Alternatives included sertraline with evidence of potential improved effectiveness and safety versus other SSRIs [48,50,51]. We are also aware that Health Boards in Scotland have also assessed factors associated with higher doses of SSRIs being prescribed [20,52]. Available evidence does not support the routine prescribing of higher doses of SSRIs for the treatment of depression as this is known to increase anxiety, agitation and insomnia [53].
As a result of multiple activities in Scotland, rates of INN prescribing for the SSRIs were as high as 98–99% of their total utilization in 2007 [13]. This coupled with initiatives to limit the prescribing of escitalopram versus citalopram resulted in expenditure on the SSRIs falling in Scotland by 59% between 2001 and 2007 despite a 2.37-fold increase in their utilization [13]. This compares with appreciably increased expenditure for the SSRIs in Ireland (72% higher) and Portugal (93% higher) in 2008 and 2007 versus 2001 respectively where there were limited measures in both these countries to encourage the prescribing of lower cost multiple sourced SSRIs (generics) versus originators as well as on-patent escitalopram [13,54]. Such activities are important among high income countries with universal healthcare systems due to the continuous growth in the prescribing of medicines for patients with noncommunicable diseases including patients with depression resulting in constant financial pressures, which is enhanced by the continual launch of new premium priced medicines to address areas of unmet need [2,4,6,54-56]. Obtaining low prices for good quality generics, and promoting their use, is also very important in low and middle income countries where access to medicines can be an issue with high patient copayment levels [57,58]. Without such considerations, illness among family members can be potentially catastrophic for them [58,59]. Currently, fluoxetine is included in the WHO list of essential medicines [60].
Consequently, the objectives of this paper are multiple. First, to assess the influence of the various multiple measures in Scotland on the overall volume and expenditure on the SSRIs in recent years, building on the earlier analysis [13]. Second, assess the extent of INN prescribing as well as the extent of price reductions for SSRIs following generic availability to help fund increased prescribing volumes without increasing costs, again building on the earlier analysis [13]. Third, assess the extent of changes in the utilization of citalopram, escitalopram, paroxetine and sertraline in recent years as a result of multiple initiatives and safety warnings. The findings will help guide future activities in Scotland as well as other countries, as all countries are looking to improve the quality and efficiency of their prescribing due to continuing pressures on resources.
We are also aware that there is a growing requirement for research evidence to guide future activities and initiatives to improve the selection, affordability and rationality of prescribing of medicines for patients with mental disorders, which can be considered as public health psychopharmacology [61]. We hope our findings help to start addressing this deficit.
Methodology
Utilization & expenditure data
We used the prescription costs analysis (PCA) data in Scotland to analyze utilization and expenditure data in ambulatory care [62]. The PCA data is compiled by the Information Services Division of NHS Scotland, which is an open source dataset collecting data on the utilization and expenditure of medicines dispensed in community pharmacies in Scotland. The NHS in Scotland is a tax payer funded, free at point of access, health service, with currently no copayment for medicines.
Information extracted from the PCA for each SSRI (N06AB – [63]) between 2001 and 2017 included: their generic name, commercial name(s), formulation(s), drug strength(s), number of dispensed units, cost per unit and total expenditure. The costs are in pounds sterling (GB£s) and include the gross ingredient costs and cost per item for all SSRIs medicines dispensed during this period. No adjustment for inflation for prices was made, which is in line with previous studies, typically due to the rapid reduction in prices in the UK once originators become available as generics [12,13,64].
While we are aware NHS Scotland routinely uses defined daily doses (DDDs) when presenting and discussing utilization data in line with international guidance [23,63,65], especially when different strengths are available such as citalopram (10, 20 and 40 mg) and sertraline (50 and 100 mg), we used items dispensed as we wanted to track this to reflect individual prescriptions, especially following changes in prescribing guidance, similar to the situation with lipid-lowering agents and PPIs [15,19]. In the case of patients with chronic diseases such as depression, a prescription in terms of ‘items dispensed’ is usually for 28 or 56 days. However, as previously identified, there can be a tendency in recent years for physicians to increase the length of a prescription to help with their growing workloads [15].
Demand-side measures
As before, ongoing activities within the Health Boards and NHS Scotland to encourage INN prescribing as well as selected SSRIs have been collated using the 4E methodology: Education, Engineering, Economics and Enforcement [12,13,15,66]. Education refers to initiatives such as prescribing guidance and guidelines; engineering refers to organizational or managerial interventions such as prescribing targets; economics to financial incentives such as prescribing incentive schemes; and enforcement refers to regulations from health authorities [13,15,66]. However, the latter is rare in Scotland with no actual enforcement of regulations as seen for instance in Sweden with compulsory generic substitution and prescribing restrictions for statins in Finland and Norway following generic simvastatin [67–69].
We did not typically undertake any time-series analyses as multiple interventions with interlinked activities were undertaken at different times both nationally and regionally between 2001 and 2017. However, we did undertake such a time-series analysis comparing the changes in the items dispensed for citalopram and escitalopram before and after the warnings regarding possible QTc interval prolongation and any subsequent influence on the utilization of recommended SSRIs such as sertraline [70]. A p-value > 0.05 was seen as significant.
Results
Generic availability of SSRIs
Table 1 contains details of the year of patent expiry of the different SSRIs in Scotland.
| Generic name | Commercial name (originator) | ATC code | Year of patent expiration |
|---|---|---|---|
| Fluvoxamine | Faverin® | N06AB08 | Prior to 2000 |
| Fluoxetine | Prozac® | N06AB03 | 2000 |
| Paroxetine | Seroxat® | N06AB05 | Prior to 2000 |
| Citalopram | Cipramil® | N06AB04 | 2002 |
| Sertraline | Lustral® | N06AB06 | 2005 |
| Escitalopram | Cipralex® | N06AB10 | 2014 |
Influence of multiple measures
A number of demand-side measures have been introduced nationally and regionally in Scotland in recent years to enhance INN prescribing as well as influence the prescribing of different SSRIs due either to concerns with their safety or value [13,17,30,31,33,40,46,48,49,51,52,71–76]. These are summarized in Table 2.
| Measure | Year | National or regional | Initiative |
|---|---|---|---|
| Education | 2001–2017 | National and regional | • Physicians typically trained in medical school to prescribe by INN name with subsequent activities in GP practices coupled with IT systems to enhance INN prescribing |
| 2003 | National | • National warning regarding paroxetine in children | |
| 2003 | Regional (Lothian) | • Lothian highlighting the extent of savings from the prescribing of generic paroxetine vs originator | |
| 2006 | Regional (GGC) | • Fluoxetine and citalopram recommended SSRIs on the formulary list | |
| 2008 onward | Regional (GGC) | • Educating GPs to regularly review patients on long-term antidepressants (doses prescribed, effectiveness, treatment duration, guideline improvements and costs) | |
| 2009 | Regional (GGC) | • Fluoxetine and citalopram recommended SSRIs on the formulary list | |
| 2010 | Regional (GGC) | • Sertraline added to the recommended formulary list of SSRIs | |
| 2009/10– 2015 | Regional (GGC) | • Review of patients receiving the same antidepressant for ≥2 years conducted among 180 GP practices involving >8000 patients, the majority of whom receive SSRIs | |
| 2011 | National | • MHRA warning on QT interval prolongation with citalopram and escitalopram | |
| 2012 and 2015 | Regional (GGC) | • Escitalopram and citalopram at high risk of QT prolongation | |
| 2012 | Regional (Tayside) | • Warnings of QT interval prolongation with citalopram and escitalopram | |
| 2013 | Regional (Lothian) | • Guidance on potential risks associated with the prolongation of QTc interval with different psychotropic medicines | |
| 2017 | NHS Grampian | • Fluoxetine and sertraline recommended SSRIs with sertraline recommended in patients with cardiovascular disease (caution with citalopram) | |
| Engineering | 2002 | National | • Audit Scotland benchmarking DDDs of non-fluoxetine SSRIs and the extent of INN prescribing across Scotland |
| 2007 | National | • Health improvement, Efficiency, Governance, Access to services and Treatment (HEAT) targets. NHS Boards to reduce the annual rate of increase of defined daily dose per capita of antidepressants to zero by 2009/10 and put in place the required support framework to achieve a 10% reduction in future years | |
| 2007/2008 | Regional (Lothian) | • Total number of prescribed items of escitalopram ≤10% of all SSRIs (also linked with financial incentive schemes – Economics) | |
| 2008/09– 2012/13 | Regional (GGC) | • Fluoxetine and citalopram as a % of all SSRIs, duloxetine, mirtazapine, reboxetine and venlafaxine items ≥65% (or an absolute increase of 5%) items and linked with prescribing financial incentives (Economics) | |
| 2009/10 | Regional (GGC) | • Escitalopram prescribing <5% of all SSRIs items and linked to prescribing financial incentives (Economics) • Fluoxetine 60 mg capsules to 3 × 20 mg capsules (GB£39/patient as opposed to GB£360/patient) and linked to prescribing financial incentives (Economics) | |
| 2011/2012 | Regional (GGC) | • Citalopram and escitalopram QTc prolongation reviews of patients | |
| Economics (in addition to the above) | Ongoing | National/regional | • Practice incentive schemes for reaching agreed prescribing targets |
| Enforcement (although no actual enforcement in Scotland) | 2002/2006 | National | • Escitalopram initial rejected for use in NHS Scotland in 2002; however, accepted for use in 2006 |
DDD: Defined daily dose; GB£: Pound sterling; INN: International nonproprietary name; MHRA: Medicines and Healthcare Products Regulatory Agency; SSRI: Selective serotonin-reuptake inhibitor.
Total utilization & expenditure
There was a steady increase in the number of total SSRI items dispensed between 2001 and 2017 (Figure 1).
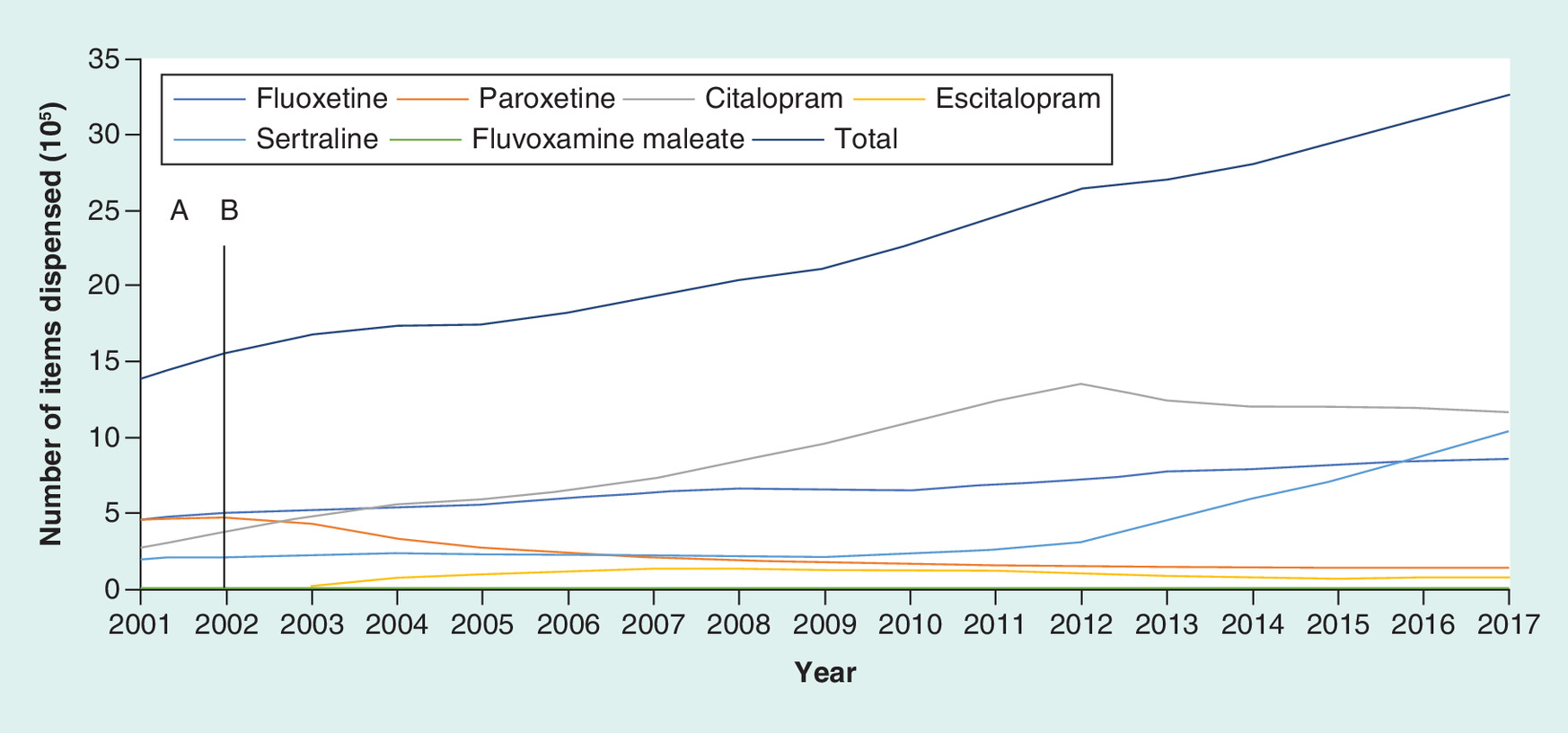
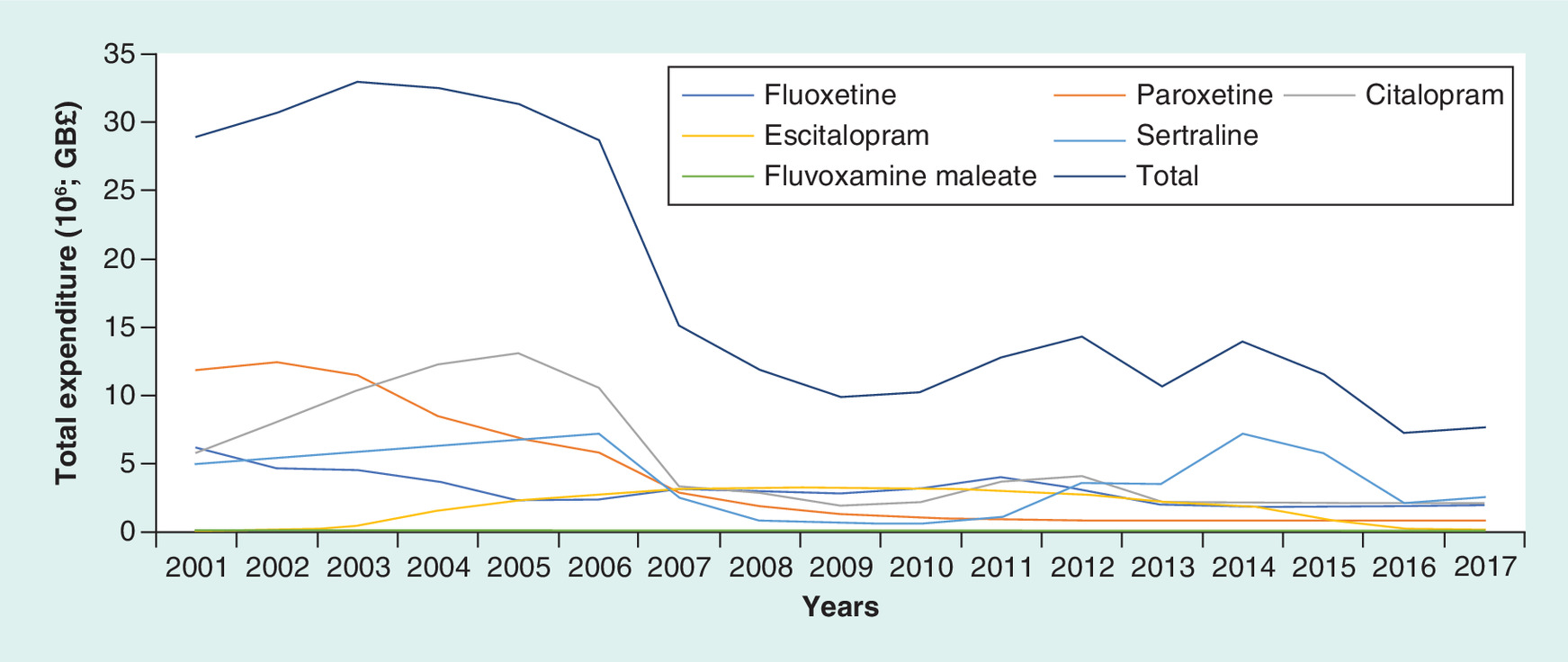
A total of 1.393 million items were dispensed in 2001 with a cost of GB£28.937 million, rising to 3.258 million items dispensed in 2017 at a cost of GB£7.613 million. This represents a 2.34-fold increase in SSRI utilization during this period but a 73.7% reduction in expenditure.
The increase in SSRI utilization during this period has been predominantly driven by increasing utilization of citalopram, initially rising from 19.8% of total SSRI items dispensed in 2001 (276 thousand items) to 51.3% in 2012 (1.352 million items) before falling to 35.6% in 2017 following concerns with QT prolongation (Table 2). During this period, sertraline utilization rose appreciably from 10.32% of total SSRI utilization in 2011 to 31.8% in 2017. Concurrent with this, fluoxetine utilization fell gradually from 33.2% of total SSRI items dispensed in 2001 to 26.3% in 2017 (Figure 1). The utilization of paroxetine fell steadily throughout the study period from 32.7% of total utilization in 2001 to 4.1% in 2017 following safety and other concerns, although these were not exclusively attributable to paroxetine. Overall during the study period, the number of items of paroxetine dispensed fell by 70.8%. There was low utilization of escitalopram throughout the study period, reaching a maximum of 6.99% of total items dispensed in 2007 before falling to 2.1% of total items dispensed in 2017 (Figure 1).
Figure 2 depicts a fall in total expenditure in recent years as more SSRIs lost their patents (Table 1).
This fall in SSRI expenditure was driven by a reduction in expenditure per item of the various SSRIs, especially after generic availability (Figure 3), with Table 3 depicting the price reductions over time for each SSRI that had lost its patent during the study period, in other words after 2001 (Table 1). Typically, the generic versions of SSRIs were dispensed once available with high rates of INN prescribing (Table 4).

| SSRI | % reduction in 2017 |
|---|---|
| Citalopram | 91.6 |
| Sertraline | 91.8 |
| Escitalopram | 90.4 |
SSRI: Selective serotonin-reuptake inhibitor.
| SSRI | % INN (items dispensed) |
|---|---|
| Paroxetine | 91.4–98.1 |
| Fluoxetine | 98.7–99.7 |
| Citalopram | 99.5–99.9 |
| Sertraline | 98.5–99.7 |
INN: International nonproprietary name; SSRI: Selective serotonin-reuptake inhibitor;
Differences in SSRI utilization patterns before & after concerns with QT prolongation
Figure 4 depicts the changes in the utilization (items dispensed) of citalopram, escitalopram and sertraline before and after concerns with potential QT prolongation with citalopram and escitalopram (Table 2), in other words 2001–2011 and after 2012
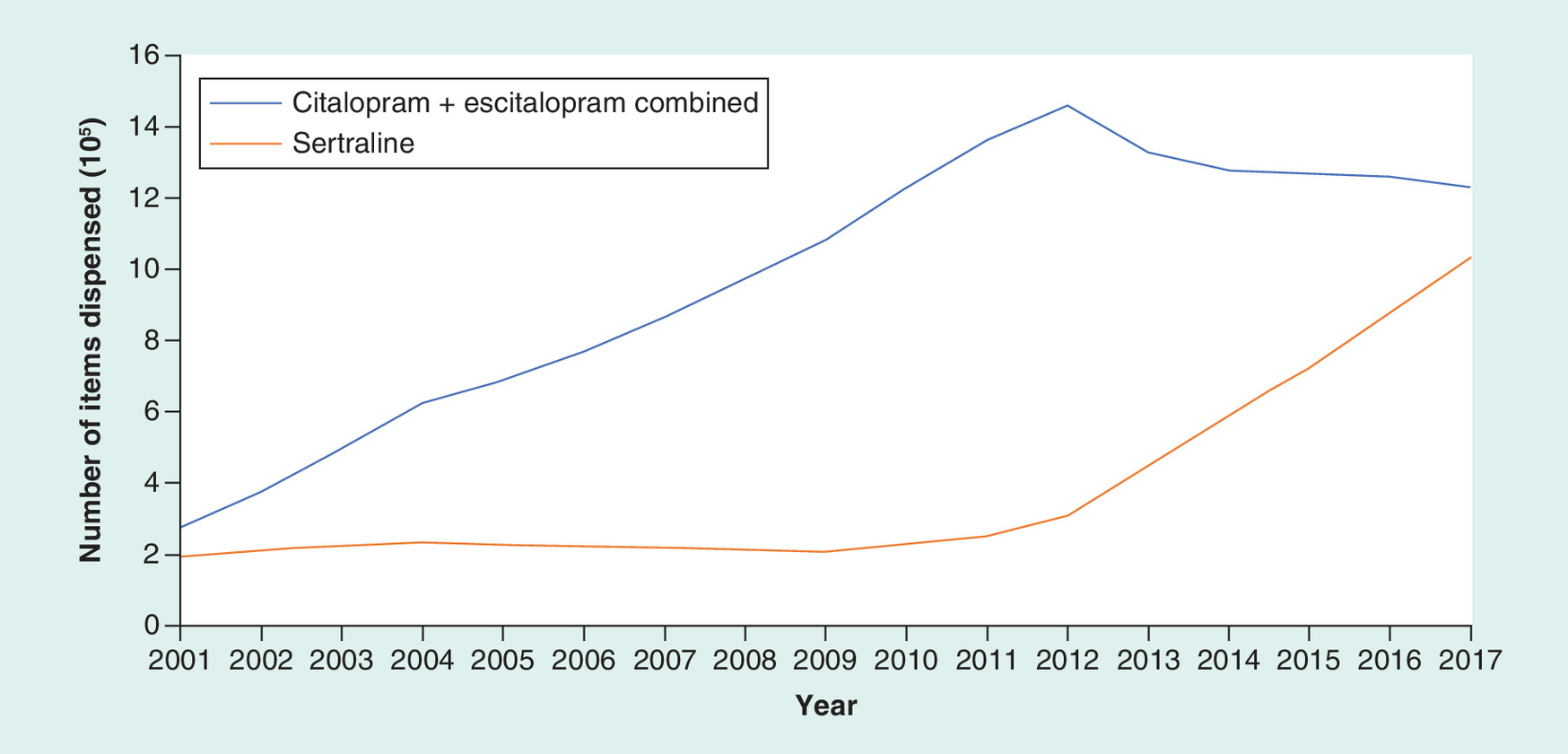
After the concerns with potential QT prolongation associated with citalopram and escitalopram use in 2012, there was a significant decreasing trend in citalopram and escitalopram use of 142, 951 items/year (p < 0.001) while the trend for prescribing of sertraline increased significantly by 141.016 items/year (p < 0.001).
Discussion
There has been an appreciable growth in SSRI items dispensed during the study period rising 2.34-fold (Figure 1). This may well be due to a widening of the indications for SSRIs to include anxiety as well as increasing diagnosis of depression as the diagnosis of depression and its management has not always been routinely recorded and coded as part of general practice contractual obligations [20,77], and depression has been underdetected and undertreated. This may lead to under reporting of this common illness even when patients are now more likely to seek help for their emotional distress [78]. The recent mental health and well-being survey suggests that one in six adults in England have a common mental disorder, with more people now seeking treatment [79]. The survey data from England indicates that there has been an increase in the proportion of people with clinical anxiety or depression disorders accessing mental health treatments, up from 24% in 2007 to 39% in 2014 [79]. There is no reason why Scotland should be any different from the findings in England. Patients are also receiving longer treatment [80]. Overall, we believe this growth in SSRI prescribing in Scotland in recent years (Figure 1) has been due to a combination of factors. These include SSRIs becoming available as low cost generics (Table 1; Figure 3) and adopted as first-line agents for the treatment of depression combined with additional prescribing targets (Table 2); an increase in prevalence rates and patients accessing mental health services; increasing long-term use; a lack of a regular proactive review of patients when they are stable and not in crisis; and the routine use of higher SSRI doses, which is contrary to current guidelines and evidence [17,30,43,52,77–82].
The potential associated costs with this growth in SSRI utilization have been offset by a considerable reduction in the cost/item for the various SSRIs apart from fluvoxamine (Figure 3). The price reductions seen for the various SSRIs over time (Table 3) mirror those for the lipid-lowering agents, losartan, PPIs and risperidone [15,19,83,84]. This coupled with high INN (Table 4) prescribing rates has resulted in an appreciable reduction in SSRI expenditure (73.7% reduction in 2017 vs 2001) to GB£7.613 million in 2017 (Figure 2). This is similar to the situation with lipid-lowering agents and PPIs in Scotland [15,19] providing guidance to other countries struggling with resource pressures.
The high rate of INN prescribing for the SSRIs in Scotland as a result of multiple activities (Table 2) is also similar to the situation seen with generic PPIs, statins, renin–angiotensin drugs and antipsychotics in Scotland [13,15,19,84,85]. This is encouraging and suggests no problems with the effectiveness and safety of generic SSRIs over many years. This is important for countries where there is still considerable prescribing of originator antidepressants despite the availability of good quality generics. This is not in the best interest of any key stakeholder group long term with potential resources being wasted, which could have been used to fund improved care in other situations including new medicines in patients with unmet need.
The reduction and then rise in the cost/item for fluvoxamine (Figure 3) may be a reflection of its limited use (Figure 1); consequently, limited competition and a need to reduce prices. This is seen in other situations across Europe [86]. However, this situation has made limited difference to the overall expenditure on SSRIs in Scotland with typically expenditure on fluvoxamine ranging from 0.21 to 0.85% of total SSRI expenditure during the study period.
The low utilization of escitalopram in 2007 in Scotland at 6.99% of total SSRIs dispensed (7.0% DDD basis) and 6.51% in 2008 compares favorably with 17.3% in Portugal (DDD basis) in 2007 and 30.8% in Ireland in 2008 [13] following multiple initiatives (Table 2). This is the only example of generic availability (citalopram) influencing the prescribing of patented SSRIs (escitalopram). As mentioned, general practitioners certainly in Glasgow were encouraged to switch suitable patients who were prescribed escitalopram prior to citalopram to citalopram. This was seen as an effective measure to conserve resources without compromising care with, as mentioned, typically 90% of patients remaining on citalopram at the 3-month review. Otherwise, there was no routine switching of SSRIs between patients. This was unlike the situation with the PPIs and statins in Scotland with no perceived differences in effectiveness between them [15,19]. Unlike the PPIs and statins, there were no national indicators encouraging the prescribing of particular SSRIs, although there were regional targets discouraging the prescribing of escitalopram (Table 2) [15,19,24]. This recognizes the fact that patients being treated for depression are considered more vulnerable and therefore their medication once seen as effective and tolerated is typically not changed. In addition, antidepressants certainly initially are prescribed as courses rather than life-long chronic treatment; consequently, a change to a different SSRI was generally through trying to influence the initial prescription rather than switching patients once prescribed a particular SSRI (Table 2). The situation with escitalopram was different (Table 2) as there was perceived limited clinical differences with citalopram; however, considerable differences in costs once generic citalopram became available (Figure 3).
The utilization patterns for paroxetine (Figure 1) were in line with expectations following the safety warnings; however, these were not exclusive to paroxetine although paroxetine was singled out initially [37,38,41]. In addition, concerns with the need for lengthier dose reductions following the decision to stop prescribing [43].
The significant reduction in the utilization citalopram and escitalopram, coupled with significantly increased use of sertraline in recent years, is also encouraging following safety warnings (Table 2; Figure 4). This further illustrates the favorable influence of both national and regional initiatives on effecting physician prescribing habits, which is not always the case [87–89]. As a result, again providing guidance to other countries.
Limitations
We are aware of a number of limitations with this study. This includes the fact that we were only able to analyze prescriptions dispensed and not their indication. However, two large studies in one Scottish Health Board area indicated that 87% of antidepressants were prescribed for depression, and less than 3% were prescribed for nonlicensed indications [20,77]. We could also not analyze the strength of doses prescribed to ascertain whether there were any change in the doses of SSRIs prescribed although two regional Scottish studies indicate that higher SSRIs doses are possibly being prescribed more commonly [20,78]. We are aware that there are multiple factors associated with prescribing of higher SSRI doses, including which anxiety disorders are being treated. For depression, which general practice a patient attends, if they are prescribed an SSRI for 2 years or more, and if they are coprescribed benzodiazepines and/or z-hypnotics for more than 8 weeks [20]. We also did not analyze utilization in terms of DDDs, which would have been more sensitive to changes in the doses of SSRIs prescribed; however, such studies have been undertaken. We could also not assess patient outcomes with the changes in SSRI prescribing patterns. Finally, from a safety perspective assessing the impact of the MHRA warning on the incidence of QTc prolongation and sudden cardiac death is very challenging as QT prolongation as a cause of death cannot be confirmed at autopsy. From an efficacy and wellness perspective, there are challenges with routinely collecting patient-level outcome data in ambulatory care for common mental health problems; consequently, limiting a national assessment of the impact of SSRI prescribing. Despite these limitations, we believe our findings are robust and provide guidance for the future.
Conclusion
The considerable reduction in the cost of SSRIs over the years once generics became available has resulted in lower costs despite an appreciable increase in SSRI utilization. This is to the benefit of all key stakeholders since the savings can be used in other disease areas such as funding new medicines that address current unmet need within a resource constrained environment.
Overall, the loss of patents has not influenced SSRI prescribing patterns apart from escitalopram. This is unlike the situation seen with the PPIs and lipid-lowering medicines, and reflects the differences in the effectiveness and safety of the different SSRIs.
The changes in the prescribing patterns of paroxetine, citalopram and escitalopram are encouraging and show healthcare professionals in Scotland act quickly on safety and other warnings, providing an example to other countries.
Finally, we believe analyses such as this as part of public health psychopharmacology are justified and provide practical research findings to guide future care. Consequently, we see this discipline growing in the future.
There is increasing use of antidepressants including selective serotonin-reuptake inhibitors (SSRIs) in Scotland in recent years with expanding of indications, greater awareness and medicalization of depression and greater number of patients accessing treatment for their depression.
There have also been safety concerns with some SSRIs including initially paroxetine and subsequently citalopram and escitalopram.
The increasing availability of generic SSRIs, coupled with the need to conserve costs including limiting prescribing of patented escitalopram, and safety concerns has resulted in multiple initiatives in Scotland in recent years.
High international nonproprietary name prescribing (up to 99.9%) and generics up to 92% below originator prices, coupled with initiatives to limit escitalopram prescribing, resulted in a 73.7% reduction in SSRI expenditure between 2001 and 2017 despite a 2.34-fold increase in utilization.
The safety warnings resulted in a significant reduction in the prescribing of paroxetine, citalopram and escitalopram coupled with a significant increase in the prescribing of sertraline.
Overall the multiple initiatives have increased the quality and efficiency of prescribing.
Financial & competing interests disclosure
The production of this paper was facilitated by a grant to Alec Morton by the University of Strathclyde under the university's New Professors’ Fund. CF Johnson, M Bennie, S Hurding and S MacBride-Stewart are all employed by NHS Scotland. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Garattini S, Bertele V, Godman B, Haycox A, Wettermark B, Gustafsson LL. Enhancing the rational use of new medicines across European healthcare systems. Eur. J. Clin. Pharmacol. 64(12), 1137–1138 (2008).
2.
Malmstrom RE, Godman BB, Diogene E et al. Dabigatran – a case history demonstrating the need for comprehensive approaches to optimize the use of new drugs. Front. Pharmacol. 4, 39 (2013).
3.
Godman B, Ortwijn W, de Waure C et al. Links between Pharmaceutical R&D Models and Access to Affordable Medicines. A Study for the ENVI COMMITTEE (2016). www.europarl.europa.eu/RegData/etudes/STUD/2016/587321/IPOL_STU(2016)587321_EN.pdf.
4.
WHO. Access to new medicines in Europe: technical review of policy initiatives and opportunities for collaboration and research. www.euro.who.int/__data/assets/pdf_file/0008/306179/Access-new-medicines-TR-PIO-collaboration-research.pdf?ua=1.
5.
Godman B, Malmstrom RE, Diogene E et al. Are new models needed to optimize the utilization of new medicines to sustain healthcare systems? Expert Rev. Clin. Pharmacol. 8(1), 77–94 (2015).
6.
Godman B, Acurcio F, Guerra Junior AA et al. Initiatives among authorities to improve the quality and efficiency of prescribing and the implications. J. Pharmaceut. Care Health Sys. 1(3), 1–15 (2014).
7.
Duerden MG, Hughes DA. Generic and therapeutic substitutions in the UK: are they a good thing? Brit. J. Clin. Pharmacol. 70(3), 335–341 (2010).
8.
MHRA. Antiepileptic drugs: updated advice on switching between different manufacturers’ products (2017). www.gov.uk/drug-safety-update/antiepileptic-drugs-updated-advice-on-switching-between-different-manufacturers-products#chm-review-and-update.
9.
Labiris G, Fanariotis M, Kastanioti C et al. Greek physicians’ perceptions on generic drugs in the era of austerity. Scientifica 2015, 251792 (2015). www.ncbi.nlm.nih.gov/pmc/articles/PMC4589622/.
10.
Dunne SS, Shannon B, Cullen W, Dunne CP. Beliefs, perceptions and behaviours of GPs towards generic medicines. Fam. Pract. 31(4), 467–474 (2014).
11.
Fadare JO, Adeoti AO, Desalu OO et al. The prescribing of generic medicines in Nigeria: knowledge, perceptions and attitudes of physicians. Expert Rev. Pharmacoecon. Outcomes Res. 16(5), 639–650 (2016).
12.
Bennie M, Godman B, Bishop I, Campbell S. Multiple initiatives continue to enhance the prescribing efficiency for the proton pump inhibitors and statins in Scotland. Expert Rev. Pharmacoecon. Outcomes Res. 12(1), 125–130 (2012).
13.
Godman B, Bishop I, Finlayson AE, Campbell S, Kwon HY, Bennie M. Reforms and initiatives in Scotland in recent years to encourage the prescribing of generic drugs, their influence and implications for other countries. Expert Rev. Pharmacoecon. Outcomes Res. 13(4), 469–482 (2013).
14.
Ferner RE, Lenney W, Marriott JF. Controversy over generic substitution. BMJ 340, c2548 (2010).
15.
Leporowski A, Godman B, Kurdi A et al. Ongoing activities to optimize the quality and efficiency of lipid-lowering agents in the Scottish national health service: influence and implications. Expert Rev. Pharmacoecon. Outcomes Res. 18(6), 655–666 (2018).
16.
NHS Scotland. The Scottish Government. National Therapeutic Indicators 2013 – Baseline Report (2013). www.sehd.scot.nhs.uk/publications/DC20131029nti.pdf.
17.
NHS Lothian. LOTHIAN PRESCRIBING BULLETIN. April/May 2008 (2018). www.ljf.scot.nhs.uk/PrescribingBulletins/2008/lpb/LPB%20Issue%20No%2032%20-%20FINAL.pdf.
18.
NHS Greater Glasgow and Clyde. Medicines Update Extra. ORAL PROTON PUMP INHIBITORS (2015). www.ggcprescribing.org.uk/media/uploads/ps_extra/mu_extra_04_-_2015.pdf.
19.
Godman B, Kurdi A, McCabe H et al. Ongoing activities to influence the prescribing of proton pump inhibitors within the Scottish National Health Service: their effect and implications. GaBI J. 7(4), (2018).
20.
Johnson CF, Dougall NJ, Williams B, MacGillivray SA, Buchanan AI, Hassett RD. Patient factors associated with SSRI dose for depression treatment in general practice: a primary care cross sectional study. BMC Fam. Pract. 15, 210 (2014).
•• Good study assessing factors affecting the prescribing of selective serotonin-reuptake inhibitors in the UK.
21.
Pilgrim D, Bentall R. The medicalisation of misery: a critical realist analysis of the concept of depression. J. Mental Health 8(3), 261–274 (1999).
22.
Dowrick C, Frances A. Medicalising unhappiness: new classification of depression risks more patients being put on drug treatment from which they will not benefit. BMJ 347, f7140 (2013).
23.
NHS Scotland, ISD Scotland. Medicines for mental health – years 2007/08 to 2017/18 (2018). www.isdscotland.org/Health-Topics/Prescribing-and-Medicines/Publications/data-tables2017.asp?id=2020#2020.
24.
Godman B, Baker A, Leporowski A et al. Initiatives to increase the prescribing of low cost generics; the case of Scotland in the international context. Med. Res. Arch. 5(3), 1–34 (2017).
25.
Godman B, Bucsics A, Burkhardt T et al. Potential to enhance the prescribing of generic drugs in patients with mental health problems in austria; implications for the future. Front. Pharmacol. 3, 198 (2012).
26.
Martin A, Godman B, Miranda J et al. Measures to improve angiotensin receptor blocker prescribing efficiency in the UK: findings and implications. J. Comp. Eff. Res. 3(1), 41–51 (2014).
27.
Cipriani A, Furukawa TA, Salanti G et al. Comparative efficacy and acceptability of 21 antidepressant drugs for the acute treatment of adults with major depressive disorder: a systematic review and network meta-analysis. Lancet 391(10128), 1357–1366 (2018).
•• Comprehensive study assessing the efficacy and acceptability of different antidepressants.
28.
Thorlund K, Druyts E, Wu P, Balijepalli C, Keohane D, Mills E. Comparative efficacy and safety of selective serotonin reuptake inhibitors and serotonin–norepinephrine reuptake inhibitors in older adults: a network meta-analysis. J. Am. Geriatr. Soc. 63(5), 1002–1009 (2015).
• Good study assessing the comparative effectiveness and safety of different selective serotonin-reuptake inhibitors.
29.
Bauer M, Pfennig A, Severus E, Whybrow PC, Angst J, Moller HJ. World Federation of Societies of Biological Psychiatry (WFSBP) guidelines for biological treatment of unipolar depressive disorders, part 1: update 2013 on the acute and continuation treatment of unipolar depressive disorders. World J. Biol. Psychiatry 14(5), 334–385 (2013).
30.
NHS Greater Glasgow and Clyde Annual Review 2010 Self Assessment (2010). www.nhsggc.org.uk/media/230557/nhsggc_annual_review_2009-10_self_assessment.pdf.
31.
Scottish Medicines Consortium. Escitalopram 5mg, 10mg and 20mg tablets (Cipralex) No. 253/06 (2006). www.scottishmedicines.org.uk/files/escitalopram_Cipralex__253-06_.pdf.
32.
Svensson S, Mansfield PR. Escitalopram: superior to citalopram or a chiral chimera? Psychother. Psychosom. 73(1), 10–16 (2004).
33.
NHS Lothian. LOTHIAN PRESCRIBING BULLETIN. www.ljf.scot.nhs.uk/PrescribingBulletins/2007/lpb/LPB%20Issue%20No%2026.pdf.
34.
Godman B, Persson M, Miranda J et al. Changes in the utilization of venlafaxine after the introduction of generics in Sweden. Appl. Health Econ. Health Policy 11(4), 383–393 (2013).
• Interesting study assessing the impact of restricting prescribing of antidepressants in Sweden.
35.
Wagner G, Schultes M-T, Titscher V, Teufer B, Klerings I, Gartlehner G. Efficacy and safety of levomilnacipran, vilazodone and vortioxetine compared with other second-generation antidepressants for major depressive disorder in adults: a systematic review and network meta-analysis. J. Affect. Disord. 228, 1–12 (2018).
36.
Hertfordshire Partnership University, NHS Foundation Trust East and North Hertfordshire Clinical Commissioning Group, Herts Valleys Clinical Commissioning Group. Guidelines on Choice and Selection of Antidepressants for the Management of Depression (2016). www.hpft.nhs.uk/media/1584/guidelines-on-choice-and-selection-of-antidepressants-for-the-management-of-depression-final-oct-2016.pdf.
37.
Wooltorton E. Paroxetine (Paxil, Seroxat), increased risk of suicide in pediatric patients. CMAJ 169(5), 446 (2003).
38.
Aursnes I, Tvete IF, Gaasemyr J, Natvig B. Suicide attempts in clinical trials with paroxetine randomised against placebo. BMC Med. 3(1), 14 (2005).
39.
Breggin P. Court filing makes public my previously suppressed analysis of paxil's effects. Ethical Hum. Psychol. Psychiatry 8(1), 77–84 (2006).
40.
Waechter F. Paroxetine must not be given to patients under 18. BMJ 326(7402), 1282 (2003).
41.
Sharma T, Guski LS, Freund N, Gotzsche PC. Suicidality and aggression during antidepressant treatment: systematic review and meta-analyses based on clinical study reports. BMJ 352, i65 (2016).
42.
Stone M, Laughren T, Jones ML et al. Risk of suicidality in clinical trials of antidepressants in adults: analysis of proprietary data submitted to US Food and Drug Administration. BMJ 339, b2880 (2009).
43.
NICE. Depression in adults: recognition and management. Clinical guideline [CG90] published October 2009 (2018). www.nice.org.uk/guidance/cg90/chapter/1-Guidance#treatment-choice-based-on-depression-subtypes-and-personal-characteristics.
44.
Tran E, Dishman B. Citalopram-induced QTc prolongation: a brief review of the data. Mental Health Clinician 2(6), 139–141 (2012).
45.
Tampi RR, Balderas M, Carter KV et al. Citalopram, QTc Prolongation, and Torsades de Pointes. Psychosomatics 56(1), 36–43 (2015).
46.
NHS Greater Glasgow and Clyde. Medicines Update Extra. Drug induced Qt prolongation (2015). www.ggcprescribing.org.uk/media/uploads/ps_extra/medicines_update_extra_qt_prolongation_may_15_incl_hydroxyzine.pdf.
47.
NHS Greater Glasgow and Clude. Post Script Extra. Drug Induced Qt Prolongation (2012). www.ggcprescribing.org.uk/media/uploads/ps_extra/pse_21.pdf.
48.
TAYSIDE PRESCRIBER. Citalopram & escitalopram:QT interval prolongation (2012). www.nhstaysideadtc.scot.nhs.uk/Antibiotic%20site/pdf%20docs/Tayside%20Prescriber%20122%20-%20escitalopram%20and%20citalopram%20May%2012.pdf.
49.
MHRA. Medicines and healthcare products regulatory agency. Citalopram and escitalopram: QT interval prolongation (2011). www.gov.uk/drug-safety-update/citalopram-and-escitalopram-qt-interval-prolongation.
50.
Cipriani A, La Ferla T, Furukawa TA et al. Sertraline versus other antidepressive agents for depression. Cochrane Database Syst. Rev. (4), Cd006117 (2010).
• Good study assessing the effectiveness and safety of sertraline.
51.
NHS Grampian. NHS Grampian Guidance for Initiating Antidepressants (2017). http://foi.nhsgrampian.org/globalassets/foidocument/foi-public-documents1---all-documents/AntDepS.pdf.
52.
Johnson CF, Williams B, MacGillivray SA, Dougall NJ, Maxwell M. ‘Doing the right thing’: factors influencing GP prescribing of antidepressants and prescribed doses. BMC Fam. Pract. 18(1), 72 (2017).
•• Interesting study assessing factors influencing the prescribing of antidepressants in the UK.
53.
Adli M, Baethge C, Heinz A, Langlitz N, Bauer M. Is dose escalation of antidepressants a rational strategy after a medium-dose treatment has failed? A systematic review. Eur. Arch. Psychiatry Clin. Neurosci. 255(6), 387–400 (2005).
54.
Godman B, Wettermark B, van Woerkom M et al. Multiple policies to enhance prescribing efficiency for established medicines in Europe with a particular focus on demand-side measures: findings and future implications. Front. Pharmacol. 5, 106 (2014).
55.
Abbing-Karahagopian V, Huerta C, Souverein PC et al. Antidepressant prescribing in five European countries: application of common definitions to assess the prevalence, clinical observations, and methodological implications. Eur. J. Clin. Pharmacol. 70(7), 849–857 (2014).
56.
Lewer D, O'Reilly C, Mojtabai R, Evans-Lacko S. Antidepressant use in 27 European countries: associations with sociodemographic, cultural and economic factors. Brit. J. Psych. 207(3), 221–226 (2015).
• Interesting study assessing antidepressant prescribing across Europe.
57.
WHO. Improving access to and appropriate use of medicines for mental disorders (2017). http://apps.who.int/iris/bitstream/handle/10665/254794/9789241511421-eng.pdf;jsessionid=EA10F15C6B514516A8AD9CCED0C55F9C?sequence=1.
58.
Cameron A, Ewen M, Ross-Degnan D, Ball D, Laing R. Medicine prices, availability, and affordability in 36 developing and middle-income countries: a secondary analysis. Lancet 373(9659), 240–249 (2009).
59.
Cameron A, Mantel-Teeuwisse AK, Leufkens HG, Laing RO. Switching from originator brand medicines to generic equivalents in selected developing countries: how much could be saved? Value Health 15(5), 664–673 (2012).
60.
WHO. WHO Model List of Essential Medicines – March 2017; Amended August 2017. www.who.int/medicines/publications/essentialmedicines/20th_EML2017_FINAL_amendedAug2017.pdf?ua=1.
61.
Barbui C, Ostuzzi G, Godman B. Public health psychopharmacology: a new research discipline comes of age? Epidemiol. Psychiatr. Sci. 27(1), 24–28 (2018).
62.
ISD Scotland. Community dispensing. Prescription cost analysis. http://isdscotland.org/Health-Topics/Prescribing-and-Medicines/Community-Dispensing/Prescription-Cost-Analysis/.
63.
WHO. WHO Collaborating Centre for Drug Statistics Methodology. ATC/DDD Index. www.whocc.no/.
64.
Godman B, Shrank W, Andersen M et al. Comparing policies to enhance prescribing efficiency in Europe through increasing generic utilization: changes seen and global implications. Expert Rev. Pharmacoecon. Outcomes Res. 10(6), 707–722 (2010).
65.
NHS Scotland. National therapeutic indicators. 2012 – baseline data. www.sehd.scot.nhs.uk/pca/PCA2012(M)08report.pdf.
66.
Wettermark B, Godman B, Jacobsson B, Haaijer-Ruskamp FM. Soft regulations in pharmaceutical policy making: an overview of current approaches and their consequences. Appl. Health Econ. Health Policy 7(3), 137–147 (2009).
67.
Godman B, Wettermark B, Hoffmann M, Andersson K, Haycox A, Gustafsson LL. Multifaceted national and regional drug reforms and initiatives in ambulatory care in Sweden: global relevance. Expert Rev. Pharmacoecon. Outcomes Res. 9(1), 65–83 (2009).
68.
Godman B, Sakshaug S, Berg C, Wettermark B, Haycox A. Combination of prescribing restrictions and policies to engineer low prices to reduce reimbursement costs. Expert Rev. Pharmacoecon. Outcomes Res. 11(1), 121–129 (2011).
69.
Martikainen JE, Saastamoinen LK, Korhonen MJ, Enlund H, Helin-Salmivaara A. Impact of restricted reimbursement on the use of statins in Finland: a register-based study. Med. Care 48(9), 761–766 (2010).
70.
Fulcher BD, Little MA, Jones NS. Highly comparative time-series analysis: the empirical structure of time series and their methods. J. R. Soc. Interface 10(83), 20130048 (2013).
71.
NHS Greater Glasgow and Clyde. The Greater Glasgow and Clyde Formualary. Third Edition August 2009 (2009). www.nhsggc.org.uk/media/226772/Document%207%20NHS%20Formulary%202009.pdf.
72.
Scottish Medicines Consortium. Escitalopram (Cipralex) (2003). www.scottishmedicines.org.uk/media/1651/escitalopramresubmission_070303_.pdf.
73.
Audit Scotland. Supporting prescribing in general practice - a progress report (2003). www2.gov.scot/Publications/2010/01/18120533/3.
74.
LOTHIAN PRESCRIBING BULLETIN (2003). www.ljf.scot.nhs.uk/PrescribingBulletins/2003/lpb/LPB%20Issue%20No%202.pdf.
75.
NHS Lothian Prescribing Bulletin January 2013 (2013). www.ljf.scot.nhs.uk/PrescribingBulletins/2013Issues/LPB/Lothian%20Prescribing%20Bulletin%20Issue%2059%20Jan%202013%20FINAL.pdf.
76.
NHS Scotland. Mental Health Collaborative Programme Newsletter (2009). www2.gov.scot/Publications/2009/02/13140255/0.
77.
Johnson CF, Macdonald HJ, Atkinson P, Buchanan AI, Downes N, Dougall N. Reviewing long-term antidepressants can reduce drug burden: a prospective observational cohort study. Brit. J. Gen. Pract. 62(604), e773–e779 (2012).
•• Good study discussing the rationale for reviewing patients on long-term antidepressants.
78.
Lockhart P, Guthrie B. Trends in primary care antidepressant prescribing 1995–2007: a longitudinal population database analysis. Brit. J. Gen. Pract. 61(590), e565–e572 (2011).
79.
McManus S, Bebbington P, Jenkins R, Brugha T. Mental health and wellbeing in England – Adult Psychiatric Morbidity Survey 2014 Executive Summary (2014). https://files.digital.nhs.uk/pdf/s/5/adult_psychiatric_study_executive_summary_web.pdf.
80.
Moore M, Yuen HM, Dunn N, Mullee MA, Maskell J, Kendrick T. Explaining the rise in antidepressant prescribing: a descriptive study using the general practice research database. BMJ 339, b3999 (2009).
81.
Sinclair JE, Aucott LS, Lawton K, Reid IC, Cameron IM. The monitoring of longer term prescriptions of antidepressants: observational study in a primary care setting. Fam. Pract. 31(4), 419–426 (2014).
82.
Cleare A, Pariante CM, Young AH et al. Evidence-based guidelines for treating depressive disorders with antidepressants: a revision of the 2008 British Association for Psychopharmacology guidelines. J. Psychopharmacol. 29(5), 459–525 (2015).
83.
Godman B, Wettermark B, Miranda J, Bennie M, Martin A, Malmstrom RE. Influence of multiple initiatives in Sweden to enhance ARB prescribing efficiency following generic losartan; findings and implications for other countries. Int. J. Clin. Pract. 67(9), 853–862 (2013).
84.
Bennie M, Bishop I, Godman B et al. Are specific initiatives required to enhance prescribing of generic atypical antipsychotics in Scotland?: international implications. Int. J. Clin. Pract. 67(2), 170–80 (2013).
85.
Bennie M, Bishop I, Godman B et al. Are prescribing initiatives readily transferable across classes: the case of generic losartan in Scotland? Qual. Prim. Care 21(1), 7–15 (2013).
86.
Dylst P, Simoens S. Does the market share of generic medicines influence the price level?: a European analysis. PharmacoEconomics 29(10), 875–882 (2011).
87.
Fitzgerald A, Lethaby A, Cikalo M, Glanville J, Wood H. Review of Systematic Reviews Exploring the Implementation/Uptake of Guidelines. Yorh Health Economics Consortium. www.nice.org.uk/guidance/ph56/evidence/evidence-review-2-431762366.
88.
Brusamento S, Legido-Quigley H, Panteli D et al. Assessing the effectiveness of strategies to implement clinical guidelines for the management of chronic diseases at primary care level in EU Member States: a systematic review. Health Policy 107(2–3), 168–183 (2012).
89.
Sandora TJ, Fung M, Melvin P, Graham DA, Rangel SJ. National variability and appropriateness of surgical antibiotic prophylaxis in US children's hospitals. JAMA Pediatrics 170(6), 570–576 (2016).
Information & Authors
Information
Published In
Copyright
© 2019 Future Medicine Ltd.
History
Received: 23 November 2018
Accepted: 11 February 2019
Published online: 26 April 2019
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Ongoing initiatives within the Scottish National Health Service to affect the prescribing of selective serotonin reuptake inhibitors and their influence. (2019) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2018-0132
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Esther de Vries, Petra Denig, Taco B. M. Monster, Peter G. M. Mol, Mixed Impact of Direct Healthcare Professional Communications When Considering Proximal Outcomes and the Targeted Population: A Systematic Review, Pharmacoepidemiology and Drug Safety, 10.1002/pds.70135, 34, 3, (2025).
- Weimiao Li, Xiaoyu Li, Yaoguang He, Luwen Shi, Jing Chen, Effects of Generic Entry on Market Shares and Prices of Originator Drugs: Evidence from Chinese Pharmaceutical Market, PharmacoEconomics - Open, 10.1007/s41669-025-00570-6, 9, 4, (639-648), (2025).
- Mathieu Charbonneau, Steven G. Morgan, Camille Gagnon, Cheryl A. Sadowski, James L. Silvius, Cara Tannenbaum, Justin P. Turner, Factors influencing the effects of policies and interventions to promote the appropriate use of medicines in high-income countries: A rapid realist review, Health Policy, 10.1016/j.healthpol.2024.105027, 142, (105027), (2024).
- Irina Iaru, Camelia Bucsa, Andreea Farcas, Cristina Pop, Anamaria Cristina, Sebastian Armean, Irina Brumboiu, Oliviu Vostinaru, Cristina Mogosan, Utilization of psychotropic medicines in Romania during 1998–2018, Frontiers in Pharmacology, 10.3389/fphar.2023.1157231, 14, (2023).
- Hye-Young Kwon, Brian Godman, Editorial: Pharmaceutical policy, impact and health outcomes, Frontiers in Pharmacology, 10.3389/fphar.2023.1150055, 14, (2023).
- Rogério Hoefler, Taís Freire Galvão, Inês Ribeiro-Vaz, Marcus Tolentino Silva, Trends in Brazilian market of antidepressants: A five-year dataset analysis, Frontiers in Pharmacology, 10.3389/fphar.2022.893891, 13, (2022).
- Ileana Mardare, Stephen M. Campbell, Johanna C. Meyer, Israel Abebrese Sefah, Amos Massele, Brian Godman, Enhancing Choices Regarding the Administration of Insulin Among Patients With Diabetes Requiring Insulin Across Countries and Implications for Future Care, Frontiers in Pharmacology, 10.3389/fphar.2021.794363, 12, (2022).
- Brian Godman, Magdalene Wladysiuk, Stuart McTaggart, Amanj Kurdi, Eleonora Allocati, Mihajlo Jakovljevic, Francis Kalemeera, Iris Hoxha, Anna Nachtnebel, Robert Sauermann, Manfred Hinteregger, Vanda Marković-Peković, Biljana Tubic, Guenka Petrova, Konstantin Tachkov, Juraj Slabý, Radka Nejezchlebova, Iva Selke Krulichová, Ott Laius, Gisbert Selke, Irene Langner, András Harsanyi, András Inotai, Arianit Jakupi, Svens Henkuzens, Kristina Garuolienė, Jolanta Gulbinovič, Patricia Vella Bonanno, Jakub Rutkowski, Skule Ingeberg, Øyvind Melien, Ileana Mardare, Jurij Fürst, Sean MacBride-Stewart, Carol Holmes, Caridad Pontes, Corinne Zara, Marta Turu Pedrola, Mikael Hoffmann, Vasileios Kourafalos, Alice Pisana, Rita Banzi, Stephen Campbell, Bjorn Wettermark, Utilisation Trend of Long‐Acting Insulin Analogues including Biosimilars across Europe: Findings and Implications, BioMed Research International, 10.1155/2021/9996193, 2021, 1, (2021).
- Amanj Kurdi, Opioids and Gabapentinoids Utilisation and Their Related-Mortality Trends in the United Kingdom Primary Care Setting, 2010–2019: A Cross-National, Population-Based Comparison Study, Frontiers in Pharmacology, 10.3389/fphar.2021.732345, 12, (2021).
- Brian Godman, Joseph Fadare, Hye-Young Kwon, Carolina Zampirolli Dias, Amanj Kurdi, Isabella Piassi Dias Godói, Dan Kibuule, Iris Hoxha, Sylvia Opanga, Zikria Saleem, Tomasz Bochenek, Vanda Marković-Peković, Ileana Mardare, Aubrey C Kalungia, Stephen Campbell, Eleonora Allocati, Alice Pisana, Antony P Martin , Johanna C Meyer, Evidence-based public policy making for medicines across countries: findings and implications for the future, Journal of Comparative Effectiveness Research, 10.2217/cer-2020-0273, 10, 12, (1019-1052), (2021).