Efficacy of gelatin tannate for acute diarrhea in children: a systematic review and meta-analysis
Abstract
Aim: To investigate by meta-analysis the efficacy of gelatin tannate (GT), a mucosal barrier protector, in children with acute gastroenteritis. Methods: A comprehensive literature search was conducted. Studies were selected according to PICO: Participants: children aged 0−12 years with acute diarrhea; Intervention: GT; Comparison: oral rehydration solution and/or placebo; Outcomes: diarrhea-related outcomes. Results: Three published randomized controlled trials were identified of pediatric diarrhea treated with GT (n = 203) or control (n = 204). GT significantly (p < 0.01) reduced stool frequency at 12 h in two randomized controlled trials. A significant treatment effect (risk ratio = 0.74; p < 0.01) in favor of GT was found for the exploratory composite outcome of ‘diarrhea or liquid stools at 24 h’ in three studies. Risk ratios in a single study which reported the percentage of patients with liquid stools at 12, 24 and 48 h favored GT at all time points. No significant differences were found between GT and control for patients with diarrhea at 12 or 24 h or for duration of diarrhea. Conclusion: GT improved stool frequency and stool consistency in children with acute diarrhea, although further well-controlled studies would be useful to confirm a beneficial treatment effect.
Diarrheal diseases are common and are a leading cause of preventable death, especially among young children in developing countries [1]. In 2013, the global incidence of acute diarrheal diseases was 2.7 billion [2]. In children and adolescents, the global number of deaths in 2013 due to diarrheal diseases was 590,607, with the vast majority occurring in developing countries. Diarrhea was also the most common cause of death among older children (aged 5–9 years), with more than 38,000 deaths estimated globally in 2013 [3]. In Europe, acute gastroenteritis is the most common cause of primary care consultations among children less than 5 years of age [4].
There is considerable heterogeneity in pathogen-specific causes of community-acquired diarrhea in developing countries. Norovirus, rotavirus, Campylobacter species, astrovirus and Shigella species are all common causes of diarrhea in infants aged up to 2 years [5]. In European countries, rotavirus is the most common cause of pediatric acute gastroenteritis, although norovirus is fast gaining ground as the leading cause of medically-attended acute gastroenteritis in countries with high rotovirus vaccination coverage [6]. Adenovirus and Salmonella species are also responsible for significant morbidity and hospital admissions [6-8].
Dehydration is the most serious consequence of acute gastroenteritis in children [6]. European guidelines recommend oral rehydration with a hypo-osmolar solution as the mainstay of treatment for dehydration [6]. If required, the duration and severity of diarrhea can be reduced by active treatment with specific probiotics such as Lactobacillus GG or Saccharomyces boulardii or with the antidiarrheal drugs diosmectite or racecadotril [6].
The mucosal barrier protector, gelatin tannate (GT), is a new therapeutic option for treating acute gastroenteritis and diarrhea. GT is a complex of tannic acid and gelatin which forms a protein-based biofilm on the intestinal mucosa [9-11]. The antidiarrheal effects of GT have been demonstrated in adults [12] and in children when co-administered with an oral rehydration solution (ORS) [13].
In this study, we performed a systematic review and meta-analysis of randomized controlled trials (RCTs) that investigated the efficacy of GT in children with acute gastroenteritis.
Methodology
Search strategy
A systematic search of Medline [14] was performed in December 2017 by one reviewer using the search terms ((‘gelatin’[MeSH Terms] OR ‘gelatin’[All Fields]) AND ‘tannate’[All Fields]) AND ((‘diarrhoea’[All Fields] OR ‘diarrhea’[MeSH Terms] OR ‘diarrhea’[All Fields]) OR (‘gastroenteritis’[MeSH Terms] OR ‘gastroenteritis’[All Fields])) AND ((‘child’[MeSH Terms] OR ‘child’[All Fields] OR ‘children’[All Fields]) OR (‘pediatrics’[MeSH Terms] OR ‘paediatrics’[All Fields] OR ‘pediatric’[All Fields])). Alternative searches omitted the terms child/children and pediatric/paediatrics, but filtered the results with ‘humans’ from 0 to 12 years; and searched only with ‘gelatin’ AND ‘tannate’ and filtered the results for ‘humans’ from 0 to 12 years. Searches were restricted to papers published in English. The search term ‘gelatin tannate’ was then used to search Google Scholar [15], Cochrane Library Plus [16], and two clinical trials databases: ClinicalTrials.gov [17] and the EU Clinical Trials Register [18]. These searches identified no additional articles.
Inclusion & exclusion criteria
Studies were selected according to PICO (participant, intervention, comparison and outcomes) [19] as follows: Participants: children aged 0−12 years with acute diarrhea; Intervention: gelatin tannate; Comparison: ORS and/or placebo; Outcomes: diarrhea-related outcomes.
Exclusion criteria were: duplicate publications; studies without usable data; reviews, letters and single case reports; and preclinical studies.
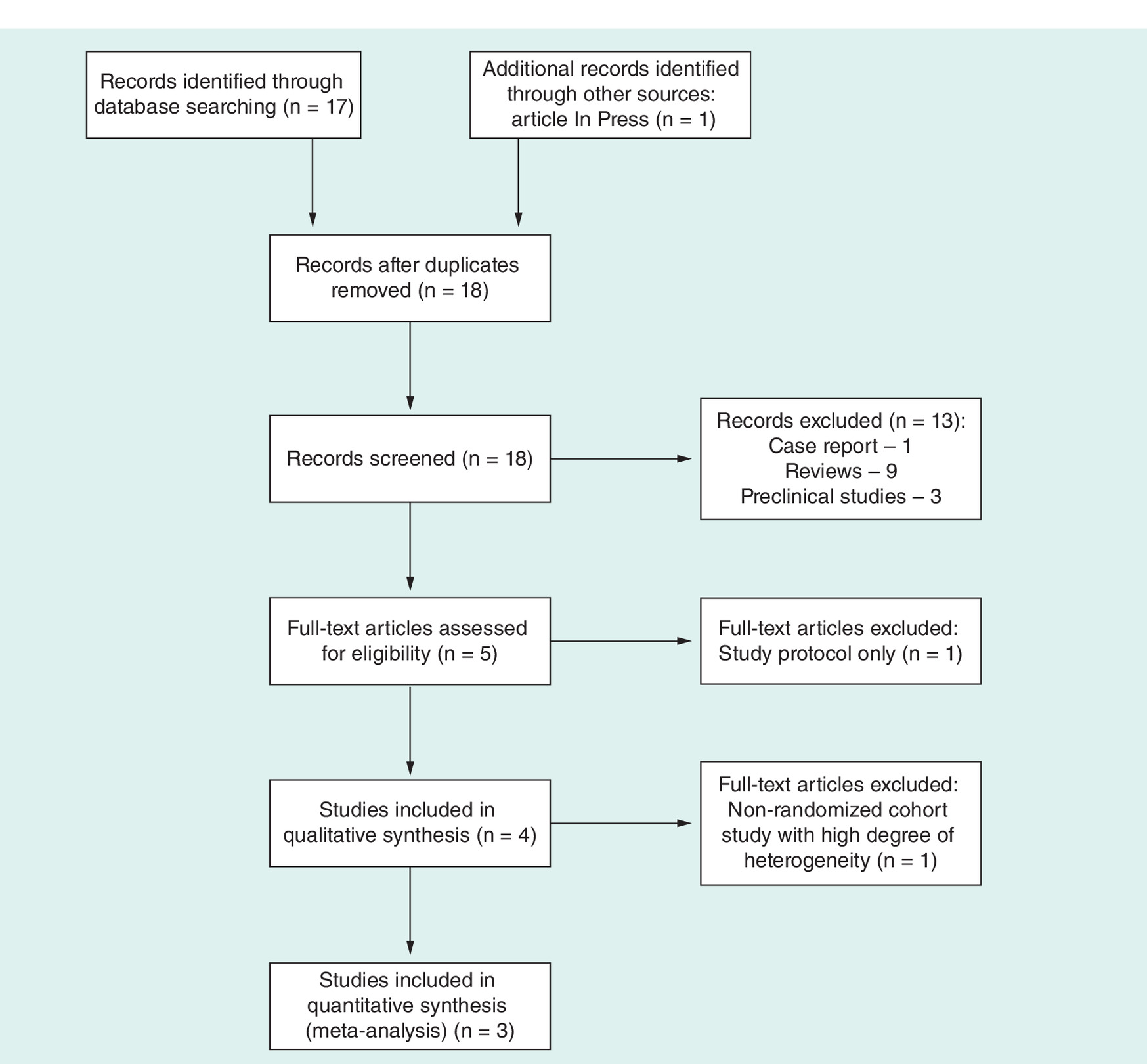
Four published clinical studies [13,20–22] and one completed but as yet unpublished clinical study [23,24] investigating GT for the treatment of acute diarrhea in children were identified. The study by Esteban Carretero et al. [13] was excluded due to the lack of randomization and high degree of heterogeneity within the study. The study of Michałek et al. [23] was excluded due to the absence of clinical data at the time of analyses. A flow diagram of the study search and selection process is provided in Figure 1.
Data from the three studies included in the quantitative synthesis were extracted independently by two reviewers. Discrepancies between reviewers were identified and resolved by consensus. Data were extracted for the main design variables which were: study design; experimental and control treatments; indication; patients’ baseline status; main inclusion and exclusion criteria; age and gender; sample size in experimental and control groups. Data were extracted for outcome variables measuring our prespecified evaluation criteria (stool frequency and consistency, and duration of diarrhea): number of stools at 12 or 24 h (mean ± standard deviation [SD]); liquid stools at 12 or 24 h (proportion of patients); persistence of diarrhea at 12 or 24 h (proportion of patients); and duration of diarrhea in hours (mean ± SD). Other outcomes data (e.g., symptoms), which were reported in only one or two studies, were not extracted. In some instances, the required data were not readily available in the text or tables of the articles, but could be estimated from other documented quantities or graphics:
In the study of Çagan et al. [21], the percentage of patients with diarrhea at 24 h, and the percentage of patients with liquid stools at 12, 24 and 48 h, was estimated from a graph (Figure 1C of the original article); and the SD of number of stools at 12 h, which was not provided in Figure 2, was estimated from the baseline SD then halved because the rate of 12 h to baseline SD values was about 0.5 in the other studies.
In the study of Kara et al. [22], the SDs of duration of diarrhea were not documented and, instead, were estimated by assuming an exponential distribution.
Data analysis
Results from studies were combined using the following methods: for continuous outcomes (number of stools and duration of diarrhea), the mean difference (MD) and 95% CI were calculated; for binary variables (proportions of patients with liquid stools or persistence of diarrhea), the absolute frequency (count) was computed from the reported percentage and sample size. The Mantel–Haenszel method was used to combine study results, and treatment effects were estimated by calculation of the risk ratio (RR). Heterogeneity between studies was assessed by the χ2 heterogeneity test and the I2 statistic. Both fixed effect and random effects models were run, with the random effects model used for analysis of studies with high heterogeneity. All analyses were conducted using the R language (The R Foundation, Vienna, Austria) [26], using the ‘meta’ package [27] for meta-analysis.
Results
Search-identified studies
The systematic search identified five studies investigating GT for treatment of acute pediatric diarrhea. The study of Esteban Carretero et al. [13] was excluded following a quality assessment and, at the time of analysis, results were not yet available for a recently completed study (Clinicaltrials.gov identifier: NCT02280759) [23,24].
The design features of the three RCTs included for meta-analysis, and characteristics of the respective patient populations, are summarized in Table 1. One study compared GT + ORS with ORS alone [20]; one study compared GT +ORS with placebo + ORS [21]; and one study compared GT and placebo (with no declared ORS) [22]. The age range for eligible patients across studies was 3 months to 12 years. Two studies stated acute diarrhea, and one study stated acute gastroenteritis, as the study indication. All studies specified a minimum stools frequency of 3 movements/day, including the study of Çağan et al. which also graded stool consistency according to the Bristol Stool Scale [28]. Use of other antidiarrheal agents was not permitted in any study. Çağan et al. allowed use of antibiotics. A total of 203 and 204 patients were enrolled in the GT and control groups, respectively. Mennini et al. reported median age (20 months for GT + ORS; 18 months for ORS) and a range of 3–66 months. The other two studies reported mean age of about 3.5 years. As Çağan et al. reported mean (SD) age and gender distribution for the entire per protocol population instead of by treatment group, the same values are applied to the GT and control groups in Table 1.
| Study (year) | Design | Comparator groups | Age range | Indication | Stools | Exclusion criteria | Gelatin tannate | Control | Ref. | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | Mean age ± SD | Males (%) | n | Mean age ± SD | Males (%) | ||||||||
| Mennini et al. (2017) | RCT, single-blind | GT + ORS vs ORS | 3 m–6 y | Acute gastroenteritis | >3/d for >24 h, low stool consistency | Acute gastroenteritis (>3 days) or other gastrointestinal diseases | 29 | 20 m (range 3–66 m)† | 48 | 31 | 18 m (range 7–43 m)† | 52 | [20] |
| Çagan et al. (2017) | RCT, double-blind | GT + ORS vs placebo + ORS | 3 m–12 y | Acute infectious and non-infectious diarrhea | ≥3/d; BSS grade 7 ‡ | Chronic or toxic diarrhea, celiac disease, lactose intolerance, immune diseases, infantile colic, other gastrointestinal diseases e.g. Crohn's disease | 103 | 40 ± 36 m§ | 57.6§ | 100 | 40 ± 36 m§ | 57.6§ | [21] |
| Kara et al. (2017) | RCT, single-blind | GT vs placebo | 6 m–10 y | Acute diarrhea in previous 12–72 h | >3/d | Severe dehydration, malnutrition, immunodeficiency, other chronic diseases | 71 | 44 ± 35.7 m | 59.1 | 73 | 44 ± 31.8 m | 42.4 | [22] |
†Reported as median age.
‡Bristol Stool Scale (BSS) 7 = watery stools, no solid pieces, entirely liquid [28].
§Details were provided for the per protocol study population and therefore applied to both treatment groups.
d: day; h: hour; m: month; RCT: randomized controlled trial; y: year.
Risk of bias in the individual studies was assessed according to the Cochrane Handbook and is reported in Table 2. All studies were described as randomized, but the studies of Çagan et al. and Kara et al. did not mention allocation concealment, and the limited information provided by the authors about the treatment allocation process raises doubts as to the adequacy of randomization in these two studies. The studies of Mennini et al. and Kara et al. were reported as single-blind, although both conducted a blind assessment of study outcomes. The study of Çagan et al. was described as double-blind. All three studies described dropouts and withdrawals, although Çagan et al. did not provide information about exclusions per treatment group.
| Study (year) | Domain | Risk | Reasons | Ref. |
|---|---|---|---|---|
| Mennini et al. (2017) | Random sequence generation (selection bias) | Low | Quote: “All children were randomly assigned to the groups using a computer-generated randomization list” | [20] |
| Allocation concealment (selection bias) | Low | Quote: “The sequence was concealed and envelopes for consecutive patients prepared accordingly. As each patient was recruited, the next envelope in sequence was opened to determine the allocation of the patient” | ||
| Blinding of participants and personnel (performance bias) | High | Quote: “This was a single-blind, prospective, randomized, parallel study…” | ||
| Blinding of outcome assessment (detection bias) | Low | Comment: Although the study is described as single-blind, outcomes data (number of stools and consistency) were collected by parents using a symptom diary | ||
| Incomplete outcome data (attrition bias) | Low | Comment: CONSORT flow diagram and results suggest that all randomized patients were analyzed | ||
| Selective reporting (reporting bias) | Low | Comment: Outcomes were prespecified and analyzed as documented in the ClinicalTrials.gov registry | ||
| Other sources of bias (other bias) | Low | Comment: Limitations and possible sources of bias were addressed in the Discussion section and, apparently, were managed correctly | ||
| Çagan et al. (2017) | Random sequence generation (selection bias) | Unclear | Comment: Despite the study being repeatedly described as randomized, no description of the sequence generation was provided Quote: “Every 2–3 weeks patient numbers were calculated and recruitment adjustments made, if necessary, to try to equalize group numbers” Comment: The above quote raises doubts about the randomness of the treatment allocation process | [21] |
| Allocation concealment (selection bias) | Unclear | Comment: Allocation concealment is not mentioned, and the information provided is insufficient to make a judgement | ||
| Blinding of participants and personnel (performance bias) | Low | Quote: “The study was conducted on a ‘triple-blind’ basis: physicians and nurses did not know whether the study drug administered was placebo or gelatin tannate; patients were not informed about whether they were being given placebo or gelatin tannate; and physicians and nurses did not know from which clinical service each patient had been referred” | ||
| Blinding of outcome assessment (detection bias) | Low | Comment: Although blinding of outcome assessment is not specifically addressed in Methods, we consider detection bias to be unlikely since physicians and nurses were blinded to treatment | ||
| Incomplete outcome data (attrition bias) | Unclear | Comment: A per protocol analysis is reported, after exclusion of 48/251 patients, but no information is provided on per group exclusions (CONSORT flow diagram not provided) | ||
| Selective reporting (reporting bias) | Unclear | Comment: No statement on prespecification of outcomes, and reference to either the study protocol or clinical trial registry is lacking | ||
| Other sources of bias (other bias) | Low | Comment: Study limitations are addressed in the Discussion; no other potential sources of bias were identified by reviewers | ||
| Kara et al. (2017) | Random sequence generation (selection bias) | High | Comment: Despite the study being described as randomized in the Abstract and Methods section, note the following: Quote: “Eligible patients were randomized on the basis of order of presentation, the first to present being included in the patient group, and the second in the control group, etc” Comment: Not properly randomized | [22] |
| Allocation concealment (selection bias) | High | Comment: In view of the comment above, treatment allocation could be expected | ||
| Blinding of participants and personnel (performance bias) | High | Quote: “Single-blinded” Quote: “The care-givers were blinded to the treatment type” | ||
| Blinding of outcome assessment (detection bias) | Unclear | Comment: Relevant information on outcome assessment is unavailable | ||
| Incomplete outcome data (attrition bias) | High | Quote: “Children not complying with the study protocol were excluded” Comment: A flow chart documents 29/100 and 27/100 exclusions after randomization | ||
| Selective reporting (reporting bias) | Unclear | Comment: No information on the protocol or ClinicalTrials.gov (or similar) registry was provided | ||
| Other sources of bias (other bias) | Low | Comment: Limitations and possible sources of bias were addressed in the Discussion section |
Outcomes data from the three clinical studies included in the meta-analysis are summarized in Table 3.
| Study (year) | Number of stools, mean ± SD | Liquid stools (% of patients) | Persistence of diarrhea (% of patients) | Duration of diarrhea (hours), mean ± SD | Ref. | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Time point | GT | Control† | Time point | GT | Control† | Time point | GT | Control† | GT | Control† | ||
| Mennini et al. (2017) | 24 h | 2.9 ± 1.0 | 3.0 ± 1.1 | 24 h | 61.0 | 75.0 | 76.8 ± 19.2 | 108.0 ± 24.0 | [20] | |||
| Çagan et al. (2017) | 12 h | 2.0 ± 2.5 | 3.0 ± 2.5 | 12 h | 59.2 | 77.0 | 12 h | 33.6 | 66.7 | [21] | ||
| Kara et al. (2017) | 12 h | 3.0 ± 1.8 | 3.6 ± 1.9 | 12 h | 83.0 | 91.7 | 42.0 ± 42.0 | 44.0 ± 44.0 | [22] | |||
| 24 h | 41.7 | 67.0 | 24 h | 63.3 | 75.3 | |||||||
†Oral rehydration solution or placebo.
GT: Gelatin tannate; SD: Standard deviation.
Stool frequency
Stool frequency (number of stools) was reported in all three studies, although it was assessed at 24 h in one study [20], and at 12 h in two studies [21,22]. Analysis of the number of stools at 12 h in two RCTs indicated no study heterogeneity (I2 = 0%), and the results obtained under both the fixed effect and random effects models demonstrated a significant treatment effect in favor of GT (p < 0.01 for both models; Figure 2), with a difference in means of -0.8 [-1.2, -0.3] for the fixed effect model.

Figure 2. Stools frequency: mean difference in the number of stools at 12 h in two randomized controlled trials.
CI: Confidence interval; GT: Gelatin tannate; MD: Mean difference; SD: Standard deviation.
Stool consistency
One study [21] reported the percentage of patients with liquid stools at different time points (12, 24 and 48 h), which favored GT at all time points. The relative risk of diarrhea decreased from 0.77 (95% CI: 0.63–0.93) at 12 h, to 0.62 (95% CI: 0.48–0.81) at 24 h and to 0.16 (95% CI: 0.08–0.3) at 48 h.
Patients with diarrhea at 12 or 24 h
Two RCTs reported the number of patients with diarrhea at 12 h [21,22] or at 24 h [20,22]. Neither analysis produced significant results. Analysis of 12 h data showed significant heterogeneity between studies (I2 = 95%; p < 0.01) with a calculated p-value of 0.33 for the overall treatment effect under the random effects model (Figure 3). Analysis of 24 h data showed homogeneity between studies (I2 = 0%) with a calculated p-value of 0.07 for the overall treatment effect under both the fixed effect and random effects models. The calculated RR was 0.84 (95% CI: 0.70–1.01) for both models (Figure 4).

Figure 3. Patients with diarrhea: risk ratio of the proportion of patients with diarrhea at 12 h in two randomized controlled trials.
CI: Confidence interval; GT: Gelatin tannate; RR: Risk ratio.

Figure 4. Patients with diarrhea: risk ratio of the proportion of patients with diarrhea at 24 h in two randomized controlled trials.
CI: Confidence interval; GT: Gelatin tannate; RR: Risk ratio.
Patients with diarrhea or liquid stools at 24 h
As diarrhea and liquid stools are highly related variables, an analysis was conducted on the proportion of patients with diarrhea at 24 h, using liquid stools at 24 h as a proxy for studies in which numbers of patient with diarrhea were not reported. Despite marked heterogeneity between the three studies (I2 = 41%; p = 0.18), both the fixed effect and random effects models indicated a statistically significant treatment effect (p < 0.01) in favor of GT, with a RR = 0.74 (95% CI: 0.63–0.86) for the fixed effect model (Figure 5).
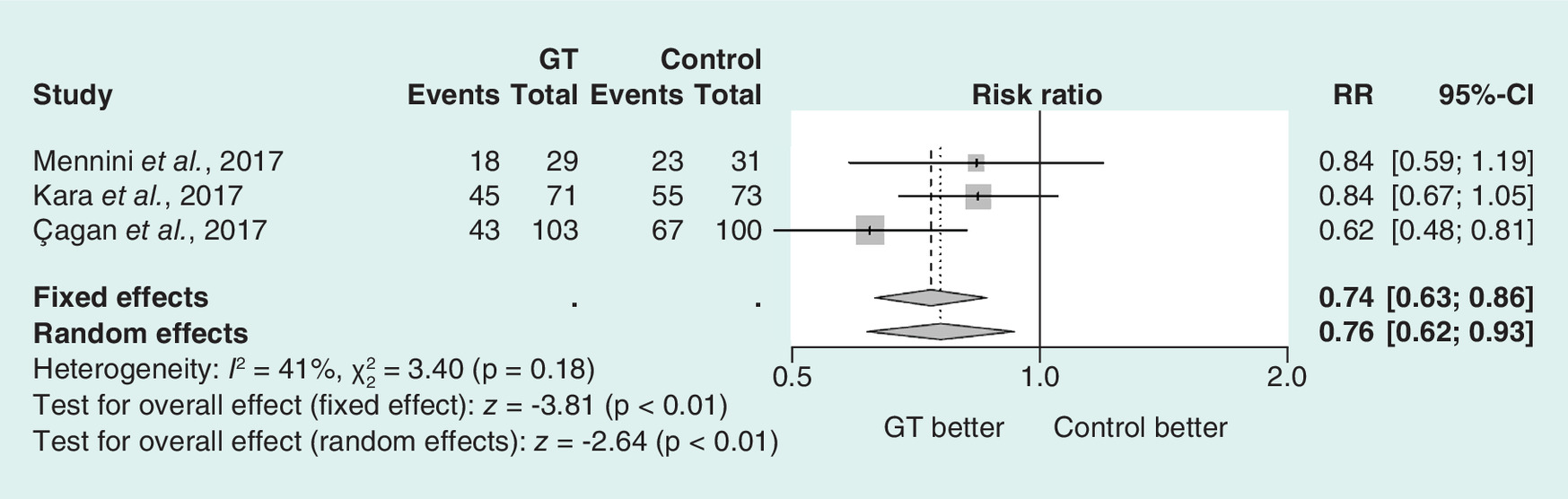
Figure 5. Patients with diarrhea or liquid stools: risk ratio of the proportion of patients with diarrhea or liquid stools at 24 h (composite outcome) in three randomized controlled trials.
CI: Confidence interval; GT: Gelatin tannate; RR: Risk ratio.
Duration of diarrhea
The duration of diarrhea, which was reported in two RCTs [20,22], showed a high degree of heterogeneity (I2 = 90%; p < 0.01), and the random effects model failed to demonstrate a significant treatment effect (p = 0.25), despite an estimated MD of -16.9 h (95% CI: -45.6–11.7) compared with control (Figure 6).

Figure 6. Duration of diarrhea: mean difference of the duration of diarrhea (h) in two randomized controlled trials.
CI: Confidence interval; GT: Gelatin tannate; SD: Standard deviation.
Discussion
Oral rehydration therapy using a hypo-osmolar solution is the mainstay of treatment for acute gastroenteritis in children, and both the duration and severity of diarrhea may be reduced by additional active therapy as required [6]. The meta-analyses conducted here included three RCTs comprising two studies which compared GT + ORS with placebo ± ORS [20,21] and a third study which compared GT and placebo (with no declared ORS) [22].
Meta-analyses demonstrated treatment effects in favor of GT for reduction of stool frequency. Analysis of stool frequency at 12 h in two RCTs showed a significant (p < 0.01) MD of -0.8 in favor of GT compared with control [21,22]. The probability of patients having ‘diarrhea or liquid stools at 24 h’ was significantly lower with GT than placebo (RR = 0.74; p < 0.01) [20 22], although the result can be regarded as exploratory only as this composite outcome was not prespecified but was selected after data extraction in order to maximize the available information. A single study which reported on patients with liquid stools at 12, 24 and 48 h favored GT at all time points, with a consistent pattern of increasing effect (shown by decreasing relative risk) from 12 to 48 h [21].
Conversely, analyses of the proportion of patients with diarrhea at either 12 h or at 24 h, with the study of Kara et al. [22] being common to both, showed no statistically significant differences. Studies which reported on patients with diarrhea at 24 h [20,22] had relatively small sample sizes, with implied low power and imprecision of the estimated overall treatment effect. It is possible that the p-value attained (p = 0.07) in this analysis may have reached statistical significance with larger sample sizes.
The high degree of study heterogeneity evident in two analyses necessitated use of the random effects model. Specifically, there was significant heterogeneity (p < 0.01) between the studies of Çağan et al. and Kara et al. [21,22] for proportion of patients with diarrhea at 12 h, and near-significant heterogeneity (p < 0.06) between the studies of Mennini et al. and Kara et al. [20,22] for duration of diarrhea. Unfortunately, the small number of studies included in the analysis precluded any opportunity to explain heterogeneity through meta-regression.
Although the safety of GT was not formally examined in this meta-analysis, the complex appears to have a good safety profile based on the absence of adverse events reported in any of the three RCTs analyzed [20 22]. This likely reflects its mechanism of action, as GT acts as a mucosal barrier protector and is not systemically absorbed [9 11].
The main limitation of this meta-analysis is the small number of studies and the poor methodological quality of some studies. A degree of caution is advised in interpreting the results as the study of Çagan et al. was not truly randomized, and the study of Kara et al. was limited by a potential high risk of selection, performance and/or attrition bias. Since these analyses were conducted, a fourth RCT investigating GT in the management of acute gastroenteritis in children has been published [29]. This study randomized 72 children to receive GT or placebo as adjunct to ORS for 5 days, and found no significant differences between treatment arms for duration of diarrhea (primary end point) or any other study end point. The reasons for the lack of agreement between this more recent study and previous RCTs are not fully understood. An important methodological difference in Kolodziej et al. was the inclusion of children with diarrhea lasting up to 5 days prior to enrollment compared with 3 days in earlier studies, possibly limiting the ability of GT to show a treatment effect. Although further well-controlled studies are clearly required to reach a definitive conclusion about the efficacy of GT in pediatric acute diarrhea, the bulk of evidence suggests that GT can improve certain symptoms more effectively than control.
European guidelines for the management of acute gastroenteritis in children make several recommendations about adjunctive treatment to ORS. Specifically, the guidelines recommend that selected probiotics, notably Lactobacillus rhamnosus GG and Saccharomyces boulardii, can be used as adjunctive therapy (strong recommendation; low-quality evidence); and indicate that the adsorbent, diosmectite, and antisecretory drug, racecadotril, can be considered in the management of acute gastroenteritis (weak recommendation; moderate-quality evidence) [6], although this latter recommendation has not gained international consensus [30]. The European guidelines, published in 2014, do not recommend GT for the management of children with acute gastroenteritis [6]. However, the strength of this recommendation was assessed as weak, and was based on very low quality evidence from a single publication [13]. In light of more recently published evidence for GT, as analyzed and referenced herein, a re-evaluation of the role of GT in the management of acute gastroenteritis in children would be timely. Three of four RCTs indicate that GT, as adjunct to ORS, can improve symptoms of acute diarrhea and has a good safety profile in young children.
Conclusion
The multiple meta-analyses conducted in this study show that GT can improve symptoms of acute diarrhea in young children as evidenced by significant reductions in stool frequency at 12 h, and in the proportion of patients with a composite outcome of diarrhea or liquid stools at 24 h. One study showed improvement in stool consistency with GT versus placebo over time. A trend in favor of GT was observed in the meta-analyses of stool frequency at 12 or 24 h and duration of diarrhea, but high study heterogeneity and/or small sample sizes likely limited the power of the analyses to show a treatment effect. Although the quality of the included studies was not high, collectively the results suggest benefit with GT in attenuating the symptoms of acute diarrhea in children.
GT is known to form a biofilm in the gastrointestinal mucosa, providing mechanical protection and causing precipitation of proinflammatory proteins [31]. This unique mechanism, together with the lack of systemic absorption of GT, make this device an interesting addition to the current armamentarium for treating acute gastroenteritis in children. In light of a recent RCT failing to show benefit versus placebo, further studies would be useful to confirm the efficacy of GT in this clinical setting.
In Europe, acute gastroenteritis is the most common cause of primary care consultations among children less than 5 years of age.
Gelatin tannate (GT), a mucosal barrier protector, is a new therapeutic option for treating acute gastroenteritis and diarrhea.
A systematic review identified three published randomized controlled trials (RCTs) of pediatric diarrhea treated with GT (n = 203) or control (n = 204).
Meta-analyses showed that GT was effective in reducing symptoms in children with acute diarrhea.
GT reduced stool frequency at 12 h in two RCTs (p < 0.01).
GT reduced the composite outcome of diarrhea or liquid stools at 24 h in all three studies (risk ratio [RR] = 0.74; p < 0.01).
A single study which reported the proportion of patients with liquid stools at 12 (RR = 0.77), 24 (RR = 0.62) and 48 (RR = 0.16) h favored GT at all time points.
GT did not differ significantly from control for proportion of patients with diarrhea at either 12 or 24 h or for duration of diarrhea.
No adverse events were reported in any of the RCTs analyzed.
The unique mechanism and lack of systemic absorption of GT make this device an interesting addition to the current armamentarium for treating acute gastroenteritis in children, although further studies are needed to confirm a beneficial treatment effect.
Author contributions
M Aloi and M Mennini were involved in the conception and design of the study, in the analysis and interpretation of the data; in the drafting of the paper or revising it critically for intellectual content; and in the final approval of the version to be published. All authors agree to be accountable for all aspects of the work.
Financial & competing interests disclosure
This meta-analysis was realized with the support of Noventure S.L. (Barcelona, Spain). The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing assistance was provided by Content Ed Net (Madrid, Spain), with funding from Noventure S.L (Barcelona, Spain).
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Keusch GT, Fontaine O, Bhargava A et al. Diarrheal diseases. In: Disease Control Priorities in Developing Countries (2nd Edition). Jamison DT, Breman JG, Measham AR et al. (Eds). The International Bank for Reconstruction and Development/The World Bank, Washington, DC, USA; Oxford University Press, NY, USA (2006).
2.
Global Burden of Disease Study 2013 Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet 386(9995), 743–800 (2015).
3.
Global Burden of Disease Pediatrics Collaboration, Kyu HH, Pinho C et al. Global and national burden of diseases and injuries among children and adolescents between 1990 and 2013: findings from the Global Burden of Disease 2013 Study. JAMA Pediatr. 170(3), 267–287 (2016).
4.
van Damme P, Giaquinto C, Huet F et al. Multicenter prospective study of the burden of rotavirus acute gastroenteritis in Europe, 2004–2005: the REVEAL study. J. Infect. Dis. 195(Suppl. 1), S4–S16 (2007).
5.
Platts-Mills JA, Babji S, Bodhidatta L et al. Pathogen-specific burdens of community diarrhoea in developing countries: a multisite birth cohort study (MAL-ED). Lancet Glob. Health 3, e564–e575 (2015).
6.
Guarino A, Ashkenazi S, Gendrel D, Lo Vecchio A, Shamir R, Szajewska H. European Society for Pediatric Gastroenterology, Hepatology, and Nutrition; European Society for Pediatric Infectious Diseases. European Society for Pediatric Gastroenterology, Hepatology, and Nutrition/European Society for Pediatric Infectious Diseases evidence-based guidelines for the management of acute gastroenteritis in children in Europe: update 2014. J. Pediatr. Gastroenterol. Nutr. 59(1), 132–152 (2014).
•• Current European guidelines for management of acute gastroenteritis in children.
7.
Wiegering V, Kaiser J, Tappe D, Weissbrich B, Morbach H, Girschick HJ. Gastroenteritis in childhood: a retrospective study of 650 hospitalized pediatric patients. Int. J. Infect. Dis. 15, e401–e407 (2011).
8.
Ogilvie I, Khoury H, Goetghebeur MM, El Khoury AC, Giaquinto C. Burden of community-acquired and nosocomial rotavirus gastroenteritis in the pediatric population of Western Europe: a scoping review. BMC Infect. Dis. 12, 62 (2012).
9.
Ruszczyński M, Urbańska M, Szajewska H. Gelatin tannate for treating acute gastroenteritis: a systematic review. Ann. Gastroenterol. 27, 121–124 (2014).
10.
Lopetuso LR, Scaldaferri F, Bruno G, Petito V, Franceschi F, Gasbarrini A. The therapeutic management of gut barrier leaking: the emerging role for mucosal barrier protectors. Eur. Rev. Med. Pharmacol. Sci. 19(6), 1068–1076 (2015).
11.
Lopetuso L, Graziani C, Guarino A, Lamborghini A, Masi S, Stanghellini V. Gelatin tannate and tyndallized probiotics: a novel approach for treatment of diarrhea. Eur. Rev. Med. Pharmacol. Sci. 21(4), 873–883 (2017).
12.
Allegrini A, Costantini M. Gelatine tannate for the treatment of acute diarrhoea in adults. J. Gastroint. Dig. Syst. 2, 3 (2012).
13.
Esteban Carretero J, Durbán Reguera F, López-Argüeta Alvarez S, López Montes J. A comparative analysis of response to vs. ORS + gelatin tannate pediatric patients with acute diarrhea. Rev. Esp. Enferm. Dig. 101(1), 41–48 (2009).
• This cohort study compared gelatin tannate + oral rehydration solution (ORS) versus ORS.
14.
PubMed.gov. Bethesda, MD, USA: U.S. National Library of Medicine; National Institutes of Health. www.ncbi.nlm.nih.gov/pubmed.
15.
Google Académico. Mountain View, CA USA: Google LLC. http://scholar.google.es.
16.
La Biblioteca Cochrane Plus. London, UK: John Wiley & Sons, Inc. www.bibliotecacochrane.com/.
17.
ClinicalTrials. gov. Bethesda, MD, USA: U.S. National Library of Medicine; National Institutes of Health. https://clinicaltrials.gov/.
18.
EU Clinical Trials Register. London, UK: European Medicines Agency. www.clinicaltrialsregister.eu/.
19.
Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA Statement. Open Med. 3, e123–e130 (2009).
20.
Mennini M, Tolone C, Frassanito A, Midulla F, Cucchiara S, Aloi M. Gelatin tannate for acute childhood gastroenteritis: a randomized, single-blind controlled trial. Paediatr. Drugs 19(2), 131–137 (2017).
•• This single-blind randomized controlled trial (RCT) compared gelatin tannate + ORS versus ORS.
21.
Çağan E, Ceylan S, Mengi S, Çağan HH. Evaluation of gelatin tannate against symptoms of acute diarrhea in pediatric patients. Med. Sci. Monit. 23, 2029–2034 (2017).
•• This double-blind RCT compared gelatin tannate + ORS versus placebo + ORS.
22.
Kara SS, Volkan B, Erten I. The therapeutic effect of gelatin tannate in acute diarrhea in children. Turk J. Pediatr. 59(5), 531–536 (2017).
•• This single-blind RCT compared gelatin tannate versus placebo.
23.
Michałek D, Kołodziej M, Konarska Z, Szajewska H. Efficacy and safety of gelatine tannate for the treatment of acute gastroenteritis in children: protocol of a randomised controlled trial. BMJ Open 6(2), e010530 (2016).
24.
Clinical trials database. Bethesda, MD, USA: U.S. National Library of Medicine; National Institutes of Health. NCT02280759 (2014). https://clinicaltrials.gov/ct2/show/NCT02280759
25.
WebPlotDigitizer, 2017. Oakland, CA, USA: Ankit Rohatgi (2016). https://automeris.io/WebPlotDigitizer/
26.
R Core Team. R: a language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria (2017). www.R-project.org/
27.
Schwarzer G meta: an R package for meta-analysis. R News 7(3), 40–45 (2007). http://bioconductor.statistik.tu-dortmund.de/cran/doc/Rnews/Rnews_2007-3.pdf#page=40
28.
Schiller LR, Pardi DS, Spiller R et al. Gastro 2013 APDW/WCOG Shanghai working party report: chronic diarrhea: definition, classification, diagnosis. J. Gastroenterol. Hepatol. 29(1), 6–25 (2014).
29.
Kołodziej M, Bebenek D, Konarska Z, Szajewska H. Gelatine tannate in the management of acute gastroenteritis in children: a randomised controlled trial. BMJ Open 8(5), e020205 (2018).
•• Most recent RCT comparing gelatin tannate versus placebo in patients with acute gastoenteritis.
30.
Guarino A, Lo Vecchio A, Dias JA et al. Universal recommendations for the management of acute diarrhea in non-malnourished children. J. Pediatr. Gastroenterol. Nutr. 67(5), 586–593 (2018).
31.
Chung KT, Stevens SE, Jr, Lin WF, Wei CI. Growth inhibition of selected food-borne bacteria by tannic acid, propyl gallate and related compounds. Lett. Appl. Microbiol. 17, 29–32 (1993).
Information & Authors
Information
Published In
Copyright
© 2018 Future Medicine Ltd.
History
Received: 23 October 2018
Accepted: 5 November 2018
Published online: 22 November 2018
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Efficacy of gelatin tannate for acute diarrhea in children: a systematic review and meta-analysis. (2018) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2018-0115
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Francesco Rettura, Christian Lambiase, Riccardo Tedeschi, Antonio Grosso, Lorenzo Cancelli, Angelo Ricchiuti, Andrea Bottari, Luca Giacomelli, Nicola de Bortoli, Massimo Bellini, Mucoprotectants and gut barrier: mechanisms of action and clinical applications in IBS. Is there a possible role?, Frontiers in Pharmacology, 10.3389/fphar.2025.1538791, 16, (2025).
- Andera Salama-Müller, Nadine Roese, Antidiarrheal Properties of the Combination of Tannin Albuminate and Ethacridine Lactate - A Narrative Review, Natural Product Communications, 10.1177/1934578X231170998, 18, 5, (2023).
- Vilma Vranová, Karel Vašut, Pharmacotherapy of infectious diarrhoea, Farmacie pro praxi, 10.36290/lek.2023.008, 19, 1, (51-62), (2023).
- Hélène Eutamene, Catherine Beaufrand, Cherryl Harkat, Vassilia Theodorou, Effect of Two Mucoprotectants, Gelatin Tannate and Xyloglucan plus Gelatin, on Cholera Toxin-Induced Water Secretion in Rats, Gastrointestinal Disorders, 10.3390/gidisord4040030, 4, 4, (324-332), (2022).
- Martin Gregora, Self-treatment of diarrheal diseases in children - what to recommend in the pharmacy, Praktické lékárenství, 10.36290/lek.2022.019, 18, 2, (92-95), (2022).
- E. R. Meskina, A. Yu. Ushakova, M. K. Khadisova, T. V. Stashko, A. N. Antonenko, The efficacy and safety of the cytomucoprotector gelatin tannate in the treatment of acute gastroenteritis in children, Meditsinskiy sovet = Medical Council, 10.21518/2079-701X-2021-17-163-173, 17, (163-173), (2021).
- Marina Fortea, Mercé Albert-Bayo, Mar Abril-Gil, John-Peter Ganda Mall, Xavier Serra-Ruiz, Alejandro Henao-Paez, Elba Expósito, Ana María González-Castro, Danila Guagnozzi, Beatriz Lobo, Carmen Alonso-Cotoner, Javier Santos, Present and Future Therapeutic Approaches to Barrier Dysfunction, Frontiers in Nutrition, 10.3389/fnut.2021.718093, 8, (2021).
- Martin Gregora, Common and rare complications of gastroenteitis, Pediatrie pro praxi, 10.36290/ped.2021.023, 22, 2, (125-128), (2021).
- Carmen Alonso-Cotoner, Mar Abril-Gil, Mercé Albert-Bayo, John-P. Ganda Mall, Elba Expósito, Ana M. González-Castro, Beatriz Lobo, Javier Santos, The Role of Purported Mucoprotectants in Dealing with Irritable Bowel Syndrome, Functional Diarrhea, and Other Chronic Diarrheal Disorders in Adults, Advances in Therapy, 10.1007/s12325-021-01676-z, 38, 5, (2054-2076), (2021).
- Javier Santos, Virgil Musta, Catalina Mihaela Luca, Oana Andreea Belei, Simona Claudia Cambrea, Randomized, placebo-controlled trial of xyloglucan and gelose for the treatment of acute diarrhea in children, Expert Review of Gastroenterology & Hepatology, 10.1080/17474124.2021.1833715, 15, 3, (325-331), (2020).