Gastrointestinal complications in patients treated with ipilimumab and nivolumab combination therapy or monotherapy
Abstract
Aim & methods: A retrospective study using the IBM Explorys Universe Database assessed the risk of gastrointestinal events (enterocolitis or diarrhea) among melanoma and lung cancer patients treated with ipilimumab and nivolumab combination or monotherapy. Results & conclusion: There were 904 melanoma patients (607 ipilimumab, 140 nivolumab and 157 combo) and 1641 lung cancer patients (68 ipilimumab, 1542 nivolumab and 31 combo). Approximately, 37% of lung patients and 46% of melanoma patients experienced at least one adverse event. After adjusting for covariates, patients receiving combination therapy were more likely to have a gastrointestinal event compared with ipilimumab monotherapy patients (melanoma hazard ratio: 1.54; 95% CI: 1.06–2.25; lung hazard ratio: 2.93; 95% CI: 1.09–7.89).
Recent advances in cancer therapy have focused on enhancing the immune response through inhibition of immune checkpoint proteins including cell surface receptors CTLA-4 and PD-1 [1]. Although many questions remain, it is believed that CTLA-4 and PD-1 play complementary roles in suppressing autoreactive T-cells at different stages of the immune response [2–4]. Enhancing the immune response by blocking these pathways with monoclonal antibodies is proving to be a novel and effective way to treat a variety of aggressive and otherwise refractory malignancies, such as metastatic melanoma and advanced lung cancer [5].
Metastatic melanoma is an aggressive disease with a 5-year relative survival rate of 20% based on Surveillance, Epidemiology and End Results data from 2007 to 2013 [6]. This survival rate has been improving over time, in part due to the introduction of immune checkpoint inhibitors, such as ipilimumab for CTLA-4 and nivolumab for PD-1 [6–9]. In addition to working independently, early evidence has shown that inhibition of CLTA-4 and PD-1 has synergistic effects, and early results from Phase II and Phase III trials of nivolumab plus ipilimumab in patients with advanced melanoma have shown increased progression-free survival and higher overall survival (OS) rates in patients treated with the combination compared with ipilimumab alone [10,11].
Since 2014, nivolumab has been approved for the treatment of a number of malignancies – including non-small-cell lung cancer, colorectal cancer and hepatocellular cancer – which have proven intractable to the classic modalities of cancer therapy: surgery, radiation and chemotherapy [12–14]. New approaches to lung cancer treatment are of particular interest, as it remains the leading cause of cancer-related deaths due its high incidence (estimated 234,030 new cases in 2018) and poor prognosis (5-year survival of 5%) [6]. Nivolumab has been shown to improve median OS compared with docetaxel with fewer treatment-related Grade 3 or 4 adverse events (AEs) in both squamous and nonsquamous non-small-cell lung cancer, and there are efforts to improve survival further with the addition of ipilimumab [14–16].
However, these immunotherapies are not without risks; specifically, by dysregulating the process which normally prevents autoimmune reactions, use of these agents can result in immune-related adverse events (IRAEs) including diarrhea, colitis, hepatitis and hypophysitis [17,18]. One study, which used aggregated safety data of clinical trials in melanoma, reported IRAE frequencies of 62.0, 73.2 and 87.9% for nivolumab, ipilimumab and combination therapy, respectively [19]. Severe grade 3 and 4 AEs, which are most likely to lead to discontinuation, were most common for the combination therapy and predominately impacted the gastrointestinal (GI) and hepatic systems [19,20]. Current first-line treatment for IRAEs involves delay or discontinuation of the immunotherapy and administration of corticosteroids [21,22]. For those who can restart treatment, the use of immunosuppressants does not appear to reduce OS; however, many patients, particularly those with GI complications, do not restart therapy [23]. Gastrointestinal complications have been found to be one of the most common reasons for discontinuation of checkpoint inhibitor therapies [18]
With the combined targeting of PD-1 and CTLA-4 growing in usage [24–26], it is critical to obtain a better understanding of the frequency and severity of IRAEs. Current data on the frequency IRAEs are limited to clinical trials, single-site reports and the US FDA Adverse Event Reporting System [19,20,23]. This retrospective cohort study uses electronic medical records (EMRs) to examine the real-world rate of AEs including IRAEs and other GI AEs in patients with advanced melanoma or lung cancer treated with nivolumab, ipilimumab or combination therapy.
Methods
Data source
This study utilized patient-level deidentified US EMR data from the IBM Explorys Universe Dataset (Explorys; IBM, NY, USA) for the period from 1 September 2010 to 8 May 2017. Explorys contains data for approximately 55 million patients (∼15% of the US population) derived from integrated data networks across 23 large health systems, comprising approximately 360 hospitals and 330,000 providers. The data provide a full longitudinal view of a patient's medical history across the care continuum, including diagnoses, procedures and medications.
Study design & patient selection
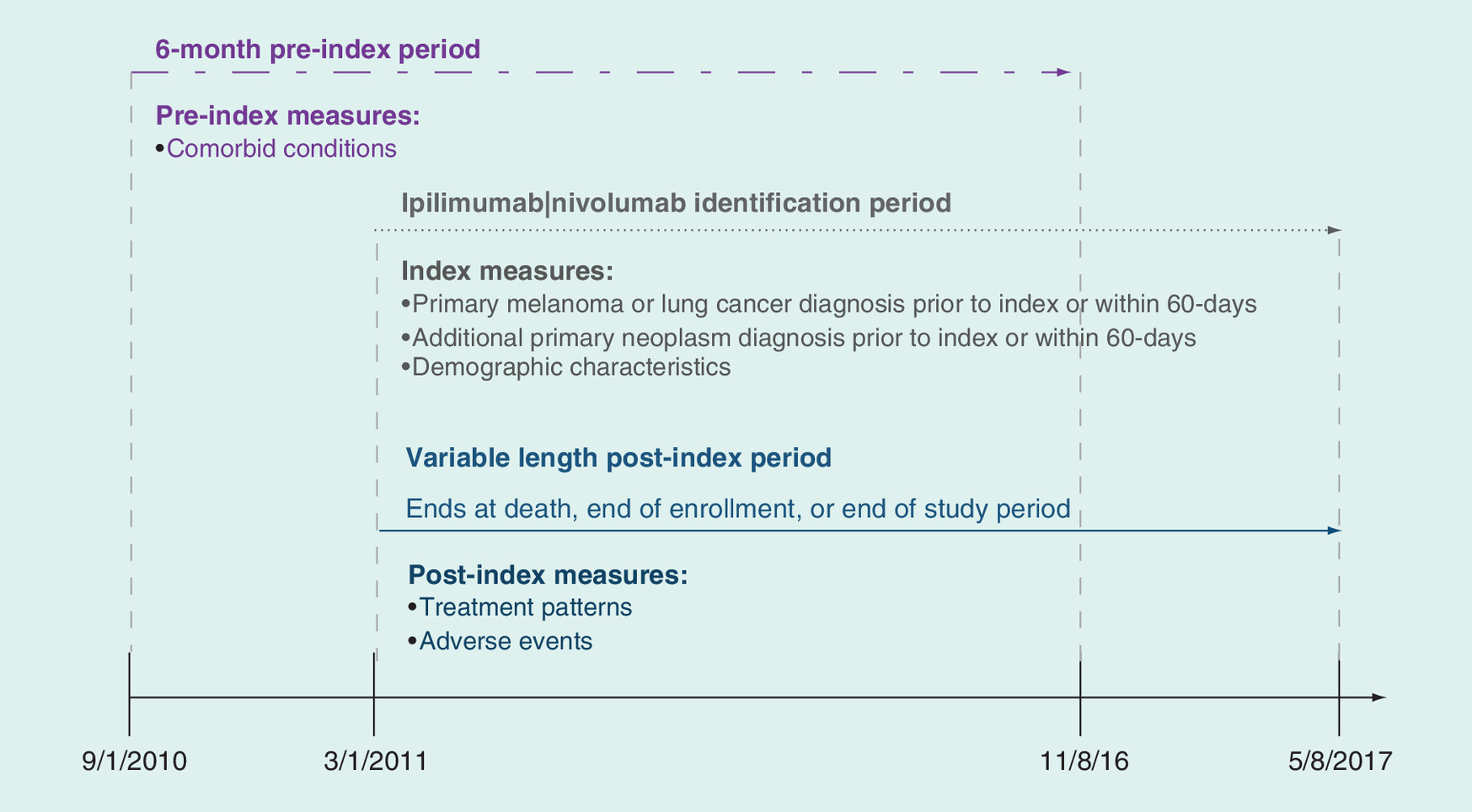
This retrospective longitudinal observational cohort study used a large real-world EMR database to evaluate the rate of GI events among melanoma and lung cancer patients treated with ipilimumab, nivolumab or ipilimumab/nivolumab combination (combo) therapy. Patients were included if they had at least one prescription for ipilimumab or nivolumab between 1 March 2011 and 8 May 2017. The date of the earliest prescription was defined as the index date, and patients were required to be at least 18 years of age on the index date. Any patients with a diagnosis of metastatic melanoma or lung cancer prior to or within 60 days after of the index date were included in the study. Each cancer cohort (melanoma or lung) was then separated into three treatment subcohorts (ipilimumab, nivolumab or combo) based on the index checkpoint inhibitor therapy. The analysis period for each patient was from 6 months preindex until the end of data availability due to patient death, end of EMR enrollment or end of the study period (Figure 1).
Baseline characteristics
Patient demographics were measured on the index date and included age, gender, race, smoking status, BMI and index year. Racial categories were Caucasian, African–American, Hispanic, other and unknown.
Primary cancer diagnosis was captured during the 6-month preindex period and the first 60 days postindex. The National Cancer Institute (NCI) modification of the Deyo Charlson Comorbidity Index (DCCI) was calculated for the 6-month preindex period [27,28]. Comorbidities of interest were captured during the preindex period and included cerebrovascular disease, cardiac dysrhythmia, chronic obstructive pulmonary disorder, congestive heart failure, Crohn's disease, dementia, depression, hemiplegia or paraplegia, HIV infection, hypertension, hypotension, ischemic heart disease, liver disease, myocardial infarction, peptic ulcer, peripheral vascular disease, renal disease, rheumatologic disease, Type 2 diabetes mellitus and ulcerative colitis.
Outcomes
The index treatment regime began on the index date and comprised all agents prescribed within 28 days of the index date. The duration of therapy was calculated from the index date to the earliest of the following: addition of a new agent after 28 days; a gap of 60 days or more following the last administration of either nivolumab or ipilimumab; death recorded in Explorys or end of study period (8 May 2017). In addition to duration of therapy, the number, type and name of all systemic agents in the index treatment regime were recorded. Systemic agents captured in addition to ipilimumab and nivolumab included targeted therapies (cobimetinib, dabrafenib, trametinib and vemurafenib), immunotherapies (granulocyte-macrophage colony-stimulating factor, IL-2, IL α-2b and pembrolizumab), chemotherapeutic agents (carboplatin, carmustine, cisplatin, dacarbazine, docetaxel, paclitaxel, temozolomide and vinblastine) and immunosuppressants (corticosteroids and adalimumab).
The incidence of GI AEs was calculated for the duration of the index treatment regime. Only new events (i.e., events not present in the 6-month preindex period) were included in the analysis. These events included abdominal cramping/pain, anorexia, constipation, diarrhea, dyspepsia, enterocolitis, gingivitis, mucositis, nausea/vomiting and pancreatitis
Statistical analysis
The count and percentage of patients in each treatment cohort were calculated for categorical variables. The mean and standard deviation was calculated for continuous variables. Association between index treatment regimen (ipilimumab, nivolumab or combo) and the risk of incident GI complications (enterocolitis or diarrhea) was assessed using Cox proportional hazard models to control for baseline demographic and clinical characteristics. Separate models were built for the lung cancer and melanoma cohorts. The vector of covariates included in both models included age, sex, BMI, NCI DCCI, preindex neutropenia or leukopenia, preindex GI symptoms of nausea, vomiting, abdominal cramping/pain and constipation. Hazard ratios were computed for each variable and Kaplan–Meier curves were prepared for each treatment subcohort. The α level for all statistical analysis was set a priori at 0.05. Data management and statistical analyses were conducted using SAS software, version 9.4 (SAS Institute Inc, NC, USA).
Results
Patient identification & demographic characteristics
During the identification period, 2545 metastatic melanoma and lung cancer patients were treated with nivolumab or ipilimumab, and, of these, 53.7% had a diagnosis of metastatic lung cancer and 29.6% had a diagnosis of metastatic melanoma. Baseline demographic characteristics by treatment subcohort within each diagnosis cohort are reported in Table 1. Patients in the lung cancer cohort had a mean age of 67.3 ± 10.3 years: 55% were male, 82% were Caucasian, 16% were current smokers and the average BMI was 22.8 ± 9.7. There was no substantial difference between treatment subcohorts. Patients in the melanoma cohort had a mean age of 63.5 ± 13.8 years: 65% were male, 93% were Caucasian, 9% were current smokers and the average BMI was 22.8 ± 12.7. Patients on nivolumab tended to be older (62.4 ± 13.5 years ipilimumab vs 70.8 ± 13.1 years nivolumab vs 61.0 ± 13.8 combo), but otherwise, the three treatment subcohorts were similar.
| Lung cancer | Melanoma | |||||
|---|---|---|---|---|---|---|
| Ipilimumab | Nivolumab | Combo | Ipilimumab | Nivolumab | Combo | |
| n = 68 | n = 1542 | n = 31 | n = 607 | n = 14 | n = 157 | |
| Age, mean ± SD | 64.8 ± 12.7 | 67.5 ± 10.2 | 64.2 ± 11.0 | 62.4 ± 13.5 | 70.8 ± 13.1 | 60.0 ± 13.8 |
| Male, n (%) | 42 (61.8) | 844 (54.7) | 18 (58.1) | 381 (62.8) | 98 (70.0) | 111 (70.7) |
| Race/ethnicity, n (%) | ||||||
| – Caucasian | 61 (89.7) | 1262 (81.8) | 27 (87.1) | 561 (92.4) | 127 (90.7) | 152 (96.8) |
| – African–American | 3 (4.4) | 153 (9.9) | 0 (0.0) | 6 (1.0) | 3 (2.1) | 0 (0.0) |
| – Hispanic | 0 (0) | 4 (0.3) | 0 (0.0) | 1 (0.2) | 0 (0.0) | 0 (0.0) |
| – Other | 0 (0) | 47 (3.0) | 0 (0.0) | 8 (1.3) | 1 (0.7) | 1 (0.6) |
| – Unknown | 4 (5.9) | 76 (4.9) | 4 (12.9) | 31 (5.1) | 9 (6.4) | 4 (2.5) |
| Current smoker, n (%) | 7 (10.3) | 259 (16.8) | 3 (9.7) | 52 (8.6) | 14 (10.0) | 15 (9.6) |
| BMI, mean ± SD | 23.6 ± 11.6 | 22.7 ± 9.6 | 24.4 ± 9.6 | 22.3 ± 13.4 | 22.3 ± 11.2 | 25.2 ± 11.1 |
| NCI modified DCCI‡, mean ± SD | 0.7 ± 1.1 | 0.8 ± 1.0 | 0.4 ± 0.6 | 0.4 ± 0.8 | 0.6 ± 1.0 | 0.4 ± 0.7 |
| General comorbidities†‡, n (%) | ||||||
| – Cerebrovascular disease | 7 (10.3) | 123 (8.0) | 2 (6.5) | 56 (9.2) | 15 (10.7) | 12 (7.6) |
| – Cardiac dysrhythmia | 11 (16.2) | 152 (9.9) | 5 (16.1) | 62 (10.2) | 19 (13.6) | 7 (4.5) |
| – Chronic obstructive pulmonary disorder | 17 (25.0) | 649 (42.1) | 6 (19.4) | 75 (12.4) | 25 (17.9) | 22 (14.0) |
| – Congestive heart failure | 6 (8.8) | 118 (7.7) | 0 (0.0) | 27 (4.4) | 13 (9.3) | 3 (1.9) |
| – Crohn's disease | 0 (0.0) | 1 (0.1) | 0 (0.0) | 0 (0.0) | 1 (0.7) | 0 (0.0) |
| – Dementia | 0 (0.0) | 8 (0.5) | 0 (0.0) | 5 (0.8) | 5 (3.6) | 1 (0.6) |
| – Depression | 6 (8.8) | 204 (13.2) | 3 (9.7) | 51 (8.4) | 10 (7.1) | 17 (10.8) |
| – Hypertension | 38 (55.9) | 685 (44.4) | 15 (48.4) | 233 (38.4) | 78 (55.7) | 59 (37.6) |
| – Hypotension | 3 (4.4) | 19 (1.2) | 0 (0.0) | 6 (1.0) | 2 (1.4) | 3 (1.9) |
| – Ischemic heart disease | 10 (14.7) | 262 (17.0) | 5 (16.1) | 64 (10.5) | 26 (18.6) | 18 (11.5) |
| – Liver disease | 0 (0.0) | 30 (1.9) | 0 (0.0) | 7 (1.2) | 1 (0.7) | 0 (0.0) |
| – Peripheral vascular disease | 2 (2.9) | 245 (15.9) | 4 (12.9) | 34 (5.6) | 17 (12.1) | 12 (7.6) |
| – Renal disease | 4 (5.9) | 138 (8.9) | 1 (3.2) | 23 (3.8) | 17 (12.1) | 5 (3.2) |
| – Rheumatologic disease | 1 (1.5) | 32 (2.1) | 0 (0.0) | 14 (2.3) | 4 (2.9) | 2 (1.3) |
| – Type 2 diabetes mellitus | 10 (14.7) | 231 (15.0) | 3 (9.7) | 86 (14.2) | 24 (17.1) | 13 (8.3) |
| – Ulcerative colitis | 1 (1.5) | 3 (0.2) | 0 (0.0) | 2 (0.3) | 2 (1.4) | 0 (0.0) |
†The following general comorbidities were evaluated but occurred in less than 3% of any cohort: hemiplegia or paraplegia, HIV infection, myocardial infarction, peptic ulcer.
‡Measured during the 6-month preindex period.
BMI: Body mass index; DCCI: Deyo Charlson Comorbidity Index; NCI: National Cancer Institute; SD: Standard deviation.
Clinical characteristics
Clinical characteristics from the preindex period are reported in Table 1. Approximately 10–20% of patients had at least two primary cancer diagnosis in their EMR record. On average, the NCI DCCI was below 1.0 for both lung cancer patients (0.7 ± 1.1 ipilimumab vs 0.8 ± 1.0 nivolumab vs 0.4 ± 0.6 combo) and melanoma patients (0.4 ± 0.8 ipilimumab vs 0.6 ± 1.0 nivolumab vs 0.4 ± 0.7 combo). The top five comorbid conditions, in order of percentage of patients diagnosed, were hypertension (38−56%), chronic obstructive pulmonary disorder (12–42%), ischemic heart disease (11−19%), Type 2 diabetes mellitus (8−17%) and cardiac dysrhythmia (5−16%). Among lung cancer patients, the mean duration of time on therapy was 117.9 ± 216.8 days for the ipilimumab subcohort, 138.1 ± 145.1 days for the nivolumab subcohort and 112.4 ± 95.8 days for the combination drug subcohort; among melanoma patients, the mean duration of time on therapy was 107.2 ± 174.7 days for the ipilimumab subcohort, 120.8 ± 138.2 days for the nivolumab subcohort and 129.2 ± 126.5 days for the combination drug subcohort (data not shown).
Adverse events
New incident events of GI diagnoses were common during the index therapy regime (Table 2). At least 30% of patients in any subcohort had one or more AEs with similar treatment-related trends in both the lung cancer (63.2% ipilimumab vs 35.7% nivolumab vs 41.9% combo) and melanoma (49.3% ipilimumab vs 32.9% nivolumab vs 44.6% combo) cohorts. The four most common incidence of AEs – by rate per 1000 person-years, for all subcohorts, regardless of diagnosis – were abdominal cramping/pain (lung cancer: 134.6 ipilimumab vs 148.9 nivolumab vs 291.5 combo; melanoma: 133.3 ipilimumab vs 175.8 nivolumab vs 208.3 combo), constipation (lung cancer: 141.0 ipilimumab vs 226.7 nivolumab vs 312.1 combo; melanoma: 111.6 ipilimumab vs 228.8 nivolumab vs 189.1 combo), diarrhea (lung cancer: 172.4 ipilimumab vs 104.1 nivolumab vs 327.3 combo; melanoma: 160.7 ipilimumab vs 194.1 nivolumab vs 371.3 combo) and nausea/vomiting (lung cancer: 300.0 ipilimumab vs 202.9 nivolumab vs 608.1 combo; melanoma: 187.0 ipilimumab vs 236.8 nivolumab vs 415.3 combo). The unadjusted rate of enterocolitis (per 1000 person-years) was lowest among patients on nivolumab and highest for those on combination therapy for both lung cancer (86.6 ipilimumab vs 50.9 nivolumab vs 112.5 combo) and melanoma (96.7 ipilimumab vs 90.1 nivolumab vs 166.6 combo). The time to first diarrhea or enterocolitis diagnosis during the treatment regimen is depicted in Figure 2. These AEs occurred significantly earlier for the combination treatment compared with the ipilimumab or nivolumab monotherapy (mean time to first diarrhea event lung cancer: ipilimumab 354 days, nivolumab 145 days, combo 138 days; melanoma diarrhea: ipilimumab 196 days, nivolumab 120 days, combo 119 days; lung cancer enterocolitis: ipilimumab 314 days, nivolumab 152 days, combo 106 days; melanoma enterocolitis: ipilimumab 169 days, nivolumab 156 days, combo 75 days).
| Incidence of adverse events | Lung cancer | Melanoma | ||||
|---|---|---|---|---|---|---|
| Ipilimumab | Nivolumab | Combo | Ipilimumab | Nivolumab | Combo | |
| n = 68 | n = 1542 | n = 31 | n = 607 | n = 140 | n = 157 | |
| Abdominal cramping/pain, n (%) | 11 (16.2) | 146 (9.5) | 5 (16.1) | 100 (16.5) | 15 (10.7) | 21 (13.4) |
| Rate of abdominal cramping/pain† | 134.6 | 148.9 | 291.5 | 133.3 | 175.8 | 208.3 |
| Anorexia, n (%) | 8 (11.8) | 140 (9.1) | 2 (6.5) | 58 (9.6) | 12 (8.6) | 13 (8.3) |
| Rate of anorexia† | 85.5 | 140.4 | 113.5 | 68.5 | 130.1 | 124.3 |
| Constipation, n (%) | 13 (19.1) | 215 (13.9) | 5 (16.1) | 91 (15.0) | 20 (14.3) | 19 (12.1) |
| Rate of constipation† | 141 | 226.7 | 312.1 | 111.6 | 228.8 | 189.1 |
| Diarrhea, n (%) | 15 (22.1) | 104 (6.7) | 5 (16.1) | 122 (20.1) | 16 (11.4) | 33 (21) |
| Rate of diarrhea† | 172.4 | 104.1 | 327.3 | 160.7 | 194.1 | 371.3 |
| Dyspepsia, n (%) | 4 (5.9) | 26 (1.7) | 2 (6.5) | 19 (3.1) | 4 (2.9) | 5 (3.2) |
| Rate of dyspepsia† | 41.2 | 24.4 | 120 | 21.5 | 43 | 46.5 |
| Enterocolitis, n (%) | 8 (11.8) | 53 (3.4) | 2 (6.5) | 80 (13.2) | 8 (5.7) | 17 (10.8) |
| Rate of enterocolitis† | 87.1 | 50.9 | 112.5 | 96.7 | 90.1 | 166.6 |
| Nausea/vomiting, n (%) | 24 (35.3) | 189 (12.3) | 8 (25.8) | 138 (22.7) | 20 (14.3) | 37 (23.6) |
| Rate of nausea/vomiting† | 300 | 202.9 | 608.1 | 187 | 236.8 | 415.3 |
| Pancreatitis, n (%) | 4 (5.9) | 15 (1.0) | 0 (0.0) | 14 (2.3) | 0 (0.0) | 2 (1.3) |
| Rate of pancreatitis† | 40.3 | 14.1 | 0 | 15.8 | 0 | 18 |
†per 1000 person years.
SD: Standard deviation.
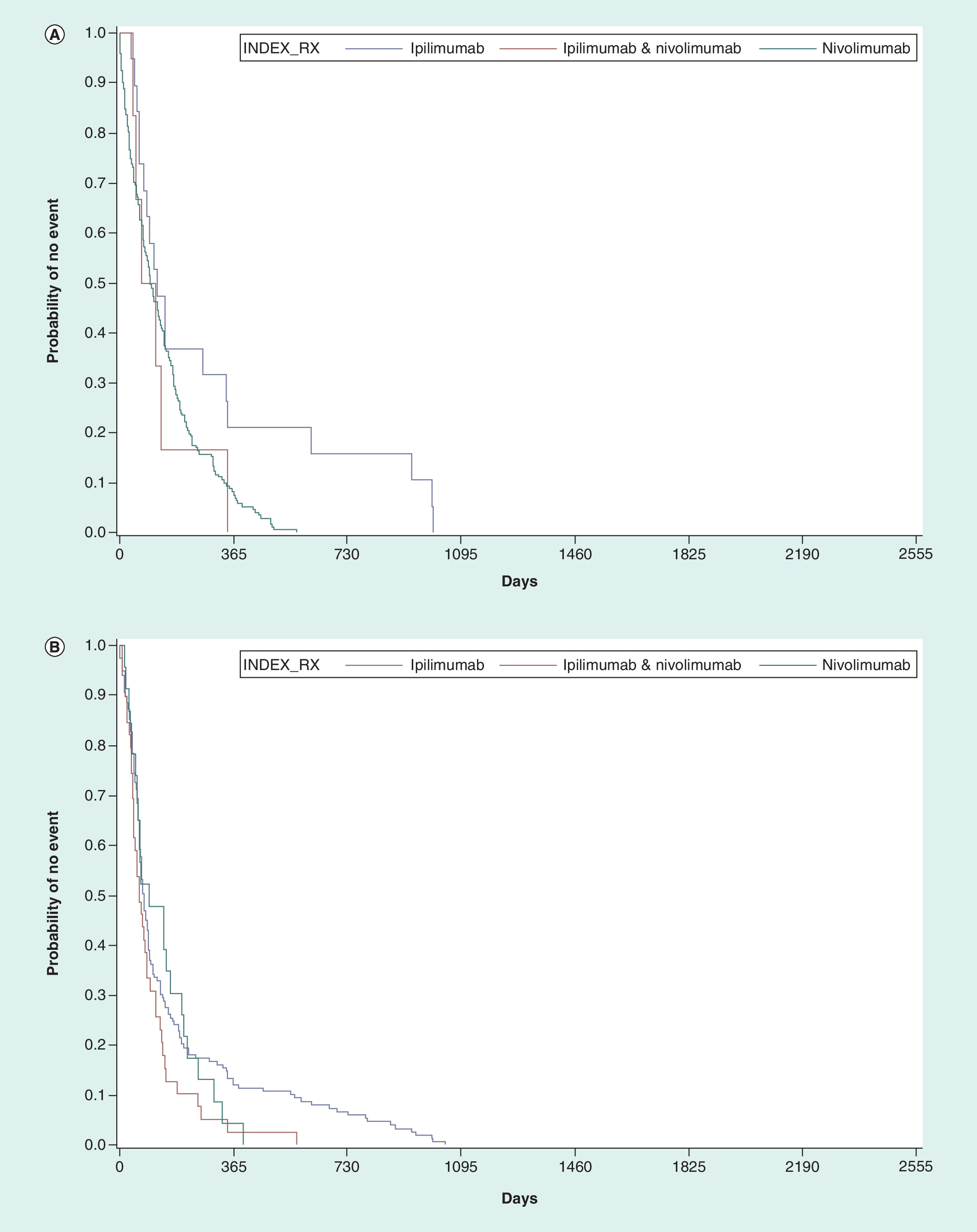
Figure 2. Adjusted hazard ratios of incident enterocolitis or diarrhea.
(A) Lung cancer. (B) Melanoma. Ipilimumab monotherapy is the control subcohort. Models controlled for age, sex, BMI, National Cancer Institute modification of the Deyo Charlson Comorbidity Index, preindex neutropenia or leukopenia, nausea or vomiting, abdominal cramping/pain and constipation. None of the covariates were statistically significant in the model.
Cox proportional hazard models were used to assess the hazard of incident enterocolitis or diarrhea among lung cancer and melanoma patients following the initiation of index drug. After adjusting for age, sex, BMI and comorbid conditions, compared with those receiving ipilimumab monotherapy, lung cancer patients receiving the combination therapy (hazard ratio [HR] = 2.93; 95% CI: 1.09−7.89; p = 0.03) or nivolumab monotherapy (HR = 2.13; 95% CI: 1.21−3.76; p = 0.009) had a statistically higher risk of a GI event (Figures 2A and 3). Among melanoma patients, the hazard of incident GI events was equivalent between patients on nivolumab and patients on ipilimumab (HR = 1.07; 95% CI: 0.68−1.70; p = 0.76) but significantly higher for patients on combination therapy compared with ipilimumab alone (HR = 1.54; 95% CI: 1.06−2.25; p = 0.02; Figures 2B and 3). None of the demographic or clinical covariates in either the lung cancer or melanoma models were statistically significant in the models.
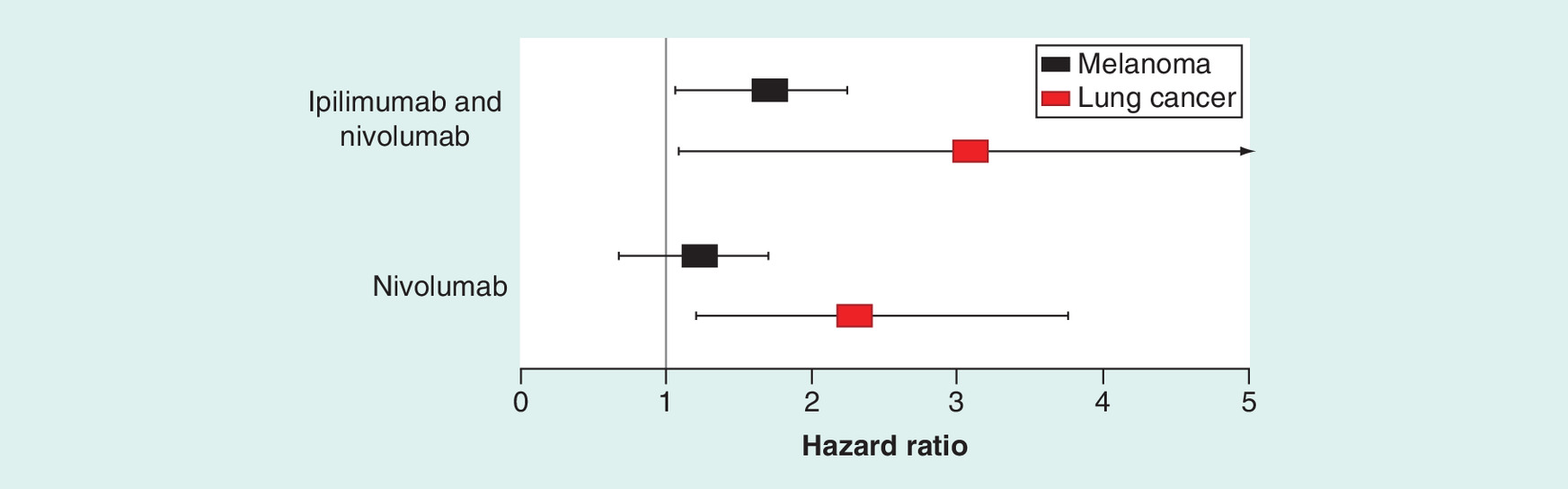
Figure 3. Time-to-incident enterocolitis or diarrhea during the duration of the index treatment regimen.
Lung cancer patients (bottom, red) and melanoma patients (top, black).
Discussion
This retrospective study used EMR data to evaluate incident GI AEs among patients with melanoma and lung cancer taking ipilimumab or nivolumab monotherapy or combination therapy. Incident GI AEs were common, and over 30% of patients in any subcohort had at least one event. The rate of AEs per 1000 patient-years ranged from 160.7 to 371.3 for diarrhea and from 50.9 to 166.6 for enterocolitis. The highest rates of enterocolitis were experienced by patients on the combination therapy (112.5 per 1000 lung cancer patient-years and 166.6 per 1000 melanoma person-years).
After adjusting for covariates, the hazard of incident enterocolitis or diarrhea was 1.5-times higher for melanoma patients on the combination of ipilimumab and nivolumab compared with ipilimumab monotherapy, and no statistical difference was observed when comparing the two monotherapies. In the lung cancer cohort, the hazard of incident enterocolitis or diarrhea was 2.9-times higher on the combination of ipilimumab and nivolumab, and 2.1-times higher on nivolumab monotherapy when compared with ipilimumab monotherapy. Patients in this real-world study were older than patients enrolled in previously reported clinical trials so it is possible that the age distribution of these real-world patients may have accounted for the relationship found between combination ipilimumab and nivolumab therapy and GI AEs [18]. However, this is not likely because the relationship between combination therapy and GI events remained after controlling for age, gender, comorbid conditions and other clinical variables in the multivariable models. In addition, none of these covariates were statistically significant in the models.
To our knowledge, this is the first study to compare the incidence rates of GI events between checkpoint inhibitors among melanoma and lung cancer patients using real-world data. Hassel et al. pooled AE data from four large advanced melanoma clinical trials on ipilimumab, nivolumab and/or combination therapy (Checkmate -037, -066, -067 and -069) [19]. They report the aggregated frequency of any GI events to be 42% for ipilimumab, 18% for nivolumab and 46% for combination therapy. The reported frequency of diarrhea was 34% for ipilimumab, 17% for nivolumab and 43% for combination therapy. The reported frequency of colitis was 12% for ipilimumab, 1% for nivolumab and 14% for combination therapy. These numbers are similar to the real-world data observed in this study. In general, patients in this study had slightly shorter durations of treatment compared with some of the clinical trials [29–32]. However, it is difficult to directly compare with clinical trial data because trials tend to have more stringent patient selection criteria (e.g., exclusion of patients who are less healthy or who have specific comorbid conditions) and protocol driven treatment regimens which likely impacts time on therapy.
A review of the published data for these trials found several differences in demographic and clinical characteristics between the real-world population in this study and the selected clinical trial populations [29–32] which may account for some of the differences seen. Patients in this real-world study were older than patients enrolled in previously reported clinical trials [18]. For example, although the mean age was similar, 58–65 years old, a greater proportion of the real-world population was 75 years or older (real-world = 21%; clinical trial = 13%). It is possible that the age distribution of these real-world patients may have accounted for the relationship found between combination ipilimumab and nivolumab therapy and GI AEs. However, this is not likely because the relationship between combination therapy and GI events remained after controlling for age, gender, comorbid conditions and other clinical variables in the multivariable models. In addition, none of these covariates were statistically significant in the models.
Limitations
Misclassification error is possible when relying on diagnosis coding from EMR, where the extent of missing or inaccurate codes is unknown. Patients’ medical and prescription history was limited to EMR during the reporting months in this study. The identification of AEs is accomplished by identifying patients with ICD-9 and ICD-10 diagnoses recorded in the EMR data during the duration of the treatment episode. The EMR data does not indicate the grade, severity or duration of the AEs nor does it provide direct attribution of the AE to the specific medications used during the treatment episode. The EMR data, including diagnoses, prescriptions and procedures are only available when the patient is seen by a contributor to the EHR system, and any services conducted by providers external to contributing EMR systems were not captured. The Explorys Universe Database is a convenient sample of contributing data sources in the USA, and thus, findings may not be generalizable to other US or international patient populations. Multivariate analyses of outcomes provided further adjustment for potentially confounding covariates used in the matching process and an additional degree of robustness in cohort comparisons; however, the potential for unmeasured confounders is always present.
Conclusion
Incident GI AEs were common in patients treated with ipilimumab or nivolumab, and the rate of GI AEs increased when these drugs were used in combination. Our results suggest that there is an unmet clinical need for the treatment of GI AEs in patients on combination therapy to minimize treatment disruption and/or discontinuation.
Future perspective
Clinical trials have shown improved survival for advanced melanoma and lung cancer patients on combination ipilimumab and nivolumab therapy, and additional trials are ongoing in other cancer types. It seems likely that the use of ipilimumab and nivolumab combination therapy will continue to grow and, with the expanded use of these therapies, it is anticipated that treatment outcomes including survival will improve. However, improved outcomes are accompanied with an increased risk of GI-related AEs compared with older therapies. The GI AEs represent a major barrier to sustained adherence to these medications and they are one of the leading causes for treatment discontinuation [18]. Discontinuation and reduced adherence may negate the expected treatment benefits. Given that these newer therapies are costly to the healthcare system, improved adherence through mitigating GI AEs would be a key component to long-term cost-effectiveness. New treatments for these GI AEs are needed to reduce symptoms and to maximize the potential positive clinical impact of these immunotherapies. Future studies should examine the relationship of treatment adherence, AEs and the impact on outcomes such as OS.
This retrospective cohort study examined the hazard of incident gastrointestinal (GI) adverse events (enterocolitis or diarrhea) in melanoma and lung cancer patients treated with (ipilimumab alone, nivolumab alone or in combination).
Data on patients with ≥1 record for ipilimumab or nivolumab between 1 March 2011 and 8 May 2017 and a diagnosis of melanoma (607 on ipilimumab, 140 on nivolumab and 157 on combo) or lung cancer (68 on ipilimumab, 1542 on nivolumab and 31 on combo) was extracted from a deidentified EMR dataset.
Index treatment regime, time on therapy and rate of any GI events were assessed using descriptive statistics for each cancer type.
In the lung cancer cohort, for patients on ipilimumab, nivolumab or combo therapy, the average time on therapy was 117.9 ± 216.8 days versus 138.1 ± 145.1 days versus 112.4 ± 95.8 days, the percentage of patients with at least one GI adverse event was 63.2 versus 35.7 versus 41.9%, and the rate of enterocolitis was 87.1 versus 50.9 versus 112.5 per 1000 patient-years.
In the melanoma cohort, for patients on ipilimumab, nivolumab or combo therapy, the average time on therapy was 107.2 ± 174.7 days versus 120.8 ± 138.2 days versus 129.2 ± 126.5 days, the percentage of patients with at least one GI adverse event was 49.3 versus 32.9 versus 44.6%, and the rate of enterocolitis was 96.7 versus 90.1 versus 166.6 per 1000 patient-years.
Cox proportional hazard models were used to estimate the hazard ratio (HR) of any incident enterocolitis or diarrhea by index drug group, adjusting for age, sex, BMI and comorbid conditions.
In the hazard model for GI events, melanoma and lung patients on the combination therapy were at a significantly increased risk of enterocolitis or diarrhea while on therapy compared with those on ipilimumab monotherapy (melanoma HR: 1.54; 95% CI: 1.06−2.25; p = 0.02; lung HR: 2.93; 95% CI: 1.09−7.89; p = 0.03).
There is an unmet clinical need for the management of GI events in patients treated with ipilimumab and nivolumab combo therapy.
Financial & competing interests disclosure
This study was sponsored by Takeda Oncology, Cambridge, MA, USA. JA Bell, A Galaznik and I Garcia-Ribas are employed by Takeda Oncology. D Irwin and B Davis are employed by IBM Watson Health as consultants and received funding from Takeda Oncology to conduct this study. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Medical writing support was provided by JP Winer-Jones of IBM Watson Health. Medical writing services were paid for by Takeda Oncology.
Author contributions
All authors contributed to the conception of the study, analysis of the data, writing of the manuscript and approval of the final draft.
Ethical conduct of research
All study data were accessed with protocols compliant with US patient confidentiality requirements, including the Health Insurance Portability and Accountability Act of 1996 regulations. As all database used in the study are fully deidentified and compliant with the Health Insurance Portability and Accountability Act, this study was exempted from Institutional Review Board approval.
Supplementary Material
File (supplementary content.docx)
- Download
- 41.57 KB
References
Papers of special note have been highlighted as: • of interest
1.
Pardoll DM. The blockade of immune checkpoints in cancer immunotherapy. Nature Rev. Cancer 12(4), 252–264 (2012).
2.
Sliwkowski MX, Mellman I. Antibody therapeutics in cancer. Science 341(6151), 1192 (2013).
3.
Grosso JF, Jure-Kunkel MN. CTLA-4 blockade in tumor models: an overview of preclinical and translational research. Cancer Immun. 13, 5 (2013).
4.
Zou W, Wolchok JD, Chen L. PD-L1 (B7-H1) and PD-1 pathway blockade for cancer therapy: mechanisms, response biomarkers and combinations. Sci. Transl. Med. 8(328), 328rv324–328rv324 (2016).
5.
Buchbinder EI, Desai A. CTLA-4 and PD-1 pathways: similarities, differences, and implications of their inhibition. Am. J. Clin. Oncol. 39(1), 98–106 (2016).
• Provides a comprehensive review of biology behind cytotoxic T-lymphocyte-associated 4 and programmed cell death receptor 1 immunotherapy in cancer.
6.
Siegel RL, Miller KD, Jemal A. Cancer statistics, 2018. CA Cancer J. Clin. 68(1), 7–30 (2018).
7.
Jemal A, Siegel R, Xu J, Ward E. Cancer statistics, 2010. CA Cancer J. Clin. 60(5), 277–300 (2010).
8.
Hodi FS, O'Day SJ, Mcdermott DF et al. Improved survival with ipilimumab in patients with metastatic melanoma. New Engl. J. Med. 363(8), 711–723 (2010).
• First published Phase III trial of ipilimumab for metastatic melanoma reported that 7.3% of patients on ipilimumab experienced colitis.
9.
Weber JS, D'Angelo SP, Minor D et al. Nivolumab versus chemotherapy in patients with advanced melanoma who progressed after anti-CTLA-4 treatment (CheckMate 037): a randomised, controlled, open-label, Phase III trial. Lancet Oncol. 16(4), 375–384 (2015).
10.
Hodi FS, Chesney J, Pavlick AC et al. Two-year overall survival rates from a randomised Phase II trial evaluating the combination of nivolumab and ipilimumab versus ipilimumab alone in patients with advanced melanoma. Lancet Oncol. 17(11), 1558–1568 (2016).
11.
Larkin J, Chiarion-Sileni V, Gonzalez R et al. Combined nivolumab and ipilimumab or monotherapy in untreated melanoma. New Engl. J. Med. 373(1), 23–34 (2015).
• 1:1:1 Phase III study comparing nivolumab, ipilimumab and the combination therapy, the respective proportion of patients who were diagnosed with colitis was 1.3, 11.6 and 11.8%.
12.
El-Khoueiry AB, Sangro B, Yau T et al. Nivolumab in patients with advanced hepatocellular carcinoma (CheckMate 040): an open-label, non-comparative, Phase I/II dose escalation and expansion trial. Lancet 389(10088), 2492–2502 (2017).
13.
Overman MJ, Mcdermott R, Leach JL et al. Nivolumab in patients with metastatic DNA mismatch repair-deficient or microsatellite instability-high colorectal cancer (CheckMate 142): an open-label, multicentre, Phase II study. Lancet Oncol. 18(9), 1182–1191 (2017).
14.
Borghaei H, Paz-Ares L, Horn L et al. Nivolumab versus docetaxel in advanced nonsquamous non-small-cell lung cancer. New Engl. J. Med. 373(17), 1627–1639 (2015).
15.
Brahmer J, Reckamp KL, Baas P et al. Nivolumab versus docetaxel in advanced squamous-cell non-small-cell lung cancer. New Engl. J. Med. 373(2), 123–135 (2015).
16.
Hellmann MD, Rizvi NA, Goldman JW et al. Nivolumab plus ipilimumab as first-line treatment for advanced non-small-cell lung cancer (CheckMate 012): results of an open-label, Phase I, multicohort study. Lancet Oncol. 18(1), 31–41 (2017).
17.
Michot JM, Bigenwald C, Champiat S et al. Immune-related adverse events with immune checkpoint blockade: a comprehensive review. Eur. J. Cancer 54, 139–148 (2016).
18.
Mearns ES, Bell JA, Galaznik A et al. Gastrointestinal adverse events with combination of checkpoint inhibitors in advanced melanoma: a systematic review. Melanoma Manag. 5(1), MMT01 (2018).
19.
Hassel JC, Heinzerling L, Aberle J et al. Combined immune checkpoint blockade (anti-PD-1/anti-CTLA-4): evaluation and management of adverse drug reactions. Cancer Treat. Rev. 57, 36–49 (2017).
• A study pooling safety data of 1551 patients from publicly available drug trials reported rates of any colitis and enterocolitis of 1.1% for nivolumab, 11.8% for ipilimumab and 14.5% for combination therapy.
20.
Ali AK, Watson DE. Pharmacovigilance assessment of immune-mediated reactions reported for checkpoint inhibitor cancer immunotherapies. Pharmacotherapy 37(11), 1383–1390 (2017).
• An analysis of data from the US FDA Adverse Event Reporting System found that colitis was the most commonly reported immune-related adverse event (IRAE) and it accounted for 553 (63.2%) of IRAE for ipilimumab and 72 (40.7%) of IRAEs for nivolumab.
21.
Melanoma (version 2.2018) (February 2, 2018), (2018). www.nccn.org/professionals/physician_gls/pdf/melanoma.pdf.
22.
Kumar V, Chaudhary N, Garg M, Floudas CS, Soni P, Chandra AB. Current diagnosis and management of immune related adverseeEvents (IRAEs) induced by immune checkpoint inhibitor therapy. Front. Pharmacol. 8, 49 (2017).
23.
Horvat TZ, Adel NG, Dang T-O et al. Immune-related adverse events, need for systemic immunosuppression, and effects on survival and time to treatment failure in patients with melanoma treated with ipilimumab at Memorial Sloan Kettering Cancer Center. J. Clin. Oncol. 33(28), 3193–3198 (2015).
• A single site retrospective review of IRAEs in 298 melanoma patients treated with ipilimumab including frequency, treatment approach and outcomes. A total of 19% discontinued therapy because of IRAEs with diarrhea being the most common cause, 35% required systemic corticosteroid treatment, but occurrence or treatment of IRAEs did not affect overall survival.
24.
Hammers HJ, Plimack ER, Infante JR et al. Expanded cohort results from CheckMate 016: a Phase I study of nivolumab in combination with ipilimumab in metastatic renal cell carcinoma (mRCC). J. Clin. Oncol. 33(15 Suppl.), 4516 (Abstract 4516) (2015).
25.
Janjigian YY, Bendell JC, Calvo E et al. CheckMate-032: Phase I/II, open-label study of safety and activity of nivolumab (nivo) alone or with ipilimumab (ipi) in advanced and metastatic (A/M) gastric cancer (GC). J. Clin. Oncol. 34(15 Suppl.), 4010–4010 (2016).
26.
Overman MJ, Kopetz S, Mcdermott RS et al. Nivolumab ± ipilimumab in treatment (tx) of patients (pts) with metastatic colorectal cancer (mCRC) with and without high microsatellite instability (MSI-H): CheckMate-142 interim results. J. Clin. Oncol. 34(15_suppl), 3501–3501 (2016).
27.
Deyo RA, Cherkin DC, Ciol MA. Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J. Clin. Epidemiol. 45(6), 613–619 (1992).
28.
SEER-Medicare: calculation of comorbidity weights (March 6, 2017). https://healthcaredelivery.cancer.gov/seermedicare/considerations/calculation.html.
29.
Phase IIIstudy of nivolumab or nivolumab plus ipilimumab versus ipilimumab alone in previously untreated advanced melanoma (CheckMate 067) (March 5, 2018). https://ClinicalTrials.gov/show/NCT01844505.
30.
Study of nivolumab (BMS-936558) compared with dacarbazine in untreated, unresectable, or metastatic melanoma (March 5, 2018). https://ClinicalTrials.gov/show/NCT01721772.
31.
Study of nivolumab (BMS-936558) plus ipilimumab compared with ipilimumab alone in the treatment of previously untreated, unresectable, or metastatic melanoma (March 5, 2018). https://ClinicalTrials.gov/show/NCT01927419.
32.
Bristol-Myers S. A study to compare BMS-936558 to the physician's choice of either dacarbazine or carboplatin and paclitaxel in advanced melanoma patients that have progressed following anti-CTLA-4 therapy (CheckMate 037) (March 5, 2018), (2016). https://ClinicalTrials.gov/show/NCT01721746.
Information & Authors
Information
Published In
Copyright
© 2018 Future Medicine Ltd.
History
Received: 18 July 2018
Accepted: 5 November 2018
Published online: 14 December 2018
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Gastrointestinal complications in patients treated with ipilimumab and nivolumab combination therapy or monotherapy. (2018) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2018-0072
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Süleyman Can, Are We Underestimating the Toxicity of Combination Immune Checkpoint Inhibitors? Real-World Evidence Challenging Current Guideline Predictions., Medical Science and Discovery, 10.36472/msd.v12i12.1343, 12, 12, (327-329), (2025).
- Agnès Calsina-Berna, Jesús González-Barboteo, Silvia Llorens-Torromé, Joaquim Julià-Torras, Antitumoral Agent-Induced Constipation: A Systematic Review, Cancers, 10.3390/cancers16010099, 16, 1, (99), (2023).
- Abdulaali R. Almutairi, Marion Slack, Brian L. Erstad, Ali McBride, Ivo Abraham, Association of immune-checkpoint inhibitors and the risk of immune-related colitis among elderly patients with advanced melanoma: real-world evidence from the SEER–Medicare database, Therapeutic Advances in Drug Safety, 10.1177/2042098621991279, 12, (2021).
- Carolina Lopes, Sandra Morgado, Ana I. Plácido, Fátima Roque, Manuel Morgado, Critical Analysis of Immune Checkpoint Inhibitor Immunotoxicity Management, SN Comprehensive Clinical Medicine, 10.1007/s42399-020-00670-w, 3, 1, (84-94), (2021).
- Pauline Hulo, Yann Touchefeu, Estelle Cauchin, Isabelle Archambeaud, Nicolas Chapelle, Céline Bossard, Jaafar Bennouna, Acute Ulceronecrotic Gastritis With Cytomegalovirus Reactivation: Uncommon Toxicity of Immune Checkpoint Inhibitors in Microsatellite Instability–High Metastatic Colorectal Cancer, Clinical Colorectal Cancer, 10.1016/j.clcc.2020.04.006, 19, 4, (e183-e188), (2020).
- Abdulaali R. Almutairi, Ali McBride, Marion Slack, Brian L. Erstad, Ivo Abraham, Potential Immune-Related Adverse Events Associated With Monotherapy and Combination Therapy of Ipilimumab, Nivolumab, and Pembrolizumab for Advanced Melanoma: A Systematic Review and Meta-Analysis, Frontiers in Oncology, 10.3389/fonc.2020.00091, 10, (2020).
- Alice C. Shieh, Ezgi Guler, David Pfau, Ethan Radzinsky, Daniel A. Smith, Christopher Hoimes, Nikhil H. Ramaiya, Sree Harsha Tirumani, Imaging and clinical manifestations of immune checkpoint inhibitor-related colitis in cancer patients treated with monotherapy or combination therapy, Abdominal Radiology, 10.1007/s00261-019-02334-3, 45, 10, (3028-3035), (2019).