Hospital cost impact of orbital atherectomy with angioplasty for critical limb ischemia treatment: a modeling approach
Abstract
Aim: The incremental cost of peripheral orbital atherectomy system (OAS) plus balloon angioplasty (BA) versus BA-only for critical limb ischemia was estimated. Materials & methods: A deterministic simulation model used clinical and healthcare utilization data from the CALCIUM 360° trial and current cost data. Incremental cost of OAS + BA versus BA-only included differential utilization during the procedure and adverse-event costs at 3, 6 and 12-months. Results: For every 100 procedures, incremental annual costs to the hospital were US$350,930 lower with OAS + BA compared with BA-only. Despite higher upfront costs, savings were realized due to reduced need for revascularization, amputation and end-of-life care over 6–12-month postoperative period. Conclusion: Atherectomy with OAS prior to BA was associated with cost savings to the hospital.
Critical limb ischemia (CLI) is the most serious manifestation of peripheral artery disease (PAD). Considered as the ‘end stage’ of PAD, it involves a chronic lack of blood supply leading to persistent ischemic rest pain in the feet or toes, nonhealing wounds and ulcers, and gangrene [1]. CLI often results in amputation of the affected limb(s) with roughly 25% of CLI patients receiving at least one lower extremity amputation [2]. The economic burden of CLI-diagnosed Medicare patients exceeds US$3.1 billion annually, with most of this cost reflecting the high incidence of hospitalizations related to limb loss and the need for major amputation [3].
Treating CLI patients has remained quite challenging, since the associated calcification requires a unique mechanism of action to treat the lesion without damaging the vessel [4]. Balloon angioplasty (BA) continues to be the first-line of revascularization strategy in patients where procedural success via less invasive, nonsurgical approach is favored despite consistently poor intermediate and long-term patency outcomes [5,6]. The latter has been attributed to the presence of calcified plaque in femoropopliteal lesions, with arterial wall calcium associated with higher rates of procedural complications, and flow-limiting dissections that frequently require stent deployment in order to maintain vessel patency [4–6]. Furthermore, restenosis rates as high as 40–60% within 1 year of postprocedure and poor correlation between primary patency and limb preservation have been reported. But the American College of Cardiology/American Heart Association guidelines currently recommend against primary stenting of femoropopliteal lesions with atherectomy and stent devices indicated for ‘bailout’ purposes following suboptimal BA results [5]. Stenting in calcified segments after a prior failed BA often results in stent under expansion and malapposition [6,7]. These are recognized predictors of long-term stent patency and indicate an increased risk of subsequent stent fracture and/or restenosis. Additionally, biomechanical stresses across the dynamic femoropopliteal segment increase the complexity of the pathophysiology and treatment decision making.
In 2007, Cardiovascular Systems, Inc's Diamondback 360 Peripheral Orbital Atherectomy System (OAS; Cardiovascular Systems Inc., MN, USA) was cleared by the US FDA as an OAS indicated for use as therapy in patients with occlusive atherosclerotic disease in peripheral arteries and considered as acceptable candidates for percutaneous transluminal atherectomy. This percutaneous, minimally invasive endovascular device system is composed of a single-use, low-profile catheter with a diamond-coated crown that orbits at high speeds while removing a thin layer of calcific plaque with each pass of the crown [8]. Randomized clinical trial (RCT) evidence indicated that CLI patients receiving BA plus atherectomy involving OAS had a lower rate of complications [9–12], and medial damage [8], and reduced need for bailout stenting [12], thus preserving future treatment options.
While cost containment remains a priority for hospitals, policymakers and other stakeholders, there is limited economic evidence regarding this new technology. Weinstock et al. conducted a cost–effectiveness analysis of employing OAS + BA versus BA only procedure for above-the-knee (ATK) calcified femoropopliteal lesions [6]. The study found that index procedure hospital costs (US$15,100 vs US$11,016) were expectedly higher for OAS + BA but this difference was not statistically significant compared with BA alone. Furthermore, the 1-year incremental cost of OAS + BA versus BA alone was estimated to be US$549, with an incremental cost–effectiveness ratio of US$3441, well below the acceptable US$50,000–US$100,000 threshold. But little is known about selecting optimal endovascular treatment strategies for treating calcified infrapopliteal lesions below-the-knee (BTK). Therefore, the objective of this economic evaluation was to perform an incremental cost analysis of the OAS + BA procedure versus BA-only for BTK CLI patients from a US-inpatient perspective in order to assess the affordability and the overall economic impact of implementing this technology.
Materials & methods
A deterministic decision tree simulation model was constructed using TreeAge Pro 2015 analysis software (TreeAge Software Inc., MA, USA). The model assumed a hypothetical cohort of 100 PAD-CLI patients with moderate/severe calcified BTK lesions undergoing an endovascular revascularization procedure in a US hospital/health system. The model estimated the incremental cost difference to the hospital to perform OAS followed by BA versus BA only by examining the clinical and economic end points associated with the initial procedure visit and over multiple postprocedure time windows (3, 6 and 12 months). Figures 1 and 2 illustrate the model scaffold and the decision tree, respectively. The model was reconstructed using Microsoft Excel for validation purposes.
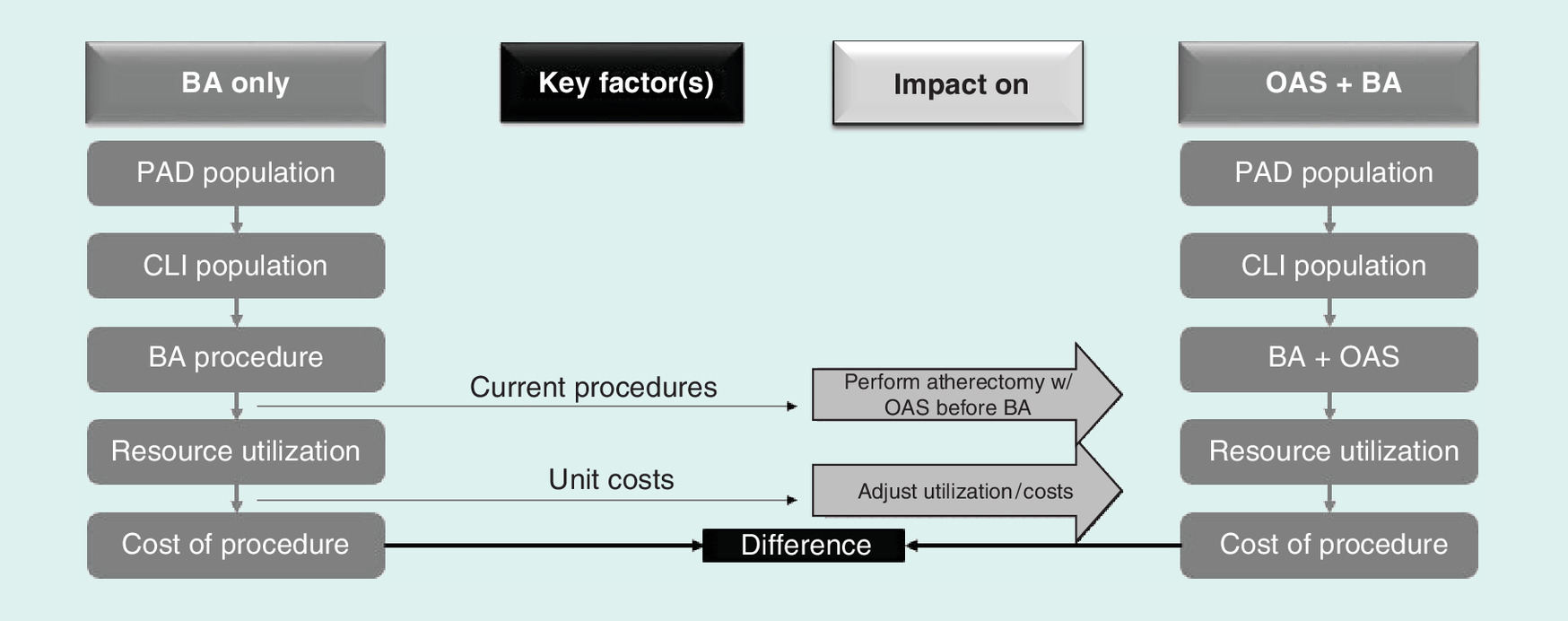
Figure 1. Economic model scaffold.
BA: Balloon angioplasty; CLI: Critical limb ischemia; OAS: Diamondback 360° Orbital Atherectomy System; PAD: Peripheral artery disease.
Adapted with permission from [13].
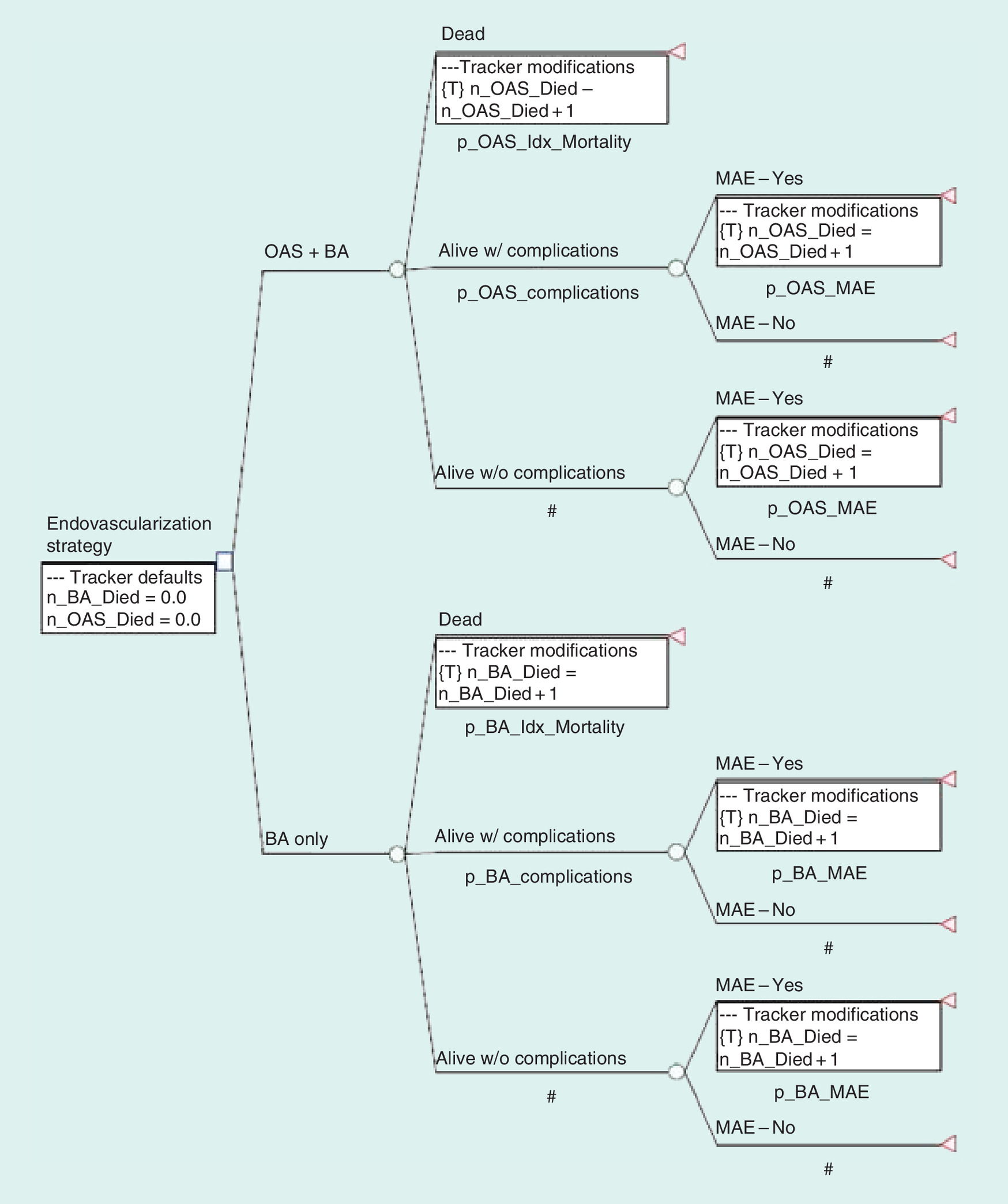
Figure 2. TreeAge decision tree snapshot.
p_xxx_xxx are probability variables associated with branch after a chance node (O). The hash (#) is a residual probability symbol used in place of a probability expression for one branch to have TreeAge automatically calculate the complement during calculations. n_xxx_xxxx are tracker variables; in this case they track specifically simulations that end in a patient's death.
BA: Balloon angioplasty; MAE: Major adverse event; OAS: Diamondback 360°Orbital Atherectomy System.
Clinical end points
Clinical and healthcare utilization estimates (Table 1) were primarily derived from the CALCIUM 360° RCT [11]. This was a prospective, multicenter, 1:1 randomized pilot study that compared the performance of the Diamondback 360 OAS + BA to BA-alone in treating severe lower extremity PAD (≥50% stenosis in Rutherford class 4–6) involving the popliteal, and tibial vessels. The study enrolled 25 patients (29 lesions) randomized to the OAS + BA arm, while 25 others (35 lesions) were assigned to the BA only control arm across eight centers in the USA. The following utilization measures were included in the simulation model: use of OAS device, number of balloon(s), and number of bare metal stents used for bailout. The mean OAS device run time as reported in the trial was approximately 2.4 min. It was hypothesized that beyond the actual device costs and its run time costs in the operating room, any additional impact associated with employing OAS technology (e.g., set-up, anesthesia time) was marginal and negligible to the standard BA procedure costs to the hospital. Perioperative complications under consideration included perforation, dissection, major bleeding, acute myocardial infarction, embolism, thrombus, and/or death occurring during the procedure visit. For the postoperative follow-up timeframes (3, 6 and 12 months), adverse events (AEs) included target lesion and vessel revascularization (TLR/TVR), major amputation (i.e., ATK), and/or all-cause mortality. A composite outcome – major adverse event (MAE) – was defined as the sum of ATK amputation, TLR/TVR and mortality from all causes. The composite metric was considered as our primary outcome since the CALCIUM 360° trial results found a statistically significant difference between the OAS + BA and BA-only groups at 6 and 12 months.
| Population characteristics | CALCIUM 360 | Costs | Ref. | ||
|---|---|---|---|---|---|
| OAS + BA | BA-only | Basecase (US$) | Range (US$) | ||
| Mean number of balloons per patient | 1.9 | 3.0 | 301 | 226–376 | [14] |
| Proportion receiving bail-out stenting (%)§ | 6.9 | 14.3 | 3395 | 2546–4244 | [14] |
| Bare metal stent receipt | 100 | 100 | 1460 | 1095–1825 | [14] |
| Mean number of stents used per patient | 1.0 | 1.4 | [14] | ||
| Device running time in operating room (min)¶ | 2.4 | 0 | 25.99/min | 25–26.5 | [15] |
| Perioperative complications (%) | |||||
| Acute myocardial infarction | 0 | 0 | 14,223 | 9,439–14,350 | [15] |
| Dissection | 10.3 | 17.1 | 0# | [11] | |
| Embolism | 0 | 2.9 | 375 | 281–469 | [16] |
| Major bleeding | 0 | 0 | 32,088 | 30,890–33,285 | [15] |
| Perforation | 0 | 2.9 | 0# | [11] | |
| Thrombus | 0 | 0 | 375 | 281–469 | [16] |
| All-cause death | 0 | 0 | 10,809 | 8107–13,511 | [17] |
| Adverse events (3 months) | |||||
| ATK amputation | 0 | 0 | 48,614 | 36,461–60,768 | [18] |
| TLR/TVR | 0 | 4.3 | 22,688 | 17,016–28,360 | [6] |
| All-cause death | 0 | 4.3 | 10,809 | 8107–13,511 | [17] |
| MAE‡ | 0 | 8.7 | 16,749 | 8107–28,360 | Weighted average |
| Adverse events (6 months) | |||||
| ATK amputation | 0 | 0 | 48,614 | 36,461–60,768 | [18] |
| TLR/TVR | 0 | 15.0 | 22,688 | 17,016–28,360 | [6] |
| All-cause death | 0 | 17.4 | 10,809 | 8107–13,511 | [17] |
| MAE† ‡ | 0 | 26.1 | 16,309 | 8107–28,360 | Weighted average |
| Adverse events (1 year) | |||||
| ATK amputation | 0 | 0 | 48,614 | 36,461–60,768 | [18] |
| TLR/TVR | 6.7 | 20.0 | 22,688 | 17,016–28,360 | [6] |
| All-cause death† | 0 | 31.6 | 10,809 | 8107–13,511 | [17] |
| MAE† ‡ | 6.7 | 42.1 | 16,249 | 8107–28,360 | Weighted average |
†These results were significant (p < 0.05) in the CALCIUM 360° trial.
‡Defined as the occurrence of any of the major 1-year adverse events (AE): ATK amputation, TLR/TVR and/or all-cause death.
§Defined as unplanned stent placement due to suboptimal results post treatment with balloon angioplasty or atherectomy (allowed at the physician's discretion). Suboptimal results in the CALCIUM 360 were defined as: less than 30% stenosis was not achieved; dissections of types C–F requiring treatment; or, significant vessel recoil was evident.
¶Defined as the cumulative amount of time that the OAS device was activated (crown spinning in an orbital motion) to treat the lesion.
#The reason that these values are set to is 0 is because dissection and perforation typically lead to a stent placement and we already included these costs in the patients receiving stents. Depending on their severity, dissections are assigned different classes varying between A and F, and anything from C to F requires a stent. A and B are too minor to require any treatment. Thus, we did not assign a cost to dissection itself in order to avoid double counting. We similarly did not assign a cost to perforation to avoid double counting.
ATK: Above-the-knee; BA: Balloon angioplasty; MAE: Major adverse event; OAS: Diamondback 360° orbital atherectomy System; SD: Standard deviation; TLR: Target lesion revascularization; TVR: Target vessel revascularization.
Cost end points
The unit costs of the OAS device, balloons, and bare metal stents were obtained from average selling price information that was provided by Cardiovascular Systems, Inc. The 2014 Healthcare Cost and Utilization Project (HCUP) Nationwide Inpatient Sample of 35.4 million discharges was queried to determine the costs of the perioperative complications: acute myocardial infarction (DRG code 280) and major bleeding (ICD-9-CM diagnosis code 904.xx and procedure code 83.14) [15]. HCUP is a family of healthcare databases and related software tools sponsored by the Agency for Healthcare Research and Quality. It is based on statewide data collection by individual data organizations across the USA and includes the largest collection of longitudinal hospital care data in the USA, encompassing all-payer, discharge-level information. The other AE and complication-related treatment cost data were obtained using the published literature [16–19]. These cost estimates were then inflated to 2016 (October) US dollars using the Medical Care Component of the Consumer Price Index [20]. MAE cost was calculated by weighting the costs of the AEs under consideration (ATK amputation, TLR/TVR and all-cause mortality) with their occurrence rate in any given time period of interest.
Incremental costs
The simulation model estimated the incremental cost of performing 100 OAS + BA procedures versus 100 BA-only procedures (with bailout stenting) as the total sum of differences in [1] costs related to complications and AEs and [2] costs corresponding to balloon, stent and/or OAS-related usage during the procedure. These cumulative cost differences were compared at several different time horizons: at the time of index procedure and the available three follow-up timeframes.
Sensitivity analyses
To gauge the robustness of the results, both one-way and probabilistic sensitivity analyses were performed for the 12-month time window. One-way sensitivity included varying the individual model parameters by ±25% from their baseline values and recalculating the incremental cost difference between OAS + BA and BA-only. A tornado diagram was then generated to visually demonstrate the impact of the individual model parameter values.
A probabilistic sensitivity analysis was also performed by running 10,000 Monte-Carlo trial simulations. Given that there was only a single source for both the primary and secondary analyses, we lacked dispersion data to accompany the estimates from the CALCIUM 360° trial in order to generate detailed distributions needed for performing the Monte Carlo simulations. To address this issue, the literature-derived sample-size weighted standard deviation values were used for all the BA-only and OAS + BA distribution parameters. Specifically, normal and beta distributions were assumed for the utilization and complication estimates, respectively, based on published evidence [21]. A triangular distribution was used for the costs, with ±25% of the baseline value used to set up the distribution's range (i.e., the minimum and maximum). Based on the Monte-Carlo trial simulations, the proportion of trials for which OAS + BA demonstrated cost savings and therefore the economic value versus standalone BA was subsequently estimated.
Scenario analysis
The main limitation of the CALCIUM 360° trial was its small sample size. This was particularly significant in the case of all-cause mortality in the BA-only arm, observed to be 31.6%, a much higher than expected figure. A secondary concern was the 0% rates reported for some of the AEs and complications (e.g., amputation, perioperative death, etc.) in both the treatment arms in the CALCIUM 360° trial. It is plausible that these were relatively rare events, too small to be observed in a sample of 25 patients. In order to overcome these limitations, and account only for the outcomes the pilot trial was powered to detect, we replaced all the rare event rates (defined as <5% in either of the treatment arms of the trial at 1-year follow-up) with values obtained from the literature. With the same value powering both the arms, this approach would negate any inadvertently offered advantage to the OAS + BA treatment arm and yield a conservative dollar impact of introducing OAS 360 to the current standard of care.
To supplement the trial data with existing published data points, we performed a best evidence review of the current literature. Studies were chosen if the following inclusion criteria were satisfied: English language publications between 2005 and 2015; adult subjects (≥18 years of age) who received BA or percutaneous transluminal angioplasty or angioplasty with or without concurrent atherectomy involving only OAS for calcified BTK lesions; reported one or more of the aforementioned clinical or utilization related outcomes of interest; and a minimum of 25 angioplasty procedures were performed. Studies were excluded if: outcome data were not specific to BTK lesions; patient population was primarily composed of those with lesion severity 3 or less as defined by Rutherford classification; in vitro, animal, or cadaver research; and case reports, commentaries and editorials. Outcome occurrence rates were adjusted to 1 year if different follow-up timeframes were available as long as they were for a reasonable time period (≥6 months). A total of 13 studies were identified [22–34]. Patient demographic, PAD-CLI disease and comorbid risk profiles were extracted from each study to evaluate their clinical compatibility to the CALCIUM 360°'s BA-only population (since both receive similar surgeries). Individual outcome data (where reported) were obtained from each of the above 13 studies. These data points were pooled and sample sizes were used to calculate weighted proportions and means for the rarer events of interest (see Table 2).
| Population characteristics | OAS + BA | BA-only | Literature reported range | Ref. |
|---|---|---|---|---|
| Perioperative complications (%) | ||||
| Acute myocardial infarction | 1.4† | 0–4 | [22–24] | |
| Dissection | 10.3 | 17.1 | 3.5–19.2 | [25–29] |
| Embolism | 0.4† | 0.2–0.6 | [22,24,28] | |
| Major bleeding | 1.1† | 0.8–1.4 | [22,24,27] | |
| Perforation | 4.7† | 2–5.9 | [22,25] | |
| Thrombus | 1.2† | 0.9–1.5 | [24] | |
| All-cause death | 1.2† | 0.2–3.0 | [22,24,27] | |
| Adverse events (12 months) | ||||
| ATK amputation | 8.1† | 0.7–26.5 | [23–28,30–32] | |
| TLR/TVR | 6.7 | 20 | 3–43.3 | [23–28,30–33] |
| All-cause death | 13.9† | 31.6 | 4.5–24 | [23,25–34] |
| MAE‡ (Wt. cost = US$18,581) | 28.8 | 42.1 | 13.9–49.3 | [23,25,26,28,30] |
†These rare event rates were replaced by sample size weighted estimates from published literature.
‡Defined as the occurrence of any of the major 1-year adverse events (AE): ATK amputation, TLR/TVR and/or all-cause death.
ATK: Above-the-knee; BA: Balloon angioplasty; MAE: Major adverse event; OAS: Diamondback 360°orbital atherectomy; TLR: Target lesion revascularization; TVR: Target vessel revascularization; Wt.: Weighted.
Results
Incremental costs
For a hospital or a health system performing 100 BTK endovascular procedures annually, the expected costs for the index procedure visit were US$413,002 for OAS + BA compared with US$119,529 for BA alone leading to an incremental cost of US$293,472 or US$2,935 per patient in the case of OAS + BA. The majority of this difference was attributable to the OAS device unit costs (see Table 3). The BA-only approach continued to be an economical option for the 3-month postoperative period since procedure plus 3-month AE costs for OAS + BA were calculated at US$413,002 versus BA-only’ costs of US$264,654, leading to a net cost difference of US$1483 per patient. However, increased revascularizations (US$340,320) for stand-alone BA (US$649,013) at 6 months compared with OAS + BA (US$413,002) meant that the latter incurred aggregate cost savings of US$236,012. At the end of 1-year follow-up, OAS + BA procedural patients were expected to average US$565,011 versus US$915,941 for BA-only patients. Therefore, the hospital is expected to yield incremental cost savings up to US$3509 per annum for every procedure performed. These cost savings are primarily reflected through a reduction in the occurrence and treatment of major amputation, TLR/TVR, and dollars spent towards end-of-life care, despite the higher upfront technology costs.
| Expected costs | OAS + BA (US$) | BA-only (US$) | Cost difference (US$) |
|---|---|---|---|
| Procedure visit | |||
| Supply costs | 413,002 | 119,529 | 293,473 |
| Adverse event costs | 0 | 1,088 | -1,088 |
| Total incremental cost difference (procedure) | 292,385 | ||
| Postprocedure complication costs (3 months) | |||
| MAE: | 0 | 144,037 | -144,037 |
| – ATK amputation | 0 | 0 | 0 |
| – TLR/TVR | 0 | 97,558 | -97,558 |
| – All-cause death | 0 | 46,479 | -46,479 |
| Total incremental cost difference (procedure + 3-month follow-up) | 148,348 | ||
| Postprocedure complication costs (6 months) | |||
| MAE: | 0 | 528,397 | -528,397 |
| – ATK amputation | 0 | 0 | 0 |
| – TLR/TVR | 0 | 340,320 | -340,320 |
| – All-cause death | 0 | 188,077 | -188,077 |
| Total incremental cost difference (procedure + 6-month follow-up) | -236,012 | ||
| Postprocedure complication costs (12 months) | |||
| MAE: | 152,010 | 795,324 | -643,314 |
| – ATK amputation | 0 | 0 | 0 |
| – TLR/TVR | 152,010 | 453,760 | 301,750 |
| – All-cause death | 0 | 341,564 | -341,564 |
| Total incremental cost difference (procedure + 12-month follow-up) | -350,930 | ||
| Scenario analysis | |||
| Procedure visit: | |||
| – Supply costs | 413,002 | 119,529 | 293,472 |
| – Adverse event costs | 69,659 | 69,659 | 0 |
| Total incremental cost difference (procedure) | 293,472 | ||
| Postprocedure complication costs (12 months) | |||
| MAE: | 697,811 | 1,190,556 | -492,745 |
| – ATK amputation | 395,232 | 395,232 | 0 |
| – TLR/TVR | 152,010 | 453,760 | -301,750 |
| – All-cause death | 150,569 | 341,564 | -190,995 |
| Total incremental cost difference (procedure + 12-month follow-up) | -199,273 | ||
ATK: Above-the-knee; BA: Balloon angioplasty; MAE: Major adverse event; OAS: Diamondback 360° orbital atherectomy; TLR: Target lesion revascularization; TVR: Target vessel revascularization.
Sensitivity analysis
One-way sensitivity analysis demonstrated that the OAS + BA procedure was economically superior in comparison to stand-alone BA with bailout stenting and that these results were robust. It also revealed that the model was most sensitive to the following parameters: frequency of TLR/TVR and its treatment cost, 1-year mortality rate and end-of-life care cost, and OAS device cost (see Figure 3).

Figure 3. One-way sensitivity analysis.
AMI: Acute myocardial infarction; BA: Balloon angioplasty; OAS: Diamondback 360° orbital atherectomy system; TLR: Target lesion revascularization; TVR: Target vessel revascularization.
In the probabilistic sensitivity analysis, cost savings were observed in 81.6% of the Monte Carlo simulations, indicating that OAS + BA was a dominant treatment strategy. Of the remaining 18.4% simulations, OAS + BA was found to cost a mean additional US$3574 versus BA-only per patient. Incorporating the number of lives lost by each treatment strategy during the course of the year, the incremental cost–effectiveness ratio (ICER), defined as the ratio of the cost difference between OAS + BA and BA-only and the corresponding difference in mortality rate, was calculated to be US$11,207.
Scenario analysis
We found that the CALCIUM 360° BA-only arm and the literature-derived cohort were largely similar in terms of demographics: males (60 vs 63.8%), mean age (71.8 vs 70.4 years); and disease severity as measured by the average Rutherford class scoring system (4.6 vs 4.97) and lesions per subject (1.4 vs 1.2). While the two cohorts were quite similar with respect to the prevalence of coronary artery disease (56 vs 54.7%) and prior MI (20 vs 19.6%), the trial population had a higher number of hypertension (HTN) patients (84 vs 60.8%), and past or current smokers (60 vs 43%). Conversely, the constructed BA cohort had a higher prevalence of diabetis mellitus (DM; 56 vs 65.9%) and renal insufficiency/dialysis (24 vs 35.3%) patients, although the magnitude of this difference was smaller than what was observed for HTN and smoking history as indicated above. Overall, it appears that the BA-only population of the CALCIUM 360° trial and the synthesized cohort may be considered as clinically comparable as there is no evidence of a major difference between the two cohorts. In any event, after replacing the rarer event estimates from CALCIUM 360° with those derived from the published literature, there was a small uptick in the incidence of all peri-operative complications (excluding dissection; see Table 3). The MAE rate for OAS + BA increased from 6.7 to 28.8% and this was primarily attributable to ATK amputation which increased from 0 to 8.1% and all-cause mortality which was amplified from 0 to 13.9%.
The scenario analysis evaluated the cost impact of the procedural plus 1-year composite outcome between the two treatment strategies. Cost savings averaged US$199,273 (US$1,166,960 vs US$1,366,233) for every 100 procedures or US$1993 per patient for the OAS + BA approach. A 10,000 trial Monte-Carlo simulation found that OAS + BA was dominant (i.e., lesser costs) in 49.2% of the trials. Among the remaining 50.8% of simulations, the mean cost difference (US$5338) and the number of lives lost between OAS + BA and BA-only was calculated. incremental cost effectiveness ratio estimating cost per life saved was thus estimated to be US$30,108, well below the accepted US$50,000 or US$100,000 thresholds. As such, the OAS + BA may be considered a dominant or cost-effective revascularization even using the conservative strategy of literature-derived values for rare events.
Discussion
PAD affects an estimated 8.9–16.1 million adults in the USA [35,36]. Estimates of the prevalence of PAD with CLI vary in the published literature primarily because of variations in the underlying at-risk patient profiles (e.g., older age, comorbidities such as DM, HTN and heart and kidney disease) being evaluated and the study design being deployed. A 2014 retrospective cohort study of insured adults ≥40 years of age estimated that the annualized prevalence of PAD patients with CLI was 1.33% [36]. Goodney et al. estimated that diagnosed CLI currently affected roughly 1 million Americans [3]. With an aging population, coupled with the escalating DM and other vascular disease groups, CLI is an epidemic that is on the rise.
Cost containment in healthcare has become an increasingly important objective in recent years. In such an environment, a thorough cost assessment of both short- and long-term impact of any clinically promising technology is crucial. As Barshes et al. note, ensuring the provision of optimal and cost-effective care is of very high priority to vascular surgeons in the USA for several reasons [37]. First, the US population is increasingly elderly and/or diabetic, two characteristics that are strongly associated with CLI. For instance, septuagenarians and octogenarians are projected to double and triple in size, respectively, by 2050 from their current numbers [38], and those with DM are expected to keep pace [39]. Second, care for CLI patients remains expensive, laborious and frequently results in limb loss despite intensive efforts to avoid it. The immediate cost directly attributed to amputation is greater than US$40,000 per visit, and the subsequent rehabilitation doubles these costs [40]. The lifetime per patient cost calculations for amputees suggest dollar amounts ranging between US$800,000 and US$1.81 million [41,42], which more than 1.4- to 3.2-times the lifetime medical cost for the average person (US$562,880) [43]. In addition, following an initial lower extremity amputation, 27% of patients will have one or more reamputation(s) within a year [18,44], and 40% progress to a higher level of limb loss within a year of receiving a minor amputation [44]. Evidence suggests that improper ischemic limb management adversely impacts survival and/or quality of life. Postamputation mortality rates are dismal, with 5-year mortality at 25.6–81.5% [18,24]. Considering these high complication and mortality rates, the cost of healthcare for an amputee becomes even more overwhelming.
Many amputees also suffer from increased anxiety, depression and lower quality of life overall [45,46]. Despite the initiation of limb salvage programs, race and/or ethnic origins appear to drive some of the ongoing inadequate vascular medicine practices. Multiple studies have demonstrated that African-Americans, Hispanics and Asians comprise a disproportionately higher proportion of patients admitted for CLI and undergoing amputation, with a lower proportion undergoing revascularization [47,48]. With the overall minority population growth rate projected to be in the double digits in the coming decades [38], finding ways to deliver quality and cost-effective care especially to those currently predisposed to poorer outcomes is critical. The ‘ideal’ CLI treatment pathway as recommended by the Society for Vascular Surgery and the European Society for Vascular Surgery suggests that 70% of patients should be revascularized, with the remaining undergoing primary amputation or palliative therapy [1]. Therefore, it is safe to assume that as the prevalence of PAD-CLI increases, the need for revascularization will continue to grow. A recent HCUP-based study found that atherectomy use in conjunction with angioplasty (with or without stenting) was associated with improved in-hospital outcomes including lower amputation rates, mortality and postprocedural complications [49]. New atherectomy technologies like OAS hold the possibility of improving safety and outcomes while controlling costs. But these technologies must be evaluated carefully to understand their potential clinical and economic value.
The present study is, to our knowledge, the first economic evaluation comparing the value of using OAS prior to performing a BA for the treatment of BTK in moderate-to severely calcified PAD-CLI patients. The results suggest that the OAS + BA approach is associated with postoperative 12-month cost savings of US$3509 per patient. While this may be attributable to the lower TLR/TVR and all-cause mortality rates which lead to treatment cost savings and lesser end-of-life care costs, these savings are expected to be realized over a 1-year follow-up time horizon. At the procedural visit level, the higher technology costs lead to an excess of US$2924 per patient. At 3 months, the cost difference between the two groups is estimated to decline to an additional US$1483 for OAS + BA. But by 6 months, lower revascularizations in the OAS + BA cohort lead to an overall cost savings of US$2360 per patient. This study suggests that an endovascular-first intervention strategy involving atherectomy by OAS prior to a BA for patients presenting with CLI and moderate-to-severely calcified BTK lesions can be supported even in a cost-conscious healthcare environment as it represents a dominant or cost-effective management approach, with cost savings realized from reduced AEs and complications over a 6–12-month period.
Limitations
We acknowledge there are several limitations to the current study. The OAS + BA parameters were derived from a single head-to-head RCT with a limited sample size and follow-up. Thus, these results must be viewed with caution. It is essential that the current results be validated using data from larger trial and real-world data sources when they become available. While the issue of small sample size for the BA arm was addressed by replacing the rare event trial data with evidence from the published literature, the latter still represented a mix of controlled trial and real-world experiences, a broader range of settings, and patient and physician profiles. Third, the model does not include costs attributed to differences between the two approaches in terms of labor, anesthesia time and operating room expenses as they are expected to be nominal. Fourth, data paucity prevented inclusion of infrequent but potentially relevant (e.g., allergic reaction to contrast agent, wound debridement) and/or expensive (e.g., BTK amputation visits, contrast nephropathy, infections, pulmonary edema) AEs. The study also compares only two interventions and does not consider, for instance, BA + stent procedures. Moreover, the study does not consider the impact on patient's health-related quality of life. This economic evaluation must be considered a preliminary investigation since it utilized only the 1-year postprocedure outcomes currently available for OAS + BA. Short-term impacts including 30- and 60-day outcomes (e.g., readmission) were not assessed in this study. Further follow-up is needed to fully explore the performance (clinical and economic) of the OAS + BA approach and its benefits to patients, stakeholders and society overall.
Conclusion
CLI remains a costly and resource-intensive condition to treat. Given an aging population and increasing prevalence of comorbid conditions recognized as PAD-CLI risk factors, the CLI burden is projected to increase. This analysis suggests that an interventional strategy involving atherectomy by OAS prior to a BA is associated with 6- and 12-month cost savings up to US$2360 and US$3509 per patient to the hospital/health system, respectively. The observed cost savings and OAS + BA's economic value were attributable to a reduced need for major amputation and TLR/TVR, and dollars spent toward end-of-life care despite high upfront technology costs. Sensitivity analyses revealed these findings were robust to the specified parameter value ranges. Larger trial and ‘real-world’ analyses will be useful in validating the current results and in further understanding the long-term impact and potential value of the OAS device in conjunction with a BA procedure.
This manuscript describes the model inputs, assumptions and results of a decision tree simulation model estimating the incremental cost of the Diamondback 360 peripheral orbital atherectomy system (OAS) plus balloon angioplasty (BA) versus BA-only for critical limb ischemia (CLI) patients with moderate/severe calcified lesions undergoing an endovascular revascularization in a US hospital.
The deterministic decision tree simulation model was constructed using clinical and healthcare utilization data obtained from the CALCIUM 360° trial. Cost data (2016 dollars) was obtained from published literature and government reports.
The incremental cost for performing OAS + BA versus BA-only included balloon, stent, and/or OAS-related differential usage costs during the procedure and perioperative complication and postoperative adverse event treatment costs at 3, 6 and 12-month time periods.
One-way and probabilistic sensitivity analyses were performed to gauge the model's robustness.
A scenario analysis was also performed where rare event (<5% incidence) data points in either of the treatment arms were replaced with values published rates derived from a best evidence review of the literature, and parameters were weighted by sample sizes of the eligible studies to obtain values for rare events.
At the procedural visit level, the higher technology costs lead to an excess of US$2924 per patient. At 3 months, the cost difference between the two groups is estimated to decline to an additional US$1483 for OAS + BA. At 6 months, lower revascularizations in the OAS + BA cohort lead to an overall cost savings of US$2360 per patient.
For every 100 procedures, the incremental annual costs to the hospital were US$350,930 lower with OAS + BA compared with BA-only. Despite higher upfront technology costs, the cost savings were realized due to a reduced need for revascularization in the target lesion and/or vessel (TLR/TVR), amputation and end-of-life care over a 6–12-month postoperative period.
Sensitivity analysis demonstrated that the model was most sensitive to the OAS device cost, TLR/TVR and mortality rates and their corresponding costs.
Compared to stand-alone BA, performing atherectomy with OAS prior to the BA procedure is associated with 1-year per-patient cost savings of US$3509 to the hospital.
This study suggests that an endovascular-first intervention strategy of atherectomy prior to a BA for patients presenting with CLI and moderate-to-severely calcified below the knee lesions can be supported even in a cost-conscious healthcare environment as it represents a cost-effective management approach (dominant), with cost savings realized from reduced adverse events and reduced complications over a 6–12-month period.
Financial & competing interests disclosure
This study was sponsored by Cardiovascular Systems, Inc (CSI), MN, USA. NW Shammas receives educational grants from CSI and educational and research grants from Boston Scientific and is the national principal investigator on the Calcium 360° trial. CW Boyes has consulting agreements with CSI and Cook. SR Palli was an employee at the time of analysis and JA Rizzo is a consultant to CTI Clinical Trial and Consulting Services Inc., which is a paid consultant to CSI. BJ Martinsen and H Kotlarz are employees of CSI, the study sponsor. JA Mustapha is a consultant to CSI. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Baser O, Verpillat P, Gabriel S, Wang L. Prevalence, incidence, and outcomes of critical limb ischemia in the US Medicare population. Vasc. Dis. Manage. 10(2), E26–E36 (2013).
2.
Henry AJ, Hevelone ND, Belkin M, Nguyen LL. Socioeconomic and hospital-related predictors of amputation for critical limb ischemia. J. Vasc. Surg. 53(2), 330.e331–339.e331 (2011).
3.
Goodney PP, Travis LL, Nallamothu BK et al. Variation in the use of lower extremity vascular procedures for critical limb ischemia. Circ. Cardiovasc. Qual. Outcomes 5(1), 94–102 (2012).
4.
Mustapha JA, Diaz-Sandoval LJ. Arterial deposition of calcium and outcomes of peripheral interventions: is it time to redefine the “gold standard?” Vasc. Dis. Manage. 10(10), E208–E211 (2013).
5.
Hirsch AT, Haskal ZJ, Hertzer NR et al. ACC/AHA 2005 guidelines for the management of patients with peripheral arterial disease (lower extremity, renal, mesenteric, and abdominal aortic): executive summary a collaborative report from the American Association for Vascular Surgery/Society for Vascular Surgery, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, Society of Interventional Radiology, and the ACC/AHA Task Force on Practice Guidelines (Writing Committee to Develop Guidelines for the Management of Patients With Peripheral Arterial Disease) endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation; National Heart, Lung, and Blood Institute; Society for Vascular Nursing; TransAtlantic Inter-Society Consensus; and Vascular Disease Foundation. J. Am. Coll. Cardiol. 47(6), 1239–1312 (2006).
6.
Weinstock B, Dattilo R, Diage T. Cost–effectiveness analysis of orbital atherectomy plus balloon angioplasty vs balloon angioplasty alone in subjects with calcified femoropopliteal lesions. Clinicoecon. Outcomes Res. 6, 133–139 (2014).
• Evaluated the 1-year index procedure cost and cost–effectiveness for orbital atherectomy system + balloon angioplasty (BA) versus BA-alone in above-the-knee calcified lesions and presented evidence indicating atherectomy's cost–effectiveness and advocating their use for treatment of calcified femoropopliteal lesions.
7.
Iida O, Nanto S, Uematsu M, Ikeoka K, Okamoto S, Nagata S. Influence of stent fracture on the long-term patency in the femoro-popliteal artery: experience of 4 years. J. Am. Coll. Cardiol. Intv 2(7), 665–671 (2009).
8.
Adams GL, Khanna PK, Staniloae CS, Abraham JP, Sparrow EM. Optimal techniques with the Diamondback 360 degrees system achieve effective results for the treatment of peripheral arterial disease. J. Cardiovasc. Transl. Res. 4(2), 220–229 (2011).
• Presents a detailed evidence surrounding the orbital atherectomy device concept and design along with and its effectiveness.
9.
Safian RD, Niazi K, Runyon JP et al. Orbital atherectomy for infrapopliteal disease: device concept and outcome data for the OASIS trial. Catheter Cardiovasc. Interv. 73(3), 406–412 (2009).
10.
Das T, Mustapha J, Indes J et al. Technique optimization of orbital atherectomy in calcified peripheral lesions of the lower extremities: the CONFIRM series, a prospective multicenter registry. Catheter Cardiovasc. Interv. 83(1), 115–122 (2014).
• Presents the results of the CONFIRM registry series evaluating the use of orbital atherectomy peripheral lesions of the lower extremities as calcified arteries are a strong predictor of angioplasty treatment failure ultimately leading to amputations.
11.
Shammas NW, Lam R, Mustapha J et al. Comparison of orbital atherectomy plus balloon angioplasty vs balloon angioplasty alone in patients with critical limb ischemia: results of the CALCIUM 360 randomized pilot trial. J. Endovasc. Ther. 19(4), 480–488 (2012).
•• The results of the CALCIUM 360 randomized clinical trial, a key resource for the clinical parameters of the current study, are discussed.
12.
Dattilo R, Himmelstein SI, Cuff RF. The COMPLIANCE 360 degrees Trial: a randomized, prospective, multicenter, pilot study comparing acute and long-term results of orbital atherectomy to balloon angioplasty for calcified femoropopliteal disease. J. Invasive Cardiol. 26(8), 355–360 (2014).
13.
Brosa M, Gisbert R, Rodriguez JM, Soto J. Principios, métodos y aplicaciones del análisis del impacto presupuestario en el sector sanitario. PharmacoEconomics Spanish Res. Articles 2(2), 65–78 (2005).
14.
Cardiovascular Systems, Inc. Proprietary data on file. Provided by CSI on 14 January 2016.
15.
Agency for Healthcare Research and Quality. Healthcare cost and utilization project nationwide inpatient sample. http://hcupnet.ahrq.gov/.
16.
Ha CD, Calcagno D. Amplatzer vascular plug to occlude the internal iliac arteries in patients undergoing aortoiliac aneurysm repair. J. Vasc. Surg. 42(6), 1058–1062 (2005).
17.
Garrison LP Jr, Lewin J, Young CH et al. The clinical and cost burden of coronary calcification in a Medicare cohort: an economic model to address under-reporting and misclassification. Cardiovasc. Revasc. Med. 16(7), 406–412 (2015).
18.
Jindeel A, Narahara KA. Nontraumatic amputation: incidence and cost analysis. Int. J. Low Extrem. Wounds 11(3), 177–179 (2012).
19.
Grossi EA, Moore M, Mallow PJ, Rizzo JR. The cost of an operating room minute for heart valve procedures. JHEOR 2(2), 170–180 (2015).
20.
United States Bureau of Labor Statistics. US medical care consumer price index 2016. http://data.bls.gov/cgi-bin/surveymost?cu.
21.
Diehr P, Yanez D, Ash A, Hornbrook M, Lin DY. Methods for analyzing health care utilization and costs. Annu. Rev. Public Health 20, 125–144 (1999).
22.
Adam DJ, Beard JD, Cleveland T et al. Bypass versus angioplasty in severe ischaemia of the leg (BASIL): multicentre, randomised controlled trial. Lancet 366(9501), 1925–1934 (2005).
23.
Liistro F, Porto I, Angioli P et al. Drug-eluting balloon in peripheral intervention for below the knee angioplasty evaluation (DEBATE-BTK): a randomized trial in diabetic patients with critical limb ischemia. Circulation 128(6), 615–621 (2013).
24.
Faglia E, Clerici G, Clerissi J et al. Early and five-year amputation and survival rate of diabetic patients with critical limb ischemia: data of a cohort study of 564 patients. Eur. J. Vasc. Endovasc. Surg. 32(5), 484–490 (2006).
25.
Ferraresi R, Centola M, Ferlini M et al. Long-term outcomes after angioplasty of isolated, below-the-knee arteries in diabetic patients with critical limb ischaemia. Eur. J. Vasc. Endovasc. Surg. 37(3), 336–342 (2009).
26.
Scheinert D, Katsanos K, Zeller T et al. A prospective randomized multicenter comparison of balloon angioplasty and infrapopliteal stenting with the sirolimus-eluting stent in patients with ischemic peripheral arterial disease: 1-year results from the ACHILLES trial. J. Am. Coll. Cardiol. 60(22), 2290–2295 (2012).
27.
Conrad MF, Kang J, Cambria RP et al. Infrapopliteal balloon angioplasty for the treatment of chronic occlusive disease. J. Vasc. Surg. 50(4), 799.e794–805.e794 (2009).
28.
Zeller T, Baumgartner I, Scheinert D et al. Drug-eluting balloon versus standard balloon angioplasty for infrapopliteal arterial revascularization in critical limb ischemia: 12-month results from the IN.PACT DEEP randomized trial. J. Am. Coll. Cardiol. 64(15), 1568–1576 (2014).
29.
Bosiers M, Peeters P, D'archambeau O et al. AMS INSIGHT – absorbable metal stent implantation for treatment of below-the-knee critical limb ischemia: 6-month analysis. Cardiovasc. Intervent. Radiol. 32(3), 424–435 (2009).
30.
Zeller T, Beschorner U, Pilger E et al. Paclitaxel-coated balloon in infrapopliteal arteries: 12-month results from the BIOLUX P-II randomized trial (BIOTRONIK'S-First in Man study of the Passeo-18 LUX drug releasing PTA balloon catheter vs the uncoated Passeo-18 PTA balloon catheter in subjects requiring revascularization of infrapopliteal arteries). J. Am. Coll. Cardiol. Intv. 8(12), 1614–1622 (2015).
31.
Iida O, Soga Y, Hirano K et al. Midterm outcomes and risk stratification after endovascular therapy for patients with critical limb ischaemia due to isolated below-the-knee lesions. Eur. J. Vasc. Endovasc. Surg. 43(3), 313–321 (2012).
32.
Nakano M, Hirano K, Iida O et al. Prognosis of critical limb ischemia in hemodialysis patients after isolated infrapopliteal balloon angioplasty: results from the Japan below-the-knee artery treatment (J-BEAT) registry. J. Endovasc. Ther. 20(1), 113–124 (2013).
33.
Bradbury AW, Adam DJ, Bell J et al. Bypass versus Angioplasty in Severe Ischaemia of the Leg (BASIL) trial: an intention-to-treat analysis of amputation-free and overall survival in patients randomized to a bypass surgery-first or a balloon angioplasty-first revascularization strategy. J. Vasc. Surg. 51(5 Suppl.), S 5–S17 (2010).
34.
Romiti M, Albers M, Brochado-Neto FC, Durazzo AE, Pereira CA, De Luccia N. Meta-analysis of infrapopliteal angioplasty for chronic critical limb ischemia. J. Vasc. Surg. 47(5), 975–981 (2008).
35.
Pande RL, Perlstein TS, Beckman JA, Creager MA. Secondary prevention and mortality in peripheral artery disease: National Health and Nutrition Examination Study, 1999 to 2004. Circulation 124(1), 17–23 (2011).
36.
Nehler MR, Duval S, Diao L et al. Epidemiology of peripheral arterial disease and critical limb ischemia in an insured national population. J. Vasc. Surg. 60(3), 686.e682–695.e682 (2014).
37.
Barshes NR, Chambers JD, Cohen J, Belkin M. Cost–effectiveness in the contemporary management of critical limb ischemia with tissue loss. J. Vasc. Surg. 56(4), 1015.e1011–1024.e1011 (2012).
38.
Ortman JM, Velkoff VA, Hogan H. An aging nation: the older population in the United States, current population reports, P25–1140. US Census Bureau, Washington, DC, USA (2014). www.census.gov/prod/2014pubs/p25-1140.pdf.
39.
Boyle JP, Thompson TJ, Gregg EW, Barker LE, Williamson DF. Projection of the year 2050 burden of diabetes in the US adult population: dynamic modeling of incidence, mortality, and prediabetes prevalence. Popul. Health Metr. 8, 29 (2010).
40.
Norgren L, Hiatt WR, Dormandy JA, Nehler MR, Harris KA, Fowkes FG. Inter-society consensus for the management of peripheral arterial disease (TASC II). J. Vasc. Surg. 45(Suppl. S), S5–S67 (2007).
41.
Mackenzie EJ, Jones AS, Bosse MJ et al. Health-care costs associated with amputation or reconstruction of a limb-threatening injury. J. Bone Joint Surg. Am. 89(8), 1685–1692 (2007).
• The substantial lifetime cost burden following amputations are estimated.
42.
Blough DK, Hubbard S, Mcfarland LV, Smith DG, Gambel JM, Reiber GE. Prosthetic cost projections for servicemembers with major limb loss from Vietnam and OIF/OEF. J. Rehabil. Res. Dev. 47(4), 387–402 (2010).
43.
Alemayehu B, Warner KE. The lifetime distribution of health care costs. Health Serv. Res. 39(3), 627–642 (2004).
44.
Dillingham TR, Pezzin LE, Shore AD. Reamputation, mortality, and health care costs among persons with dysvascular lower-limb amputations. Arch. Phys. Med. Rehabil. 86(3), 480–486 (2005).
45.
Remes L, Isoaho R, Vahlberg T, Viitanen M, Koskenvuo M, Rautava P. Quality of life three years after major lower extremity amputation due to peripheral arterial disease. Aging Clin. Exp. Res. 22(5–6), 395–405 (2010).
46.
Amputee Coalition of America. Limb Loss Research & Statistics Program. www.amputee-coalition.org/wp-content/uploads/2014/09/lsp_people-speak-out_191214–012622.pdf.
47.
Hughes K, Seetahal S, Oyetunji T et al. Racial/ethnic disparities in amputation and revascularization: a nationwide inpatient sample study. Vasc. Endovascular Surg. 48(1), 34–37 (2014).
48.
Loja MN, Brunson A, Li CS et al. Racial disparities in outcomes of endovascular procedures for peripheral arterial disease: an evaluation of California hospitals, 2005–2009. Ann. Vasc. Surg. 29(5), 950–959 (2015).
49.
Panaich SS, Arora S, Patel N et al. In-hospital outcomes of atherectomy during endovascular lower extremity revascularization. Am. J. Cardiol. 117(4), 676–684 (2016).
Information & Authors
Information
Published In
Copyright
© 2017 Shammas et al.
History
Received: 5 September 2017
Accepted: 10 October 2017
Published online: 26 October 2017
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Hospital cost impact of orbital atherectomy with angioplasty for critical limb ischemia treatment: a modeling approach. (2017) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2017-0070
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Rajiv Parakh, undefined Vivekananda, Vimal Someshwar, Tarun Grover, Robbie George, Vijay Thakore, Mathew Cherian, Virender Sheorain, Varinder S Bedi, Prem Chand Gupta, Ajay Yadav, Raghuram Sekhar, Tapish Sahu, Ravul Jindal, Surinder Kher, Orbital Atherectomy in the Treatment of Calcified Peripheral Arteries: An Evidence- and Survey-based Position Paper, Indian Journal of Vascular and Endovascular Surgery, 10.4103/ijves.ijves_12_26, 13, 2, (245-255), (2026).
- Keith Pereira, Tools for Plaque Modification in Peripheral Arterial Disease, Techniques in Vascular and Interventional Radiology, 10.1016/j.tvir.2026.101104, 29, 1, (101104), (2026).
- Jeffrey G. Carr, Ralf Langhoff, Brian G. DeRubertis, Kristin L. Hood, Prakash Krishnan, Vikram Puttaswamy, Thomas Zeller, Eric A. Secemsky, Published Evidence on Peripheral Atherectomy: A Meta-analysis and Systematic Literature Review of More Than 300 Original Investigations, Journal of the Society for Cardiovascular Angiography & Interventions, 10.1016/j.jscai.2025.104009, 4, 11, (104009), (2025).
- Jun Li, Ramon Varcoe, Marco Manzi, Steven Kum, Osamu Iida, Andrej Schmidt, Mehdi H. Shishehbor, Below-the-Knee Endovascular Revascularization, JACC: Cardiovascular Interventions, 10.1016/j.jcin.2023.11.040, 17, 5, (589-607), (2024).
- Haichao Wu, Dandan Zheng, Long Zhou, Qiang Wang, Tao Wang, Siyuan Liang, A Systematic Review and Meta-analysis of Atherectomy Plus Balloon Angioplasty Versus Balloon Angioplasty Alone for Infrapopliteal Arterial Disease, Journal of Endovascular Therapy, 10.1177/15266028231209236, 32, 4, (957-968), (2023).
- Kevin Herman, John H. Rundback, Atherectomy Before Angioplasty or Stenting for Peripheral Arterial Disease: Point—The Data Indicate That Atherectomy Before Definitive Endovascular Therapy Is Beneficial, American Journal of Roentgenology, 10.2214/AJR.22.28517, 220, 5, (642-643), (2023).
- Naoya Kurata, Osamu Iida, Mitsutoshi Asai, Shin Okamoto, Takayuki Ishihara, Kiyonori Nanto, Takuya Tsujimura, Yosuke Hata, Taku Toyoshima, Naoko Higashino, Sho Nakao, Toshiaki Mano, Factors in Sufficient Endovascular Vessel Preparation for Severely Calcified Femoropopliteal Lesions, Circulation Journal, 10.1253/circj.CJ-22-0444, 87, 3, (424-431), (2023).
- Krishna Jain, Mekala Neelakantan, Phillip Key, Limitations in the Analysis of Atherectomy Using Medicare Big Data, Journal of Endovascular Therapy, 10.1177/1526602820951917, 28, 1, (117-122), (2020).