Therapeutic approach for patients with venous thromboembolism attended in emergency departments during routine clinical practice: the EDITH study
Abstract
Aim: To analyze treatment at discharge/follow-up of patients diagnosed with venous thromboembolism (VTE) in the emergency department (ED). Materials & methods: Ambispective study (50 Spanish centers) of consecutive patients (October–December 2014) with VTE diagnosed in ED. Results: VTE was diagnosed in 775 patients (295 pulmonary embolism [PE] without deep vein thrombosis [DVT], 389 DVT without PE and 91 PE + DVT); 95.5% received anticoagulants (90.7% low-molecular-weight heparin [LMWH], 4% LMWH + vitamin K antagonists and <1% direct oral anticoagulants). Overall, 23.3% were discharged from ED and 74.5% hospitalized (98.6% with PE and 50.4% with DVT). After discharge/90/180 days, 43.6/21.0/13.5% were taking LMWH, with similar rates in nononcologic patients. Conclusion: There is a poor adherence to international guidelines in management of VTE patients in Spain.
The main objectives of treatment of venous thromboembolism (VTE) are to prevent thrombus extension and development of pulmonary embolism (PE) and to reduce the risk of recurrence. In addition, during long-term follow-up, treatment of VTE should prevent late relapses and complications such as post-thrombotic syndrome (PTS) and chronic thromboembolic pulmonary hypertension. Traditionally, the treatment of VTE has been divided into three phases: the initial treatment phase (usually the first 5–10 days), which corresponds to the period when patients historically have been treated with parenteral therapy; the short-term or classically long-term treatment phase (next 3–6 months) and the long-term or classically extended treatment phase (beyond 3–6 months) [1]. Until recently, the only oral anticoagulants available were vitamin K antagonists (VKAs). Clinical guidelines recommend parenteral anticoagulation therapy with early initiation of oral anticoagulation for the prevention of recurrence of VTE in nononcologic patients, the therapeutic strategy being similar for patients with PE and for patients with deep vein thrombosis (DVT). The decision to continue anticoagulant treatment in patients with VTE at moderate risk of recurrence beyond the first 3 months (extended treatment phase) is based on balance between the risk of recurrence and bleeding. In patients with cancer, the recommendation is to continue with parenteral anticoagulation, namely, low-molecular-weight heparin (LMWH). Patients presenting uncorrected risk factors and patients with unprovoked VTE may receive extended therapy, provided that the risk of bleeding is not excessive [1].
Epidemiological studies performed in Spain have shown that patients are treated and followed mainly at hospital and less frequently in primary care. In these studies, differences were reported in the duration of follow-up, monitoring and prescription of treatments depending on the physicians’ medical specialty and type of VTE [2].
The development of direct oral anticoagulants (DOACs) [3], the possibility of outpatient control for selected patients (including those with PE) [4] and the identification of new predictors of the risk of recurrence [5] have changed the management of patients with VTE in recent years. Analysis of the therapeutic strategies selected for specific cases and the events occurring during follow-up of patients with previous VTE could facilitate the recognition of gaps in practice, and consequently, lead to an improvement in secondary prevention. Furthermore, little is known about the therapeutic management of VTE in the emergency department (ED) or about how it is modified during follow-up.
The primary objective of this study was to analyze the therapeutic approach to patients diagnosed with VTE in the ED, with a particular focus on treatment at discharge after admission and during follow-up. The secondary objectives of the study were to assess the modifications of treatment during follow-up, to analyze the evolution of patients (VTE recurrence and bleeding risk), the consumption of healthcare resources (hospital length of stay, regular visits to the specialist or primary care physician, unscheduled visits and mean duration of treatment), as well as gaps between clinical practice and guidelines.
Materials & methods
Study design & inclusion criteria
We performed an epidemiological, observational and ambispective study in 50 centers throughout Spain. The study population comprised consecutive patients aged ≥18 years with a diagnosis of VTE confirmed by objective testing in the ED between October and December 2014 and with available data for the 6-month period after discharge. The study was approved by the Institutional Ethics Committee of Hospital Clínic, Barcelona (Spain) and was conducted in accordance with the principles of the Declaration of Helsinki. All patients signed the written informed consent document before inclusion.
Study variables & data collection
Investigators retrospectively collected data on demographics, comorbidities and VTE risk factors. Data were also collected in relation to the therapeutic management of patients diagnosed with VTE in the ED, as follows: pharmacological and nonpharmacological treatments administered during the ED visit and at discharge from the ED; modifications to treatment during admission and at discharge from hospital; modifications to treatment during follow-up at 30, 90 and 180 days; and reasons for changing therapy. We also evaluated the length of stay for hospitalized patients.
We recorded the following: number of VTE recurrences, bleeding events, hospitalizations and deaths; number of care visits to the specialist or the primary care physician; the medical specialty responsible for clinical follow-up; and the number of unscheduled visits. We excluded patients for whom the data necessary to evaluate the study objectives were missing from their clinical history.
Data were collected by reviewing the clinical histories of each hospital and consulting administrative healthcare databases. Data were compared according to the presence of PE with or without DVT and isolated DVT.
Statistical analysis
Data were summarized using descriptive statistics. Continuous variables were expressed as the mean, median, standard deviation and interquartile ranges. Categorical values were expressed as absolute and relative frequencies. The χ2 or the Fisher’s exact test was used for comparisons of qualitative variables while the Student’s t-test for quantitative variables. Differences between groups were considered statistically significant with p < 0.05. Statistical analyses were performed using the SAS® 9.3 software (SAS Institute Inc., NC, USA).
Results
Baseline clinical characteristics of the study population
A total of 795 patients were recruited but 20 patients were excluded from the study, since they did not meet all the inclusion criteria (19 patients were not diagnosed with VTE in the ED and in one patient, data from follow-up were not allowed). As a result, a total of 775 patients (97.5%) with VTE were included: 386 with PE (91 also with DVT) and 389 with DVT (Figure 1). Mean age was 66.3 ± 17.3 years, and 47.7% of patients (n = 370) were men. The baseline clinical characteristics of the study population are shown in Table 1. Active cancer was recorded in 15.3% of patients.

Figure 1. Patients’ flow diagram after discharge from emergency department (n,%).
DVT: Deep venous thrombosis; ED: Emergency department; ICU: Intensive care unit; PE: Pulmonary embolism; SSU: Short stay unit; VTE: Venous thromboembolism.
| Variable | Value |
|---|---|
| n | 775 |
| Age, years: – Mean ± SD – Median (IQR) | 66.3 ± 17.3 70 (55–79) |
| Gender, male (n, %) | 370 (47.7) |
| Body mass index (n, %): – Underweight (<18.5 kg/m2) – Normal weight (18.5–24.99 kg/m2) – Overweight (25–29.99 kg/m2) – Obesity (≥30 kg/m2) | 16 (2.1%) 206 (26.6%) 311 (40.1%) 242 (31.2%) |
| Type of VTE (n, %): – PE – DVT – PE + DVT | 295 (38.1%) 389 (50.2%) 91 (11.7%) |
| Active smoker (n, %) | 104 (13.4%) |
| Comorbidities (n, %): – Hypertension – Dyslipidemia – Diabetes – Ischemic heart disease – Chronic obstructive pulmonary disease – Rheumatic disease – Stroke – Dementia – Chronic renal disease – Alcoholism – Heart failure – Others† | 410 (52.9%) 269 (34.7%) 89 (11.5%) 70 (9.0%) 68 (8.8%) 61 (7.9%) 57 (7.3%) 53 (6.8%) 45 (5.8%) 42 (5.4%) 39 (5.0%) 141 (18.2%) |
| VTE risk factors (n, %): – Immobilization – Previous VTE – Active neoplasm – Hospitalization before VTE – Surgery before VTE – Infection before VTE – Hormonal therapy – Trauma before VTE – Others‡ | 181 (23.3%) 134 (17.3%) 119 (15.4%) 89 (11.5%) 80 (10.3%) 53 (6.8%) 50 (6.4%) 48 (6.2%) 45 (5.8%) |
†Other includes various pulmonary diseases, obstructive sleep apnea syndrome, atrial fibrillation, peripheral artery disease, inflammatory bowel disease and HIV/AIDS.
‡Other includes previous thrombophilia, 6-h journey in the last 3 weeks, respiratory insufficiency, postpartum period and third trimester of pregnancy.
DVT: Deep vein thrombosis; IQR: Interquartile range; PE: Pulmonary embolism; SD: Standard deviation; VTE: Venous thromboembolism.
Therapeutic management in the ED
Overall, 740 patients (95.5%) started anticoagulant treatment in the ED, mainly LMWH (Table 2). The most common LMWH prescribed in the ED was enoxaparin. Only 4% of patients were taking LMWH and VKAs concomitantly, and less than 1% were receiving DOACs.
| Treatment | Overall | PE | DVT | p-value |
|---|---|---|---|---|
| n | 775 | 386 | 389 | – |
| Anticoagulant treatment started in the ED (n, %) | 740 (95.5) | 374 (96.9) | 366 (94.1) | NS |
| LMWH†: – Enoxaparin‡ – Bemiparin‡ – Tinzaparin‡ – Dalteparin‡ | 671 (90.7) 556 (82.9) 115 (17.1) 24 (3.6) 22 (3.3) | 335 (89.6) 290 (86.6) 45 (13.4) 9 (2.7) 15 (4.5) | 336 (91.8) 266 (79.2) 70 (20.8) 15 (4.5) 7 (2.1) | NS 0.03 0.01 NS NS |
| LMWH plus VKA† | 30 (4.1) | 14 (3.7) | 16 (4.4) | NS |
| DOACs† | 7 (0.9) | 4 (1.1) | 3 (0.8) | NS |
| Unfractionated heparin† | 16 (2.1) | 10 (2.7) | 6 (1.6) | NS |
| Other treatments§: – Oxygen therapy – Analgesics – Plasma expanders – Fibrinolysis – Percutaneous thrombus removal – Surgical thrombus removal – Inotropic agents – Inferior vena cava filter | 325 (43.9) 374 (50.5) 12 (17.1) 7 (0.9) 5 (0.7) 0 3 (0.4) 5 (0.6) | 311 (80.6) 158 (40.9) 12 (3.1) 7 (1.8) 3 (0.8) 0 3 (0.8) 4 (1) | 14 (3.6) 216 (55.2) 0 0 2 (0.5) 0 0 1 (0.2) | <0.01 <0.01 0.04 0.03 NS NS NS NS |
†Among all anticoagulated patients.
‡Among all patients anticoagulated with LMWH.
§Among all patients; +in the ED, among all DOACs, only rivaroxaban was prescribed.
DOAC: Direct oral anticoagulant; DVT: Deep vein thrombosis; ED: Emergency department; LMWH: Low-molecular-weight heparin; NS: Non-significant; PE: Pulmonary embolism; VKA: Vitamin K antagonist.
In-hospital treatment & complications
A total of 181 patients (23.3%) were discharged from the ED and 577 (74.5%) were hospitalized. Mean and median length of stay were 10.1 and 8 days, respectively, for PE patients and 5.8 and 4 days for DVT patients. The most common anticoagulant therapy prescribed during hospitalization was heparin monotherapy (51.3%); heparin and VKAs were taken concomitantly in 38.3%. Complications during hospital stay were recorded in 43 patients (9.1%), including 25 bleeding events, six recurrences of VTE and 12 other fatal complications (Table 3). Complications during hospitalization according to anticoagulant therapy are shown in Table 4. No significant differences were found regarding bleeding and recurrences according to the type of anticoagulant. However, death was more common in patients taking LMWH than in patients taking LMWH plus VKA (p = 0.0003).
| Treatment/complications | Overall | PE | DVT | p-value |
|---|---|---|---|---|
| n | 577† | 381† | 196† | – |
| Hospital stay, days (mean) | 8.1 | 10.1 | 5.8 | <0.01 |
| Median (IQR) | – | 8 (6–11) | 4 (2–7) | <0.01 |
| Anticoagulant therapy (n, %): – LMWH only‡ – LMWH plus VKA‡ – VKA only – DOACs‡ | 554 (96.0) 296 (51.3) 221 (38.3) 28 (4.8) 9 (1.5) | 371 (97.4) 176 (47.4) 167 (43.8) 22 (5.8) 6 (1.6) | 183 (93.4) 120 (65,6) 54 (27,5) 6 (3) 3 (1.5) | 0.03 <0.01 <0.01 0.03 NS |
| Any bleeding (n, %) | 25 (4.5) | 21 (5.7) | 4 (2.2) | <0.01 |
| Bleeding complications‡ | ||||
| Major bleeding: – Fatal bleeding – Critical organ bleeding – Decrease in hemoglobin ≥2 g/dl, or bleeding leading to transfusion of ≥2 units of whole blood or red cells | 3 (0.5) 0 2 (0.4) 1 (0.2) | 2 (0.5) 0 1 (0.3) 1 (0.3) | 1 (0.5) 0 1 (0.5) 0 | NS NS NS NS |
| Nonmajor clinically relevant bleeding | 8 (1.4) | 7 (1.9) | 1 (0.5) | 0.03 |
| No clinically relevant bleeding | 14 (2.5) | 12 (3.2) | 2 (1) | 0.01 |
| Recurrences ‡ | 6 (1.1) | 6 (1.1) | 2 (1.1) | NS |
| PE | 2 (0.4) | 2 (0.5) | 0 | NS |
| DVT | 3 (0.5) | 2 (0.5) | 2 (0.5) | NS |
| PE + DVT | 1 (0.2) | 0 | 0 | NS |
| Mortality § | 19 (3.3) | 14 (3.7) | 5 (2.5) | NS |
| Bleeding | 0 | 0 | 0 | NS |
| Recurrence | 7 (1.2) | 6 (1.6) | 1 (0.5) | NS |
| Others | 12 (2.1) | 8 (2.1) | 4 (2) | NS |
†Among all hospitalized patients.
‡Among all anticoagulated patients.
§Among all patients.
DOAC: Direct oral anticoagulant; DVT: Deep vein thrombosis; IQR: Interquartile range; LMWH: Low-molecular-weight heparin; NS: Non-significant; PE: Pulmonary embolism; VKA: Vitamin K antagonist.
| Complications | LMWH only | LMWH plus VKA | VKA only | DOACs |
|---|---|---|---|---|
| n | 296 | 221 | 28 | 9 |
| Any bleeding† | 9 (3.0) | 14 (6.3) | 0 | 0 |
| Bleeding complications | ||||
| Major bleeding: – Fatal bleeding – Critical organ bleeding – Decrease in hemoglobin ≥2 g/dl, or bleeding leading to transfusion of ≥2 units of whole blood or red cells | 1 (0.3) 0 1 (0.3) 0 | 1 (0.5) 0 0 1 | 0 0 0 0 | 0 0 0 0 |
| Nonmajor clinically relevant bleeding | 3 (1.0) | 4 (1.8) | 0 | 0 |
| No clinically relevant bleeding | 5 (1.7) | 9 (4.1) | 0 | 0 |
| Recurrences ‡ | 2 (0.7) | 2 (0.9) | 1 (3.6) | 0 |
| PE | 1 (0.3) | 1 (0.5) | 0 | 0 |
| DVT | 1 (0.3) | 1 (0.5) | 0 | 0 |
| PE + DVT | 0 | 0 | 1 (3.6) | 0 |
| Mortality § | 17 (5.7) | 0 | 0 | 0 |
| Bleeding | 0 | 0 | 0 | 0 |
| Recurrence | 6 (2.0) | 0 | 0 | 0 |
| Others | 11 (3.7) | 0 | 0 | 0 |
†p = NS between LMWH only and LMWH plus VKA.
‡p = NS between LMWH only and LMWH plus VKA.
§p = 0.0003 between LMWH only and LMWH plus VKA.
DOAC: Direct oral anticoagulant; DVT: Deep vein thrombosis; LMWH: Low-molecular-weight heparin; NS: Non-significant; PE: Pulmonary embolism; VKA: Vitamin K antagonist.
Treatment at discharge & during follow-up
The most common anticoagulant therapy prescribed at discharge was heparin alone (49.5%) followed by VKAs (27.2%). DOACs were administered very infrequently (Table 5). After discharge from hospital, all patients were referred to a specialist, and 377 (55.9%) were also followed by the primary care physician.
| Treatment | Overall (n,%) | PE (n,%) 381 | DVT (n,%) 196 | p-value |
|---|---|---|---|---|
| LMWH | 374 (49.5) | 125 (33.6) | 249 (65.0) | <0.01 |
| LMWH + VKA† | 143 (18.9) | 63 (16.9) | 80 (20.9) | <0.01 |
| VKA† | 205 (27.2) | 164 (44.1) | 41 (10.7) | <0.01 |
| Direct oral anticoagulants | 17 (2.3) | 10 (2.7) | 7 (1.8) | NS |
| None | 16 (2.1) | 10 (2.7) | 6 (1.6) | NS |
†Acenocoumarol or warfarin.
DVT: Deep vein thrombosis; LMWH: Low-molecular-weight heparin; NS: Non-significant; PE: Pulmonary embolism; VKA: Vitamin K antagonist.
A total of 670 patients (86.5%) completed the 6-month follow-up period. Figure 2 shows the anticoagulant therapy prescribed from discharge to 6 months of follow-up.
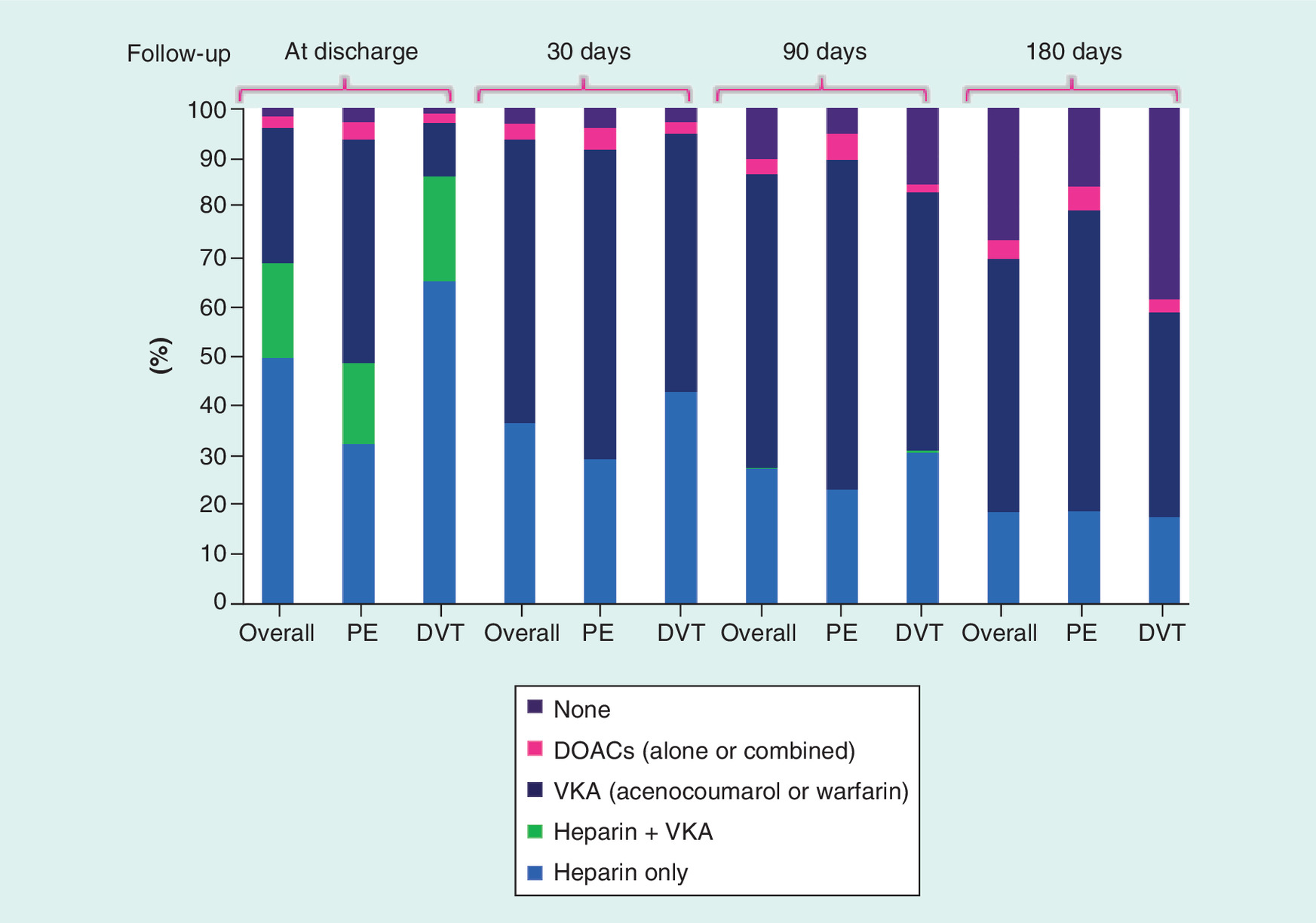
Figure 2. Anticoagulant therapy from discharge to the end of follow-up.
DOAC: Direct oral anticoagulant; DVT: Deep vein thrombosis; PE: Pulmonary embolism; VKA: Vitamin K antagonist.
30 days after discharge, patients were receiving monotherapy with LMWH (36.6%), VKAs (56.7%) or DOACs (3.0%). The most common reasons for change of anticoagulant therapy were dose adjustment (34.8%), physician’s indication (22.6%), initiation of DOACs (10.5%), bleeding complication (3.9%), VTE recurrence/relapse (3.3%) and other (20.3%). During the first month after discharge, 467 patients were attended in a healthcare service (67.2, 70.2% of patients with DVT and 62.1% of patients with PE), mainly the primary care setting (48.0%) and hematology department (33.8%).
At 90 days after discharge, 84.4% of DVT patients and 94.6% of PE patients remained on anticoagulants. At this time, 462 patients (70.6%) were attended by primary care physicians (48.0%), hematologists (25.1%) and internists (22.1%).
After 180 days of follow-up, 61.2% of patients and 85.2% of PE patients remained on anticoagulant therapy. At the end of the study, patients were receiving monotherapy with LMWH (18.7%), VKAs (50.7%) or DOACs (3.7%). Between the third and sixth months of follow-up, anticoagulant therapy was changed in 41.6% of DVT patients and 25.4% of PE patients. The most common reason for changing anticoagulant therapy was dose adjustment. At this time, 407 patients (66.3%) were attended by primary care physicians (48.2%), hematologists (23.6%) and internists (21.9%).
Overall, 114 bleeding events were reported in 99 patients (12.8%): 25 during hospitalization and 89 during the 6-month follow-up period. 19 major bleeds were recorded during the study (three during hospitalization and 16 during the 6-month follow-up period). 32 patients (4.1%) had a recurrence of VTE, six during hospitalization and 26 after discharge. A total of 90 patients (11.6%) died during the study (71 after discharge, mainly due to other causes different to VTE recurrence [6.7%] or bleeding [7.8%]). 33 (36.7%) patients died due to cancer. Median time (interquartile range) to the first bleed, the first recurrence of VTE and death was 25.8 (8.0–25.0), 32.0 (8.5–72.5) and 44.0 (24.0–80.0) days, respectively.
Antithrombotic treatment in nononcologic patients
Of the 775 patients included, 656 (84.7%) were nononcologic patients. Mean and median (interquartile range) duration of anticoagulant treatment were 5.4 and 5.8 (5.6–5.9) months, respectively, for PE patients, and 5.0 and 5.9 (3.9–6.1) months for DVT patients. In the ED, the most common anticoagulant therapy prescribed was LMWH (91.7% in PE patients and 88.2% in DVT patients); 3.7% of PE patients and 4.9% of DVT patients were treated with VKA or heparin followed by VKA and 1.2% of PE patients and 0.9% of DVT patients were treated with DOACs. At discharge, 41.1% of PE patients and 56.7% of DVT patients were receiving LMWH; 48.3% of PE patients and 31.7% of DVT patients were receiving heparin followed by VKA. These numbers were 6.9 and 3.7% for VKA alone and 1.9 and 1.8%, respectively, for DOACs. At 180 days, 14.7% of PE patients and 40.1% of DVT patients were not receiving any anticoagulant treatment; 13.6% of PE patients and 13.4% of DVT patients were receiving LMWH. These percentages were 66.4 and 43.5% for VKA and 5.2 and 3.0% for DOACs, respectively (Figure 3). During follow-up, 48.1% of patients were hospitalized owing to problems with control of anticoagulation and 39% owing to associated comorbidities.
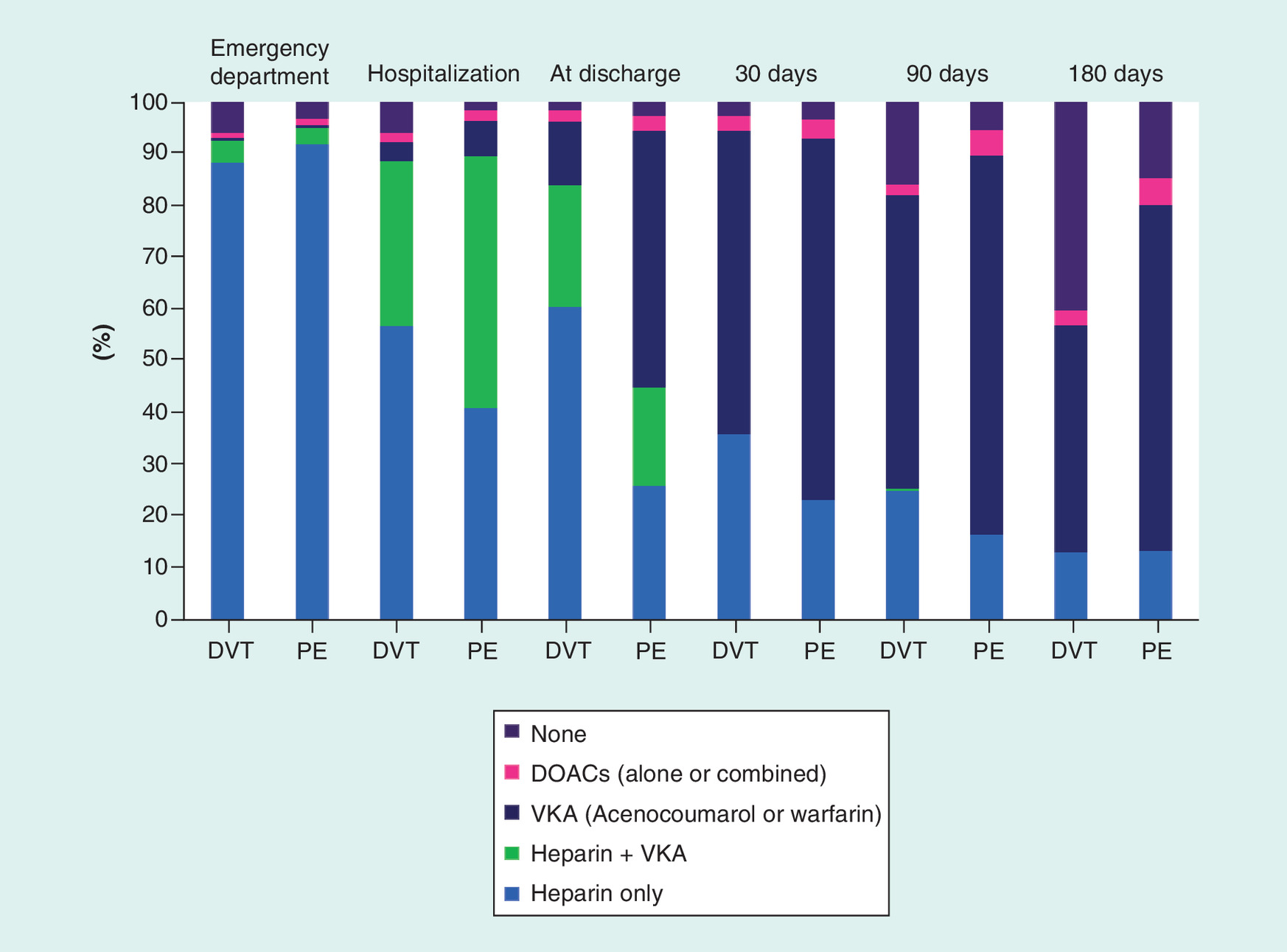
Figure 3. Anticoagulant therapy during the study in nononcologic patients.
DOAC: Direct oral anticoagulant; DVT: Deep vein thrombosis; PE: Pulmonary embolism; VKA: Vitamin K antagonist.
Discussion
Our analysis of the treatment of VTE in patients attended in the ED in Spain and the management of treatment during a 6-month follow-up period demonstrated a high proportion of patients treated with LMWH alone, during all phases of treatment, even in nononcologic patients. In contrast to the guidelines published during the study, which recommended early initiation of VKA [1], heparin was maintained for 90 and 180 days after discharge in a high proportion of the study population. These findings have been described previously [6], and the reasons can be: the perception of physicians that LMWH is more effective than VKA, no need of control, no interactions with food or other treatments and the superiority of LMWH in prevention of PTS compared with VKA, in DVT patients [7]. In patients without active cancer, current guidelines recommend early initiation of oral anticoagulants after parenteral anticoagulation (some DOACs, such as rivaroxaban and apixaban, can be initiated at diagnosis of PE or DVT, in the initial phase) and suggest DOACs as long-term anticoagulant therapy over VKA and VKA over LMWH [1]. Our study showed poor adherence to current recommendations, with extensive use of LMWH and scarce use of DOACs, not only at diagnosis or hospitalization, but also during follow-up. Other prospective and observational studies performed in a real-world setting have also shown poor adherence to guidelines. In the RIETE registry, only 65.2% of VTE patients without cancer started treatment with a VKA during the first 7 days after diagnosis, and 17.7% of patients were taking LMWH in monotherapy during the 3-month follow-up period [6].
Current evidence supports home treatment of both DVT and PE for selected patients; however, in our study, a high proportion of patients with DVT, and most of those with PE, were hospitalized [4,8–10]. During hospitalization, dual therapy with heparin and VKA was more common in patients with PE than in patients with DVT, likely owing to the longer hospital stay in patients with PE. This is because PE is generally considered to be associated with higher recurrence and mortality rates than DVT [11,12]. In fact, in our study, all-cause mortality and death due to recurrence of VTE during hospitalization were higher in PE patients.
After discharge, more than a half of patients were referred to both a specialist and a primary care physician. During follow-up, most visits were to the general practitioner. It therefore seems that many VTE patients were managed in the community, pointing to a potential positive impact on healthcare costs. However, there is much room for improvement. In addition, although optimal timing of follow-up visits after discharge is of great interest for reducing the risk of complications, especially in the elderly, it remains undetermined [13].
During the 6-month follow-up period, anticoagulant medication was maintained for slightly longer in PE patients than in DVT patients and clearly longer than reported in other studies [14,15]. These differences may be due to the specific methods of data collection used (clinical history vs administrative healthcare databases) or differences in the clinical characteristics of the patients included (hospitalized vs outpatient). Anticoagulant treatment may be discontinued for a variety of reasons, including the high risk of bleeding/low risk of recurrence, physicians’ knowledge about the appropriate duration of treatment according to guidelines [16], patients’ preferences or adherence to medication likely associated with the demographic and socioeconomic status [17,18] or death. In our study, after 6 months of follow-up, anticoagulant treatment was discontinued in almost 10.0% of patients because of bleeding events, of which 2.1% were major/fatal bleeds. Because the clinical characteristics of patients and type of event differ from one case to another, the duration of anticoagulant therapy after VTE should be tailored to the risk of recurrence of VTE and of bleeding [19].
Of note, the use of DOACs as maintenance therapy was infrequent in our study, despite the evidences and their advantages over standard therapy (oral therapy vs LMWH, no monitoring of anticoagulation activity or dose adjustments are required vs VKA, etc.) [20,21]. Our results show that promoting the use of DOACs for prophylaxis and treatment of VTE is important, since these drugs are associated with a lower risk of bleeding than VKA, but with a similar efficacy across a wide range of patients, except for risk of recurrence in patients with previous VTE events, where the relative risk of recurrence decreased by around 50% with rivaroxaban [20,21]. As a result, clinicians should be familiar with the particularities of these agents, including appropriate dose selection according to specific clinical conditions. However, despite all these benefits, in Spain there are important restrictions for the prescription of DOACs in the public healthcare system because they are not reimbursed for DVT or PE treatment and for that reason they have a limited use in clinical practice.
Observational studies have reported higher rates of major bleeding than in randomized clinical trials [4,5,22]. Differences between the clinical characteristics of patients included in clinical trials and observational studies, particularly with regard to the risk of bleeding, could also explain the poor adherence to current recommendations reported in observational studies [6,23,24]. By contrast, other prospective studies performed in a real-life setting, such as the XALIA study, have shown that the risk of major bleeding tends to be lower with rivaroxaban than with standard therapy [25]. In fact, DOACs seem to have a better safety profile than VKAs and are recommended over VKAs [1]. It is likely that with the introduction of DOACs, adherence to guidelines will improve during the coming years. In our study, recurrence of VTE was reported in 4.7% of patients throughout the study period (during ED stay, hospitalization and 6-month follow-up). Data from the RIETE registry (6361 VTE patients) showed that recurrence of thromboembolic events occurred in 3.0% of patients after 3 months of follow-up [26], a finding that is similar to our estimated VTE recurrence rate (3.1%).
Our study is subject to a series of limitations. Since patients were attended in the ED, they were probably symptomatic. Therefore, the results of our study may not be generalizable to less severe outpatients referred to the specialist from primary care or to patients who develop VTE during hospitalization for other reasons and whose condition is generally more severe. Furthermore, only data available from the clinical history were recorded. Thus, the information about risk factors and previous VTE events could be limited in some cases. After controlling for specific confounders, such as family history of VTE, it was difficult to assess the presence of genetic alterations or polymorphisms associated with risk of VTE. Remarkably, these factors may influence physicians’ practice regarding anticoagulation. Moreover, clinical data on relative and absolute contraindications to anticoagulation including thrombocytopenia and coagulopathies were lacking. However, the strength of our study was that treatment patterns rather than outcomes of subgroups of patients were analyzed. In addition, the study was performed under real-world conditions, thus illustrating gaps between recommendations in guidelines and clinical practice. At last, our data could be applied only to countries with the same healthcare system and similar clinical profile.
Conclusion
Our study provides relevant information about the therapeutic approach to patients with VTE, from admission to the ED to 6 months afterwards in Spain. LMWH was the most common antithrombotic treatment prescribed in the ED. Patients were rarely switched to oral anticoagulation during hospitalization. The use of oral anticoagulation in nononcologic patients during the follow-up was less frequent than recommended, and the prescription of DOACs was marginal. Overall, the duration of anticoagulation was likely longer than recommended. Our data strongly suggest that there were major discrepancies between guidelines and clinical practice and highlight the need for further investigation to assess potential barriers and thus reduce this gap. Promoting the use of DOACs could simplify the treatment of VTE and may facilitate home management of this entity in selected patients. The information provided by our study should serve as a guide for the optimal implementation of prophylaxis and treatment of VTE, and consequently, may help to reduce recurrences of VTE.
Treatment of venous thromboembolism
The objectives of treatment of venous thromboembolism (VTE) are to prevent thrombus extension, pulmonary embolism, relapses and complications.
Little is known about the management of VTE in the emergency department and in the subsequent months. Analysis of management of VTE could reveal gaps in current practice.
In-hospital management
Heparin monotherapy is the most common anticoagulant therapy during hospitalization for VTE, followed by vitamin K antagonists.
Direct oral anticoagulants (DOACs) were administered very infrequently due to lack of reimbursement and when prescribed, rivaroxaban was the most common one.
Management at discharge & follow-up
The most common treatment at discharge is heparin monotherapy followed by vitamin K antagonists. DOACs were prescribed infrequently.
Conclusion
Adherence to current recommendations is poor, with extensive use of low-molecular-weight heparin, in nononcologic patients and scarce use of DOACs, not only at diagnosis and during hospitalization, but also during follow-up.
Despite current evidence in favor of home treatment of deep vein thrombosis and pulmonary embolism, in the present study, a high percentage of patients received their therapy in hospital.
Further investigations can reduce the discrepancies between guidelines and clinical practice.
Author’s contributions
All authors contributed equally to this work.
Acknowledgements
Investigators of EDITH study:
A Antolín, A Rodríguez, A Segura, A Ortiz, A Fernández, A Alvarez, A Pichel, A Castro, A Duarte, C Suero, E Martínez, E Gené, F Baquedano, FJ Callado, FJ Navarro, F Navarro, F Temboury, I Ayala, J Millán, J Naranjo, J Cruzado, JM Armentia, J Eduardo, JJ Oribe, JL Gálvez, JM Ferreras, JM Junquera, JM Franco, L Sánchez, LM Mateo, MJ Pérez, MJ Rodríguez, MR Arcega; MT Martínez, M Cancio, M Quintana, M Calderón, MdM Carrizosa, M Merlo, ML Castro, O Díez, P Herrero, P Piñera; P Marco, P Ruiz, R Siendones, R Perales, R Rodriguez, R Molina, V Sendín, X López.
Members of ETV -SEMES
M Merlo (Madrid); X López (Barcelona); A Antolín (Barcelona); M Duran (Tarragona); ML Castro (Madrid); I Blasco (Sevilla); D Sánchez (Valencia); S Diego (Asturias); V Sendín (Madrid); A Álvarez (Sevilla); J Naranjo (Salamanca); J Pedraza (Córdoba); LM Mateo (Tarragona); J Fernández (Badajoz); A Ortega (Madrid); P Aparicio (Madrid); J Castillo (Madrid); L Lozano (Barcelona); J Abelaira (Madrid); J Carriel (Madrid); A Peiró (Valencia); H Alonso (Santander); D Jiménez (Madrid); P Ruiz (Madrid), S Jimenez (Barcelona), JM Pedrajas (Madrid).
Financial & competing interests disclosure
The Edith study was funded by Bayer Hispania S.L. The study sponsor had no involvement in the study design, data collection, analysis and interpretation of data, drafting of the manuscript or in the decision to submit the manuscript for publication. The decision to submit the manuscript for publication was solely that of the authors. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing assistance was provided by Content Ed Net, Madrid, Spain and funded by Bayer Hispania.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.
References
Papers of special note have been highlighted as: • of interest
1.
Kearon C, Akl EA, Comerota AJ et al. Antithrombotic therapy for VTE disease: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest physicians evidence-based clinical practice guidelines. Chest 141(2 Suppl.), E419S–E496S (2012).
2.
Multidisciplinary group of thromboembolic disease in Spain, Study of thromboembolic disease in Spain. www.fesemi.org/sites/default/files/documentos/publicaciones/estudio-etv.pdf
3.
Cowell RP. Direct oral anticoagulants: integration into clinical practice. Postgrad. Med. J. 90(1067), 529–539 (2014).
• Compared with vitamin K antagonists, optimal implementation of direct oral anticoagulants in the hospital setting will improve patient outcomes.
4.
Aujesky D, Roy PM, Verschuren F et al. Outpatient versus inpatient treatment for patients with acute pulmonary embolism: an international, open-label, randomized, noninferiority trial. Lancet 378(9785), 41–48 (2011).
• Study highlighting that in selected low-risk patients with pulmonary embolism, outpatient care can be used safely and effectively instead of inpatient care.
5.
Palareti G. Recurrent venous thromboembolism: what is the risk and how to prevent it. Scientifica (Cairo) 2012, 391734 (2012).
• Review of incidence and risk factors for recurrence of venous thromboembolism (VTE), possibility of predicting individual risk of recurrence and recommendations on anticoagulant treatment after a first VTE.
6.
Mahé I, Sterpu R, Bertoletti L et al. Long-term anticoagulant therapy of patients with venous thromboembolism. What are the practices? PLoS ONE 10(6), e0128741 (2015).
• Study based on data from RIETE to identify predictors of anticoagulant choice in patients with and without cancer.
7.
Hull RD, Liang J, Townshend G. Long-term low-molecular-weight heparin and the post-thrombotic syndrome: a systematic review. Am. J. Med. 124(8), 756–765 (2011).
8.
Levine M, Gent M, Hirsh J et al. A comparison of low-molecular-weight heparin administered primarily at home with unfractionated heparin administered in the hospital for proximal deep-vein thrombosis. N. Engl. J. Med. 334(11), 677–681 (1996).
9.
Koopman MM, Prandoni P, Piovella F et al. Treatment of venous thrombosis with intravenous unfractionated heparin administered in the hospital as compared with subcutaneous low-molecular-weight heparin administered at home. The Tasman Study Group. N. Engl. J Med. 334(11), 682–687 (1996).
10.
Zidane M, van Hulsteijn LH, Brenninkmeijer BJ, Huisman MV. Out of hospital treatment with subcutaneous low molecular weight heparin in patients with acute deep-vein thrombosis: a prospective study in daily practice. Haematologica 91(8), 1052–1058 (2006).
11.
Douketis JD, Kearon C, Bates S, Duku EK, Ginsberg JS. Risk of fatal pulmonary embolism in patients with treated venous thromboembolism. JAMA 279(6), 458–462 (1998).
12.
Lecumberri R, Alfonso A, Jimenez D et al. Dynamics of case-fatality rates of recurrent thromboembolism and major bleeding in patients treated for venous thromboembolism. Thromb. Haemost. 110(4), 834–843 (2013).
13.
Storm M, Siemsen IM, Laugaland K, Dyrstad DN, Aase K. Quality in transitional care of the elderly: key challenges and relevant improvement measures. Int. J. Integr. Care 14, e013 (2014).
14.
Deitelzweig SB, Lin J, Kreilick C, Hussein M, Battleman D. Warfarin therapy in patients with venous thromboembolism: patterns of use and predictors of clinical outcomes. Adv. Ther. 27(9), 623–633 (2010).
15.
Tagalakis V, Patenaude V, Kahn SR, Suissa S. Treatment patterns of venous thromboembolism in a real-world population: the Q-VTE study cohort. Thromb. Res. 134(4), 795–802 (2014).
16.
Caprini JA, Tapson VF, Hyers TM et al. Treatment of venous thromboembolism: adherence to guidelines and impact of physician knowledge, attitudes and beliefs. J. Vasc. Surg. 42(4), 726–733 (2005).
• Study analzying problems with treatment of VTE and gap between actual practice and clinical guidelines.
17.
Gebler-Hughes ES, Kemp L, Bond MJ. Patients’ perspectives regarding long-term warfarin therapy and the potential transition to new oral anticoagulant therapy. Ther. Adv. Drug Saf. 5(6), 220–228 (2014).
18.
Kneeland PP, Fang MC. Current issues in patient adherence and persistence: focus on anticoagulants for the treatment and prevention of thromboembolism. Patient Prefer. Adherence 4, 51–60 (2010).
19.
de Jong PG, Coppens M, Middeldorp S. Duration of anticoagulant therapy for venous thromboembolism: balancing benefits and harms on the long term. Br. J. Haematol. 158(4), 433–441 (2012).
20.
Gomez-Outes A, Terleira-Fernandez AI, Lecumberri R, Suarez-Gea ML, Vargas-Castrillon E. Direct oral anticoagulants in the treatment of acute venous thromboembolism: a systematic review and meta-analysis. Thromb. Res. 134(4), 774–782 (2014).
21.
Prins MH, Lensing AW, Bauersachs R et al. Oral rivaroxaban versus standard therapy for the treatment of symptomatic venous thromboembolism: a pooled analysis of the EINSTEIN–DVT and PE randomized studies. Thromb. J. 11(1), 21 (2013).
• This pooled analysis of the EINSTEIN-deep vein thrombosis and pulmonary embolism randomized studies showed that rivaroxaban in monotherapy had a similar efficacy than the standard-therapy, but with a significantly lower rate of major bleeding.
22.
Nordstrom M, Lindblad B, Bergqvist D, Kjellstrom T. A prospective study of the incidence of deep-vein thrombosis within a defined urban population. J. Intern. Med. 232(2), 155–160 (1992).
23.
Ageno W, Becattini C, Brighton T, Selby R, Kamphuisen PW. Cardiovascular risk factors and venous thromboembolism: a meta-analysis. Circulation 117(1), 93–102 (2008).
24.
Bai J, Ding X, Du X, Zhao X, Wang Z, Ma Z. Diabetes is associated with increased risk of venous thromboembolism: a systematic review and meta-analysis. Thromb. Res. 135(1), 90–95 (2015).
25.
Ageno W, Mantovani LG, Haas S et al. Safety and effectiveness of oral rivaroxaban versus standard anticoagulation for the treatment of symptomatic deep-vein thrombosis (XALIA): an international, prospective, noninterventional study. Lancet Haematol. 3(1), E12–E21 (2016).
• In this international, prospective and noninterventional study, rivaroxaban was a safe and effective alternative to standard anticoagulation therapy in a broad range of patients with symptomatic deep vein thrombosis.
26.
Nieto JA, De Tuesta AD, Marchena PJ et al. Clinical outcome of patients with venous thromboembolism and recent major bleeding: findings from a prospective registry (RIETE). J. Thromb. Haemos. 3(4), 703–709 (2005).
Information & Authors
Information
Published In
Copyright
© 2018 Future Medicine Ltd.
History
Received: 4 August 2017
Accepted: 31 October 2017
Published online: 23 March 2018
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Therapeutic approach for patients with venous thromboembolism attended in emergency departments during routine clinical practice: the EDITH study. (2018) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2017-0061
Export citation
Select the citation format you wish to export for this article or chapter.