Comparable effects of exercise and analgesics for pain secondary to knee osteoarthritis: a meta-analysis of trials included in Cochrane systematic reviews
Abstract
Aim: Evidence of comparative effectiveness of different treatment approaches is important for clinical decision-making, yet absent for most recommended treatments of knee osteoarthritis pain. The objective of this study was to estimate the comparative effectiveness of exercise versus orally administered analgesics for pain in patients with knee osteoarthritis. Methods: The Cochrane Database of systematic reviews was searched for meta-analyses of randomized controlled studies comparing exercise or analgesics with a control group (placebo or usual care) and with pain as an outcome. Individual study estimates were identified and effect sizes were calculated from group differences. We combined study-level effects on pain with a random effects meta-analysis and compared effect sizes between exercise trials and trials with analgesic interventions. Results: We included six Cochrane reviews (four pharmacology, two exercise). From these, 54 trials were eligible (20 pharmacology, 34 exercise), with 9806 participants (5627 pharmacology, 4179 exercise). The pooled effect size of pharmacological pain interventions was 0.41 (95% CI: 0.23–0.59) and for exercise 0.46 standardized mean difference (95% CI: 0.34–0.59). There was no statistically significant difference between the two types of intervention (difference: 0.06 standardized mean difference [95% CI: -0.28–0.16; p = 0.61]). Conclusion: This meta-epidemiological study provides indirect evidence that for knee osteoarthritis pain, the effects from exercise and from oral analgesics are comparable. These results may support shared decision-making where a patient for some reason is unable to exercise or who consider exercise as unviable and analgesics as a more feasible choice.
PROSPERO registration: CRD42013006924
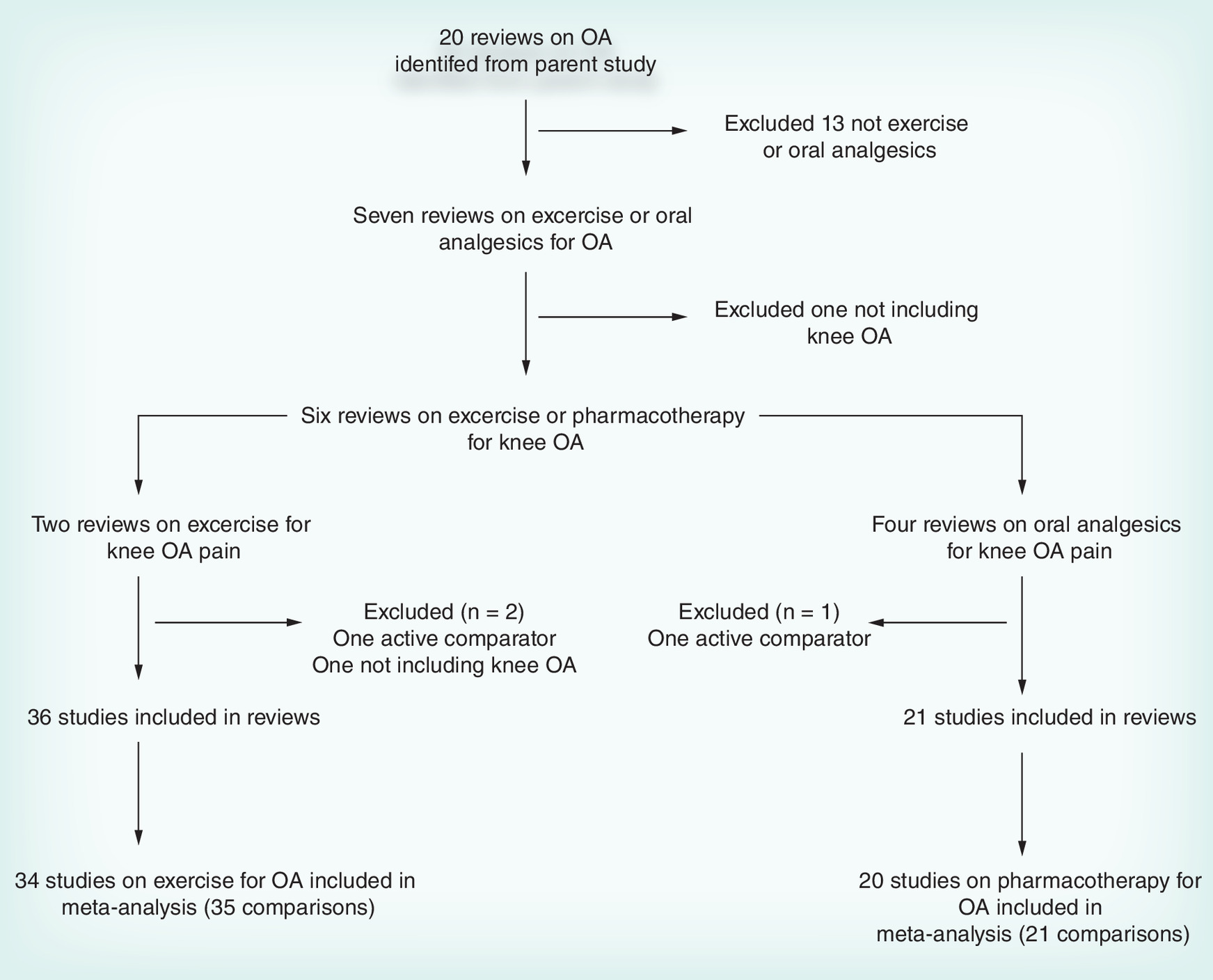
Figure 1. Flow diagram of study selection.
OA: Osteoarthritis.
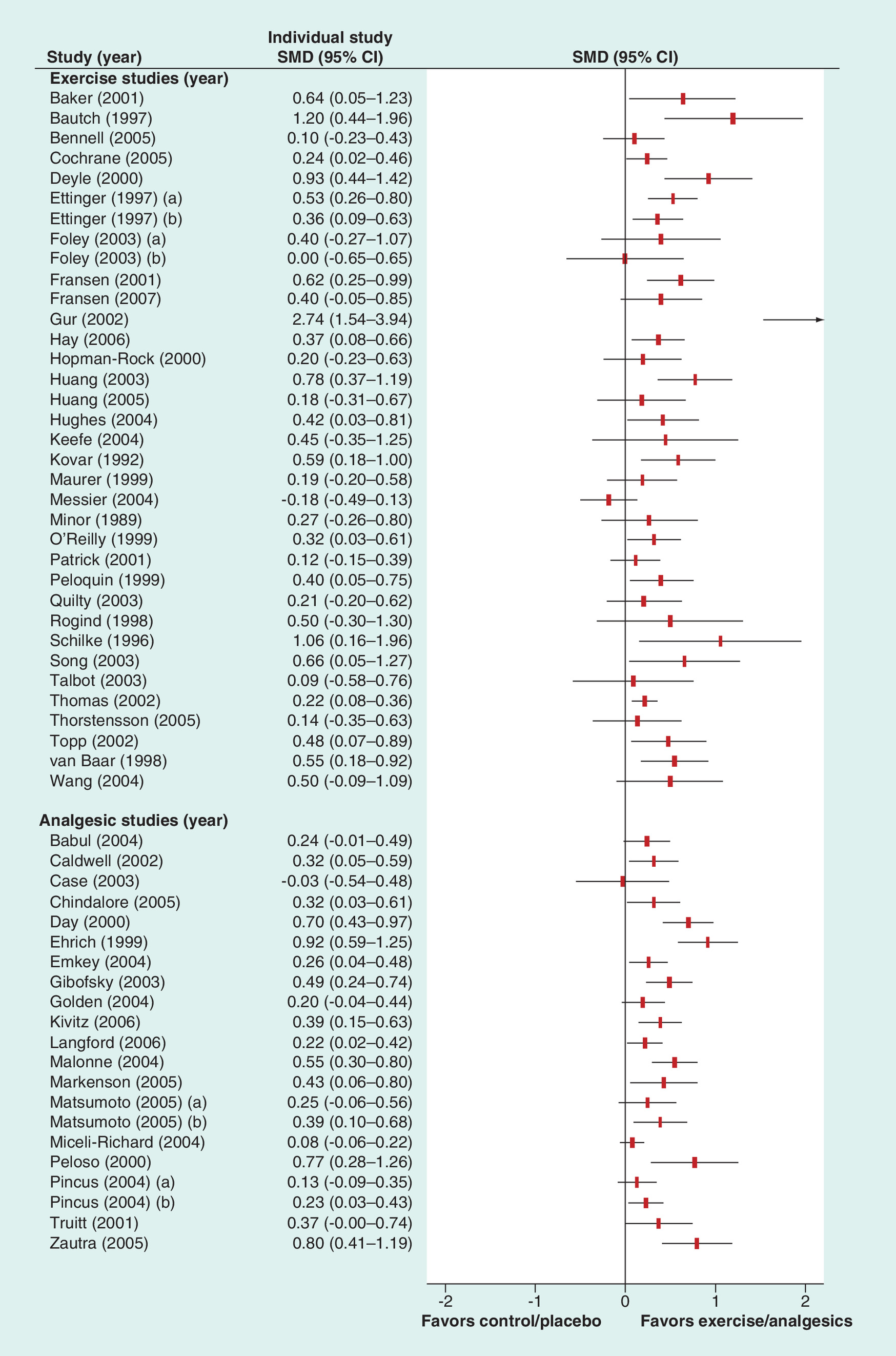
Figure 2. Forest plot of effect sizes for exercise and orally administered analgesics interventions for knee osteoarthritis pain.
Arrow indicates an estimate beyond the current x-axis scale.
SMD: Standardized mean difference.
First draft submitted: 28 January 2016; Accepted for publication: 11 April 2016; Published online: 27 June 2016
Osteoarthritis (OA) of the knee is a chronic condition with pain as the cardinal symptom. There is currently no cure for OA; management focuses on reducing pain and restoring physical function. Recommended management strategies include nonpharmacological and/or pharmacological treatments. Among the nonpharmacological management strategies for knee OA, exercise is considered a core treatment [1–3] with a small-to-moderate effect on pain. [4,5] Although several exercise types have been evaluated, no specific type has proven more effective at relieving pain than others [6]. Pharmacological treatments are recommended as adjunctive and in the lowest effective dose [1,3,7]. Acetaminophen is recommended for use as an analgesic in knee OA. [1,3] For symptomatic knee OA flare-ups, short periods of NSAIDs have documented effects on pain but carry a risk of considerable and potentially harmful side effects. [8]
Despite the priority of exercise over pharmacological treatments in the recommended treatment algorithm [1,3], some patients may not be able to exercise or view exercise as unviable and may prefer pharmacological treatments. While a crude comparison of the pooled effect sizes of exercise and analgesics suggests similar magnitudes, [5] comparative studies are very sparse. One randomized trial in patients with knee OA compared 8 weeks of home exercise and NSAID treatment and found pain improvement in both groups but no significant group differences. [9] Further comparative effectiveness studies are needed in order to provide clinicians, patients and policy makers with relevant information about comparative effects of exercise and pharmacological treatment for knee OA pain.
To illuminate this issue, we performed a meta-epidemiological study based on published Cochrane reviews to make an indirect comparison [10] of the comparative effectiveness of exercise and pharmacological treatment of knee OA pain from existing evidence.
Methods
This study is a systematic review and meta-analysis based on an overarching systematic review titled ‘Assessing bias in osteoarthritis trials included in Cochrane reviews: a meta-epidemiological study’ [11]. The protocol for the parent study is registered on PROSPERO (CRD42013006924) and published [11]. This report conforms to the ‘Preferred Reporting Items for Systematic Reviews and Meta-Analyses’ statement [12].
Identification of cochrane reviews
From the original literature search of the Cochrane Database of Systematic Reviews, eligible trials were identified from published Cochrane reviews (i.e., meta-analyses). Eligible Cochrane reviews had to focus on knee OA and orally administered pharmaceutical analgesics or therapeutic exercise, and their analyses had to include pain as an outcome. Two reviewers (JB Hansen and L Klokker) independently assessed the eligibility of the individual Cochrane reviews; disagreement was resolved by discussing with a third arbiter (R Christensen).
Individual study identification, eligibility & data extraction
From the included reviews, individual studies were identified, assessed for eligibility and their data extracted. Individual studies were excluded if they were not randomized controlled trials (RCTs), if they did not include patients with knee OA, if they did not include pain as an outcome or if the control condition was not considered inert (i.e., sham, placebo or no intervention control). Two reviewers (JB Hansen and L Klokker) independently assessed the eligibility of the individual studies, and disagreement was resolved by discussing with a third arbiter (M Henriksen). From the eligible studies, the following data were extracted: author, year of publication, journal, intervention (drug name or exercise type), comparator type, number of participants, pain outcome measure, study duration and effect estimates on pain (either by groups or as differences among groups), with uncertainty stated typically as standard deviations or confidence limits. If more than one analysis on pain was included in a study, we extracted estimates from the first available analysis, which was assumed to be the main analysis on pain. Two reviewers (JB Hansen and L Klokker) independently extracted data from each included study and resolved their disagreements by discussion. The risk of bias within each full-text trial was assessed using the risk of bias tool as recommended by the Cochrane Collaboration [13]. The risk of bias tool comprises assessment of reported methods for generating allocation sequence, managing incomplete outcome data and maintaining allocation concealment and blinding, as well as an assessment of risk of reporting bias. Each bias item was rated as adequate, inadequate or unclear.
Evidence synthesis
Effect sizes on pain were expressed as standardized mean differences (SMDs) estimated from each trial's mean and standard deviations abstracted from the Cochrane reviews. Assuming that there is no relevant difference in the SMD's based on follow-up and change data we decided to combine these estimates [14].
Using generic inverse variance analysis, we calculated pooled effect sizes for exercise and analgesics using a random effects model (restricted maximum likelihood), allowing for anticipated differences in treatment effects from study to study [15]. We stratified the analysis by treatment (pharmacology and exercise, respectively) comparing the pooled effect sizes. For sensitivity purposes we repeated the analysis using a fixed effects model to test the robustness of our findings.
Results
The literature search in the parent study was carried out on 31 January 2014 [11]. From the Cochrane reviews included in the original search, we identified six eligible Cochrane reviews, of which four were related to oral analgesics and two to exercise (Figure 1 & Supplementary data). From the included Cochrane reviews, we identified 54 trials that fulfilled the inclusion criteria (34 exercise, 20 analgesics), including 9806 patients with OA (4179 exercise, 5627 analgesics) in 56 comparisons (35 exercise and 21 analgesics). Of the included trials, 34 included knee OA patients exclusively and 20 studied a mixed population of hip and knee OA. An overview of included studies is presented in Table 1. The individual study SMDs are illustrated in Figure 2.
The 35 comparisons of exercise with no intervention, sham or standard care were associated with an overall statistically significant benefit on pain, with an effect size of 0.46 (95% CI: 0.34–0.59) for pain (Table 2). Similarly, oral analgesics were associated with a statistically significant benefit on pain when compared with placebo or standard care, with an effect size of 0.41 (95% CI: 0.23–0.59). The comparison of the estimates allowed us to infer that for pain, exercise and orally administered analgesics demonstrated comparable effect sizes (judged by the width of the 95% CI), with a statistically nonsignificant difference in the SMDs of 0.06 (95% CI: -0.16 to -0.28).
The fixed effects analysis gave similar results but with lower SMDs for both exercise and pharmacological analgesics and with a statistically significant difference of 0.10 (95% CI: 0.01–0.19) in favor of exercise (Table 2).
Across all studies, the overall between-study heterogeneity was high, with an inconsistency index (I2) of 54% (48% in the exercise trials and 63% in the pharmacology trials). In an attempt to explain between-study heterogeneity, we performed an additional stratification of the exercise and analgesics trials into more specified intervention types. Exercise trials were stratified by land and aquatic exercise, and the analgesics trials were stratified as acetaminophen, NSAID and opioids. No statistically significant differential responses on pain were observed (Table 2) and the additional stratified analysis did not result in lower between-study heterogeneity (I2 = 54%). We further stratified for population (knee OA vs mixed knee and hip OA patients) and found similar estimates for these populations; knee OA: SMD = 0.47 (95% CI: 0.34–0.60); mixed knee and hip OA: SMD = 0.40 (95% CI: 0.23–0.57), with no statistically significant difference in the SMDs (difference: 0.07 [95% CI: -0.14–0.29] in potential favor of the knee OA only population).
Risk of bias assessments
Among the 21 comparisons examining analgesics for treating pain in OA, the participants’ knowledge of the allocated intervention was adequately prevented in 86% (18) of the comparisons. In the 35 studies on exercise, only 6% (two studies) adequately prevented the participants’ knowledge of the allocated intervention. The handling of missing data was reported adequately in 95% of the analgesics comparisons, as opposed to only 57% of the exercise comparisons. For blinding of key study personnel, 71% of the analgesics comparisons adequately prevented the knowledge of the allocated intervention versus 49% of the exercise comparisons. Concerning the reported methods to generate allocation sequences, 57% of the analgesics comparisons and 69% of the exercise group performed it adequately. Concealment of allocation was adequate in 38% of the analgesics group and 43% of the exercise group.
Discussion
This meta-epidemiological study based on trials included in Cochrane reviews, included 54 RCTs with 9806 patients, suggests comparable effects of exercise and orally administered analgesics for the conservative management of pain secondary to knee OA. Almost two-thirds of the reviewed trials pertained to exercise, which points out a trend toward testing exercise interventions for knee OA pain. This highlights the changed landscape of management and research in knee OA pain, which increasingly favors nonpharmacological interventions over drug interventions.
Our results indicate that exercise and oral analgesics are comparable in terms of their pain relieving benefits, which supports the recommendation that exercise should be considered as the first choice, possibly accompanied by analgesics for control of severe pain or pain exacerbations [1–3]. The feasibility of a standardized analgesic prescription to allow for participation in exercise therapy has recently been demonstrated, although this needs to be confirmed in a randomized trial [73]. However, for patients who are unable to exercise or prefer not to engage in an exercise program, these results indicate that oral analgesics yield similar benefits for knee OA pain.
We considered exercise interventions as a group. However, more nuanced considerations of the effectiveness of different types, intensities, frequencies and durations of exercise are warranted. A recent systematic review concluded that – based on available evidence – it is not possible to identify one particular type of exercise as superior for knee OA [6]. Thus, present recommendations are simply that ‘any exercise’ is beneficial for managing knee OA pain; the optimal exercise program in terms of application and content is elusive, and comparative effectiveness studies are needed. This contrasts with pharmacological interventions, in which dosage and frequencies are established in preclinical phases of drug development.
We also considered oral analgesics as a group in the main analysis (i.e., we pooled analgesics covering acetaminophen, NSAIDs and opioids). These analgesics have different mechanisms of action and are intended for different populations of people with knee OA; intermittent use of over-the-counter acetaminophen is recommended as basic pain management in people without significant comorbidities, whereas in the absence of satisfactory clinical response, a full-dose of acetaminophen (4000 mg/day) or switching to NSAIDs is recommended [1,74]. Finally, opioids are recommended for patients with severe pain and inadequate response to both first-line pharmacological and nonpharmacological modalities [1,74]. However, in our stratified analyses we could not identify differential effects of the various analgesics against the different exercise types. Importantly, the majority of the included trials on oral analgesics and all included trials on aquatic exercise studied mixed populations of knee and hip OA patients, whereas as the included land-based exercise trials focused on knee OA patients alone. Although we found no differential effects based on population, this highlights that differences in study populations among different drug and exercise trials are important to consider when comparing effect estimates.
The stratified analyses should be interpreted cautiously, mainly due to the indirectness of the comparisons, but also because the different stratified comparisons are based on relatively few studies and are associated with broad confidence intervals meaning that further research is very likely to change the estimated differences in effects between the various analgesics and exercise types.
The Osteoarthritis Research Society International guidelines for the nonsurgical management of knee OA pain emphasize exercise as a core treatment appropriate for all individuals with knee OA [3]. However, the dearth of evidence on exercise type, frequency, intensity and duration leaves substantial uncertainty about which patients would benefit more from what type of exercise, and which forms of exercise may not be effective in different settings and subpopulations. Similarly, it is also not fully established which patient populations that benefit more from specific pharmacological interventions. A further complicating matter is the limited evidence on the potential harmful effects of exercise; adverse events associated with exercise are not systematically reported in individual trials. This contrasts the studies on analgesics, in which safety considerations are mandatory. Although exercise is generally considered safe, the statement that the potential risks associated with exercise are lower than those associated with drugs is weakly supported by evidence. Such a statement highlights the need for careful considerations about potential harms associated with prescribing exercise for knee OA patients to manage pain and also recording of harms in exercise trials.
It is worth noting that the analgesic trials mainly used placebo comparators (20/21 comparisons; Table 1), whereas the exercise trials mainly used ‘no-intervention control’ or ‘care as usual’ comparators (34/35 comparisons; Table 1). Thus, the estimated effect size of analgesics represents the net effect (i.e., gross effect minus the placebo effect), whereas the effect sizes of exercise represent the gross effect, including participant nonblinding and attention biases that are difficult to avoid in exercise studies. This finding suggests that the estimated effect size of exercise may be inflated (relative to the placebo controlled studies on analgesics), and the difference between analgesics and exercise may be underestimated. In fact, a study testing nonpharmacological interventions against placebo found a considerably reduced effect size [46]. On the other hand, in most exercise studies, concurrent use of oral analgesics is typically not prohibited – at least not in ‘no-intervention control’ or ‘care as usual’ groups. This could suggest that the estimated effect of exercise reflects the added benefit of exercise over and above the benefit conferred from habitual analgesic usage. However, very few exercise studies report on or regulate concomitant habitual analgesic usage.
Strengths & limitations of this study
A strength of our meta-review approach is our inclusion of relevant high-quality evidence only, as Cochrane reviews are considered the highest level of evidence in the hierarchy of study designs and are unlikely to conflict with other high-quality systematic reviews. Also, Cochrane reviews represent the first-line source of evidence information for many clinicians, and thus the present study provides a clinically relevant, yet indirect, comparison that is otherwise unavailable. However, it is an important limitation that Cochrane reviews were the only source of study estimates included, and the omission of other systematic reviews or primary studies may have resulted in underrepresentation of the available evidence. Indeed, the included reviews were last updated in 2007–2009, except for the Cochrane review on land-based exercise that was recently updated [75]. The updated Cochrane review on land-based exercise was published after the current literature search and was thus not included in the present study. However, the updated review [75] came to the same conclusion as the review we included, [4] with only a slight increase in the estimated effect size on pain. Furthermore, a recent systematic review concluded that already in 2002, the cumulative evidence supporting exercise for managing knee OA pain was sufficient and that further RCTs were unlikely to change the estimated effects of exercise [76]. With regards to the lack of recent updates of the Cochrane reviews on the analgesics, the estimates related to the analgesics included here are also considered stable [5] and compares well with estimates from a recent systematic review and network meta-analysis on pharmacological interventions for knee OA. [77] Thus, although the source of our data is 5–7 years old, we believe our estimated comparative effectiveness on pain is robust.
Although our results suggest that exercise and oral analgesics seem to have comparable effectiveness, our findings should be interpreted with caution, given the indirectness of the comparison and different settings and populations involved in the underlying studies. For example, selection criteria in pharmaceutical trials are usually more restrictive (e.g., exclusion of subjects with cardiac disease) than in exercise trials, although the majority of the pharmaceutical trials included in this review targeted a mixed population of knee and hip OA patients. The between-study heterogeneity was not negligible and it is possible that potential imbalances in the distribution of unobserved or unmeasured modifiers across interventions affected the comparative estimates. It should also be noted that we compared only effects on pain. Physical function and overall well being are also considered as core outcomes in knee OA, but the comparative effectiveness of these outcomes remains unknown.
Studies on therapeutic exercise for knee OA generally lack clear descriptions of many potential factors that may explain the success or failure of the intervention, such as the setting in which the exercise was undertaken, content of the exercise program and how it was carried out. It is particularly important to characterize the so-called ‘contextual factors’ and ‘supportive information’ (e.g., extent of supervision, progression protocols, individualized vs group exercise, facility or home based among others), which can allow clinicians to replicate successful interventions. There is an urgent need to improve the reporting on frequency, intensity, type and time factors of exercise therapy. This concerns both the exercise program as intended, as well as the exercise program as actually performed (because of nonadherence). Most exercise trials are inherently biased due to their lack of patient blinding and their inclusion of a no-intervention control group as comparator, whereas pharmacological trials are more easily designed to minimize such biases. The included exercise trials are generally smaller and with longer durations than the trials on analgesics that on the other hand typically are done in a multicenter setup. The included exercise trials are mostly supported by nonprofit funding sources, whereas pharmacological studies typically are funded by for-profit sources, which may also introduce risks of bias. Finally, an important limitation is a missing comparison of safety. However, safety is difficult to compare because adverse reactions to exercise are extremely rarely reported.
Despite these limitations we believe that this meta-epidemiological overview provides an informative summary of the comparative effectiveness of exercise-based and pharmacological pain relief in knee OA, which may guide clinical discussions and decisions. Despite comparable effects, the evidence is indirect and future studies on comparative effectiveness and safety are warranted. The present study have synthesized the useful conclusions that can be drawn from Cochrane Systematic Reviews to support evidence-based decisions for conservative management of knee OA pain and to inform future clinical research agendas.
Conclusion
This meta-epidemiological study provides indirect evidence of comparable effects of exercise and oral analgesics for treating pain secondary to knee OA. These results can inform and support clinical management of patients that for some reason are unable to exercise or who consider exercise unviable.
| Source cochrane review (year) | Study (year) | Population | Intervention | ITT population (n) | Intervention group (n) | Control group (n) | Study duration (weeks) | Control intervention | Outcome |
|---|---|---|---|---|---|---|---|---|---|
| Garner (2008) [16] | Day (2000) [17] | Mixed knee and hip | NSAID | 316 | 242 | 74 | 6 | Sham/placebo | WOMAC pain |
| Ehrich (1999) [18] | Mixed knee and hip | NSAID | 145 | 73 | 72 | 6 | Sham/placebo | WOMAC pain | |
| Gibofsky (2003) [19] | Mixed knee and hip | NSAID | 286 | 190 | 96 | 6 | Sham/placebo | VAS global | |
| Truitt (2001) [20] | Mixed knee and hip | NSAID | 108 | 56 | 52 | 6 | Sham/placebo | VAS global | |
| Nüesch (2009) [21] | Peloso (2000) [22] | Mixed knee and hip | Opioids | 66 | 31 | 35 | 4 | Sham/placebo | VAS global |
| Langford (2006) [23] | Mixed knee and hip | Opioids | 399 | 202 | 197 | 8 | Sham/placebo | VAS global | |
| Caldwell (2002) [24] | Mixed knee and hip | Opioids | 295 | 222 | 73 | 4 | Sham/placebo | WOMAC pain | |
| Markenson (2005) [25] | Mixed knee and hip | Opioids | 107 | 56 | 51 | 13 | Standard care | WOMAC pain | |
| Chindalore (2005) [26] | Mixed knee and hip | Opioids | 360 | 309 | 51 | 4 | Sham/placebo | WOMAC pain | |
| Matsumoto (2005) (a) [27] | Mixed knee and hip | Opioids | 179 | 120 | 59 | 4 | Sham/placebo | WOMAC pain | |
| Zautra (2005) [28] | Mixed knee and hip | Opioids | 104 | 55 | 49 | 13 | Sham/placebo | VAS global | |
| Matsumoto (2005) (b) [27] | Mixed knee and hip | Opioids | 288 | 228 | 60 | 4 | Sham/placebo | WOMAC pain | |
| Kivitz (2006) [29] | Mixed knee and hip | Opioids | 357 | 270 | 87 | 2 | Sham/placebo | VAS global | |
| Towheed (2009) [30] | Case (2003) [31] | Knee | Acetaminophen | 57 | 29 | 28 | 12 | Sham/placebo | WOMAC pain |
| Pincus (2004) (a) [32] | Mixed knee and hip | Acetaminophen | 343 | 171 | 172 | 6 | Sham/placebo | WOMAC pain | |
| Pincus (2004) (b) [32] | Mixed knee and hip | Acetaminophen | 367 | 185 | 182 | 6 | Sham/placebo | WOMAC pain | |
| Golden (2004) [33] | Knee | Acetaminophen | 294 | 145 | 149 | 1 | Sham/placebo | 0–4 Scale | |
| Miceli-Richard (2004) [34] | Mixed knee and hip | Acetaminophen | 774 | 401 | 373 | 6 | Sham/placebo | VAS | |
| Cepeda (2009) [35] | Babul (2004) [36] | Knee | Acetaminophen | 246 | 124 | 122 | 12 | Sham/placebo | VAS |
| Emkey (2004) [37] | Knee | Acetaminophen | 306 | 153 | 153 | 13 | Sham/placebo | VAS | |
| Malonne (2004) [38] | Mixed knee and hip | Acetaminophen | 230 | 111 | 119 | 2 | Sham/placebo | VAS | |
| Bartels (2007) [39] | Cochrane (2005) [40] | Mixed knee and hip | Exercise aquatic | 310 | 152 | 158 | 12 | Standard care | WOMAC pain |
| Foley (2003) (a) [41] | Mixed knee and hip | Exercise aquatic | 47 | 35 | 12 | 6 | No intervention | WOMAC pain | |
| Wang (2004) [42] | Mixed knee and hip | Exercise aquatic | 43 | 21 | 22 | 12 | Standard care | VAS | |
| Patrick (2001) [43] | Mixed knee and hip | Exercise aquatic | 215 | 98 | 117 | 20 | Standard care | HAQ pain | |
| Fransen (2009) [4] | Baker (2001) [44] | Knee | Exercise land based | 44 | 22 | 22 | 16 | Standard care | WOMAC pain |
| Bautch (1997) [45] | Knee | Exercise land based | 30 | 15 | 15 | 12 | Standard care | VAS | |
| Bennell (2005) [46] | Knee | Exercise land based | 140 | 73 | 67 | 12 | Sham/placebo | VAS | |
| Deyle (2000) [47] | Knee | Exercise land based | 69 | 33 | 36 | 8 | Standard care | WOMAC pain | |
| Ettinger (1997) (a) [48] | Knee | Exercise land based | 218 | 144 | 74 | 12 | Standard care | FASTx6 | |
| Ettinger (1997) (b) [48] | Knee | Exercise land based | 221 | 146 | 75 | 12 | Standard care | FASTx6 | |
| Foley (2003) (b) [41] | Knee | Exercise land based | 35 | 21 | 14 | 6 | No intervention | WOMAC pain | |
| Fransen (2001) [49] | Knee | Exercise land based | 126 | 83 | 43 | 8 | No intervention | WOMAC pain | |
| Fransen (2007) [50] | Knee | Exercise land based | 77 | 41 | 36 | 12 | No intervention | WOMAC pain | |
| Gur (2002) [51] | Knee | Exercise land based | 23 | 17 | 6 | 8 | No intervention | VAS | |
| Hay (2006) [52] | Knee | Exercise land based | 182 | 93 | 89 | 12 | No intervention | WOMAC pain | |
| Hopman-Rock (2000) [53] | Knee | Exercise land based | 80 | 45 | 35 | 6 | No intervention | VAS | |
| Huang (2003) [54] | Knee | Exercise land based | 132 | 99 | 33 | 8 | No intervention | VAS | |
| Hughes (2004) [55] | Knee | Exercise land based | 111 | 68 | 43 | 8 | No intervention | WOMAC pain | |
| Huang (2005) [56] | Knee | Exercise land based | 65 | 30 | 35 | 8 | No intervention | VAS | |
| Keefe (2004) [57] | Knee | Exercise land based | 25 | 16 | 9 | 12 | No intervention | AIMS pain | |
| Kovar (1992) [58] | Knee | Exercise land based | 92 | 47 | 45 | 8 | Standard care | AIMS pain | |
| Maurer (1999) [59] | Knee | Exercise land based | 98 | 49 | 49 | 8 | Standard care | WOMAC pain | |
| Messier (2004) [60] | Knee | Exercise land based | 158 | 80 | 78 | 24 | Standard care | WOMAC pain | |
| Minor (1989) [61] | Knee | Exercise land based | 68 | 49 | 19 | 12 | Standard care | AIMS pain | |
| O'Reilly (1999) [62] | Knee | Exercise land based | 180 | 108 | 72 | 24 | No intervention | WOMAC pain | |
| Peloquin (1999) [63] | Knee | Exercise land based | 124 | 59 | 65 | 12 | No intervention | AIMS pain | |
| Quilty (2003) [64] | Knee | Exercise land based | 87 | 43 | 44 | 20 | No intervention | VAS | |
| Rogind (1998) [65] | Knee | Exercise land based | 23 | 11 | 12 | 12 | No intervention | VAS | |
| Schilke (1996) [66] | Knee | Exercise land based | 20 | 10 | 10 | 8 | No intervention | OASI pain | |
| Song (2003) [67] | Knee | Exercise land based | 43 | 22 | 21 | 12 | Standard care | WOMAC pain | |
| Talbot (2003) [68] | Knee | Exercise land based | 34 | 17 | 17 | 12 | Standard care | McGill | |
| Thomas (2002) [69] | Knee | Exercise land based | 783 | 467 | 316 | 104 | No intervention | WOMAC pain | |
| Thorstensson (2005) [70] | Knee | Exercise land based | 61 | 30 | 31 | 6 | No intervention | KOOS pain | |
| Topp (2002) [71] | Knee | Exercise land based | 102 | 67 | 35 | 16 | No intervention | WOMAC pain | |
| van Baar (1998) [72] | Knee | Exercise land based | 113 | 54 | 59 | 12 | Standard care | VAS |
(a) and (b) denotes that a study had two intervention groups that are being treated as two trials.
AIMS: Arthritis Impact Measurement Scale; ITT: Inten-to-treat; KOOS: Knee Injury and Osteoarthritis Outcome Score; OASI: Osteoarthritis Screening Index; VAS: Visual Analog Scale; WOMAC: Western Ontario and McMaster Universities Osteoarthritis Index.
| Analysis | SMD | SE | 95% CI: | p-value | I² (%) |
|---|---|---|---|---|---|
| Random effects analysis | |||||
| Overall | 0.44 | 0.06 | -0.54 to -0.33 | <0.0001 | 54 |
| Exercise | 0.46 | 0.07 | 0.34–0.59 | <0.0001 | 48 |
| Analgesics | 0.41 | 0.09 | 0.23–0.59 | <0.0001 | 63 |
| Exercise versus pharma | 0.06 | 0.11 | -0.16–0.28 | 0.61 | – |
| Stratified analysis | |||||
| Exercise aquatic | 0.22 | 0.19 | -0.16–0.60 | 0.259 | 0 |
| Exercise land | 0.49 | 0.07 | 0.36–0.63 | 0.000 | 51 |
| Acetaminophen | 0.23 | 0.16 | -0.08–0.53 | 0.143 | 41 |
| NSAIDS | 0.60 | 0.19 | 0.22–0.98 | 0.002 | 51 |
| Opioids | 0.45 | 0.14 | 0.18–0.71 | 0.001 | 23 |
| Ex. aqua versus acetaminophen | -0.01 | 0.25 | -0.50–0.48 | 0.97 | – |
| Ex. aqua versus NSAIDs | -0.38 | 0.28 | -0.92–0.16 | 0.16 | – |
| Ex. aqua versus opioids | -0.23 | 0.24 | -0.69–0.24 | 0.34 | – |
| Ex. land versus acetaminophen | 0.27 | 0.17 | -0.07–0.60 | 0.12 | – |
| Ex. land versus NSAIDs | -0.11 | 0.21 | -0.51–0.30 | 0.60 | – |
| Ex. land versus opioids | 0.05 | 0.15 | -0.25–0.35 | 0.75 | – |
SE: Standard error; SMD: Standardized mean difference.
Comparative effectiveness of different recommended treatments of knee osteoarthritis pain is lacking.
In this study the comparative effectiveness of exercise versus orally administered analgesics for pain in patients with knee osteoarthritis was assessed.
We made an indirect comparison of the effectiveness of exercise and oral analgesics on knee osteoarthritis pain from published Cochrane reviews.
The results provide indirect evidence of comparable effects of exercise and oral analgesics for treating pain secondary to knee osteoarthritis
These results can inform and support clinical management of patients that for some reason are unable to exercise or who consider exercise unviable.
Author contributions
M Henriksen had full access to all the data in the study and takes responsibility of for the integrity of the data and the accuracy of the data analysis. The study was conceptualised and designed by M Henriksen, H Bliddal, R Christensen. Data was acquired, analyzed and interpreted by all authors. The manuscript was drafted by M Henriksen and subsequently critically revised for important intellectual content by all authors. The statistical analyses were carried out by R Christensen. Administrative, technical, or material support: M Henriksen, H Bliddal, R Christensen. Details of the literature search, the search results and reasons for exclusion are available from the corresponding author M Henriksen.
Disclosure
The Parker Institute holds a grant from The Oak Foundation.
Financial & competing interests disclosure
Funding was obtained by H Bliddal. The authors have no other relevant affiliations or financial involvements with any organization or entity with a financial interest in or financial conflict with the subjext matter or materials dicussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Hochberg MC, Altman RD, April KT et al. American College of Rheumatology 2012 recommendations for the use of nonpharmacologic and pharmacologic therapies in osteoarthritis of the hand, hip, and knee. Arthritis Care Res. (Hoboken.) 64(4), 465–474 (2012).
2.
Fernandes L, Hagen KB, Bijlsma JW et al. EULAR recommendations for the non-pharmacological core management of hip and knee osteoarthritis. Ann. Rheum. Dis. 72(7), 1125–1135 (2013).
3.
McAlindon TE, Bannuru RR, Sullivan MC et al. OARSI guidelines for the non-surgical management of knee osteoarthritis. Osteoarthritis Cartilage 22(3), 363–388 (2014).
4.
Fransen M, McConnell S. Exercise for osteoarthritis of the knee. Cochrane Database Syst. Rev. 4, CD004376 (2008).
5.
Zhang W, Nuki G, Moskowitz RW et al. OARSI recommendations for the management of hip and knee osteoarthritis: part III: changes in evidence following systematic cumulative update of research published through January 2009. Osteoarthritis Cartilage 18(4), 476–499 (2010).
6.
Juhl C, Christensen R, Roos EM, Zhang W, Lund H. Impact of exercise type and dose on pain and disability in knee osteoarthritis: a systematic review and meta-regression analysis of randomized controlled trials. Arthritis Rheumatol. 66(3), 622–636 (2014).
7.
Zhang W, Moskowitz RW, Nuki G et al. OARSI recommendations for the management of hip and knee osteoarthritis, Part II: OARSI evidence-based, expert consensus guidelines. Osteoarthritis Cartilage 16(2), 137–162 (2008).
8.
McGettigan P, Henry D. Use of non-steroidal anti-inflammatory drugs that elevate cardiovascular risk: an examination of sales and essential medicines lists in low-, middle-, and high-income countries. PLoS Med. 10(2), e1001388 (2013).
9.
Doi T, Akai M, Fujino K et al. Effect of home exercise of quadriceps on knee osteoarthritis compared with nonsteroidal antiinflammatory drugs: a randomized controlled trial. Am. J. Phys. Med. Rehabil. 87(4), 258–269 (2008).
10.
Bucher HC, Guyatt GH, Griffith LE, Walter SD. The results of direct and indirect treatment comparisons in meta-analysis of randomized controlled trials. J. Clin. Epidemiol. 50(6), 683–691 (1997).
11.
Hansen JB, Juhl CB, Boutron I et al. Assessing bias in osteoarthritis trials included in Cochrane reviews: protocol for a meta-epidemiological study. BMJ Open 4(10), e005491 (2014).
12.
Liberati A, Altman DG, Tetzlaff J et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. PLoS Med. 6(7), e1000100 (2009).
13.
Higgins JP, Altman DG, Gotzsche PC et al. The Cochrane Collaboration's tool for assessing risk of bias in randomised trials. BMJ 343, d5928 (2011).
14.
da Costa BR, Nuesch E, Rutjes AW et al. Combining follow-up and change data is valid in meta-analyses of continuous outcomes: a meta-epidemiological study. J. Clin. Epidemiol. 66(8), 847–855 (2013).
15.
Riley RD, Higgins JP, Deeks JJ. Interpretation of random effects meta-analyses. BMJ 342, d549 (2011).
16.
Garner SE, Fidan DD, Frankish R, Maxwell L. Rofecoxib for osteoarthritis. Cochrane Database Syst. Rev. 2005(1), CD005115 (2005).
17.
Day R, Morrison B, Luza A, Castaneda O, Strusberg A, Nahir M et al. A randomized trial of the efficacy and tolerability of the COX-2 inhibitor rofecoxib vs ibuprofen in patients with osteoarthritis. Rofecoxib/Ibuprofen Comparator Study Group. Arch Intern Med. 160(12), 1781–1787 (2000).
18.
Ehrich EW, Schnitzer TJ, McIlwain H, Levy R, Wolfe F, Weisman M et al. Effect of specific COX-2 inhibition in osteoarthritis of the knee: a 6 week double blind, placebo controlled pilot study of rofecoxib. Rofecoxib Osteoarthritis Pilot Study Group. J. Rheumatol. 26(11), 2438–2447 (1999).
19.
Gibofsky A, Williams GW, McKenna F, Fort JG. Comparing the efficacy of cyclooxygenase 2-specific inhibitors in treating osteoarthritis: appropriate trial design considerations and results of a randomized, placebo-controlled trial. Arthritis Rheum. 48(11), 3102–3111 (2003).
20.
Truitt KE, Sperling RS, Ettinger WH Jr, Greenwald M, DeTora L, Zeng Q et al. A multicenter, randomized, controlled trial to evaluate the safety profile, tolerability, and efficacy of rofecoxib in advanced elderly patients with osteoarthritis. Aging (Milano) 13(2), 112–121 (2001).
21.
Nüesch E, Rutjes AW, Husni E, Welch V, Juni P. Oral or transdermal opioids for osteoarthritis of the knee or hip. Cochrane Database Syst. Rev. 4, CD003115 (2009).
22.
Peloso PM, Bellamy N, Bensen W, Thomson GT, Harsanyi Z, Babul N et al. Double blind randomized placebo control trial of controlled release codeine in the treatment of osteoarthritis of the hip or knee. J. Rheumatol. 27(3), 764–771 (2000).
23.
Langford R, McKenna F, Ratcliffe S, Vojtassak J, Richarz U. Transdermal fentanyl for improvement of pain and functioning in osteoarthritis: a randomized, placebo-controlled trial. Arthritis Rheum. 54(6), 1829–1837 (2006).
24.
Caldwell JR, Rapoport RJ, Davis JC, Offenberg HL, Marker HW, Roth SH et al. Efficacy and safety of a once-daily morphine formulation in chronic, moderate-to-severe osteoarthritis pain: results from a randomized, placebo-controlled, double-blind trial and an open-label extension trial. J. Pain Symptom Manage 23(4), 278–291 (2002).
25.
Markenson JA, Croft J, Zhang PG, Richards P. Treatment of persistent pain associated with osteoarthritis with controlled-release oxycodone tablets in a randomized controlled clinical trial. Clin. J. Pain 21(6), 524–535 (2005).
26.
Chindalore VL, Craven RA, Yu KP, Butera PG, Burns LH, Friedmann N. Adding ultralow-dose naltrexone to oxycodone enhances and prolongs analgesia: a randomized, controlled trial of Oxytrex. J. Pain 6(6), 392–399 (2005).
27.
Matsumoto AK, Babul N, Ahdieh H. Oxymorphone extended-release tablets relieve moderate to severe pain and improve physical function in osteoarthritis: results of a randomized, double-blind, placebo- and active-controlled Phase III trial. Pain Med. 6(5), 357–366 (2005).
28.
Zautra AJ, Smith BW. Impact of controlled-release oxycodone on efficacy beliefs and coping efforts among osteoarthritis patients with moderate to severe pain. Clin. J. Pain 21(6), 471–477 (2005).
29.
Kivitz A, Ma C, Ahdieh H, Galer BS. A 2-week, multicenter, randomized, double-blind, placebo-controlled, dose-ranging, Phase III trial comparing the efficacy of oxymorphone extended release and placebo in adults with pain associated with osteoarthritis of the hip or knee. Clin. Ther. 28(3), 352–364 (2006).
30.
Towheed TE, Maxwell L, Judd MG, Catton M, Hochberg MC, Wells G. Acetaminophen for osteoarthritis. Cochrane Database Syst. Rev. 1, CD004257 (2006).
31.
Case JP, Baliunas AJ, Block JA. Lack of efficacy of acetaminophen in treating symptomatic knee osteoarthritis: a randomized, double-blind, placebo-controlled comparison trial with diclofenac sodium. Arch Intern Med. 163(2), 169–178 (2003).
32.
Pincus T, Koch G, Lei H, Mangal B, Sokka T, Moskowitz R et al. Patient Preference for Placebo, Acetaminophen (paracetamol) or Celecoxib Efficacy Studies (PACES): two randomised, double blind, placebo controlled, crossover clinical trials in patients with knee or hip osteoarthritis. Ann. Rheum. Dis. 63(8), 931–939 (2004).
33.
Golden HE, Moskowitz RW, Minic M. Analgesic efficacy and safety of nonprescription doses of naproxen sodium compared with acetaminophen in the treatment of osteoarthritis of the knee. Am. J. Ther. 11(2), 85–94 (2004).
34.
Miceli-Richard C, Le BM, Schmidely N, Dougados M. Paracetamol in osteoarthritis of the knee. Ann. Rheum. Dis. 63(8), 923–930 (2004).
35.
Cepeda MS, Camargo F, Zea C, Valencia L. Tramadol for osteoarthritis. Cochrane Database Syst. Rev. 3, CD005522 (2006).
36.
Babul N, Noveck R, Chipman H, Roth SH, Gana T, Albert K. Efficacy and safety of extended-release, once-daily tramadol in chronic pain: a randomized 12-week clinical trial in osteoarthritis of the knee. J. Pain Symptom Manage 28(1), 59–71 (2004).
37.
Emkey R, Rosenthal N, Wu SC, Jordan D, Kamin M. Efficacy and safety of tramadol/acetaminophen tablets (Ultracet) as add-on therapy for osteoarthritis pain in subjects receiving a COX-2 nonsteroidal antiinflammatory drug: a multicenter, randomized, double-blind, placebo-controlled trial. J. Rheumatol. 31(1), 150–156 (2004).
38.
Malonne H, Coffiner M, Sonet B, Sereno A, Vanderbist F. Efficacy and tolerability of sustained-release tramadol in the treatment of symptomatic osteoarthritis of the hip or knee: a multicenter, randomized, double-blind, placebo-controlled study. Clin. Ther. 26(11), 1774–1782 (2004).
39.
Bartels EM, Lund H, Hagen KB, Dagfinrud H, Christensen R, Danneskiold-Samsoe B. Aquatic exercise for the treatment of knee and hip osteoarthritis. Cochrane Database Syst. Rev. 4, CD005523 (2007).
40.
Cochrane T, Davey RC, Matthes Edwards SM. Randomised controlled trial of the cost–effectiveness of water-based therapy for lower limb osteoarthritis. Health Technol. Assess. 9(31), 1–114 (2005).
41.
Foley A, Halbert J, Hewitt T, Crotty M. Does hydrotherapy improve strength and physical function in patients with osteoarthritis – a randomised controlled trial comparing a gym based and a hydrotherapy based strengthening programme. Ann. Rheum. Dis. 62(12), 1162–1167 (2003).
42.
Wang TJ. Aquatic Exercise Improves Flexibility, Strength, and Walk Time in Osteoarthritis [PhD Thesis]. University of Washington, WA, USA (2004).
43.
Patrick DL, Ramsey SD, Spencer AC, Kinne S, Belza B, Topolski TD. Economic evaluation of aquatic exercise for persons with osteoarthritis. Med. Care 39(5), 413–424 (2001).
44.
Baker KR, Nelson ME, Felson DT, Layne JE, Sarno R, Roubenoff R. The efficacy of home based progressive strength training in older adults with knee osteoarthritis: a randomized controlled trial. J. Rheumatol. 28(7), 1655–1665 (2001).
45.
Bautch JC, Malone DG, Vailas AC. Effects of exercise on knee joints with osteoarthritis: a pilot study of biologic markers. Arthritis Care Res. 10(1), 48–55 (1997).
46.
Bennell KL, Hinman RS, Metcalf BR et al. Efficacy of physiotherapy management of knee joint osteoarthritis: a randomised, double blind, placebo controlled trial. Ann. Rheum. Dis. 64(6), 906–912 (2005).
•• A very well conducted trials comparing exercise to placebo.
47.
Deyle GD, Henderson NE, Matekel RL, Ryder MG, Garber MB, Allison SC. Effectiveness of manual physical therapy and exercise in osteoarthritis of the knee. A randomized, controlled trial. Ann. Intern Med. 132(3), 173–181 (2000).
48.
Ettinger WH Jr, Burns R, Messier SP, Applegate W, Rejeski WJ, Morgan T et al. A randomized trial comparing aerobic exercise and resistance exercise with a health education program in older adults with knee osteoarthritis. The Fitness Arthritis and Seniors Trial (FAST). JAMA 277(1), 25–31 (1997).
49.
Fransen M, Crosbie J, Edmonds J. Physical therapy is effective for patients with osteoarthritis of the knee: a randomized controlled clinical trial. J. Rheumatol. 28(1), 156–164 (2001).
50.
Fransen M, Nairn L, Winstanley J, Lam P, Edmonds J. Physical activity for osteoarthritis management: a randomized controlled clinical trial evaluating hydrotherapy or Tai Chi classes. Arthritis Rheum. 57(3), 407–414 (2007).
51.
Gur H, Cakin N, Akova B, Okay E, Kucukoglu S. Concentric versus combined concentric-eccentric isokinetic training: effects on functional capacity and symptoms in patients with osteoarthrosis of the knee. Arch Phys. Med. Rehabil. 83(3), 308–316 (2002).
52.
Hay EM, Foster NE, Thomas E, Peat G, Phelan M, Yates HE et al. Effectiveness of community physiotherapy and enhanced pharmacy review for knee pain in people aged over 55 presenting to primary care: pragmatic randomised trial. BMJ 333(7576), 995 (2006).
53.
Hopman-Rock M, Westhoff MH. The effects of a health educational and exercise program for older adults with osteoarthritis for the hip or knee. J. Rheumatol. 27(8), 1947–1954 (2000).
54.
Huang MH, Lin YS, Yang RC, Lee CL. A comparison of various therapeutic exercises on the functional status of patients with knee osteoarthritis. Semin. Arthritis Rheum. 32(6), 398–406 (2003).
55.
Hughes SL, Seymour RB, Campbell R, Pollak N, Huber G, Sharma L. Impact of the fit and strong intervention on older adults with osteoarthritis. Gerontologist 44(2), 217–228 (2004).
56.
Huang MH, Yang RC, Lee CL, Chen TW, Wang MC. Preliminary results of integrated therapy for patients with knee osteoarthritis. Arthritis Rheum. 53(6), 812–820 (2005).
57.
Keefe FJ, Blumenthal J, Baucom D, Affleck G, Waugh R, Caldwell DS et al. Effects of spouse-assisted coping skills training and exercise training in patients with osteoarthritic knee pain: a randomized controlled study. Pain 110(3), 539–549 (2004).
58.
Kovar PA, Allegrante JP, MacKenzie CR, Peterson MG, Gutin B, Charlson ME. Supervised fitness walking in patients with osteoarthritis of the knee. A randomized, controlled trial. Ann. Intern Med. 116(7), 529–534 (1992).
59.
Maurer BT, Stern AG, Kinossian B, Cook KD, Schumacher HR Jr. Osteoarthritis of the knee: isokinetic quadriceps exercise versus an educational intervention. Arch Phys. Med. Rehabil. 80(10), 1293–1299 (1999).
60.
Messier SP, Loeser RF, Miller GD, Morgan TM, Rejeski WJ, Sevick MA et al. Exercise and dietary weight loss in overweight and obese older adults with knee osteoarthritis: the Arthritis, Diet, and Activity Promotion Trial. Arthritis Rheum. 50(5), 1501–1510 (2004).
61.
Minor MA, Hewett JE, Webel RR, Anderson SK, Kay DR. Efficacy of physical conditioning exercise in patients with rheumatoid arthritis and osteoarthritis. Arthritis Rheum. 32(11), 1396–1405 (1989).
62.
O'Reilly SC, Muir KR, Doherty M. Effectiveness of home exercise on pain and disability from osteoarthritis of the knee: a randomised controlled trial. Ann. Rheum. Dis. 58(1), 15–19 (1999).
63.
Peloquin L, Bravo G, Gauthier P, Lacombe G, Billiard JS. Effects of a cross-training exercise program in persons with osteoarthritis of the knee a randomized controlled trial. J. Clin. Rheumatol. 5(3), 126–136 (1999).
64.
Quilty B, Tucker M, Campbell R, Dieppe P. Physiotherapy, including quadriceps exercises and patellar taping, for knee osteoarthritis with predominant patello–femoral joint involvement: randomized controlled trial. J. Rheumatol. 30(6), 1311–1317 (2003).
65.
Rogind H, Bibow-Nielsen B, Jensen B, Moller HC, Frimodt-Moller H, Bliddal H. The effects of a physical training program on patients with osteoarthritis of the knees. Arch Phys. Med. Rehabil. 79(11), 1421–1427 (1998).
66.
Schilke JM, Johnson GO, Housh TJ, O'Dell JR. Effects of muscle-strength training on the functional status of patients with osteoarthritis of the knee joint. Nurs. Res. 45(2), 68–72 (1996).
67.
Song R, Lee EO, Lam P, Bae SC. Effects of tai chi exercise on pain, balance, muscle strength, and perceived difficulties in physical functioning in older women with osteoarthritis: a randomized clinical trial. J. Rheumatol. 30(9), 2039–2044 (2003).
68.
Talbot LA, Gaines JM, Huynh TN, Metter EJ. A home-based pedometer-driven walking program to increase physical activity in older adults with osteoarthritis of the knee: a preliminary study. J. Am. Geriatr. Soc. 51(3), 387–392 (2003).
69.
Thomas KS, Muir KR, Doherty M, Jones AC, O'Reilly SC, Bassey EJ. Home based exercise programme for knee pain and knee osteoarthritis: randomised controlled trial. BMJ 325(7367), 752 (2002).
70.
Thorstensson CA, Roos EM, Petersson IF, Ekdahl C. Six-week high-intensity exercise program for middle-aged patients with knee osteoarthritis: a randomized controlled trial [ISRCTN20244858]. BMC Musculoskelet. Disord. 6, 27 (2005).
71.
Topp R, Woolley S, Hornyak J III, Khuder S, Kahaleh B. The effect of dynamic versus isometric resistance training on pain and functioning among adults with osteoarthritis of the knee. Arch. Phys. Med. Rehabil. 83(9), 1187–1195 (2002).
72.
van Baar ME, Assendelft WJ, Dekker J, Oostendorp RA, Bijlsma JW. Effectiveness of exercise therapy in patients with osteoarthritis of the hip or knee: a systematic review of randomized clinical trials. Arthritis Rheum. 42(7), 1361–1369 (1999).
73.
van Tunen JA, van der Leeden M, Bos WH et al. Optimization of analgesics for greater exercise therapy participation among patients with knee osteoarthritis and severe pain: a feasibility study. Arthritis Care Res.(Hoboken.) 68(3), 332–340 (2016).
• An important feasibility trial on combination of analgesics and exercise therapy for osteoarthritis pain.
74.
National Institute for Health and Clinical Excellence. Osteoarthritis: national clinical guideline for care and management in adults (2014). www.nice.org.uk/guidance/cg177.
75.
Fransen M, McConnell S, Harmer AR, van der Esch M, Simic M, Bennell KL. Exercise for osteoarthritis of the knee. Cochrane. Database. Syst. Rev. 1, CD004376 (2015).
76.
Uthman OA, van der Windt DA, Jordan JL et al. Exercise for lower limb osteoarthritis: systematic review incorporating trial sequential analysis and network meta-analysis. BMJ 347, f5555 (2013).
77.
Bannuru RR, Schmid CH, Kent DM, Vaysbrot EE, Wong JB, McAlindon TE. Comparative effectiveness of pharmacologic interventions for knee osteoarthritis: a systematic review and network meta-analysis. Ann. Intern. Med. 162(1), 46–54 (2015).
Information & Authors
Information
Published In
Copyright
© Future Medicine Ltd.
History
Published online: 27 June 2016
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Comparable effects of exercise and analgesics for pain secondary to knee osteoarthritis: a meta-analysis of trials included in Cochrane systematic reviews. (2016) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2016-0007
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Yu Fu, Hairui Li, Mingke You, Li Wang, Weizhi Liu, Kai Zhou, Lingcheng Wang, Xi Chen, Gang Chen, Evaluation of Large Language Models in Generating Physical Exercise Rehabilitation Programs for Musculoskeletal Disorders Across Multiple Clinical Scenarios, Healthcare, 10.3390/healthcare14152389, 14, 15, (2389), (2026).
- Dmitriy Viderman, Sultan Kalikanov, Akerke Mazhibiyeva, Alua Shagirova, Malika Toleubekova, Mina Aubakirova, Yerkin G. Abdildin, Impact of therapeutic exercises on pain-related outcomes in patients with knee osteoarthritis: an umbrella review of 116 systematic reviews, Frontiers in Pain Research, 10.3389/fpain.2026.1717540, 7, (2026).
- Caterina Mauri, Charles James Steward, Attilio Parisi, Mathew Hill, Sara Severoni, Claudia Cerulli, Elisa Grazioli, The Effects of 24 Weeks Sensorimotor Training on Balance, Physical Function, and Pain in Women with Knee Osteoarthritis, Sports, 10.3390/sports14010043, 14, 1, (43), (2026).
- Lisa A. Mandl, Kelli D. Allen, Amanda E. Nelson, Musculoskeletal disorders: focus on osteoarthritis, Women and Health, 10.1016/B978-0-443-45863-7.00115-3, (2159-2178), (2026).
- Xueliang Peng, Xuanning Chen, Yifan Zhang, Zhichao Tian, Meihua Wang, Zhuoyue Chen, Advances in the pathology and treatment of osteoarthritis, Journal of Advanced Research, 10.1016/j.jare.2025.01.053, 78, (257-283), (2025).
- Sıdıka Büyükvural Şen, Burhan Fatih Koçyiğit, Emine Aygül Ortaç, Meryem Kösehasanoğulları, Nilüfer Aygün Bilecik, Comparison of the effects of high-intensity laser therapy and low-level laser therapy in knee osteoarthritis, Clinical Rheumatology, 10.1007/s10067-025-07657-9, 44, 11, (4661-4669), (2025).
- N. Savouroux, Kinesiterapia della gonartrosi, EMC - Medicina Riabilitativa, 10.1016/S1283-078X(25)50366-8, 32, 2, (1-24), (2025).
- N. Savouroux, Kinesiterapia de la gonartrosis, EMC - Kinesiterapia - Medicina Física, 10.1016/S1293-2965(25)50347-X, 46, 2, (1-25), (2025).
- Rana S. Hinman, Michelle Hall, Sarah Comensoli, Kim L. Bennell, Exercise and Sports Science Australia (ESSA) updated Position Statement on exercise and physical activity for people with hip/knee osteoarthritis, Pensar en Movimiento: Revista de Ciencias del Ejercicio y la Salud, 10.15517/pensarmov.v22i2.62992, 22, 2, (e62992), (2024).
- Lynette Law, Joshua L Heerey, Brooke L Devlin, Peter Brukner, Joanne L Kemp, Amanda Attanayake, Mark D Hulett, Alysha De Livera, Andrea B Mosler, Hayden G Morris, Nathan P White, Adam G Culvenor, Effectiveness of an anti-inflammatory diet versus low-fat diet for knee osteoarthritis: the FEAST randomised controlled trial protocol, BMJ Open, 10.1136/bmjopen-2023-079374, 14, 4, (e079374), (2024).
- See more