An overview and discussion of the Patient-Centered Outcomes Research Institute's decision aid portfolio
Abstract
Decision aids (DAs) help patients make informed healthcare decisions in a manner consistent with their values and preferences. Despite their promise, DAs developed with public research dollars are not being implemented and adopted in real-world patient care settings at a rate consistent with which they are being developed. To appraise the sum of the parts of the portfolio and create a strategic imperative surrounding future funding, the Patient-Centered Outcomes Research Institute (PCORI) tasked the Duke Evidence Synthesis Group with evaluating its DA portfolio. This paper describes PCORI's portfolio of DAs according to the Duke Evidence Synthesis Group's analysis in the context of PCORI's mission and the field of decision science. The results revealed a diversity within PCORI's portfolio of funded DA projects. Findings support the movement toward more rigorous DA development, assessment and maintenance. PCORI's funding priorities related to DAs are clarified and comparative questions of interest are posed.
First draft submitted: 7 January 2016; Accepted for publication: 10 April 2016; Published online: 13 June 2016
Aim
The Patient-Centered Outcomes Research Institute (PCORI) is an independent nonprofit, nongovernmental organization with the mission of informing healthcare decisions and improving health outcomes by producing and promoting high-integrity, evidence-based information that comes from research, guided by patients, caregivers and the healthcare community. Specifically, we fund comparative clinical effectiveness research (CER), as well as work to improve the methods used to conduct such studies. The goal of PCORI's work is to determine which of the many healthcare options available to patients and those who care for them work best in particular circumstances. We do this by taking a particular approach to CER called patient-centered outcomes research (PCOR) that addresses the questions and concerns most relevant to patients. An important part of PCORI's mission is to make information and evidence accessible and understandable to multiple audiences, including patients, caregivers and clinicians. Producing information is not enough; the information must be clear, comprehensible and reach those who need it to make healthcare decisions.
PCORI views decision aids (DAs) as a promising means to help patients make informed healthcare decisions in a manner consistent with their values and preferences. DAs are intended to help people weigh benefits and harms of treatment options, which often involve scientific uncertainty [1], by educating patients about their options, clarifying personal values and encouraging shared decision-making with clinicians. DAs are the most frequently discussed modality for promoting shared decision-making between patient and clinicians. Shared decision-making is a process of communication, deliberation and decision-making in which: the clinician shares information about relevant testing or treatment options with the patient, including the severity and probability of potential harms and benefits; the patient explores and shares his or her preferences with the clinicians regarding these harms, benefits and potential outcomes and the clinician and patient reach a mutual decision about the treatment plan through an interactive process of reflection and discussion [2].
A recent systematic review of 115 randomized trials found that use of DAs was associated with increased patient knowledge regarding options, lower decisional conflict, greater value concordance with decisions, more active decision-making and more accurate risk perceptions [1]. Hundreds of DAs have been produced by a mix of nonprofit, academic and commercial organizations, many of which are accessible online [3]. However the quality of these tools has been shown to vary, with some failing to cite evidence sources and others demonstrating presentation biases [4]. Citing the need for DA developers to follow recognized methods, avoid bias and cite valid and current evidence sources, The International Patient Decision Aids Standards (IPDAS) [5] collaboration was established to enhance the quality and effectiveness of patient DAs by establishing an evidence-informed framework aimed at improving the content, development, implementation and evaluation of DAs.
Promoting high-quality evidence-based DAs is consistent with PCORI's mission. PCORI has funded DAs projects across several of its national priority programs. The projects have been diverse in their disease focus, methods, aims and design and have been funded at different points in the trajectory of DA development. For example, some funded projects proposed developing, testing and comparing new DAs, while others proposed comparing DAs with established efficacy.
Despite their promise, evidence suggests that DAs developed with public research dollars are not being implemented and adopted in real-world patient care settings at a rate consistent with which they are being developed [6–10]. Recent research and commentary has emphasized the need to move effective DAs into clinical practice more efficiently and effectively [11–13]. With this in mind, PCORI examined its current DA portfolio, aiming to assess early lessons and identify opportunities to refine priorities in DA research funding at PCORI. As part of this work, PCORI tasked the Duke Evidence Synthesis Group (ESG) to evaluate and describe the contents of PCORI's DA portfolio.
The purpose of this paper is to describe the PCORI portfolio of DAs according to the ESG's analysis in the context of PCORI's mission and the field of decision science and to articulate the implications of this analysis on PCORI's DA funding strategy going forward.
Data abstraction methodology
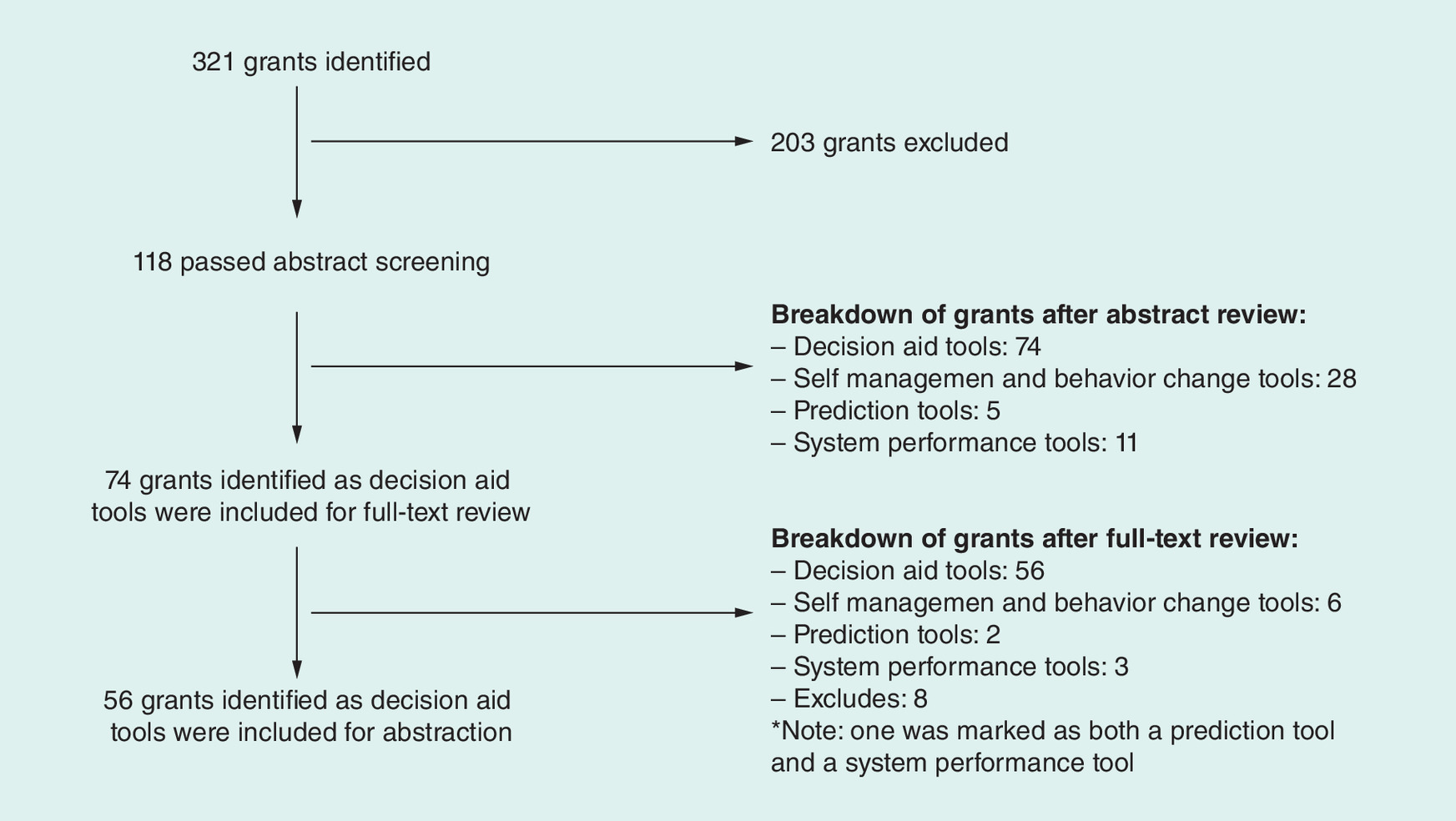
In order to facilitate the consistent identification of PCORI projects for the DA portfolio, the Duke ESG and PCORI agreed upon a working definition for DAs: “tools that help patients understand evidence about clinical management options and their preferences about clinical outcomes”. Using this definition, the Duke ESG sought to identify DA-relevant projects by reviewing titles and abstracts of all PCORI-funded projects through January 2015. Two independent investigators screened each project and either included projects as being relevant or excluded them from further consideration. When the two investigators could not agree upon a project's disposition, a third investigator's input was sought to determine a majority opinion, which was used to categorize the project. Figure 1 presents the process for the retrieval, screening and review of PCORI projects which were ultimately included for abstraction (n = 56).
Following title and abstract screening, a data abstraction form was developed to systematically characterize the identified DA projects. This abstraction form was reviewed and approved by PCORI and implemented in a DistillerSR database (Evidence Partners Inc., ON, Canada). One of three Duke ESG team members (ER Myers, JM Gierisch, MJ Crowley) reviewed the proposal for each project and abstracted relevant data elements. A fourth team member (GD Sanders) reviewed and confirmed the entries on each data abstraction form; any conflicts were resolved through discussion. Data abstraction relied upon the application for funding for each project, and did not incorporate additional information from progress reports, program officers or investigator teams.
PCORI's DA portfolio was described by summarizing DA target diseases, target populations, relevant patient-centered outcomes and numerous other characteristics. Features of evaluation studies were examined by including study designs, sample characteristics and outcomes. Data presented do not identify specific investigators or projects. Project-specific information for all PCORI funded projects is available online [14].
Descriptive overview of PCORI's funded decision aid portfolio
The review of PCORI's portfolio revealed that, as of January 2015, PCORI had funded 56 projects with a DA component, covering a broad range of health states and decisions. These projects comprised 17% of PCORI's funded portfolio at that time, an investment of US$81.3 million.
Table 1 highlights target diseases for the identified DA projects. Most projects targeted either cancer (36%) or cardiovascular health (20%). Mental health, muscular/skeletal disorders and multiple chronic conditions were each addressed by 11% of projects. In total, 39% of projects addressed more than one disease and 7% had no specific target disease. DAs projects represented more than 50% of PCORI's overall research in the areas of allergies/immune disorders, cancer, cardiovascular health, digestive system diseases, infectious diseases and muscular and skeletal disorders.
Table 2 describes target populations for the 56 funded DA projects. Target populations included any demographic group specified as being of interest within the project proposal; the enrolled population did not have to be limited to the target population. Projects commonly identified older adults (63%), racial/ethnic minority groups (55%) and/or residents of rural areas (27%) as relevant target populations.
Projects were categorized based on where along the care continuum they sought to address: primary prevention, secondary prevention and tertiary prevention/management [16]. Projects spanned these categories, but a large majority (70%) addressed tertiary prevention/management rather than primary (25%) or secondary prevention (20%). Of note, six projects addressed choices spanning more than one category.
DAs provided information that could be personalized for individual users in approximately 75% of the 56 funded projects. Tailored information included clinical characteristics (e.g., disease state, clinical location), patient characteristics (e.g., age, gender, language, literacy), patient values and others. DAs can affect a broad set of patient-centered outcomes by informing and facilitating choices between different options. Projects aimed to facilitate decisions that would affect patients’ quality of life (75%), knowledge (71%), treatment burden (70%), adverse effects (70%) and length of life (61%).
As part of their aims, 52 of the 56 funded projects (93%) proposed a study evaluating at least one DA. Patients were among the specified users for 93% of all DAs. Patients were the sole specified user in 46% of DAs; otherwise, patient-oriented DAs were designed for shared use by a patient and provider (26%), patient and caregiver (15%) or patient, provider and caregiver (6%). Providers were the sole users for 4% of DAs. In total, 34% of DAs were designed for use prior to or outside of a clinical encounter, 32% for use at the clinic but prior to the clinical encounter and 22% for use during a clinic encounter together with a provider.
Proposed DAs utilized a variety of formats (e.g., text, pictures/graphics, video) and delivery platforms (e.g., paper-based, web-based, tablet-based). Of DAs with specified formats, delivery platforms varied widely and many DAs used more than one; 34% of DAs utilized a web-based platform, 26% utilized tablets and 25% were paper-based (categories not mutually exclusive).
In total, 52 funded projects proposed a study evaluating a DA. Approximately 70% of projects proposed an RCT, 23% proposed cohort studies and 6% proposed a pre-/post-intervention design. Target sample sizes varied, with the largest number of projects (44% or 23/52) planning to include between 100 and 500 patients. Table 3 describes the primary and secondary outcomes that studies were designed to examine. While chosen outcomes varied widely, 63% of projects anticipated evaluating the impact of a DA on what treatment choices patients made. Investigators proposed examining patient satisfaction with the DA in 46% of studies, decisional conflict in 42% of studies and DA user-friendliness/ease of use in 25% of studies. Eight of the 52 projects (15%) listed only one evaluation outcome, while 34 projects (65%) listed three or more outcomes.
Given the leadership of the IPDAS collaboration, PCORI sought to determine how many projects explicitly mentioned incorporating the IPDAS recommendations into their DA development. Of the 56 projects, 32 did not cite IPDAS in any form in their proposal. The remaining 24 projects included references to using the IPDAS quality criteria and checklists during their DA development and/or evaluation.
In terms of DA availability, 15 projects explicitly indicated that the studied DAs would be publicly available following the funding period. Most of these DAs will be made available via the internet. Four projects involved explicitly proprietary DAs. The availability of the remaining 37 projects is not known based on the funded proposals. All 56 projects included a data sharing and dissemination plan, but many did not indicate whether the sharing of the DA would be free and/or whether any websites developed would be able to be accessed without restrictions.
Primary observations from portfolio overview
PCORI sought the Duke ESG's assistance in analyzing its portfolio of funded DA projects. In the context of PCORI's mission and the evolving field of decision science, the following four observations are particularly useful and actionable in helping PCORI set a strategic direction to guide future DA funding priorities:
1. The majority of DAs in the PCORI portfolio targeted cancer and cardiovascular disease;
2. There was substantial variability observed in the outcomes being utilized for evaluating DAs being studied;
3. The majority of projects did not explicitly reference IPDAS criteria in planned development and/or evaluation efforts;
4. The extent to which DAs will be made publicly available and readily maintained following the funding period, and how, is unclear in the majority of funded proposals.
Each of these observations is discussed in more detail below in the context of broader actionable themes, for which, PCORI provides rationale and guidance both for ourselves and for researchers in the relevant fields regarding PCORI's current funding prerogative and consider its implications. Our hope is that this discussion provides clarity about the ways in which PCORI will (and will not) support future DA research. Detail about which specific observation each theme is addressing is provided in parentheses below.
The need for DAs across key preference-sensitive clinical decisions (addresses observation 1)
Applications and corresponding projects utilizing efficacious or widely used DAs in a comparative effectiveness framework are of real interest to the communication and dissemination research program at PCORI, regardless of condition or disease area. The representation of cancer and cardiovascular disease in the current portfolio is a reflection of those applications which have fared best in the merit review and funding selection process to date – cancer and cardiovascular disease-focused DAs have not been prioritized over other disease areas by PCORI. PCORI is very interested in diversifying our portfolio to include DAs across a wide variety of preference-sensitive and practice-varying conditions. As such we invite and encourage DA researchers who are poised to conduct comparative effectiveness research on preference-sensitive clinical decisions to apply for PCORI funds. We also remain interested in comparative effectiveness of DAs in cancer and cardiovascular disease that answer remaining research questions and compliment the existing portfolio. We especially invite applications on PCORI high-priority topics listed for our pragmatic clinical studies program and our targeted studies program.
The need for standardization of DA development & evaluation (addresses observations 2 & 3)
To date, many DAs have been developed and introduced by myriad producers, with variation in quality. Variation in the use of conceptual frameworks and evaluation outcomes in DA studies makes comparing evidence of their effectiveness challenging. The IPDAS collaboration has made significant progress toward developing a process and corresponding checklist for DA developers to assess their products against which includes criteria for tool content, development process and effectiveness [4]. IPDAS has also developed an instrument (IPDASi) to allow for the independent rating of tool quality and published ‘minimum standards’ detailing which parts of DAs are considered ‘essential’ and which are merely ‘desirable’ [17]. Although PCORI is not currently funding development of new DAs as part of its strategic imperative, we remain concerned about the potential consequences should DAs with questionable accuracy, quality and/or efficacy reach patients. We therefore support the movement toward rigorous DA development and assessment and strongly encourage the field of DA researchers to map their DA development processes to the IPDAS criteria. We strongly encourage those submitting DA-directed comparative effectiveness projects to PCORI to adhere to IPDAS criteria related to the development and evaluation of their tools and to demonstrate adherence to these criteria in their PCORI applications.
The need for DA accessibility among patients, caregivers & healthcare providers (addresses observation 4)
PCORI's authorizing legislation mandates that we make the results of PCORI's funded studies available to patients, clinicians and the general public. PCORI supports making DAs widely accessible, because we believe that access to quality DAs is of the utmost importance for patients and providers. PCORI recognizes that a research portfolio consisting simply of research findings does not meet the intent of the authorizing legislation; the information must be available to the patient, it must be clear and comprehensible and it must be actionable. How best to make DAs widely available and maximize their use in real-world settings is a complex question. The shifting evidence base of many areas (e.g., oncology) requires regular updating of DA content; this can be both time and resource intensive, making DA repositories difficult to maintain over time. Intellectual property issues further complicate the matter. Under PCORI's current policy, funded institutions own the rights to DAs while PCORI maintains a nonexclusive license to provide access to the DAs. However, ensuring public accessibility to DAs via online repository or library is not sufficient for addressing the issue; since public posting does little to incorporate DAs into clinical practice nor does it ensure their routine incorporation of new research findings. If clinicians and patients are unaware of a publicly posted DA, or if a clinician does not trust a DA discovered by a patient, then the chance for the tool to influence decision-making is small. Ensuring the public availability of effective DAs is an important issue and a challenging one to solve given the reasons outlined above. PCORI will continue to work to ensure public awareness and availability of effective DAs without compromising decision-making by exposing patients, caregivers and providers to out of date content.
The need for integration & implementation of DAs into routine clinical care (addresses observations 2–4)
Challenges with maintaining DAs and integrating them into clinical care are in part why PCORI has chosen to focus on comparative effectiveness of DAs and other communication and dissemination approaches, rather than focusing on further DA development. Only when DAs are made accessible and incorporated into the clinical systems that support shared decision-making will there be sufficient uptake to inform decision-making. It is PCORI's hope that demonstrating the benefits of using DAs in different circumstances and settings and identifying effective dissemination and implementation strategies for translating effective DAs in to real-world practice (as determined by CER) will advance the business case for DAs, and emphasize the need for DA maintenance, so that tools remain relevant for decision-making. This interest in understanding the benefits of dissemination of high-quality DAs into real-world settings drive PCORI's priorities in DA research.
A path forward: PCORI's DA research agenda in the communication & dissemination research program
To date, PCORI has made a significant investment in DAs, reflecting a dedication to helping people make informed healthcare decisions and to exploring shared decision-making as a means to this end. Yet, despite the abundance of existing DAs and strong evidence for their efficacy in many areas, the rate of DA implementation in real-world care settings has been slow [17,18]. Consequently, few studies have evaluated the real-world impact of DAs on patient-centered outcomes and widespread adoption has not occurred [16]. PCORI is uniquely poised to fund research that aims to understand the comparative effectiveness of rigorously developed and evaluated DAs in the context of real-world care delivery settings. Moving forward, PCORI intends to focus its efforts and investment in DAs in order to help fill this important implementation gap.
One of PCORI's many goals is to help people make informed healthcare decisions based upon the best available evidence. The development of new DAs is not sufficient to attain this goal – it is only when effective DAs are utilized in real-world settings that they are able to have a true impact. As such, PCORI's focus moving forward is on measuring the comparative effectiveness of efficacious and/or widely used DAs (and other communication and dissemination interventions) in real-world settings. PCORI is not funding the development of new DAs and tools that might never reach patients in routine clinical practice or in their homes. DAs that never see public use, even if developed with rigor, fail to impact patients’ ability to make evidence-based, preference-sensitive decisions. PCORI remains very interested in DAs within a patient-centered, comparative effectiveness framework and strongly encourages researchers to consider research studies along these lines. Some specific questions of interest include:
What is the comparative effectiveness of different types (e.g., format, medium) of DAs in different settings and populations?
What is the comparative effectiveness of DAs versus other dissemination and translation strategies designed to optimize communication and facilitate shared decision-making in everyday practice?
What is the comparative effectiveness of DAs on informing diagnostic and treatment decisions for patients with limited English-language proficiency, limited education, hearing or visual impairments or mental health problems?
What is the comparative effectiveness of different dissemination and implementation strategies aimed at translating effective DAs in to real-world practice?
What are the best methods for communicating uncertainty and applicability issues using DAs?
Focusing PCORI's DA funding around the answers to these (and other) important comparative questions regarding the impact of DAs on patient-centered outcomes, and best practices for disseminating and implementing effective DAs into practice, aligns with PCORI's mandate and fills a critical gap in the current understanding of the successful facilitators and barriers to real-world DA integration and use.
Limitations
Several limitations warrant mention related to this analysis. First, there was opportunity for interpretation bias when conducting the DA categorization due to the fact information was solely obtained from project applications, rather than directly with project investigators. While most information used for categorization was explicit, interpretation was required in some instances. Similarly, the analysis does not account for changes and modifications made to PCORI-funded projects over time. It is not uncommon for research plans to evolve between the submission of application, award announcement and the conduct of the proposed project. Thus this analysis is limited by the fact that it reports on PCORI's DAs as proposed in applications, rather than as they are now. Additionally, this paper represents PCORI's experience with PCORI's first 2.5 years of research funding in this field. Given the limited scope of funding at one research funding institution, the findings may not be representative of the DA research field as a whole. The findings do, however, help PCORI reflect on our own experiences and help us to determine future issues to address.
Future perspective
Healthcare choices are becoming more complex and trade-offs between different alternatives more difficult to conceptualize. Patient expectations as partners and even drivers of their healthcare are changing the dynamic of how care is delivered and received. Decision makers have different needs and tolerances for uncertainty. Policy makers often take a population-based approach and look for guidance for decision-making using a point-estimate perspective. Individual patients and their clinicians will frequently take a much more personalized perspective on how well the evidence relates to the unique aspects of an individual or what is the degree of uncertainty in the findings as they apply to individual patient characteristics and circumstances. Patients and their clinicians have differing degrees of tolerance for risk and uncertainty and the tolerances are dynamic, changing as circumstances change.
As treatment choices become more complex, efforts to help patients sort through their options, personal values and tolerances will become even more important than they are today. This will pose challenges and opportunities to incorporate DAs into more routine practice and to make sure the DAs that are used are based on evidence that is current. The increasing emphasis on patient centricity will increase the need for the seamless incorporation of DAs into healthcare decision-making and that will place a burden on developers and funders of these aids to make sure that they represent the most innovative delivery methods, scientific rigor and the most current evidence. Building of off the work and goals of the IPDAS collaboration, the National Quality Forum recently announced plans to set national standards and develop a process for certifying high-quality DAs. While national standards and acknowledgement of ‘best practices’ in their development will likely be instrumental in keeping this field vital, recognizing that investments need to be made in maintaining and facilitating their use will also be essential for DAs to fully reach their potential and place in healthcare.
Conclusion
To date, PCORI has made a significant investment in DA comparative effectiveness research, reflecting a dedication to helping people make informed healthcare decisions and to exploring shared decision-making as a means to this end.
The results of the analysis revealed a wide diversity within PCORI's portfolio of funded DA project applications. These findings, along with trends in the field of decision science emphasizing the implementation of effective DAs into routine clinical care support the movement toward more rigorous DA development, assessment and maintenance. PCORIs emphasis on the study of the comparative effectiveness of efficacious and widely used DAs in real-world settings, rather than the development of new DAs, addresses an important implementation gap in the field of decision science and aligns optimally with PCORI's mission to promote informed healthcare decision-making and its goal of increasing the dissemination, implementation and adoption of DAs in real-world care settings.
| Target diseases or health conditions | Decision aid projects n (%), (n = 56)† | Complete PCORI portfolio n (%), (n = 365)†‡ | Proportion of complete portfolio that include decision aid (%) |
|---|---|---|---|
| Allergies and immune disorders | 1 (2) | 1 (0.3) | 100 |
| Cancer | 20 (36) | 34 (9.3) | 59 |
| Cardiovascular health | 11 (20) | 19 (5.2) | 58 |
| Digestive system diseases | 2 (4) | 2 (0.5) | 100 |
| Infectious diseases | 3 (5) | 5 (1.4) | 60 |
| Kidney disease | 2 (4) | 6 (1.6) | 33 |
| Liver disease | 1 (2) | 2 (0.5) | 50 |
| Mental/behavioral health | 6 (11) | 34 (9.3) | 18 |
| Multiple/comorbid chronic conditions | 6 (11) | 14 (3.8) | 43 |
| Muscular and skeletal disorders | 6 (11) | 8 (2.2) | 75 |
| Neurological disorders | 3 (5) | 16 (4.4) | 19 |
| Nutritional and metabolic disorders | 3 (5) | 16 (4.4) | 19 |
| Rare diseases | 4 (7) | 13 (3.6) | 31 |
| Reproductive and perinatal health | 4 (7) | 11 (3.0) | 36 |
| Respiratory diseases | 1 (2) | 17 (4.7) | 6 |
| Skin diseases | 0 (0) | 1 (0.3) | 0 |
| Trauma/injury | 1 (2) | 9 (2.5) | 11 |
| Other | 10 (18) | 20 (5.5) | 50 |
| No target disease | 4 (7) | NA | NA |
†Categories are not mutually exclusive.
‡Categorization of complete PCORI portfolio was performed using the PCORI website [15] and searching on primary condition/disease.
NA: Not applicable; PCORI: Patient-Centered Outcomes Research Institute.
| Target populations identified in study applications† | n (%), (n = 56‡) |
|---|---|
| Racial and ethnic minority groups | 31 (55) |
| Low-income groups | 12 (21) |
| Women | 12 (21) |
| Children (aged 0–17 years) | 8 (14) |
| Older adults (aged 65 years and older) | 35 (63) |
| Residents of rural areas | 15 (27) |
| Individuals with special healthcare need, including individuals with disabilities | 5 (9) |
| Individuals with multiple chronic diseases | 8 (14) |
| Individuals with rare diseases | 2 (4) |
| Individuals whose genetic makeup affects their medical outcomes | 1 (2) |
| Patients with low health literacy/numeracy and limited English proficiency | 6 (11) |
| Lesbian, gay, bisexual, transgender persons | 0 (0) |
| None of the above | 4 (7) |
†Target populations included any demographic group specified as being of interest within the proposal; the enrolled population did not have to be limited to the target population.
‡Categories not mutually exclusive.
| Primary and secondary outcomes to be evaluated in study | n (%)†, (n = 52) |
|---|---|
| Treatment choices made | 33 (63) |
| Patient satisfaction | 24 (46) |
| Decisional conflict | 22 (42) |
| User-friendliness/ease of use/acceptability | 13 (25) |
| Understanding of risk | 7 (13) |
| Decisional regret | 10 (19) |
| Decision quality | 9 (17) |
| Value-treatment concordance | 4 (8) |
| Feasibility | 3 (6) |
| Guideline concordant decisions | 1 (2) |
| Psychometric properties | 1 (2) |
| Other | 37 (71) |
†Categories are not mutually exclusive.
Purpose
Patient-Centered Outcomes Research Institute (PCORI) worked with the Duke Evidence Synthesis Group to better understand and evaluate the PCORI portfolio of decision aids (DAs). This review describes PCORI's DA portfolio in the context of PCORI's mission and the field of decision science and articulates the implications of this analysis on PCORI's DA funding strategy going forward.
Descriptive portfolio overview
The review of PCORI's portfolio revealed that, as of January 2015, PCORI had funded 56 projects with a DA component, covering a broad range of health states and decisions. These projects comprised 17% of PCORI's funded portfolio at that time, an investment of US$81.3 million.
Observations from portfolio overview
The analysis revealed a diversity within PCORI's portfolio of funded DA project applications with respect to disease focus, evaluation outcomes, explicit reference to IPDAS criteria and detail regarding public availability of DAs.
PCORI's decision aid research agenda
PCORI's focus moving forward is on measuring the comparative effectiveness of efficacious and/or widely used DAs (and other communication and dissemination interventions) in real-world settings.
Focusing on answers to important comparative questions regarding the impact of DAs on patient-centered outcomes, and best practices for disseminating and implementing effective DAs into practice helps to fill a critical gap in the current understanding of the successful facilitators and barriers to real-world DA integration and use.
Acknowledgements
The authors thank our colleagues who provided valuable insights related to this analysis and in developing this article: D Bild, S Chew, Y-P Chiang, M Henton, D Hickam and H Sox (PCORI); M Chobot and R Gray (Duke).
Financial & competing interests disclosure
MJ Crowley is supported by a Career Development Award from Veterans Affairs Health Services Research and Development (CDA 13-261). The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed
No writing assistance was utilized in the production of this manuscript.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
References
1.
Stacey D, Legare F, Col NF et al. Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst. Rev. 1, CD001431 (2014).
2.
Alston C, Berger Z, Brownlee S et al. Shared decision making strategies for best care: patient decision aids. Inst. Med. 1–49 (2014).
3.
Evans R, Elwyn G, Edwards A. Making interactive decision support for patients a reality. Inform. Prim. Care 12(2), 109–113 (2004).
4.
Elwyn G, O'Connor A, Stacey D et al. Developing a quality criteria framework for patient decision aids: online international Delphi consensus process. BMJ 333(7565), 417 (2006).
5.
International Patient Decision Aid Standards Collaboration. http://ipdas.ohri.ca/.
6.
Butler M, Ratner E, Mccreedy E, Shippee N, Kane RL. Decision Aids for Advance Care Planning. Rockville, MD, USA (2014).
7.
Butler M, Ratner E, McCreedy E, Shippee N, Kane RL. Decision aids for advance care planning: an overview of the state of the science. Ann. Intern. Med. 161(6), 408–418 (2014).
8.
Gravel K, Legare F, Graham ID. Barriers and facilitators to implementing shared decision-making in clinical practice: a systematic review of health professionals’ perceptions. Implement. Sci. 1, 16 (2006).
9.
Jimbo M, Rana GK, Hawley S et al. What is lacking in current decision aids on cancer screening? CA Cancer J. Clin. 63(3), 193–214 (2013).
10.
O'Donnell S, Cranney A, Jacobsen MJ, Graham ID, O'Connor AM, Tugwell P. Understanding and overcoming the barriers of implementing patient decision aids in clinical practice. J. Eval. Clin. Pract. 12(2), 174–181 (2006).
11.
Adesoye T, Greenberg CC, Neuman HB. Optimizing cancer care delivery through implementation science. Front. Oncol. (2016) (Epub ahead of print).
12.
Barry MJ. Resolving the decision aid paradox. JAMA Intern. Med. 175(5), 799–800 (2015).
13.
Tulsky JA. Decision aids in serious illness: moving what works into practice. JAMA Intern. Med. 175(7), 1221–1222 (2015).
14.
Patient-Centered Outcomes Research Institute. www.pcori.org.
15.
Patient-Centered Outcomes Research Institute. Research and Results. www.pcori.org/research-results.
16.
Katz D AA. Preventive medicine, integrative medicine and the health of the public. Commissioned paper for IOM Summit on Intergrative Medicine and the Health of the Public (2009). www.nationalacademies.org/hmd.
17.
Elwyn G, Scholl I, Tietbohl C et al. “Many miles to go …”: a systematic review of the implementation of patient decision support interventions into routine clinical practice. BMC Med. Inform. Decis. Mak. 13(Suppl. 2), S14 (2013).
18.
Wang EH, Gross CP, Tilburt JC et al. Shared decision making and use of decision AIDS for localized prostate cancer: perceptions from radiation oncologists and urologists. JAMA Intern. Med. 175(5), 792–799 (2015).
Information & Authors
Information
Published In
Copyright
© PCORI.
History
Published online: 14 June 2016
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
An overview and discussion of the Patient-Centered Outcomes Research Institute's decision aid portfolio. (2016) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2016-0002
Export citation
Select the citation format you wish to export for this article or chapter.