Transportability of the comparative effect of finerenone for the treatment of symptomatic chronic heart failure with left ventricular ejection fraction of ≥40%: insights from the FINEARTS-HF trial
Publication: Journal of Comparative Effectiveness Research
Abstract
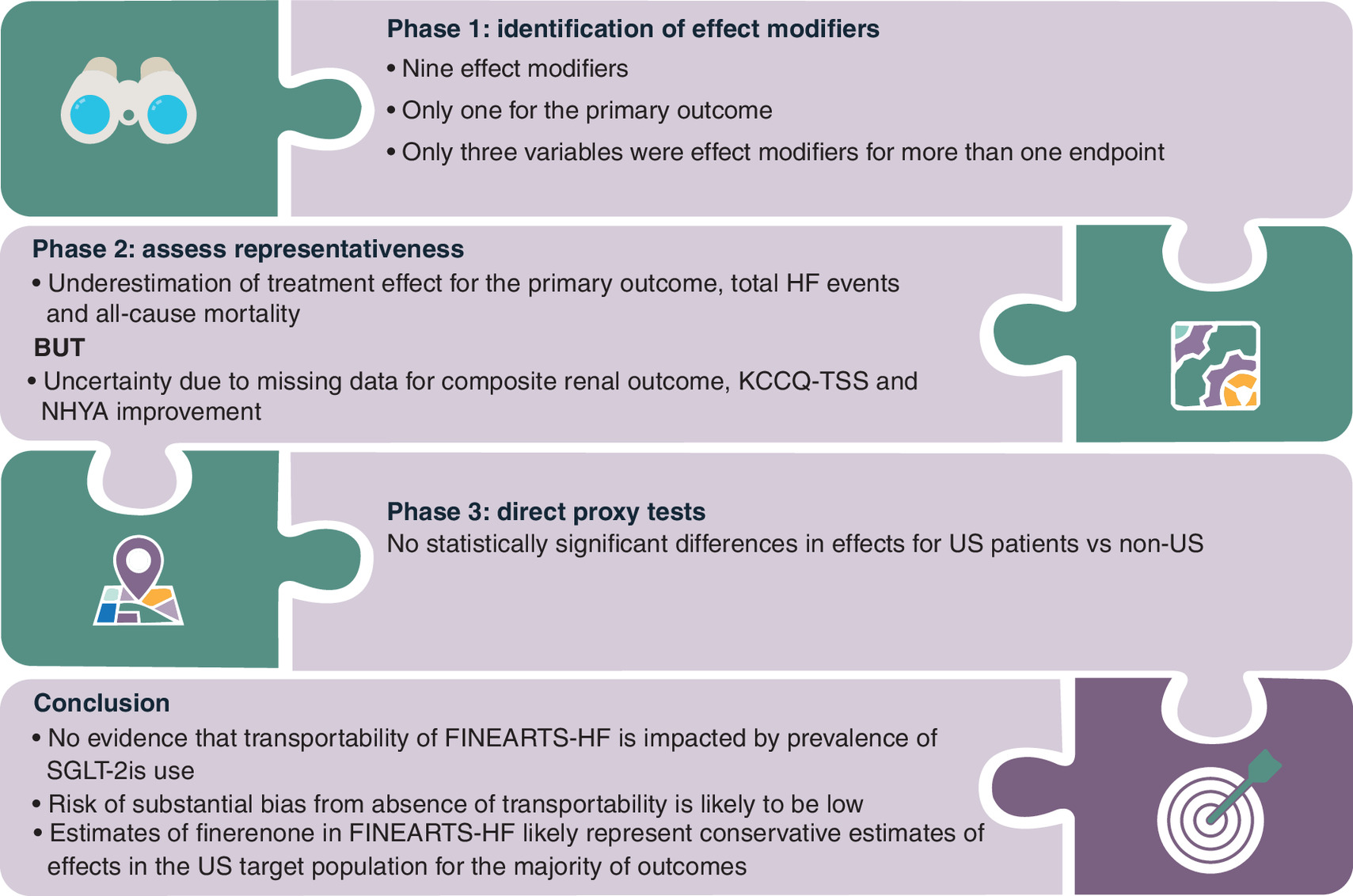
Aim: Global randomized controlled trials (RCTs) are used to inform reimbursement decisions in multiple markets, meaning the transportability of findings from these RCTs to multiple country-specific populations is critical for evidence-based decision making. This study evaluated the transportability of the FINEARTS-HF trial, which assessed finerenone in patients with heart failure (HF) and left ventricular ejection fraction ≥40%, to a real-world US population. Materials & methods: A three-phase transportability assessment was conducted. First, potential effect modifiers were identified through systematic literature review and confirmed through interaction analyses using data from FINEARTS-HF. Second, representativeness was assessed by comparing the distribution of effect modifiers in the trial and a population derived from a US electronic health record dataset. Third, direct proxy tests explored heterogeneity of treatment effects in FINEARTS-HF between US and non-US patients. Results: Effect modifier analysis identified that treatment effects of finerenone were homogeneous across subgroups, with limited evidence of effect modification. Comparisons with the US target population indicated overall good alignment across key characteristics, with only modest imbalances, suggesting that the trial results may underestimate positive treatment effects in the US target population (i.e., effect on the primary outcome over 0.84 [0.74; 0.95]). Direct proxy tests found no statistically significant regional heterogeneity in treatment effects. Conclusion: This study provides a structured assessment of finerenone trial transportability. Findings support the robustness of FINEARTS-HF results for US clinical practice and are not impacted by the prevalence of SGLT2-is use. The risk of transportability bias is likely to be low.
Plain language summary: Can results from a global heart failure trial be used in different countries?
What is this article about?
Clinical trials are often run in many countries. However, patients from trials may not always look the same as patients treated in everyday clinical practice in a specific country. This raises an important question: can results from a trial be reliably used to inform decisions at a country level? This article examines whether the results of the FINEARTS-HF trial, evaluating finerenone in patients with chronic heart failure and a left ventricular ejection fraction ≥40%, are applicable to patients from the US.
How was this assessed?
The researchers used a step-by-step approach. First, they identified patient characteristics that could influence how well the treatment works. Next, they compared these characteristics between people in the trial and patients treated in routine care in the US. Finally, they checked whether the treatment worked differently in patients enrolled in the US compared with those enrolled in other countries.
What were the results?
The people included in the trial were similar to patients treated in routine practice. There was no evidence that finerenone worked differently in one country compared with another. The small differences observed suggest that the trial results may slightly underestimate how much benefit patients could experience.
What do the results mean?
Using the US as an example, the study shows that results from the FINEARTS-HF trial can be applied with confidence across different healthcare settings. This approach can help decision-makers judge whether results from global clinical trials are relevant in their own countries.
Graphical abstract
Supplementary Material
Reference
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
National Institute for Health and Care Excellence. NICE real-world evidence framework. (2022). https://www.nice.org.uk/corporate/ecd9
• Provides guidance on the use of real-world evidence in health technology assessment (HTA) decision-making.
2.
Institute for Quality and Efficiency in Health Care. General methods. (2020). https://www.iqwig.de/methoden/allgemeine-methoden_v8-0.pdf
3.
Makady A, Ham RT, de Boer A et al. Policies for use of real-world data in health technology assessment (HTA): a comparative study of six HTA agencies. Value Health 20(4), 520–532 (2017).
• Describes how health technology assessment (HTA) agencies incorporate real-world data into decision-making frameworks.
4.
Westreich D, Edwards JK, Lesko CR et al. Transportability of trial results using inverse odds of sampling weights. Am. J. Epidemiol. 186(8), 1010–1014 (2017).
5.
Rothwell PM. Factors that can affect the external validity of randomised controlled trials. PLOS Clin. Trials 1(1), e9 (2006).
6.
Turner AJ, Sammon C, Latimer N et al. Transporting comparative effectiveness evidence between countries: considerations for health technology assessments. Pharmacoeconomics 42(2), 165–176 (2024).
• Highlights practical challenges of transportability in HTA across jurisdictions.
7.
Dahabreh IJ, Robertson SE, Steingrimsson JA et al. Extending inferences from a randomized trial to a new target population. Stat. Med. 39(14), 1999–2014 (2020).
•• Provides a foundational statistical framework for extending trial results to target populations.
8.
Degtiar I, Rose S. A review of generalizability and transportability. Annu. Rev. Stat. Appl. 10(1), 501–524 (2023).
•• Comprehensive and up-to-date review of transportability and generalizability methods.
9.
Drummond M, Barbieri M, Cook J et al. Transferability of economic evaluations across jurisdictions: ISPOR good research practices task force report. Value Health 12(4), 409–418 (2009).
10.
Goeree R, He J, O'Reilly D. Transferability of health technology assessments and economic evaluations: a systematic review of approaches for assessment and application. Clin. Outcomes Res. 3, 89–104 (2011).
11.
Ling AY, Montez-Rath ME, Carita P. An overview of current methods for real-world applications to generalize or transport clinical trial findings to target populations of interest. Epidemiology 34(5), 627–636 (2023).
12.
Pearl J, Bareinboim E. External validity: from do-calculus to transportability across populations. Stat. Sci. 29(4), 579–595 (2014).
•• Establishes the causal inference foundations of transportability theory.
13.
Stuart EA, Bradshaw CP, Leaf PJ. Assessing the generalizability of randomized trial results to target populations. Prev. Sci. 16(3), 475–485 (2015).
14.
Jaksa A, Arena PJ, Chan KKW et al. Transferability of real-world data across borders for regulatory and health technology assessment decision-making. Front. Med. (Lausanne) 9, 1073678 (2022).
15.
Levy NS, Arena PJ, Jemielita T et al. Use of transportability methods for real-world evidence generation: a review of current applications. J. Comp. Eff. Res. 13(11), e240064 (2024).
16.
Vuong Q, Metcalfe RK, Ling A et al. Systematic review of applied transportability and generalizability analyses: a landscape analysis. Ann. Epidemiol. 104, 61–70 (2025).
17.
Solomon SD, McMurray JJV, Vaduganathan M et al. Finerenone in heart failure with mildly reduced or preserved ejection fraction. N. Engl. J. Med. 391(16), 1475–1485 (2024).
•• Pivotal randomized trial forming the basis of the present transportability assessment.
18.
Lam CSP, Fonarow GS, Fung YM et al. Guideline-directed medical therapy treatment patterns in patients with newly diagnosed heart failure stratified by left ventricular ejection fraction in the United States. Presented at: Heart Failure Society of America. (26–29 September 2025).
19.
Lam CSP, Fonarow GS, Fung YM et al. Clinical outcomes after onset of heart failure with left ventricular ejection fraction in the US. Presented at: Heart Failure Society of America. (26–29 September 2025).
20.
Kittleson MM, Panjrath GS, Amancherla K et al. 2023 ACC expert consensus decision pathway on management of heart failure with preserved ejection fraction. J. Am. Coll. Cardiol. 81(18), 1835–1878 (2023).
21.
Cochrane. Cochrane Handbook for Systematic Reviews of Interventions. (2024). https://www.cochrane.org/authors/handbooks-and-manuals/handbook
Information & Authors
Information
Published In
Copyright
© 2026 Bayer AG, HEOR & HTA, Wuppertal, Germany. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 9 January 2026
Accepted: 31 March 2026
Published online: 6 May 2026
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Transportability of the comparative effect of finerenone for the treatment of symptomatic chronic heart failure with left ventricular ejection fraction of ≥40%: insights from the FINEARTS-HF trial. (2026) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2026-0003
Export citation
Select the citation format you wish to export for this article or chapter.