Personalized management of angina and heart failure in clinical practice in the Middle East: a narrative review
Publication: Journal of Comparative Effectiveness Research
Abstract
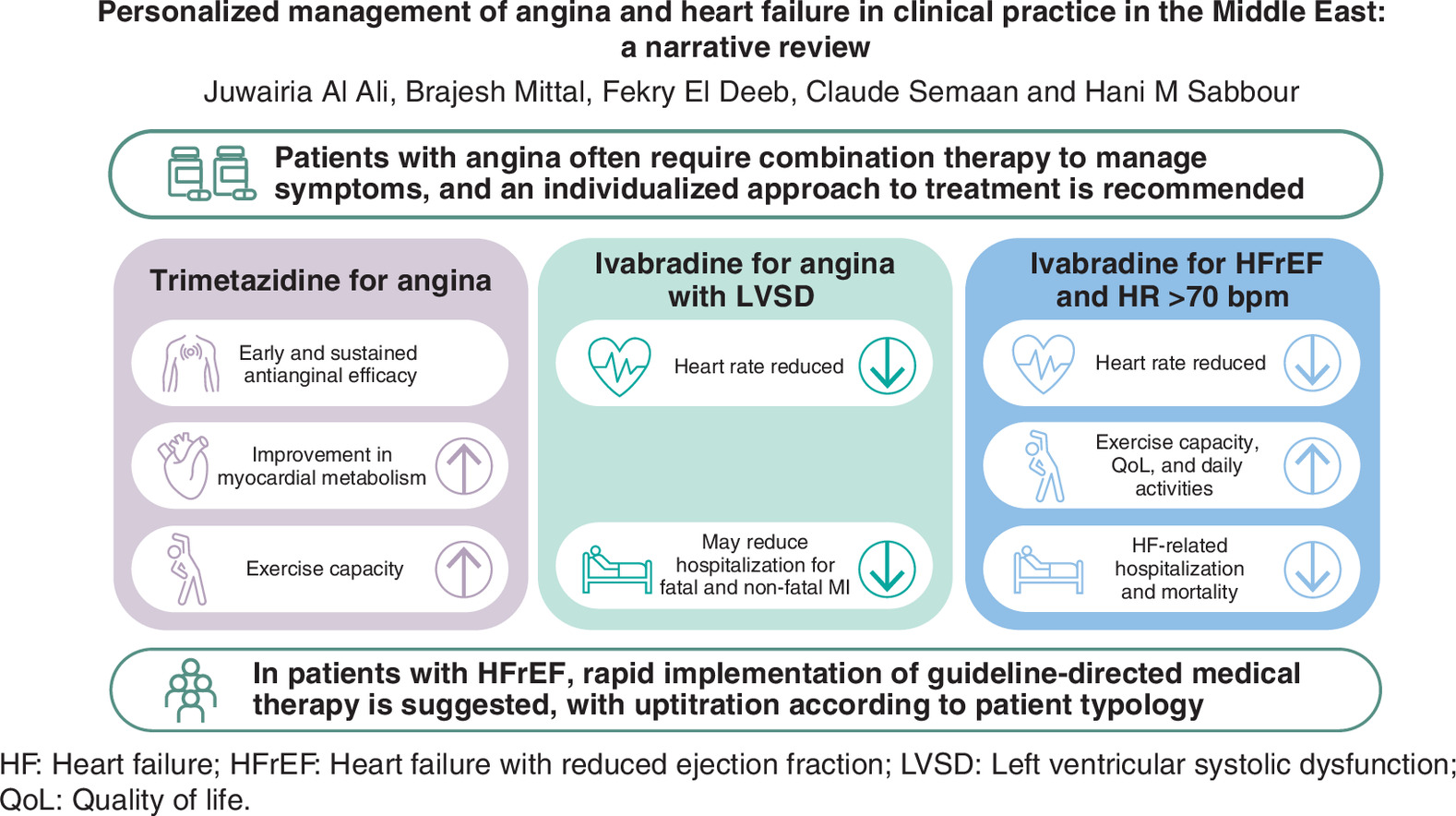
More interventions that better manage cardiovascular disease are urgently needed in the Middle East. To discuss this issue, we held a symposium at the Heart Masters Middle East 2023 congress (Dubai, UAE; May 2023) on personalized management of angina and heart failure (HF). This narrative review summarizes the content of our symposium. Many patients with chronic stable angina have ongoing symptoms and poor quality of life (QoL) despite beta-blocker + calcium-channel blocker therapy and revascularization. Further, angina is often under-recognized in clinical practice. Clinicians should consider adding newer antianginal agents (long-acting nitrates, ranolazine, trimetazidine, ivabradine) to beta-blockers + calcium-channel blockers based on patient risk factors. Individualized therapy is recommended because several mechanisms can cause angina. Agents that act at a cellular level (e.g., trimetazidine) can prevent ischemia in cardiomyocytes. Trimetazidine provides early and sustained antianginal effects, with improvements in myocardial metabolism and exercise capacity. In our view, trimetazidine may be considered as second-line therapy for angina that is suboptimally controlled on first-line therapy, and could be added to first-line therapy for angina occurring after myocardial infarction or revascularization, and comorbid with diabetes. Ivabradine reduces elevated heart rate and, when added to beta-blockers, improves angina symptoms, exercise capacity and QoL. Few patients with HF with reduced ejection fraction receive medications at target doses. Guidelines suggest rapid initiation of first-line agents from four drug classes, with a simultaneous strategy favored over a sequential one. In patients with HF with reduced ejection fraction in sinus rhythm and elevated heart rate, ivabradine should be added to maximum tolerated doses of beta-blockers. Adding ivabradine to first-line therapy improves heart rate control and QoL, and reduces HF-related hospitalization and mortality.
Plain language summary: Improving personalized care in patients with angina and/or heart failure in the Middle East
What is this article about?
This article summarizes discussions from a workshop on the treatment of cardiovascular disease (CVD) in the Middle East. Ischemic heart disease, which reduces the heart’s ability to pump blood, is a common type of CVD and often causes heart failure (HF). Chest pain (or angina) is a frequent symptom of ischemic heart disease and is caused by reduced blood flow to the heart.
What methodology is described?
A group of specialists in CVD gave presentations based on evidence from the literature and clinical experience, and provided their recommendations for improving personalized care in patients with angina and/or HF.
What was discussed?
Many patients with angina have ongoing symptoms despite standard therapy with beta-blockers and calcium-channel blockers, and procedures to restore the heart’s blood flow. However, other drugs can be added to standard therapy to improve symptoms. For example, trimetazidine improves blood flow and prevents heart muscle damage, and ivabradine reduces heart rate and improves angina symptoms when added to beta-blockers.
Why is this important?
Patients with HF should receive early treatment with multiple medications started together rather than starting one drug class after another, but many patients do not receive appropriate doses of these medications. In patients with HF and an elevated heart rate, addition of ivabradine to standard therapy improves heart rate control and reduces the need for hospitalization due to worsening HF or cardiovascular-related mortality.
Graphical abstract
Supplementary Material
File (supplementary material.docx)
- Download
- 23.90 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
World Heart Federation. Middle East & North Africa. (2024). Accessed: 28 February 2024. https://world-heart-federation.org/where-we-work/middle-east-north-africa/
2.
Bhagavathula AS, Shehab A, Ullah A, Rahmani J. The burden of cardiovascular disease risk factors in the Middle East: a systematic review and meta-analysis focusing on primary prevention. Curr. Vasc. Pharmacol. 19(4), 379–389 (2021).
3.
Motlagh B, O'Donnell M, Yusuf S. Prevalence of cardiovascular risk factors in the Middle East: a systematic review. Eur. J. Cardiovasc. Prev. Rehabil. 16(3), 268–280 (2009).
4.
Roth GA, Mensah GA, Johnson CO et al. Global burden of cardiovascular diseases and risk factors, 1990–2019: update from the GBD 2019 study. J. Am. Coll. Cardiol. 76(25), 2982–3021 (2020).
5.
Aminorroaya A, Saeedi Moghaddam S, Tavolinejad H et al. Burden of ischemic heart disease and its attributable risk factors in North Africa and the Middle East, 1990 to 2019: results from the GBD study 2019. J. Am. Heart Assoc. 13(2), e030165 (2024).
6.
Elasfar AA, Alhabeeb W, Elasfar S. Heart failure in the Middle East Arab countries: current and future perspectives. J. Saudi. Heart Assoc. 32(2), 236–241 (2020).
• Provides a summary of the current status of heart failure (HF) in Middle East Arab countries using registry data.
7.
GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 392(10159), 1789–1858 (2018).
8.
Steg PG, Greenlaw N, Tendera M et al. Prevalence of anginal symptoms and myocardial ischemia and their effect on clinical outcomes in outpatients with stable coronary artery disease: data from the International Observational CLARIFY Registry. JAMA Intern. Med. 174(10), 1651–1659 (2014).
9.
Sulaiman K, Panduranga P, Al-Zakwani I et al. Clinical characteristics, management, and outcomes of acute heart failure patients: observations from the Gulf acute heart failure registry (Gulf CARE). Eur. J. Heart Fail. 17(4), 374–384 (2015).
10.
Alhabib KF, Gamra H, Almahmeed W et al. Acute myocardial infarction and acute heart failure in the Middle East and North Africa: study design and pilot phase study results from the PEACE MENA registry. PLoS One 15(7), e0236292 (2020).
11.
Zarif B, Cavusoglu Y, Al Badarin F et al. Clinical characteristics and treatment patterns in patients with heart failure: results from the iCaReMe Middle East and Africa cohort [AHA Scientific Sessions abstract 14017]. Circulation 148(Suppl. 1), A14017 (2023).
12.
Manla Y, Almahmeed W. The pandemic of coronary heart disease in the Middle East and North Africa: what clinicians need to know. Curr. Atheroscler. Rep. 25(9), 543–557 (2023).
13.
Skouri HN, Çavuşoğlu Y, Bennis A et al. Expert recommendations to bridge gaps in heart failure patient support in the Middle East and Africa Region. Anatol. J. Cardiol. 28(1), 2–18 (2024).
14.
Montalescot G, Sechtem U, Achenbach S et al. 2013 ESC guidelines on the management of stable coronary artery disease: the Task Force on the management of stable coronary artery disease of the European Society of Cardiology. Eur. Heart J. 34(38), 2949–3003 (2013).
15.
Spertus JA, Dawson J, Masoudi FA et al. Prevalence and predictors of angina pectoris one month after myocardial infarction. Am. J. Cardiol. 98(3), 282–288 (2006).
16.
Ellis SG, Kereiakes DJ, Metzger DC et al. Everolimus-eluting bioresorbable scaffolds for coronary artery disease. N. Engl. J. Med. 373(20), 1905–1915 (2015).
17.
Stone GW, Ellis SG, Gori T et al. Blinded outcomes and angina assessment of coronary bioresorbable scaffolds: 30-day and 1-year results from the ABSORB IV randomised trial. Lancet 392(10157), 1530–1540 (2018).
18.
Crea F, Bairey Merz CN, Beltrame JF et al. Mechanisms and diagnostic evaluation of persistent or recurrent angina following percutaneous coronary revascularization. Eur. Heart J. 40(29), 2455–2462 (2019).
19.
Crea F, Camici PG, Bairey Merz CN. Coronary microvascular dysfunction: an update. Eur. Heart J. 35(17), 1101–1111 (2014).
20.
Ashokprabhu ND, Quesada O, Alvarez YR, Henry TD. INOCA/ANOCA: mechanisms and novel treatments. Am. Heart J. Plus. 30, 100302 (2023).
21.
Parlati ALM, Nardi E, Sucato V et al. ANOCA, INOCA, MINOCA: the new frontier of coronary syndromes. J. Cardiovasc. Dev. Dis. 12(2), 64 (2025).
22.
Vrints C, Andreotti F, Koskinas KC et al. 2024 ESC guidelines for the management of chronic coronary syndromes. Eur. Heart J. 45(36), 3415–3537 (2024).
23.
Pepine CJ, Douglas PS. Rethinking stable ischemic heart disease: is this the beginning of a new era? J. Am. Coll. Cardiol. 60(11), 957–959 (2012).
24.
Kunadian V, Chieffo A, Camici PG et al. An EAPCI expert consensus document on ischaemia with non-obstructive coronary arteries in collaboration with European Society of Cardiology Working Group on coronary pathophysiology & microcirculation endorsed by Coronary Vasomotor Disorders International Study Group. Eur. Heart J. 41(37), 3504–3520 (2020).
25.
Ferrari R, Camici PG, Crea F et al. Expert consensus document: a ‘diamond’ approach to personalized treatment of angina. Nat. Rev. Cardiol. 15(2), 120–132 (2018).
26.
Moran AE, Forouzanfar MH, Roth GA et al. The global burden of ischemic heart disease in 1990 and 2010: the Global Burden of Disease 2010 study. Circulation 129(14), 1493–1501 (2014).
27.
Hlatky MA, Boothroyd DB, Melsop KA et al. Medical costs and quality of life 10 to 12 years after randomization to angioplasty or bypass surgery for multivessel coronary artery disease. Circulation 110(14), 1960–1966 (2004).
28.
Beltrame JF, Weekes AJ, Morgan C, Tavella R, Spertus JA. The prevalence of weekly angina among patients with chronic stable angina in primary care practices: The Coronary Artery Disease in General Practice (CADENCE) Study. Arch. Intern. Med. 169(16), 1491–1499 (2009).
29.
Ben-Yehuda O, Kazi DS, Bonafede M et al. Angina and associated healthcare costs following percutaneous coronary intervention: a real-world analysis from a multi-payer database. Catheter Cardiovasc. Interv. 88(7), 1017–1024 (2016).
30.
Qintar M, Spertus JA, Gosch KL et al. Effect of angina under-recognition on treatment in outpatients with stable ischaemic heart disease. Eur. Heart J. Qual. Care Clin. Outcomes 2(3), 208–214 (2016).
31.
Kop WJ, Verdino RJ, Gottdiener JS, O'Leary ST, Bairey Merz CN, Krantz DS. Changes in heart rate and heart rate variability before ambulatory ischemic events. J. Am. Coll. Cardiol. 38(3), 742–749 (2001).
32.
Fox KM, Ferrari R. Heart rate: a forgotten link in coronary artery disease? Nat. Rev. Cardiol. 8(7), 369–379 (2011).
33.
Marzilli M, Merz CN, Boden WE et al. Obstructive coronary atherosclerosis and ischemic heart disease: an elusive link! J. Am. Coll. Cardiol. 60(11), 951–956 (2012).
34.
Fillmore N, Mori J, Lopaschuk GD. Mitochondrial fatty acid oxidation alterations in heart failure, ischaemic heart disease and diabetic cardiomyopathy. Br. J. Pharmacol. 171(8), 2080–2090 (2014).
35.
Fragasso G, Perseghin G, De Cobelli F et al. Effects of metabolic modulation by trimetazidine on left ventricular function and phosphocreatine/adenosine triphosphate ratio in patients with heart failure. Eur. Heart J. 27(8), 942–948 (2006).
36.
Guarini G, Huqi A, Morrone D, Capozza PFG, Marzilli M. Trimetazidine and other metabolic modifiers. Eur. Cardiol. 13(2), 104–111 (2018).
37.
Glezer M. Real-world evidence for the antianginal efficacy of trimetazidine from the Russian observational CHOICE-2 study. Adv. Ther. 34(4), 915–924 (2017).
38.
Coppola S, Froio S, Chiumello D. β-blockers in critically ill patients: from physiology to clinical evidence. Crit. Care 19(1), 119 (2015).
39.
El-Kady T, El-Sabban K, Gabaly M, Sabry A, Abdel-Hady S. Effects of trimetazidine on myocardial perfusion and the contractile response of chronically dysfunctional myocardium in ischemic cardiomyopathy: a 24-month study. Am. J. Cardiovasc. Drugs 5(4), 271–278 (2005).
•• Pivotal randomized study showing long-term benefits of trimetazidine in patients with coronary artery disease.
40.
Rodríguez Padial L, Maicas Bellido C, Velázquez Martín M, Gil Polo B. A prospective study on trimetazidine effectiveness and tolerability in diabetic patients in association to the previous treatment of their coronary disease. DIETRIC study [in Spanish]. Rev. Clin. Esp. 205(2), 57–62 (2005).
41.
Michaelides AP, Spiropoulos K, Dimopoulos K, Athanasiades D, Toutouzas P. Antianginal efficacy of the combination of trimetazidine-propranolol compared with isosorbide dinitrate-propranolol in patients with stable angina. Clin. Drug Invest. 13(1), 8–14 (1997).
• Early study demonstrating antianginal efficacy of trimetazidine.
42.
Hu B, Li W, Xu T, Chen T, Guo J. Evaluation of trimetazidine in angina pectoris by echocardiography and radionuclide angiography: a meta-analysis of randomized, controlled trials. Clin. Cardiol. 34(6), 395–400 (2011).
•• Meta-analysis of randomized controlled trial that indicates antianginal effects of trimetazidine.
43.
Glezer M. The effectiveness of trimetazidine treatment in patients with stable angina pectoris of various durations: results from the CHOICE-2 study. Adv. Ther. 35(7), 1103–1113 (2018).
44.
Glezer MG, Vygodin VA. ODA investigators. Effectiveness of trimetazidine in patients with stable angina pectoris of various durations: results from ODA. Cardiol. Ther. 9(2), 395–408 (2020).
45.
Ferrari R, Fox K. Heart rate reduction in coronary artery disease and heart failure. Nat. Rev. Cardiol. 13(8), 493–501 (2016).
46.
DiFrancesco D, Camm JA. Heart rate lowering by specific and selective If current inhibition with ivabradine: a new therapeutic perspective in cardiovascular disease. Drugs 64(16), 1757–1765 (2004).
47.
Skalidis EI, Hamilos MI, Chlouverakis G, Zacharis EA, Vardas PE. Ivabradine improves coronary flow reserve in patients with stable coronary artery disease. Atherosclerosis 215(1), 160–165 (2011).
48.
Dillinger JG, Maher V, Vitale C et al. Impact of ivabradine on central aortic blood pressure and myocardial perfusion in patients with stable coronary artery disease. Hypertension 66(6), 1138–1144 (2015).
49.
Glezer M, Vasyuk Y, Karpov Y. Efficacy of ivabradine in combination with beta-blockers versus uptitration of beta-blockers in patients with stable angina (CONTROL-2 study). Adv. Ther. 35(3), 341–352 (2018).
50.
Tendera M, Borer JS, Tardif JC. Efficacy of If inhibition with ivabradine in different subpopulations with stable angina pectoris. Cardiology 114(2), 116–125 (2009).
51.
Tardif JC, Ponikowski P, Kahan T. Efficacy of the If current inhibitor ivabradine in patients with chronic stable angina receiving beta-blocker therapy: a 4-month, randomized, placebo-controlled trial. Eur. Heart J. 30(5), 540–548 (2009).
52.
Amosova E, Andrejev E, Zaderey I, Rudenko U, Ceconi C, Ferrari R. Efficacy of ivabradine in combination with beta-blocker versus uptitration of beta-blocker in patients with stable angina. Cardiovasc. Drugs Ther. 25(6), 531–537 (2011).
53.
Fox K, Ford I, Steg PG, Tendera M, Robertson M, Ferrari R. Relationship between ivabradine treatment and cardiovascular outcomes in patients with stable coronary artery disease and left ventricular systolic dysfunction with limiting angina: a subgroup analysis of the randomized, controlled BEAUTIFUL trial. Eur. Heart J. 30(19), 2337–2345 (2009).
54.
Werdan K, Perings S, Köster R et al. Effectiveness of ivabradine treatment in different subpopulations with stable angina in clinical practice: a pooled analysis of observational studies. Cardiology 135(3), 141–150 (2016).
55.
AlShammeri O, Al Saif S, Al Shehri H et al. Saudi Heart Association guidelines on best practices in the management of chronic coronary syndromes. J. Saudi. Heart Assoc. 34(3), 182–211 (2022).
•• Current guidelines for the management of chronic coronary syndrome in Saudi Arabia.
56.
Belsey J, Savelieva I, Mugelli A, Camm AJ. Relative efficacy of antianginal drugs used as add-on therapy in patients with stable angina: a systematic review and meta-analysis. Eur. J. Prev. Cardiol. 22(7), 837–848 (2015).
57.
Manolis AJ, Boden WE, Collins P et al. State of the art approach to managing angina and ischemia: tailoring treatment to the evidence. Eur. J. Intern. Med. 92, 40–47 (2021).
58.
Greene SJ, Butler J, Albert NM et al. Medical therapy for heart failure with reduced ejection fraction: the CHAMP-HF registry. J. Am. Coll. Cardiol. 72(4), 351–366 (2018).
59.
Greene SJ, Fonarow GC, DeVore AD et al. Titration of medical therapy for heart failure with reduced ejection fraction. J. Am. Coll. Cardiol. 73(19), 2365–2383 (2019).
60.
Jarjour M, Henri C, de Denus S et al. Care gaps in adherence to heart failure guidelines: clinical inertia or physiological limitations? JACC Heart Fail. 8(9), 725–738 (2020).
61.
Fonarow GC, Albert NM, Curtis AB et al. Incremental reduction in risk of death associated with use of guideline-recommended therapies in patients with heart failure: a nested case-control analysis of IMPROVE HF. J. Am. Heart Assoc. 1(1), 16–26 (2012).
62.
Vaduganathan M, Claggett BL, Jhund PS et al. Estimating lifetime benefits of comprehensive disease-modifying pharmacological therapies in patients with heart failure with reduced ejection fraction: a comparative analysis of three randomised controlled trials. Lancet 396(10244), 121–128 (2020).
63.
Allen LA, Teerlink JR, Gottlieb SS, Ahmad T, Lam CSP, Psotka MA. Heart failure spending function: an investment framework for sequencing and intensification of guideline-directed medical therapies. Circ. Heart Fail. 15(4), e008594 (2022).
64.
Lam CSP, Butler J. Victims of success in failure. Circulation 142(12), 1129–1131 (2020).
65.
Sharma A, Verma S, Bhatt DL et al. Optimizing foundational therapies in patients with HFrEF. How do we translate these findings into clinical care? JACC Basic Transl. Sci. 7(5), 504–517 (2022).
66.
Greene SJ, Butler J, Metra M. Another reason to embrace quadruple medical therapy for heart failure: medications enabling tolerance of each other. Eur. J. Heart Fail. 23(9), 1525–1528 (2021).
67.
Böhm M, Swedberg K, Komajda M et al. Heart rate as a risk factor in chronic heart failure (SHIFT): the association between heart rate and outcomes in a randomised placebo-controlled trial. Lancet 376(9744), 886–894 (2010).
68.
Docherty KF, Shen L, Castagno D et al. Relationship between heart rate and outcomes in patients in sinus rhythm or atrial fibrillation with heart failure and reduced ejection fraction. Eur. J. Heart Fail. 22(3), 528–538 (2020).
69.
McAlister FA, Wiebe N, Ezekowitz JA, Leung AA, Armstrong PW. Meta-analysis: beta-blocker dose, heart rate reduction, and death in patients with heart failure. Ann. Intern. Med. 150(11), 784–794 (2009).
70.
Swedberg K, Komajda M, Böhm M et al. Ivabradine and outcomes in chronic heart failure (SHIFT): a randomised placebo-controlled study. Lancet 376(9744), 875–885 (2010).
•• Pivotal randomized placebo-controlled trial demonstrating the benefits of ivabradine in patients with chronic HF.
71.
Böhm M, Borer J, Ford I et al. Heart rate at baseline influences the effect of ivabradine on cardiovascular outcomes in chronic heart failure: analysis from the SHIFT study. Clin. Res. Cardiol. 102(1), 11–22 (2013).
72.
Komajda M, Böhm M, Borer JS et al. Efficacy and safety of ivabradine in patients with chronic systolic heart failure according to blood pressure level in SHIFT. Eur. J. Heart Fail. 16(7), 810–816 (2014).
73.
Voors AA, van Veldhuisen DJ, Robertson M et al. The effect of heart rate reduction with ivabradine on renal function in patients with chronic heart failure: an analysis from SHIFT. Eur. J. Heart Fail. 16(4), 426–434 (2014).
74.
Komajda M, Tavazzi L, Swedberg K et al. Chronic exposure to ivabradine reduces readmissions in the vulnerable phase after hospitalization for worsening systolic heart failure: a post-hoc analysis of SHIFT. Eur. J. Heart Fail. 18(9), 1182–1189 (2016).
75.
Swedberg K, Komajda M, Böhm M et al. Effects on outcomes of heart rate reduction by ivabradine in patients with congestive heart failure: is there an influence of beta-blocker dose? Findings from the SHIFT (Systolic Heart failure treatment with the If inhibitor ivabradine Trial) study. J. Am. Coll. Cardiol. 59(22), 1938–1945 (2012).
76.
Tardif JC, O'Meara E, Komajda M et al. Effects of selective heart rate reduction with ivabradine on left ventricular remodelling and function: results from the SHIFT echocardiography substudy. Eur. Heart J. 32(20), 2507–2515 (2011).
77.
Faragli A, Tano GD, Carlini C et al. In-hospital heart rate reduction with beta blockers and ivabradine early after recovery in patients with acute decompensated heart failure reduces short-term mortality and rehospitalization. Front. Cardiovasc. Med. 8, 665202 (2021).
78.
Lee YH, Lin PL, Chiou WR et al. Combination of ivabradine and sacubitril/valsartan in patients with heart failure and reduced ejection fraction. ESC Heart Fail. 8(2), 1204–1215 (2021).
79.
Ponikowski P, Voors AA, Anker SD et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 37(27), 2129–2200 (2016).
80.
McDonagh TA, Metra M, Adamo M et al. 2021 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure. Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). With the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. J. Heart Fail. 24(1), 4–131 (2022).
81.
Al Habeeb W, Tash A, Elasfar A et al. 2023 National Heart Center/Saudi Heart Association focused update of the 2019 Saudi Heart Association guidelines for the management of heart failure. J. Saudi. Heart Assoc. 35(1), 71–134 (2023).
•• Current guidelines for the management of HF in Saudi Arabia.
82.
Heidenreich PA, Bozkurt B, Aguilar D et al. 2022 AHA/ACC/HFSA guideline for the management of heart failure: executive summary. A report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 79(17), 1757–1780 (2022).
83.
McDonald M, Virani S, Chan M et al. CCS/CHFS heart failure guidelines update: defining a new pharmacologic standard of care for heart failure with reduced ejection fraction. Can. J. Cardiol. 37(4), 531–546 (2021).
84.
Bakhsh A, Jelaidan I, Chaudhary AG et al. A case-based implementation of heart failure therapies, a consensus pathway by the Saudi Heart Failure Working Group. J. Saudi. Heart Assoc. 36(2), 79–90 (2024).
•• A recent consensus statement on the management of HF from the Saudi Heart Failure group.
85.
Rosano GMC, Moura B, Metra M et al. Patient profiling in heart failure for tailoring medical therapy. A consensus document of the Heart Failure Association of the European Society of Cardiology. Eur. J. Heart Fail. 23(6), 872–881 (2021).
86.
Komajda M. Prognostic and symptomatic benefits with ivabradine: lessons from the SHIFT trial. Eur. Heart J. Suppl. 17(Suppl_G), G30–G36 (2015).
Information & Authors
Information
Published In
Copyright
© 2026 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 25 July 2025
Accepted: 11 February 2026
Published online: 12 March 2026
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Personalized management of angina and heart failure in clinical practice in the Middle East: a narrative review. (2026) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2025-0119
Export citation
Select the citation format you wish to export for this article or chapter.