Hospital readmission among patients with unruptured intracranial aneurysms undergoing stent-assisted endovascular coiling using the ENTERPRISE® 2 stent versus Neuroform® Atlas stent
Publication: Journal of Comparative Effectiveness Research
Abstract
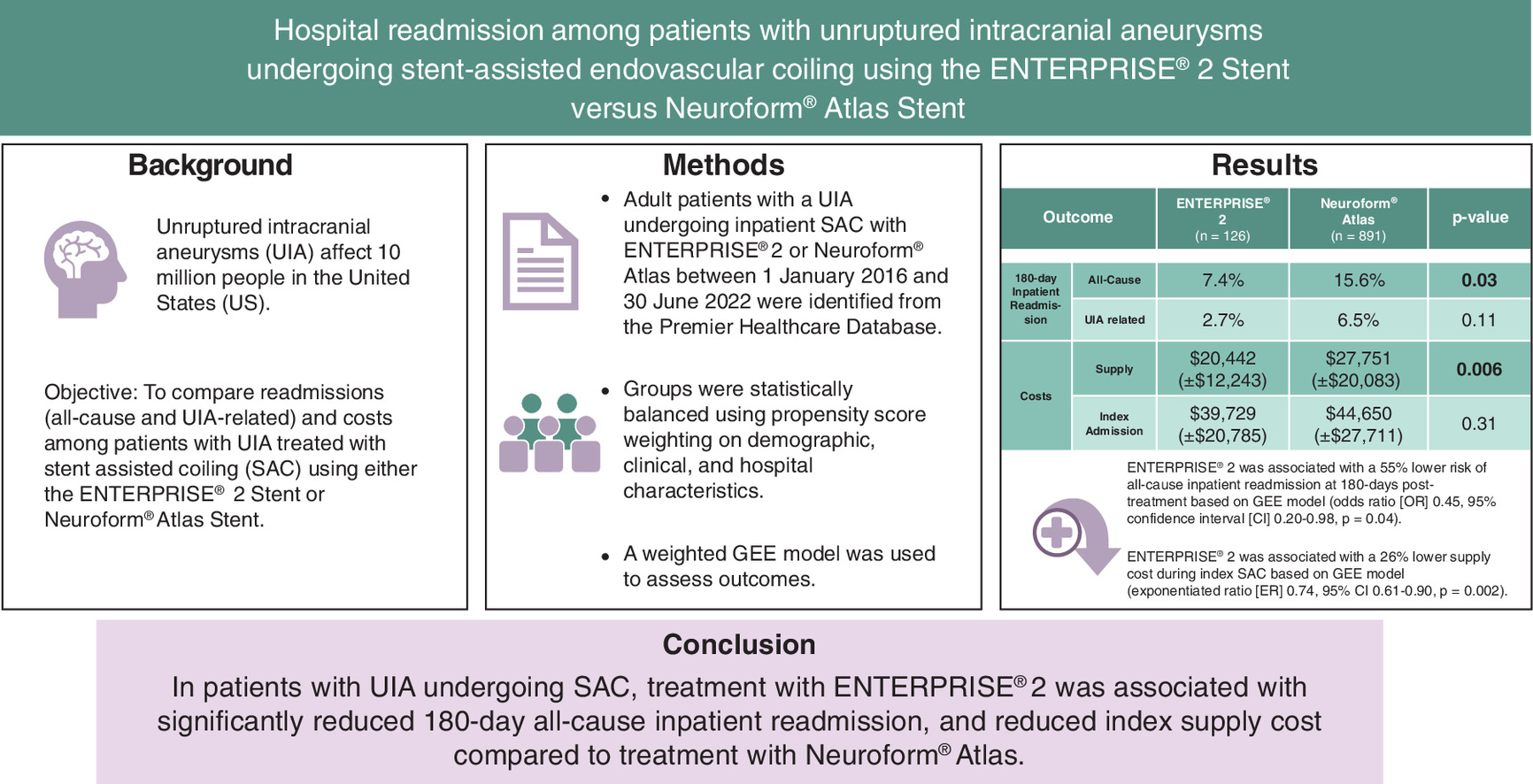
Aim: Stent-assisted endovascular coiling is a safe and effective treatment for unruptured intracranial aneurysms (UIAs). This study compared 180-day inpatient readmission and cost among patients with UIA who underwent stent-assisted coiling (SAC) using the ENTERPRISE® 2 or Neuroform® Atlas stent. Materials & methods: In this retrospective cohort study, adults with UIA undergoing SAC were identified in the Premier Healthcare Database (2016–2022) and grouped based on the stent used: ENTERPRISE 2 or Neuroform Atlas. Outcomes included all-cause and UIA-related inpatient readmission in the 180 days following treatment, index admission and supply cost. Inverse probability of treatment weighting of propensity score method balanced the two cohorts on study covariates. A weighted generalized estimating equation model assessed study outcomes. Results: A total of 1017 patients were included (ENTERPRISE 2, n = 126; Neuroform Atlas, n = 891). Hospital and patient characteristics except race were well-balanced after weighting. Patients treated with ENTERPRISE 2 versus Neuroform Atlas were 55% less likely to have an all-cause inpatient readmission in the 180-day follow-up period (odds ratio 0.45, 95% CI: 0.20–0.98, p = 0.04). Further, the ENTERPRISE 2 cohort had significantly lower index supply cost ($20,442 vs $27,561, exponentiated ratio 0.74, 95% CI: 0.61–0.90, p = 0.002) compared with the Neuroform Atlas cohort. No significant differences were observed in UIA-related inpatient readmission or total index admission cost between cohorts. Conclusion: Among patients with UIA undergoing SAC, the use of ENTERPRISE 2 stent was associated with a significantly reduced risk of all-cause inpatient hospital readmission and significantly lower index supply cost compared with the Neuroform Atlas stent.
Plain language summary
What is this article about?
Unruptured intracranial aneurysms (UIAs) affect about 3% of the population. Stent-assisted endovascular coiling is a common treatment modality for UIA. This study compared readmissions and costs among UIA patients undergoing stent-assisted endovascular coiling using the ENTERPRISE® 2 stent versus Neuroform® Atlas stent.
What were the results?
Patients treated with ENTERPRISE 2 stent had a significantly lower risk of all-cause inpatient hospital readmission and lower cost of supplies during admission for coiling procedure compared with those treated with Neuroform Atlas stent. There were no differences in UIA related inpatient readmission or total admission cost between the two groups.
What do the results mean?
The use of ENTERPRISE 2 stent (vs Neuroform Atlas stent) was associated with lower costs and hospital readmission rates following stent-assisted endovascular coiling for UIA.
Graphical abstract
Supplementary Material
File (supplementary figure.docx)
- Download
- 37.30 KB
References
Papers of special note have been highlighted as: • of interest
1.
Korja M, Lehto H, Juvela S. Lifelong rupture risk of intracranial aneurysms depends on risk factors: a prospective Finnish cohort study. Stroke 45(7), 1958–1963 (2014).
2.
Wiebers DO, Whisnant JP, Huston J et al. Unruptured intracranial aneurysms: natural history, clinical outcome, and risks of surgical and endovascular treatment. Lancet 362(9378), 103–110 (2003).
3.
Brown RD. Unruptured intracranial aneurysms. Semin. Neurol. 30(5), 537–544 (2010).
4.
Nieuwkamp DJ, Setz LE, Algra A, Linn FH, de Rooij NK, Rinkel GJ. Changes in case fatality of aneurysmal subarachnoid haemorrhage over time, according to age, sex, and region: a meta-analysis. Lancet Neurol. 8(7), 635–642 (2009).
5.
Vlak MH, Algra A, Brandenburg R, Rinkel GJ. Prevalence of unruptured intracranial aneurysms, with emphasis on sex, age, comorbidity, country, and time period: a systematic review and meta-analysis. Lancet Neurol. 10(7), 626–636 (2011).
6.
Smith GA, Dagostino P, Maltenfort MG, Dumont AS, Ratliff JK. Geographic variation and regional trends in adoption of endovascular techniques for cerebral aneurysms. J. Neurosurg. 114(6), 1768–1777 (2011).
7.
Hwang JS, Hyun MK, Lee HJ et al. Endovascular coiling versus neurosurgical clipping in patients with unruptured intracranial aneurysm: a systematic review. BMC Neurol. 12, 99 (2012).
8.
Brinjikji W, Rabinstein AA, Lanzino G, Kallmes DF, Cloft HJ. Patient outcomes are better for unruptured cerebral aneurysms treated at centers that preferentially treat with endovascular coiling: a study of the national inpatient sample 2001–2007. Am. J. Neuroradiol. 32(6), 1065–1070 (2011).
9.
Li L, Xu GQ, Gao HL et al. Endovascular treatment of intracranial vertebral artery unruptured dissecting aneurysms: comparison of flow diversion and stent-assisted coiling or stenting alone. Front. Neurol. 13, 919866 (2022).
10.
Lo YL, Bih ZL, Yu YH, Li MC, Chen HM, Wu SY. Long-term medical resource consumption between surgical clipping and endovascular coiling for aneurysmal subarachnoid hemorrhage: a propensity score–matched, nationwide, population-based cohort study. Int. J. Environ. Res. Public Health 18(11), 5989 (2021).
11.
el-Chalouhi N, Jabbour PM, Tjoumakaris SI et al. Treatment of large and giant intracranial aneurysms: cost comparison of flow diversion and traditional embolization strategies. World Neurosurg. 82(5), 696–701 (2014).
12.
Bairstow P, Dodgson A, Linto J, Khangure M. Comparison of cost and outcome of endovascular and neurosurgical procedures in the treatment of ruptured intracranial aneurysms. Australas. Radiol. 46(3), 249–251 (2002).
13.
Maud A, Lakshminarayan K, Suri MF, Vazquez G, Lanzino G, Qureshi AI. Cost-effectiveness analysis of endovascular versus neurosurgical treatment for ruptured intracranial aneurysms in the United States. J. Neurosurg. 110(5), 880–886 (2009).
14.
Armoiry X, Turjman F, Hartmann D et al. Endovascular treatment of intracranial aneurysms with the WEB device: a systematic review of clinical outcomes. Am. J. Neuroradiol. 37(5), 868–872 (2016).
15.
Hendricks BK, Yoon JS, Yaeger K et al. Wide-neck aneurysms: systematic review of the neurosurgical literature with a focus on definition and clinical implications. J. Neurosurg. 133(1), 159–165 (2019).
16.
Park HS, Kwon SC, Park ES, Park JB, Kim MS. A new definition for wide-necked cerebral aneurysms. J. Cerebrovasc. Endovasc. Neurosurg. 21(4), 193–198 (2019).
17.
Kadkhodayan Y, Rhodes N, Blackburn S, Derdeyn CP, Cross DT, Moran CJ. Comparison of Enterprise with Neuroform stent-assisted coiling of intracranial aneurysms. Am. J. Roentgenol. 200(4), 872–878 (2013).
• This study highlights that ENTERPRISE® stent use was associated with statistically significant superior deployment rate and occlusion rate as compared with Neuroform® stent.
18.
Hwang S-K, Hwang G, Bang JS, Oh CW, Kwon OK. Endovascular Enterprise stent-assisted coil embolization for wide-necked unruptured intracranial aneurysms. J. Clin. Neurosci. 20(9), 1276–1279 (2013).
19.
Leacy R, Kottenmeier E, Lee SH, Khanna R, Spiotta AM. Endovascular treatment with the Enterprise stent versus the Neuroform or low-profile visualized intraluminal support stent for unruptured aneurysms. J. Comp. Eff. Res. 10(4), 295–305 (2021).
• This retrospective cohort study suggests that ENTERPRISE stent use was associated with significantly lower risk of readmissions versus other stent including Neuroform stent.
20.
Wang J, Vargas J, Spiotta A et al. Stent-assisted coiling of cerebral aneurysms: a single-center clinical and angiographic analysis. J. Neurointerv. Surg. 10(7), 687–692 (2018).
21.
Gentric JC, Biondi A, Piotin M et al. Safety and efficacy of neuroform for treatment of intracranial aneurysms: a prospective, consecutive, French multicentric study. Am. J. Neuroradiol. 34(6), 1203–1208 (2013).
22.
Dong L, Wang J, Chen X et al. Stent-assisted coiling using the Neuroform Atlas stent for treatment of aneurysms that recur after coil embolization. Front. Neurol. 13, 967942 (2022).
23.
Caragliano AA, Papa R, Pitrone A et al. The low-profile Neuroform Atlas stent in the treatment of wide-necked intracranial aneurysms – immediate and midterm results: an Italian multicenter registry. J. Neuroradiol. 47(6), 421–427 (2020).
24.
King B, Vaziri S, Singla A, Fargen KM, Mocco J. Clinical and angiographic outcomes after stent-assisted coiling of cerebral aneurysms with Enterprise and Neuroform stents: a comparative analysis of the literature. J. Neurointerv. Surg. 7(12), 905–909 (2015).
• This literature review demonstrates that ENTERPRISE use is associated with lower rates of hardware failure at deployment, peri-procedural intracranial hemorrhage and recanalization and higher rates of complete occlusion as compared to Neuroform stent.
25.
Kono K, Terada T. In vitro experiments of vessel wall apposition between the Enterprise and Enterprise 2 stents for treatment of cerebral aneurysms. Acta Neurochir. (Wien) 158(2), 241–245 (2016).
26.
Chihara H, Ishii A, Kikuchi T, Ikeda H, Arai D, Miyamoto S. Deployment technique that takes advantage of the characteristics of Enterprise VRD2: an in vitro study. J. Neurointerv. Surg. 9(10), 969–973 (2017).
27.
Li Z, Xuan J, Fang X et al. Comparison of Enterprise stent 2 with 1 in assisting coiling of ruptured aneurysms: a real-world study. J. Comp. Eff. Res. 11(12), 879–887 (2022).
28.
Jankowitz BT, Hanel R, Jadhav AP et al. Neuroform Atlas Stent System for the treatment of intracranial aneurysm: primary results of the Atlas Humanitarian Device Exemption cohort. J. Neurointerv. Surg. 11(8), 801–806 (2019).
29.
Daou BJ, Palmateer G, Linzey JR et al. Stent-assisted coiling of cerebral aneurysms: head to head comparison between the Neuroform Atlas and EZ stents. Interv. Neuroradiol. 27(3), 353–361 (2021).
30.
Austin PC, Stuart EA. Moving towards best practice when using inverse probability of treatment weighting (IPTW) using the propensity score to estimate causal treatment effects in observational studies. Stat. Med. 34(28), 3661–3679 (2015).
31.
Iwakami T, Fujii N, Son J. Comparison of the physical characteristics of support stents for cerebral aneurysm embolization. J. Neuroendovasc. Ther. 15(12), 778–786 (2021).
32.
Kato N, Yuki I, Otani K et al. Flow Diverter apposition in patients with large or giant intracranial aneurysms evaluated on three-dimensional fusion images acquired by high-resolution cone-beam computed tomography and digital subtraction angiography. World Neurosurg. 147, e388–e395 (2021).
33.
Heller R, Calnan DR, Lanfranchi M, Madan N, Malek AM. Incomplete stent apposition in Enterprise stent-mediated coiling of aneurysms: persistence over time and risk of delayed ischemic events. J. Neurosurg. 118(5), 1014–1022 (2013).
Information & Authors
Information
Published In
Copyright
© 2025 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 13 June 2025
Accepted: 18 July 2025
Published online: 1 August 2025
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Hospital readmission among patients with unruptured intracranial aneurysms undergoing stent-assisted endovascular coiling using the ENTERPRISE® 2 stent versus Neuroform® Atlas stent. (2025) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2025-0096
Export citation
Select the citation format you wish to export for this article or chapter.