Comparative safety of B/F/TAF versus other antiretroviral therapy regimens for treatment-experienced people with HIV-1: a systematic literature review and network meta-analysis
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: With modern antiretroviral therapy (ART), HIV-1 has now become a manageable chronic condition. Among treatment-experienced (TE) people with HIV-1 (PWH), ART regimens can influence metabolic and renal outcomes and adverse events such as nausea. Regimen selection increasingly prioritizes safety, tolerability and long-term acceptability. This study compared bictegravir/emtricitabine/tenofovir alafenamide (B/F/TAF) with other ART regimens in TE PWH using multilevel network meta-regression (ML-NMR), focusing on lipid profile, renal function and overall safety. Materials & methods: A systematic literature review (SLR) in June 2023 identified Phase III/IV randomized controlled trials reporting safety in adult TE PWH. ML-NMR was conducted at week 48 adjusting for age, sex, race and CD4 cell count, using individual patient data from three Phase III B/F/TAF trials (GS-US-380-1844, -1878, -4030) and aggregate data from comparator trials. Results: At week 48, B/F/TAF demonstrated similar changes in total cholesterol (TC) to HDL ratio and LDL versus comparators. Compared with NNRTI (+ or /) F/TDF, changes in TC favored B/F/TAF (mean difference [MD; 95% CrI]: -12.43 [-23.26, -1.53]), but favored the NNRTI-based regimen for HDL (-4.35 [-7.76, -0.70]). Triglycerides changes favored B/F/TAF versus DTG/ABC/3TC (-15.01 [-29.18, -1.06]) and protease inhibitor (+ or /) b + 2 NRTIs (-24.48 [-41.60, -7.47]). eGFR changes favored B/F/TAF versus DTG/ABC/3TC (3.81 [1.74, 5.97]). With some exceptions of statistical differences in both directions, B/F/TAF generally had similar levels of adverse events and discontinuations as other ART. Conclusion: Switching to or remaining on B/F/TAF in TE PWH was generally well tolerated and did not worsen lipid, renal or safety outcomes versus most other contemporary ART. Improvements in select lipid parameters and stable renal function, with low rates of adverse events and discontinuation, support B/F/TAF as a safe option for long-term management in TE PWH.
Plain language summary: Comparative safety of B/F/TAF in people with HIV-1 who have previously received treatment
What is this article about?
B/F/TAF is a single-tablet treatment for HIV-1 which combines three medications: bictegravir (B), emtricitabine (F) and tenofovir alafenamide (TAF). This medication is used by people living with HIV-1, including those who have been on other treatments before.
This article examines whether B/F/TAF is as safe as other HIV-1 medications for people who have already been treated for HIV-1, looking specifically at effects on cholesterol, kidney health and side effects.
Why is this important?
With modern treatments, people with HIV-1 can live long, healthy lives. For those who have been on HIV-1 medication before, it is essential to ensure that any treatment remains safe over time and does not cause other health problems.
What methods were used in the research?
Researchers reviewed clinical trials of HIV-1 medications and compared them to assess cholesterol changes, kidney function and side effects in people who had received prior HIV-1 treatment.
What were the results?
B/F/TAF performed well compared with other HIV-1 medications. People taking B/F/TAF experienced favorable outcomes for certain cholesterol measurements and maintained stable kidney function. Additionally, B/F/TAF was associated with lower rates of nausea and fewer treatment-related side effects than some other options.
What do the results mean?
For people who have been on HIV-1 medications before, B/F/TAF appears to be a well-tolerated choice that maintains good safety outcomes. The findings support B/F/TAF as an appropriate long-term treatment option.
Modern antiretroviral therapy (ART) has transformed HIV from an infection with high mortality to a manageable chronic condition. Guideline-recommended initiation and strict adherence to ART regimens can suppress viral replication, preserve immune function and extend life expectancy to near-normal levels, narrowing the gap with the general population in the contemporary ART era [1,2]. This success has led to a large and growing population of people with HIV (PWH) on long-term therapy. Consequently, the majority of PWH are now considered treatment-experienced (TE), mostly consisting of individuals who are virologically suppressed (VS), reflecting the long-term effectiveness of their therapy. As of 2023, an estimated 77% of PWH globally were receiving ART, underscoring the scale of this cohort [3–5].
While VS individuals represent the majority, the term TE encompasses a clinically heterogeneous population with varied treatment histories. Broadly, it includes individuals with prior ART exposure, that may have a history of virologic failure and/or drug resistance [6]. Compared with treatment-naive PWH, TE PWH are typically older, with a higher burden of comorbidities and exposure to polypharmacy, increasing their vulnerability to adverse events (AEs) and drug–drug interactions [4,7,8].
In the absence of curative intervention, ART remains a lifelong requirement for PWH, with sustained viral suppression contingent upon consistent adherence. However, adherence patterns may fluctuate over the course of an individual’s life due to a variety of clinical, psychosocial and structural factors. Therefore, selecting an ART regimen that is not only safe and effective, but also incorporates a high barrier to resistance and forgiveness in the context of potential suboptimal adherence, is paramount to achieving long-term treatment success [9–12].
As efficacy is comparable across guideline-recommended first-line ART options, treatment decisions are increasingly guided by safety, tolerability and long-term acceptability, which are critical factors in promoting adherence and quality of life [9,10,12].
Aging, increased risk of comorbidities, cumulative drug exposure and potential intolerance or AEs from long-term ART elevate the importance of safety considerations during regimen selection for TE PWH [4,9,13].
Bictegravir/emtricitabine/tenofovir alafenamide (B/F/TAF) is a once-daily, single-tablet regimen (STR) that combines bictegravir, an integrase strand transfer inhibitor (INSTI) with a high-barrier to resistance, plus a dual nucleos(t)ide reverse transcriptase inhibitor (NRTI) backbone of emtricitabine and tenofovir alafenamide (F/TAF), a prodrug designed to reduce systemic tenofovir exposure and mitigate renal and bone toxicity [14,15]. In real-world and clinical-trial settings, B/F/TAF has demonstrated high persistence, low rates of discontinuation due to AEs and stable renal and lipid parameters in diverse populations, including those with prior treatment exposure [16–19].
Objective
Given the established and similar efficacy of modern ART in adherent populations, understanding safety and tolerability differences can help to select optimal treatment regimens. Long-term management of outcomes such as lipids (as important markers of cardiovascular risk), renal function (given the high prevalence of impairment in PWH and age-related decline in kidney function) and overall safety profile are of paramount importance as they reflect the tolerability and real-world acceptability of ART regimens, which may impact adherence, quality of life and long-term treatment success.
A limited number of head-to-head randomized controlled trials (RCTs) comparing B/F/TAF versus other guideline-recommended ART exist, but these have not been conducted versus all available guideline-recommended ARTs [16,17,19,20]. To our knowledge, no prior studies have comprehensively assessed the safety and tolerability of B/F/TAF with other guideline-recommended ARTs in VS TE adults with HIV-1. As such, this study aimed to evaluate key outcomes to compare the safety profile of B/F/TAF with other guideline-recommended ARTs in VS TE adults with HIV-1 via an adjusted indirect comparison in the absence of sufficient head-to-head evidence.
Materials & methods
SLR methods
A systematic literature review (SLR) was conducted to identify relevant B/F/TAF and comparator studies in adults (aged ≥18 years) with HIV-1 infection, who were TE and VS, published 2000 onwards to ensure relevance to modern ART standards. MEDLINE, Embase and The Cochrane Library, including Cochrane Database of Systematic Reviews (CDSR) and Cochrane Central Register of Controlled Trials (CENTRAL) were last searched on 14 June 2023 using search terms detailed in Supplementary Table 1. Database searches were supplemented by manual searches of key conference proceedings and ClinicalTrials.gov (from 2015 to 2023) to ensure that no studies were missed. Predefined eligibility criteria based on the Population, Intervention, Comparison, Outcomes, and Study design were used to review all studies identified from these searches in two stages. Detailed eligibility criteria are provided in Supplementary Table 2. Two independent reviewers assessed each title, abstract, and full text against the inclusion/exclusion criteria. Disagreements were resolved through discussion, with a third independent reviewer making the final decision if needed.
Data extraction process
Data were extracted into pre-specified Microsoft Excel templates based on guidelines from the University of York Centre for Reviews and Dissemination (CRD) [21]. Extracted data included study design, population characteristics, efficacy outcomes, safety end points and resistance profiles. Data were extracted by a single individual and independently verified by a second individual. Data extraction strategy is further detailed in the Supplementary Materials.
Quality assessment
The quality of all RCTs included in the SLR was assessed using the criteria provided by the Cochrane Collaboration’s tool for assessing risk of bias (version 2.0) [22].
Feasibility assessment
Variation between the studies included in the analysis was considered to determine whether there were any meaningful differences in the study design, population and outcome definitions between the studies, which may lead to differences in the observed intervention effects. The SLR identified a connected network of RCTs, confirming the feasibility of conducting a network meta-analysis (NMA).
Heterogeneity assessment
A systematic assessment of heterogeneity was conducted to identify key treatment effect modifiers (TEMs) and ensure that they were balanced in the population adjustment analysis. The following clinically relevant baseline characteristics were compared across studies: viral load, cluster of differentiation 4 (CD4) cell count, age, race/ethnicity, body weight, hepatitis B/C co-infection status, comorbidities and renal function (estimated glomerular filtration rate [eGFR]).
Age, sex, race and CD4 cell count were identified as potentially clinically relevant variables for model adjustment. In the absence of definitive prior literature specifically identifying TEMs for this population, selection was guided by expert clinical judgment and existing knowledge of HIV disease progression and treatment response patterns. For instance, age can impact tolerability and the risk of AEs due to comorbidities and polypharmacy, potentially affecting treatment discontinuation [23]. Sex and race may influence drug pharmacokinetics and susceptibility to specific AEs [23,24]. Baseline CD4 cell count remains a key prognostic factor for long-term immune health and clinical stability, even among VS individuals. These variables were therefore considered essential for inclusion in the population adjustment model to ensure a valid comparison.
Other potential effect modifiers related to treatment history were also examined, including duration of prior treatment, number of prior regimens, type/class of prior regimens and whether treatment switching was due to treatment failure or lack of tolerability. Following a baseline assessment, these variables were found to be comparable across the included trials and were therefore not carried forward into the adjustment model.
In anticipation of clinical heterogeneity across trial populations, an multilevel network meta-regression (ML-NMR) was selected as the primary analytical method. This population-adjustment approach, an extension of standard NMA methods which do not allow for population-adjustment using individual patient data (IPD), was chosen to account for potential differences in pre-specified TEMs, thereby allowing for a robust comparison of treatment effects across the evidence base.
Interventions, outcomes & timepoints of interest
Treatment regimens included in the network comprised both two- and three-drug antiretroviral combinations, which combined a dual NRTI backbone with a third agent from a relevant class (nonnucleoside reverse transcriptase inhibitor [NNRTI], INSTI, or boosted protease inhibitor [PI]), or combinations of INSTIs, PIs, lamivudine (3TC), or rilpivirine (RPV). Multi-tablet regimens and STRs were considered equivalent and are denoted by the notation (+ or /) where both apply. A full list of eligible regimens is provided in the PICOTS table (Supplementary Table 2).
To ensure comparability with the B/F/TAF trials, only studies with a ‘switch’ design were included, regardless of whether this was a ‘switch versus switch’ design (participants in all treatment arms switched to a new regimen following randomization) or a ‘switch versus continue’ design (participants in the control arm stayed on the treatment they received prior to randomization). However, studies with a ‘switch versus delayed switch’ design were not included as this study design was considered incompatible with the designs of other studies in the network and typically did not provide comparative evidence at week 48.
Multiple studies (e.g., GS-US-380-1878, BESTT and STRATEGY) in the analysis reported on either a ‘pooled PI’ or ‘pooled NNRTI’ node [17,25,26]. For example, in the study BESTT, participants in the continue arm were reported to receive different PIs (ritonavir-boosted PIs + TDF/FTC) [26]. These pooled regimens reported at the study-level by more than one study were considered to be equivalent and grouped into single treatment nodes, where required to improve network connectivity and to facilitate class-level comparisons. Specifically, pooled regimens with different NNRTIs were considered equivalent and grouped into a single ‘pooled NNRTI’ treatment node. Similarly, pooled regimens with different boosted PIs were grouped into a ‘pooled PI’ node. This approach allowed for the inclusion of studies that permitted various third agents within the same class. Conversely, to maintain the integrity of these class-based nodes, treatment arms that allowed for third agents from different drug classes were excluded from the analysis. This approach of allowing for pooled regimens introduces heterogeneity, as agents within the NNRTI and PI classes differ in tolerability and drug–drug interaction potential, which should be considered when interpreting class-level comparisons.
Additionally, an assumption was placed on the equivalence of booster doses for PI regimens, where these were also assumed to be equal in the TE setting, and is denoted as (+ or /) b in this study.
For example, the PI-containing arms in GS-US-380-1878, SPARE and STRATEGY-PI were all combined in networks in a single node of PI (+ or /) b + 2 NRTI [17,25,27]. A key assumption for this grouping was that the two different boosting agents used across these trials, ritonavir (r) and cobicistat (c), were considered pharmacologically equivalent for the purpose of the analysis.
The selection of outcomes was guided by the clinical importance of long-term renal and metabolic safety in treatment-experienced PWH. Therefore, the primary renal outcome was the change from baseline (CfB) in eGFR at week 48. Metabolic outcomes included CfB at week 48 in high-density lipoprotein (HDL), low-density lipoprotein (LDL), total cholesterol (TC), the TC/HDL ratio and triglycerides. Although weight gain was investigated, a network analysis was unfeasible as only two studies (BESTT and GS-US-380-1878) reported on weight change [17,26].
Safety outcomes of interest in this study were overall treatment-related AEs (TRAEs), grade 3 or 4 treatment-emergent AEs (TEAEs), diarrhea, nausea, all-cause discontinuation and discontinuation due to AEs at week 48.
Indirect comparison methods
Data input
IPD from three Phase III B/F/TAF trials (GS-US-380-1844, GS-US-380-1878, GS-US-380-4030) were combined with aggregate treatment arm-level data from the five remaining trials [16,17,19]. Treatment-arm level inputs used for the aggregate data trials included: number of events and sample size for binary outcomes (overall TRAE, grade 3 or 4 TEAE, diarrhea, nausea, all-cause discontinuation and discontinuation due to AE) and mean CfB with reported standard errors for continuous outcomes (CfB in eGFR, HDL, LDL, TC, total TC/HDL, triglycerides). Where studies reported median values rather than means for continuous outcomes, medians were assumed to be equal to means for analysis [28]. All lipid outcome data were converted to mg/dl to ensure consistency across studies.
Furthermore, the mean age and CD4 cell count at baseline as well as the proportion of female and non-White patients were recorded for each arm of the aggregate data trials to allow for covariate adjustment. All four covariates (for age, sex, race and baseline CD4 cell count) were available for all treatment arms included in the analysis; no imputations or assumptions regarding missing covariate data were required.
No direct participant data collection occurred, and all source trials had prior ethics approval. Due to the use of anonymized, pre-existing data, this study did not require additional Institutional Review Board review.
Summaries of input data are available in the Supplementary Materials (Supplementary Tables 11–13).
Analyses conducted
ML-NMR was used to integrate IPD from three B/F/TAF studies with aggregate data for other included studies. This approach enabled the adjustment for cross-trial differences in key pre-specified effect modifiers. By accounting for this heterogeneity, ML-NMR reduces the risk of bias in comparative efficacy and safety estimates compared with a standard, unadjusted NMA.
Methodology for ML-NMR followed the approach described by Phillippo et al. [29]. The model was estimated in a Bayesian framework using the software Stan, [30] through the R package multinma [31]. To account for differences in participant characteristics across trials, analyses were performed using three different modeling approaches:
•
Adjusting for age, sex, race and baseline CD4 cell count, treating them as potential effect modifiers. This allowed their impact on outcomes to vary by treatment class. For this purpose, treatment classes were categorized as B/F/TAF, other INSTI-containing regimens and non-INSTI-containing regimens;
•
Adjusting for the same covariates as in (1), but as prognostic factors, assuming a uniform effect across all treatment classes; and
•
Models without covariate adjustment.
The ML-NMR methodology is described in further detail in the Supplementary Materials.
Assessment of model fit
A fixed effects model was used, as no direct comparison in the network was informed by more than one study, and the use of a random effects model was considered unlikely to provide stable or reliable estimates. However, random effects models were also run to check for any residual heterogeneity remaining after adjusting for clinically relevant variables. The deviance information criterion and total residual deviance were generated and compared across models.
Simulation parameters & prior distributions
Model parameters were estimated using quasi-Monte-Carlo sampling based on Sobol's sequences as implemented in the multinma package [31]. Vague priors were specified for all basic model parameters (with half-normal distributions for variance parameters, and normal distributions otherwise), with prior distribution parameters modified according to the scale of the outcome.
Assessment of convergence
Convergence was assessed by using the potential scale reduction factor Rhat, effective sample sizes and Monte Carlo standard errors.
Results output
The ML-NMR model produced population-average marginal treatment effects, which were standardized to the covariate distribution of the pooled B/F/TAF IPD. For continuous outcomes, the posterior medians of mean differences (MDs) and for binomial outcomes, the posterior medians of risk differences (RDs), odds ratios (ORs) and risk ratios (RRs) were produced alongside 95% credible intervals (CrIs).
Results
SLR & feasibility assessment
Eligibility assessment
Of the 79 RCTs identified in the SLR, 40 were performed in VS TE PWH. The definitions of TE varied between the different studies, but generally included participants with prior exposure to ART. Most studies required participants to have been on an ART regimen for at least 6 months prior to baseline or achievement of a minimum level of virologic suppression. The flow of records through the various review stages is presented in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) diagram in Figure 1. The following steps were followed when assessing eligibility of studies for the NMA:
•
Studies that had an incompatible study design (switch vs delayed switch study design, or reported on a post hoc nonrandomized analysis or open-label extension) were excluded (n = 4)
○
Although switch versus delayed switch design provides insight into the longitudinal performance of a switch regimen, these studies (n = 2) were excluded from the analysis for the following reasons: first, the delayed switch in the continue arm typically occurred at week 24, meaning the continue arm no longer represented a valid comparator at the week 48 timepoint of interest; and second, once the delayed switch occurred, the continue arm did not connect to the broader evidence network
•
Studies that did not report on a treatment regimen of interest (treatment arms permitting multiple third agents across treatment classes, only investigating different dosing regimens for the same NNRTI, only investigating different regimens within PIs, or only investigating two- vs three-drug antiretroviral combinations for the same PI) were excluded (n = 20)
•
Studies that did not report data at timepoints of interest (at or after week 48) for the outcomes of interest were excluded (n = 2)
•
Studies that did not connect to outcome networks were excluded (n = 6)
•
Eight studies were eligible for inclusion in analyses
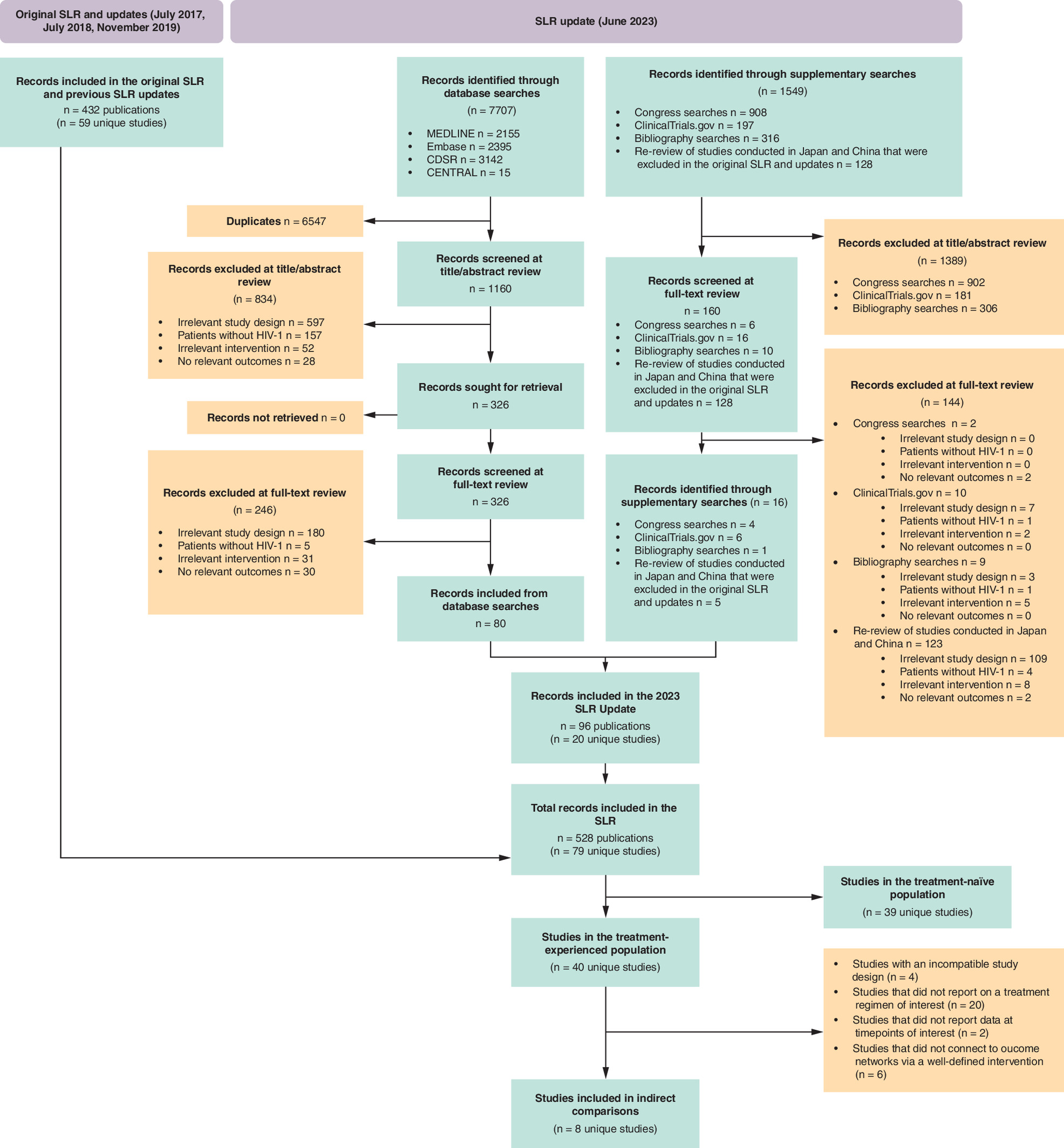
Figure 1. PRISMA flowchart for inclusion in systematic literature review and indirect treatment comparisons.
CENTRAL: Cochrane Central Register of Controlled Trials; CDSR: Cochrane Database of Systematic Review; HIV-1: Human immunodeficiency virus type 1; ITC: Indirect treatment comparison; SLR: Systematic literature review.
A list of excluded studies is reported in Supplementary Table 8.
Study characteristics
Study characteristics of all included studies are detailed in Supplementary Table 4.
Of the eight included studies, five were conducted in multiple countries, whereas three trials took place in a single country.
The majority of studies (n = 7) were Phase III or IIIb studies with one Phase IV study. Blinding was only carried out in two studies (GS-US-380-1844 and GS-US-380-1844) [19,32]. The predominance of open-label designs is a common and important limitation in contemporary ART trials, often due to the practical difficulty of blinding different STRs. The majority of studies (n = 5) were reported as being noninferiority studies. A key finding regarding the study characteristics was the inconsistent and often incomplete reporting of treatment history details. Where reported (n = 2), the number of prior regimens was no more than two, only one study permitted PWH who had failed prior treatments, and three studies permitted PWH who had switched due to lack of tolerability on prior regimens. Furthermore, baseline resistance data were generally not reported, limiting a comprehensive characterization of the populations' resistance profiles at study entry. All included studies were of a switch versus continue design, meaning that the prior regimen participants had received typically featured in the design of the study under investigation.
Quality assessment
A detailed risk of bias assessment for the eight studies included in indirect comparisons is presented in the Supplementary Materials (Supplementary Table 5) and top-line summaries of the quality assessments are presented in Supplementary Table 6. Overall, randomization and treatment allocation were carried out appropriately, and treatment arms were well-balanced in terms of prognostic factors at baseline. However, reporting of outcomes was potentially biased in two studies. The most substantial limitation of the RCTs overall was a lack of blinding (only two studies were double-blinded), which may have led to bias in the ascertainment and reporting of safety outcomes.
Baseline characteristics
Heterogeneity in participants' baseline characteristics was assessed across studies eligible for analysis. Baseline characteristics are summarized below and presented in Supplementary Table 7. Sample sizes ranged from 58 to 670. While no study was excluded based on small sample sizes alone, SPARE was not included in analyses of discontinuation outcomes as the combination of the study’s small sample size and the rare nature of these outcomes did not allow for a robust comparison based on this study [27]. The mean age of study populations was between 37.0–50.4 years across studies and the populations were predominantly male, except for the BESTT study, which had a female-only population [26].
The baseline characteristics of the included trial populations were broadly consistent with the established clinical profile of a modern, VS, treatment-experienced cohort. For example, participants were typically immunologically stable, with mean baseline CD4 cell counts consistently high (between 500 and 700 cells/μl) across all studies. However, significant heterogeneity was observed in key demographic characteristics, particularly race and ethnicity (Supplementary Table 7). While most studies predominantly enrolled White participants, the BESTT study included a high proportion of Black PWH, and the SPARE study exclusively enrolled Asian PWH [26,27]. The differences observed here also justified the use of the ML-NMR approach selected for this analysis, which permits robust adjustment for these potential effect modifiers. In contrast, the prevalence of Hepatitis B and C coinfection was low and generally well-balanced where reported, ranging from 0 to 6.7%.
Finally, studies varied regarding previous treatment regimens. A similar number of studies recruited PWH who were previously on a PI, INSTI and NNRTI. Emtricitabine/tenofovir disoproxil fumarate (F/TDF) was the most frequent backbone of the previous regimen in most studies, followed by emtricitabine/tenofovir alafenamide (F/TAF) and ABC/3TC.
Outcomes assessment
Outcome definitions were broadly aligned across studies for all outcomes investigated as part of the feasibility assessment (Supplementary Table 9). Heterogeneity was observed in the definitions of CfB in eGFR. Specifically, while most studies reported the absolute change in eGFR via the Cockcroft-Gault formula, the SPARE study reported mean percentage change, and the BESTT study used an eGFR calculation adjusted for body surface area [26,27]. All other outcome definitions were considered homogeneous. Furthermore, SOLAR was the only study that reported alternative definitions for grade 3/4 TEAEs, reporting grade 3–5 TEAEs in contrast to other studies which reported grade 3/4 TEAEs [20]. However, this outcome was deemed comparable. In contrast, the definition reported for diarrhea in SOLAR (drug-related diarrhea) was not deemed comparable to the definition used in other studies (treatment-emergent diarrhea) and SOLAR was therefore excluded from comparisons of diarrhea. There was no heterogeneity in the definitions of all other outcomes.
All outcomes investigated as part of the feasibility assessment were reported by at least 4/8 studies and at most 7/8 studies. CfB in eGFR and overall TRAEs were reported by 4/8 studies, CfB in lipid outcomes and nausea were reported by 5/8 studies and grade 3/4 TEAEs and diarrhea were reported by 6/8 studies. All interventions for which there were reported outcome data connected to B/F/TAF in the relevant network. Most of the treatment regimens connected either directly to B/F/TAF or via one common comparator. A list of treatment regimens of interest included in this analysis are summarized in Supplementary Table 3.
ML-NMR results
For each outcome, a base-case (unadjusted) model was compared with models that adjusted for baseline covariates (age, sex, race and CD4 cell count). The preferred model was selected based on statistical fit. The results presented below are from the preferred model for each specific outcome, as summarized in Supplementary Table 10. For adjusted outcomes, the results represent population-average marginal effects, standardized to the B/F/TAF trial population. For unadjusted outcomes, the results represent standard NMA estimates.
Lipid outcomes
Results for lipid outcomes at week 48 are presented below. Network diagrams for each outcome are presented in Figure 2, forest plots in Figure 5 and a summary of results in Table 1. Data for absolute outcomes, MDs and associated 95% CrIs are presented in units of mg/dl.
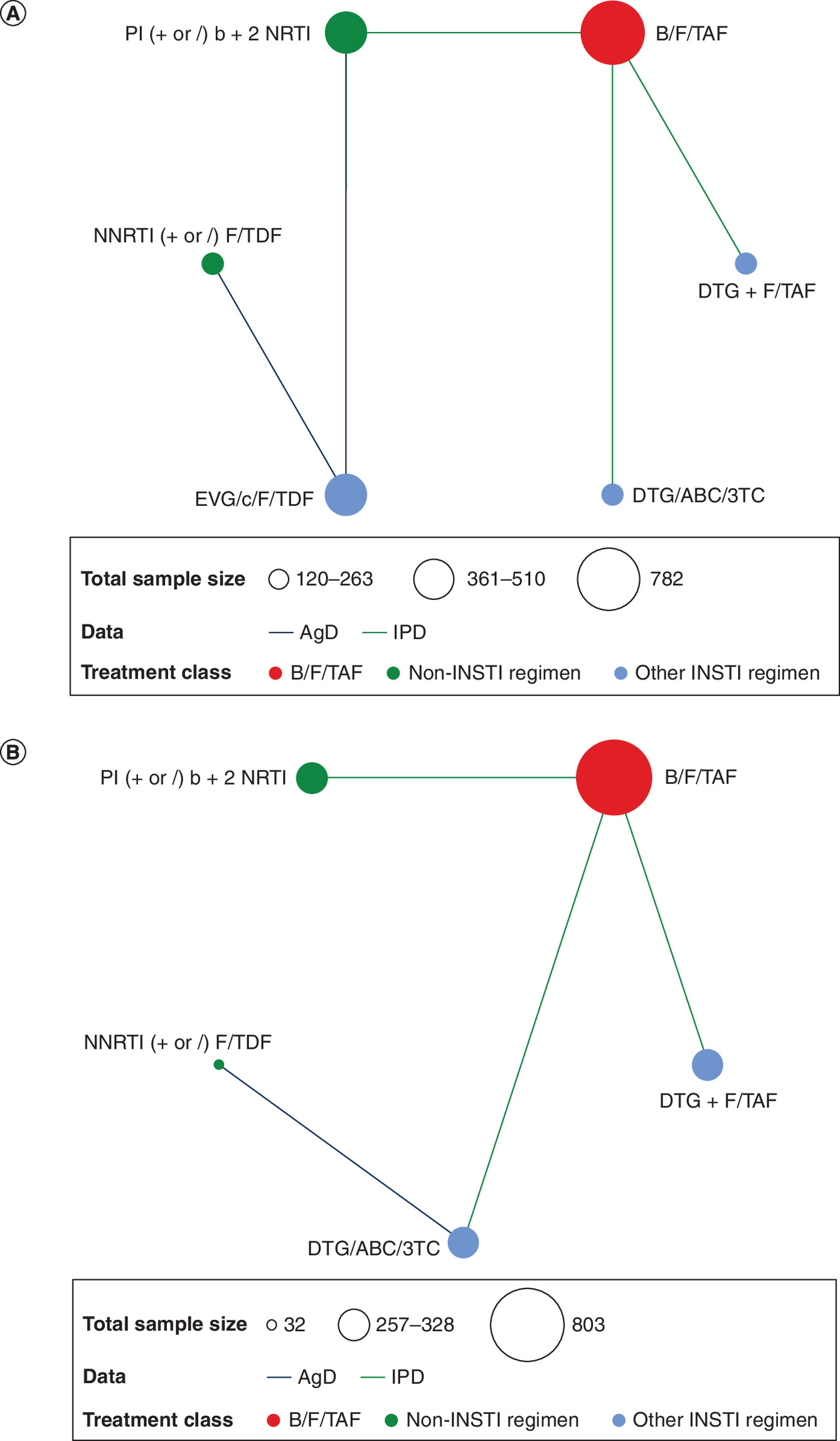
Figure 2. Analysis networks at week 48: lipid and renal outcomes.
(A) CfB in lipid outcomes (HDL, LDL, TC, TC:HDL ratio, triglycerides) and (B) CfB in eGFR.
AgD: Aggregate data; ABC/3TC: Abacavir/lamivudine; CfB: Change from baseline; DTG: Dolutegravir; eGFR: Estimated glomerular filtration rate; EVG/c: Elvitegravir/cobicistat; F/TAF: Emtricitabine/tenofovir alafenamide; F/TDF: Emtricitabine/tenofovir disoproxil fumarate; HDL: High density lipoprotein; INSTI: Integrase strand transfer inhibitor; IPD: Individual participant data; LDL: Low density lipoprotein; NRTI: Nucleoside reverse transcriptase inhibitors; NNRTI: Non-nucleoside reverse transcriptase inhibitors; PI: Protease inhibitor; TC: Total cholesterol.
| Third agent class | Comparator | Mean difference (95% CrI) of B/F/TAF vs comparators | |||||
|---|---|---|---|---|---|---|---|
| eGFR, ml/min§ | HDL, mg/dl | LDL, mg/dl | Total cholesterol, mg/dl | Total cholesterol:HDL ratio | Triglycerides, mg/dl | ||
| INSTI-containing | DTG + F/TAF | 1.30 (-0.90, 3.48) | -1.13 (-2.66, 0.41) | -0.21 (-5.14, 4.89) | -0.16 (-5.70, 5.27) | 0.08 (-0.10, 0.26) | 1.62 (-12.33, 15.46) |
| DTG/ABC/3TC | 3.81 (1.74, 5.97)† | -1.37 (-3.11, 0.34) | 3.22 (-1.26, 7.76) | 0.81 (-4.23, 6.06) | 0.10 (-0.10, 0.30) | -15.01 (-29.18, -1.06)† | |
| EVG/c/F/TDF | – | -1.22 (-4.00, 1.72) | -5.52 (-13.97, 2.72) | -7.57 (-16.71, 1.72) | 0.24 (-0.43, 0.89) | 5.46 (-22.26, 33.29) | |
| Non-INSTI containing | NNRTI (+ or /) F/TDF | -4.54 (-10.41, 1.50) | -4.35 (-7.76, -0.70)‡ | -8.50 (-18.64, 1.32) | -12.43 (-23.26, -1.53)† | 0.34 (-0.34, 1.01) | 4.71 (-28.04, 36.72) |
| PI (+ or /) b + 2 NRTI | -3.53 (-5.91, -1.08)‡ | 1.13 (-0.60, 2.83) | -5.56 (-11.71, 0.57) | -5.72 (-12.16, 0.94) | -0.06 (-0.30, 0.18) | -24.48 (-41.60, -7.47)† | |
The table shows mean differences for B/F/TAF vs comparators for all lipid outcomes at week 48.
†
Indicates where mean differences showed a statistically significant improvement for B/F/TAF vs comparator.
‡
Indicates where mean differences showed a statistically significant improvement for comparator vs B/F/TAF.
§
BESTT reported eGFR change from baseline in eGFR in mL/min/1.73 m2.
ABC/3TC: Abacavir/lamivudine; CrI: Credible interval; DTG: Dolutegravir; eGFR: Estimated glomerular filtration rate; EVG/c: Elvitegravir/cobicistat; F/TAF: Emtricitabine/tenofovir alafenamide; F/TDF: Emtricitabine/tenofovir disoproxil fumarate; HDL: High density lipoprotein; INSTI: Integrase strand transfer inhibitor; LDL: Low density lipoprotein; ML-NMR: Multilevel network meta-regression; NRTI: Nucleoside reverse transcriptase inhibitors; NNRTI: Non-nucleoside reverse transcriptase inhibitor; PI: Protease inhibitor.
CfB in HDL
The estimated absolute mean CfB in HDL was 0.76 (0.27, 1.23) for B/F/TAF. The adjusted analysis showed B/F/TAF was associated with a significantly smaller increase in HDL compared with NNRTI (+ or /) F/TDF, as indicated by a MD (95% CrI) of -4.35 (-7.76, -0.70). B/F/TAF showed no significant difference in HDL versus PI (+ or /) b + 2 NRTI (MD [95% CrI]: 1.13 [-0.60, 2.83]), as well as dolutegravir- and elvitegravir-based regimens, with MD (95% CrI) -1.13 (-2.66, 0.41) versus DTG + F/TAF, -1.37 (-3.11, 0.34) versus DTG/ABC/3TC, and -1.22 (-4.00, 1.72) versus EVG/c/F/TDF.
CfB in LDL
The estimated absolute mean CfB in LDL was 1.64 (0.15, 3.16) for B/F/TAF. In the adjusted analysis, no significant differences were observed in CfB in LDL levels when switching to B/F/TAF compared with any regimen, with MD (95% CrI) ranging from -8.50 (-18.64, 1.32) versus NNRTI (+ or /) F/TDF to 3.22 (-1.26, 7.76) versus DTG/ABC/3TC.
CfB in total cholesterol
The estimated absolute mean CfB in TC was 0.17 (-1.51, 1.90) for B/F/TAF. Adjusted analysis showed B/F/TAF was associated with a statistical reduction in TC levels versus NNRTI (+ or /) F/TDF (MD [95% CrI]: -12.43 [-23.26, -1.53]). In comparisons with other regimens, B/F/TAF showed no statistically significant differences in CfB in TC levels, including EVG/c/F/TDF, PI (+ or /) b + 2 NRTI, DTG + F/TAF and DTG/ABC/3TC.
CfB in TC to HDL ratio
The estimated absolute mean CfB in TC to HDL ratio was -0.03 (-0.09, 0.03) for B/F/TAF. In the unadjusted model, changes in the TC to HDL ratio were similar when switching to B/F/TAF versus all other regimens in the network, with no statistically significant differences observed.
CfB in triglycerides
The estimated absolute mean CfB in triglycerides was 1.13 (-3.12, 5.42) for B/F/TAF. In the unadjusted model, B/F/TAF showed a statistical reduction in triglyceride levels after switch versus DTG/ABC/3TC and PI (+ or /) b + 2 NRTI (MD [95% CrI]: -15.01 [-29.18, -1.06] and -24.48 [-41.60, -7.47], respectively). B/F/TAF showed no differences in CfB in triglyceride levels versus DTG + F/TAF, EVG/c/F/TDF and NNRTI (+ or /) F/TDF.
Renal outcomes (CfB in eGFR)
Results for CfB in eGFR at week 48 are presented below. Network diagram for this outcome is presented in Figure 2, forest plot in Figure 5 and a summary of results in Table 1.
The estimated absolute mean CfB in eGFR was -0.72 (-1.37, -0.06) for B/F/TAF. Adjusting for baseline effect modifiers, the decline in eGFR was significantly greater on DTG/ABC/3TC compared with switching to B/F/TAF, leading to a positive MD [95% CrI] of 3.81 [1.74, 5.97] between B/F/TAF and DTG/ABC/3TC. B/F/TAF was associated with a statistically greater decline in eGFR compared with PI (+ or /) b + 2 NRTI (MD [95% CrI]: -3.53 [-5.91, -1.08]). Compared with other regimens, switching to B/F/TAF generally resulted in similar or stable eGFR values, including DTG + F/TAF (MD [95% CrI]: 1.30 [-0.90, 3.48]) and NNRTI (+ or /) F/TDF (MD [95% CrI]: -4.54 [-10.41, 1.50]).
Adverse events outcomes
Results for adverse event outcomes at week 48 are presented below. The network diagrams for each outcome are presented in Figure 3, forest plots in Figure 6 and a summary of results in Table 2.
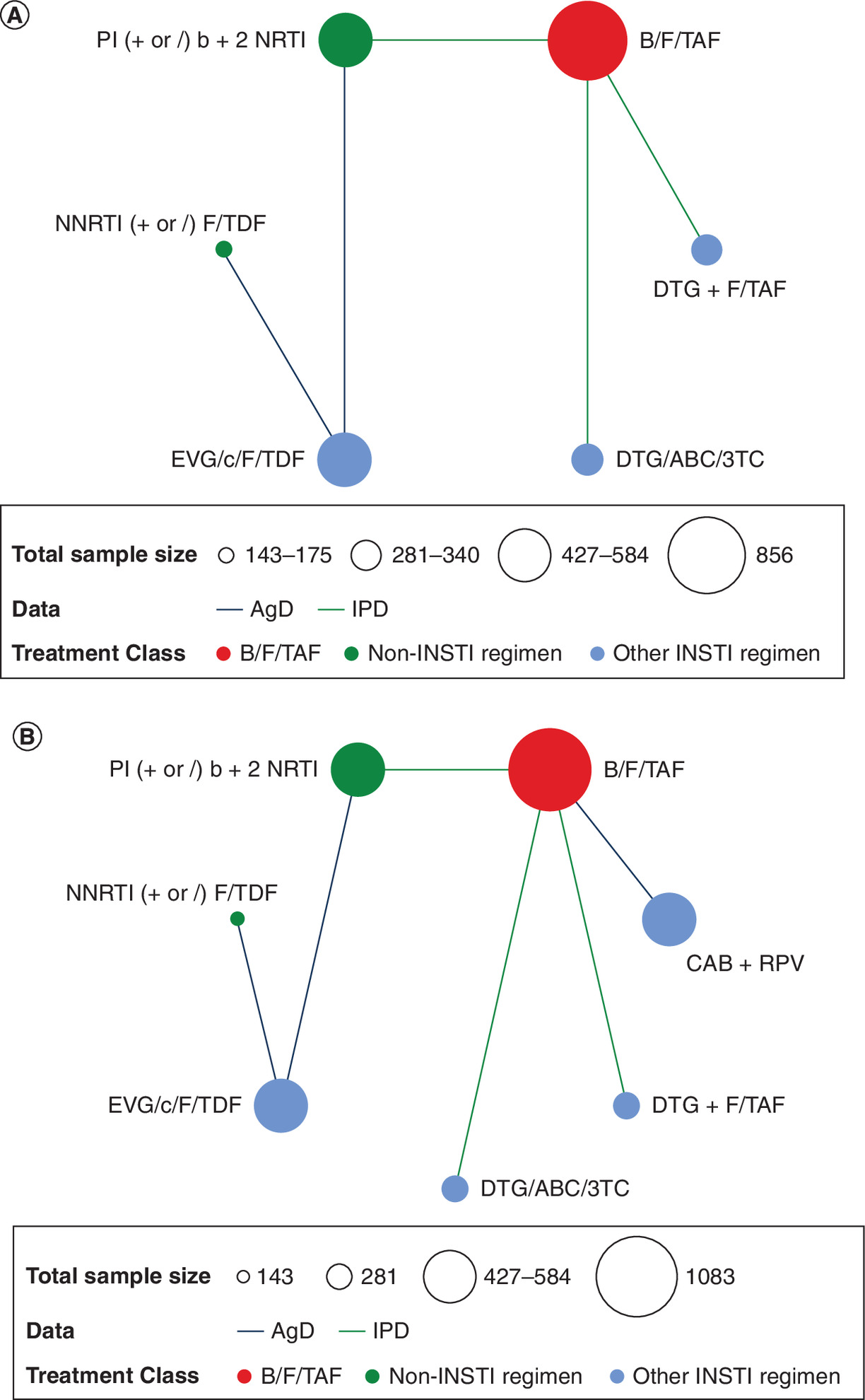
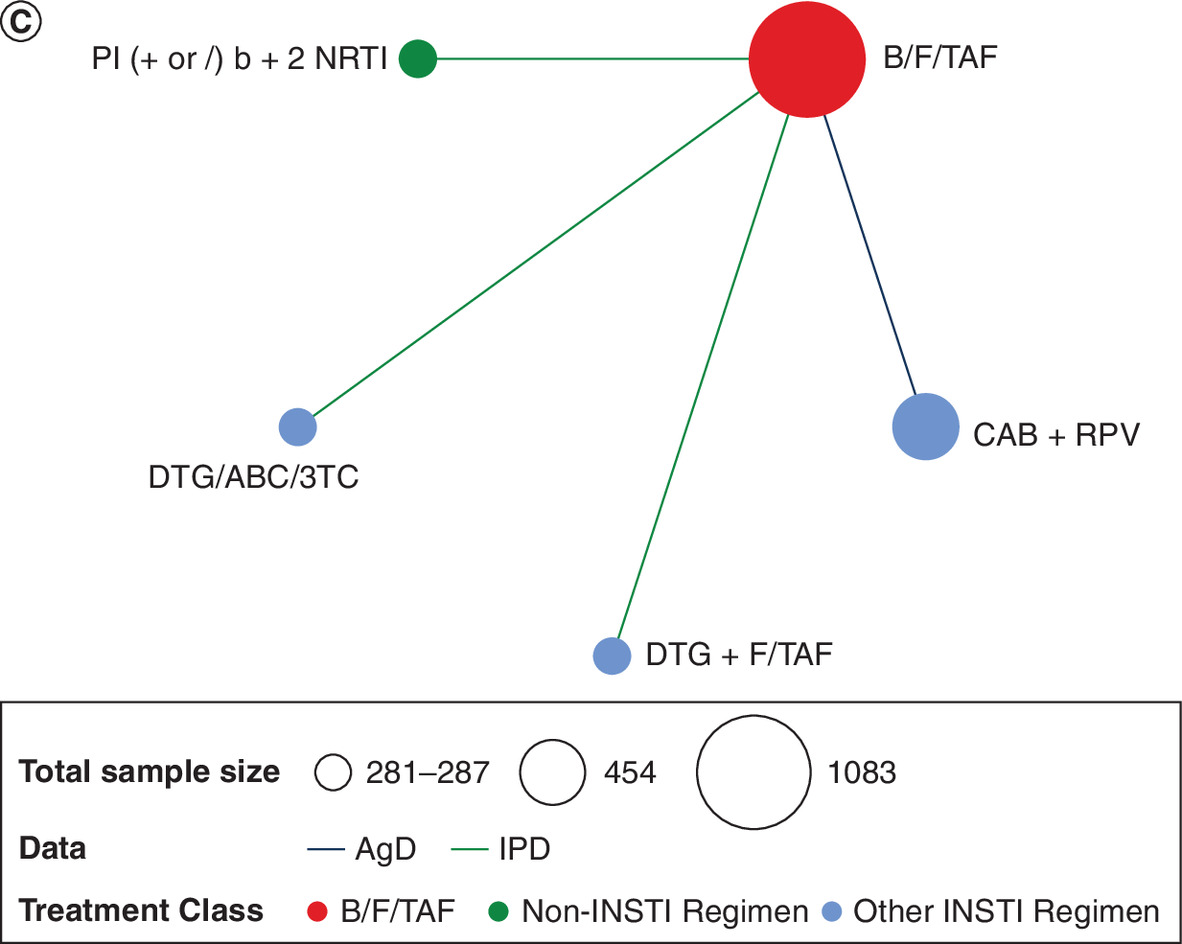
Figure 3. Analysis networks at week 48: adverse events outcomes.
(A) Risk of diarrhea and risk of nausea and (B) Grade 3/4 TEAE and (C) Overall TRAE.
AgD: Aggregate data; ABC/3TC: Abacavir/lamivudine; CAB: Cabotegravir; DTG: Dolutegravir; EVG/c: Elvitegravir/cobicistat; F/TAF: Emtricitabine/tenofovir alafenamide; F/TDF: Emtricitabine/tenofovir disoproxil fumarate; INSTI: Integrase strand transfer inhibitor; IPD: Individual participant data; NRTI: Nucleoside reverse transcriptase inhibitors; NNRTI: Non-nucleoside reverse transcriptase inhibitor; PI: Protease inhibitor; RPV: Rilpivirine; TEAE: Treatment emergent adverse event; TRAE: Treatment-related adverse event.
| Third agent class | Comparator | Risk difference (95% CrI) of B/F/TAF vs comparators | |||||
|---|---|---|---|---|---|---|---|
| Diarrhea | Nausea | Grade 3 or 4 TEAE | Overall TRAE | All cause discontinuation | Discontinuation due to AE | ||
| INSTI-containing | CAB + RPV | – | – | 0.01 (-0.02, 0.03) | -0.69 (-0.84, -0.43)† | – | -0.09(-0.44, -0.01)† |
| DTG + F/TAF | -0.03 (-0.10, 0.01) | 0.00 (-0.04, 0.02) | 0.03 (0.00, 0.05)‡ | 0.04 (-0.00, 0.07) | -0.03 (-0.10, 0.01) | -0.00 (-0.03, 0.01)§ | |
| DTG/ABC/3TC | 0.03 (-0.02, 0.06) | -0.06 (-0.19, -0.01)† | 0.00 (-0.05, 0.04) | -0.12 (-0.23, -0.04)† | 0.02 (-0.03, 0.05) | 0.01 (-0.01, 0.02) | |
| EVG/c/F/TDF | 0.03 (-0.06, 0.06) | -0.00 (-0.12, 0.03)§ | 0.01 (-0.08, 0.05) | – | 0.03 (-0.02, 0.06) | 0.01 (-0.03, 0.02) | |
| Non-INSTI containing | NNRTI (+ or /) F/TDF | 0.04 (-0.07, 0.07) | 0.02 (-0.04, 0.04) | 0.01 (-0.12, 0.06) | – | 0.01 (-0.08, 0.05) | 0.01 (0.00, 0.02)‡,¶ |
| PI (+ or /) b + 2 NRTI | 0.02 (-0.03, 0.05) | 0.02 (-0.00, 0.03) | -0.03 (-0.12, 0.01) | 0.11 (0.09, 0.13)‡ | -0.04 (-0.11, 0.01) | 0.01 (-0.04, 0.02) | |
The table shows risk differences for B/F/TAF vs comparators for all safety outcomes at week 48.
†
Indicates where risk differences showed a statistically lower risk for B/F/TAF vs comparator.
‡
Indicates where risk differences showed a statistically higher risk for B/F/TAF vs comparator.
§
Results are presented as ‘-0.00’ if they were negative but round to 0 at two decimal places.
¶
The value was >0 for the lower bound but rounds to zero for two decimal places.
ABC/3TC: Abacavir/lamivudine; AE: Adverse event; CAB: Cabotegravir; CrI: Credible interval; DTG: Dolutegravir; EVG/c: Elvitegravir/cobicistat; F/TAF: Emtricitabine/tenofovir alafenamide; F/TDF: Emtricitabine/tenofovir disoproxil fumarate; INSTI: Integrase strand transfer inhibitor; ML-NMR: Multilevel network meta-regression; NRTI: Nucleoside reverse transcriptase inhibitors; NNRTI: Non-nucleoside reverse transcriptase inhibitors; PI: Protease inhibitor; RPV: Rilpivirine; TEAE: Treatment emergent adverse event; TRAE: Treatment-related adverse event.
PWH experiencing overall TRAE
The estimated absolute risk of overall TRAEs for B/F/TAF was 12%. In the adjusted model, B/F/TAF was associated with a statistically higher risk compared with PI (+ or /) b + 2 NRTI (0.11 [0.09, 0.13]), and a similar risk versus DTG + F/TAF (0.04 [-0.00, 0.07]). Conversely, B/F/TAF showed a statistically lower risk of overall TRAEs compared with CAB + RPV (RD [95% CrI]: -0.69 [-0.84, -0.43]) – largely driven by injection site reactions (ISRs) – and DTG/ABC/3TC (-0.12 [-0.23, -0.04]).
PWH experiencing grade 3 or 4 TEAEs
The estimated absolute risk of PWH experiencing grade 3 or 4 TEAEs for B/F/TAF was 7%. Overall, in the adjusted model, B/F/TAF showed a higher risk compared with DTG + F/TAF with a RD (95% CrI) of 0.03 (0.00, 0.05). Other comparisons were not significant, including versus CAB + RPV (0.01 [-0.02, 0.03]), DTG/ABC/3TC (0.00 [-0.05, 0.04]), EVG/c/F/TDF (0.01 [-0.08, 0.05]), NNRTI (+ or /) F/TDF (0.01 [-0.12, 0.06]) and PI (+ or /) b + 2 NRTI (-0.03 [-0.12, 0.01]).
Diarrhea
The estimated absolute risk for B/F/TAF of TE PWH experiencing diarrhea was 9%. In the adjusted model, no significant differences were observed versus the included comparators, with RDs (95% CrI) ranging from -0.03 (-0.10, 0.01) versus DTG + F/TAF to 0.04 (-0.07, 0.07) for NNRTI (+ or /) F/TDF.
Nausea
The estimated absolute risk of experiencing nausea for B/F/TAF was 4%. The adjusted model showed that B/F/TAF had a statistically lower risk of nausea compared with DTG/ABC/3TC, with an RD (95% CrI) of -0.06 (-0.19, -0.01). Differences were otherwise small and nonsignificant versus DTG + F/TAF (0.00 [-0.04, 0.02]), EVG/c/F/TDF (-0.00 [-0.12, 0.03]), NNRTI (+ or /) F/TDF (0.02 [-0.04, 0.04]), and PI (+ or /) b + 2 NRTI (0.02 [-0.00, 0.03]).
Discontinuation outcomes
Results for discontinuation outcomes at week 48 are presented below. Network diagrams for each outcome are presented in Figure 4, forest plots in Figure 7 and a summary of results in Table 2.
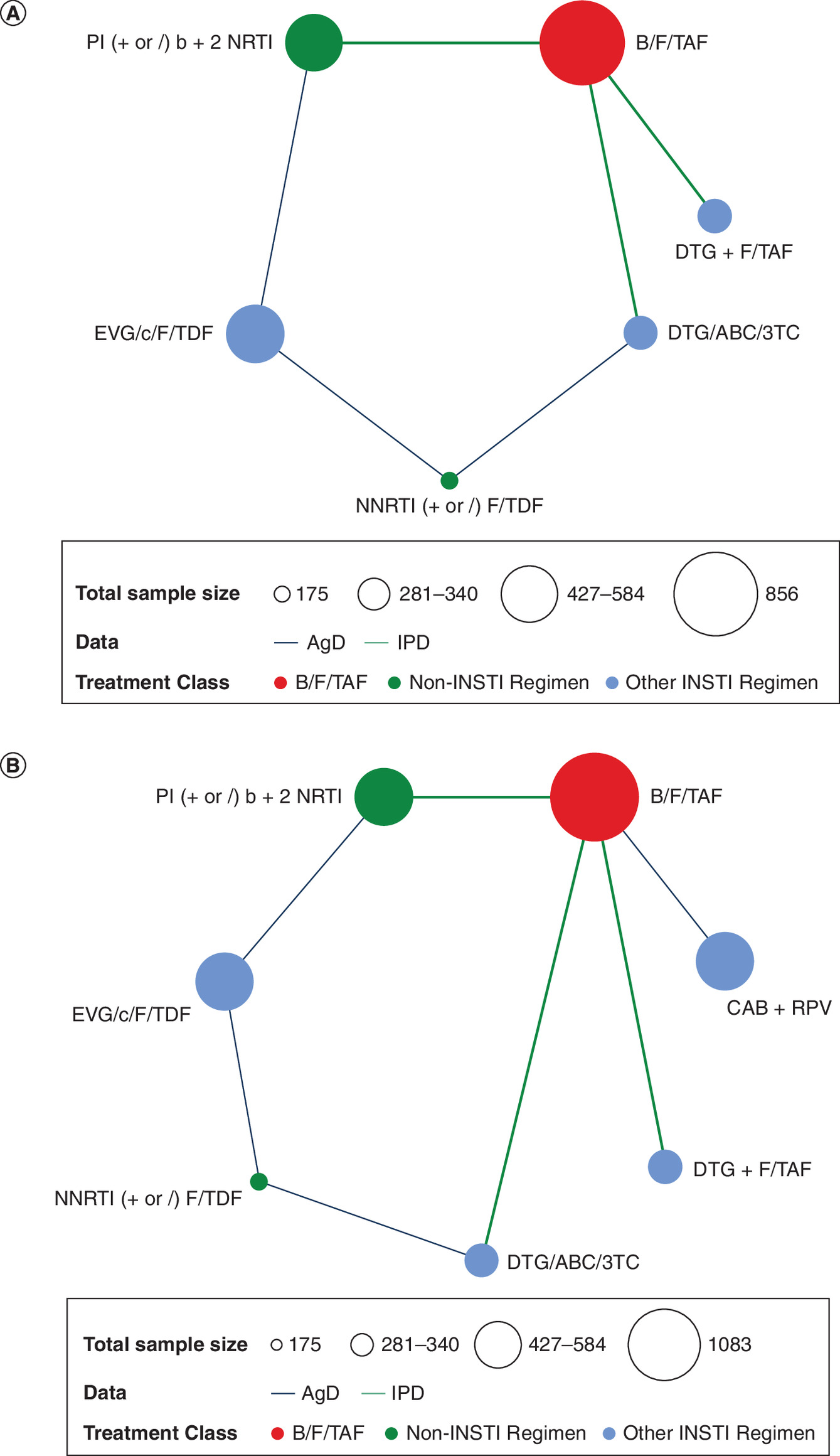
Figure 4. Analysis networks at week 48: discontinuation outcomes.
(A) All-cause discontinuation and (B) Discontinuation due to AE.
AgD: Aggregate data; ABC/3TC: Abacavir/lamivudine; AE: Adverse event; CAB: Cabotegravir; DTG: Dolutegravir; EVG/c: Elvitegravir/cobicistat; F/TAF: Emtricitabine/tenofovir alafenamide; F/TDF: Emtricitabine/tenofovir disoproxil fumarate; INSTI: Integrase strand transfer inhibitor; IPD: Individual participant data; NRTI: Nucleoside reverse transcriptase inhibitors; NNRTI: Non-nucleoside reverse transcriptase inhibitor; PI: Protease inhibitor; RPV: Rilpivirine.
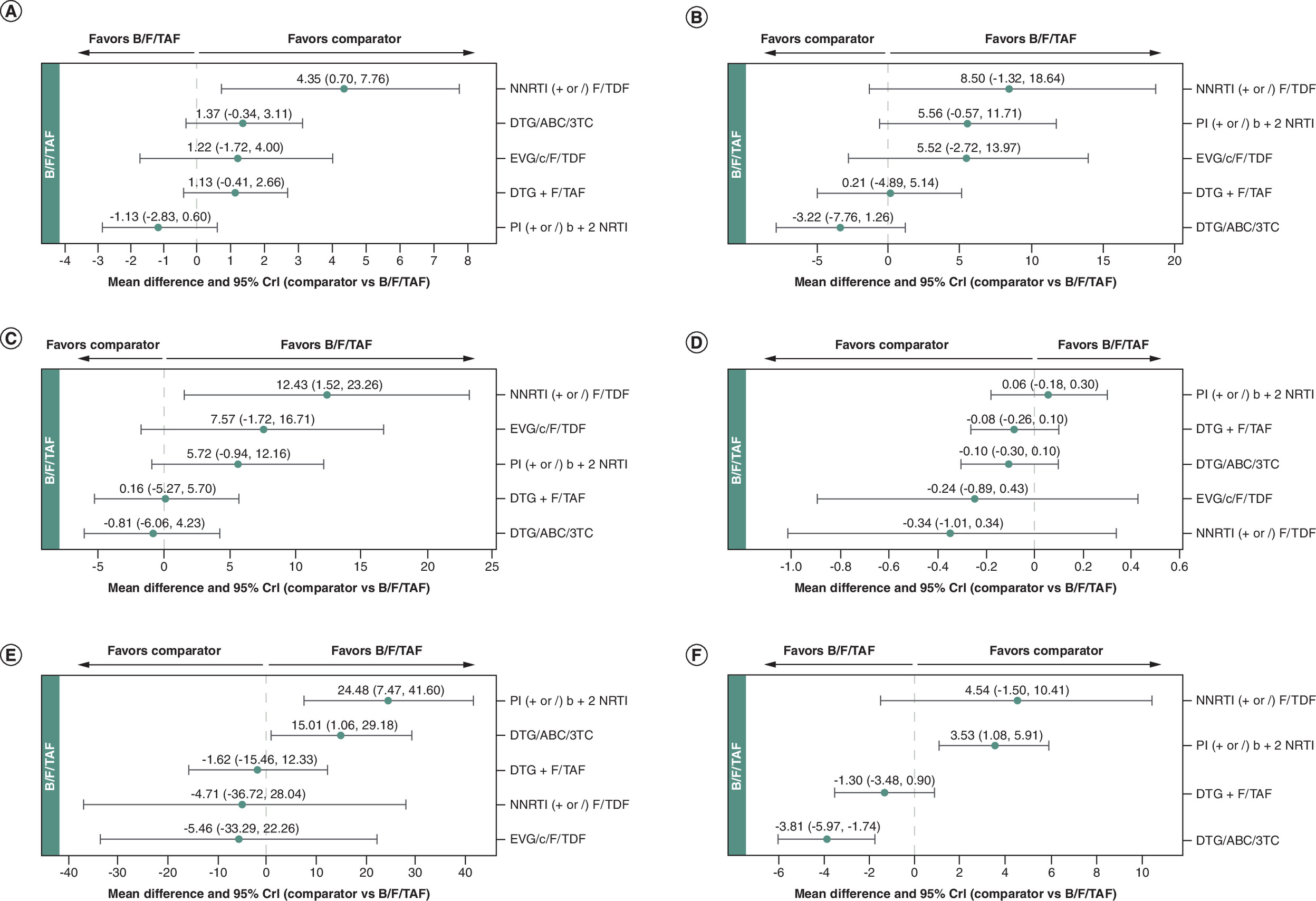
Figure 5. Forest plots: lipid and renal outcomes (comparators vs B/F/TAF).
(A) CfB in HDL; (B) CfB in LDL; (C) CfB in total cholesterol; (D) CfB in total cholesterol to HDL ratio; (E) CfB in triglycerides and (F) CfB in eGFR.
ABC/3TC: Abacavir/lamivudine; CfB: Change from baseline; CrI: Credible interval; DTG: Dolutegravir; eGFR: Estimated glomerular filtration rate; EVG/c: Elvitegravir/cobicistat; F/TAF: Emtricitabine/tenofovir alafenamide; F/TDF: Emtricitabine/tenofovir disoproxil fumarate; HDL: High density lipoprotein; LDL: Low density lipoprotein; NRTI: Nucleoside reverse transcriptase inhibitors; NNRTI: Non-nucleoside reverse transcriptase inhibitor; PI: Protease inhibitor.
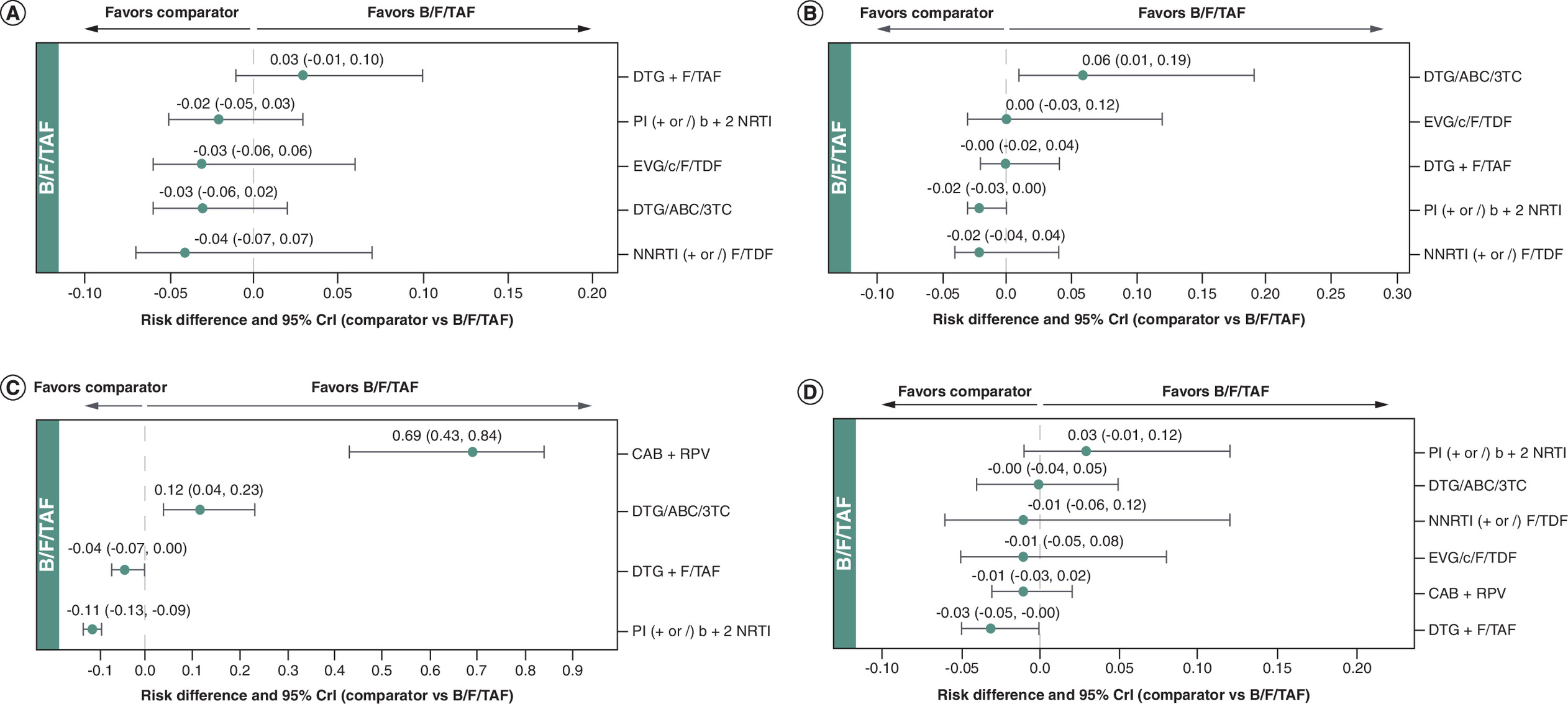
Figure 6. Forest plots: adverse events outcomes (comparators vs B/F/TAF).
(A) Diarrhea; (B) Nausea; (C) Overall TRAE and (D) Grade 3/4 TEAE.
ABC/3TC: Abacavir/lamivudine; CAB: Cabotegravir; CrI: Credible interval; DTG: Dolutegravir; EVG/c: Elvitegravir/cobicistat; F/TAF: Emtricitabine/tenofovir alafenamide; F/TDF: Emtricitabine/tenofovir disoproxil fumarate; NRTI: Nucleoside reverse transcriptase inhibitors; NNRTI: Non-nucleoside reverse transcriptase inhibitor; PI: Protease inhibitor; RPV: Rilpivirine; TEAE: Treatment emergent adverse event; TRAE: Treatment-related adverse event.
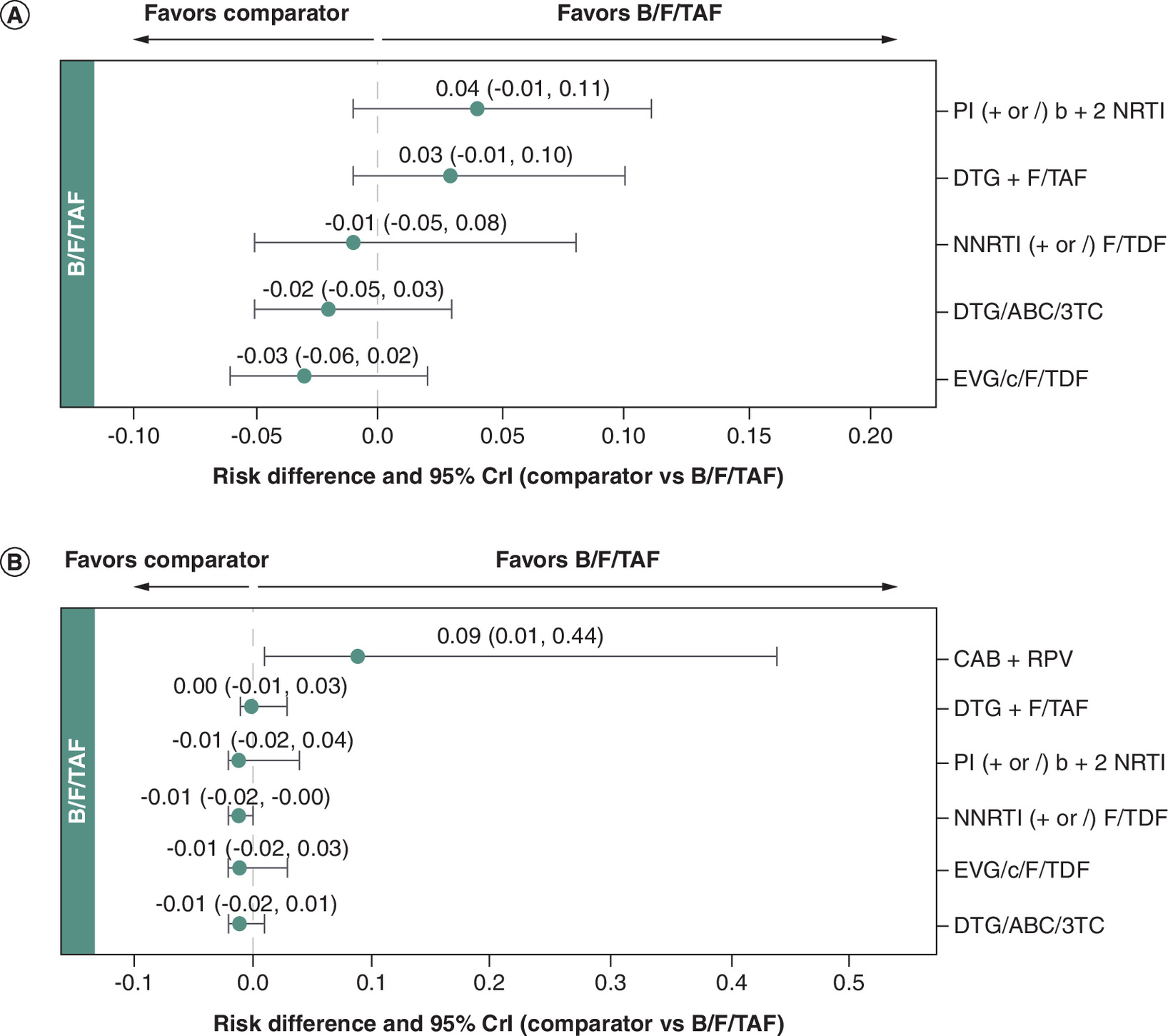
Figure 7. Forest plots: discontinuation outcomes (comparators vs B/F/TAF).
(A) All-cause discontinuation and (B) Discontinuation due to AE.
ABC/3TC: Abacavir/lamivudine; AE: Adverse event; CAB: Cabotegravir; CrI: Credible interval; DTG: Dolutegravir; EVG/c: Elvitegravir/cobicistat; F/TAF: Emtricitabine/tenofovir alafenamide; F/TDF: Emtricitabine/tenofovir disoproxil fumarate; NRTI: Nucleoside reverse transcriptase inhibitors; NNRTI: Non-nucleoside reverse transcriptase inhibitors; PI: Protease inhibitor; RPV: Rilpivirine.
All-cause discontinuation
The estimated absolute risk of experiencing discontinuation due to any cause for B/F/TAF was 8%. Overall, in the adjusted model, B/F/TAF showed a similar risk of discontinuation compared with all other ARTs, with RD (95% CrI) ranging from -0.04 (-0.11, 0.01) for PI (+ or /) b + 2 NRTI to 0.03 (-0.02, 0.06) for EVG/c/F/TDF.
Discontinuation due to AEs
The estimated absolute risk for B/F/TAF of PWH discontinuing due to AEs was 1%. The unadjusted model showed that B/F/TAF was associated with a statistically lower risk of discontinuation due to AEs compared with CAB + RPV, with a RD (95% CrI) of -0.09 (-0.44, -0.01), and a statistically higher risk versus NNRTI (+ or /) F/TDF (0.01 [0.00, 0.02]). For other comparators, differences were not statistically significant.
Discussion
This study compared B/F/TAF with ARTs in VS TE PWH, focusing on lipid profile, renal function and overall safety and tolerability. These outcomes were selected because HIV infection is associated with chronic immune activation and systemic inflammation, which contribute to cardiovascular and renal risk. Specific antiretroviral agents and prolonged treatment exposure may further increase this risk, particularly in the context of comorbid conditions [33–38].
Summary of findings
This ML-NMR demonstrated that switching to or remaining on B/F/TAF resulted in a lipid profile that was largely comparable to other antiretroviral regimens, including those containing TDF, which is associated with lipid-lowering effects (Table 1). B/F/TAF showed a statistically significant decrease in triglyceride levels versus PI-based regimens and DTG/ABC/3TC, which may have important implications for long-term cardiovascular risk. Importantly, despite expectations of lipid increases when discontinuing TDF, switching to B/F/TAF did not lead to clinically meaningful worsening of lipid parameters. The TC/HDL ratio remained stable, LDL changes were negligible, and improvements in triglycerides were observed compared with select regimens (such as PI-based regimens and DTG/ABC/3TC), suggesting no adverse impact on overall cardiovascular risk profile. In addition to improvements in select lipid parameters, when switching from boosted regimens, there is a reduced potential for drug–drug interactions including with statins known to reduce cardiovascular risk. This makes B/F/TAF and DTG-based regimens suitable options for PWH who require statin therapy for cardiovascular prevention.
Moreover, independent of changes in lipids, there is increasing evidence linking ABC to adverse cardiovascular outcomes [39,40]. Recently, a secondary analysis of the REPRIEVE study demonstrated a significant increase in major adverse cardiovascular events with ABC-containing regimens compared with TAF-based regimens [41]. Reflecting this accumulating evidence, the US Department of Health and Human Services (US DHHS) and International Antiviral Society-USA (IAS-USA) guidelines removed DTG/ABC/3TC from the list of preferred ART for first-line therapy. Guidelines recommend avoiding, using with caution or otherwise switching from ABC in PWH with, or at high risk for cardiovascular disease [42,43].
In terms of renal outcomes, important for people aging with HIV, switching to B/F/TAF was associated with a statistically significant increase in eGFR versus DTG/ABC/3TC. While switching to PI-containing regimens showed statistically better results than B/F/TAF for CfB in eGFR, it is important to note that bictegravir (BIC), DTG, RPV and cobicistat all inhibit secretion of creatinine at the renal tubules. Specifically, BIC and DTG are known inhibitors of the renal organic cation transporter 2, which results in a benign increase in creatinine and corresponding reduction in eGFR rather than a clinically meaningful difference in overall glomerular filtration [44,45]. This interpretation is supported by iohexol-based studies, which suggest that changes in eGFR observed with INSTI-based regimens do not correspond to changes in measured GFR, indicating no substantial impact on true renal filtration capacity [46]. B/F/TAF is approved by the US FDA for use in adults and pediatric PWH with eGFR as low as 30 ml/min/1.73 m2, and is also indicated for switching in individuals on chronic dialysis, underscoring its established renal safety profile in populations with advanced kidney impairment [47].
Most studies included in these analyses were open-label, a design that tends to be associated with higher reporting rates of AEs and treatment discontinuations [48–50]. This is particularly evident in switch trials, where participants switching from a stable regimen to be more likely to report AEs or discontinue treatment compared with those remaining on their current regimen [50–53]. Despite this, switching to B/F/TAF resulted in a generally comparable AE profile versus all regimens (Table 2). Notably, B/F/TAF was associated with a statistically lower risk of nausea compared with DTG/ABC/3TC, and a statistically lower risk of overall TRAEs versus DTG/ABC/3TC. These findings were primarily driven by GS-US-380-1844, a double-blind study in which B/F/TAF was the switch arm, and DTG/ABC/3TC was the continue arm [16]. Additionally, switching to B/F/TAF was associated with a statistically lower risk of overall TRAEs versus CAB + RPV, which was largely driven by ISRs. Despite the potential for bias in the remaining switch arms of open-label trials across the network (CAB + RPV, DTG/ABC/3TC [in BESTT], EVG/c/F/TDF), switching to B/F/TAF did not generally result in a statistically significantly higher number of AEs or discontinuations compared with other ARTs in the network.
Regarding treatment discontinuation, B/F/TAF demonstrated a significantly lower risk of discontinuation due to AEs compared with CAB + RPV. However, it should be noted that inclusive in the discontinuations from CAB + RPV are ISRs. The SOLAR study investigated switching stable, VS PWH on B/F/TAF to CAB + RPV. Driven by ISRs, there were significantly more discontinuations, accounting for 20% of participants in the CAB + RPV arm, compared with less than 1% in the B/F/TAF arm. The RD in our analysis suggests the risk of discontinuation due to an AE is 9% lower when staying on B/F/TAF versus switching to CAB + RPV, driven by ISRs. These findings underscore the importance of considering ISRs when engaging patients in shared-decision making. Otherwise, all-cause discontinuation rates were generally similar across all other regimens, indicating comparable overall treatment persistence.
Strengths & limitations
This analysis has several strengths. First, it was informed by a comprehensive SLR and feasibility assessment. Outcome definitions were broadly aligned across included studies for most outcomes assessed, facilitating suitable cross-study comparisons. Furthermore, the network of evidence was well-connected, with all relevant comparators linking to B/F/TAF either directly or through a common comparator, allowing for comparisons across a wide range of regimens. A strength of this work was adjustment for key treatment effect modifying variables, addressing potential heterogeneity across trials. This involved comparing unadjusted (standard NMA) models to ML-NMR models adjusting for key baseline covariates (age, sex, race and CD4 cell count) and selecting the model with the best statistical fit. The general finding that several key long-term safety outcomes, including eGFR and most lipid parameters, required covariate adjustment underscores the importance of accounting for population differences when comparing the metabolic and renal effects of ART. Conversely, for other end points where the unadjusted model was preferred, such as discontinuation due to adverse events, this analysis suggests a more consistent treatment effect across different demographic subgroups.
However, some limitations should be acknowledged. Some heterogeneity was identified in the definitions of specific outcomes, notably CfB in eGFR. The BESTT study reported eGFR adjusted by total body surface area, while the SPARE study reported mean percentage change in eGFR. All studies reporting on CfB in eGFR reported this as derived according to the Cockcroft-Gault equation. The SOLAR study reported renal outcomes, but used cystatin C instead of serum creatinine or eGFR [20]. The number of studies contributing data for each outcome was modest, limiting the number of comparisons versus relevant ART, particularly for outcomes such as CfB in eGFR and overall TRAEs (each reported by four of eight studies), while lipid outcomes and nausea were reported by five studies, and grade 3/4 TEAEs and diarrhea by six studies. At last, while most treatment comparisons were informed by disaggregated regimen-specific data, some analyses used pooled treatment groups (e.g., pooled NNRTI as reported in BESTT and STRATEGY-NNRTI studies, and PI-based regimens as reported in SPARE and STRATEGY-PI studies) [25–27,54].
The inclusion of ‘pooled’ NNRTI and PI treatment arms as nodes in the network introduces additional heterogeneity, as individual agents within these classes differ in tolerability, drug–drug interaction potential and lipid and renal effects. For the pooled PI node, GS-US-380-1878 (which contributed to both the renal and lipid networks) specifically enrolled participants on ritonavir- or cobicistat-boosted atazanavir or darunavir plus either FTC/TDF or ABC/3TC. Atazanavir and darunavir differ in their lipid and renal profiles; notably, atazanavir is associated with a risk of nephrolithiasis and tubular effects, which could have influenced the eGFR outcomes observed in this arm [55]. For the lipid network, STRATEGY-PI also contributed to the pooled PI node but did not report the breakdown of individual PI agents within the ritonavir-boosted PI arm. For the pooled NNRTI node, the NNRTI composition was incompletely reported across contributing studies: in BESTT (which contributed to both the renal and lipid networks), efavirenz accounted for 59% of NNRTI use, with nevirapine (18%) and rilpivirine (23%) comprising the remainder at baseline, while STRATEGY-NNRTI, which contributed to the lipid network, included participants on various NNRTIs and stratified randomization by efavirenz use, suggesting efavirenz was the predominant agent, though the precise composition of the pooled treatment arm was not reported. Given the known lipid effects of efavirenz, including elevations in TC, LDL and triglycerides, compared with more lipid-neutral NNRTIs such as rilpivirine, the composition of this arm may have influenced the observed lipid comparisons [56,57]. To the extent that efavirenz was the predominant agent in this arm, its known effects of raising both TC and HDL simultaneously may explain the observed pattern whereby B/F/TAF showed significantly lower TC but a smaller HDL increase versus the pooled NNRTI comparator, with no significant difference in the TC/HDL ratio, suggesting no net adverse impact on cardiovascular risk profile from this comparison. While this pooling approach provides a broad perspective of B/F/TAF’s performance across the current treatment practice including established NNRTI and PI regimens, potential additional heterogeneity should be considered when interpreting class-level findings. As such, comparisons involving these groups may mask heterogeneity within the class and limit the ability to draw conclusions about individual agents.
A further limitation is the absence of established minimal clinically important differences for the continuous renal and lipid outcomes analyzed. This makes it challenging to definitively translate statistically significant between-group differences into a uniform measure of patient-level clinical impact. Our interpretation therefore relied on contextualizing the results within current clinical practice guidelines, which may vary by region and over time.
Finally, a limitation of this study is that the underlying SLR was completed in June 2023, while the present analyses and manuscript were finalized in 2025. Although this time gap could raise concerns regarding the currency of the evidence base, targeted horizon scans and review of trial registries through September 2025 did not identify any new Phase III or IV RCTs in TE PWH that would meaningfully alter the evidence network. The interval also reflects the extended timelines required for data access, cleaning and integration necessary for IPD-based ML-NMR analyses. Therefore, the findings are considered reflective of the contemporary treatment landscape and remain relevant for informing clinical decision-making.
As is common in network meta-analyses with a limited number of studies per treatment contrast, formal statistical assessment of reporting bias through funnel plots was not feasible; however, the included studies were all registered Phase III or IV RCTs, which reduces the likelihood of selective reporting. Additionally, the underlying SLR was restricted to English-language publications, which may have resulted in the exclusion of relevant studies published in other languages and could limit the global applicability of the findings.
Conclusion
Where comparisons involved pooled class-level nodes, specifically NNRTI- and PI-based regimens, findings should be interpreted at the class level and not extrapolated to individual agents, given known within-class differences in lipid effects, renal safety and tolerability. Regimen-specific comparisons (for example, B/F/TAF vs DTG/ABC/3TC and CAB + RPV) are more directly interpretable and represent the most robust conclusions of this analysis.
Collectively, these findings indicate that TE PWH who switch to or remain on B/F/TAF maintain a stable lipid profile and renal function, supporting its use as a cardiovascular and renally safe option for PWH. B/F/TAF also showed a generally similar tolerability profile compared with other ARTs assessed in this analysis, with more favorable adverse event outcomes versus CAB + RPV and DTG/ABC/3TC. Combined with its established long-term efficacy and safety profile, these data further support B/F/TAF as a well-tolerated option for TE PWH, supporting long-term treatment success.
Summary points
•
With modern antiretroviral therapy (ART), HIV-1 has become a manageable chronic condition, requiring careful consideration of long-term safety, tolerability and metabolic outcomes in treatment selection.
•
Among treatment-experienced (TE) people with HIV-1 (PWH), different ART regimens can have varying effects on metabolic and renal outcomes, including lipid levels, kidney function and adverse events such as nausea.
•
The aim of this systematic literature review (SLR) and multilevel network meta-regression (ML-NMR) was to compare the safety profile of B/F/TAF with other ART regimens in TE PWH, with emphasis on lipid parameters, renal function and overall safety outcomes.
•
A comprehensive search of MEDLINE, Embase, CDSR and CENTRAL databases was conducted in June 2023, supplemented by grey literature searches to identify Phase III/IV randomized controlled trials reporting safety outcomes in adult TE PWH.
•
ML-NMR analysis at week 48 utilized individual patient data from three Phase III B/F/TAF trials and aggregate data from comparator trials, with adjustments for age, sex and race.
•
At week 48, B/F/TAF showed comparable changes in total cholesterol to high-density lipoprotein ratio and low-density lipoprotein levels versus comparators, with favorable triglyceride changes compared with DTG/ABC/3TC and regimens containing protease inhibitors.
•
B/F/TAF demonstrated superior renal safety compared with DTG/ABC/3TC, with favorable changes in estimated glomerular filtration rate.
•
B/F/TAF was associated with statistically lower risks of nausea compared with DTG/ABC/3TC and fewer overall treatment-related adverse events compared with DTG/ABC/3TC and CAB + RPV.
•
Switching to or remaining on B/F/TAF in TE PWH showed favorable safety outcomes without worsening lipid or renal parameters, supporting its use as a safe and acceptable option for long-term HIV-1 management in treatment-experienced populations.
Author contributions
T Curteis, A Karlsson, H Luedke, BG Patel, N Unger, U Mordi, J Jarrett, M Chen contributed to study design. H Luedke, AM Khalsa, M Rubinstein, M Hempfling, J Gurney contributed to acquisition of data. A Karlsson, M Rubinstein, M Hempfling, J Gurney, T Curteis contributed to the analysis of data. All authors contributed to the interpretation of data. T Curteis, LA Eddowes, A Karlsson, H Luedke, M Rubinstein, M Hempfling, J Gurney contributed to drafting the article or revising it critically for important intellectual content. All authors contributed to the final approval of the version of the article to be published.
Acknowledgments
The authors thank Ania Bobrowska (formerly of Costello Medical, Cambridge, UK) for leading the SLR and Katherine Massey (Costello Medical, Singapore) for supporting the clinical interpretation of the findings.
Financial disclosure
This study was funded by Gilead Sciences, Inc. (CA, USA).
Competing interests disclosure
M Chen, U Mordi, BG Patel, J Jarrett, N Unger are employees and shareholders of Gilead Sciences, Inc. T Curteis, LA Eddowes, A Karlsson, H Luedke, M Rubinstein, M Hempfling, J Gurney are employees of Costello Medical, which was funded by Gilead Sciences, Inc. to conduct the study. EM Sherman has no conflict of interest to report. MS McKellar reports research grants to her institution from Gilead Sciences, Inc., and ViiV Healthcare. A Lipps has no conflict of interest to report. K Mounzer reports payment or honoraria for lectures, presentations, speakers' bureaus, and manuscript writing from Gilead Sciences, Inc., Janssen Therapeutics, ViiV Healthcare and Epividian/Merck. AM Khalsa reports consulting fees and payment or honoraria from Gilead Sciences, Inc. WL Dinges reports consulting fees from Gilead Sciences, Inc.; payments to his institution (Seattle Infectious Disease Clinic, SIDC) for HIV and PrEP advisory boards; honoraria from Gilead Sciences, Inc.; payment for expert legal case review (paid to SIDC); patents planned, issued, or pending (no payments or financial gain to date); unpaid advisory board role at Lumen Bioscience with unexercised stock options; receipt of medication samples of Biktarvy and Descovy from Gilead Sciences, Inc., and Cabenuva from ViiV Healthcare for patient use via SIDC; and ownership of Seattle Infectious Disease Clinic. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing disclosure
Medical writing support was provided by Eesha Dinkar of Costello Medical, Cambridge, UK, and was funded by Gilead Sciences, Inc.
Data sharing statement
The authors certify that this manuscript reports the secondary analysis of clinical trial data that have been shared with them, and that the use of this shared data is in accordance with the terms (if any) agreed upon their receipt. The source of this data is: BESTT, GS-US-380-1844 (OVERRIDE, NCT02603120), GS-US-380-1878 (NCT02603107), GS-US-380-4030 (NCT03110380), SOLAR (NCT04542070), SPARE (NCT01294761), STRATEGY-NNRTI (NCT01495702), STRATEGY-PI (NCT01475838). The individual patient data used in this analysis were obtained from clinical trials sponsored by Gilead Sciences, Inc. and are not publicly available. Aggregate-level results presented in this manuscript are available within the article and its supplementary materials.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary material.pdf)
- Download
- 607.50 KB
References
Papers of special note have been highlighted as: •• of considerable interest
1.
Adam Trickey MTM, Jorg-Janne Vehreschild, Niels Obel et al. Survival of HIV-positive patients starting antiretroviral therapy between 1996 and 2013: a collaborative analysis of cohort studies. Lancet HIV 4(8), e349–e356 (2017).
2.
Trickey A, Sabin CA, Burkholder G et al. Life expectancy after 2015 of adults with HIV on long-term antiretroviral therapy in Europe and North America: a collaborative analysis of cohort studies. Lancet HIV 10(5), e295–e307 (2023).
3.
Deeks SG, Lewin SR, Havlir DV. The end of AIDS: HIV infection as a chronic disease. Lancet 382(9903), 1525–1533 (2013).
4.
Smit M, Brinkman K, Geerlings S et al. Future challenges for clinical care of an ageing population infected with HIV: a modelling study. Lancet Infect. Dis. 15(7), 810–818 (2015).
5.
Sossen B, Kubjane M, Meintjes G. Tuberculosis and HIV coinfection: progress and challenges towards reducing incidence and mortality. Int. J. Infect. Dis. 155, 107876 (2025).
6.
Mocellin LP, Ziegelmann PK, Kuchenbecker R. A systematic review and meta-analysis assessing antiretroviral therapy for treatment-experienced HIV adult patients using an optimized background therapy approach: is there evidence enough for a standardized third-line strategy? Syst. Rev. 11(1), 243 (2022).
7.
Cutrell J, Jodlowski T, Bedimo R. The management of treatment-experienced HIV patients (including virologic failure and switches). Ther. Adv. Infect. Dis. 7, 2049936120901395 (2020).
8.
Edelman EJ, Rentsch CT, Justice AC. Polypharmacy in HIV: recent insights and future directions. Curr. Opin. HIV AIDS 15(2), 126–133 (2020).
9.
Ambrosioni J, Levi LI, Alagaratnam J et al; EACS Governing Board. Major revision version 13.0 of the European AIDS Clinical Society guidelines 2025. HIV Med. 27(1), 18–32 (2026).
10.
Ambrosioni J, Levi L, Alagaratnam J et al. Major revision version 12.0 of the European AIDS Clinical Society guidelines 2023. HIV Med. 24(11), 1126–1136 (2023).
11.
Castro-Gonzalez S, Colomer-Lluch M, Serra-Moreno R. Barriers for HIV cure: the latent reservoir. AIDS Res. Hum. Retroviruses 34(9), 739–759 (2018).
12.
Waters L, Winston A, Reeves I et al. BHIVA guidelines on antiretroviral treatment for adults living with HIV-1 2022. HIV Med. 23(Suppl. 5), 3–115 (2022).
13.
Legarth RA, Ahlström MG, Kronborg G et al. Long-term mortality in HIV-infected individuals 50 years or older: a nationwide, population-based cohort study. J. Acquir. Immune Defic. Syndr. 71(2), 213–218 (2016).
14.
Gallant J, Lazzarin A, Mills A et al. Bictegravir, emtricitabine, and tenofovir alafenamide versus dolutegravir, abacavir, and lamivudine for initial treatment of HIV-1 infection (GS-US-380-1489): a double-blind, multicentre, phase 3, randomised controlled non-inferiority trial. Lancet 390(10107), 2063–2072 (2017).
15.
Sax PE, Rockstroh J, Luetkemeyer A et al. Switching to a single-tablet regimen bictegravir, emtricitabine, and tenofovir alafenamide (B/F/TAF) from dolutegravir (DTG) plus emtricitabine and either tenofovir alafenamide or tenofovir disoproxil fumarate (F/TAF or F/TDF). J. Int. AIDS Soc. 22(Suppl. 5), e25327 Abstract MOAB0105 (2019).
16.
Brar I, Ruane PJ, Berhe M et al. Efficacy and safety of switch to bictegravir/emtricitabine/tenofovir alafenamide from dolutegravir/abacavir/lamivudine: results from an open-label extension of a Phase III randomized, double-blind, multicenter, active-controlled, non-inferiority study. Medicine (Baltimore) 104(8), e41482 (2025).
17.
Daar ES, DeJesus E, Ruane P et al. Efficacy and safety of switching to fixed-dose bictegravir, emtricitabine, and tenofovir alafenamide from boosted protease inhibitor-based regimens in virologically suppressed adults with HIV-1: 48 week results of a randomised, open-label, multicentre, Phase III, non-inferiority trial. Lancet HIV 5(7), e347–e356 (2018).
•• One of the pivotal trials that compared B/F/TAF to other antiretroviral therapy (ART) regimens in the treatment-experienced (TE) population.
18.
Rieke A, De Wet J, Esposito V et al. Real-world effectiveness and tolerability of bictegravir/emtricitabine/tenofovir alafenamide (B/F/TAF) in treatment-experienced (TE) people with HIV with a history of CKD: TH-PO1072. J. Am. Soc. Nephrol. 34(Suppl. 11), 392–393 (2023).
19.
Sax PE, Rockstroh JK, Luetkemeyer AF et al. Switching to bictegravir, emtricitabine, and tenofovir alafenamide in virologically suppressed adults with human immunodeficiency virus. Clin. Infect. Dis. 73(2), e485–e493 (2021).
•• One of the pivotal trials that compared B/F/TAF to other ART regimens in the TE population.
20.
Ramgopal MN, Castagna A, Cazanave C et al. Efficacy, safety, and tolerability of switching to long-acting cabotegravir plus rilpivirine versus continuing fixed-dose bictegravir, emtricitabine, and tenofovir alafenamide in virologically suppressed adults with HIV, 12-month results (SOLAR): a randomised, open-label, Phase IIIb, non-inferiority trial. Lancet HIV 10(9), e566–e577 (2023).
21.
Higgins J, Thomas J, Chandler J et al. Cochrane handbook for systematic reviews of interventions version 6.3 (updated February 2022). https://training.cochrane.org/handbook
22.
Sterne JAC, Savović J, Page MJ et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ 366, l4898 (2019).
23.
Paudel M, Prajapati G, Buysman EK et al. Comorbidity and polypharmacy among people with HIV stratified by age, sex, and race. HIV Res. Clin. Pract. 25(1), 2361176 (2024).
24.
Cescon A, Patterson S, Chan K et al. Gender differences in clinical outcomes among HIV-positive individuals on antiretroviral therapy in Canada: a multisite cohort study. PloS One 8(12), e83649 (2013).
25.
Arribas JR, Pialoux G, Gathe J et al. Simplification to coformulated elvitegravir, cobicistat, emtricitabine, and tenofovir versus continuation of ritonavir-boosted protease inhibitor with emtricitabine and tenofovir in adults with virologically suppressed HIV (STRATEGY-PI): 48 week results of a randomised, open-label, Phase IIIb, non-inferiority trial. Lancet Infect. Dis. 14(7), 581–589 (2014).
26.
Ibrahim F, Samarawickrama A, Hamzah L et al. Bone mineral density, kidney function, weight gain and insulin resistance in women who switch from TDF/FTC/NNRTI to ABC/3TC/DTG. HIV Med. 22(2), 83–91 (2021).
27.
Nishijima T, Gatanaga H, Shimbo T et al. Switching tenofovir/emtricitabine plus lopinavir/r to raltegravir plus darunavir/r in patients with suppressed viral load did not result in improvement of renal function but could sustain viral suppression: a randomized multicenter trial. PLoS One 8(8), e73639 (2013).
28.
Higgins JP, Li T, Deeks JJ. Choosing effect measures and computing estimates of effect. In: Cochrane Handbook for Systematic Reviews of Interventions. Higgins JPT, Thomas J, Chandler Jet al. et al. (Eds). (2019) https://doi.org/10.1002/9781119536604.ch6
29.
Phillippo DM, Dias S, Ades AE et al. Multilevel network meta-regression for population-adjusted treatment comparisons. J. R. Stat. Soc. Ser. A Stat. Soc. 183(3), 1189–1210 (2020).
30.
Carpenter B, Gelman A, Hoffman MD et al. Stan: a probabilistic programming language. J. Stat. Software 76, 1–32 (2017).
31.
Phillippo DM. multinma: bayesian network meta-analysis of individual and aggregate data. R package version 0.7.0. doi: (2024). (Epub ahead of print).
32.
Molina JM, Ward D, Brar I et al. Switching to fixed-dose bictegravir, emtricitabine, and tenofovir alafenamide from dolutegravir plus abacavir and lamivudine in virologically suppressed adults with HIV-1: 48 week results of a randomised, double-blind, multicentre, active-controlled, Phase III, non-inferiority trial. Lancet HIV 5(7), e357–e365 (2018).
•• One of the pivotal trials that compared B/F/TAF to other ART regimens in the TE population.
33.
Freiberg MS, Chang CH, Skanderson M et al. Association between HIV infection and the risk of heart failure with reduced ejection fraction and preserved ejection fraction in the antiretroviral therapy era: results from the veterans aging cohort study. JAMA Cardiol. 2(5), 536–546 (2017).
34.
Opravil M, Sereni D. Natural history of HIV-associated pulmonary arterial hypertension: trends in the HAART era. AIDS 22(Suppl. 3), S35–S40 (2008).
35.
Chow FC, Regan S, Feske S, Meigs JB, Grinspoon SK, Triant VA. Comparison of ischemic stroke incidence in HIV-infected and non-HIV-infected patients in a US health care system. J. Acquir. Immune Defic. Syndr. 60(4), 351–358 (2012).
36.
Feinstein MJ, Steverson AB, Ning H et al. Adjudicated heart failure in HIV-infected and uninfected men and women. J. Am. Heart Assoc. 7(21), e009985 (2018).
37.
Chawla A, Wang C, Patton C et al. A review of long-term toxicity of antiretroviral treatment regimens and implications for an aging population. Infect. Dis. Ther. 7(2), 183–195 (2018).
38.
Mocroft A, Lundgren JD, Ross M et al. Cumulative and current exposure to potentially nephrotoxic antiretrovirals and development of chronic kidney disease in HIV-positive individuals with a normal baseline estimated glomerular filtration rate: a prospective international cohort study. Lancet HIV 3(1), e23–e32 (2016).
39.
Dorjee K, Choden T, Baxi SM, Steinmaus C, Reingold AL. Risk of cardiovascular disease associated with exposure to abacavir among individuals with HIV: a systematic review and meta-analyses of results from 17 epidemiologic studies. Int. J. Antimicrob. Agents 52(5), 541–553 (2018).
40.
Nan C, Shaefer M, Urbaityte R et al. Abacavir use and risk for myocardial infarction and cardiovascular events: pooled analysis of data from clinical trials. Open Forum Infect. Dis. 5(5), ofy086 (2018).
41.
Davies Smith E, Malvestutto C, Ribaudo HJ et al. Cardiovascular hazards of abacavir- versus tenofovir-containing antiretroviral therapies: insights from an analysis of the REPRIEVE trial cohort. Open Forum Infect. Dis. 12(4), ofaf177 (2025).
42.
Gandhi RT, Landovitz RJ, Sax PE et al. Antiretroviral drugs for treatment and prevention of HIV in adults: 2024 recommendations of the international antiviral society–USA panel. JAMA 333(7), 609–628 (2025).
43.
Panel on antiretroviral guidelines for adults and adolescents. Guidelines for the use of antiretroviral agents in adults and adolescents with HIV. Department of Health and Human Services. (2025). Available at: https://clinicalinfo.hiv.gov/en/guidelines/hiv-clinical-guidelines-adult-and-adolescent-arv/whats-new
44.
Koteff J, Borland J, Chen S et al. A Phase I study to evaluate the effect of dolutegravir on renal function via measurement of iohexol and para-aminohippurate clearance in healthy subjects. Br. J. Clin. Pharmacol. 75(4), 990–996 (2013).
45.
Yombi JC, Pozniak A, Boffito M et al. Antiretrovirals and the kidney in current clinical practice: renal pharmacokinetics, alterations of renal function and renal toxicity. AIDS 28(5), 621–632 (2014).
46.
Margolick JB, Jacobson LP, Schwartz GJ et al. Factors affecting glomerular filtration rate, as measured by iohexol disappearance, in men with or at risk for HIV infection. PloS One 9(2), e86311 (2014).
47.
Eron JJ, Ramgopal M, Osiyemi O et al. Bictegravir/emtricitabine/tenofovir alafenamide in adults with HIV-1 and end-stage kidney disease on chronic haemodialysis. HIV Med. 26(2), 302–307 (2025).
48.
Bakalos G, Zintzaras E. Drug discontinuation in studies including a switch from an originator to a biosimilar monoclonal antibody: a systematic literature review. Clin. Therapeut. 41(1), 155–173.e113 (2019).
49.
Mouillet GA-O, Efficace FA-O, Thiery-Vuillemin A et al. Investigating the impact of open label design on patient-reported outcome results in prostate cancer randomized controlled trials. Cancer Med. 9(20), 7363–7374 (2020).
50.
Rolle CA-O, Castano J, Nguyen V, Hinestrosa FA-O, DeJesus E. Efficacy, safety, and tolerability of switching from bictegravir/emtricitabine/tenofovir alafenamide to dolutegravir/lamivudine among adults with virologically suppressed HIV: the DYAD study. Open Forum Infect. Dis. 11(10), ofae560 (2024).
51.
Osiyemi O, De Wit S, Ajana F et al. Efficacy and safety of switching to dolutegravir/lamivudine versus continuing a tenofovir alafenamide-based 3- or 4-drug regimen for maintenance of virologic suppression in adults living with human immunodeficiency virus type 1: results through week 144 from the Phase III, noninferiority TANGO randomized trial. Clin. Infect. Dis. 75(6), 975–986 (2022).
52.
Llibre JM, Brites C, Cheng CY et al. Efficacy and safety of switching to the 2-drug regimen dolutegravir/lamivudine versus continuing a 3- or 4-drug regimen for maintaining virologic suppression in adults living with human immunodeficiency virus 1 (HIV-1): week 48 results from the Phase III, noninferiority SALSA randomized Trial. Clin. Infect. Dis. 76(4), 720–729 (2023).
53.
Aboud M, Orkin C, Podzamczer D et al. Efficacy and safety of dolutegravir-rilpivirine for maintenance of virological suppression in adults with HIV-1: 100-week data from the randomised, open-label, Phase III SWORD-1 and SWORD-2 studies. Lancet HIV 6(9), e576–e587 (2019).
54.
Pozniak A, Markowitz M, Mills A et al. Switching to coformulated elvitegravir, cobicistat, emtricitabine, and tenofovir versus continuation of non-nucleoside reverse transcriptase inhibitor with emtricitabine and tenofovir in virologically suppressed adults with HIV (STRATEGY-NNRTI): 48 week results of a randomised, open-label, Phase IIIb non-inferiority trial. Lancet Infect. Dis. 14(7), 590–599 (2014).
55.
Lafaurie M, De Sousa B, Ponscarme D et al. Clinical features and risk factors for atazanavir (ATV)-associated urolithiasis: a case-control study. PLoS One 9(11), e112836 (2014).
56.
Dave JA, Lambert EV, Badri M, West S, Maartens G, Levitt NS. Effect of nonnucleoside reverse transcriptase inhibitor–based antiretroviral therapy on dysglycemia and insulin sensitivity in South African HIV-infected patients. J. Acquir. Immune Defic. Syndr. 57(4), 284–289 (2011).
57.
Karen TT, Linda B, Elizabeth A, Esther A, Timothy PF. Lipid changes in patients initiating efavirenz-and indinavir-based antiretroviral regimens. HIV Clin. Trials 4(1), 29–36 (2003).
Information & Authors
Information
Published In
Copyright
© 2026 Gilead Sciences Inc. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 20 January 2026
Accepted: 22 April 2026
Published online: 28 May 2026
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Comparative safety of B/F/TAF versus other antiretroviral therapy regimens for treatment-experienced people with HIV-1: a systematic literature review and network meta-analysis. (2026) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2026-0013
Export citation
Select the citation format you wish to export for this article or chapter.