Estimating the societal impact of medical interventions: a case study in metastatic breast cancer
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Additional value elements like productivity are currently rarely included in economic evaluations since quantitative assessment may be complex or lack clear guidance. In this study we present a practical framework for estimating the societal impact of medical interventions by incorporating additional value elements into economic evaluations. Materials & methods: We applied this framework in the case of trastuzumab deruxtecan (T-DXd) for patients with metastatic breast cancer in five European countries (EU5). In this study we considered the following elements: productivity losses in paid and unpaid work, quality-adjusted life years (QALYs) valued at willingness-to-pay thresholds, the impact on childcare responsibilities, costs associated with formal caregivers, the effect on informal caregivers and impact on governmental accounts including tax revenue, pension and disability benefits. Results: Our findings indicated that some of the value elements included may lead to a positive societal value for the intervention, while others may result in additional costs. Positive impacts were seen in gains to patient productivity (€589 million), QALYs (€1.7 billion), unpaid work (€259 million), childcare responsibilities (€5 million) and tax revenue (€165 million). Conversely, our findings highlighted a greater demand for formal and informal care (-€29 million and -€7 million, respectively) and increased public spending on disability benefits (-€380 million) and pensions (-€44 million) attributed to T-DXd. The main causes of increased costs were the improvement in progression-free and overall survival achieved with T-DXd. Conclusion: Overall, this framework aims to quantify the societal value of new healthcare interventions. This metastatic breast cancer case study illustrates how key value elements can be integrated into economic evaluations, beyond the classical cost–effectiveness analysis, to further support reimbursement decisions.
Plain language summary
What is this article about?
Current economic evaluations typically focus on clinical end points and direct medical costs. This research introduces a scalable framework, serving as a user guide for evaluating broader value elements. Specifically, this analysis presents six additional value elements that could be integrated into economic evaluations expanding the economic perspective toward a broader definition of value generated by innovative health interventions.
What methodology is described
The proposed framework outlines the calculation steps needed to include selected value elements into economic evaluations. It provides guidance on assessing patient productivity effects, economic impact for formal and informal caregivers, and the fiscal impacts on government accounts.
Why is this important?
The analysis contributes to ongoing discussions about incorporating broader value components into economic evaluations. Positioning this research as a user guide may serve as a foundation for future assessments of additional value elements.
In recent years, advances in clinical practice and the introduction of innovative health interventions have led to improved clinical outcomes. However, these innovations often come with increased expenditure. To manage these additional costs, decision-makers are relying on health and economic evaluation frameworks of such products [1]. This process primarily focuses on the classical health technology assessment (HTA) procedure, which aims to provide evidence for regulatory approval and reimbursement of healthcare interventions. While the primary HTA focus is on evaluating the impact of interventions on health outcomes and direct costs, several stakeholders prefer to adopt a broader societal perspective [2], by including elements such as, patient productivity, spillover effects in the family, value of hope, etc. According to a systematic review, productivity losses of patients and caregivers are the most frequently captured value elements [2,3].
Additionally, methodological approaches such as the Health Impact Assessment and the Social Return on Investment [4], have been developed to include broader societal value of health interventions. Unlike established practices, these approaches extend their evaluation beyond clinical outcomes and direct costs [4], in domains such as social participation, caregiving, mental well-being and other indirect consequences of disease and treatment. Moreover, the 2018 ISPOR (The Professional Society for Health Economics and Outcomes Research) Special Task Force Report introduced the concept of ‘value flower’. The ‘value flower’ represents a well-established framework that includes eight additional value elements, aiming to complement traditional HTA outcomes such as quality-adjusted life years (QALYs) and direct medical costs [3]. Although the ‘value flower’ framework has influenced public discussion, it has not been widely adopted in the decision-making process. Researchers have argued that the true value of healthcare interventions could be more accurately captured by considering this broader evaluation approach [5], yet empirical studies that include these elements remains scarce [6]. This literature gap suggests a need to establish a transparent methodology for capturing such elements to facilitate broader decision-making use beyond the academic setting.
Further, recognizing this need and building on previous research, Shafrin et al. [1] implemented the generalized cost–effectiveness analysis (GCEA) approach to overcome several key limitations of traditional CEAs. GCEA offers a structured and transparent research tool for capturing a wide range of costs and benefits associated with innovative healthcare technologies, especially those that matter to patients and caregivers from a societal perspective. Specifically, the authors assessed 15 value elements and incorporated those into four wider value categories namely: uncertainty (e.g., disease risk reduction, value of knowing), dynamics (e.g., dynamic prevalence and scientific spillover), beneficiary (e.g., equity and family spillover), and additionally value elements (e.g., productivity and community spillovers). Overall, GCEA offers a promising foundation toward wider integration of additional value elements in CEAs to account for a variety of potential components that may influence patient's health and society as a whole in the short- or the long-term. Nevertheless, Shafrin et al. [1], also recognized limitations associated with such a broad assessment. However, they highlighted that the potential limitations and associated assumptions should not prevent the incorporation and adoption of the petals of the proposed ‘value flower’ (i.e., the elements in each petal of the ‘value flower’ this research proposed).
Breast cancer (BC) is the most prevalent cancer, with 7.8 million women diagnosed between 2015 and 2020 [7]. It affects women globally with higher risk in later life, being more prevalent in the age group 45–69 years [8]. Incidence trends in the European Union (EU) are rising, possibly due to factors like reproductive changes, obesity, physical inactivity and increased screening [9]. The mortality rate of BC is 16%, surpassing lung (14%) and colorectal cancer (13%) [9]. Additionally, BC is associated with significant socio-economic impact, resulting in €15 billion annual costs in the EU, which represent the 12% of all cancer expenses [10]. Considering the healthcare costs alone (e.g., primary care, inpatient/outpatient care, emergency care and drugs), the total annual EU expenditure reaches €6.73 billion [10,11]. Finally, BC mortality contributes to a total cost of €6.9 billion in Europe, making it the second most expensive cancer in terms of premature death among the 24 common cancers [12].
T-DXd is a recently approved treatment for human epidermal growth factor receptor 2 (HER2)-low and HER2-positive mBC who had previously received chemotherapy. The purpose of this case study was to apply a societal impact evaluation to estimate the societal implications of introducing T-DXd to treat mBC patients.
Expanding on the aforementioned research, the present study aims to establish a methodological approach that can serve as a practical user guide to quantify key societal value elements. By positioning this study as a methodological guide, the focus is on developing a reproducible and pragmatic framework that can be applied into multiple contexts, i.e., different diseases, countries and diverse patient populations. Thus, the aim is to assist researchers, policymakers and other stakeholders to adopt a broader perspective when evaluating healthcare interventions and not strictly focusing on clinical outcomes and direct costs such as drug prices.
To illustrate the practical application of the proposed framework, we conducted a case study to assess the societal impact of T-DXd in patients with HER2-low and HER2-positive metastatic breast cancer (mBC) who had previously received chemotherapy, compared with standard of care (SOC) alone. In this context, we considered the societal effects experienced by patients, their caregivers and society. The analysis was performed for the UK, Germany, France, Spain and Italy allowing us to capture the effects in multiple contexts, while testing the flexibility and adaptability of this framework in different countries.
Materials & methods
We developed a comprehensive framework to assess the societal value of a new medicine that incorporates several elements from the ISPOR ‘value flower’ as well as additional, societally relevant value dimensions. In line with the value flower, our analysis quantified QALYs, paid and unpaid work productivity, caregiver burden and includes additional governmental effects. However, the value elements we included build on, but are not identical to those proposed in previous research [1,3]. For example, the governmental impact of health interventions was not described or included in the aforementioned research, but we chose to incorporate it into this study. We choose to include the fiscal impact of interventions because health innovations may influence public finances, for example, through changes in tax revenue, and social transfers, making the evaluation of such effect relevant when considering the wider societal value framework. Additionally, only value elements with available empirical evidence for quantification were included (Figure 1), to ensure methodological robustness.
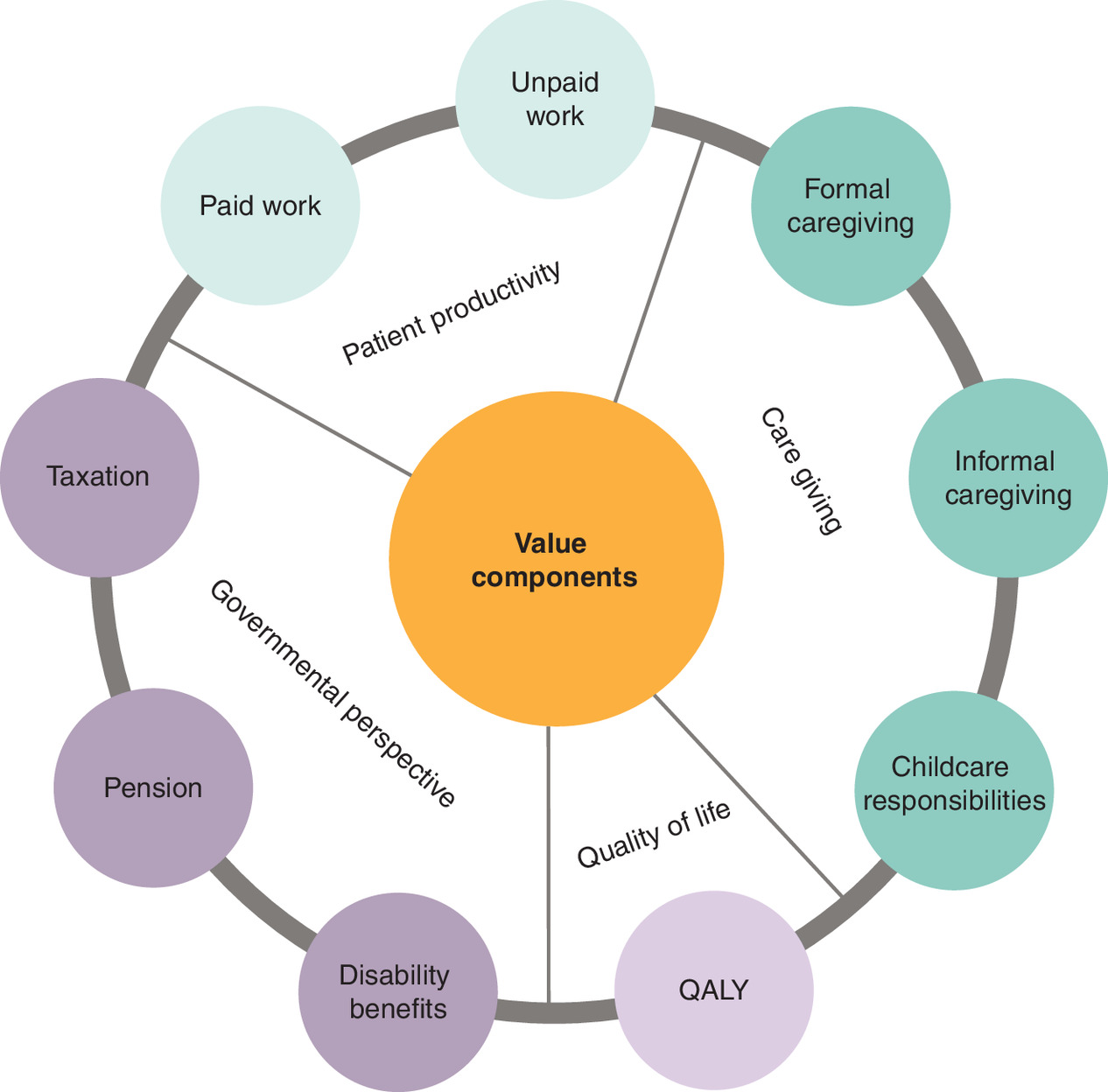
Figure 1. Societal value elements included in our analysis.
Paid work: reflects the ability of patients to participate in the workforce. Treatment effectiveness can influence productivity impairment due to disease. Unpaid work: captures non-market activities such as household tasks, volunteering and community engagement that may be affected by illness and treatment. Formal caregiving: includes professional care services, which may be required when a patient’s health deteriorates. Informal caregiving: represents care provided by family members or friends, often unpaid, which has economic implications such as lost work hours. Childcare responsibilities: reflects the impact on parents or guardians with dependent children, considering potential disruptions in their ability to care for their families due to illness or treatment. QALY: a common metric used in health economic evaluations to assess the impact of a treatment on both the length and quality of life. Disability benefits: costs associated with social support for patients unable to work due to illness or disability. Pension: financial implications for government pension systems if patients retire earlier due to illness. Taxation: loss of tax revenue due to reduced workforce participation and decreased earnings.
QALY: Quality-adjusted life years.
As such, some value elements suggested in the classical ‘value flower’ have not been incorporated in our analysis, due to methodological constraints (i.e., lack of empirical evidence [6] and difficulties in quantification [13]). Specifically, the excluded elements are the value of hope, the value of knowing, the real option value, the insurance value, the severity of disease, equity, fear of contagion and scientific spillovers. Furthermore, in this study we did not evaluate the direct medical costs as these are usually extensively evaluated in other economic analysis, (i.e., cost–effectiveness evaluations) [14].
Case study: societal value of a treatment for mBC
We developed a model consisting of the following health states: progression free survival (PFS), post-progression survival and death (Figure 2). Evidence around comparators and health states, were derived from cost–effectiveness models (CEMs) of T-DXd in mBC patients [15,16]. The hypothetical cohort was defined to represent metastatic cancer patients eligible for T-DXd. Model inputs were derived from published literature. Specifically, patients with HER2-low and HER2-positive mBC who had previously received chemotherapy were modeled based on evidence derived from the DESTINY-Breast04 and DESTINY-Breast03 trials, respectively [17,18]. These clinical trials were selected for this exemplary case study based on their relevance to the intervention of interest, and their provision of key clinical end points such as PFS. The SOC consisted of the comparators in the respective clinical trials (refer to as counterfactual scenario). The model followed the progression of five incident cohorts from treatment initiation to lifetime. Each cohort was entered in successive years from 2023 to 2027. We chose five cohorts to mitigate the potential impact of changes in socioeconomic circumstances in the long term and evolving clinical practices. We implemented a hypothetical scenario based on the assumption of 100% market share for T-DXd versus 100% market share of SOC. This assumption represents the maximum health and societal impact for eligible patients.
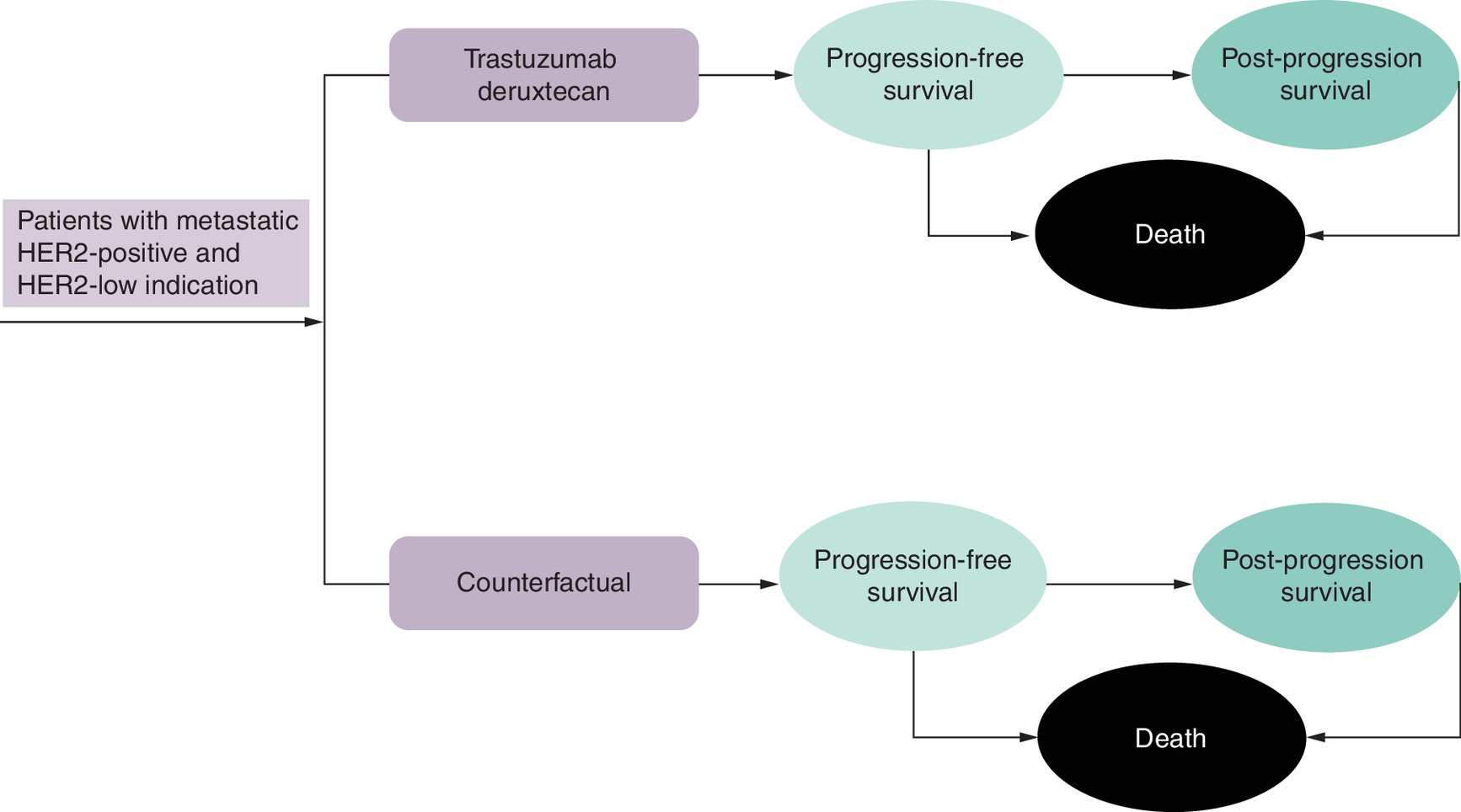
Figure 2. Modeling framework.
The model considers three core health states for both treatment arms: progression-free survival, post-progression survival and death.
HER2: Human epidermal growth factor receptor 2.
To estimate the patient population at the start of each year, we considered BC incidence [19] (Appendices, Supplementary Table 1). To restrict our population to mBC only, we assumed a mBC prevalence of 7.39% [20]. Subsequently we multiplied the result by 50% for HER2-low [21], and by 20% for HER2-positive patients [22]. We assumed a consistent median age of diagnosis, at 55 years [17,18], which likely represents a conservative approach. Extrapolated survival probabilities derived from previously developed CEMs were used to determine the number of patients in each cohort with no disease progression, those with disease progression, and those who died during each annual model cycle (Figure 3). In the underlying CEMs, survival beyond trial follow-up was extrapolated using standard parametric survival functions, with model selection informed by statistical goodness-of-fit criteria and clinical plausibility. Both health and monetary outcomes were discounted using a discount rate of 3.5% [23,24].
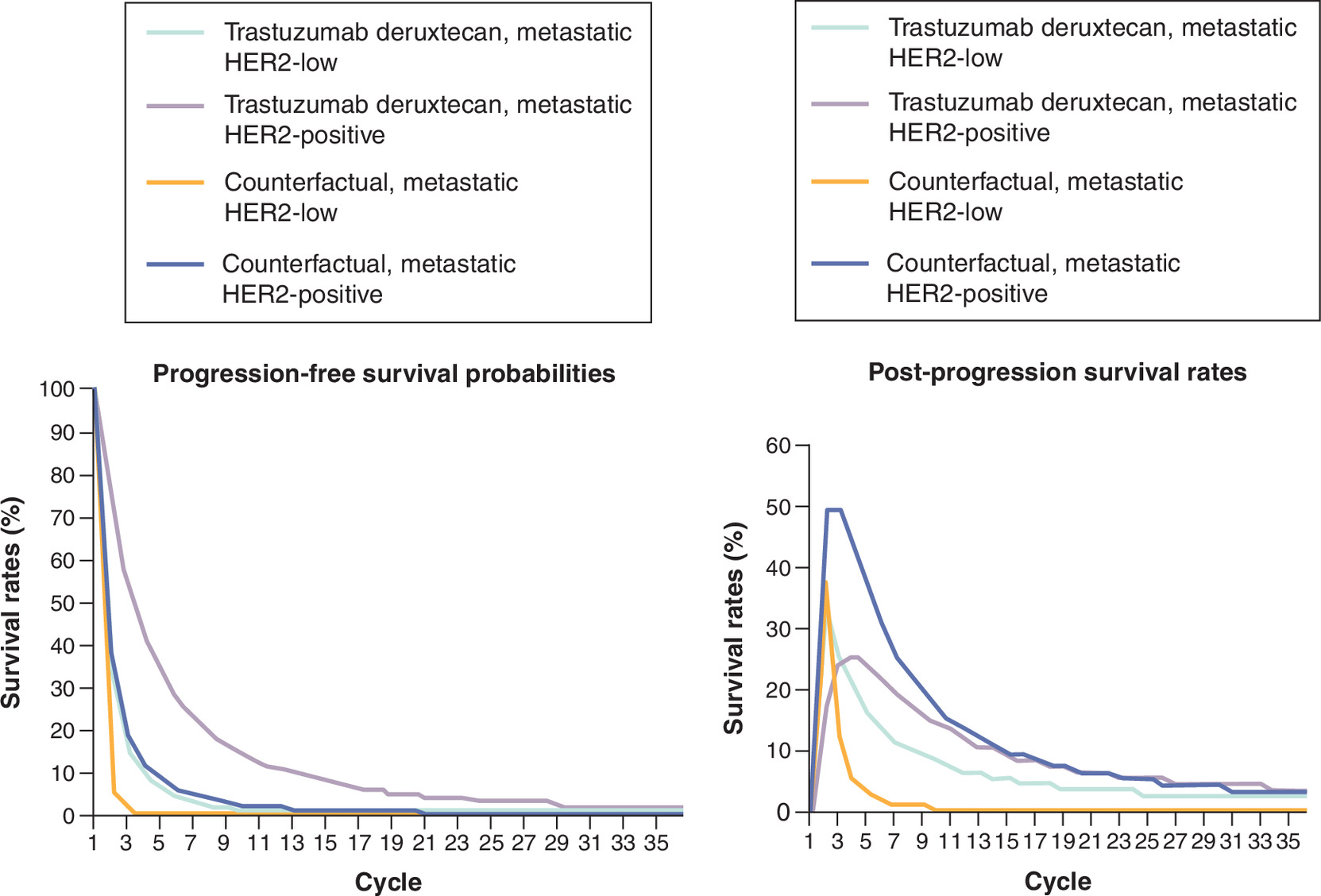
Figure 3. Progression-free and post progression survival rates of trastuzumab deruxtecan (T-DXd) and counterfactual treatment scenarios.
The progression-free survival graph starts at 100% because the model assumes that all patients are initially progression-free. Over time, the progression-free curve shows the decreasing probability of remaining in this state. In contrast, the post-progression survival curve starts at 0%, reflecting that no patients are in the post-progression state at the start of the analysis. In subsequent cycles, the post-progression survival curve initially shows an increasing trend as patients move from progression-free to post-progression. Eventually, the curve declines due to the decreasing proportion of patients remaining in the progression-free state.
HER2: Human epidermal growth factor receptor 2.
Estimating the societal impact
The societal value components presented in Figure 1 were evaluated using the following approaches:
Patient paid & unpaid productivity
The evaluation of both paid and unpaid productivity losses is a key element distinguishing economic evaluations based solely on the healthcare perspective from those adopting a broader societal perspective. Productivity losses resulting from ill health – or avoided losses due to improved health outcomes attributed to innovative treatments – provide insights into how health interventions impact not only the individual patient but also the wider economy. This consideration is particularly important in the context of chronic and life-threatening conditions, such as mBC, especially when they affect individuals of working age who contribute substantially to economic productivity.
In our case study, to estimate the paid and unpaid consequences attributed to T-DXd, we employed a methodology consistent with prior cancer research [25]. Specifically, we translated the incremental difference in PFS into reductions in both paid and unpaid productivity losses. This approach assumes that more time spent in PFS is associated with increased capacity to participate in the labor force.
To implement this, we controlled for patients’ employment status at diagnosis, likelihood of returning to work and work-related impairments due to mBC [26–28], as cancer patients may experience impaired health post-treatment (Appendices, Supplementary Table 2) [29]. Available evidence suggests a short-term reduction in work ability for approximately 2 years followed by a return to work [29]. Thus, we assumed that mBC cancer patients returning to the workforce will experience health-related limitations for 2 years. Additionally, we assumed that patients participate in paid work until the official retirement age in each EU5 [30–34]. The avoided paid productivity losses was monetized using gross value added (GVA) (Appendices, Supplementary Table 3), aligned with previous literature [35–37]. GVA serves as an economic indicator describing the value of produced goods in an industry or sector of economy. In this metric, only the added value created in the production process is included [38]. Thus, the patient productivity impact was determined as per the formula below:
(Equation 1)
where j represents low or positive mBC patients, t the cycle, ER is the employment rate, WI is work impairment and RTW is the return-to-work rate.
Unpaid work was defined according to the third-person criterion [39,40]. In this context, unpaid work includes any non-market activity that could be substituted by another individual. This distinction allows for differentiation between unpaid work, such as household activities, cooking, cleaning etc., from leisure time which is not associated with economic value creation. Information on the included unpaid activities are presented in the Appendices, Supplementary Table 4 [41,42]. In our approach we assumed that patients who returned to work were also capable of engaging in unpaid work as well. However, we excluded the probability of working at the time of diagnosis, i.e., the employment rate, as this is not relevant to unpaid work. Moreover, we assumed that individuals may continue performing unpaid work beyond the official retirement age in each country. Equivalently to paid work, the model assumed a certain level of activity impairment due to mBC in the first 2 years after treatment [28]. To monetize the avoided unpaid productivity losses we used the average value of unpaid work [43,44]. Relevant input data are detailed in Appendices, Supplementary Table 4.
(Equation 2)
where UP is the number of patients able to resume unpaid work, AI is the activity impairment, UH is the number of unpaid hours and UC is the cost of unpaid work.
Informal caregiver productivity impact
Informal caregiving is a crucial component when evaluating the broader societal implications of a disease or the value generated from an innovative health intervention. Informal caregivers, mainly referring to families, spouses and friends, play a substantial role in supporting the patients and are often significantly affected by consequences of illnesses, particularly in chronic or advanced conditions. Thus, the burden associated with informal caregiving may be substantial, frequently leading to disruptions of their working lives. This impact may result in productivity losses that extend beyond the household, further affecting the whole society.
In this assessment we defined informal caregivers as family members who provide assistance to mBC patients [45]. To quantify the productivity losses experienced by informal caregivers, we focused on post-progression patients, during the initial year following cancer progression [46]. Additionally, we applied a probability factor to account for the likelihood of individuals receiving informal care [47]. Our assessment was restricted to the quantification of paid work losses. Research indicates that informal caregivers may miss approximately two working days annually due to caregiving [45]. Hence, the impact on working hours due to caregiving was quantified and subsequently assigned a monetary value through the GVA as follows:
(Equation 3)
where PP refers to the post progression patients, prIC is the probability of having an informal carer, DM is the average days missed per family per year and HWD is the working hours per day.
Input data concerning productivity losses for informal caregivers is provided in Supplementary Table 3 of the appendices.
Formal caregiver impact
Incorporating the impact of formal (paid) caregiving is essential for a comprehensive societal evaluation of healthcare interventions. As disease progresses, particularly in conditions like mBC, patients often require professional support services such as home nursing, physiotherapy or domestic assistance. These services may represent a tangible cost to patients, families and healthcare systems. By quantifying changes in the need for formal care between the two treatment scenarios, we can better incorporate the full cost implications of a disease, and the potential cost offsets associated with a new treatment option.
Analogous to informal caregivers, we focused the evaluation of paid care on the first-year post-progression patients. To align with the evidence used, we defined paid care as home nurse, home help services, physiotherapist, adult day care and cleaning help [47]. By utilizing evidence on time spent per day of formal care [47] and on the probability of having a formal carer [45] we calculated the incremental difference between the two treatment scenarios, expressed as hours. Subsequently, we converted these into monetary values, utilizing evidence on the average costs associated with paid caregiving [48,49]. Thus, we can illustrate the calculation steps as follows:
(Equation 4)
where PP is the number of post-progression patients, prFC is the probability of having a formal carer, HPC is the average hours of paid care per day and CPC is the average cost of paid care per hour. The required input data can be found in Supplementary Table 4 within the appendices.
Childcare impact
Chronic illnesses like mBC can substantially affect a patient's ability to engage in childcare, usually leading to reliance on paid services. Like unpaid work, by improving health outcomes through effective treatments, patients may continue with childcare activities, resulting in cost savings for households. For this assessment, we excluded childcare from unpaid activities as described above and evaluated this as a separate element.
We relied on the assumption that improved health outcomes associated with T-DXd allow more patients to engage in childcare activities, resulting in monetary savings due to avoided paid services. As with unpaid work, we assumed that patients who return to work are also capable of restarting unpaid work and thereby, childcare duties. Further, we applied a proportionate percentage of childcare responsibilities that are associated to formal caregiving and a probability of belonging in a household with no-sibling children (i.e., be responsible for a dependent child). Finally, by applying the average childcare cost per hour, the total savings in childcare costs were computed as follows:
(Equation 5)
where UP is the number of patients able to fulfill childcare duties, prCH is the probability of living in a household with no-sibling child, HCC is the average hours of childcare per person per year, FCC is the proportion of childcare that is formal and CC is the average cost of childcare per hour. In Supplementary Table 4 of the appendices, we present the essential input data concerning childcare impact.
Quality-adjusted life years (QALY)
QALYs are a widely accepted metric in health economic evaluations, combining both the quantity and quality of life gained from a medical intervention. Capturing and monetizing QALY gains is essential for understanding the full value of treatment not only in terms of survival but also in reduced morbidity.
For this reason and given T-DXd’s superior efficacy in comparison to SOC and the health-related quality of life benefits that have been observed in several trials [17,50,51], we assessed the incremental gain in QALYs relative to the counterfactual scenario. This incremental gain includes extended life years and an enhancement in the quality of life. We derived the incremental QALYs from the CEMs [15,16]. The monetization was implemented using a willingness to pay (WTP) value per QALY [52], (Appendices, Supplementary Table 3) as follows:
(Equation 6)
where P is the total number of patients and QD is the incremental difference in the number of QALYs.
Fiscal impact
Fiscal impact refers to the influence of morbidity and mortality changes on public accounts, including government revenues (e.g., taxes) and expenditures (e.g., social transfers). Events such as premature mortality, long-term disability or reduced labor force participation can lead to decreased tax contributions and increased reliance on state-funded benefits. In contrast, improved health outcomes – such as longer life expectancy and reduced morbidity – may result in sustained tax revenues while minimizing public spending on disability benefits. Therefore, fiscal impact analysis offers valuable insight into how healthcare innovations affect government budgets, further highlighting the broader societal value of new and innovative interventions.
To quantify the impact of T-DXd on governmental accounts we relied on a previously developed and a widely implemented methodological approach [53–55]. Specifically, we modeled fiscal consequences by considering revenue streams and transfer payments between individuals and the government. Revenue sources included direct income taxes and indirect taxes on consumer consumption. Transfer payments included benefits provided to individuals as financial support due to disability and old age pensions. Specifically, sickness and disability benefits can be claimed by patients as financial support due to loss of working capability. In our assessment, the changes in sickness and disability benefits arise from better health. Therefore, we connected return to work with the reduction in these payments. Further, we evaluated transfer payments received by patients who did not previously work. In this case, however, only disability benefits were applied. Thus, sickness and disability benefits were driven by progression-free and overall survival. Particularly, extended survival is likely to lead to increased benefits and pensions received. In other words, changes in physical functioning, illustrated by PFS, were linked to employment outcomes, which in turn determined tax contributions and receipt of disability-related transfers. Administrative costs were not assessed. Data on sickness and disability benefits was sourced from national statistical offices [56–59] (Appendices, Supplementary Table 5). We calculated the government expenditure on sickness and disability benefits over time, as follows:
(Equation 7)
where NtSB,j is the number of patients receiving disability and sickness benefits, SB is the monetary amount of sickness and disability benefits per year, NtDB,j is the number of patients receiving only disability benefits, and DB declares the monetary amount of disability benefits per year.
The incremental number of patients returning to work impacts tax revenues. Aligned with existing literature, income taxes were quantified by taking the average gross income within each country [60] and subsequently multiplying it by the country specific tax wedge [61] (Appendices, Supplementary Table 4). The quantification of indirect taxes involved multiplying the value-added (VAT) [62–66] by the disposable income [67–71] of individuals. Thus, the calculation steps are as follows:
(Equation 8)
where WP is the incremental number of patients returning to work, I is the gross income, tw refers to the tax wedge, DI to the disposable income and VAT is the value added tax.
For pensions, our case study relied on how improved survival and return to work rates from the health intervention may lead to old-age pensions. We restricted our analysis of old age pensions to patients who returned to work, considering the official retirement age in each country, and mortality (i.e., how long the patients will survive post-retirement).
We calculated the impact on pensions as:
(Equation 9)
where WP is the incremental number of patients returning to work (thus eligible for old-age pension when reaching retirement ager), and APc is the average pension per year in each EU5 country.
Sensitivity analysis
To address uncertainty and ensure robustness of the model results, we conducted a probabilistic sensitivity analysis (PSA). The PSA introduced probability distributions to key input parameters (Appendices, Supplementary Tables 3 & 4). Specifically, we executed 1000 Monte Carlo simulations for each country and presented the results using 95% credible interval (CrI), to demonstrate the uncertainty around our estimates.
Further, as we relied on UK published evidence on overall productivity and activity impairment to assess the societal impact on paid and unpaid work, we performed a targeted scenario analysis. Specifically, to assess the potential structural uncertainty associated with this assumption, we varied the respective inputs by ±20% in Italy, Spain, France and Germany.
Results
Table 1 summarizes the incremental societal value of T-DXd in mBC by each value component in all the EU5 countries as compared with the counterfactual scenario. The results demonstrate the expected maximum impact of T-DXd, since the analysis considered a market share of 100%. In terms of avoided losses in patient paid productivity, T-DXd resulted in savings of €589 million in the EU5, attributed to increased PFS and thus, increased patient working years. Avoided productivity losses in terms of unpaid work was associated with a societal gain of €259 million in EU5. The economic impact associated with childcare activities was approximately €5 million. Increased taxation resulted in a governmental surplus of €165 million in the EU5, attributed to increased labor force participation. Monetized QALYs presented the most pronounced positive societal impact, of approximately €1.7 billion across EU5.
| UK | Germany | France | Spain | Italy | |
|---|---|---|---|---|---|
| Patients entering the model, n, cohorts 1–5 | 14,535 | 16,731 | 16,883 | 9229 | 12,580 |
| Patient GVA† | 131 (95% CrI: 123, 139) | 154 (95% CrI: 144,159) | 136 (95% CrI: 126, 140) | 64 (95% CrI: 60,67) | 102 (95% CrI: 84,114) |
| QALY† | 378 (95% CrI: 301, 457) | 404 (95%CrI: 330,482) | 385 (95% CrI: 348,488) | 175 (95% CrI: 150, 232) | 311 (95% CrI: 223, 340) |
| Carer GVA† | -1.5 (95% CrI: 1.2, 1.4) | -2 (95% CrI: -2.5, -1.2) | -1.7 (95% CrI: -2.9, -1.4) | -0.6 (95% CrI: -1, -0.5) | -1 (95% CrI: -1.5, -0.8) |
| Unpaid work† | 48 (95% CrI: 45, 79) | 59 (95% CrI: 39,73) | 59 (95% CrI: 43,77) | 35 (95% CrI: 21,37) | 56 (95% CrI: 36,61 |
| Tax impact† | 26 (95% CrI: 25, 35) | 51 (95% CrI: 42,60) | 45 (95% CrI: 36,53) | 14 (95% CrI: 12, 17) | 28 (95% CrI: 24,34) |
| Disability benefits† | -99 (95% CrI: -121, -75) | -166 (95% CrI-281, -152) | -52 (95% CrI: -66, -39) | -35 (95% CrI: -45, -24) | -29 (95% CrI: -39, -20 |
| Paid care cost† | -9 (95% CrI: -13, -7) | -8 (95% CrI: -13, -3) | -5 (95% CrI: -9, -2) | -2 (95% CrI: -2.6, -1.5) | -4 (95% CrI: -5, -3) |
| Childcare cost† | 1.3 (95%CrI: 1,1.5) | 0.6 (95% CrI: 0.44, 0.87) | 1 (95% CrI: 0.6, 1.4) | 0.8 (95% CrI: 0.5, 0.9) | 0.7 (95% CrI: 0.4, 0.8) |
| Pensions† | -7 (95% CrI: -8, -5) | -8 (95% CrI: -10, -7) | -17 (95% CrI: -20, -13) | -5 (95% CrI: -5.7, -4) | -8 (95% CrI: -9.4, -6.4) |
†
Rounded numbers (million €).
95% CrI: 95% credible interval; GVA: Gross value added; QALY: Quality-adjusted life years.
Nonetheless, there were some net negative socioeconomic implications of T-DXd, which were mainly attributed to increased survival, leading to accumulation of the respective costs. This included a -€7 million GVA impact for caregivers, -€27 million in paid care costs, -€380 million in disability benefits and a -€44 million impact on pensions in EU5 (Table 1). Results on the change in working patient years, in the number of patients able to fulfil unpaid activities, QALY gains and incremental first-year post-progression patients are available in Appendices, Supplementary Table 5.
Varying productivity and activity impairment inputs by ±20% had a limited impact on productivity outcomes (Appendices, Supplementary Table 6).
Discussion
This analysis was implemented across the EU5 countries as they represent the largest pharmaceutical markets, because of their policy relevance, and their importance for the pharmaceutical industry in Europe [72]. Within Europe France, Germany, Italy, Spain and the UK have the majority of innovative launches, and they represent the primary focus of pharmaceutical and market analysis [73].
As interest grows among stakeholders in analyses evaluating the wider societal impact of health innovations, it is essential that professionals in health economics and outcomes research can apply relevant and suitable methods. Previously, robust methodologies have been developed such as the Social Return on Investment. These methodologies aim to provide guidance on incorporating and evaluating the wider social value of health interventions considering social, economic and environmental dimensions [4]. Thus, evidence exists that capturing the non-financial aspects of health interventions which add value to patient's life and society is essential to understanding the broader societal impact. Additionally, Shafrin et al. [1], has contributed substantially to this area by introducing the GCEA concept. In particular, the GCEA framework provides guidance on evaluation of fifteen value elements including outcome uncertainty, disease risk reduction, value of knowing, dynamic net health system cost, dynamic disease prevalence and others.
Despite recent advances in research, a standardized methodological approach for valuing these elements has not yet been widely adopted. Furthermore, several proposed value elements e.g., value of hope, or insurance value, cannot be fully incorporated in economic analyses as they remain difficult to quantify, requiring further research and methodological development [2]. Additionally, in many cases the lack of empirical evidence further limits the applicability and integration of these elements. These challenges may explain why these are not frequently assessed. However, discussions on the inclusion of broader value components in economic analysis, are increasing [5,6,74].
Nevertheless, the exclusion of certain value elements is expected to have implications for the estimated societal value. Based on the extended GCEA framework [1], the inclusion of elements for example scientific spillovers, caregiver spillovers and equity considerations would likely increase the estimated value of the intervention. In contrast, elements such as direct healthcare costs and those negatively affected by extended survival may lead to additional economic burdens, while others may have varying specific effects depending on the disease area and patient population. Although the quantification of all potential value elements was beyond the scope of the current analysis, it is important to note that the estimates in our study may represent a conservative approximation of the true societal value. Future research should focus on better understanding and estimating the value elements that are most likely to influence overall results.
This study presents a methodological approach for incorporating specific value elements into economic evaluation, going beyond the classical cost effectiveness approach. By extending the focus the aim is to complement traditional HTA processes to provide a wider perspective on the value associated with health innovations. It is important to note that similar to previous research [1,4], this study does not aim to provide a framework to replace existing CEAs. It aims to provide an extension framework of the current standard practice to complement the traditional HTA. By focusing on value elements with existing robust methodological background and measurable outcomes, this approach offers a defensible and feasible pathway for analysts and decision makers to begin incorporating such elements into economic evaluations. This framework may be particularly relevant in contexts where treatments meaningfully affect survival, functional capacity, or labor force participation, such as oncology or chronic disabling conditions. In such settings, relying solely on direct costs and QALYs may underestimate the broader value generated by effective therapies.
Our case study showed that specific value-added elements, such as paid and unpaid productivity losses, childcare, tax revenue and QALYs lead to increased socioeconomic value creation attributed to T-DXd. In this case study, this was mainly driven by increased probabilities of PFS and the favorable health outcomes. Moreover, patients receiving T-DXd achieved higher QALYs. These positive health outcomes could be translated into socio-economic benefits. However, higher costs for formal and informal care, pensions and disability benefits were observed. These increases were driven by extended survival and should therefore be interpreted as survival-driven expenditure rather than negative consequences of the intervention. Life-extending therapies should be expected to lead to higher expenditures in certain domains, as patients who live longer continue to consume healthcare and social resources. This is an important consideration in societal evaluations where costs may increase alongside substantial gains in QALYs. Thus, these outcomes should be evaluated closely in relation to the health impact achieved rather than interpreted in isolation. Recognizing this dynamic may prevent misrepresenting the true value of the new intervention [75]. Taken together, the direction of effects across all individual components supports a positive overall impact of the intervention.
This analysis focused on elements with existing methodological support or prior application and included fiscal impact as an additional value element [1,3].A key advantage of this analysis is the ability to contextualize the outcomes within other societal variables to better understand their implications. For example, the avoided patient productivity losses reflected as GVA gains along with monetized impact on unpaid work and childcare may be comparable to the equivalent of the annual salaries of 5466 hospital nurses in the UK, 4612 hospital nurses in Germany, 5917 hospital nurses in France, 2624 hospital nurses in Spain, and 5698 hospital nurses in Italy for 1 year [76]. Further, the increased taxation is equivalent to pharmaceutical expenditures for 65,221 people in UK, 62,570 people in Germany, 66,103 people in France, 26,470 people in Spain and 45,523 people in Italy within 1 year [77].
From a policy perspective, both the methodology and the findings, together with existing evidence, highlight the importance of considering broader societal effects of an intervention alongside traditional healthcare costs and clinical end points. For policymakers, these results may support the inclusion of such elements in decision-making, particularly when evaluating treatments with long-term benefits. For HTA bodies, this research underscores the need to further develop and standardize robust methodologies for capturing the societal value of interventions, particularly with respect to productivity and caregiver effects. From a clinical perspective, the findings highlight the importance of timely and effective treatment strategies that improve patient health outcomes and, consequently, reduce associated socioeconomic impacts. Finally, these results may help inform future research priorities by identifying areas where additional value could be generated.
Overall, this case study has several limitations. To reduce the methodological challenges in applying the same data across all countries, we initially aimed to use country specific evidence. However, due to limited data availability, this was not feasible for productivity and activity impairment associated with mBC. Therefore, we derived evidence from one study conducted in the UK [28] and applied it to the remaining countries, as it was the only one identified specifically for metastatic patients. This approach is subject to several assumptions. We assumed that the healthcare systems in the UK and other EU countries are comparable in terms of BC care and management, since treatment protocols for BC in Europe do not demonstrate significant variations due to the common regulatory agency (EMA) and to European Society for Medical Oncology (ESMO) guidelines [78], although national guidelines and healthcare systems might differ. Similarly, organizations such as the European Society of Breast Cancer Specialists (EUSOMA) aim to improve and harmonize BC care across Europe and to set uniform care standards [79]. Furthermore, the EU health policy also contributes to a common health strategy across EU countries [80]. Therefore, considering the data limitations, and the fact that this study focused on EU countries, where we may assume that healthcare and social security systems that are reasonably comparable relative to other regions [81–86], we do not expect that these assumptions would have substantial influence on the conclusions.
However, it is noteworthy that differences in national labor law, sick leave and disability benefit schemes may affect return to work patterns [87]. As a result, this may affect the calculated productivity and fiscal impacts. Future research should aim to incorporate country-specific data on return to work and overall work impairment due to disease. Nevertheless, an additional targeted scenario analysis has been conducted in which we varied the productivity and activity impairment inputs by 20% to assess the potential structural uncertainty introduced by this assumption. The scenario analysis did not indicate a significant impact on productivity outcomes.
In addition, due to limited available evidence, we applied the same probability of having a formal and informal caregiver in all EU5 countries. Furthermore, based on the available evidence, we applied productivity impairment rates only for the first 2 years after re-entering the workforce. However, it is likely that impairment will persist for a longer period [29]. In the absence of analogous data concerning activity impairment, we assumed the same impairment duration. Notably, the duration of impairment may vary across settings with respect to labor market conditions and social protection systems [87]. Additionally, this analysis focused on a single framework for evaluating the governmental perspective [88]. This framework has been widely adopted in literature for several countries worldwide. Nevertheless, the fiscal impact components were parametrized using country-specific inputs. Given the aforementioned assumptions, we performed additional PSA analysis, which reassured the model’s robustness to variations in these inputs.
The 100% market share assumption does not represent real-world practice. In this analysis, the intervention was applied to the eligible population rather than treated patients, capturing the maximum impact of T-DXd. This assumption does not reflect real-world uptake which may be gradual and typically varies across settings. However, as the primary aim of this analysis was to demonstrate the application of additional value elements rather than assessing the real-world societal value of T-DXd, the framework provides a basis for similar applications and can be adapted accordingly.
Differences in standard of care between countries have not been adjusted for, and the analysis did not account for potential treatment advancements, including newer and more effective therapies that may emerge as SOC. The focus of this analysis was on the inclusion of broader value elements rather than direct costs associated with T-DXd. Hence, direct costs such as drug costs, administration costs, resource costs etc., were not considered. Nonetheless, direct costs are usually integrated into HTA to facilitate reimbursement decisions and T-DXd has already been assessed from this perspective in the EU5 [89–94].
A potential limitation of a societal impact analysis is the risk of double counting societal effects. For example, QALYs may partially capture functional limitations that also influence work and daily activities. To mitigate the risk of double counting, we have refrained from aggregating the distinct societal effects into total value. Further investigation is needed to adequately address any potential double counting effect. In addition, certain assumptions, such as the return-to-work rate influence multiple elements in this analysis including productivity and fiscal effects. While this will not lead to double counting within individual domains, it may introduce structural dependencies. Nevertheless, in the present analysis none of the societal elements were combined to avoid misinterpretation and potential double counting.
Finally, monetization of QALYs has been performed using WTP values. However, WTP is based on HTA threshold, which might be subject to change if health policy changes.
Recommendation for future research
The potential double counting between value components remain a methodological challenge. Specifically, both the presence and the extent of overlap should be assessed, including which components may overlap and to what degree. Overall, future research should aim to develop approaches to better distinguish between these components. In particular, the use of patient-level or longitudinal data may enable more precise estimation of individual value elements, as well as a clearer separation between health-related outcomes, functional status, and workforce participation, thereby reducing reliance on simplifying assumptions. Another important direction is the development of adjustment methods to account for potential double counting when combining multiple value elements.
Moreover, estimating and incorporating country-specific data on key inputs – such as labor market participation and activity impairment – would improve the accuracy and contextual relevance of societal impact estimates across different settings.
In this context, such frameworks may also support policy discussions around broader benefits medicines and associated pricing, which are not typically captured in current HTA evaluation.
Conclusion
This study presents a methodological approach to incorporate and quantify additional value elements in the economic evaluation of healthcare interventions. By extending beyond traditional healthcare metrics, such as direct medical costs and QALYs, we attempted to capture a broader set of societal elements – including paid and unpaid work productivity, caregiving, childcare activities and fiscal outcomes. Using T-DXd in mBC as a case study, we demonstrated how these elements can be assessed and monetized to reflect the full societal value of innovative treatments. In our case study, T-DXd was associated with positive impacts on productivity (€589 million), QALYs (€1.7 billion), unpaid work (€259 million), childcare impact (€5 million) and taxation (€165 million). Meanwhile we accounted for increased formal and informal caregiver costs (-€27 million, -€7 million), disability benefits (-€380 million) and pensions (-€44 million). Our approach provides empirical evidence that the economic value of healthcare interventions extends beyond traditional healthcare metrics and shows how these can be quantitatively assessed. This research offers relevant insights for various stakeholders, including healthcare payers, finance ministries, HTA bodies, patient groups and physicians, while providing a consistent framework to assess societal impact.
Summary points
•
Traditional economic evaluations are mainly focused on direct costs, often neglecting broader value elements that capture how innovative health interventions may impact patients, family and society.
•
This study introduces a framework, serving as a guiding tool, to establish a consistent and transparent assessment of selected additional value elements.
•
This framework also considers consequences on governmental accounts making it particularly relevant for stakeholders in finance and public policy.
•
A case study was conducted for metastatic breast cancer (mBC) across five European countries, using trastuzumab deruxtecan (T-DXd) as an example intervention.
•
The methodology described is adaptable and scalable to different countries, diseases and populations to support societal-perspective evaluations.
•
The additional value elements assessed may result in positive economic impact or additional costs, depending on the impact of the intervention on patient outcomes.
•
Beyond direct medical costs, excess costs may be introduced due to prolonged survival. Longer survival may increase public and caregiver costs, potentially biasing economic evaluations against effective treatments.
•
When positive societal effects occur, these can be substantial.
Author contributions
All listed authors made substantial contributions to the development of this research. F Tsotra, K Dunton, M Rosenlund and S Johal contributed to the study conception and design. F Tsotra conducted the analysis and L Steinbeck contributed to the literature review, identification and validation of model inputs. K Dunton, M Rosenlund and S Johal provided supervision throughout the study. All authors contributed to the interpretation of the data, critically revised the manuscript for important intellectual content, and approved the final version of the manuscript.
Acknowledgments
The authors thank Ahmed Seddik for his early contributions to the development of this work.
Financial disclosure
This work was supported by funding from Daiichi Sankyo Europe GmbH and AstraZeneca.
Competing interests disclosure
K Dunton is an employee of Daiichi Sankyo UK Ltd, S Johal is an employee of AstraZeneca and holds stock in AstraZeneca, M Rosenlund is an employee of Daiichi Sankyo Europe GmbH, Munich, Germany, F Tsotra is an employee of the WifOR Institute, Athens, Greece, L Steinbeck was an employee of the WifOR Institute, Germany, at the time the study was conducted. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing disclosure
No funded writing assistance was utilized in the production of this manuscript. The authors used an AI-based language model (ChatGPT, OpenAI) to assist only with language editing and proofreading.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary material.docx)
- Download
- 58.89 KB
References
Papers of special note have been highlighted as: • of interest
1.
Shafrin J, Kim J, Cohen JT et al. Valuing the societal impact of medicines and other health technologies: a user guide to current best practices. Forum Health Econ. Policy 27(1), 29–116 (2024).
• This research is particularly important for this study as it aligns with the shift toward a broader societal perspective, and it provides methodological guidance for including additional value elements.
2.
Hofmann S, Branner J, Müller M et al. Assessing the value of medicines beyond patients' health benefit. A literature review on the concepts and methods for pharmaceutical value assessments from a societal perspective. https://insights.wifor.com/en/hta-download
3.
Neumann PJ, Garrison LP, Willke RJ. The history and future of the “ISPOR Value Flower”: addressing limitations of conventional cost-effectiveness analysis. Value Health 25(4), 558–565 (2022).
• The ISPOR ‘value flower’ introduced the concept of additional value elements that should be captured in health economic evaluations and is now a widely accepted framework in the field.
4.
Ashton K, Parry-Williams L, Dyakova M, Green L. health impact and social value of interventions, services, and policies: a methodological discussion of health impact assessment and social return on investment methodologies. Front. Public Health 8, 49 (2020).
5.
Chou J, Graf M. Generalized cost-effectiveness analysis to assess treatment value in hepatitis C. Am. J. Manag. Care 29(12), 696–703 (2023).
6.
Ma S, Olchanski N, Cohen JT, Ollendorf DA, Neumann PJ, Kim DD. The impact of broader value elements on cost-effectiveness analysis: two case studies. Value Health 25(8), 1336–1343 (2022).
7.
World Health Organisation (WHO). Breast cancer [Internet]. (2023). https://www.who.int/news-room/fact-sheets/detail/breast-cancer
8.
European Cancer Information System (ECIS). Breast cancer factsheet in 2020 for EU-27 countries [Internet]. https://ecis.jrc.ec.europa.eu/pdf/factsheets/Breast_cancer_en-Dec_2020.pdf
9.
Europa Donna. Breast cancer facts [Internet]. (2022). https://www.europadonna.org/breast-cancer/
10.
Luengo-Fernandez R, Leal J, Gray A, Sullivan R. Economic burden of cancer across the European Union: a population-based cost analysis. Lancet Oncol. 14(12), 1165–1174 (2013).
11.
Bermejo De Las Heras B, Cortes Ramon Y, Cajal J et al. The economic burden of metastatic breast cancer in Spain. Eur. J. Hosp. Pharm. 27(1), 19–24 (2020).
12.
Hanly P, Soerjomataram I, Sharp L. Measuring the societal burden of cancer: the cost of lost productivity due to premature cancer-related mortality in europe. Int. J. Cancer 136(4), E136–E145 (2015).
13.
Sun L, Li S, Peng X. Should additional value elements be included in cost-effectiveness analysis in pharmacoeconomic evaluation: a novel commentary. Cost Eff. Resour. Alloc. 21(1), 79 (2023).
14.
Yang J, Han J, Zeng N, Yan X. Cost-effectiveness of trastuzumab deruxtecan in previously treated human epidermal growth factor receptor 2-low metastatic breast cancer. Ther. Adv. Med. Oncol. 15, 17588359231169983 (2023).
15.
Postma A, van Schoonhoven A. Global cost-effectiveness & budget impact model for T-DXd in HER2-low metastatic and/or unresectable breast cancer. Unpublished. Asc Academics. (2022).
16.
Paulissen J, Sloof B. Global cost-effectiveness & budget impact model for T-DXd in HER2-positive metastatic and/or unresectable breast. Unpublished. Asc Academics. (2021).
17.
Cortés J, Kim S-B, Chung W-P et al. Trastuzumab deruxtecan versus trastuzumab emtansine for breast cancer. N. Engl. J. Med. 386(12), 1143–1154 (2022).
• Several core clinical inputs for this study was sourced from this clinical trial.
18.
Modi S, Jacot W, Yamashita T et al. Trastuzumab deruxtecan in previously treated HER2-low advanced breast cancer. N. Engl. J. Med. 387(1), 9–20 (2022).
• Several core clinical inputs for this study was sourced from this clinical trial.
19.
International Agency for research in cancer (IARC). Estimated age-standardized incidence rates (World) in 2020, breast, females, ages 0–74 [Internet]. (2020). https://gco.iarc.fr/today/online-analysis-map?v=2020&mode=population&mode_population=continents&population=900&populations=900&key=asr&sex=2&cancer=20&type=0&statistic=5&prevalence=0&population_group=0&ages_group%5B%5D=0&ages_group%5B%5D=14&nb_items=10&group_cancer=1&include_nmsc=0&include_nmsc_other=0&projection=natural-earth&color_palette=default&map_scale=quantile&map_nb_colors=5&continent=0&show_ranking=0&rotate=%255B10%252C0%255D
20.
Paulissen J, Sloof B.Technical Report: global cost-effectiveness & budget impact model for T-DXd in HER2-positive metastatic and/or unresectable breast. Asc Academics. (2021).
21.
Shirman Y, Lubovsky S, Shai A. HER2-low breast cancer: current landscape and future prospects. Breast Cancer Targets Ther. 15, 605–616 (2023).
22.
Exman P, Tolaney SM. HER2-positive metastatic breast cancer: a comprehensive review. Clin. Adv. Hematol. Oncol. 19(1), 40–50 (2021).
23.
O'Mahony JF, Paulden M. NICE's selective application of differential discounting: ambiguous, inconsistent, and unjustified. Value Health 17(5), 493–496 (2014).
24.
GOV.UK. The Green Book (2022) [Internet]. GOV.UK (2023). https://www.gov.uk/government/publications/the-green-book-appraisal-and-evaluation-in-central-government/the-green-book-2020
25.
Hofmann S, Himmler S, Ostwald DA, Dünzigner U, Launonen A, Salmen H. The societal impact of obinutuzumab in the first line treatment of patients with follicular lymphonma in Germany. ISPOR 21st Annual European Congress, Barcelona, Spain (10–14 November 2018).
26.
Sesto ME, Carroll CB, Zhang X et al. Unmet needs and problems related to employment and working as reported by survivors with metastatic breast cancer. Support. Care Cancer 30(5), 4291–4301 (2022).
27.
Molina Villaverde R, Feliu Batlle J, Villalba Yllan A et al. Employment in a cohort of breast cancer patients. Occup. Med. 58(7), 509–511 (2008).
28.
Verrill M, Wardley AM, Retzler J et al. Health-related quality of life and work productivity in UK patients with HER2-positive breast cancer: a cross-sectional study evaluating the relationships between disease and treatment stage. Health Qual. Life Outcomes 18(1), 353 (2020).
29.
Boelhouwer IG, Vermeer W, van Vuuren T. The associations between late effects of cancer treatment, work ability and job resources: a systematic review. Int. Arch. Occup. Environ. Health 94(2), 147–189 (2021).
30.
Federal Ministry of Labour and Social Affairs. Old age security in Germany [Internet]. http://www.bmas.de (2023). https://www.bmas.de/EN/Social-Affairs/Old-age-security-in-Germany/old-age-security-in-germany-art.html
31.
Age UK. State Pension Advice [Internet]. Age UK (2023). https://www.ageuk.org.uk/information-advice/money-legal/pensions/state-pension/
32.
CLEISS. Raising the statutory retirement age to 64 in France [Internet]. (2023). https://www.cleiss.fr/actu/2023/2305-raising-statutory-retirement-age-to-64-france.html
33.
Ministerio de Inclusion, Securidad Social Y Migraciones. Seguridad social: benefits / pensions for workers [Internet]. https://www.seg-social.es/wps/portal/wss/internet/Trabajadores/PrestacionesPensionesTrabajadores/10963/28393/28396/28472
34.
European Commission. Italy - Employment, Social Affairs & Inclusion - European Commission [Internet]. (2023). https://ec.europa.eu/social/main.jsp?catId=1116&langId=en&intPageId=4625
35.
Himmler S, Branner JC, Ostwald DA. The societal impact of a biologic treatment of ankylosing spondylitis: a case study based on secukinumab. J. Comp. Eff. Res. 10(2), 143–155 (2021).
36.
Hofmann S, Himmler S, Ostwald D, Dünzinger U, Launonen A, Thuresson P-O. The societal impact of obinutuzumab in the first-line treatment of patients with follicular lymphoma in Germany. J. Comp. Eff. Res. 9(14), 1017–1026 (2020).
• This research is particularly relevant as it explores productivity losses in cancer patients.
37.
Ostwald DA, Schmitt M, Peristeris P, Gerritzen T, Durand A. The societal impact of Inclisiran in England: evidence from a population health approach. Value Health 26(9), 1353–1362 (2023).
38.
WifOR Institute. Glossary. Health Economics. [Internet]. https://insights.wifor.com/en/glossary-health-economics
39.
Reid MG. Economics of household production. J. Wiley & Sons, NY, USA (2021).
40.
Reid M. Economics of Household Production. Ann. Am. Acad. Pol. Soc. Sci. 178(1), 213 (1935).
41.
Ferrant G, Pesando LM, Nowacka K. Unpaid Care Work: the missing link in the analysis of gender gaps in labour outcomes [Internet]. (2014). https://www.oecd.org/dev/development-gender/Unpaid_care_work.pdf
42.
Eurostat. Zeitverwendung, Teilnahmezeit und Teilnahmerate für die Hauptaktivität nach Geschlecht und Altersgruppe [Internet]. (2023). https://ec.europa.eu/eurostat/web/products-datasets/-/tus_00age
43.
Eurostat. Overview - Harmonised European Time Use Surveys (HETUS) - Eurostat [Internet]. (2024). https://ec.europa.eu/eurostat/web/time-use-surveys
44.
Office for National Statistics (ONS). Unpaid work calculator (based on household satellite accounts and annual survey of hours and earnings). (2016).
45.
Wan Y, Gao X, Mehta S, Wang Z, Faria C, Schwartzberg L. Indirect costs associated with metastatic breast cancer. J. Med. Econ. 16(10), 1169–1178 (2013).
46.
Yabroff KR, Kim Y. Time costs associated with informal caregiving for cancer survivors. Cancer 115(Suppl. 18), 4362–4373 (2009).
47.
Baitar A, Buntinx F, De Burghgraeve T et al. The utilization of formal and informal home care by older patients with cancer: a Belgian cohort study with two control groups. BMC Health Serv. Res. 17(1), 644 (2017).
48.
NHS. Paying for your own care (self-funding) [Internet]. (2022). https://www.nhs.uk/conditions/social-care-and-support-guide/money-work-and-benefits/paying-for-your-own-care-self-funding/
49.
SalaryExpert (ERI Economic Research Institute). Salary data and compensation estimates by job and location. [Internet]. https://www.salaryexpert.com/salary
50.
Fehm TN, Cottone F, Dunton K et al. 186O Patient-reported outcomes (PROs) from DESTINY-Breast02, a randomized Phase III study of trastuzumab deruxtecan (T-DXd) vs treatment of physician's choice (TPC) in patients (pts) with HER2–positive (HER2+) metastatic breast cancer (mBC). ESMO Open 8(1), 101375 (2023).
51.
Ueno NT, Jacot W, Yamashita T et al. 217O Patient-reported outcomes (PROs) from DESTINY-Breast04, a randomized Phase III study of trastuzumab deruxtecan (T-DXd) vs treatment of physician's choice (TPC) in patients (pts) with HER2-low metastatic breast cancer (MBC). Ann. Oncol. 33, S632–S633 (2022).
52.
Minacori R, Geale K, Geale K. Is there evidence of a difference between willingness to pay and willingness to accept thresholds? A review of NICE Technology Appraisals. Value Health 19(7), A492–A493 (2016).
53.
Martins R, Kotsopoulos N, Michalowsky B, Pemberton-Ross P, Urbich M, Connolly MP. Evaluation of the fiscal costs and consequences of Alzheimer's disease in Germany: microsimulation of patients' and caregivers' pathways. J. Prev. Alzheimers Dis. 9(4), 758–768 (2022).
• This research is important as it set a robust methodological approach for measuring the fiscal impact of healthcare interventions.
54.
Connolly MP, Kotsopoulos N. Estimating the fiscal consequences of National Immunization Programs using a “Government Perspective” public economic framework. Vaccines 8(3), E495 (2020).
55.
Kotsopoulos N, Connolly MP, Li J. Estimating the public economic consequences of cardiovascular disease-attributable events and evolocumab treatment in Australia. J. Med. Econ. 24(1), 123–130 (2021).
56.
Federal Ministry of Labour and Social Affairs. Labour and Social Affairs [Internet]. (2023). https://www.bmas.de/EN/Home/home.html
57.
l'Assurance Maladie. ameli, le site de l'Assurance Maladie en ligne | ameli.fr | Assuré [Internet]. (2023). https://www.ameli.fr/assure
58.
Seguridad Social. Social security: internet [Internet]. https://www.seg-social.es/wps/portal/wss/internet/Inicio
59.
National Institute for Social Security (INPS). Social security [Internet]. Sito Uff. INPS Ist. Naz. Previd. Soc. https://www.inps.it
60.
OECD. OECD Statistics [Internet]. (2021). https://stats.oecd.org/
61.
OECD. Tax - Tax wedge - OECD Data [Internet]. The OECD. http://data.oecd.org/tax/tax-wedge.htm
62.
PwC. Italy - Corporate - Other taxes [Internet]. (2023). https://taxsummaries.pwc.com/italy/corporate/other-taxes
63.
GOV.UK. VAT rates [Internet]. GOV.UK (2023). https://www.gov.uk/vat-rates
64.
PwC. Spain - Corporate - Other taxes [Internet]. (2023). https://taxsummaries.pwc.com/spain/corporate/other-taxes
65.
PwC. Germany - Corporate - Other taxes [Internet]. (2023). https://taxsummaries.pwc.com/germany/corporate/other-taxes
66.
PwC. France - Corporate - Other taxes [Internet]. (2023). https://taxsummaries.pwc.com/france/corporate/other-taxes
67.
OECD Better Life Index. Italy - how's life [Internet]. (2023). https://www.oecdbetterlifeindex.org/countries/italy/
68.
Nomis - Official Census and Labour Market Statistics. Regional gross disposable household income - [Internet]. (2023). https://www.nomisweb.co.uk/datasets/gdhi
69.
INE base. Standard of living and living conditions (CPI) /Living conditions /Household Budget Survey. Base 2006/Latest data [Internet]. INE. https://www.ine.es/dyngs/INEbase/en/operacion.htm?c=Estadistica_C&cid=1254736176806&menu=ultiDatos&idp=1254735976608
70.
Destatis. Income, receipts and expenditure of households by territory [Internet]. Fed. Stat. Off. (2023). https://www.destatis.de/EN/Themes/Society-Environment/Income-Consumption-Living-Conditions/Income-Receipts-Expenditure/Tables/liste-Income-receipts-expenditure-households.html
71.
Statista. France: household disposable income [Internet]. (2023). https://www.statista.com/statistics/513021/average-annual-household-disposable-income-france/
72.
European Federation of Pharmaceutical Industries and Associations (EFPIA). The pharmaceutical industry in figures_key data [Internet]. https://www.efpia.eu/media/uj0popel/the-pharmaceutical-industry-in-figures-2025.pdf
73.
IQVIA. The Global Use of Medicines Outlook Through 2029 [Internet]. https://www.iqvia.com/insights/the-iqvia-institute/reports-and-publications/reports/the-global-use-of-medicines-outlook-through-2029
74.
Institute for Clinical and Economic Review (ICER). Health Economics Methods Advisory Group selects first area for study: assessing treatment benefits appropriate to consider in HTA decision-making [Internet]. (2024). https://icer.org/news-insights/press-releases/health-economics-methods-advisory-group-selects-first-area-for-study-assessing-treatment-benefits-appropriate-to-consider-in-hta-decision-making/
75.
Retzler J, Davies H, Jenks M, Kiff C, Taylor M. The impact of increased post-progression survival on the cost-effectiveness of interventions in oncology. Clin. Outcomes Res. 11, 309–324 (2019).
76.
OECD. Stat. Healthcare resources: remuneration of health professionals [Internet]. (2023). https://stats.oecd.org/index.aspx?queryid=30025
77.
OECD. Pharmaceutical spending [Internet]. (2023). https://data.oecd.org/healthres/pharmaceutical-spending.htm
78.
Zagouri F, Sergentanis TN, Tsigginou A et al. Female breast cancer in Europe: statistics, diagnosis and treatment modalities. J. Thorac. Dis. [Internet] 6(6), 589 (2014). https://jtd.amegroups.org/article/view/2662
79.
European Society of Breast Cancer Specialists (EUSOMA). About Us [Internet]. (2023). https://www.eusoma.org/en/about%2dus/1-105-1
80.
European Commission. Public Health [Internet]. (2023). https://health.ec.europa.eu/eu-health-policy/overview_en
81.
Aguiar-Fernández F, Rodríguez-Castro Y, Botija M, Martínez-Román R. Experiences of female breast cancer survivors concerning their return to work in Spain. Behav. Sci. 11(10), 135 (2021).
82.
Gobierno de Espana. Procedures and formalities – temporary disability benefits [Internet]. (2023). https://www.seg-social.es/wps/portal/wss/internet/InformacionUtil/44539/44667
83.
Gobierno de Espana. Procedures and formalities – permanent disability pension [Internet]. (2023). https://www.seg-social.es/wps/portal/wss/internet/InformacionUtil/44539/45982
84.
Baigey E. Sick Leave UK: laws, pay and how to build a sickness and absence policy [Internet]. Factorial (2023). https://factorialhr.co.uk/blog/sick-leave-uk/
85.
Maunder S. Social security in Italy [Internet]. Expatica (2023). https://www.expatica.com/it/living/gov-law-admin/social-security-italy-82918/
86.
Velocity Global. Employee benefits in France: a guide to mandatory and common benefits [Internet]. Veloc. Glob. (2023). https://velocityglobal.com/resources/blog/employee-benefits-in-france/
87.
OECD. Sickness, disability and work: breaking the barriers: a synthesis of findings across OECD countries [Internet]. OECD. https://www.oecd.org/en/publications/sickness-disability-and-work-breaking-the-barriers_9789264088856-en.html
88.
Connolly MP, Kotsopoulos N, Postma MJ, Bhatt A. The fiscal consequences attributed to changes in morbidity and mortality linked to investments in health care: a government perspective analytic framework. Value Health 20(2), 273–277 (2017).
89.
NICE. The National Institute for Health and Care Excellence [Internet]. (2024). https://www.nice.org.uk/
90.
HAS. Economic and Public Health Evaluation Committee [Internet]. (2024). https://www.has-sante.fr/jcms/c_2036304/en/economic-and-public-health-evaluation-committee
91.
G-BA. Gemeinsamer Bundesausschuss [Internet]. (2024). https://www.g-ba.de/
92.
HAS. Haute Autorité de Santé [Internet]. (2024). https://www.has-sante.fr/
93.
AEMPS. Agencia Española de Medicamentos y Productos Sanitarios [Internet]. (2024). https://www.aemps.gob.es/
94.
AIFA. Agenzia Italiana del Farmaco [Internet]. (2024). https://www.aifa.gov.it/
Information & Authors
Information
Published In
Copyright
© 2026 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 7 January 2026
Accepted: 14 April 2026
Published online: 22 May 2026
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Estimating the societal impact of medical interventions: a case study in metastatic breast cancer. (2026) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2026-0005
Export citation
Select the citation format you wish to export for this article or chapter.