Readmissions and retreatment among stent-assisted endovascular coiling patients with unruptured intracranial aneurysm using ENTERPRISE® 2 stent versus LVIS™ stent
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: The treatment of wide-necked unruptured intracranial aneurysms (UIA) remains clinically challenging. Stent-assisted coiling (SAC) is a commonly used treatment modality for UIAs. The objective of this study was to examine the differences in 180-day all-cause inpatient readmissions, UIA-related inpatient readmission, and retreatment among UIA patients treated with the laser cut nitinol ENTERPRISE® 2 stent versus the braided nitinol LVIS™ stent during SAC procedures. Materials & methods: Using Premier Healthcare Database (PHD), a US nationwide hospital database, UIA patients aged ≥18 years old undergoing SAC were identified. Patients were then classified into ENTERPRISE 2 and LVIS cohorts based on the stent used. Study outcomes, including 180-day all-cause and UIA-related inpatient readmissions, and UIA-related retreatment, were compared between the two cohorts. Inverse probability of treatment weighting of propensity score approach was used to balance covariates (i.e., patient demographic, clinical characteristics and hospital characteristics) between the two study groups. Chi-square test and weighted generalized estimating equation (GEE) model was used to assess outcomes among the weighted ENTERPRISE 2 and LVIS cohorts. Results: A total of 249 patients were included after applying study inclusion and exclusion criteria (with 130 in the ENTERPRISE 2 cohort and 119 in the LVIS cohort). Patient characteristics were well balanced after weighting. Bivariate analysis revealed that patients undergoing stent-assisted endovascular coiling using ENTERPRISE 2 stent had a significantly lower rate of 180-day all-cause inpatient readmissions (9.1% vs 24.3%, chi-square p = 0.016) and a significantly lower rate of 180-day UIA-related inpatient readmission (2.6% vs 12.4%, chi-square p = 0.036) compared with those treated with LVIS stent. GEE regression model indicated that patients in the ENTERPRISE2 stent cohort were 69% less likely to have 180-day all-cause inpatient readmissions (odds ratio: 0.31, 95% CI: 0.12–0.82, GEE p = 0.018) versus the LVIS cohort. However, no significant difference in 180-day UIA-related inpatient readmission and 180-day UIA-related retreatment was observed in GEE analysis. Conclusion: Patients who were treated with the laser-cut ENTERPRISE 2 stent during endovascular coiling were observed to have significantly lower risk of all-cause inpatient readmissions compared with those treated with the braided LVIS stent. No significant differences were observed for 180-day UIA-related readmission and retreatment among the study cohorts.
Plain language summary
What is this article about?
Unruptured intracranial aneurysm (UIA) is a disease of blood vessel in the brain. a third of patients with UIA will experience a rupture of their aneurysms, which can be fatal. Wide-necked UIA is a subtype of UIA and is more difficult to treat. Stent-assisted coiling (SAC) is used for treating the wide-necked UIA. This study compared hospital readmission rates and retreatment rate after SAC procedure performed using two different stents: ENTERPRISE® 2 stent and LVIS™ stent.
What were the results?
This study assessed data of 130 patients treated by ENTERPRISE 2 and 119 patients treated by LVIS during the SAC procedure. Patients undergoing SAC using the ENTERPRISE 2 stent were 69% less likely to experience hospital readmissions in 180 days after the procedure compared with those treated with LVIS stent. Patients treated with ENTERPRISE 2 stent had similar rate of UIA-related readmissions and retreatment than those treated with LVIS stent.
What do the results mean?
These findings suggest that the use of ENTERPRISE 2 stent may offer improvements in patient outcomes as compared with the LVIS stent.
Unruptured intracranial aneurysm (UIA) affects approximately 3% of the general population globally [1]. An estimated a third of patients with UIA will experience a rupture during their lifetime [2], which accounts for 80% of subarachnoid hemorrhage (SAH) [3]. Endovascular coiling is a commonly used treatment for UIA [4]. Stent-assisted coiling (SAC) has been developed as an advanced and safer modality for treating wide-necked UIA, a UIA subtype which poses increased therapeutic challenges. The integration of stent in coiling procedure can provide a permanent scaffold, allowing for increase in volumetric filling, preventing coil prolapse and promoting aneurysm thrombosis [5].
The ENTERPRISE® 2 Vascular Reconstruction Device (Johnson & Johnson MedTech, USA) and the Low-profile Visualized Intraluminal Support (LVIS™; MicroVention-Terumo, USA) stent are two commonly used stents during endovascular coiling procedures, both having a closed-cell design. The ENTERPRISE2 stent is a self-expanding laser-cut nitinol stent, which offers advantages over braided stents, including good flexibility and stability, high vascular compliance and low rates of thromboembolic events [6]. The LVIS stent is a self-expanding braided nitinol stent, which can provide greater pore density and greater metal surface area coverage, allowing for protection across the aneurysm neck and theoretically a degree of flow diversion [7]. These differences in stent features may be associated with different clinical outcomes between patients treated with laser-cut versus braided stents. It has been reported that laser-cut stents (such as ENTERPRISE 2) are associated with a significantly higher rate of successful deployment and lower rate of periprocedural intracranial hemorrhage; while braided stents (such as LVIS) were associated with a significantly lower rate of permanent morbidity [6].
When comparing the use of ENTERPRISE (including ENTERPRISE 2) versus LVIS in stent-assisted coiling procedures for treating UIA, differences in clinical outcomes have also been demonstrated, including occlusion rates, procedural complications and healthcare resource utilization [8–13]. Though these studies provide useful information, their utility may be limited as they often combined stents of different generations and types, which hinders their generalizability. In addition, other studies revealed inconsistent results in the comparison of clinical outcomes between the two stents [8,9,14].
Studies assessing real-world outcomes, particularly long-term resource utilization, among patients with UIA treated with ENTERPRISE2 versus LVIS stents are currently lacking. The objective of this study was to examine 6-month (180-day) readmission rates among patients with UIA who underwent stent-assisted endovascular coiling using ENTERPRISE 2 stent versus LVIS stent (Figure 1).
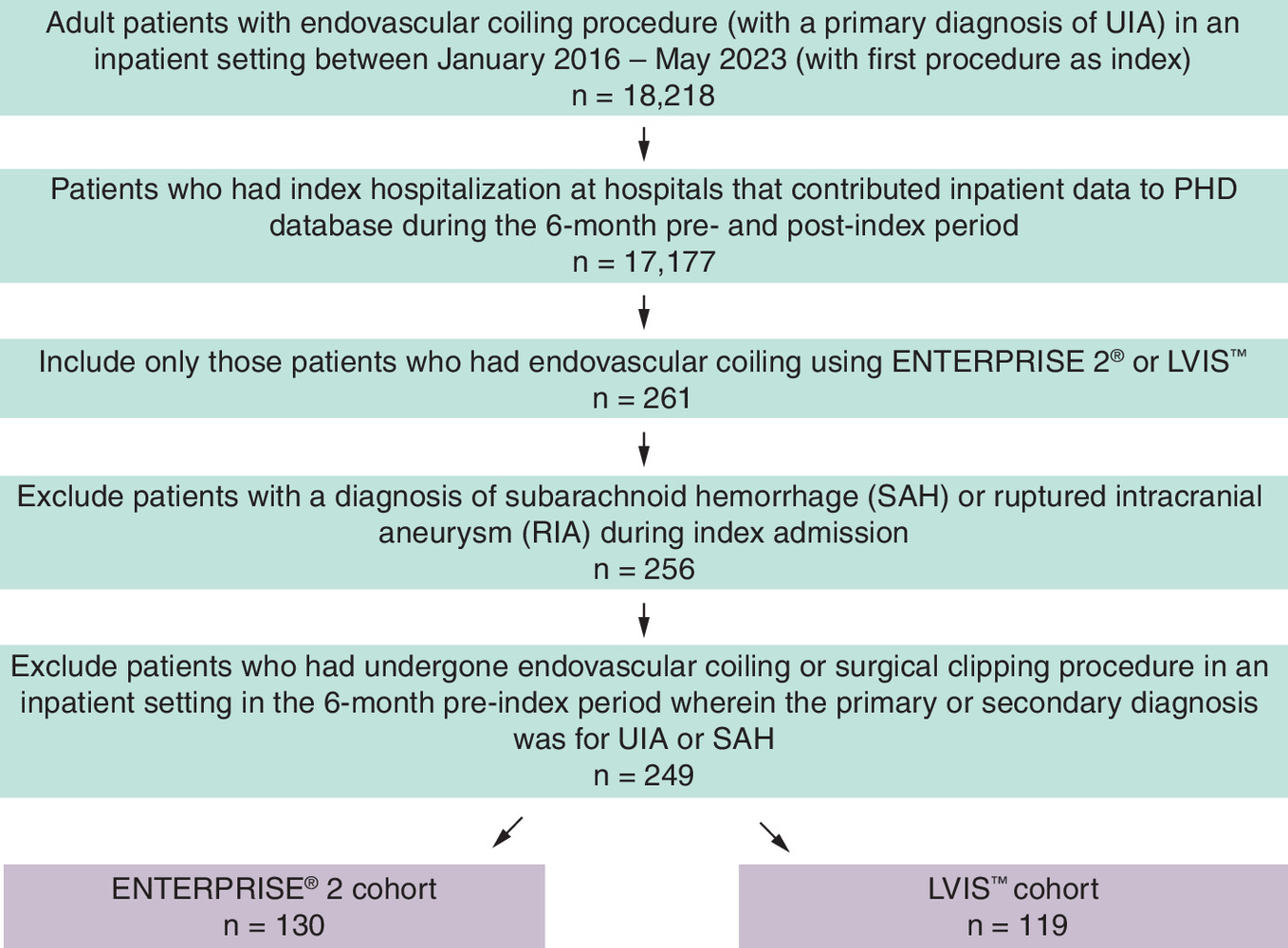
Figure 1. Patients' attrition diagram.
PHD: Premier healthcare database; RIA: Ruptured intracranial aneursym; SAH: Subarachnoid hemorrhage; UIA: Unruptured intracranial aneurysms.
Materials & methods
Data source
Using a retrospective cohort design, the current study analyzed the 2015–2023 Premier Healthcare Database (PHD). The PHD includes billing data from more than 1000 hospitals throughout the US, representing different bed sizes, teaching statuses, and geographic regions. The PHD contains complete clinical coding, hospital cost, and patient billing data from participating hospitals in its healthcare alliance. Medical device use information is also identifiable in the PHD. As dictated by Title 45 Code of Federal Regulations (45 CFR 46.101(b)(4))) (https://www.govinfo.gov/content/pkg/CFR-2011-title45-vol1/pdf/CFR-2011-title45-vol1.pdf), Institutional Review Board (IRB) oversight was not required for our analysis using the PHD.
Study population
Adult patients with a primary diagnosis of UIA (International Classification of Diseases, Tenth Revision, Clinical Modification code: I67.1) undergoing an inpatient SAC procedure with ENTERPRISE 2 stent or LVIS stent (excluding LVIS Jr. stent) between 1 January 2016 and 31 May 2023 were identified. The identification and validation of stents was based on text search strategy that used a combination of manufacturer’s catalog/reference number and device name. The first observed hospital admission during this period meeting these criteria was designated as the index hospital admission. Patients who had dual use of both ENTERPRISE 2 and LVIS stents were excluded. Patients with a concomitant diagnosis of SAH or ruptured aneurysm, or those who had undergone inpatient endovascular coiling or surgical clipping in the180 day pre-index period with a primary diagnosis of UIA or SAH were excluded.
Study covariates
Patient demographic, clinical characteristics and hospital characteristics were evaluated as covariates. Patient demographics included age (18–49, 50–59, 60–69 and 70+ years), sex (male, female), race (white, nonwhite), marital status (married, non-married) and payer type (commercial, Medicare/Medicaid/other). Patient clinical characteristics included the Elixhauser Comorbidity Index score (0–1, 2–3, 4+), comorbidity of diabetes, hypertension, congestive heart failure, transient ischemic attack (TIA) or stroke, obesity and depression, which were captured based on diagnoses present during the index admission. Hospital characteristics included size (<500 beds, 500+ beds), geographic region (Midwest/West, South, Northeast), hospital type (teaching, non-teaching) and 180 day pre-index endovascular coiling procedure volume of the index hospital.
Study outcomes
Study outcomes were 180 day all-cause inpatient readmission, 180-day UIA-related inpatient readmission (i.e., primary diagnosis of UIA), and 180-day UIA-related inpatient retreatment (defined as repeat endovascular coiling procedure in an inpatient setting) in the post-index endovascular coiling procedure period. In PHD, only readmissions related to the original index hospital are identifiable; therefore, our readmission outcomes are confined to those cases who were admitted to the hospital where the index procedure was performed.
Statistical analysis
Descriptive statistics for the two cohorts were reported for all study variables. The inverse probability of treatment weighting (IPTW) of propensity score approach was used to minimize a potential confounders effect and balance the cohorts on study covariates [15]. Each patient was assigned a weight in accordance with IPTW based on the propensity score for receiving either ENTERPRISE 2 stent or LVIS stent. The absolute standardized mean difference (SMD) was used to determine the distribution of covariates among the two cohorts. Covariates were considered well-balanced if the absolute value was within the 0.25 to -0.25 range. To examine study outcomes, bivariate comparisons were conducted post-weighting using chi-square tests. A weighted generalized estimating equation (GEE) model (with exchangeable within cluster correlation and robust variance estimator) with logit link and the binomial distribution function was used to adjust for hospital clustering to account for correlations in outcomes among patients who underwent an index coiling procedure in the same hospital. The Benjamini–Hochberg (BH) correction method was used to control the false discovery rate caused by multiple comparisons for outcomes assessed in the regression analysis. A p-value of <0.05 was considered statistically significant (for BH corrections, the highest p-value smaller than the BH critical value was identified [by using a false discovery rate of 0.10] and all p-values above the highest p-value were considered significant). All analyses were conducted using R software (Version 4.1.2; R Foundation for Statistical Computing, Vienna, Austria).
Results
A total of 249 patients met the study criteria, with 130 patients treated with ENTERPRISE 2 stent and 119 patients with LVIS. Before weighting (Table 1), the ENTERPRISE 2 group had a lower proportion of patients over 60 years of age (52.3% vs 58.0%, absolute SMD [aSMD]: 0.195). The ENTERPRISE2 group had a higher proportion of patients with commercial payor type (50.8% vs 34.5%, aSMD: 0.335) than the LVIS group. Elixhauser score was lower for the ENTERPRISE 2 group (2–3: 36.9% vs 44.5%; 4+: 13.1% vs 18.5%; aSMD: 0.270) versus the LVIS group. ENTERPRISE2 group had a lower proportion of patients with hypertension (60.8% vs 73.1%, aSMD: 0.265) and obesity (5.4% vs 13.4%, aSMD: 0.279) compared with those who were treated by the LVIS stent. A lower proportion of patients from the ENTERPRISE 2 group were treated in teaching hospitals (76.9% vs 94.1%, aSMD: 0.504) versus those in the LVIS group. Study cohorts were well-balanced for all covariates after weighting (aSMD <0.25).
| Pre-weighted | Post-weighted | |||||
|---|---|---|---|---|---|---|
| ENTERPRISE® 2, n (%) | LVIS™, n (%) | aSMD | ENTERPRISE® 2, % | LVIS™, % | aSMD | |
| 130 | 119 | |||||
| Age range, (years) | 0.195 | 0.122 | ||||
| 18–49 | 28 (21.5%) | 18 (15.1%) | 17.4% | 15.4% | ||
| 50–59 | 34 (26.2%) | 32 (26.9%) | 26.5% | 31.9% | ||
| 60–69 | 35 (26.9%) | 40 (33.6%) | 31.0% | 29.7% | ||
| 70+ | 33 (25.4%) | 29 (24.4%) | 25.1% | 23.0% | ||
| Sex | 0.110 | 0.007 | ||||
| Male | 38 (29.2%) | 29 (24.4%) | 26.0% | 26.3% | ||
| Female | 92 (70.8%) | 90 (75.6%) | 74.0% | 73.7% | ||
| Race | 0.004 | 0.007 | ||||
| White | 97 (74.6%) | 89 (74.8%) | 76.0% | 76.3% | ||
| Non-white | 33 (25.4%) | 30 (25.2%) | 24.0% | 23.7% | ||
| Marital status | 0.300 | 0.049 | ||||
| Married | 75 (57.7%) | 51 (42.9%) | 49.7% | 47.8% | ||
| Non-married | 55 (42.3%) | 68 (57.1%) | 50.3% | 52.2% | ||
| Payor type | 0.335 | 0.088 | ||||
| Commercial | 66 (50.8%) | 41 (34.5%) | 42.7% | 47.1% | ||
| Medicare/Medicaid/other | 64 (49.2%) | 78 (65.5%) | 57.3% | 52.9% | ||
| Elixhauser score | ||||||
| 0–1 | 65 (50.0%) | 44 (37.0%) | 0.270 | 42.0% | 45.5% | 0.072 |
| 2–3 | 48 (36.9%) | 53 (44.5%) | 43.0% | 40.1% | ||
| 4 and above | 17 (13.1%) | 22 (18.5%) | 15.0% | 14.4% | ||
| Diabetes | 20 (15.4%) | 24 (20.2%) | 0.125 | 16.6% | 15.5% | 0.030 |
| Hypertension | 79 (60.8%) | 87 (73.1%) | 0.265 | 66.7% | 60.9% | 0.123 |
| Congestive heart failure | 3 (2.3%) | 2 (1.7%) | 0.045 | 2.2% | 2.2% | 0.001 |
| TIA/stroke | 22 (16.9%) | 26 (21.8%) | 0.125 | 16.7% | 16.3% | 0.012 |
| Obesity | 7 (5.4%) | 16 (13.4%) | 0.279 | 10.1% | 9.3% | 0.029 |
| Depression | 13 (10.0%) | 21 (17.6%) | 0.223 | 11.7% | 12.0% | 0.010 |
| Hospital beds size | 0.062 | 0.065 | ||||
| <500 | 18 (13.8%) | 14 (11.8%) | 12.2% | 14.4% | ||
| 500+ | 112 (86.2%) | 105 (88.2%) | 87.8% | 85.6% | ||
| Hospital region | 0.190 | 0.088 | ||||
| Midwest/West | 22 (16.9%) | 25 (21.0%) | 21.8% | 18.3% | ||
| Northeast | 9 (6.9%) | 13 (10.9%) | 7.5% | 7.9% | ||
| South | 99 (76.2%) | 81 (68.1%) | 70.7% | 73.8% | ||
| Hospital type | 0.504 | 0.150 | ||||
| Teaching | 100 (76.9%) | 112 (94.1%) | 84.3% | 78.5% | ||
| Non-teaching | 30 (23.1%) | 7 (5.9%) | 15.7% | 21.5% | ||
| Endovascular coiling volume (mean, SD) | 27.58 (13.77) | 28.09 (12.92) | 0.038 | 27.38 (14.35) | 27.44 (12.90) | 0.004 |
aSMD: Absolute standard mean difference; SD: Standard deviation.
As showed in Table 2, the bivariate analysis after weighting revealed that patients treated with ENTERPRISE 2 stent had significantly lower rates of all-cause inpatient readmission and UIA-related inpatient readmission in the 180-day post-SAC procedure period compared with those who were treated with LVIS stent (all-cause readmission: 9.1% vs 24.3%, chi-square p = 0.016; UIA-related readmission: 2.6% vs 12.4%, chi-square p = 0.036). No significant differences in 180-day UIA-related retreatment was observed between the ENTERPRISE2 and LVIS groups (2.6% vs 11.6%, chi-square p = 0.056). Results from the GEE regression analysis (Table 3) suggested that patients treated with ENTERPRISE 2 stent had a 69% lower risk of 180-day all-cause inpatient readmission as compared with those treated with LVIS stent (odds ratio [OR]: 0.31, 95% CI: 0.12–0.82], p = 0.018). No significant difference in 180-day UIA-related inpatient readmission and retreatment was observed among the ENTERPRISE 2 cohort versus LVIS cohort (UIA-related readmission: OR: 0.19, 95% CI: 0.03–1.04, GEE p = 0.056; UIA-related retreatment: OR: 0.20, 95% CI: 0.03–1.20, GEE p = 0.079).
| Outcomes in 180 days post index | ENTERPRISE® 2† | LVIS™† | Chi-square test, p-value | Absolute rate difference |
|---|---|---|---|---|
| All-cause inpatient readmission | 11.8/129.4 (9.1%) | 30.5/125.5 (24.3%) | 0.016 | -15.2% (-30.2% to -0.2%) |
| UIA-related inpatient readmission‡ | 3.4/129.4 (2.6%) | 15.6/125.5 (12.4%) | 0.036 | -9.8% (-24.9% to 5.2%) |
| UIA-related retreatment§ | 3.4/129.4 (2.6%) | 14.6/125.5 (11.6%) | 0.056 | -9.0% (-24.1% to 6.0%) |
†
Counts and rates of weighted cohort.
‡
UIA-related inpatient readmission was defined as hospitalization with a primary diagnosis of UIA.
§
UIA-related retreatment was defined as inpatient endovascular coiling procedure with a primary diagnosis of UIA.
¶
The results after Benjamini–Hochberg (BH) correction remained consistent and indicated significant differences for all-cause readmission.
UIA: Unruptured intracranial aneurysm.
| Outcomes in 180 days post index | Odds ratio | 95% Confidence interval | GEE regression model, p-value¶ |
|---|---|---|---|
| All-cause inpatient readmission† | 0.31 | 0.12–0.82 | 0.018 |
| UIA-related inpatient readmission‡ | 0.19 | 0.03–1.04 | 0.056 |
| UIA-related retreatment§ | 0.20 | 0.03–1.20 | 0.079 |
†
All-cause inpatient readmission cases were from 22 hospitals.
‡
UIA-related inpatient readmission was defined as hospitalization with a primary diagnosis of UIA. UIA-related inpatient readmission cases were from 8 hospitals.
§
UIA-related retreatment was defined as inpatient endovascular coiling procedure with a primary diagnosis of UIA. UIA-related retreatment cases were from 7 hospitals.
¶
The results after Benjamini Hochberg (BH) correction remained consistent and indicated significant differences for all-cause readmission.
GEE: Generalized estimating equation; UIA: Unruptured intracranial aneurysm.
Discussion
In this retrospective cohort study using a US hospital-based database, patients with UIA who underwent stent-assisted endovascular coiling using the ENTERPRISE2 versus LVIS stent were 69% less likely to have an all-cause inpatient readmission in the 180 days post procedure period. When examining the underlying primary diagnosis associated with these admissions, 70% of all all-cause admissions were observed to be aneurysm-related. Bivariate analysis revealed a significantly lower rate of 180-day UIA-specific inpatient readmission among ENTERPRISE 2 cohort versus LVIS cohort; however, this difference was not significant in GEE analysis. No significant difference was observed for 180-day UIA-related retreatment (repeat inpatient endovascular coiling procedure) among the study cohorts.
A few studies that have compared outcomes among patients with UIA who underwent endovascular SAC using ENTERPRISE stents versus LVIS stents have reported mixed clinical results [9–14,16]. Some studies have demonstrated the use of LVIS stents was associated with improved procedural outcomes, such as significantly higher rates of complete and near-complete occlusion rates [8–10], greater reduction in velocity at the neck plane and wall shear stress on the aneurysm [11], and higher flow diversion effect [12] as compared with ENTERPRISE stent. In regard to complications, however, a study by Wang et al. found a greater rate of intra-procedural stent related thrombotic events in the LVIS group as compared with other stents including ENTERPRISE [10]. Similar to readmission outcomes, another study by De Leacy et al. found UIA patients using ENTERPRISE stent to have significantly lower risk of UIA-related inpatient readmissions 1 year post SAC procedure versus other stent users, including LVIS [13]. Notably, there are other studies that have reported no significant difference in in-stent stenosis [14], occlusion rate [14], recanalization rates [14] and procedural-related complications [8,9], between the ENTERPRISE and LVIS stents. Though informative, none of these studies specifically focused on the ENTERPRISE 2 stent (excluding the first-generation ENTERPRISE stent), and LVIS stent (excluding the LVIS Jr. stent) thereby limiting their utility to impact decision making as it pertains to the use of these two stents.
To our knowledge, ours is the first study that compares readmission outcomes between LVIS stent versus ENTERPRISE 2 stent. The second-generation ENTERPRISE 2 stent was designed to improve stent-wall apposition in complex and curved vessels, to avoid kinking and to provide enhanced radio-opacity under fluoroscopy [17,18]. The decreased likelihood of readmission outcomes associated with ENTERPRISE 2 stent versus LVIS stent observed in our study could potentially be in part related to these aforementioned improvements and iterations in laser cut stent design and fabrication when compared with braided stents, such as the LVIS stent. The ENTERPRISE 2 stent has easier visualization in a deployed state, higher deployment accuracy with limited foreshortening, and preserved ease for navigation through tortuous anatomy. Furthermore, the ENTERPRISE 2 stent has higher strut tension and compression strength, which may lead to less deformation during microcatheter operation [19]. The arrangement of filaments can change in braided stents as they adapt to the curvature of the parent vessel, resulting in a variable metal coverage [20]. This variation, along with the potential for a ‘flow diversion’ effect with braided stents, might increase the risk of occlusion in branch vessels or within the stent construct itself [20]. Additionally, braided stents shorten significantly during the transition from constrained to unconstrained during deployment, whereas the laser cut stents tend not to shorten to a significant between pre and after deployment [20]. The stability in the ENTERPRISE2 stent possibly result in greater ease of successful deployment and lower occurrence of intraprocedural complications [6], such as nontarget deployment, which could potentially decrease the risk of readmissions post procedure.
There are limitations in the current study. Firstly, the PHD can only assess a readmission if the patient returned to the same hospital. As such, our rate of readmission may underestimate the true rate of readmission. This limitation, however, is likely to cause non-differential bias and will not affect the directionality of our results. Second, a combination of the device name and catalog identifiers was used for the device search strategy. This method may have led to device misidentification. Third, the hospitals that are not federally funded and that are based in the US are not covered by the PHD. We also only focused on inpatient procedures within US hospitals. These may all lead to less generalizability of our findings. Additionally, the data we collected lacked specificity in determining patients with wide-neck aneurysms, clinical details including the precise location or size of the aneurysm, neck morphology, antiplatelet therapy or surgeon-level data (e.g. experiences). Potential differences in these factors between the two groups (residual confounding) might explain the observed difference in readmission outcomes. Moreover, relatively small sample size of this study may limit the statistical power for detecting differences in outcomes of UIA-related readmission and retreatment.
Conclusion
Among patients with UIA who underwent SAC procedures with data tracked and collected from the Premier Healthcare Database (PHD), treatment with the laser-cut ENTERPRISE 2 stent were associated with significantly lower risk of all-cause inpatient readmission in the 6-month (180-day) period following the procedure when compared with the use of LVIS stent. No statistically significant differences were found in UIA-related readmission and retreatment. As SAC procedures form the mainstay endovascular treatment option for wide-necked UIA, the uniqueness of ENTERPRISE 2 stent could potentially offer incremental improvements in patient outcomes as compared with the LVIS stent.
Summary points
•
Stent-assisted coiling (SAC) procedure has emerged as the mainstay endovascular treatment option for wide-necked unruptured intracranial aneurysms (UIA). Differences in stent features, such as laser-cut (ENTERPRISE® 2 stent) versus braided (LVIS™ stent) stents, may be associated with different clinical outcomes.
•
This observational cohort study assessed 180-day all-cause inpatient readmissions, UIA-related inpatient readmissions and UIA-related retreatment in patients with UIA who underwent SAC with the ENTERPRISE2 stent versus LVIS stent.
•
Data from 249 patients with UIA treated with SAC using ENTERPRISE2 stent versus LVIS stent between 2016 and 2023 were identified from the Premier Healthcare Database (US hospital-based database).
•
Patients who underwent SAC using the ENTERPRISE2 stent were 69% less likely to have 180-day post-procedure all-cause inpatient readmissions as compared with those treated using the LVIS stent.
•
No significant differences in 180-day UIA-related inpatient readmissions and retreatment were observed between the ENTERPRISE2 cohort and LVIS cohort.
Author contributions
All authors were responsible for study conception and design; R Khanna and Y Rong were responsible for acquisition of data; R Khanna and Y Rong were responsible for data analysis. All authors contributed to draft review and revision of the manuscript.
Financial disclosure
This work was supported by Johnson & Johnson MedTech Neurovascular (USA).
Competing interests disclosure
R De Leacy has received consulting fees and participated on a scientific advisory board for Johnson & Johnson MedTech Neurovascular, and served as the secretary for the Society of Neuro Interventional Surgery (2022–2023). R Khanna, E Kottenmeier and Y Rong are employed by Johnson & Johnson. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing disclosure
No funded writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The use of Premier Healthcare Database (PHD) was reviewed by the New England Institutional Review Board (IRB) and was determined to be exempt from broad IRB approval, as this study does not involve human subjects’ research. Confidentiality of data subject records were maintained at all times. All study reports contained aggregate data only and did not identify individual data subjects or physicians.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Vlak MH, Algra A, Brandenburg R, Rinkel GJ. Prevalence of unruptured intracranial aneurysms, with emphasis on sex, age, comorbidity, country, and time period: a systematic review and meta-analysis. Lancet Neurol. 10(7), 626–636 (2011).
2.
Korja M, Lehto H, Juvela S. Lifelong rupture risk of intracranial aneurysms depends on risk factors. Stroke 45(7), 1958–1963 (2014).
3.
Brown RD. Unruptured intracranial aneurysms. Semin. Neurol. 30(5), 537–544 (2010).
4.
Smith GA, Dagostino P, Maltenfort MG, Dumont AS, Ratliff JK. Geographic variation and regional trends in adoption of endovascular techniques for cerebral aneurysms. J. Neurosurgeons 114(6), 1768–1777 (2011).
5.
Kadkhodayan Y, Rhodes N, Blackburn S, Derdeyn CP, Cross DT, Moran CJ. Comparison of ENTERPRISE with Neuroform stent-assisted coiling of intracranial aneurysms. Am. J. Roentgenol. 200(4), 872–878 (2013).
6.
Zhang L, Chen X, Dong L et al. Clinical and angiographic outcomes after stent-assisted coiling of cerebral aneurysms with laser-cut and braided stents: a comparative analysis of the literatures. Front. Neurol. 12, 666481 (2021).
• This literature review evaluates outcomes of stent-assisted coiling (SAC) using laser-cut versus braided stents and found that braided stents were associated with lower rates of permanent morbidity, whereas laser-cut stents was linked to higher successful-deployment rates and lower rates of periprocedural intracranial hemorrhage.
7.
Turner RD, Turk A, Chaudry I. Low-profile visible intraluminal support device: immediate outcome of the first three US cases. J. Neurointerv. Surg. 5(2), 157–160 (2013).
8.
Ge H, Lv X, Yang X, He H, Jin H, Li Y. LVIS Stent vrsus ENTERPRISE stent for the treatment of unruptured intracranial aneurysms. World Neurosurg. 91, 365–370 (2016).
9.
Wu ZP, Yin JL, Liu SK et al. ENTERPRISE stents versus low-profile visualized intraluminal support stents for stent-assisted coiling of unruptured paraclinoid aneurysms. Technol. Health Care 31(5), 1855–1865 (2023).
10.
Wang J, Vargas J, Spiotta A et al. Stent-assisted coiling of cerebral aneurysms: a single-center clinical and angiographic analysis. J. Neurointerv. Surg. 10(7), 687–692 (2018).
11.
Li W, Wang Y, Zhang Y et al. Efficacy of LVIS vs. ENTERPRISE stent for endovascular treatment of medium-sized intracranial aneurysms: a hemodynamic comparison study. Front. Neurol. 10, 522 (2019).
12.
Sato H, Haraguchi K. Comparison of stent-assisted coiling for unruptured internal carotid artery aneurysms between LVIS or LVIS Jr. and ENTERPRISE VRD: a retrospective and single-center analysis. Turk. Neurosurg. 31(3), 379–384 (2021).
13.
Leacy RD, Kottenmeier E, Lee SH, Khanna R, Spiotta AM. Endovascular treatment with the ENTERPRISE stent versus the Neuroform or low-profile visualized intraluminal support stent for unruptured aneurysms. J. Comp. Eff. Res. 10(4), 295–305 (2021).
•• This retrospective cohort study suggests that ENTERPRISE stent use was associated with significantly lower risk of readmissions versus other stents including LVIS stent.
14.
Feng X, Qian Z, Liu P et al. Comparison of recanalization and in-stent stenosis between the low-profile visualized intraluminal support stent and ENTERPRISE stent-assisted coiling for 254 intracranial aneurysms. World Neurosurg. 109, e99–e104 (2018).
15.
Austin PC, Stuart EA. Moving towards best practice when using inverse probability of treatment weighting (IPTW) using the propensity score to estimate causal treatment effects in observational studies. Stat. Med. 34(28), 3661–3679 (2015).
16.
Li Z, Xuan J, Fang X et al. Comparison of ENTERPRISE Stent 2 with 1 in assisting coiling of ruptured aneurysms: a real-world study. J. Comp. Eff. Res. 11(12), 879–887 (2022).
17.
Kono K, Terada T. In vitro experiments of vessel wall apposition between the ENTERPRISE and ENTERPRISE 2 stents for treatment of cerebral aneurysms. Acta Neurochirurgica 158(2), 241–245 (2016).
18.
Chihara H, Ishii A, Kikuchi T et al. Deployment technique that takes advantage of the characteristics of ENTERPRISE VRD2: an in vitro study. J. Neurointerv. Surg. 9(10), 969–973 (2017).
19.
Iwakami T, Fujii N, Son J. Comparison of the physical characteristics of support stents for cerebral aneurysm embolization. J. Neuroendovasc. Ther. 15(12), 778–786 (2021).
20.
Cho SH, Jo WI, Jo YE, Yang KH, Park JC, Lee DH. Bench-top comparison of physical properties of 4 commercially-available self-expanding intracranial stents. Neurointervention 12(1), 31–39 (2017).
Information & Authors
Information
Published In
Copyright
© 2026 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 11 October 2025
Accepted: 13 March 2026
Published online: 13 April 2026
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Readmissions and retreatment among stent-assisted endovascular coiling patients with unruptured intracranial aneurysm using ENTERPRISE® 2 stent versus LVIS™ stent. (2026) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2025-0166
Export citation
Select the citation format you wish to export for this article or chapter.