Antiretroviral therapy persistence among treatment-experienced people with HIV and mental health disorders and/or substance use disorders in the USA (2017–2024): a retrospective cohort study
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: There are limited studies of antiretroviral therapy persistence among people with HIV (PWH) who have a mental health disorder and/or substance use disorder (MHD/SUD). This real-world study analyzed persistence among treatment-experienced PWH who had an MHD/SUD or suboptimal adherence (proportion of days covered [PDC] < 85%). Materials & methods: In this retrospective cohort study of claims from the Optum Research Database, nonpersistence (i.e., discontinuation, switch, add-on or death) was assessed in treatment-experienced PWH who switched to or restarted an antiretroviral therapy regimen of interest (i.e., bictegravir [B]/emtricitabine [F]/tenofovir alafenamide [TAF], dolutegravir [DTG]/lamivudine [3TC], DTG/abacavir [ABC]/3TC, DTG + F/TAF, DTG + F/tenofovir disoproxil fumarate [TDF] or cabotegravir + rilpivirine) from 1 July 2017 to 30 November 2023. Baseline characteristics across regimens were balanced by inverse probability treatment weighting. Kaplan–Meier analysis was conducted on weighted data to examine regimen persistence at 12 months. Adjusted Cox proportional hazards models assessed nonpersistence throughout follow-up. Results: Overall, 14,826 PWH were eligible and treatment experienced; 5310 had an MHD/SUD and 4090 had PDC < 85% during follow-up. Among treatment-experienced PWH who received B/F/TAF, persistence at 12 months was 80.3% for those with an MHD/SUD and 78.6% for those with PDC < 85%; this was greater compared with PWH who received DTG/3TC (76.7% and 70.8%), DTG/ABC/3TC (68.9% and 66.3%), DTG + F/TAF (62.4% and 58.9%) and DTG + F/TDF (36.7% and 41.9%; all p < 0.05). Compared with B/F/TAF, nonpersistence risk was greater with DTG/3TC, DTG/ABC/3TC, DTG + F/TAF and DTG + F/TDF in the MHD/SUD (all p < 0.05) and PDC < 85% (all p < 0.05 except DTG/3TC) groups. Conclusion: These results indicate that B/F/TAF may offer greater likelihood of persistence and emphasize the importance of regimen selection to optimize outcomes in treatment-experienced PWH with an MHD/SUD or suboptimal adherence.
Plain Language Summary: How many people with HIV & mental health or substance use issues stay on antiretroviral therapy after restarting or switching their regimen?
Why is this important?
People with HIV often face challenges that make it hard to stay on their HIV treatment, such as mental health issues and problems with alcohol or drugs. Discontinuing treatment can lead to negative health outcomes. In this study, we looked at how long people stayed on different HIV treatment combinations when they had these challenges.
What was done?
We used health insurance records from July 2017 through November 2023 to find people with HIV who switched to or restarted 1 of 6 modern treatment regimens. We then measured how many people were still taking their treatment after 12 months. We compared groups in a way that balanced factors such as age, race and other characteristics across the six regimens.
What were the results?
Out of 14,826 people with HIV, 5310 had mental health or substance use issues. After 12 months, 80% of those with HIV and mental health or substance use issues who were taking the combination of bictegravir/emtricitabine/tenofovir alafenamide (B/F/TAF) were still on treatment. This rate was higher than rates for the other regimens studied, including several dolutegravir-based regimens.
What do these results mean?
These findings suggest that the B/F/TAF combination may help people with HIV with mental health or substance use issues to stay on their treatment longer. Choosing the right treatment plan can improve long-term health for people with HIV.
Despite advances in modern antiretroviral therapy (ART), HIV remains a serious public health concern [1]. As of 2022, there were an estimated 1.2 million adolescents and adults living with HIV in the USA [2]. Adherence to and persistence with ART are essential for the effective long-term management of HIV [3]. Adherence has been defined as, “the extent to which a patient acts in accordance with the prescribed interval, and dose of a dosing regimen”, and persistence as, “the duration of the time from initiation to discontinuation of therapy” [4]. Suboptimal adherence or discontinuation of ART in people with HIV (PWH) heightens the risk of viral rebound, which can increase morbidity and mortality [3,5–7].
PWH experience high rates of mental health disorders (MHDs) and substance use disorders (SUDs). One observational study evaluated 122,896 PWH in the USA and Canada over a 10-year period (2008–2018) and found that 55% had been diagnosed with ≥ 1 MHD, with depressive disorders and anxiety being the most common (in 39% and 28% of PWH, respectively) [8]. A separate study conducted across seven urban sites in the USA found an overall prevalence of SUDs among PWH of 48%, which ranged from 21% to 71% across sites [9]. The most common (> 15% of PWH) substances used were marijuana (31%) and alcohol (19%).
In PWH and co-occurring MHDs and/or SUDs (MHDs/SUDs), the associated challenges are overlapping and can compound, leading to poor viral suppression and worse outcomes on the HIV care continuum [10,11]. This situation is underscored in US Department of Health and Human Services guidelines, which recognize challenges for PWH and ongoing SUDs, including difficulty getting diagnosed with HIV, initiating ART, and adhering to ART, as well as the prevalence of co-occurring MHDs [3]. Among PWH who have MHDs/SUDs, factors that can make adhering to ART challenging include unstable housing, lack of social support and social stigma, among others [3,10]. Indeed, among PWH, MHDs and SUDs are associated with suboptimal adherence and persistence to ART [12,13].
Persistence to ART is key to achieving and maintaining viral suppression and thus preventing transmission (underlying the Undetectable = Untransmittable campaign) [14]. As such, one of the remaining challenges to ending the HIV epidemic is maintaining viral suppression among the PWH who face challenges in adherence. A recent analysis of contemporary ART regimens found that nearly two-thirds of PWH were nonadherent in the first year of initiating ART [15]. Some ART regimens have been shown to be associated with viral suppression in the context of suboptimal adherence. For example, a pooled analysis of Phase III studies found that viral suppression in PWH with suboptimal adherence (< 85%) was similar to that of those with intermediate (≥ 85% – < 95%) and high (≥ 95%) adherence for those in the bictegravir (B)/emtricitabine (F)/tenofovir alafenamide (TAF) group but was significantly lower for those in the dolutegravir (DTG) + 2 nucleoside reverse transcriptase inhibitors group [16]. Given the association between MHDs/SUDs and HIV as well as the considerable overlap with MHDs, SUDs and suboptimal adherence, optimizing treatment selection for these groups of PWH is an important step in ending the HIV epidemic [10].
A variety of effective ART regimens are available for the treatment of HIV. The US Department of Health and Human Services guidelines recommend B/F/TAF, DTG + F or lamivudine (3TC) + TAF or tenofovir disoproxil fumarate (TDF), or DTG/3TC for treatment-naive PWH who do not have a history of using long-acting cabotegravir (CAB) for pre-exposure prophylaxis; these newer integrase strand transfer inhibitor (INSTI)–based regimens have demonstrated virologic efficacy, favorable tolerability and safety, and ease of use [3]. However, ART regimens vary in tolerability profiles, pill burden and associated rates of discontinuation or modification [3,17]. For instance, multi-tablet regimens are associated with lower adherence compared with single-tablet regimens [18,19]. This variation in tolerability and pill burden could lead to differences in treatment persistence and downstream consequences affecting health outcomes.
While many studies have evaluated persistence for PWH among those newly initiating ART [17–19], there is a need to better understand ART treatment patterns among treatment-experienced PWH because long-term persistence may be influenced by medication-, psychosocial- and/or economic-related challenges [20]. There is a lack of comprehensive data on real-world persistence patterns with modern ART regimens among PWH at high risk of nonpersistence, such as those with an MHD/SUD or suboptimal adherence. Gaining a deeper understanding of ART persistence among these populations could enhance clinical decision-making and contribute to improved outcomes for PWH. The objective of this study was to describe and compare ART regimen persistence for PWH after switching or restarting ART among those with an MHD/SUD or suboptimal adherence to ART.
Materials & methods
Study design
This was a retrospective analysis of medical and pharmacy claims data for individuals with commercial insurance or Medicare Advantage with Part D coverage from the Optum Research Database. The Optum Research Database allows for longitudinal analyses of patients, tracking them across plans and enrollment periods. It contains closed medical and pharmacy claims and is one of the largest and most comprehensive US claims databases.
The study period was from 1 January 2007 to 29 February 2024 (Supplementary Figure 1). The index date was the earliest date with evidence of newly switching or restarting an ART regimen during the identification period, which was from 1 July 2017 to 30 November 2023. This ART regimen was the index regimen. The identification period allowed for analyses of the ART regimens of interest after they had been on the market for > 2 years and for a lookback period of ≥ 10 years to determine prior ART experience. The baseline period was defined as 6 months prior to the index date. Follow-up was for ≥ 3 months, starting on the index date and ending at the end of the study period or at the end of the regimen.
The ART regimens of interest included B/F/TAF, DTG/3TC, DTG/abacavir (ABC)/3TC, DTG + F/TAF, DTG + F/TDF and CAB + rilpivirine (RPV). PWH were prescribed ART regimens by their healthcare provider.
Study population
The main eligibility criteria for this study were age ≥ 18 years; nonmissing age, sex, geographic region and insurance type; ≥ 1 claim with an HIV diagnosis in any position on the claim during the identification period; ≥ 1 claim for an ART regimen of interest during the identification period; and continuous enrollment in a commercial or Medicare Advantage health plan with both pharmacy and medical benefits for ≥ 6 months prior to the index date and for ≥ 3 months following the index date. The study population was further limited to PWH who were treatment experienced such that they had evidence of ART since 1 January 2007, with either the most recent ART being the same as the index regimen, with a treatment gap of ≥ 90 days before the start of the index regimen, or the ART before the index ART being different than the index ART.
The current analysis was conducted in two subsets of these treatment-experienced PWH: those who had an MHD/SUD and those who had low adherence to the index ART regimen during the follow-up period. PWH in the MHD/SUD group had ≥ 1 diagnosis of an MHD or SUD (or both). MHDs and SUDs were identified using International Classification of Diseases, Tenth Revision, Clinical Modification diagnosis and procedure codes and revenue codes (Supplementary Table 1). Suboptimal adherence was defined as having a proportion of days covered (PDC) < 85% during the follow-up period. PDC was calculated as the percentage of days, from the index date to the earliest of regimen discontinuation, switch, add-on, health plan disenrollment, death or data cutoff (29 February 2024), with disenrollment and cutoff treated as censoring events, during which PWH had their index medication(s) on hand (≥ 1 for multi-tablet regimens, or the single medication for single-tablet regimens).
Variables
Study variables included baseline demographic and clinical characteristics. Baseline adherence was also assessed and was defined as the PDC during the baseline period. This was calculated as the percentage of days, from the first date with a diagnosis of HIV or a claim for any ART (not limited to the ART regimens of interest) to the day before the index date, during which PWH had ≥ 1 ART medication on hand.
The main outcome of this study was nonpersistence, which was assessed during the follow-up period. Nonpersistence was defined as the earliest evidence of ART discontinuation (defined as a gap of all components of the index ART regimen for ≥ 90 days without initiating a new regimen; for an individual who discontinued, the regimen end date was defined as the day before the ≥ 90-day gap began), ART switch (defined as either discontinuation of some, but not all, of the medications in the index regimen or discontinuation of all medications in the regimen and start of a new regimen), ART add-on (defined as continuation of all medications in the index regimen with the addition of ≥ 1 new medication; medications from the index regimen were carried forward to the second regimen if the individual had a refill of the medication after the start of the second regimen but before the individual experienced a ≥ 90-day gap) or death. Data on mortality were captured from a variety of sources in order to provide the most complete information on death available, including the Social Security Administration Death Master File. PWH whose regimen ended because they disenrolled from the health plan or reached the end of available data were administratively censored at the end of their regimen.
Statistical analysis
Baseline demographic and clinical characteristics were recorded and analyzed descriptively. Differences in baseline adherence parameters between PWH receiving B/F/TAF and those receiving comparator regimens were evaluated by Z-test using robust standard error in least squares regression for continuous measures and logistic regression for binary measures. Inverse probability treatment weighting (IPTW) was conducted prior to nonpersistence analyses to balance demographic characteristics, baseline clinical measures and baseline healthcare costs and utilization across ART regimens in the overall study population (Supplementary Table 2). Weights were stabilized, and adjusted Cox proportional hazards models were used to control for any imbalances after weight stabilization. After IPTW, Z-tests with robust standard errors were used to determine statistical differences in baseline characteristics between the B/F/TAF and comparator regimen groups.
Kaplan–Meier analysis was used to estimate time to nonpersistence through 12 months and the proportion of PWH persistent on their ART regimen at 12 months; differences in the proportion of persistent PWH between B/F/TAF and the other regimens were calculated using the log-rank test. Adjusted hazard ratios (HRs), corresponding 95% CIs and p-values were calculated for the risk of nonpersistence over the entire follow-up period using Cox proportional hazards models. Post-IPTW nonpersistence analyses were conducted separately for the two groups of treatment-experienced PWH – those with an MHD/SUD at baseline and those with suboptimal adherence to the index ART regimen during follow-up. To adjust for any imbalances across regimens in the two groups after IPTW, all models were weighted and adjusted for covariates.
As this was a secondary analysis of existing data, institutional review board or independent ethics committee review and informed consent were not required. Patient identifiers in all data sources were removed, and the data contained no patient-identifiable fields. Patients’ anonymity was strictly maintained, and the data source was compliant with the Health Insurance Portability and Accountability Act.
Results
Study population
Among 113,705 people diagnosed with HIV-1 during the identification period, 48,902 people received an ART regimen of interest during the identification period, 20,254 people were adults who were continuously enrolled and 14,826 met all eligibility criteria and were considered treatment experienced (Figure 1).
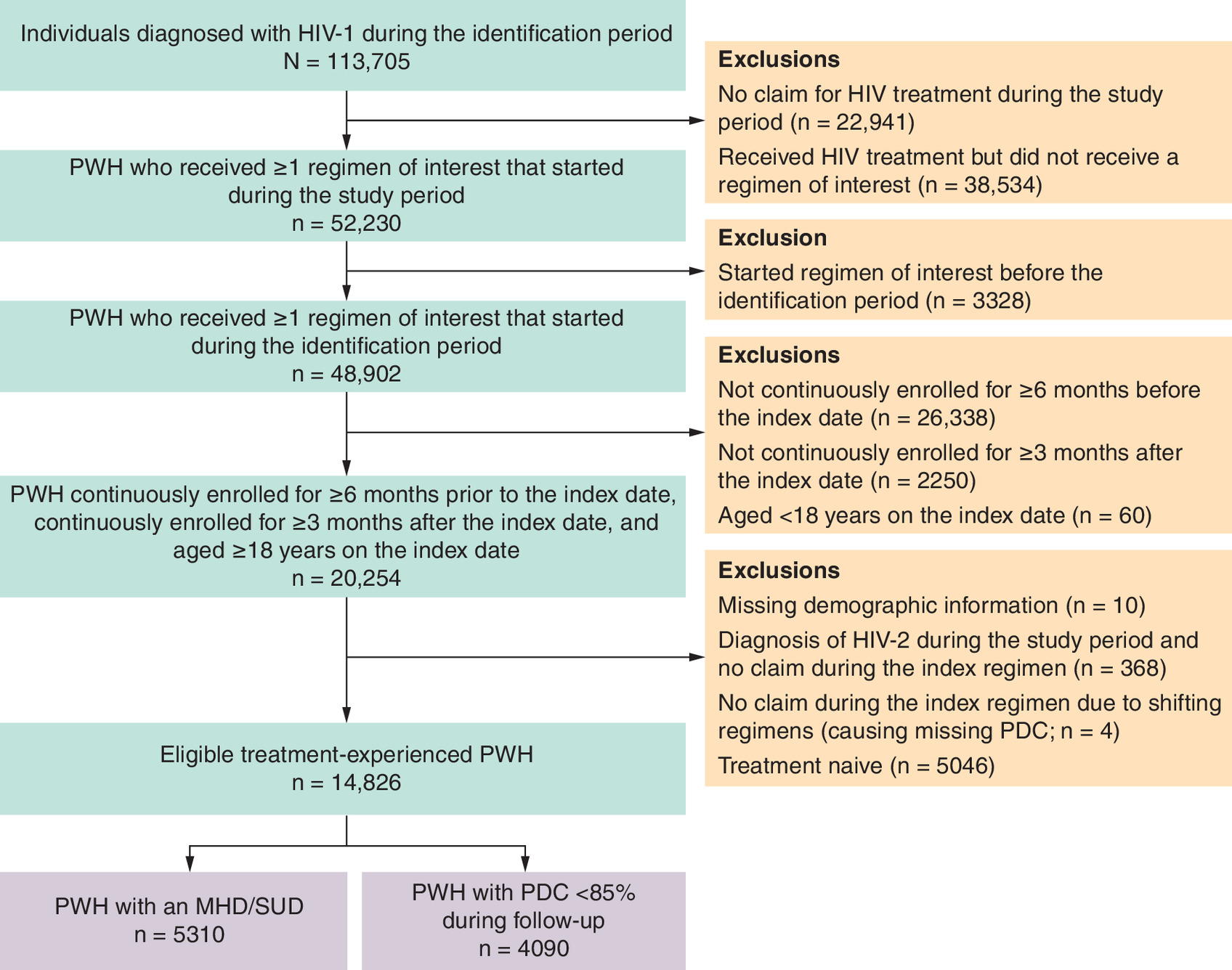
Figure 1. Study population attrition.
MHD: Mental health disorder; PDC: Proportion of days covered; PWH: People with HIV; SUD: Substance use disorder.
A total of 5310 (35.8%) PWH had an MHD/SUD at baseline (Table 1). The mean (standard deviation [SD]) age of PWH in the MHD/SUD group was 54.0 (12.3) years, 78.0% were male, 47.0% were White, 30.5% were African American/Black and 59.2% were located in the South. Overall, 91.4% of PWH had an MHD, 47.1% had a severe MHD and 24.5% had an SUD. Adherence to prior ART during the baseline period varied between PWH who received B/F/TAF on the index date and those who received other regimens on the index date (Table 2). The proportion of PWH with a > 90-day gap in all HIV medications during the baseline period was higher among those who received DTG/ABC/3TC (51.6%) or DTG + F/TDF (33.3%) and lower among those who received DTG/3TC (10.2%) or CAB + RPV (10.1%) compared with those who received B/F/TAF (22.7%; all p < 0.05). Similarly, mean (SD) PDC was lower among PWH who received DTG/ABC/3TC (66.4% [30.6%]), DTG + F/TAF (74.3% [28.2%]) or DTG + F/TDF (69.6% [29.7%]) and higher among those who received DTG/3TC (83.2% [19.2%]) or CAB + RPV (82.5% [18.3%]) compared with those who received B/F/TAF (78.5% [24.0%]; all p < 0.05). The proportion of PWH with PDC ≥ 85% during the baseline period was lower among those who received DTG/ABC/3TC (29.9%) and higher among those who received DTG/3TC (58.3%) compared with those who received B/F/TAF (48.8%; both p < 0.001).
| Characteristic | Overall (n = 5310) | B/F/TAF (n = 3178) | DTG/3TC (n = 674) | DTG/ABC/3TC (n = 680) | DTG + F/TAF (n = 477) | DTG + F/TDF (n = 84) | CAB + RPV (n = 217) |
|---|---|---|---|---|---|---|---|
| Age, years, mean (SD) | 54.0 (12.3) | 53.8 (12.3) | 55.1 (12.3) | 54.4 (12.4) | 54.5 (12.1) | 50.9 (13.3) | 52.7 (13.2) |
| Age group, n (%) | |||||||
| 18–39 years | 780 (14.7) | 481 (15.1) | 84 (12.5) | 97 (14.3) | 59 (12.4) | 16 (19.0) | 43 (19.8) |
| 40–54 years | 1736 (32.7) | 1031 (32.4) | 215 (31.9) | 231 (34.0) | 161 (33.8) | 30 (35.7) | 68 (31.3) |
| 55–64 years | 1662 (31.3) | 1006 (31.7) | 215 (31.9) | 199 (29.3) | 154 (32.3) | 28 (33.3) | 60 (27.6) |
| ≥ 65 years | 1132 (21.3) | 660 (20.8) | 160 (23.7) | 153 (22.5) | 103 (21.6) | 10 (11.9) | 46 (21.2) |
| Sex, n (%) | |||||||
| Female | 1169 (22.0) | 655 (20.6) | 148 (22.0) | 172 (25.3) | 120 (25.2) | 17 (20.2) | 57 (26.3) |
| Male | 4141 (78.0) | 2523 (79.4) | 526 (78.0) | 508 (74.7) | 357 (74.8) | 67 (79.8) | 160 (73.7) |
| Race/ethnicity, n (%) | |||||||
| White | 2497 (47.0) | 1510 (47.5) | 338 (50.1) | 299 (44.0) | 218 (45.7) | 38 (45.2) | 94 (43.3) |
| Hispanic | 695 (13.1) | 427 (13.4) | 98 (14.5) | 78 (11.5) | 54 (11.3) | 7 (8.3) | 31 (14.3) |
| African–American/Black | 1618 (30.5) | 947 (29.8) | 158 (23.4) | 259 (38.1) | 162 (34.0) | 27 (32.1) | 65 (30.0) |
| Asian | 81 (1.5) | 49 (1.5) | 14 (2.1) | 6 (0.9) | 11 (2.3) | 0 | 1 (0.5) |
| Other/unknown | 82 (1.5) | 46 (1.4) | 11 (1.6) | 9 (1.3) | 10 (2.1) | 4 (4.8) | 2 (0.9) |
| No data available | 337 (6.3) | 199 (6.3) | 55 (8.2) | 29 (4.3) | 22 (4.6) | 8 (9.5) | 24 (11.1) |
| Insurance type, n (%) | |||||||
| Commercial | 2384 (44.9) | 1424 (44.8) | 328 (48.7) | 300 (44.1) | 213 (44.7) | 40 (47.6) | 79 (36.4) |
| Medicare Advantage | 2926 (55.1) | 1754 (55.2) | 346 (51.3) | 380 (55.9) | 264 (55.3) | 44 (52.4) | 138 (63.6) |
| Region,† n (%) | |||||||
| Northeast | 691 (13.0) | 421 (13.2) | 82 (12.2) | 80 (11.8) | 68 (14.3) | 14 (16.7) | 26 (12.0) |
| Midwest | 779 (14.7) | 491 (15.4) | 86 (12.8) | 84 (12.4) | 61 (12.8) | 9 (10.7) | 48 (22.1) |
| South | 3146 (59.2) | 1850 (58.2) | 401 (59.5) | 447 (65.7) | 277 (58.1) | 53 (63.1) | 118 (54.4) |
| West | 693 (13.1) | 416 (13.1) | 104 (15.4) | 69 (10.1) | 71 (14.9) | 8 (9.5) | 25 (11.5) |
| CCI score, mean (SD) | 4.84 (2.27) | 4.84 (2.30) | 4.55 (2.15) | 4.88 (2.29) | 5.29 (2.24) | 4.55 (2.50) | 4.79 (1.82) |
| MHD, n (%) | 4855 (91.4) | 2905 (91.4) | 628 (93.2) | 606 (89.1) | 436 (91.4) | 77 (91.7) | 203 (93.5) |
| Severe MHD,‡ n (%) | 2503 (47.1) | 1535 (48.3) | 280 (41.5) | 306 (45.0) | 240 (50.3) | 48 (57.1) | 94 (43.3) |
| SUD, n (%) | 1299 (24.5) | 802 (25.2) | 126 (18.7) | 177 (26.0) | 122 (25.6) | 26 (31.0) | 46 (21.2) |
†
One PWH (who received DTG/3TC) had a region of “other”.
‡
Includes PWH with ICD-10-CM diagnosis codes for schizophrenia, bipolar disorder, or major depressive disorder.
3TC: Lamivudine; ABC: Abacavir; B: Bictegravir; CAB: Cabotegravir; CCI: Charlson Comorbidity Index; DTG: Dolutegravir; F: Emtricitabine; ICD-10-CM: International Classification of Diseases, Tenth Revision, Clinical Modification; MHD: Mental health disorder; PWH: People with HIV; RPV: Rilpivirine; SD: Standard deviation; SUD: Substance use disorder; TAF: Tenofovir alafenamide; TDF: Tenofovir disoproxil fumarate.
| Parameter | Index regimen | ||||||
|---|---|---|---|---|---|---|---|
| Overall | B/F/TAF | DTG/3TC | DTG/ABC/3TC | DTG + F/TAF | DTG + F/TDF | CAB + RPV | |
| PWH with an MHD/SUD at baseline | |||||||
| n | 5310 | 3178 | 674 | 680 | 477 | 84 | 217 |
| > 90-day gap in all HIV medications, n (%) | 1295 (24.4) | 720 (22.7) | 69 (10.2)§ | 351 (51.6)§ | 105 (22.0) | 28 (33.3)† | 22 (10.1)§ |
| PDC, %, mean (SD)¶ | 77.5 (24.9) | 78.5 (24.0) | 83.2 (19.2)§ | 66.4 (30.6)§ | 74.3 (28.2)‡ | 69.6 (29.7)† | 82.5 (18.3)‡ |
| Suboptimal adherence, n (%) | 2784 (52.4) | 1628 (51.2) | 281 (41.7)§ | 477 (70.1)§ | 246 (51.6) | 52 (61.9) | 100 (46.1) |
| PWH with PDC < 85% during follow-up | |||||||
| n | 4090 | 2323 | 366 | 739 | 436 | 81 | 145 |
| > 90-day gap in all HIV medications, n (%) | 1625 (39.7) | 889 (38.3) | 83 (22.7)§ | 488 (66.0)§ | 128 (29.4)§ | 22 (27.2)† | 15 (10.3)§ |
| PDC, %, mean (SD)# | 64.6 (27.5) | 64.9 (26.7) | 73.9 (23.3)§ | 51.7 (28.8)§ | 65.9 (28.7) | 64.8 (28.5) | 80.0 (19.6)§ |
| Suboptimal adherence, n (%) | 3066 (75.0) | 1755 (75.5) | 240 (65.6)§ | 639 (86.5)§ | 294 (67.4)§ | 60 (74.1) | 78 (53.8)§ |
†
Indicates p < 0.05 vs B/F/TAF.
‡
Indicates p < 0.01 vs B/F/TAF.
§
Indicates p < 0.001 vs B/F/TAF.
¶
Baseline adherence is reported for 4572 PWH in the MHD/SUD group (2765 receiving B/F/TAF, 633 receiving DTG/3TC, 480 receiving DTG/ABC/3TC, 422 receiving DTG + F/TAF, 69 receiving DTG + F/TDF, and 203 receiving CAB + RPV).
#
Baseline adherence is reported for 3206 PWH in the MHD/SUD group (1827 receiving B/F/TAF, 314 receiving DTG/3TC, 480 receiving DTG/ABC/3TC, 380 receiving DTG + F/TAF, 72 receiving DTG + F/TDF, and 133 receiving CAB + RPV).
3TC: Lamivudine; ABC: Abacavir; B: Bictegravir; CAB: Cabotegravir; DTG: Dolutegravir; F: Emtricitabine; MHD: Mental health disorder; PDC: Proportion of days covered; PWH: People with HIV; RPV: Rilpivirine; SD: Standard deviation; SUD: Substance use disorder; TAF: Tenofovir alafenamide; TDF: Tenofovir disoproxil fumarate.
A total of 4090 (27.6%) PWH were in the PDC < 85% group (i.e., had suboptimal adherence to the index regimen during the follow-up period; Table 3). The mean (SD) age of these PWH was 50.4 (13.5) years, 77.6% were male, 39.3% were African–American/Black, 37.5% were White and most (62.1%) were located in the South. Adherence to prior ART during the baseline period varied between PWH who received B/F/TAF and those who received other regimens on the index date (Table 2). The proportion of PWH with a > 90-day gap in all HIV medications was higher among those who received DTG/ABC/3TC (66.0%) and lower among those who received DTG/3TC (22.7%), DTG + F/TAF (29.4%), DTG + F/TDF (27.2%) or CAB + RPV (10.3%) compared with those who received B/F/TAF (38.3%; all p < 0.05). Mean (SD) PDC was lower among PWH who received DTG/ABC/3TC (51.7% [28.8%]) and higher among those who received DTG/3TC (73.9% [23.3%]) or CAB + RPV (80.0% [19.6%]) compared with those who received B/F/TAF (64.9% [26.7%]; all p < 0.001). The proportion of PWH with PDC ≥ 85% was lower among those who received DTG/ABC/3TC (13.5%) and higher among those who received DTG/3TC (34.4%), DTG + F/TAF (32.6%) or CAB + RPV (46.2%) compared with those who received B/F/TAF (24.5%; all p < 0.001).
| Characteristic | Overall (n = 4090) | B/F/TAF (n = 2323) | DTG/3TC (n = 366) | DTG/ABC/3TC (n = 739) | DTG + F/TAF (n = 436) | DTG + F/TDF (n = 81) | CAB + RPV (n = 145) |
|---|---|---|---|---|---|---|---|
| Age, years, mean (SD) | 50.4 (13.5) | 50.0 (13.4) | 50.6 (14.0) | 50.2 (13.9) | 51.8 (12.7) | 50.2 (13.5) | 53.0 (13.3) |
| Age group, n (%) | |||||||
| 18–39 years | 1022 (25.0) | 605 (26.0) | 98 (26.8) | 188 (25.4) | 78 (17.9) | 23 (28.4) | 30 (20.7) |
| 40–54 years | 1372 (33.5) | 792 (34.1) | 110 (30.1) | 250 (33.8) | 153 (35.1) | 25 (30.9) | 42 (29.0) |
| 55–64 years | 1025 (25.1) | 557 (24.0) | 92 (25.1) | 177 (24.0) | 139 (31.9) | 21 (25.9) | 39 (26.9) |
| ≥ 65 years | 671 (16.4) | 369 (15.9) | 66 (18.0) | 124 (16.8) | 66 (15.1) | 12 (14.8) | 34 (23.4) |
| Sex, n (%) | |||||||
| Female | 916 (22.4) | 493 (21.2) | 89 (24.3) | 177 (24.0) | 111 (25.5) | 20 (24.7) | 26 (17.9) |
| Male | 3174 (77.6) | 1830 (78.8) | 277 (75.7) | 562 (76.0) | 325 (74.5) | 61 (75.3) | 119 (82.1) |
| Race/ethnicity, n (%) | |||||||
| White | 1532 (37.5) | 852 (36.7) | 125 (34.2) | 262 (35.5) | 183 (42.0) | 35 (43.2) | 75 (51.7) |
| Hispanic | 524 (12.8) | 299 (12.9) | 64 (17.5) | 82 (11.1) | 58 (13.3) | 4 (4.9) | 17 (11.7) |
| African–American/Black | 1606 (39.3) | 915 (39.4) | 125 (34.2) | 347 (47.0) | 151 (34.6) | 32 (39.5) | 36 (24.8) |
| Asian | 57 (1.4) | 28 (1.2) | 2 (0.5) | 11 (1.5) | 14 (3.2) | 1 (1.2) | 1 (0.7) |
| Other/unknown | 67 (1.6) | 34 (1.5) | 14 (3.8) | 8 (1.1) | 6 (1.4) | 3 (3.7) | 2 (1.4) |
| No data available | 304 (7.4) | 195 (8.4) | 36 (9.8) | 29 (3.9) | 24 (5.5) | 6 (7.4) | 14 (9.7) |
| Insurance type, n (%) | |||||||
| Commercial | 2415 (59.0) | 1392 (59.9) | 217 (59.3) | 436 (59.0) | 256 (58.7) | 52 (64.2) | 62 (42.8) |
| Medicare Advantage | 1675 (41.0) | 931 (40.1) | 149 (40.7) | 303 (41.0) | 180 (41.3) | 29 (35.8) | 83 (57.2) |
| Region,† n (%) | |||||||
| Northeast | 508 (12.4) | 285 (12.3) | 44 (12.0) | 87 (11.8) | 62 (14.2) | 10 (12.3) | 20 (13.8) |
| Midwest | 547 (13.4) | 329 (14.2) | 35 (9.6) | 89 (12.0) | 49 (11.2) | 10 (12.3) | 35 (24.1) |
| South | 2539 (62.1) | 1437 (61.9) | 237 (64.8) | 491 (66.4) | 252 (57.8) | 49 (60.5) | 73 (50.3) |
| West | 494 (12.1) | 271 (11.7) | 50 (13.7) | 71 (9.6) | 73 (16.7) | 12 (14.8) | 17 (11.7) |
| CCI score, mean (SD) | 4.08 (2.42) | 4.05 (2.42) | 3.78 (2.33) | 4.00 (2.46) | 4.49 (2.46) | 4.25 (2.64) | 4.42 (1.93) |
†
Two PWH (1 received B/F/TAF and 1 received DTG/ABC/3TC) had a region of “other”.
3TC: Lamivudine; ABC: Abacavir; B: Bictegravir; CAB: Cabotegravir; CCI: Charlson Comorbidity Index; DTG: Dolutegravir; F: Emtricitabine; PWH: People with HIV; RPV: Rilpivirine; SD: Standard deviation; TAF: Tenofovir alafenamide; TDF: Tenofovir disoproxil fumarate.
Overlap existed between the two groups of interest. Among the 14,826 treatment-experienced PWH in the overall population, 1480 (10.0%) had an MHD/SUD at baseline and PDC < 85% during the follow-up period, whereas 3830 (25.8%) had only an MHD/SUD at baseline and 2610 (17.6%) had only PDC < 85% during the follow-up period (Supplementary Table 3). The remaining 6906 (46.6%) treatment-experienced PWH in the overall population had neither an MHD/SUD nor PDC < 85%.
In both the MHD/SUD and PDC < 85% groups, treatment regimen groups were fairly balanced after IPTW (Supplementary Tables 4–7).
PWH with an MHD/SUD
The Kaplan–Meier curve for time to nonpersistence through 12 months in PWH with an MHD/SUD is shown in Figure 2A. A significantly greater proportion of PWH who received B/F/TAF remained persistent at 12 months (80.3%) compared with PWH who received DTG/3TC (76.7%), DTG/ABC/3TC (68.9%), DTG + F/TAF (62.4%) and DTG + F/TDF (36.7%; all p < 0.05). A numerically greater proportion of PWH who received B/F/TAF were persistent at 12 months compared with those who received CAB + RPV, although this difference was not statistically significant (70.4%; p > 0.05).
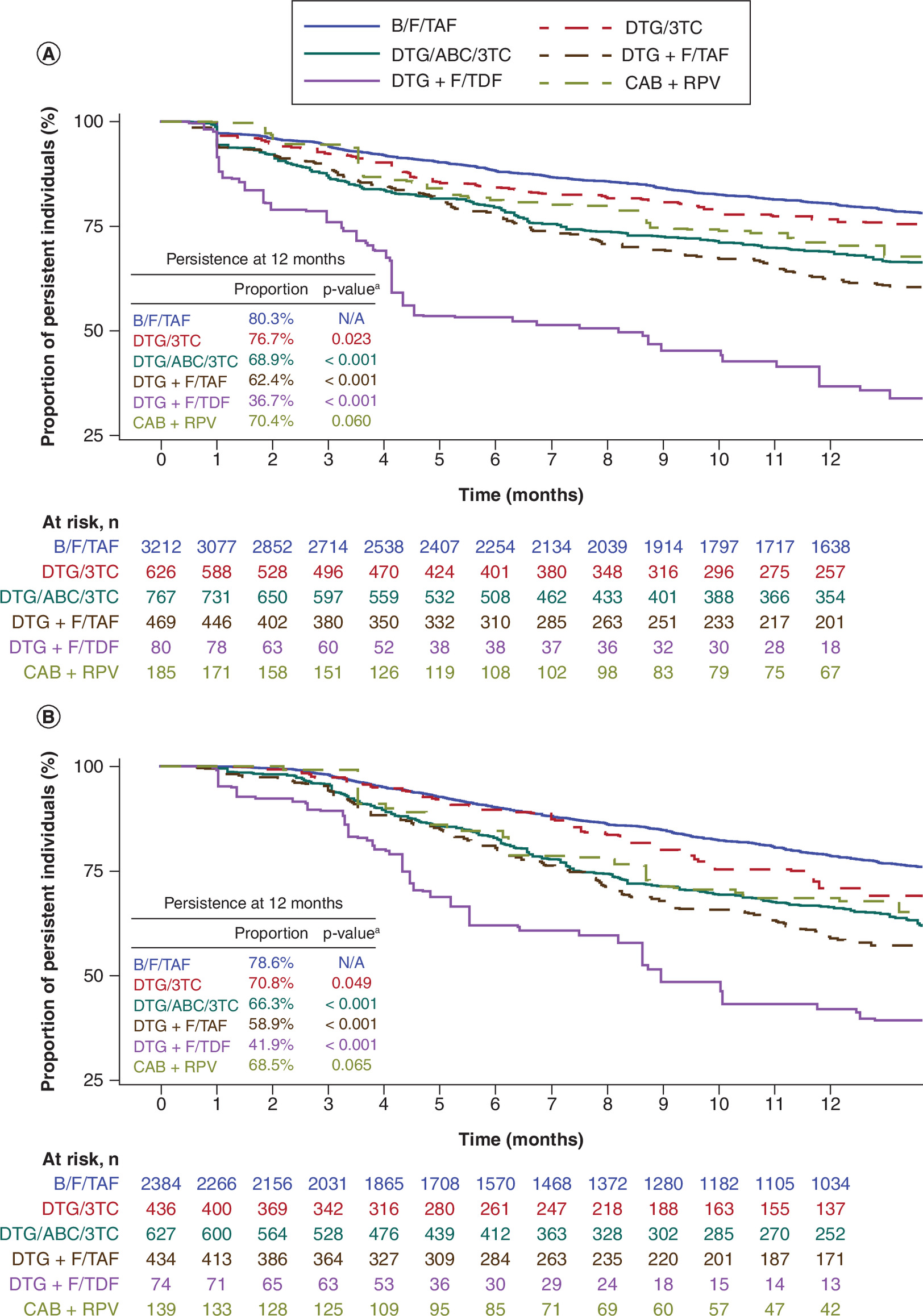
Figure 2. Kaplan–Meier curve for persistence through 12 months in US people with HIV (A) with an MHD/SUD (weighted) and (B) with PDC < 85% (weighted) receiving B/F/TAF or a comparator regimen (2017–2024).
ap-values were calculated by the log-rank test to determine statistically significant differences between B/F/TAF and comparator regimens.
3TC: Lamivudine; ABC: Abacavir; B: Bictegravir; CAB: Cabotegravir; DTG: Dolutegravir; F: Emtricitabine; MHD: Mental health disorder; N/A, not applicable; PDC: Proportion of days covered; RPV: Rilpivirine; SUD: Substance use disorder; TAF: Tenofovir alafenamide; TDF: Tenofovir disoproxil fumarate.
With regards to the risk of nonpersistence throughout the follow-up period, the adjusted Cox proportional hazards model analysis in PWH with an MHD/SUD showed that, compared with those who received B/F/TAF, PWH who received DTG/3TC, DTG/ABC/3TC, DTG + F/TAF and DTG + F/TDF were 27%, 60%, 123% and 371% more likely to be nonpersistent, respectively (all p < 0.05). The adjusted HR for nonpersistence for PWH who received CAB + RPV was 1.40 (95% CI: 0.83–2.38; p > 0.05; Table 4).
| Regimen | MHD/SUD at baseline | PDC < 85% during follow-up | ||
|---|---|---|---|---|
| Adjusted HR† (95% CI) | p-value‡ vs B/F/TAF | Adjusted HR† (95% CI) | p-value‡ vs B/F/TAF | |
| B/F/TAF | Reference | – | Reference | – |
| DTG/3TC | 1.27 (1.02–1.57) | 0.033 | 1.24 (0.96–1.59) | 0.100 |
| DTG/ABC/3TC | 1.60 (1.37–1.88) | < 0.001 | 1.59 (1.34–1.88) | < 0.001 |
| DTG + F/TAF | 2.23 (1.92–2.60) | < 0.001 | 1.95 (1.63–2.33) | < 0.001 |
| DTG + F/TDF | 4.71 (3.41–6.49) | < 0.001 | 4.81 (3.40–6.81) | < 0.001 |
| CAB + RPV | 1.40 (0.83–2.38) | 0.209 | 1.60 (0.88–2.92) | 0.123 |
†
HRs and 95% CIs were determined using Cox proportional hazards models and were adjusted by baseline demographic characteristics, CCI score, AHRQ comorbidities, AIDS-defining conditions, comedications, PDC, all-cause healthcare cost and utilization and ART copay or coinsurance.
‡
p-values were calculated using a Cox proportional hazards model to determine statistically significant differences between B/F/TAF and comparator regimens.
3TC: Lamivudine; ABC: Abacavir; AHRQ: Agency for Healthcare Research and Quality; ART: Antiretroviral therapy; B: Bictegravir; CAB: Cabotegravir; CCI: Charlson Comorbidity Index; CI: Confidence interval; DTG: Dolutegravir; F: Emtricitabine; HR: Hazard ratio; MHD: Mental health disorder; PDC: Proportion of days covered; RPV: Rilpivirine; SUD: Substance use disorder; TAF: Tenofovir alafenamide; TDF: Tenofovir disoproxil fumarate.
PWH with PDC < 85%
The Kaplan–Meier curve for time to nonpersistence in PWH with PDC < 85% for each treatment group is shown in Figure 2B. The proportion of PWH with PDC < 85% who received B/F/TAF and were persistent at 12 months (78.6%) was significantly greater compared with those who received DTG/3TC (70.8%), DTG/ABC/3TC (66.3%), DTG + F/TAF (58.9%) and DTG + F/TDF (41.9%; all p < 0.05). A numerically greater proportion of PWH who received B/F/TAF were persistent at 12 months compared with those who received CAB + RPV, although this difference was not statistically significant (68.5%; p > 0.05).
For PWH with PDC < 85%, compared with those who received B/F/TAF, PWH who received DTG/ABC/3TC, DTG + F/TAF and DTG + F/TDF, were 59%, 95% and 381%, respectively, more likely to be nonpersistent (all p < 0.001; Table 4). PWH with PDC < 85% who received DTG/3TC (HR: 1.24; 95% CI: 0.96–1.59) and CAB + RPV (HR: 1.60; 95% CI: 0.88–2.92) had a numerically higher risk of nonpersistence compared with those who received B/F/TAF (both p > 0.05).
Discussion
PWH who have MHDs/SUDs often experience challenges with ART adherence [3,12,13,21]. The primary aim of this retrospective cohort study was to examine ART regimen persistence among treatment-experienced PWH with an MHD/SUD or suboptimal adherence (i.e., PDC < 85%). In this study, those who received B/F/TAF were more likely to persist on treatment at 12 months and have a lower risk of nonpersistence throughout the follow-up period compared with those who received other regimens. Differences in these persistence outcomes were statistically significant in all cases for PWH who received B/F/TAF compared with those who received DTG/ABC/3TC, DTG + F/TAF and DTG + F/TDF. For the comparison of B/F/TAF with DTG/3TC, PWH with an MHD/SUD or suboptimal adherence were more likely to persist on treatment at 12 months and had a lower risk of nonpersistence during the follow-up period with B/F/TAF, though these results were not statistically significant for the group with suboptimal adherence. For all comparisons with CAB + RPV, although B/F/TAF was associated with numerically greater persistence at 12 months and a lower risk of nonpersistence throughout the follow-up period for both the MHD/SUD and PDC < 85% groups, none of the comparisons reached statistical significance.
In the present study, differences in baseline adherence across the regimens were observed. For both the MHD/SUD and PDC < 85% groups, adherence prior to starting the index regimen was significantly higher for PWH who received DTG/3TC or CAB + RPV as their index regimen and lower for PWH who received DTG/ABC/3TC compared with those who received B/F/TAF as their index regimen. These results may reflect a channeling bias among newer INSTI-based regimens, with PWH who were already more likely to have better adherence and persistence being prescribed DTG/3TC or CAB + RPV. In prior studies, physicians have reported a preference for prescribing B/F/TAF for PWH with a history of adherence challenges or SUD, while DTG/3TC was preferred for PWH with concerns regarding weight gain or those who had reduced renal function (although, notably, a recent assessment of major clinical trials found that DTG-, B- and TAF-containing regimens are weight neutral) [22–24]. Similarly, in the case of CAB + RPV, given that treatment-emergent resistance has been observed even in PWH who maintain adherence to the injection schedule [25–31], a history of adherence concerns could lead physicians to prescribe an oral regimen.
Of the total sample of treatment-experienced PWH considered, greater than half had an MHD/SUD at baseline, PDC < 85% during the follow-up period, or both. The presence of MHDs/SUDs may lead to myriad and overlapping social and economic challenges to improving health outcomes for PWH. These factors can act as further barriers to entering and staying in the HIV care continuum, including accessing, adhering to and persisting on treatment [10].
Among PWH with an MHD/SUD, those who received B/F/TAF were more likely to remain persistent at 12 months and had a lower risk of nonpersistence throughout the follow-up period compared with those who received DTG/3TC, DTG/ABC/3TC, DTG + F/TAF or DTG + F/TDF. These results were similar among PWH with PDC < 85%, although there was no significant difference in risk of nonpersistence between B/F/TAF and DTG/3TC in this population. These findings were consistent with a recent study by Kong et al. that demonstrated treatment-experienced PWH with an MHD/SUD who received B/F/TAF in the US HealthVerity database had a significantly lower risk of nonpersistence compared with those who received DTG/ABC/3TC, DTG + F/TAF or DTG + F/TDF [32].
In the current study, there was no significant difference in risk of nonpersistence between B/F/TAF and CAB + RPV in either population. The recent US FDA approval of CAB + RPV in 2021, and, consequently, its relatively limited availability during the identification period, may have impacted these findings. While the once every month or once every 2 months dosing and intramuscular administration of CAB + RPV may address persistence challenges for certain individuals, there are several factors that influence how PWH persist on ART, such as regimen efficacy, safety and tolerability [33–35].
The proportion of PWH with an MHD/SUD who were persistent at 12 months ranged from 36.7% with DTG + F/TDF to 80.3% with B/F/TAF. These proportions were slightly lower than those observed in a prior analysis of the general population of treatment-experienced PWH in the Optum Research Database by Cohen et al. who reported a range of 39.8% with DTG + F/TDF to 81.7% with B/F/TAF [21]. Similar to the current analysis of treatment-experienced PWH with an MHD/SUD, Cohen et al. reported a lower risk of nonpersistence with B/F/TAF compared with DTG/ABC/3TC, DTG + F/TAF and DTG + F/TDF and a similar risk of nonpersistence with B/F/TAF and CAB + RPV in the general population of treatment-experienced PWH. Overall, these findings are consistent with prior evidence of a higher risk of nonpersistence in PWH with MHDs/SUDs and provide a better understanding of recent real-world ART persistence patterns in this population.
This study had some limitations. Administrative data are collected for payment, not research, and can be subject to bias due to misclassification and errors. As such, because the analyses of persistence relied on recording oral ART prescriptions rather than direct measurements of oral ART usage, actual usage may have differed from the prescription for the oral ARTs included in this study. The calculation for adherence to CAB + RPV was further complicated because the number of days of supply (i.e., 30 vs 60 days) was not available on medical claims. It was assumed that medical claims for CAB 600 mg had a supply of 60 days. Claims for CAB 400 mg or with missing National Drug Codes were assumed to have a supply of 30 days, which could have underestimated persistence by 30 days. Moreover, any medical care not submitted to insurance for reimbursement could not be observed. Additionally, we used an algorithm to identify regimens that used empirical fill data in the claims database to determine the start and the end of the regimen. This algorithm may not have perfectly aligned with the actual duration of the regimen; therefore, PWH who systematically received part of their regimen intermittently may have been misclassified as initiating a new medication and ending their regimen. Finally, although the Optum Research Database contains national data from a variety of geographic regions and employer groups, the results of these analyses are limited to the population included in this study and may not be generalizable to other PWH in the USA, particularly groups that were not represented in this analysis, including those insured by Medicaid or those who are uninsured.
The strengths of this study include a large sample size of PWH from a variety of geographic locations, an identification period lasting > 6 years and an analysis of persistence among populations treated with a total of six contemporary ART regimens, including a newer CAB-containing ART regimen.
In conclusion, in treatment-experienced PWH with an MHD/SUD or suboptimal adherence, B/F/TAF was associated with greater persistence at 12 months and a lower risk of nonpersistence compared with several other commonly used ART regimens. These findings contribute to a better understanding of real-world persistence patterns in these populations and indicate that, for treatment-experienced PWH, B/F/TAF may have a high likelihood of treatment persistence. Multinational, prospective, observational studies comparing persistence among ART regimens are needed to confirm the findings in this study.
Summary points
•
Adherence and persistence to antiretroviral therapy (ART) are key to viral suppression and long-term health outcomes in people with HIV (PWH).
•
PWH with a mental health disorder and/or substance use disorder (MHD/SUD) may struggle with adherence and persistence to ART.
•
Treatment selection is important for PWH and an MHD/SUD or suboptimal adherence in order to optimize outcomes.
•
This real-world study used claims data to examine persistence to six ART regimens (bictegravir [B]/emtricitabine [F]/tenofovir alafenamide [TAF], dolutegravir [DTG]/lamivudine [3TC], DTG/abacavir [ABC]/3TC, DTG + F/TAF, DTG + F/tenofovir disoproxil fumarate [TDF] and cabotegravir [CAB] + rilpivirine [RPV]) among PWH with an MHD/SUD or suboptimal adherence to ART (proportion of days covered [PDC] < 85% during follow-up).
•
Between 1 July 2017 and 30 November 2023, 5310 PWH with an MHD/SUD and 4090 PWH with PDC < 85% were identified and included in the analysis.
•
At 12 months, persistence with B/F/TAF was significantly greater compared with DTG/3TC, DTG/ABC/3TC, DTG + F/TAF and DTG + F/TDF for PWH with an MHD/SUD and for PWH with PDC < 85%.
•
Persistence at 12 months with B/F/TAF was numerically greater compared with CAB + RPV for both groups but did not reach statistical significance.
•
Findings were similar for the risk of nonpersistence throughout the follow-up period, with a greater risk of nonpersistence with all DTG-based regimens than with B/F/TAF in both groups (except for DTG/3TC in the PDC < 85% group).
•
These results suggest that B/F/TAF offers a greater likelihood of persistence compared with other regimens in treatment-experienced PWH with an MHD/SUD or suboptimal adherence and can help guide regimen selection for these populations of PWH.
Author contributions
Concept and design: U Mordi, MJ Christoph, B Chastek, T Lim and S Majethia. Data acquisition: B Chastek and LB Le. Data analysis: B Chastek and LB Le. Data interpretation: U Mordi, MJ Christoph, B Chastek, T Lim, N Prata Menezes, LB Le and J Cohen. Critical review of the manuscript for important intellectual content: U Mordi, MJ Christoph, B Chastek, T Lim, N Prata Menezes, S Majethia, LB Le and J Cohen.
Acknowledgments
The authors thank Sarah Hauge for her project management support.
Financial disclosure
This study was funded by Gilead Sciences, Inc. (CA, USA).
Competing interests disclosure
U Mordi, MJ Christoph, T Lim, N Prata Menezes and S Majethia are employees and stockholders of Gilead Sciences, Inc. B Chastek and LB Le are employees of Optum and stockholders of United Health Group. J Cohen is an independent health care analyst, formerly employed by Tufts University. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing disclosure
Medical writing and editorial support were provided by Miranda Tradewell of Lumanity Communications Inc., and were funded by Gilead Sciences, Inc.
Ethical conduct of research
As this was a secondary analysis of existing data, institutional review board or independent ethics committee review and informed consent were not required. Patient identifiers in all data sources were removed, and the data contained no patient-identifiable fields. Patients' anonymity was strictly maintained, and the data source was compliant with the Health Insurance Portability and Accountability Act.
Data availability statement
The authors certify that this manuscript reports the original results of a real-world evidence study. A prespecified study protocol was developed (not publicly available). No preregistration was reported for this study. The Optum Research Database was commercially licensed from the data vendor. The data contained in the Optum Research Database include proprietary elements owned by Optum and, therefore, cannot be broadly disclosed or made publicly available at this time. The disclosure of these data to third-party clients assumes certain data security and privacy protocols are in place and that the third-party client has executed the standard license agreement, which includes restrictive covenants governing the use of the data. The underlying data and analytic code used in the analysis are not publicly available. Reporting checklists were not provided for this manuscript.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary materials.docx)
- Download
- 144.52 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
UNAIDS. Global HIV & AIDS statistics — Fact sheet. (Accessed: 13 November 2024). https://www.unaids.org/en/resources/fact-sheet
2.
HIV.gov. U.S. Statistics. (Accessed: 9 May 2025). https://www.hiv.gov/hiv-basics/overview/data-and-trends/statistics
3.
US Department of Health and Human Services Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the use of antiretroviral agents in adults and adolescents with HIV. (Accessed: 21 March 2025). https://clinicalinfo.hiv.gov/sites/default/files/guidelines/documents/adult-adolescent-arv/guidelines-adult-adolescent-arv.pdf
4.
Cramer JA, Roy A, Burrell A et al. Medication compliance and persistence: terminology and definitions. Value Health 11(1), 44–47 (2008).
5.
Clay PG, Yuet WC, Moecklinghoff CH et al. A meta-analysis comparing 48-week treatment outcomes of single and multi-tablet antiretroviral regimens for the treatment of people living with HIV. AIDS Res. Ther. 15(1), 17 (2018).
6.
de Los Rios P, Okoli C, Punekar Y et al. Prevalence, determinants, and impact of suboptimal adherence to HIV medication in 25 countries. Prev. Med. 139, 106182 (2020).
7.
Holkmann Olsen C, Mocroft A, Kirk O et al. Interruption of combination antiretroviral therapy and risk of clinical disease progression to AIDS or death. HIV Med. 8(2), 96–104 (2007).
8.
Lang R, Hogan B, Zhu J et al. The prevalence of mental health disorders in people with HIV and the effects on the HIV care continuum. AIDS 37(2), 259–269 (2023).
9.
Hartzler B, Dombrowski JC, Crane HM et al. Prevalence and predictors of substance use disorders among HIV care enrollees in the United States. AIDS Behav. 21(4), 1138–1148 (2017).
• Examines data from > 10,000 people with HIV (PWH) across multiple clinics in the USA and estimated that 48% of PWH had a substance use disorder (SUD).
10.
Remien RH, Stirratt MJ, Nguyen N, Robbins RN, Pala AN, Mellins CA. Mental health and HIV/AIDS: the need for an integrated response. AIDS 33(9), 1411–1120 (2019).
11.
O'Grady T, Inman N, Younger A et al. The characteristics and HIV-related outcomes of people living with co-occurring HIV and mental health conditions in the United States: a systematic review of literature from 2016 to 2021. AIDS Behav. 28(1), 201–224 (2024).
•• Provides an in-depth analysis of PWH and a mental health disorder (MHD) or SUD in the USA. It describes the impacts of MHDs and SUDs, their co-occurrence and impacts on medication adherence, retention and health outcomes in PWH.
12.
Ma J, Delaney JAC, Ruderman SA et al. Severity and number of substances used are independently associated with antiretroviral therapy adherence over time among people with HIV in the current treatment era. AIDS Behav. 29(2), 468–479 (2025).
• Analyzed data from > 10,000 PWH from 2010 to 2021 and examined the effects of substance use – for both type and extent – on patient-reported ART adherence. The study found that severe substance use was associated with reductions in adherence that were likely to be clinically meaningful.
13.
Springer SA, Dushaj A, Azar MM. The impact of DSM-IV mental disorders on adherence to combination antiretroviral therapy among adult persons living with HIV/AIDS: a systematic review. AIDS Behav. 16(8), 2119–2143 (2012).
14.
Nyaku M, Beer L, Shu F. Non-persistence to antiretroviral therapy among adults receiving HIV medical care in the United States. AIDS Care 31(5), 599–608 (2019).
15.
Lim T, McDwyer P, Zachry W, Christoph MJ, Weinberg AR. Prevalence of and time to suboptimal treatment patterns among people with HIV on antiretroviral therapy in the United States. AIDS Behav. (2026).
16.
Andreatta K, Sax PE, Wohl D et al. Efficacy of bictegravir/emtricitabine/tenofovir alafenamide versus dolutegravir-based three-drug regimens in people with HIV with varying adherence to antiretroviral therapy. J. Antimicrob. Chemother. 80(1), 281–291 (2025).
•• In this pooled analysis of five clinical trials, 2622 PWH on B/F/TAF or DTG + 2 nucleoside reverse transcriptase inhibitors (NRTIs) were examined with respect to adherence and viral suppression. PWH with suboptimal (< 85%) adherence to B/F/TAF maintained high levels of viral suppression; those with suboptimal adherence to DTG + 2 NRTIs had decreased viral suppression compared with those with high (≥ 95%) or intermediate (85–94%) adherence.
17.
Mounzer K, Brunet L, Fusco JS et al. Advanced HIV infection in treatment-naive individuals: effectiveness and persistence of recommended 3-drug regimens. Open Forum Infect. Dis. 9(3), ofac018 (2022).
• This was an analysis of electronic health record data from PWH with advanced HIV infection from the US Observational Pharmaco-Epidemiology Research & Analysis (OPERA) cohort. PWH who initiated B/F/TAF had a lower likelihood of discontinuation compared with those who started other regimens, including DTG.
18.
Hines DM, Ding Y, Wade RL, Beaubrun A, Cohen JP. Treatment adherence and persistence among HIV-1 patients newly starting treatment. Patient Prefer. Adherence 13, 1927–1939 (2019).
19.
Cohen J, Beaubrun A, Bashyal R, Huang A, Li J, Baser O. Real-world adherence and persistence for newly-prescribed HIV treatment: single versus multiple tablet regimen comparison among US medicaid beneficiaries. AIDS Res. Ther. 17(1), 12 (2020).
20.
Cutrell J, Jodlowski T, Bedimo R. The management of treatment-experienced HIV patients (including virologic failure and switches). Ther. Adv. Infect. Dis. 7, 2049936120901395 (2020).
21.
Cohen J, Chastek B, Mordi U et al. Antiretroviral therapy persistence following regimen switch or restart among treatment-experienced people with HIV. Future Virology 20(9), 335–345 (2025).
22.
Elion R, Dunbar M, Rivet Amico K et al. Exploring antiretroviral therapy (ART) switch decisions in clinical setting: Trio Health mixed methods study. Presented at: IDWeek; Boston, MA, USA (11–15 October 2023). Poster 1570.
• Performs a differential choice analysis among clinicians and found that clinicians preferred to prescribe B/F/TAF for PWH with viremia, poor adherence or substance use, while they preferred to prescribe DTG/3TC for PWH with weight gain or renal function concerns.
23.
Sax P, Eron J, Radtchenko J et al. What influences switching to DTG/3TC vs B/F/TAF in clinical practice? Presented at: 30th Conference on Retroviruses and Opportunistic Infections (CROI); Seattle, WA, USA (19–22 February 2023). Poster 532.
24.
Wohl DA, Koethe JR, Sax PE et al. Antiretrovirals and weight change: weighing the evidence. Clin. Infect. Dis. 79(4), 999–1005 (2024).
25.
Overton ET, Richmond G, Rizzardini G et al. Long-acting cabotegravir and rilpivirine dosed every 2 months in adults with human immunodeficiency virus 1 type 1 infection: 152-week results from ATLAS-2M, a randomized, open-label, Phase IIIb, noninferiority study. Clin. Infect. Dis. 76(9), 1646–1654 (2023).
26.
van Welzen BJ, Van Lelyveld SFL, Ter Beest G et al. Virological failure after switch to long-acting cabotegravir and rilpivirine injectable therapy: an in-depth analysis. Clin. Infect. Dis. 79(1), 189–195 (2024).
27.
Kityo C, Mambule IK, Musaazi J et al. Switch to long-acting cabotegravir and rilpivirine in virologically suppressed adults with HIV in Africa (CARES): week 48 results from a randomised, multicentre, open-label, non-inferiority trial. Lancet Infect. Dis. 24(10), 1083–1092 (2024).
28.
Orkin C, Arasteh K, Gorgolas Hernandez-Mora M et al. Long-acting cabotegravir and rilpivirine after oral induction for HIV-1 infection. N. Engl. J. Med. 382(12), 1124–1135 (2020).
29.
Swindells S, Andrade-Villanueva JF, Richmond GJ et al. Long-acting cabotegravir and rilpivirine for maintenance of HIV-1 suppression. N. Engl. J. Med. 382(12), 1112–1123 (2020).
30.
Overton ET, Richmond G, Rizzardini G et al. Long-acting cabotegravir and rilpivirine dosed every 2 months in adults with HIV-1 infection (ATLAS-2M), 48-week results: a randomised, multicentre, open-label, phase 3b, non-inferiority study. Lancet 396(10267), 1994–2005 (2021).
31.
Ramgopal MN, Castagna A, Cazanave C et al. Efficacy, safety, and tolerability of switching to long-acting cabotegravir plus rilpivirine versus continuing fixed-dose bictegravir, emtricitabine, and tenofovir alafenamide in virologically suppressed adults with HIV, 12-month results (SOLAR): a randomised, open-label, Phase IIIb, non-inferiority trial. Lancet HIV 10(9), e566–e577 (2023).
32.
Kong AM, Lucia J, Christoph MJ et al. Real-world persistence in adults with HIV and mental health or substance use disorders after restarting antiretroviral therapy in the United States. Adv. Ther. 42(12), 6261–6277 (2025).
33.
Christopoulos KA, Smith MB, Pareek P et al. Learning from the first: a qualitative study of the psychosocial benefits and treatment burdens of long-acting cabotegravir/rilpivirine among early adopters in three U.S. clinics. J. Int. AIDS Soc. 27(11), e26394 (2024).
• Discusses a real-world, qualitative study on long-acting CAB + RPV to assess its psychological and social effects across a range of PWH. Many PWH reported a range of benefits, including reduced shame and increased convenience associated with CAB + RPV; however, for others, the benefits did not outweigh treatment burdens, including injection-site pain and visit frequency.
34.
Bae JW, Guyer W, Grimm K, Altice FL. Medication persistence in the treatment of HIV infection: a review of the literature and implications for future clinical care and research. AIDS 25(3), 279–290 (2011).
35.
Colson A, Chen M, Hennessy F et al. Health care provider- and patient-reported outcomes for bictegravir/emtricitabine/tenofovir alafenamide versus other antiretroviral regimens: an observational survey in the United States (July 2021-March 2022). Curr. Med. Res. Opin. 41(7), 1319–1331 (2025).
Information & Authors
Information
Published In
Copyright
© 2026 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 1 August 2025
Accepted: 23 March 2026
Published online: 23 April 2026
Keywords:
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Antiretroviral therapy persistence among treatment-experienced people with HIV and mental health disorders and/or substance use disorders in the USA (2017–2024): a retrospective cohort study. (2026) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2025-0124
Export citation
Select the citation format you wish to export for this article or chapter.