Are you implementation ready? An alternative patient and healthcare system-centered model for pharma
Publication: Journal of Comparative Effectiveness Research
Begin with the end in mind
A famous quote from Steven Covey is, “To begin with the end in mind means to start with a clear understanding of your destination.” The quote comes from his book on The 7 Habits of Highly Effective People [1], but the message has been championed in many different areas and situations. The operating model currently used in the pharmaceutical industry does not follow this principle and, rather, relies on a model filled with siloes, each having its own destination.
A drug-focused approach to drug development inhibits patient-centricity
Clinical development units in the pharmaceutical industry focus on obtaining registration, while other parts handle launch. Key performance indicators (KPIs) differ and are the number of completed trials and approved drugs for the former, and countries launched for the latter. The focus is firmly on the drug and demonstrating what is needed to reach these individual goals [2]. This way of doing business has worked in the past but has become increasingly under scrutiny as not being sufficient to answer questions regarding optimal patient care from patients, healthcare professionals (HCPs) and payers [3].
In this drug-centric approach, implementation barriers are largely ignored although they would help ensure that healthcare systems (HCSs) are ready to integrate the innovation into clinical practice [4]. Thus, far too often, the innovation does not reach patients who would benefit from it and patient-centricity is inhibited.
Introducing ‘Implementation readiness’
A fundamental shift in the pharma model requires starting with the end goal in mind across the organization: ensuring that innovations seamlessly reach patients and integrate into HCSs. Implementation readiness is a new concept, introduced here to describe the ability of a pharma organization to deliver a product effectively into the clinical care pathway at launch and beyond. Being implementation ready means that: (a) patients agree on the benefits and risks of the drug and see it as an improvement over the standard of care; (b) HCPs agree on how and when to use the drug; (c) payers recognize the added benefit in the designated patient population and; (d) the HCS itself is suited to the challenges of delivering the drug to patients. Importantly, all of the needs (a)–(d) need to be identified and addressed before reimbursement discussion and market entry.
The focus of each function within pharma needs to shift to the implementation readiness goal of a new drug, i.e., that it actually reaches and helps patients starting at launch and with optimal clinical uptake and patient reach. Significantly, this means that the implementation readiness goal for clinical development goes well beyond the current goal of regulatory approval and that for market access goes well beyond the current goal of reimbursement. A shift to an implementation readiness goal forces patient-centricity and a new pharma model implementation readiness goal at launch will require that many new as well as enhanced activities will have to be started well before launch, at risk.
Important contributions to the implementation readiness goal will include elements from implementation research, treatment optimization studies [5] and a strong sense of co-creation and collaboration at all stages of the drug development process. ‘Lean’ and ‘back to the basics’ clinical development processes will need to adapt to the new reality of ensuring implementation readiness that might include adding elements to each phase II/III trial to anticipate and prepare for the implementation issues that will be faced [6,7].
To achieve the implementation readiness goal, many new parameters for decision making enter the optimization equation such that the current linear, sequential system used for decision-making is no longer adequate. To name a few, evidence on diagnosis, referral pathways, patient population, patient-relevant outcomes and needs, prescriber needs, changing clinical guidelines, physician practice optimization and payment flow all need to be collected and addressed by the time of launch.
Solving this new simultaneous, multiparametric optimization problem is the key to reaching the implementation goal. A new pharma model will be needed to enable the shift, one that has patient-centricity inherent in its goal (Figure 1).

Figure 1. A new pharma model where all functions work from a shared integrated implementation readiness plan, toward a common implementation goal, ensuring seamless product adoption at launch.
HEOR: Health economics and outcomes research.
This new pharma model represents a shift from traditional development and launch readiness to implementation readiness – a fundamental change in how new products enter the market.
Figure 2 includes two hypothetical scenarios illustrating the difference in uptake dynamics between the two models. In a traditional development and launch readiness approach, market adoption follows a slow ramp-up phase due to implementation barriers, followed by a gradual increase, with lower peak sales and longer time to peak. In contrast, an implementation readiness model would lead to a steeper initial adoption phase and higher peak sales achieved faster.
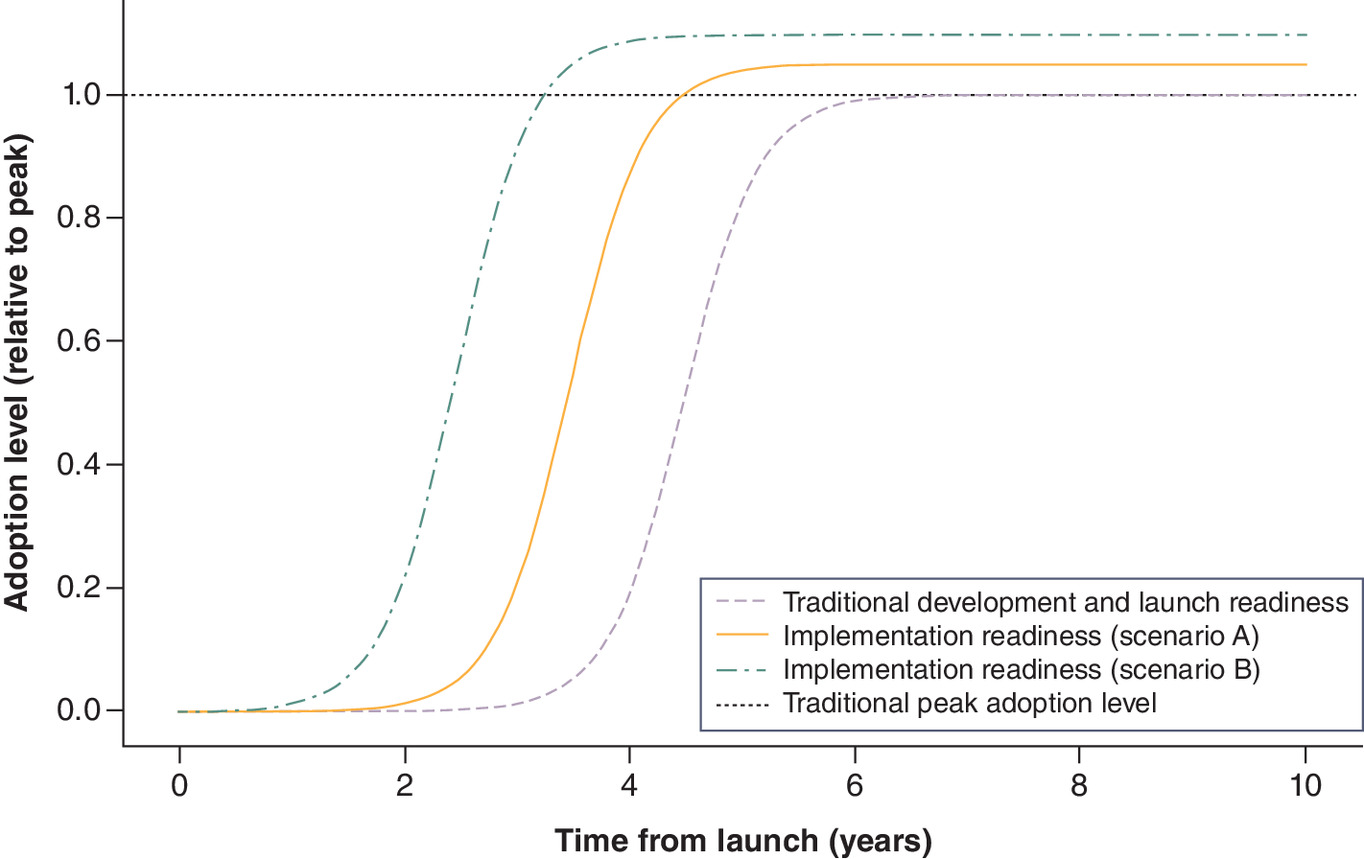
Figure 2. Impact of implementation readiness on launch uptake: comparison of traditional development and launch readiness (purple dashed), scenario A with a 1-year earlier and 5% higher peak (orange solid), and scenario B with a 2-year and 10% higher peak (green dash-dot).
The dotted horizontal line represents the traditional peak adoption level. Implementation readiness leads to faster and greater uptake, with the AUC over 10 years increasing from 5.53 (traditional) to 6.86 in scenario A and 8.28 in scenario B, representing a +24% and +50% increase, respectively.
AUC: Area under the curve.
Case studies
The journey of Qutenza® illustrates both the challenges and opportunities of adopting an implementation readiness approach. Qutenza® is a topical pain treatment that targets the source of neuropathic pain through transient defunctionalization of damaged nerve fibers followed by regeneration and restoration of nerve function [7,8]. While the treatment demonstrated clinical results in a population with a clear unmet medical need, its launch underscores the importance of having an ‘implementation readiness’ mindset to ensure successful early adoption.
The experience with Qutenza® revealed the value of early implementation science assessments. Addressing operational barriers earlier, such as inadequate referral pathways and logistical complexities, could have strengthened HCP clinical belief and sped up the product uptake. Additionally, limited organizational synergy, as the product transitioned across different companies, compounded these challenges by leaving critical implementation challenges unaddressed for longer than what would otherwise have been ideal. Lessons from this experience emphasize the need for coordinated ownership to identify and address those barriers. Furthermore, evidence that response rates improve with repeated treatment and that repeated treatment can have a meaningful impact on patients’ pain, activity levels and improve their quality of life [9,10] could have been generated earlier in the development plan, if patient optimization studies had been prioritized. In light of this new evidence, the European Medicines Agency now recommends to evaluate effectiveness of Qutenza® after three treatments [11], but having this evidence earlier could have guided physicians in their clinical practice, preventing the number of patients discontinuing due to perceived lack of efficacy and avoid treatments that are either ineffective or have adverse effects.
This is certainly not unique to Qutenza. If we allow ourselves to think beyond drugs, lipoprotein(a) [Lp(a)] testing provides another lens through which to view the transformative shift required for implementation readiness. Elevated lipoprotein(a) [Lp(a)] levels are a risk factor for cardiovascular diseases. Although US FDA-approved diagnostic assays exist, their use in clinical practice is hindered by the absence of standardized guidelines for managing elevated levels. Furthermore, although some approved therapies have shown to lower Lp(a) levels [12,13], that is not their labeled indication. This means testing rates remain low and relatively stable over time, even among patients with established cardiovascular diseases [14].
Discussion
Moving from a drug-focus to a patient-focus pharma model is more than merely performing additional tasks. The challenge lies in transforming an organization into one that plans the strategy together and performs activities, according to areas of expertise, that are bound to the overall implementation readiness goal. The specifics of how a particular pharma company should organize itself are left up to the company as there is no ‘one size fits all’ solution to organizational structure.
Implementation readiness comes with risk and costs, both of which can be mitigated to a large degree. Risks include performing new types of additional studies and/or activities that might not be positive, might identify safety risks, or might dilute the treatment effect. Costs of the additional studies and activities will be above those from a drug-focus approach. The rationale is that the additional evidence and different focus will lead to a quicker clinical uptake and an increase in the number of patients reached. In such a scenario, the return on investment will be positive and the expected net present value will increase [15].
The ability to afford the change to implementation readiness then becomes one of being able to afford some up-front costs to enjoy the payoffs later. This is exactly what the pharma industry asks payers to do [16], in particular for gene therapies. If the payers can find ways to afford such therapies, then surely pharma can find innovative ways of affording the change to implementation readiness.
The shift to implementation readiness also presents significant opportunities. This approach positions pharmaceutical companies to better meet the existing realities of the way HCSs evaluate and incorporate new innovations. In addition, it addresses emerging requirements from the recently implemented EU HTA Regulation, and aligns seamlessly with the core requirements of its Joint Clinical Assessments, which emphasize relevance to routine clinical practice across diverse HCS. Crucially, success will depend on coordination with HCS and other stakeholders, ensuring that structural and procedural adaptations match the level of evidence and planning brought forward by industry.
Conclusion
Addressing the multifaceted needs of patients, HCPs, payers and HCS through implementation readiness ensures a higher degree of patient and healthcare system centricity built into the innovation and the way it is presented for use in HCSs by the time of launch. Thus, it would benefit all stakeholders involved in getting a new technology established in clinical care. Achieving this requires a change to the pharma model and a way of thinking about risk assessment, cost allocation, goal setting and shared responsibilities. By embracing this model, the industry can accelerate product uptake by reducing initial adoption barriers, achieve peak sales sooner, increasing commercial viability and enhance patient impact by ensuring treatments reach those in need more efficiently. This new model redefines successful product launches by prioritizing patient-centricity and market integration from the start.
Financial disclosure
The authors have no financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
Disclaimer
This is an independent editorial that was not funded by Grünenthal or any other commercial entity. The views expressed are those of the authors and do not necessarily reflect the views of their affiliated organizations
Competing interests
M Olson is an employee of Olson Strategies GmbH and consults on this subject matter with RTI Health Solutions, Boehringer Ingelheim GmbH, Grunenthal S.A. and Eli Lilly and Company. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing disclosure
No writing assistance was utilized in the production of this manuscript.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Reference
1.
Covey SR, Blankenhagen D. The 7 Habits of Highly Effective People. Performance Improvement 30(10), 38 (1991).
2.
Saesen R, Lejeune S, Quaglio G, Lacombe D, Huys I. Views of European drug development stakeholders on treatment optimization and its potential for use in decision-making. Front. Pharmacol. 11, 43 (2020).
3.
Timpe C, Stegemann S, Barrett A, Mujumdar S. Challenges and opportunities to include patient-centric product design in industrial medicines development to improve therapeutic goals. Br. J. Clin. Pharmacol. 86(10), 2020–2027 (2020).
4.
Olson M (Skip), Zullig LL, Geest SD. How pharma can amplify product value with implementation science. J. Comp. Eff. Res. 13(10), (2024).
5.
Saesen R, Lacombe D, Huys I. Design, organisation and impact of treatment optimisation studies in breast, lung and colorectal cancer: the experience of the European Organisation for research and treatment of cancer. Eur. J. Cancer 151, 221–232 (2021).
6.
Van Spall HGC, Desveaux L, Finch T et al. A guide to implementation science for phase III clinical trialists: designing trials for evidence uptake. J. Am. Coll. Cardiol. 84(20), 2063–2072 (2024).
7.
Sendel M, Dunst A, Forstenpointner J, Hüllemann P, Baron R. Capsaicin treatment in neuropathic pain: axon reflex vasodilatation after 4 weeks correlates with pain reduction. Pain 164(3), 534–542 (2023).
8.
Anand P, Privitera R, Donatien P et al. Reversing painful and non-painful diabetic neuropathy with the capsaicin 8% patch: clinical evidence for pain relief and restoration of function via nerve fiber regeneration. Front. Neurol. 13, 1–18 (2022).
9.
Überall MA, Kender Z, Quandel T et al. Progressive improvements in patient-reported outcomes with the high-concentration capsaicin patch: a retrospective cohort study in patients with painful diabetic peripheral neuropathy (CASPAR study). J. Diabetes Complicat. 109085 (2025).
10.
Freynhagen R, Baron R, Huygen F, Perrot S. Narrative review of the efficacy and safety of the high-concentration (179 mg) capsaicin patch in peripheral neuropathic pain with recommendations for clinical practice and future research. Pain Rep. 10(2), E1235 (2025).
11.
European Medicines Agency (EMA). Qutenza SmPC. (accessed 2025). https://www.ema.europa.eu/en/documents/product-information/qutenza-epar-product-information_en.pdf
12.
Bittner VA, Szarek M, Aylward PE et al. Effect of alirocumab on lipoprotein(a) and cardiovascular risk after acute coronary syndrome. J. Am. Coll. Cardiol. 75(2), 133–144 (2020).
13.
O'Donoghue ML, Fazio S, Giugliano RP et al. Lipoprotein(a), PCSK9 inhibition, and cardiovascular risk: insights from the FOURIER trial. Circulation 139(12), 1483–1492 (2019).
14.
Bhatia HS, Hurst S, Desai P, Zhu W, Yeang C. Lipoprotein(a) testing trends in a large academic health system in the United States. J. Am. Heart Assoc. 12(18), 1–8 (2023).
15.
Olson M (Skip), Capkun G. The value of evidence and its role in driving product strategy. J. Comp. Eff. Res. 13(8), (2024).
16.
PwC. Six drug pricing models have emerged to improve product access and affordability. (accessed 2025). https://www.pwc.com/us/en/industries/health-industries/library/6-drug-pricing-models.html
Information & Authors
Information
Published In
Copyright
© 2025 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 12 June 2025
Accepted: 7 July 2025
Published online: 12 August 2025
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Are you implementation ready? An alternative patient and healthcare system-centered model for pharma. (2025) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2025-0094
Export citation
Select the citation format you wish to export for this article or chapter.