Health outcomes and costs in patients prescribed anticholinergic medications for overactive bladder
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Anticholinergic burden (ACB) is associated with profound clinical and economic burden; however, anticholinergic medications are often prescribed for overactive bladder (OAB). This analysis assessed risk of adverse health outcomes and costs associated with ACB among patients with OAB. Materials & methods: Adults with ≥1 pharmacy claim for ≥1 OAB anticholinergic medication and continuous coverage for ≥6 months before and after the first prescription fill date for OAB anticholinergic medication (index) from January 2010 to November 2021 in the Optum Research Database were included. Daily ACB scores were calculated postindex. The impact of ACB on risk of certain adverse health outcomes was examined using Cox proportional hazards regression with categorical and piecewise linear specifications for ACB. Time-varying total ACB association with healthcare costs was evaluated with marginal structural models. Results: Overall, 428,142 patients were included in the analysis; mean (SD) age was 65.2 (14.9) years. Mean (SD) preindex ACB was 0.53 (1.44) points/day. Postindex, OAB medications accounted for 61.0% (95% CI: 60.9%–61.1%) of total ACB. Adjusted hazard ratios for urinary tract infection (UTI), urinary retention, delirium/drowsiness, cognitive impairment, falls/fractures and cardiovascular events were >1 (vs 0 points/day) and increased with ACB. A 1-point/day increase in ACB was associated with increased risk of UTI, urinary retention, delirium/drowsiness, cognitive impairment, falls/fractures and cardiovascular events for patients with ACB ≤8 points/day preindex. Increasing ACB was associated with increased all-cause total healthcare costs and costs related to cognitive impairment and falls/fractures. Conclusion: The association between increased ACB and greater risk of certain adverse health outcomes and costs supports the reassessment of anticholinergic medication use for patients with OAB.
Plain language summary: what health outcomes & costs do patients taking anticholinergic medications for overactive bladder experience?
What is this article about?
This article answers the question of how does adding anticholinergic medication to a person’s current medication load, or increasing anticholinergic burden (ACB), affect the risk of adverse health outcomes and healthcare costs in patients with overactive bladder (OAB).
What were the results?
In this study of 428,142 patients with ≥1 pharmacy claim for ≥1 OAB anticholinergic medication, increasing ACB was strongly associated with greater risk of new-onset adverse health outcomes, including urinary tract infection, urinary retention, delirium/drowsiness, cognitive impairment, falls/fractures and cardiovascular events. Increasing ACB was also significantly associated with increased total healthcare costs, as well as costs related to cognitive impairment and falls or fractures.
What do the results mean?
These data support the reassessment of anticholinergic medication use for patients with OAB.
Anticholinergic medications are associated with adverse effects including dry mouth, headache, constipation, dizziness, vision problems and tachycardia [1]. Anticholinergic burden (ACB), the cumulative effect of ≥1 anticholinergic medication, may exacerbate adverse effects. Furthermore, higher ACB may be associated with increased risk of serious adverse health outcomes, such as falls/fractures [2], cognitive impairment [3] and dementia [4,5]. Owing to increased risk of adverse health outcomes, the American Geriatrics Society (AGS) strongly recommends avoiding the use of and minimizing the number of medications with highly anticholinergic properties (e.g., antimuscarinics, antihistamines, antidepressants) in both younger and older adults [6,7].
Despite the risks associated with anticholinergic medication use, anticholinergics are commonly prescribed for overactive bladder (OAB). OAB is a chronic disorder characterized by urinary urgency, frequency and/or nocturia, with or without urgency urinary incontinence [8], with bothersome symptoms affecting over 30 million US adults ≥40 years old [9]. Although current guidance from the American Urological Association (AUA) no longer emphasizes stepwise progression of therapy [8], earlier guidance recommended behavioral therapy with/without pharmacotherapy as first-line treatment and β3-adrenergic receptor agonists and anticholinergics as second-line treatments [10]. Insurance providers may also require a trial of anticholinergic medication before covering β3-adrenergic receptor agonists [11]. In 2017, anticholinergic medications comprised nearly 82% of medication claims for OAB and continue to be commonly prescribed for OAB in the US [12–16].
Evidence from a systematic literature review and meta-analysis suggests that anticholinergic medication use for ≥3 months is associated with a 46% increased risk of dementia compared with no anticholinergic medication use; the risk was higher with OAB anticholinergic medications compared with other anticholinergic medications [5]. A systematic literature review showed that in most studies evaluated, OAB anticholinergic medication use was linked with higher healthcare resource utilization (HCRU) – including number of hospitalizations, emergency department visits and outpatient visits – and higher associated costs [17]. Thus, ACB may be especially significant for patients with OAB.
Owing to the chronic nature of OAB, pharmacologic treatment is long term; however, changing health conditions, medications and dosages can cause an individual’s ACB to vary over time. How changes in ACB over time affect risk for adverse health outcomes and healthcare costs in patients with OAB has not been previously established. Using a large database of medical and pharmacy claims, this analysis quantified the contribution of OAB anticholinergic medications to total ACB. The analysis further determined the association of time-varying total ACB exposure with health outcomes and costs in patients with OAB.
Materials & methods
Study design, patients & assessments
This retrospective, longitudinal cohort study used medical and pharmacy claims from the Optum Research Database, which comprises deidentified medical and pharmacy claims data from >73 million US patients and complies with the Health Insurance Portability and Accountability Act (HIPAA). This study used deidentified patient data from a large, HIPAA-compliant claims database and was therefore exempt from Institutional Review Board (IRB) review and informed consent. The study reporting adheres to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for cohort studies. Adults with ≥1 pharmacy claim for ≥1 of 6 OAB anticholinergic medications (darifenacin, fesoterodine, oxybutynin, solifenacin, tolterodine, trospium) from January 2010 to November 2021 were included in the analysis.
The index date was defined as the date of the first prescription fill for the OAB anticholinergic medication. Patients had continuous enrollment in a commercial or Medicare Advantage plan with pharmacy and medical benefits for ≥6 months preindex and postindex and were followed until disenrollment or 31 May 2022 (Supplementary Figure 1).
ACB scores for each individual were calculated using prescription claims data to identify the average daily dose of each anticholinergic medication received by examining fill date, day supply, run-out date, quantity supplied and drug strength. Average daily dose was converted to daily units by dividing by the expected unit dose from the WHO. For each anticholinergic medication fill, an ACB score was calculated by multiplying the daily units by the burden value 1, 2 or 3 per the Regenstrief Institute Burden Scale [18]. The resulting ACB score was applied on all days from the fill date to run-out date, and a rolling ACB score was then calculated as the sum of all points for the previous 6 months divided by 180 and rounded to the nearest integer. Patients with ACB scores <0.5 points/day were classified as having 0 ACB points/day.
Each patient’s mean ACB over the duration of the postindex period was further classified as the portions attributable to OAB anticholinergic medications and non-OAB anticholinergic medications. To determine the association between ACB and health outcomes, the following adverse health outcomes were identified from any site of care (Supplementary Table 1): urinary tract infection (UTI), incontinence-associated dermatitis (IAD), urinary retention, delirium/drowsiness, cognitive impairment, falls/fractures, cardiovascular events and mortality.
To determine the association between ACB and healthcare costs, total costs were calculated as the combined amounts paid by the health plan and patient, adjusted using annual medical care component of the consumer price index to reflect inflation to 2021, and categorized as pharmacy or medical costs. Medical costs included subcategories for ambulatory (office and hospital outpatient), emergency services (ER), inpatient and other medical costs. Owing to increased risks with anticholinergic medication use [2–5], event-related medical costs were assessed for claims related to cognitive impairment and falls/fractures.
Statistical analysis
Data analysis was conducted between March 2023 and July 2024. Descriptive statistics were used to assess preindex measures, postindex events and association of postindex, time-varying ACB with healthcare costs. P-values were calculated with Pearson chi-square tests (binary measures) or F-test/analysis of variance (continuous measures).
The association between postindex event risk and ACB was analyzed using Cox proportional hazards models with time-varying ACB (i.e., time-varying exposure) while controlling for preindex covariates (Supplementary Table 2). Patients with evidence of the health outcomes of interest during the 6-month preindex period were excluded from event-related analyses. Models were initially developed using categorical ACB (0, 1, 2, 3, ≥4 points/day) with 0 points/day as the reference. After the initial analysis using models in which ACB was a categorical term, it was observed that patients typically increased their ACB by 1 point/day when initiating the index OAB anticholinergic medication; therefore, additional models were created using ACB as a continuous term. To account for the changing slope associated with increased ACB, continuous piecewise linear terms were used with cut points ACB of 4 and 9.
The association of ACB with postindex total healthcare costs (US$ per 6 months) and event-related medical costs was analyzed using marginal structural models (MSM). Postindex was partitioned into 6-month intervals where costs in each 6-month interval were modeled by ACB in the previous 6 months, while controlling for preindex and time-varying covariates, and reported as cost ratios. ACB was initially specified using the same categories as the Cox model (0, 1, 2, 3, ≥4 points/day) but then additionally specified as continuous from 0 to 3 points/day with a category for all ACB scores ≥4.
Results
Patients
Overall, 903,601 patients had ≥1 pharmacy claim for an anticholinergic medication for OAB during the identification period, and 428,142 patients met all inclusion criteria and were included in the analysis (Supplementary Figure 2). Mean (SD) age was 65.2 (14.9) years; 250,830 (58.6%) of patients were ≥65 years; 285,632 (66.7%) were female (Table 1 & Supplementary Table 3). Overall, 9493 (2.2%) were Asian, 49,094 (11.5%) were Black/African–American, 38,753 (9.1%) were Hispanic and 296,571 (69.3%) were White/Caucasian. Mean (SD) preindex ACB was 0.53 (1.44) points/day, and patients were followed for a mean (SD) of 1096 (862) days. Preindex, the most common conditions (occurring in ≥10% of patients) among all patients (N = 428,142) were hypertension (242,190 patients [56.6%]), coronary artery disease (63,609 [14.9%]) and OAB (58,492 [13.7%]). Preindex, 108,008 patients (25.2%) had ≥1 diagnosis code for UTI; 94,861 (22.2%), delirium/drowsiness; 92,249 (21.6%), cardiovascular events; 33,686 (7.9%), urinary retention; 32,195 (7.5%), cognitive impairment; 29,089 (6.8%), falls or fractures; and 160 (0.04%), IAD.
| Characteristic | Patients, n (%) (n = 428,142) |
|---|---|
| Age, years, mean (SD) | 65.2 (14.9) |
| Age, years, median (range) | 68.0 (18–90) |
| Age category, years | |
| 18–44 | 44,211 (10.3) |
| 45–64 | 133,101 (31.1) |
| 65–74 | 124,378 (29.1) |
| ≥75 | 126,452 (29.5) |
| Female | 285,632 (66.7) |
| Race | |
| Asian | 9493 (2.2) |
| Black/African–American | 49,094 (11.5) |
| Hispanic | 38,753 (9.1) |
| White/Caucasian | 296,571 (69.3) |
| Other or unknown‡ | 34,231 (8.0) |
| Region | |
| South | 202,641 (47.3) |
| Midwest | 118,237 (27.6) |
| West | 55,363 (12.9) |
| Northeast | 51,776 (12.1) |
| Other | 125 (0.03) |
| Insurance type | |
| Commercial | 173,328 (40.5) |
| Medicare Advantage | 254,814 (59.5) |
| Length of follow-up, mean (SD), days | 1096 (862) |
| Preindex ACB, mean (SD), points/day | 0.53 (1.44) |
| Comorbidities | |
| Overactive bladder disorder | 58,492 (13.7) |
| Hypertension | 242,190 (56.6) |
| Chronic heart failure | 26,692 (6.2) |
| Coronary artery disease | 63,609 (14.9) |
| Neurogenic detrusor overactivity | 11,063 (2.6) |
| CCI score, mean (SD) | 1.07 (1.61) |
| Medication count, mean (SD) | 7.96 (5.53) |
| Clinical events | |
| UTI | 108,008 (25.2) |
| Delirium/drowsiness | 94,861 (22.2) |
| Cardiovascular | 92,249 (21.6) |
| Urinary retention | 33,686 (7.9) |
| Cognitive impairment | 32,195 (7.5) |
| Falls/fractures | 29,089 (6.8) |
| IAD | 160 (0.04) |
| Preindex total healthcare costs§ by ACB, mean (SD), US$/month | |
| 0 | 1792.52 (5314.76) |
| 1 | 2529.49 (5559.00) |
| 2 | 2950.31 (6469.80) |
| 3 | 3133.33 (6797.71) |
| ≥4 | 3331.95 (5884.39) |
ACB: Anticholinergic burden; CCI: Charlson Comorbidity Index; IAD: Incontinence-associated dermatitis; UTI: Urinary tract infection.
†
Demographics were assessed at index.
‡
Other race and ethnic subcategories include American Indian or Alaska Native, Native Hawaiian or Other Pacific Islander and unreported.
§
Total healthcare costs includes medical and pharmacy costs.
Total ACB & OAB-specific ACB
During the preindex period, of 428,142 patients, 416,697 (97.3%) were classified as having 0–3 ACB points/day, with 309,683 (72.3%) classified as having 0 ACB points/day (Figure 1A). Patients typically maintained the same non-OAB ACB preindex to postindex. Postindex, patients added a median (range) of 0.8 (0.5–5.8) ACB points/day. For patients classified as having 0 ACB points/day preindex (includes <0.5 points/day), OAB anticholinergic medications accounted for 72.6% (95% CI: 72.5%–72.7%) of their postindex total ACB (Figure 1B). Postindex ACB attributed to OAB anticholinergic medications was significantly greater for patients ≥65 versus <65 years (mean [SD] ACB, 0.79 [1.41] vs 0.68 [1.69] points/day; p < 0.001).
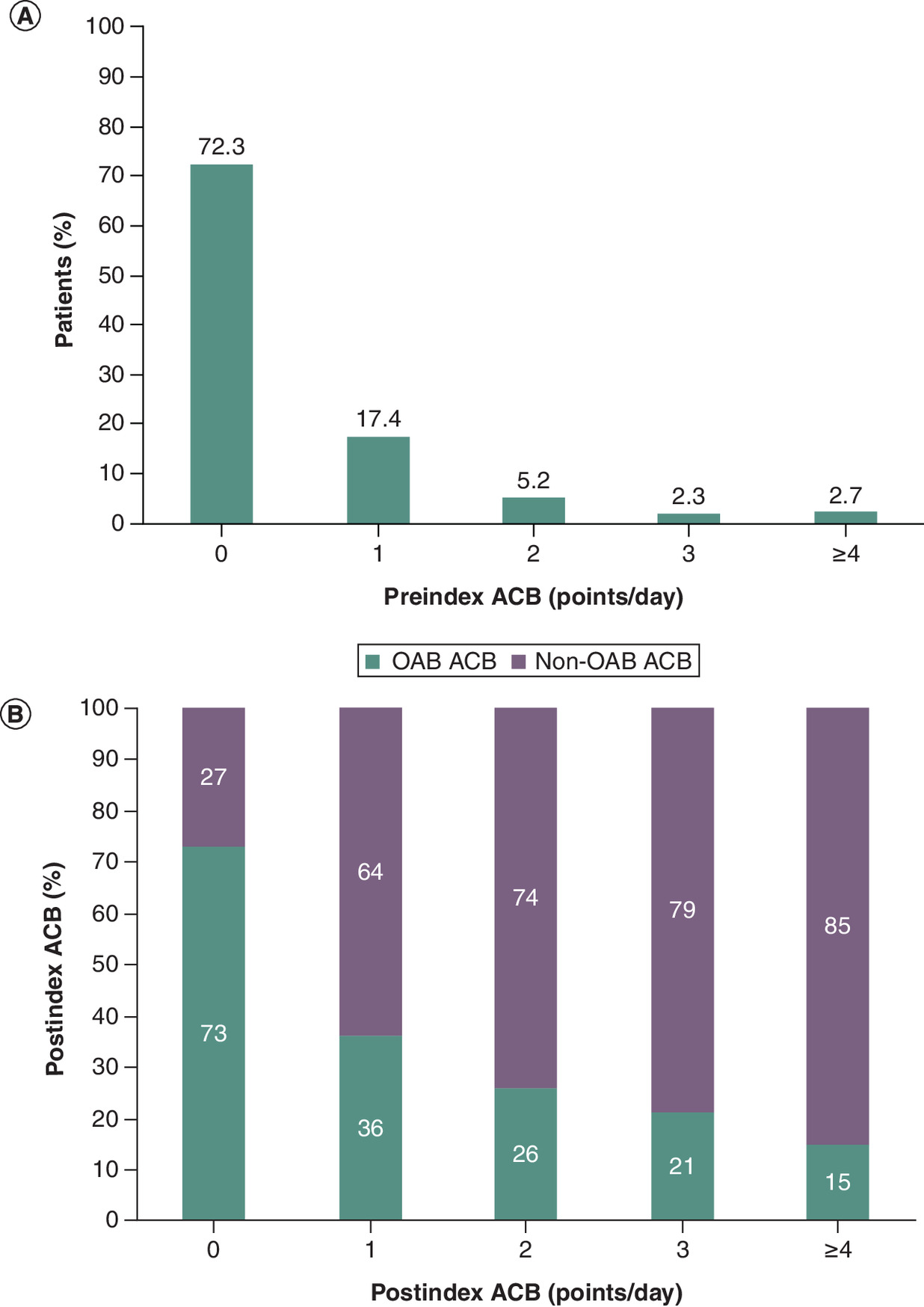
Figure 1. Preindex anticholinergic burden category and postindex anticholinergic burden attribution.
(A) Percentage of patients by preindex ACB category. (B) Percentage of ACB attributable to OAB-specific and non-OAB medications over the duration of the postindex period.
ACB: Anticholinergic burden; OAB: Overactive bladder.
ACB & adverse health outcomes
The total number of patients at risk for adverse outcomes postindex are presented in Supplementary Table 4. Using the categorical ACB specification, increasing ACB was associated with a significantly increased risk of UTI, urinary retention, delirium/drowsiness, falls/fractures and cardiovascular events (p < 0.001 for all categories vs 0 points/day; Figure 2A). Cognitive impairment had the highest association with increasing ACB (all p < 0.001 vs 0 points/day). IAD was not associated with ACB, regardless of category. Mortality was inversely associated with ACB category.
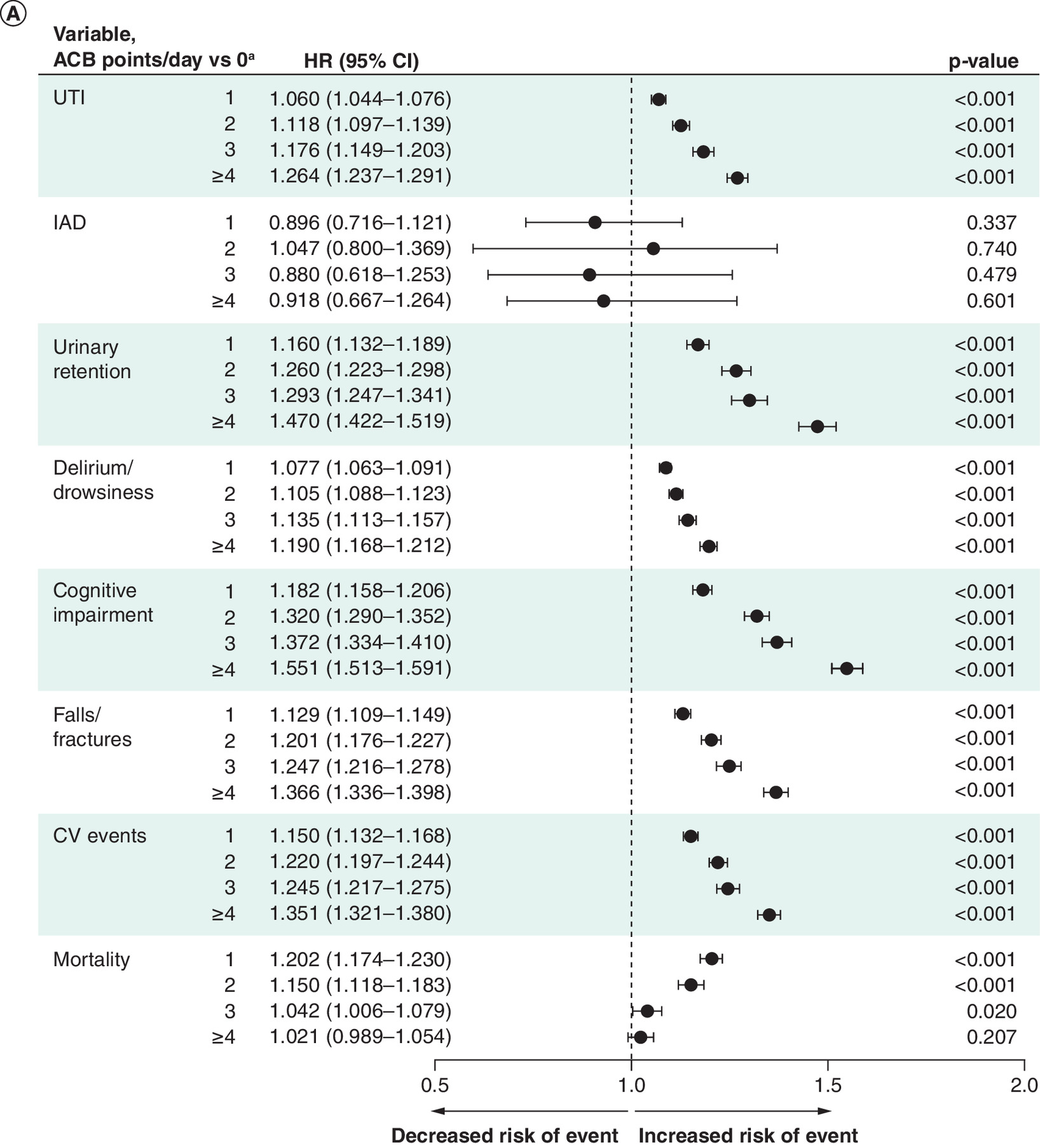
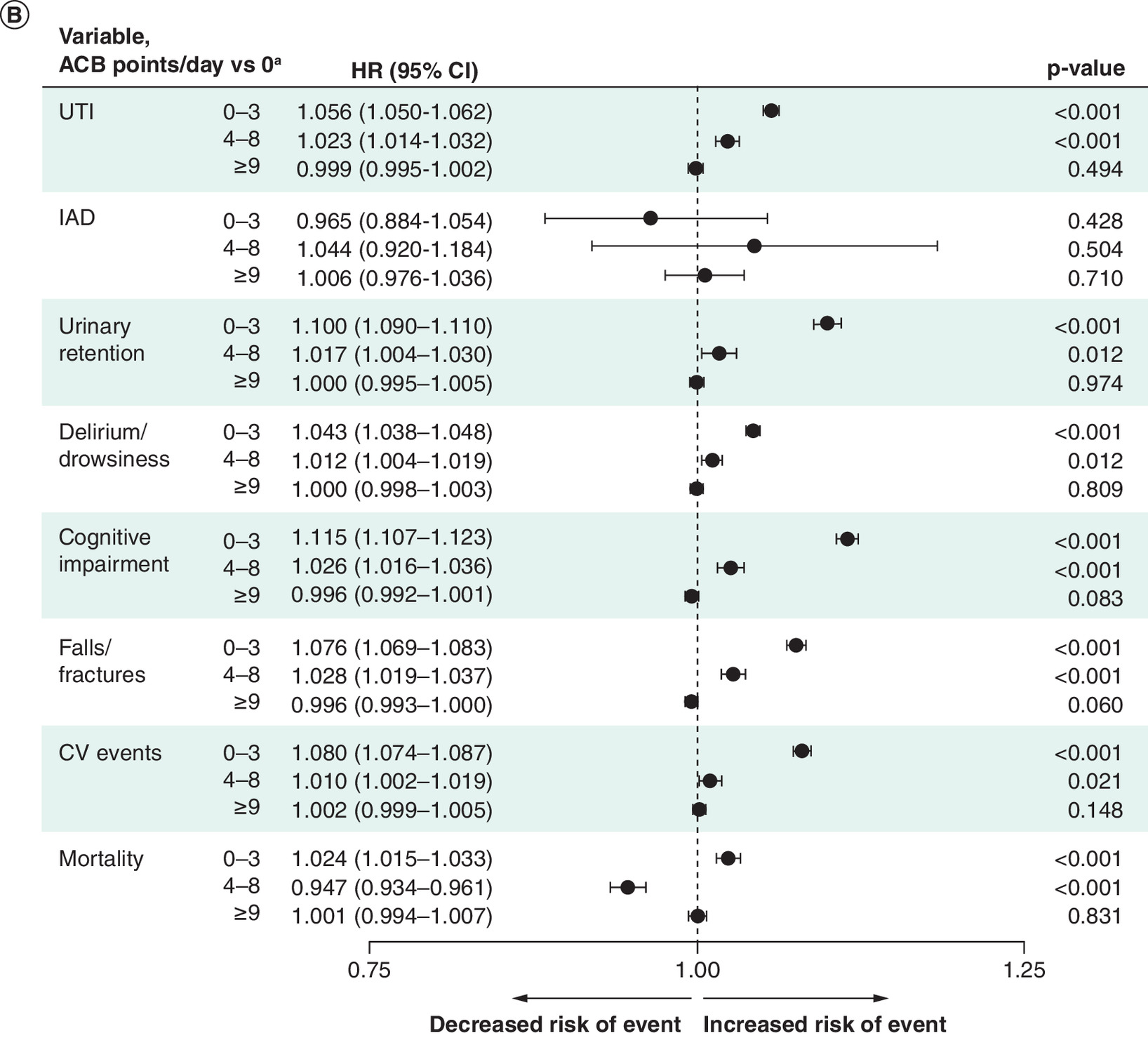
Figure 2. Risk of adverse health outcomes in the postindex period by time-varying anticholinergic burden category.
(A) Compared with 0 ACB points/day and (B) assessed with the addition of 1 ACB point/day. The x-axes present HRs (95% CIs) on a log-based scale.
a0 points/day includes rolling ACB score <0.5.
ACB: Anticholinergic burden; CI: Confidence interval; CV: Cardiovascular; HR: Hazard ratio; IAD: Incontinence-associated dermatitis; UTI: Urinary tract infection.
Using the piecewise-linear specification, a 1-point/day increase in ACB within the range of 0–3 points/day was associated with a greater risk of UTI, urinary retention, delirium/drowsiness, cognitive impairment, falls/fractures, cardiovascular events and mortality (all p < 0.001; Figure 2B). Within the range of 4–8 ACB points/day, a 1-point/day increase in ACB was associated with a greater risk of UTI, urinary retention, delirium/drowsiness, cognitive impairment, falls/fractures and cardiovascular events (all p < 0.05). Within the range of 4–8 ACB points/day, a 1-point/day increase in ACB was associated with a decreased risk of mortality (p < 0.001). Once ACB reached ≥9 points/day, a 1-point/day increase was not associated with a greater risk of adverse health outcomes.
ACB & healthcare costs
Preindex per-patient per-month (PPPM) healthcare costs increased with ACB (p < 0.001; Table 1). Postindex, PPPM total healthcare costs, including medical and pharmacy costs, also increased with ACB (p < 0.001; Figure 3A). Of costs comprising medical costs, those associated with ambulatory visits, ER visits, inpatient care and other medical expenses were also significantly increased with higher ACB (all p < 0.001; Figure 3B). Postindex, increasing ACB was also generally associated with higher costs for cognitive impairment (mean [SD]: 0 ACB points/day, $123.54 [$842.75]; 1 ACB point/day, $223.46 [$1192.08]; 2 ACB points/day, $278.73 [$1708.15]; 3 ACB points/day, $282.14 [$1548.08]; ≥4 ACB points/day, $255.55 [$1174.43]) and falls/fractures ($86.48 [$694.37], $153.43 [$949.86], $173.97 [$852.90], $187.70 [$1014.26], $212.77 [$1555.56], respectively) (Figure 3C). Using the categorical ACB specification, total all-cause medical costs during the 6-month postindex period increased as ACB increased in the prior 6-month period from 1 to ≥4 points/day (all p < 0.001 vs prior 6-month period); costs related to cognitive impairment and falls/fractures during the 6-month postindex period also increased with increased ACB in the prior 6-month period (all p < 0.001 vs previous 6-month period) (Figure 4). Using the piecewise-linear specification, each 1-point/day increase in ACB within the range of 0–3 was associated with increased total healthcare costs, as well as costs related to cognitive impairment and falls/fractures, in the 6-month postindex period versus prior 6 months (Table 2).
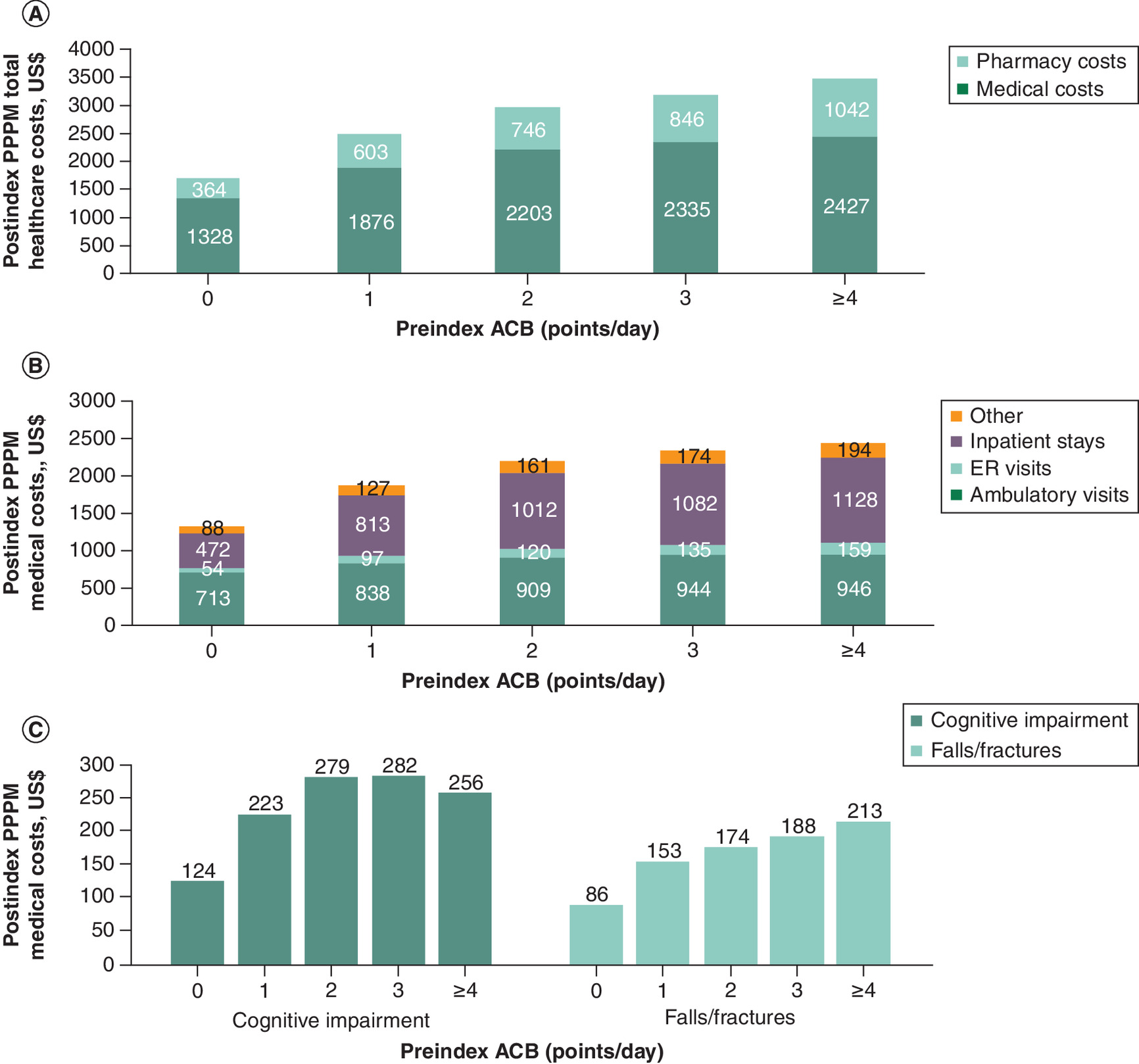
Figure 3. Postindex per-patient per-month costs by preindex anticholinergic burden category.
(A) Total healthcare, (B) medical and (C) event-related costs. Costs are in US$ per month, adjusted to reflect inflation to 2021 using the annual medical care component of the consumer price index.
ACB: Anticholinergic burden; ER: Emergency room; PPPM: Preindex per-patient per-month.
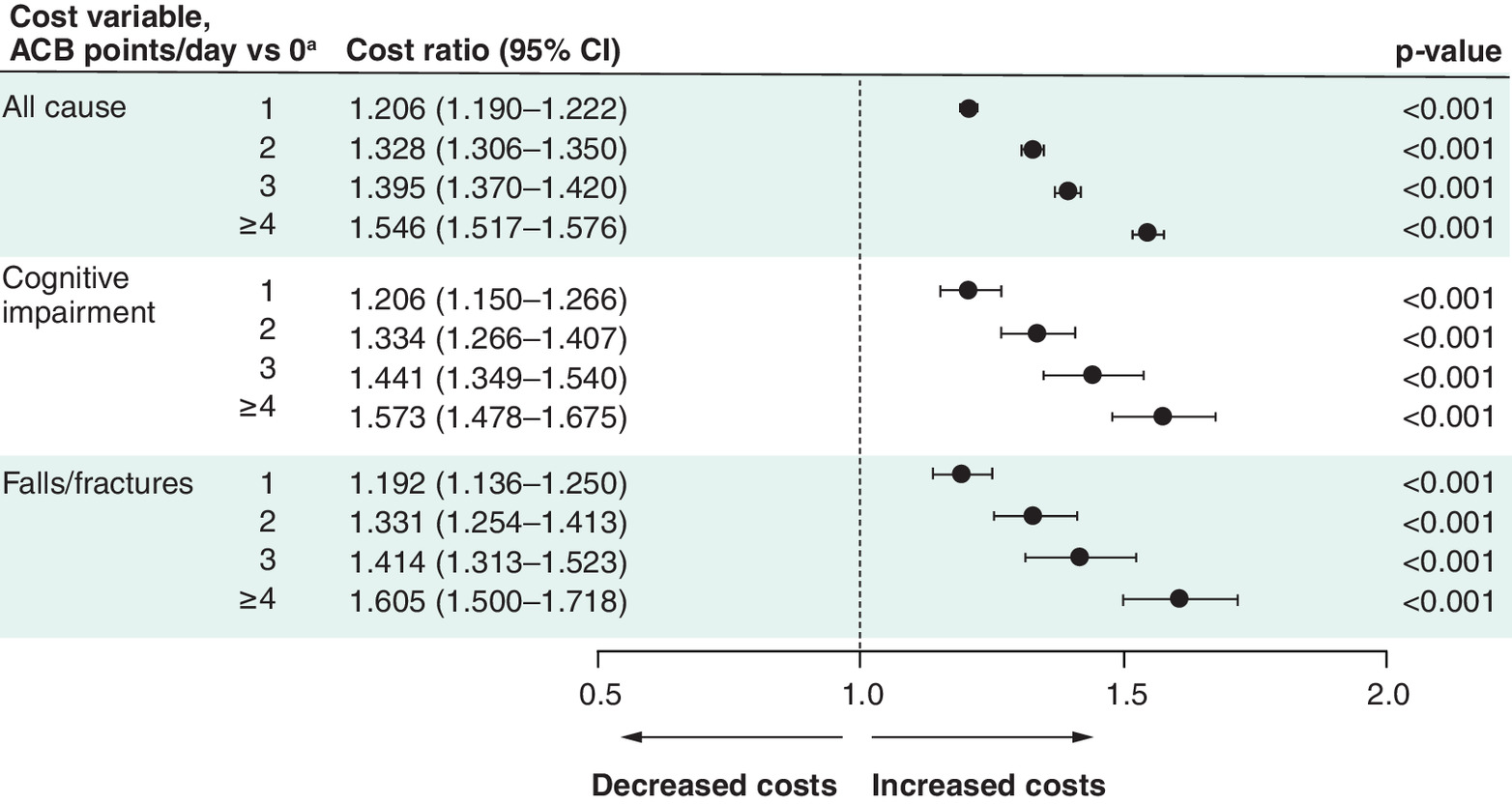
Figure 4. Risk of increased healthcare costs by time-varying anticholinergic burden.
The x-axis presents cost ratios (95% CIs) on a log-based scale.
a0 points/day includes rolling ACB score < 0.5.
ACB: Anticholinergic burden; CI: Confidence interval; PPPM: Per patient per month.
| Cost outcome | Cost ratio (95% CI) | p-value |
|---|---|---|
| Total healthcare | 1.129 (1.122–1.136) | <0.001 |
| Cognitive impairment | 1.136 (1.114–1.159) | <0.001 |
| Falls/fractures | 1.132 (1.107–1.157) | <0.001 |
ACB: Anticholinergic burden; CI: Confidence interval.
Discussion
In this large, retrospective database analysis of patients with OAB, anticholinergic medications for OAB were a major contributor to total ACB. On average, those initiating an OAB anticholinergic medication added ∼1 point/day to their ACB postindex, which was associated with a greater risk of certain adverse health outcomes for nearly all patients included in the study. Controlling for time-varying exposure, this analysis also demonstrated a positive direct correlation between increased ACB and greater healthcare costs, including all-cause medical costs, cognitive impairment–related costs and fall/fracture-related costs.
ACB may change over time owing to changes in patient health, medications and dosages or patients discontinuing anticholinergic medications potentially due to adverse effects [19,20]. In our analysis, more than half of the postindex ACB was attributed to initiating an OAB anticholinergic medication, which is in line with the contribution reported in other publications [21]. The contribution of OAB anticholinergic medications to total ACB in the postindex period was particularly pronounced in patients with a low ACB preindex, which accounted for most patients; for patients with 0 ACB points/day preindex, ACB postindex was primarily due to initiating an OAB anticholinergic medication.
Previous studies have shown that anticholinergic use is associated with increased risk of adverse health outcomes [2–4,22–26]; however, these analyses were not always specific to patients with OAB and generally did not account for time-varying changes in ACB, nor did they quantify daily anticholinergic use. Our results expand on these previous studies and show that when accounting for changes in ACB over time, increasing ACB was associated with increased risk of certain health outcomes. In our analysis, patients added ∼1 point/day to their ACB postindex regardless of preindex ACB, and each 1-point increase was generally associated with increased risk of adverse outcomes. The greatest effect of a 1-point/day increase was observed for patients with 0–3 ACB points/day, ranging from 2.4% to 11.5% greater risk per 1-point/day increase for all adverse health outcomes analyzed except IAD. Among the 4–8 ACB points/day category, a 1-point/day increase was associated with a smaller but still significantly greater risk of all adverse health outcomes assessed except IAD and mortality; thus, for a patient with a low ACB, adding an anticholinergic medication, such as an OAB anticholinergic (i.e., an additional point/day), may have a profound impact on risk of certain adverse health outcomes.
For patients with >8 ACB points/day, a 1-point/day increase was not associated with increased risk of adverse health outcomes. These results suggest that patients with high ACB are possibly already at maximum risk, alternatively, a ceiling effect may exist, in which adding ACB points may not show any further clinical impact. During the follow-up, only 2.8% of patients had a least 1 day with an ACB score >8 (data not shown); thus, the patient sample size for the group may also preclude the ability to determine an accurate association. Whether patients were deprescribed after an adverse event is unlikely, as the ACB was assessed on a continuous rolling 6-month time frame.
Of 33 studies identified in a systematic review of the effects of anticholinergic medications on cognitive function, 23 reported a significant decline in cognitive function [3]. A systematic literature review and meta-analysis reported that use of anticholinergic medications for ≥3 months was associated with a 46% increased risk of dementia compared with no anticholinergic medication use [5]. The current analysis aligns with previous reports and shows an 11.5% increased risk of cognitive impairment per 1-point/day increase in ACB among patients with relatively low (0–3 points/day) preindex ACB.
Similarly, our results also show a 7.6% increased risk of falls/fractures per 1-point/day ACB increase for patients in this lower ACB category, in alignment with a prior systematic review and meta-analysis showing an increased risk of falls associated with anticholinergic medication use [2]. In particular, in a prior retrospective claims analysis, patients with OAB with urinary incontinence had 46% higher risk of falls/fractures after initiating anticholinergic treatment compared with non-OAB patients [26], while another retrospective claims study demonstrated that risk of falls/fractures increased with higher ACB among patients with OAB [25]. Adverse events for anticholinergic medications include dizziness and vision problems [1], which may contribute to the increased risk of falling in patients initiating a new or additional anticholinergic medication.
A claims analysis of comorbidities in patients with OAB showed a 57.6% rate of any cardiovascular comorbidity [27], and post-marketing surveillance for anticholinergic medications include reports of palpitations, tachycardia and QT prolongation [28–33]; thus unsurprisingly, increased ACB was also associated with increased risk of cardiovascular events in our analysis.
The AUA/Society of Urodynamics, Female Pelvic Medicine & Urogenital Reconstruction (SUFU) guidelines recommend extreme caution for the use of anticholinergic medications in patients with OAB and a history of urinary retention due to the potential for worsening bladder emptying [8]. Anticholinergic medications for OAB inhibit contraction of the bladder/detrusor muscle thereby reducing the urge to urinate [34]. A reduced urge to urinate may lead to overfilling and residual urine on emptying. Increased residual urine in the bladder may allow bacteria to breed and increase the risk of UTI [35]; thus, urinary retention may increase the risk for UTI. Indeed, our analysis showed that increasing ACB score was associated with increased risk of both urinary retention and UTI; further supporting exercising caution when prescribing anticholinergic medications for patients with history of urinary retention.
Delirium and drowsiness are additional concerning outcomes for older adults. According to a systematic literature review and meta-analysis, older age and ACB are independent risk factors for delirium [36]. Somnolence, hallucinations and delirium have been noted as side effects of anticholinergic medications [28–30,33,37], and older adults have increased blood-brain barrier permeability [38], making them more susceptible to adverse central nervous system effects of increased ACB [39]. In our analysis, risk of delirium/drowsiness increased with higher ACB. Similarly, a systematic literature review evaluated studies investigating the association of ACB with delirium in older patients and found significantly higher ACB in patients with delirium compared with those without [40]. Systematic reviews have reported mixed results on relative mortality risk with 1 review reporting no significant association [3] and one reporting increased mortality risk with high ACB versus minimal or no ACB [41]. In our analysis, increased ACB was inversely associated with the risk of mortality. As patients approach end of life, providers may discontinue medications that are no longer consistent with care goals or that may increase the risk of adverse outcomes, such as falls or dementia [2,5]. Thus, the greater risk of mortality in our analysis among patients with lower ACB may be attributable to reduced prescribing of not only anticholinergic medications but all medications, accounting for the inverse relationship [8]. Alternatively, those that were at higher risk of mortality may have died during the study; thus, a survivor bias could account for the inverse relationship between mortality and ACB.
In the current analysis, higher ACB was associated with higher healthcare costs in the preindex and postindex periods. Postindex, compared with patients with 0 ACB points/day, total healthcare costs were up to 54.6% higher. Similar trends were seen for costs for cognitive impairment and falls/fractures. Additionally, for patients with 0–3 ACB points/day, a 1-point/day increase in ACB was associated with a 13% to 14% increase in healthcare costs, 13.6% increase in cognitive impairment–related costs and 13.2% increase in fall-/fracture-related costs. These results are largely in agreement with prior studies. A systematic literature review showed that in most retrospective claims analyses evaluated, OAB anticholinergic medication use was associated with higher HCRU and associated costs [17]. Retrospective studies of adults with OAB have reported an association between higher ACB and total HCRU and mean healthcare costs among long-term nursing home residents [23], as well as HCRU and costs related to falls/fractures in those with commercial or Medicare insurance [24]. Another retrospective analysis of Medicare beneficiaries showed use of ≥2 anticholinergic medications for ≥1 year was associated with increased rates of falls/fractures and altered mental status/delirium and associated annual medical costs [42].
The results of our analysis, in which the mean age was ∼65 years, are particularly concerning for older patients owing to the high rates of polypharmacy in this patient population [43]. The AGS Beers Criteria® for Potentially Inappropriate Medication use recommends limiting the use of anticholinergic medications, especially in older adults [6]. Furthermore, the AUA/SUFU recommend discussing the potential risk for developing dementia and cognitive impairment with patients with OAB when considering pharmacologic treatment and caution against the use of anticholinergics for patients with various comorbid conditions [8]. An evaluation of the US Centers for Medicare & Medicaid Services (CMS) data from 2013 to 2017 showed that oxybutynin was the most prescribed OAB medication [16]. Another study using CMS data from 2013 to 2019 indicated that anticholinergic medication prescriptions accounted for 85% of prescriptions for OAB; however, overall prescriptions for anticholinergics for OAB decreased from 2013 to 2019 [15]. After publication of literature linking use of anticholinergics to the risk of developing dementia, an anonymous, cross-sectional, web-based survey was conducted of American Urogynecologic Society members [11]. Most respondents reported changing their practice in response to published data; however, over half responded that for most patients a trial with anticholinergics was required by payors before authorizing a β3-adrenergic receptor agonist [11].
Strengths
The strengths of this study are the analysis of incremental increases in ACB and accounting for change in ACB over time, as opposed to a single ACB at a predetermined point in time. Another strength of this study is the large sample size. To our knowledge, our study included one of the largest cohorts of patients with OAB to date. Further, the Optum Research Database is national in scope, constructed from a variety of geographic and employer groups, and one of the most complete in the US. The Regenstreif Institute ACB scale assigns fixed scores (0–3) without accounting for prescribed dose or formulation, potentially leading to exposure misclassification; thus, another strength of this analysis is that average daily dose was first determined based on each individual’s anticholinergic medication fill history, allowing for dose-adjusted ACB estimates.
Limitations
These study results may not be generalizable to populations beyond those included in this analysis. This analysis included patients with commercial and Medicare Advantage plans; therefore, direct comparisons cannot be made to analyses derived solely from Medicare populations. Other limitations include those inherent of claims data due to the data being collected for the purpose of payment rather than research. The presence of a claim does not indicate that medication was used as prescribed. Confounders such as lifestyle modifications may not be captured in claims data. Outcome measures were based on diagnosis rather than a clinical measure. Thus, the presence of a diagnosis code does not indicate the presence of disease, and coding errors may occur. Typical to retrospective studies, the analysis is constrained by the diagnostic codes used by the clinicians. The study period may be of insufficient length to accurately describe the effects of ACB on the occurrence of certain outcomes. In particular, the length of follow-up may not be sufficient to interpret the risk of cognitive impairment in this cohort. The length of the preindex period was 6 months; patients with chronic conditions but no visits within this period may have been included in the outcomes analysis. Certain outcomes (e.g., cardiovascular events) were not separated by event type; therefore, it is possible that events are underestimated. Low rates of IAD make it infeasible to assess relative to ACB and limit the interpretation of this outcome.
This study did not specifically determine the risk of adverse health outcomes attributed to OAB anticholinergic medications but rather the risk associated with cumulative ACB; therefore, specific inferences regarding attribution of OAB anticholinergics cannot be made. Furthermore, we cannot make inferences on duration of OAB-specific anticholinergic medication use and risks of adverse health outcomes. Additionally, cause of death, which may aid in understanding deprescribing patterns, was not assessed in our study. Furthermore, patients were excluded if death occurred prior to the 6-month postindex period of continuous enrollment after index date; thus, an immortal time bias exists in the study design.
Conclusions & relevance
This retrospective, longitudinal cohort study using claims data adds to the growing body of evidence demonstrating an association between increased ACB and greater risk of certain adverse health outcomes and costs. These data inform on the overall healthcare burden resulting from the use of anticholinergic medications for OAB, underscoring the need for anticholinergic medication assessments to be performed by providers treating patients with OAB. ACB associated with OAB anticholinergic medications should be considered by national organizations involved in policy and third-party payor plans to optimize use of other pharmacologic treatment options (e.g., β3-adrenergic receptor agonist) and other advanced bladder therapies (e.g., nerve stimulation and onabotulinumtoxinA).
Summary points
•
Anticholinergic burden (ACB) is associated with significant clinical and economic burden; however, anticholinergic medications are commonly prescribed for overactive bladder (OAB) symptoms.
•
Owing to the chronic nature of OAB, pharmacologic treatment is long-term; however, changing health conditions, medications and dosages can cause an individual’s ACB to vary over time.
•
This retrospective, longitudinal, observational cohort study used claims from adults with ≥1 pharmacy claim for ≥1 OAB anticholinergic medication and continuous coverage for ≥6 months before and after the first prescription fill date for the OAB anticholinergic medication between January 2010 and November 2021 within the Optum Research Database.
•
The impact of ACB on risk of adverse health outcomes (urinary tract infection [UTI], incontinence-associated dermatitis, urinary retention, delirium/drowsiness, cognitive impairment, falls/fractures, cardiovascular events and mortality) was examined and the association of time-varying total ACB with total healthcare costs and costs related to cognitive impairment and falls/fractures was evaluated.
•
Overall, 903,601 patients had ≥1 pharmacy claim for an anticholinergic medication for OAB during the identification period, and 428,142 patients met all inclusion criteria and were included in the analysis.
•
Patients added nearly 1 ACB point/day postindex, with OAB anticholinergic medications accounting for nearly 73% of the postindex total ACB for patients who had 0 ACB points in the preindex.
•
A 1-point/day increase in ACB was associated with increased risk of UTI, urinary retention, delirium/drowsiness, cognitive impairment, falls/fractures and cardiovascular events for patients with ACB ≤8 points/day.
•
Increasing ACB was associated with increased all-cause total healthcare costs and event-related costs including cognitive impairment and falls/fractures.
•
The association between increased ACB and greater risk of certain adverse health outcomes and costs supports the reassessment of anticholinergic medication use for patients with OAB.
Author contributions
HE Richter, AK Hijaz, RR Dmochowski and J Frankel were responsible for drafting and revision of the manuscript. B Chastek, C Steiger and T Bancroft were responsible for acquisition of data, data analysis and drafting and revision of the manuscript. A Carrera, D Snyder, L Abedinzadeh and J Nesheim were responsible for study conception and design and drafting and revision of the manuscript.
Acknowledgments
These data were previously presented at the Society of Urodynamics, Female Pelvic Medicine & Urogenital Reconstruction (SUFU) 2024 Winter Meeting (20–24 February 2024, FL, USA) and the American Geriatric Society 2024 (9–11 May 2024, Virtual); additional encores at the Academy of Managed Care Pharmacy (AMCP) Meeting, 2024 (15–18 April 2024); the International Society for Pharmacoeconomics and Outcomes Research Meeting, 2024 (5–8 May 2024); the American Academy of Physician Associates (18–22 May 2024); the American Association of Nurse Practitioners National Conference 2024 (25–30 June 2024); the Gerontological Advanced Practice Nurses Association (12–14 September 2024); AMCP Nexus 2024 (14–17 October 2024) the American Urogynecologic Society Pelvic Floor Disorders Week 2024 (22–25 October 2024); the American Society of Consultant Pharmacists (7–10 November 2024); and SUFU 2025 (26 February–1 March 2025).
Financial disclosure
This study was funded by Sumitomo Pharma America, Inc.
Competing interests disclosure
HE Richter is a consultant for Allergan, Coloplast, COSM, Laborie, Neomedic and Palette Life Sciences; has received research funding from Allergan, COSM, Reia and Renovia; serves on data safety monitoring boards of BlueWind Medical, Hologic and Juniper Medical; has received royalties from UpToDate; and is on the board of SOLACE and Worldwide Fistula Fund. B Chastek, C Steiger and T Bancroft are employees of Optum. A Carrera, L Abedinzadeh and J Nesheim are employees of Sumitomo Pharma America, Inc. D Snyder was an employee of Sumitomo Pharma America, Inc., at the time the analysis was conducted. RR Dmochowski is an advisor to and principal investigator for Sumitomo Pharma America, Inc. AK Hijaz is a consultant for Caldera Medical; has received research funding from National Institute of Child Health and Human Development, Agency for Healthcare Research and Quality and Sumitomo Pharma America; and holds equity in CollaMedix Inc. J Frankel is an advisor for Sumitomo Pharma America; a meeting participant/lecturer for Pfizer and Sumitomo Pharma America; and an investigator for Astellas, Exact Sciences, Johnson & Johnson and Pfizer. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing disclosure
Medical writing support was provided by Heather Caballes, PhD, CMPP, of Citrus Health Group, Inc. (IL, USA) and was funded by Sumitomo Pharma America, Inc. (MA, USA).
Ethical conduct of research
This study used deidentified patient data from a large, HIPAA-compliant claims database and was therefore exempt from IRB review and informed consent. The study reporting adheres to the STROBE guidelines for cohort studies.
Data sharing statement
The authors certify that this manuscript reports original clinical trial data. Data reported in this manuscript are available within the article. Additional data from the study (e.g., study protocol) are available upon reasonable request.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
References
Papers of special note have been highlighted as: • of interest
1.
Rai BP, Cody JD, Alhasso A, Stewart L. Anticholinergic drugs versus non-drug active therapies for non-neurogenic overactive bladder syndrome in adults. Cochrane Database Syst. Rev. 12(12), CD003193 (2012).
2.
Stewart C, Taylor-Rowan M, Soiza RL, Quinn TJ, Loke YK, Myint PK. Anticholinergic burden measures and older people's falls risk: a systematic prognostic review. Ther. Adv. Drug Saf. 12, 20420986211016645 (2021).
3.
Fox C, Smith T, Maidment I et al. Effect of medications with anti-cholinergic properties on cognitive function, delirium, physical function and mortality: a systematic review. Age. Ageing 43(5), 604–615 (2014).
4.
Coupland CAC, Hill T, Dening T, Morriss R, Moore M, Hippisley-Cox J. Anticholinergic drug exposure and the risk of dementia: a nested case-control study. JAMA Intern. Med. 179(8), 1084–1093 (2019).
5.
Dmochowski RR, Thai S, Iglay K et al. Increased risk of incident dementia following use of anticholinergic agents: a systematic literature review and meta-analysis. Neurourol. Urodyn. 40(1), 28–37 (2021).
• This systematic literature review and meta-analysis highlights the risk of dementia among people taking various anticholinergic medications with a particular emphasis on those prescribed for overactive bladder.
6.
American Geriatrics Society Beers Criteria Update Expert Panel. American Geriatrics Society 2023 updated AGS Beers Criteria® for potentially inappropriate medication use in older adults. J. Am. Geriatr. Soc. 71(7), 2052–2081 (2023).
• These guidelines indicate that older adults should avoid anticholinergic medications owing to increased risk of associated adverse effects including cognitive decline, delirium and falls/fractures.
7.
American Geriatrics Society Beers Criteria Alternatives P. Steinman MA. Alternative treatments to selected medications in the 2023 American Geriatrics Society Beers Criteria®. J. Am. Geriatr. Soc. 73(9), 2657–2677 (2025).
8.
Cameron AP, Chung DE, Dielubanza EJ et al. The AUA/SUFU guideline on the diagnosis and treatment of idiopathic overactive bladder. J. Urol. 212(1), 11–20 (2024).
• These updated guidelines from the AUA and SUFU recommend that clinicians discuss differences in side effect profiles between anticholinergic medications and β3 adrenergic receptor agonists to choose a pharmacologic treatment option that incorporates shared-decision making.
9.
Coyne KS, Sexton CC, Vats V, Thompson C, Kopp ZS, Milsom I. National community prevalence of overactive bladder in the United States stratified by sex and age. Urology 77(5), 1081–1087 (2011).
10.
Gormley EA, Lightner DJ, Burgio KL et al. Diagnosis and Treatment of Overactive Bladder (Non-Neurogenic) in Adults: AUA/SUFU Guideline. American Urological Association, MD, USA (2019).
11.
Menhaji K, Cardenas-Trowers OO, Chang OH, Hall EF, Ringel NE, Falk KN. Anticholinergic prescribing pattern changes of urogynecology providers in response to evidence of potential dementia risk. Int. Urogynecol. J. 32(10), 2819–2826 (2021).
12.
Goldman HB, Anger JT, Esinduy CB et al. Real-world patterns of care for the overactive bladder syndrome in the United States. Urology 87, 64–69 (2016).
13.
Kinlaw AC, Jonsson Funk M, Conover MM, Pate V, Markland AD, Wu JM. Impact of new medications and $4 generic programs on overactive bladder treatment among older adults in the United States, 2000–2015. Med. Care 56(2), 162–170 (2018).
14.
Linder BJ, Gebhart JB, Elliott DS, Van Houten HK, Sangaralingham LR, Habermann EB. National patterns of filled prescriptions and third-line treatment utilization for privately insured women with overactive bladder. Female Pelvic Med. Reconstr. Surg. 27(2), e261–e266 (2021).
15.
Carr DN, Macharia A, Hacker MR, Winkelman WD. Despite recommendations, anticholinergics account for the majority of prescriptions to treat overactive bladder in the United States. Urogynecology (Phila) 29(5), 497–503 (2023).
16.
Chua KJ, Patel HV, Tabakin A et al. Yearly trends of overactive bladder medication usage. Urol. Pract. 8(5), 546–554 (2021).
• This evaluation of the US Centers for Medicare & Medicaid Services (CMS) data from 2013 to 2017 showed that oxybutynin was the most prescribed overactive bladder (OAB) medication.
17.
Duperrouzel C, Martin C, Mendell A et al. Healthcare and economic burden of anticholinergic use in adults with overactive bladder: a systematic literature review. J. Comp. Eff. Res. 11(18), 1375–1394 (2022).
• This systematic literature review demonstrates increased healthcare utilization and costs associated with increased anticholinergic burden, switching anticholinergic treatments and potentially inappropriate use of anticholinergics in patients with OAB.
18.
Regenstrief Institute, Inc. Aging Brain Program of the Indiana University Center for Aging Research. Anticholinergic Cognitive Burden Scale 2012 update (2012). Available from: (Accessed: 12 June 2024). https://corumpharmacy.com/wp-content/uploads/2020/08/Anticholinergic-cognitive-burden-scale.pdf
19.
Ali M, Grogan S, Powell S et al. Qualitative analysis of factors influencing patient persistence and adherence to prescribed overactive bladder medication in UK primary care. Adv. Ther. 36(11), 3110–3122 (2019).
20.
Benner JS, Nichol MB, Rovner ES et al. Patient-reported reasons for discontinuing overactive bladder medication. BJU Int. 105(9), 1276–1282 (2010).
• This survey study of people with OAB with ≥1 prescription for an anticholinergic evaluated the reasons for discontinuation and found that most discontinuations were owing to unmet treatment expectations and/or tolerability.
21.
Yoshida M, Kato D, Nishimura T, Van Schyndle J, Uno S, Kimura T. Anticholinergic burden in the Japanese elderly population: use of antimuscarinic medications for overactive bladder patients. Int. J. Urol. 25(10), 855–862 (2018).
22.
Araklitis G, Robinson D, Cardozo L. Cognitive effects of anticholinergic load in women with overactive bladder. Clin. Interv. Aging 15, 1493–1503 (2020).
23.
Chatterjee S, Walker D, Kimura T, Aparasu RR. The costs and healthcare resource utilization associated with anticholinergic burden in long-stay nursing home residents with overactive bladder in the US. Pharmacoecon. Open 5(4), 727–736 (2021).
24.
Lozano-Ortega G, Schermer CR, Walker DR et al. Fall/fracture-related healthcare costs and their association with cumulative anticholinergic burden in people with overactive bladder. Pharmacoecon. Open 5(1), 45–55 (2021).
25.
Szabo SM, Gooch K, Schermer C et al. Association between cumulative anticholinergic burden and falls and fractures in patients with overactive bladder: US-based retrospective cohort study. BMJ Open 9(5), e026391 (2019).
26.
Yehoshua A, Chancellor M, Vasavada S et al. Health resource utilization and cost for patients with incontinent overactive bladder treated with anticholinergics. J. Manag. Care Spec. Pharm. 22(4), 406–413 (2016).
27.
Asche CV, Kim J, Kulkarni AS, Chakravarti P, Andersson KE. Presence of central nervous system, cardiovascular and overall co-morbidity burden in patients with overactive bladder disorder in a real-world setting. BJU Int. 109(4), 572–580 (2012).
28.
Allergan. SANCTURA® (trospium chloride). Full Prescribing Information. Allergan, Inc, CA, USA (2012).
29.
Astellas Pharma US, Inc. VESIcare® (solifenacin succinate). Full Prescribing Information. Astellas Pharma US, Inc, IL, USA (2020).
30.
Janssen Pharmaceuticals. Ditropan XL (oxybutynin chloride extended release tablets). Full Prescribing Information, NJ, USA (2016).
31.
Novartis Pharma Stein AG. ENABLEX® (darifenacin). Full Prescribing Information. Novartis Pharma Stein AG, Switzerland (2008).
32.
Pfizer. Toviaz® (fesoterodine fumarate). Full Prescribing Information. Pfizer Inc, NY, USA (2011).
33.
Pfizer. Detrol (tolterodine tartrate). Full Prescribing Information. Pfizer, NY, USA (2012).
34.
Lam S, Hilas O. Pharmacologic management of overactive bladder. Clin. Interv. Aging 2(3), 337–345 (2007).
35.
National Institute for Diabetes and Digestive and Kidney Diseases. Definition & facts of urinary retention (2019). Available from: (Accessed: 15 August 2025). https://www.niddk.nih.gov/health-information/urologic-diseases/urinary-retention/definition-facts
36.
Guo D, Lin T, Deng C, Zheng Y, Gao L, Yue J. Risk factors for delirium in the palliative care population: a systematic review and meta-analysis. Front. Psych. 12, 772387 (2021).
37.
Pfizer. Effexor XR (venlafaxine). Full Prescribing Information. Pfizer (2017).
38.
Zeevi N, Pachter J, McCullough LD, Wolfson L, Kuchel GA. The blood-brain barrier: geriatric relevance of a critical brain-body interface. J. Am. Geriatr. Soc. 58(9), 1749–1757 (2010).
39.
Chancellor M, Boone T. Anticholinergics for overactive bladder therapy: central nervous system effects. CNS Neurosci. Ther. 18(2), 167–174 (2012).
40.
Ieong C, Chen T, Chen S et al. Differences of anticholinergic drug burden between older hospitalized patients with and without delirium: a systematic review and meta-analysis based on prospective cohort studies. BMC Geriatr. 24(1), 599 (2024).
41.
Taylor-Rowan M, Kraia O, Kolliopoulou C et al. Anticholinergic burden for prediction of cognitive decline or neuropsychiatric symptoms in older adults with mild cognitive impairment or dementia. Cochrane Database Syst. Rev. 8(8), CD015196 (2022).
42.
Campbell N, Shiozawa A, Epstein A, Walker D, Lockefeer A, Hines L. A retrospective study of the prevalence of anticholinergic poly-pharmacy use and its associated outcomes among Medicare patients with overactive bladder. J. Am. Geriatr. Soc. 69, S139 (2021).
43.
Delara M, Murray L, Jafari B et al. Prevalence and factors associated with polypharmacy: a systematic review and Meta-analysis. BMC Geriatr. 22(1), 601 (2022).
Information & Authors
Information
Published In
Copyright
© 2025 Sumitomo Pharma America, Inc. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 17 April 2025
Accepted: 29 October 2025
Published online: 3 December 2025
Keywords:
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Health outcomes and costs in patients prescribed anticholinergic medications for overactive bladder. (2025) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2025-0054
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Jainam Shah, Sachin Pathuri, Richard Adamovich-Zeitlin, Jessinta Oseni, Joshua Ong, John P. Berdahl, Jeffrey S. Schultz, Anurag Shrivastava, Epidemiology, Safety of Dilation, and Medication-Associated Risk of Acute Angle-Closure Crisis in the United States, American Journal of Ophthalmology, 10.1016/j.ajo.2026.07.007, (2026).