Impact analysis of expanded access to ketamine for treatment-resistant depression
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: This study aimed to estimate the economic impacts of expanded access to ketamine relative to electroconvulsive therapy (ECT) by offering intravenous ketamine to US patients with nonpsychotic treatment-resistant depression (TRD) and moderate-to-severe depression. Materials & methods: A population-level Markov simulation model with key parameters from a randomized trial was used to simulate the economic impacts of managing TRD with intravenous ketamine versus ECT over a 5-year horizon. Health states included response of depression in the acute treatment phase and continued treatment and relapse in the maintenance phase. The model estimated costs associated with healthcare utilization (direct costs) and time loss (indirect costs) from patient, caregiver, payer and societal perspectives. Model uncertainty was assessed with one-way sensitivity, probabilistic sensitivity and scenario analyses. Results: In year 1, our model included 350,000 eligible patients. In years 2 through 5, our model added 11,296 eligible patients annually. Expanded access to ketamine to manage TRD was projected to increase the number of patients receiving treatment by 75,000 patients in year 1 and 4292 patients annually in subsequent years. Over 5 years, expanded access to ketamine would result in a net positive societal savings of $828.2 million annually ($95.3 million to patients and $743.7 million to payers). However, expanded ketamine access would impose an additional $10.8 million burden on caregiver time annually. Conclusion: For US patients with TRD and moderate-to-severe depression, ketamine may be a noninferior treatment relative to ECT to improve depression symptoms. Expanded access to ketamine treatment would result in net savings to the patients, payers and society.
Plain language summary
What was the aim of this research?
To estimate the economic impacts of expanded access to intravenous ketamine relative to electroconvulsive therapy by offering ketamine to US patients with treatment-resistant depression and moderate-to-severe depression without psychotic features from the patient, caregiver, payer and societal perspectives.
How was the research carried out?
A population level Markov simulation model and annual Markov cycles was performed out to 5 years. Model parameters were identified from the literature, publicly available data sources and input from a clinical consultant. Sensitivity analyses were used to explore variations in some inputs and assumptions.
What were the results?
Results suggest that expanded access to intravenous ketamine has the potential to increase the number of patients in treatment for treatment-resistant depression and lead to annual savings to society of US$828.2 million in total or US$19,940 per patient-in-treatment. Patients and payers incurred a total saving of $95.3 million and $743.7 million, respectively, annually. However, caregivers incurred an additional cost of $10.8 million annually.
What do the results of the study mean?
Expanded access to ketamine would result in net annual savings to society, patients and payers but would impose burdens on caregivers annually due to the additional time spent transporting patients to and from treatment.
Major depressive disorder (MDD) is a common but serious mental health condition characterized by at least 2 weeks of persistent feelings of sadness or loss of interest that affects daily activities [1]. In 2021, an estimated 21.0 million US adults had at least one major depressive episode, and approximately half of these individuals received medications for their condition [2]. Failure of at least two antidepressants to improve an individual’s MDD symptoms is referred to as treatment-resistant depression (TRD), which affects about a third of individuals with MDD. TRD can have wide-ranging clinical, economic and social impacts. For example, TRD is associated with substantially higher incidence of intentional self-harm, healthcare utilization and clinical and functional disability [3–5]. The economic burden of MDD among US adults was estimated at $326 billion (2020 US dollars) annually in direct medical costs and indirect costs, with TRD accounting for 27–42% of this burden [6].
For decades, electroconvulsive therapy (ECT) has been one of the most effective strategies for management of TRD [7]. ECT occurs in an inpatient or outpatient setting and involves brief electrical stimulation of the brain while the patient is under anesthesia [8]. The initial course of treatment with ECT consists of 6–12 treatments over 3–5 weeks [7,8]. After a patient has had sufficient clinical improvement, they typically continue treatment with maintenance ECT, which means a reduced frequency of treatment sessions, and/or antidepressant medications to help prevent relapse [9].
Ketamine was approved by the US FDA as a sedative, analgesic and general anesthetic in 1970, and researchers later found that ketamine has a rapid antidepressant effect in patients with MDD [10]. Ketamine is typically administered intravenously in an outpatient setting with an initial course of treatment consisting of two treatments per week for 3 weeks [7].
Anand et al. [7] conducted a randomized controlled trial to compare the effectiveness of ECT and intravenous ketamine for management of nonpsychotic TRD. At five urban sites between March 2017 and September 2022, 403 patients with TRD aged from 21 to 75 years received either ECT or intravenous ketamine following clinical practice guidelines. The primary outcome was response to treatment with secondary outcomes including scores on memory tests and patient-reported quality of life. After the initial course of treatment, patients who had a response were followed for 6 months. A total of 55.4% of patients treated with intravenous ketamine and 41.2% of patients treated with ECT had a response. Anand et al. [7] concluded that ketamine was noninferior to ECT for management of nonpsychotic TRD.
The purpose of the current study was to estimate the economic impacts of expanded access to ketamine by offering intravenous ketamine to previously offered ECT patients for management of nonpsychotic TRD per Anand et al. [7] We identified resource requirements for both treatments and evaluated changes in direct costs associated with healthcare utilization and indirect costs associated with time loss from the patient, caregiver, payer and societal perspectives over a 5-year horizon.
Materials & methods
We developed a population-level Markov simulation model to estimate the outcomes over a 5-year horizon under two outpatient treatment regimens for management of nonpsychotic TRD. Throughout this paper, we refer to the adult population with nonpsychotic TRD and moderate-to-severe depression that are offered ECT or ketamine for TRD as the ‘eligible patient population’. Under presumed standard of care (SC), we assume that some eligible patients are offered ECT and others are offered ketamine in an outpatient setting. Under the expanded access, we assume that 100% of the eligible patients are offered ketamine. The model estimates the costs associated with healthcare utilization (direct costs) and time loss (indirect costs) across two treatments (ECT or ketamine) under two treatment regimens (SC or expanded access) from the patient, caregiver, payer and societal perspectives.
Model
The economic model in this study has two distinct components: a 1-month decision tree that simulates the outcome of an acute treatment phase (i.e., response) and a Markov model that captures the outcome of a maintenance phase (i.e., treatment continuation and relapse) over the remainder of the time horizon (Figure 1). The Markov component of the model has a 1 year (12 month) cycle, except for the first year of the cohort, which is an 11-month cycle. The model simulates the outcomes over 5 years for consistency with past studies [11–14].
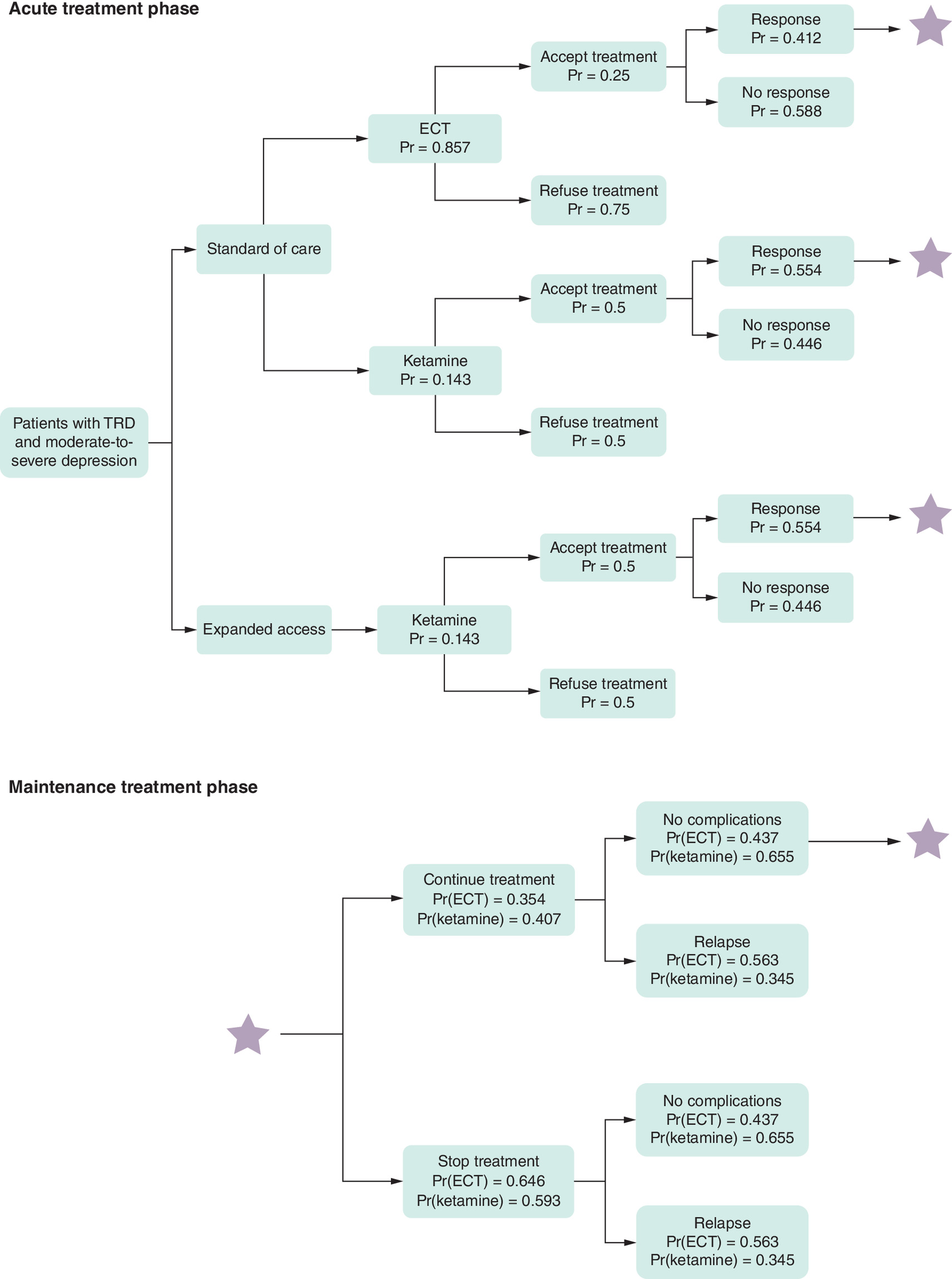
Figure 1. Model structure of expanded access to ketamine for the management of treatment-resistant depression.
This is the Markov model used for the simulation analysis. In the acute treatment phase, the standard of care pathway indicates that the eligible patient population will be offered ECT or ketamine to manage TRD and will continue through the end of a 5-year model analysis. The ‘expanded access’ pathway represents an alternative scenario in which all eligible patient population are offered ketamine. The stars on the far right of this exhibit indicate that patients who respond to treatment in the acute phase may continue into the maintenance phase, with the same possible outcomes for each cycle of the Markov model shown in the lower portion of the figure. The probabilities of transitioning to each of the post-acute states differ depending on the treatment used.
ECT: Electroconvulsive therapy; Pr: Probability; TRD: Treatment-resistant depression.
In the first year of this population simulation model, all eligible patients enter the model as the first cohort. In each subsequent year, a new cohort of eligible incident patients is added. Patients with nonpsychotic TRD enter the acute treatment phase of the model upon being offered treatment choices between ECT and intravenous ketamine. Once patients accept the treatment offer, we assume that every patient has a psychiatric diagnostic evaluation session prior to their initiation of 3 weeks of acute care.
After acute treatment, patients enter the health states of response to or no response to treatment. Patients in the cohort who are in a state of response to treatment are then included in the model’s Markov component, which captures the maintenance treatment phase. At every cycle, patients face the probability of stopping treatment and relapse. Patients who experience no complications while continuing maintenance treatment enter the next cycle of the Markov component. Patients who relapse while continuing treatment stay in ‘relapse’ state, and patients who stop treatment stay in either ‘relapse’ or ‘no complications’ states for the remainder of the time horizon.
In our model, patients enter an absorbing state if they enter ‘refuse treatment’, ‘no response’, ‘relapse’, or ‘no complications’ states while stopping treatment. Patients exit the model due to death. Mortality rates are assumed to be independent of treatment arms due to lack of long-term comparative clinical data.
Under the expanded access, we assume that 100% of the eligible patients are offered intravenous ketamine. The probabilities of transitioning to each of the states are different depending on the treatment used but are the same across SC and expanded access treatment regimes.
Model parameters
Supplementary Table A1 includes a full list of model parameters, values and sources. Where possible, we obtained model parameters from published estimates using Anand et al. [4]. Of note, we did not have access to or conduct analyses on the original data of Anand et al. [4]. Otherwise, we obtained model parameters from various sources, including literature, or estimated parameters using publicly available datasets. A 3% annual discount rate was applied to future costs, and we report all costs in 2024 US dollars.
Population & clinical parameters
We obtained a range for the number of adults in the USA with TRD and moderate-to-severe depression being offered ECT or intravenous ketamine for treatment of TRD in the base year from the clinical expert [15]. We used a lower bound of the range to include patients with nonpsychotic TRD per Anand et al. [4]. We then converted this number to the proportion of patients being offered each of the studied treatments, using the estimated number of adults in the USA and disease prevalence [16], and combined the proportion with the incidence rate of patients with TRD to estimate the number of new adult cases expected in the out-years of the model. Under SC, we assumed that 85.7% of the eligible patient population are offered ECT and 14.3% are offered intravenous ketamine [15].
We obtained parameter values for the model impacts by treatment (i.e., ECT or ketamine) from the results in Anand et al. (Supplementary Table A1). We assumed that 25% of patients who are offered ECT accept the treatment and that 50% of patients who are offered ketamine accept the treatment [15]. We also assumed a mortality rate of 0.48%, which considers the age and sex distribution of the population with depression [17].
Direct cost parameters
Direct cost parameters included direct patient copayments and medical costs for intravenous ketamine and ECT treatments and the continuing healthcare cost of TRD. Using the 2016–2019 Medical Expenditure Panel Survey data [18], we estimated that patients with depression paid 10% of the total healthcare costs. We used this estimate to calculate the direct healthcare costs borne by patients and assumed that the remaining 90% was borne by payers. We used the 2024 Medicare Physician Fee Schedule and Outpatient Prospective Payment System to estimate the average per-session costs of psychiatric evaluation, ECT and intravenous ketamine. We calculated average annual treatment costs by multiplying the average number of sessions by the per-session cost. We obtained the average number of acute-care sessions from Anand et al. and assumed that maintenance treatment was given once per month for the remainder of the time horizon.
Our estimate of per-session ECT cost included cost of medications and cost of ECT (CPT 90870), which included the cost of performing ECT, anesthesia services and recovery room service in a hospital outpatient setting. For medications, we included the cost of anesthesia and muscle relaxant using the Department of Veterans Affairs Federal Supply Schedule.
Our estimate for per-session intravenous ketamine cost included cost of the medication, cost of the physician visit and the cost of a 50 min observation after each dosing visit. For the cost of ketamine medication, we utilized the Veterans Affairs Federal Supply Schedule. We assumed patients would have a physician visit at each session. We used the reimbursement rates for a 30–39 min office visit, routine follow-up (CPT 99214) for the physician cost, and for a 50 min observation (CPT 99415).
Patients in both treatment arms also received a psychiatric diagnostic evaluation prior to initiating their treatment, which we costed out using a reimbursement rate for a 90 min office visit (CPT 99205). Patients who enter ‘refuse treatment’, ‘no-response’, or ‘relapse’ states incur the healthcare costs of TRD for the remainder of the time horizon obtained from Pilon et al. [19]. Patients who enter ‘no complications’ while stopping treatment incur no costs for the remainder of the time horizon. In practice, patients who stop treatment and experience no complications are likely to continue taking antidepressant medications. However, following clinical expert guidance, we did not incorporate these medication costs in our model as the costs are minimal at the per-person level (approximately $100 per year) and are incurred regardless of the treatment arm [17].
Indirect costs parameters
Indirect costs included the value of patient time and unpaid time provided by caregivers who accompanied the patient to appointments. To value patient and caregiver time, we used hourly wages based on the 2021 national annual earnings estimates by age/sex from Current Population Survey 2022 data adjusted to 2024 dollars and assuming a 45.3% fringe benefits rate [20]. We valued patient time using an hourly wage of $42.73 that was adjusted for the age distribution of the TRD population [16]. We valued unpaid time provided by caregivers using an hourly wage of $54.37 that was adjusted for the age distribution of caregivers [21]. We assumed that each ECT and ketamine session takes 2 and 2.5 h, respectively, including the time obtaining treatment and in observations after treatment and 1 h for traveling to and from treatment [15]. For patients receiving ECT, we further assumed that patients take the whole day off work (i.e., 8 h) for recovery and caregivers take off 2 h (the length of time of each ECT session plus travel time) [15]. We also assumed that 100% of patients, regardless of treatment arm, are accompanied to treatment by their caregivers [15]. Furthermore, we assumed that 55 and 65% of patients and caregivers, respectively, are in the labor force [20,22].
Societal cost estimation
To estimate the total societal costs, we summed the costs of patient time and out-of-pocket healthcare costs, caregiving time and payers. These calculations avoid double-counting costs to patients and payers.
Sensitivity & scenario analyses
We assessed the sensitivity of our model results using probability and one-way sensitivity analyses. Probability sensitivity analysis (PSA) produces a CI for each outcome based on 1000 iterations of the model in which all inputs could vary across a distribution of values. We identified CIs for model results using the 2.5 and 97.5 percentiles of the distribution generated by PSAs of each outcome. One-way sensitivity analyses identify parameters to which model outcomes were most sensitive by allowing the value of one input parameter to vary across a distribution, while holding all other input parameters constant. Parameter values were obtained from the literature, where the 95% CI was assumed to be the upper and lower bounds of published parameter values or varied by ±20%. Supplementary Table A2 shows the ranges and distributions of parameters used in sensitivity analyses.
Additionally, we conducted six scenario analyses. In the first scenario analysis, we changed the offer rate in the expanded access to 50% instead of 100% used in the base case scenario. In the second and third scenario analysis, we assumed that ECT patients take the day of and the day after treatment (i.e., 16 h instead of 8 h) and ketamine patients take an entire day off work (i.e., 8 h instead of 2.5 h). In the fourth scenario, we used relapse rates from alternative sources. Anand et al. [7] reported relapse rates among patients who responded to treatment in the acute phase rather than relapse rates among patients who continued maintenance treatment. Thus, our model implicitly assumed independence between relapse rates and maintenance treatment. Using relapse rates from Nordenskjöld et al. [23] and Daly et al. [24] we relaxed this independence assumption as these studies reported relapse rates among those who entered maintenance treatment. For the fifth and sixth scenario analyses, we used private insurance reimbursement rates, as opposed to Medicare reimbursement rates, for direct healthcare costs. In the fifth scenario analysis, we assumed that payers and patients incur 90% and 10% of the ketamine therapy costs, respectively. This is the same assumption used in the base case scenario. In the sixth scenario analysis, we assumed that patients bear the full direct costs of ketamine therapy.
Results
Population
Population results for the impacts of an expanded access to intravenous ketamine to all eligible patients for management of nonpsychotic TRD are reported in Table 1. Our model included an estimated 350,000 eligible patients in year 1 and added 11,296 eligible incident patients annually in each subsequent year (i.e., years 2 to 5). Findings from our model indicate that expanded access to ketamine would result in 75,000 additional patients in year 1 and 4292 additional patients annually in subsequent years receiving ketamine. This finding is a result of patients being more likely to accept ketamine if the treatment is offered relative to ECT.
| Eligible patient population | A. SC | B. Expanded access to ketamine | Difference (B-A) |
|---|---|---|---|
| Average annual patients in year 1 (n) | |||
| Offered ECT or ketamine | 350,000 | 350,000 | – |
| Receiving acute or maintenance treatment | 100,000 | 175,000 | 75,000 |
| Receiving acute treatment | 100,000 | 175,000 | 75,000 |
| Treatment response | 44,711 | 96,884 | 52,174 |
| Continuing treatment as maintenance | 7235 | 18,559 | 11,324 |
| Refused, no response, relapsed and no complications if stopping treatment | 336,672 | 305,127 | (31,545) |
| Average annual patients in years 2–5 (n) | |||
| Offered ECT or ketamine | 11,296 | 11,296 | – |
| Receiving acute or maintenance treatment | 3869 | 8161 | 4292 |
| Receiving acute treatment | 3227 | 5648 | 2420 |
| Treatment response | 1443 | 3127 | 1684 |
| Continuing treatment as maintenance | 233 | 599 | 365 |
| Receiving maintenance treatment | 642 | 2514 | 1872 |
| Receiving maintenance treatment in total | 875 | 3113 | 2237 |
| Refused, no response, relapsed and no complications if stopping treatment | 361,314 | 331,323 | (29,991) |
Values in parentheses indicate negative values.
ECT: Electroconvulsive therapy; SC: Standard of care.
In year 1 of the model, of the 75,000 additional patients who start acute treatment, 52,174 additional patients respond to acute treatment, and 11,324 of these patients continue treatment into the maintenance phase in the same year. In subsequent model years, of the 2,420 additional patients who start acute treatment each year, 1,684 additional patients respond to acute treatment annually, and 365 of these patients continue treatment into the maintenance phase. Furthermore, another 1,872 patients continue treatment as maintenance for over 1 year annually. As a result, a total of 2,237 additional patients receive treatment as maintenance annually under the expanded access. The expanded access to intravenous ketamine reduces the number of patients who refuse treatment, do not respond, relapse, or have no complications if stopping treatment by 31,545 patients in year 1 and 29,991 patients annually in subsequent years. Overall, 95% to 98% of the patients reach an absorbing state within 1 year of entering the model.
Total costs
Table 2 reports the average cost impacts across all model years. From the patient perspective, we estimated total costs savings of $95.3 million annually, including direct healthcare cost savings of $1.2 million in treatment costs and $81.4 million in continuing healthcare costs for TRD. Additionally, we estimated that patients would reduce time spent in treatment by 544,486 hours resulting in indirect cost savings of $12.7 million annually. This is a result of shorter recovery times with ketamine versus ECT (we assumed patients who receive ECT take off the entire workday).
| Outcome | A. SC | B. Expanded access to ketamine | Difference (B-A) | Annual savings per patient in treatment |
|---|---|---|---|---|
| Patient perspective | ||||
| Time (h) | 1,386,430 | 841,944 | (544,486) | 13 |
| Indirect costs of time | $32,292,416 | $19,582,547 | ($12,709,869) | $310 |
| Treatment costs | $8,215,180 | $6,971,404 | ($1,243,776) | 30 |
| Continuing healthcare costs of TRD | $988,630,799 | $907,241,937 | ($81,388,862) | $1,960 |
| Total patient healthcare costs | $996,845,979 | $914,213,341 | ($82,632,638) | $1,990 |
| Total patient costs | $1,029,138,395 | $933,795,888 | ($95,342,507) | $2,300 |
| CI | ($137,811,364) – ($58,361,467) | |||
| Caregiver perspective | ||||
| Time (h) | 412,117 | 743,148 | 331,031 | (8) |
| Total caregiver costs | $13,546,010 | $24,394,049 | $10,848,039 | ($260) |
| CI | $4,885,583 – $17,941,661 | |||
| Payer perspective | ||||
| Treatment costs | $73,936,621 | $62,742,637 | ($11,193,984) | $270 |
| Continuing healthcare costs of TRD | $8,897,677,188 | $8,165,177,429 | ($732,499,759) | $17,640 |
| Total payer costs | $8,971,613,809 | $8,227,920,066 | ($743,693,743) | $17,910 |
| CI | ($1,122,572,981) – ($440,192,587) | |||
| Societal costs | ||||
| Total societal costs | $10,017,095,720 | $9,186,110,003 | ($828,188,211) | $19,940 |
| CI | ($1,236,038,429) – ($503,821,715) | |||
Negative values are in parenthesis and indicate impacts avoided or costs saved associated with the expanded practice.
ECT: Electroconvulsive therapy; SC: Standard of care; TRD: Treatment-resistant depression.
We estimated that caregivers would incur additional costs under the expanded access scenario due to more patients receiving treatment who would require a caregiver to take them to and from appointments. We estimated that caregivers would spend an additional 331,031 h transporting patients to and from treatment which translated to indirect costs of $10.8 million.
The total costs savings for payers were estimated to be $743.7 million under the expanded access scenario compared with the SC scenario, including $11.2 million in direct treatment costs and $732.5 million in continuing healthcare costs for TRD. As a result, the expanded access to intravenous ketamine for the management of nonpsychotic TRD would result in potential societal cost savings of $828.2 million.
Per-patient costs
We estimated per patient savings of $2300 from the patient perspective in the expanded access scenario, including $1990 in out-of-pocket healthcare costs and $310 from less time spent in treatment. However, the caregiver costs would increase by $260 per patient for the additional time spent transporting patients to and from treatment. We also estimated savings of $17,910 per patient in treatment from the payer perspective, and total savings of $19,940 per patient in treatment from the societal perspective under the expanded access scenario.
Sensitivity & scenario analyses
Sensitivity analyses
PSA results of CIs for the total cost outcomes for patients, caregivers, payers and society are also shown in Table 2. Ranges that include 0 indicate uncertainty about whether the expanded access to ketamine compared with SC would result in net savings. None of the CIs for the cost outcomes include 0, suggesting that the eligible patient population’s expanded access to ketamine can result in downstream cost positive savings to patients, payers and society.
Figure 2 displays the results from our one-way sensitivity analyses showing parameters to which the total societal cost savings were most sensitive. The total societal cost savings were most sensitive to the relapse rate if patients continued the use of ketamine into the maintenance phase (range: 0.28–0.41); followed by the proportion of patients being offered ECT (range: 0.63–1.00). Total societal cost savings were also sensitive to the proportion of patients with moderate-to-severe depression (range: 0.68–1.00), the prevalence of patients with a major depressive episode who received treatment (range: 0.01–0.02) and the response rate to ketamine (range: 0.51–0.67). Supplementary Figure A1 displays the full list of parameters from the most to the least sensitive and shows that savings are positive for all one-way sensitivity analyses.
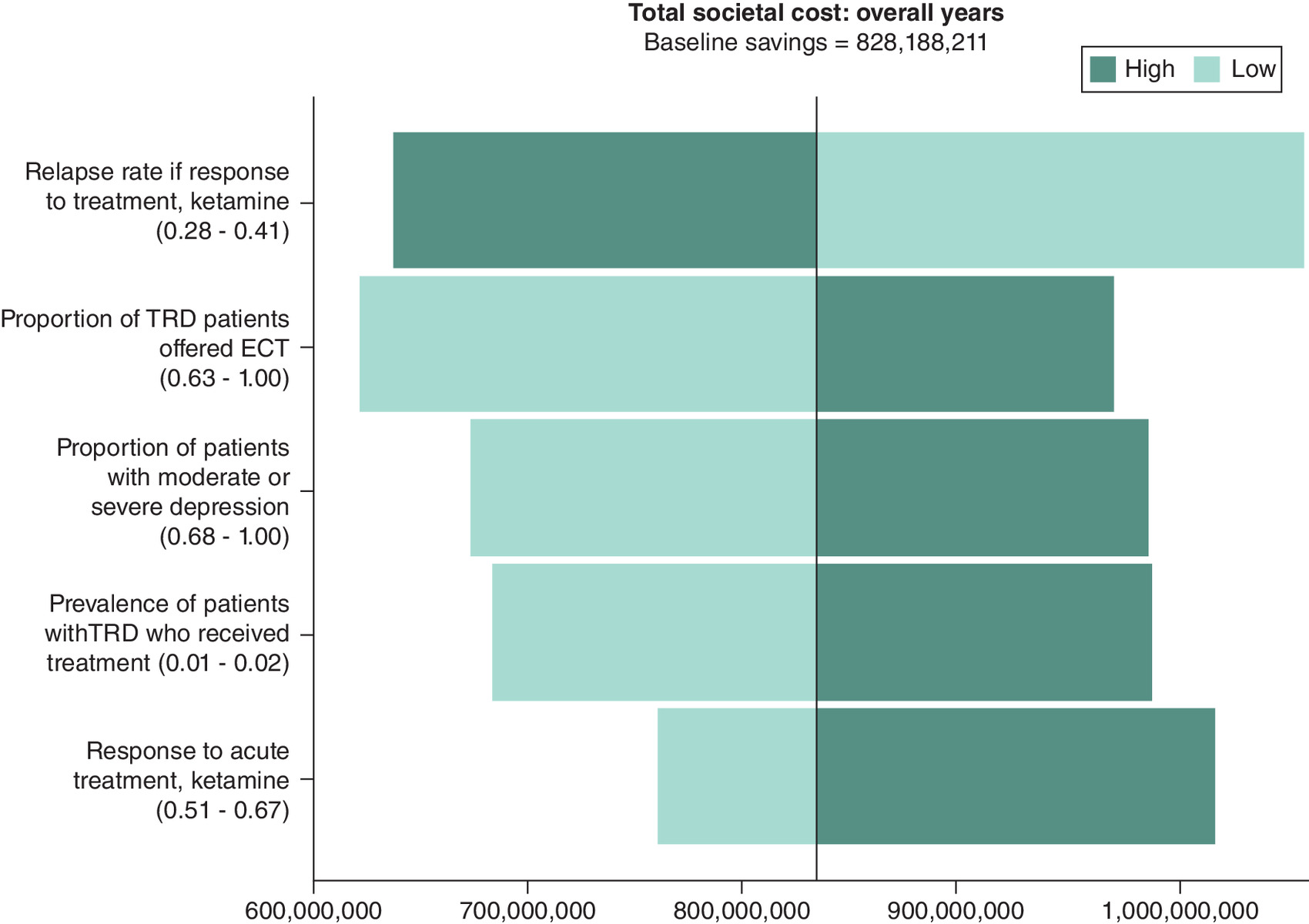
Figure 2. Tornado diagram of the difference in annual societal costs between expanded and standard of care practice over a 5-year horizon.
The vertical line represents the baseline saving estimate obtained from the main results.
ECT: Electroconvulsive therapy; TRD: Treatment-resistant depression.
Scenario analyses
Table 3 reports scenario analysis results for the total cost outcomes for patients, caregivers, payers and society. Results from our main scenario suggested that the annual total societal cost savings were $828.2 million. In the first scenario analysis, we assumed that 50% of the eligible patient population is offered intravenous ketamine and the other 50% is offered ECT. This scenario suggests a total societal cost savings of $345.1 million.
| Outcome | Total patient costs | Total caregiver costs | Total payer costs | Total societal costs |
|---|---|---|---|---|
| Base case | $95,342,507 | $(10,848,039) | $743,693,743 | $828,188,211 |
| Scenario analysis 1: 50% expansion | $39,726,045 | $(4,520,016) | $309,872,393 | $345,078,421 |
| Scenario analysis 2: patients receiving ECT take the 2 days off work | $123,850,636 | ($10,848,039) | $743,693,743 | $856,696,339 |
| Scenario analysis 3: patients receiving ketamine take the whole day off work | $62,757,256 | ($10,848,039) | $743,693,743 | $795,602,960 |
| Scenario analysis 4: varying relapse rates | $130,085,563 | $(11,654,173) | $1,053,556,145 | $1,171,987,535 |
| Scenario analysis 5: private reimbursement rates | $84,778,655 | $(10,848,039) | $648,619,074 | $722,549,690 |
| Scenario analysis 6: private reimbursement rates and patients paid 100% of ketamine costs | $(57,244,608) | $(10,848,039) | $790,642,337 | $722,549,690 |
Negative values are in parenthesis and indicate increased costs associated with the expanded access.
ECT: Electroconvulsive therapy.
In the second scenario analysis, we assumed that ECT patients take the day of and the day after treatment off work (i.e., 16 h instead of 8 h). In the third scenario analysis, we assumed that patients receiving ketamine take an entire day off work (i.e,. 8 h instead of 2.5 h). Our initial assumptions about the time missed from work due to ECT/ketamine treatment may be an underestimate as some patients undergoing treatment may not work during the treatment days. These scenarios suggest a total societal cost savings of $856.7 million and $795.6 million annually under the second and third analyses, respectively. Results of these scenario analyses indicate that our main findings on the cost savings associated with expanded ketamine treatment are robust.
In the fourth scenario analysis, we used alternative input values [23,24] for the probability of relapse if continuing treatment after the acute phase. Nordenskjöld et al. [23] reported an annual relapse rate of 32% if continuing ECT, and Daly et al. reported an annual rate of 26% if continuing ketamine. This scenario suggests a total societal cost savings of $1172.0 million annually due to the expanded access to ketamine.
The fifth and sixth scenario analyses used private insurance reimbursement rates such that the treatment cost per session was $2500 for ECT and $600 for ketamine; the healthcare costs of TRD were $21,767. These scenarios suggest a total societal cost savings of $722.5 million annually due to the expanded access to ketamine. The sixth-scenario analysis further assumes that payers do not cover ketamine reflecting the current reimbursement practice of ketamine for TRD. Patients will pay the full cost of $600 out-of-pocket for ketamine treatment per session during both the acute and maintenance phases. While the total societal cost savings of $722.5 million annually due to the expanded access to ketamine remained unchanged, this assumption shifted the cost savings from patients to payers and increased the costs for patients. Under this sixth-scenario analysis, expanded access to ketamine would result in an additional $57.2 million in total patient costs as opposed to a cost savings of $84.8 million under the fourth scenario analysis. For simplicity, both of these scenarios assume that the probability of continued treatment for ECT (40.7% if response to treatment) and ketamine (35.4% if response to treatment) does not change from the base scenario even if the payer is different.
Discussion
In this analysis of expanded access to intravenous ketamine versus ECT to manage TRD among patients with nonpsychotic TRD and moderate-to-severe depression, we found that the expanded access would reduce societal costs by $828.2 million annually compared with the SC with almost 90% of the savings accrued to payers. In the sensitivity analyses, we found that while the total societal cost savings from the expansion is most sensitive to the relapse rate of patients continuing the use of ketamine into the maintenance phase, expanded access to ketamine to the eligible patient population can result in cost savings to the patients, payers and society under all one-way and probabilistic sensitivity analyses.
We also found that the downstream cost savings to the patients, payers and society from the expanded access to intravenous ketamine hold when using alternative values for relapse rates and reimbursement costs from private insurance. However, if patients pay the full treatment costs for ketamine, patients will incur increased costs, rather than cost savings, under the expanded access scenario. This finding highlights the importance of healthcare coverage in improving access to intravenous ketamine treatment.
It is worth noting that caregivers would incur increased costs from transporting patients to and from treatment under the expanded access to ketamine scenario. The finding of increased burdens on caregivers holds under various sensitivity and scenario analyses. This finding highlights the vital role of caregivers in helping patients with (nonpsychotic) TRD to receive treatments. Along with improving patient access to ketamine, payers and policymakers should also consider improving transportation services that help patients get to medical appointments. This would ensure that patients can receive the treatment they need.
To our knowledge, no other published studies compared the economic outcomes of ECT and intravenous ketamine treatments. However, a few studies have examined the economic value of ECT or ketamine treatment for patients with (nonpsychotic) TRD relative to other treatment options. Ross et al. found that offering ECT after two failed trials of pharmacotherapy or psychotherapy, which is in alignment with the current clinical practice, is most likely to maximize the treatment’s value relative to pharmacotherapy or psychotherapy for the healthcare sector [17]. Brendle et al. found that intravenous ketamine dominates esketamine nasal spray in terms of maximizing the treatment value for patients and healthcare sector [25]. In combination with prior studies, our analysis provides additional evidence suggesting that ketamine can be an attractive treatment option for patients, payers and the society.
Limitations
Our analysis has several limitations. Our model may overstate the potential benefits of expanded access to ketamine. Our model used findings in Anand et al. [7] that reported lower response of ECT compared with other studies. Mathew et al. attributed the lower ECT response rate in Anand et al. [7] to the possibility that elderly patients and patients in inpatient settings were insufficiently enrolled, and that the trial also excluded patients with psychotic features, who are more likely to respond to ECT treatment [26]. However, results from the one-way sensitivity analysis suggested that the response rate of ECT was not one of the inputs to which the potential benefits of expanded access to ketamine on total societal cost savings are most sensitive.
Our cost inputs for intravenous ketamine treatment assumed that payers provide coverage for ketamine infusion, and the reimbursement amount is based on a billing guideline for ketamine infusion [27]. Thus, our estimate of per-session ketamine cost would be a lower bound of the reimbursement amount if ketamine were covered by insurance. Indeed, when using alternative values for reimbursement rates from private insurance, our model suggests higher societal cost savings than those under the Medicare reimbursement rates.
Our model includes some simplifying assumptions to reduce the complexity of real-world clinical practice. For example, we assumed indefinite maintenance use, excluded treatment effects on mortality, and assumed that patients who enter ‘refuse treatment’, ‘no-response’, or ‘relapse’ states would remain in these health states until the end of time horizon. However, we applied these assumptions across both treatments (ECT and ketamine) and treatment regimens (SC and expanded access). In clinical practice, these patients may try the other therapy (ECT or ketamine, depending on which they started with) or another type of therapy that is not captured in the model. A more complex model may be needed to compare a range of alternative therapies (such as repetitive transcranial magnetic stimulation or other ketamine administration modalities [28] such as intranasal ketamine, non parenteral ketamine for home use, or ketamine assisted psychotherapy) for TRD or and to fully capture the impacts of the disorder and alternative treatment strategies.
Conclusion
By modeling the expanded access to intravenous ketamine to manage nonpsychotic TRD among the eligible patient population per Anand et al. [7], we found that expanded access to ketamine has the potential to increase the number of patients in treatment by 75,000 in the first year and 4292 patients annually in subsequent years. Across all 5 years of the model, the expanded access to ketamine to manage nonpsychotic TRD would decrease the annual costs to payers by $743.7 million and patients by $95.3 million but would impose an additional burden of $10.8 million on caregivers in time cost annually. The expanded access to intravenous ketamine to all eligible patients would result in a net positive savings to the society of $828.2 million annually.
Summary points
•
Major depressive disorder is a common but serious mental health condition that affected an estimated 21.0 million US adults in 2021 with an economic burden of $326 billion annually in direct medical and indirect costs.
•
Failure of at least two antidepressants to improve an individual’s depressive symptoms is referred to as treatment-resistant depression (TRD), which affects about a third of individuals with major depressive disorder. Management of TRD may include electroconvulsive therapy (ECT) or ketamine.
•
Previous research supports that intravenous ketamine is noninferior to ECT for managing TRD.
•
This paper presents a population-level Markov simulation model to estimate the economic impacts of expanded access to intravenous ketamine relative to ECT by offering ketamine to US patients with TRD and moderate-to-severe depression over 5 years.
•
Model parameters were identified from the literature, publicly available data sources and input from a clinical consultant.
•
Results suggest that expanded access to ketamine has the potential to increase the number of patients in treatment for TRD and lead to annual savings to society of US$828.2 million in total or US$19,940 per patient-in-treatment.
•
Expanded access to ketamine would result in net annual savings to patients and payers but would impose burdens on caregivers annually due to the additional time spent transporting patients to and from treatment.
Author contributions
T Lu and O Khavjou were responsible for study conception and design. T Lu was responsible for developing the model. T Lu and M Dempsey were responsible for conducting data analysis. T Lu, S D'Angelo and Z Tayebali were drafting of the manuscript. T Lu, K Giombi and O Khavjou were responsible for revisions to the manuscript.
Acknowledgments
The authors thank JW Luccarelli, TJ Hoerger, B Lawrence and C Quinn for valuable feedback.
Disclaimer
All statements, findings and conclusions in this publication are solely those of the authors and do not necessarily represent the views of the Patient-Centered Outcomes Research Institute (PCORI). This publication was developed through a contract (PCORI contract no. IDIQ-TO#05-RTI-ENG-AOSEPP-09-20-2021) to support PCORI’s work. Questions or comments may be sent to PCORI at [email protected].
Financial disclosure
This work was funded and supported by PCORI (PCORI contract number: IDIQ-TO#05-RTI-ENG-AOSEPP-09-20-2021). The authors have received no other financial and/or material support for this research or the creation of this work apart from that disclosed.
Competing interests disclosure
The authors have no competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
Writing disclosure
Editorial support for this manuscript was supported by Marceline Murawski and Michelle Bogus from RTI International and was funded by the PCORI contract.
Data sharing statement
This manuscript uses published clinical trial estimates and the authors do not access or conduct analyses on original data from the ELEKT-D clinical trial.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
National Institute of Mental Health (NIMH). Depression. Accessed: 10 July 2024: https://www.nimh.nih.gov/health/topics/depression
2.
Zhdanava M, Pilon D, Ghelerter I et al. The prevalence and national burden of treatment-resistant depression and major depressive disorder in the United States. J. Clin. Psychiatry 82(2), 20m13699 (2021).
3.
Sussman M, O'Sullivan AK, Shah A, Olfson M, Menzin J. Economic burden of treatment-resistant depression on the U.S. health care system. J. Manag. Care Spec. Pharm. 25(7), 823–835 (2019).
4.
Taipale H, Reutfors J, Tanskanen A et al. Risk and risk factors for disability pension among patients with treatment resistant depression- a matched cohort study. BMC Psychiatry 20(1), 232 (2020).
5.
Lundberg J, Cars T, Lööv SÅ et al. Association of treatment-resistant depression with patient outcomes and health care resource utilization in a population-wide study. JAMA Psychiatry 80(2), 167–175 (2023).
6.
Greenberg PE, Fournier AA, Sisitsky T et al. The economic burden of adults with major depressive disorder in the United States (2010 and 2018). Pharmacoeconomics 39(6), 653–665 (2021).
7.
Anand A, Mathew SJ, Sanacora G et al. Ketamine versus ECT for nonpsychotic treatment-resistant major depression. N. Engl. J. Med. 388(25), 2315–2325 (2023).
•• Details the process and results of the ELEKT-D trial, the largest comparative effectiveness trial to date in the US, demonstrated that intravenous ketamine was noninferior to electroconvulsive therapy for nonpsychotic treatment-resistant depression.
8.
Mayo Clinic. Electroconvulsive therapy (ECT). Available from: https://www.mayoclinic.org/tests-procedures/electroconvulsive-therapy/about/pac-20393894
9.
Espinoza RT, Kellner CH. Electroconvulsive therapy. N. Engl. J. Med. 386(7), 667–672 (2022).
10.
Berman RM, Cappiello A, Anand A et al. Antidepressant effects of ketamine in depressed patients. Biol. Psychiatry 47(4), 351–354 (2000).
11.
Allaire B, Skinner R, King G, Honeycutt A, Esposito D. An economic evaluation of reducing colorectal cancer surveillance intensity. J. Comp. Eff. Res. 11(2), 99–107 (2022).
12.
Boyer N, Skinner R, Breck A. An impact evaluation of an education bundle for patients at risk of developing venous thromboembolism. J. Comp. Eff. Res. 11(8), 563–574 (2022).
13.
Honeycutt A, Breck A, Bass S, Esposito D. Impact analysis of expanding anti-TNF therapy for Crohn's disease. J. Comp. Eff. Res. 11(2), 79–88 (2022).
14.
Skinner R, Breck A, Esposito D. An economic evaluation of teledermatology care delivery for chronic skin diseases. J. Comp. Eff. Res. 11(2), 67–77 (2022).
15.
Luccarelli J. Personal communication. (2024).
16.
National Institute of Mental Health. Major depression. Accessed: 10 May 2024: https://www.nimh.nih.gov/health/statistics/major-depression
17.
Ross EL, Zivin K, Maixner DF. Cost-effectiveness of electroconvulsive therapy vs pharmacotherapy/psychotherapy for treatment-resistant depression in the United States. JAMA Psychiatry 75(7), 713–722 (2018).
18.
Agency for Healthcare Research and Quality (AHRQ). Medical Expenditure Panel Survey (MEPS) (2016–2019). (Accessed: 27 September 2024). https://meps.ahrq.gov/mepsweb/?_gl=1*1fxc4u*_ga*OTIyODgyNjE3LjE3Mjc0NDk2NDc
19.
Pilon D, Joshi K, Sheehan JJ et al. Burden of treatment-resistant depression in Medicare: a retrospective claims database analysis. PLOS One. 14(10), e0223255 (2019).
20.
Bureau of Labor Statistics (BLS). Employer costs for employee compensation – June 2024 USDL-24-1863. Bureau of Labor Statistics, Washington, DC, USA (10 September 2024).
21.
AARP and National Alliance for Caregiving. Caregiving in the United States. 2020. (Accessed: 27 September 2024). https://www.aarp.org/pri/topics/ltss/family-caregiving/caregiving-in-the-united-states/
22.
Frank RG, Glied SA. NB19-05: Changing Labor Markets and Mental Illness: Impacts on Work and Disability (2019). National Bureau of Economic Research, Cambridge, MA, USA, Available from: https://www.nber.org/programs-projects/projects-and-centers/retirement-and-disability-research-center/7569-nb19-05-changing-labor-markets-and-mental-illness-impacts-work-and-disability
23.
Nordenskjöld A, von Knorring L, Ljung T, Carlborg A, Brus O, Engström I. Continuation electroconvulsive therapy with pharmacotherapy versus pharmacotherapy alone for prevention of relapse of depression: a randomized controlled trial. J. ECT 29(2), 86–92 (2013).
24.
Daly EJ, Trivedi MH, Janik A et al. Efficacy of esketamine nasal spray plus oral antidepressant treatment for relapse prevention in patients with treatment-resistant depression: a randomized clinical trial. JAMA Psychiatry 76(9), 893–903 (2019).
25.
Brendle M, Ahuja S, Valle MD et al. Safety and effectiveness of intranasal esketamine for treatment-resistant depression: a real-world retrospective study. J. Comp. Eff. Res. 11(18), 1323–1336 (2022).
26.
Mathew SJ, Jha MK, Anand A. Choosing between ketamine and electroconvulsive therapy for outpatients with treatment-resistant depression-advantage ketamine? JAMA Psychiatry 80(12), 1187–1188 (2023).
•• This viewpoint article from the ELEKT-D authors discussed the clinical implication of their study findings in further detail.
27.
Osmind. Ketamine Billing Code Guide. (Accessed: 20 September 2024). https://www.osmind.org/knowledge-article/ketamine-billing-code-guide
28.
Chrenek C, Duong B, Khullar A, McRee C, Thomas R, Swainson J. Use of ketamine for treatment resistant depression: updated review of literature and practical applications to a community ketamine program in Edmonton, Alberta, Canada. Front. Psychiatry 14, 1283733 (2024).
Information & Authors
Information
Published In
Copyright
© 2025 Research Triangle Institute, dba RTI International. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 12 December 2024
Accepted: 23 April 2025
Published online: 22 May 2025
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Impact analysis of expanded access to ketamine for treatment-resistant depression. (2025) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2024-0233
Export citation
Select the citation format you wish to export for this article or chapter.