Patient characteristics, healthcare resource utilization and costs across treatment lines in diffuse large B-cell lymphoma – a German claims data study
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Given the limited availability of real world diffuse large B-cell lymphoma (DLBCL) data in Germany, we assessed the baseline characteristics, treatments, clinical complications, healthcare resource utilization and costs of DLBCL across treatment lines using German claims data. Materials & methods: In a retrospective cohort study using claims data from a German sickness fund (AOK PLUS), we identified patients with an incident DLBCL diagnosis between 2012 and 2022. Using an algorithm based on German treatment guidelines, patients were stratified into first (1L), second (2L) and third line (3L) treatment. We then descriptively analyzed baseline characteristics, treatments, clinical complications, healthcare resource utilization and costs. Results: A total of 2423 patients with DLBCL and 1L treatment were included in the study (49.1% female; mean age: 69.7 years; mean CCI: 7.0; median follow-up: 29.3 months). A total of 1209 (49.7%) and 505 (20.8%) patients progressed to 2L and 3L, respectively. A total of 209 patients received a stem cell transplant (SCT; mean age: 56.1 years); 37 received a chimeric antigen receptor T-cell therapy (CAR-T; mean age: 60.8 years). Most patients had at least one DLBCL related hospitalization during follow-up (1L: 79.2%; 2L: 60.0%; 3L: 71.9%; mean length of stay [days/patient year]: 1L: 15.2; 2L: 6.4; 3L: 14.2), with corresponding hospitalization costs of 12,777€ (1L), 5993€ (2L) and 17,408€ (3L) per patient year. Clinical complications were common, particularly in 3L, including neutropenia (1L: 31.9%; 2L: 27.0%; 3L: 46.9%), pneumonia (1L: 19.6%; 2L: 16.8%; 3L: 30.3%), anemia (1L: 17.8%; 2L: 18.7%; 3L: 35.2%), thrombocytopenia (1L: 17.3%; 2L: 21.8%; 3L: 45.1%) and sepsis (1L: 14.6%; 2L: 13.0%; 3L: 23.2%). Conclusion: The high proportion of patients with second or later-line treatment (indicating a relapse or refractory disease), the low number of SCTs together with many clinical complications and healthcare resource use underscore the need for novel effective and well-tolerated DLBCL treatment options.
Plain language summary
What is this article about?
Diffuse large B-cell lymphoma (DLBCL) is a fast-growing cancer that is usually first treated with a combination of chemotherapy and immunotherapy called R-CHOP. While R-CHOP helps most patients, for some patients the cancer returns or they do not respond to the treatment.
This study tries to better understand how DLBCL is treated in the real world, looking at treatments, complications, and the use of healthcare services among DLBCL patients. We used data from a large German health insurance fund, covering 3.5 million people from 2010 to 2022. For the study, we included patients diagnosed with DLBCL for the first time between 2012 and 2022 and followed them until 2022 or until they died. Patients were tracked through different lines of therapy.
What were the results?
We identified 2432 patients with first-line treatment, with an average age of 69.7 years. Nearly half of these patients needed further treatment lines. Most patients (about 85% in first-line treatment) received chemotherapy combined with rituximab. A small number of typically younger patients received advanced therapies like stem cell transplants or so-called chimeric antigen receptor T-cell therapy. Hospitalizations among patients were common, with around 6 to 15 hospital days per year and costs ranging from around €6000 to €17,000 per year, depending on the treatment line. Common complications included neutropenia, pneumonia, anemia, thrombocytopenia and sepsis. Blood and platelet transfusions were also common, especially in later treatment lines.
What do the results mean?
With nearly half of the patients having more than one line of treatment, our study indicates that many patients experience relapses or do not respond well to treatment initially. We also observed a high number of hospitalizations and complications, showing the negative impact of DLBCL despite current treatments. This highlights the need for new, effective and better-tolerated DLBCL treatments.
Accounting for about 25% of all new non-Hodgkin Lymphomas (NHLs), diffuse large B-cell lymphoma (DLBCL) is the most common type of NHL [1]. At incident diagnosis, the median age is 67 years in the US and up to 75 years in Europe, thus mainly affecting older patients who often also have a high comorbidity burden [2–7]. DLBCL is an aggressive cancer, requiring urgent treatment [1]. Common first-line (1L) therapy with the chemoimmunotherapy R-CHOP, consisting of rituximab, cyclophosphamide, doxorubicin, vincristine and prednisone, is effective in 50–70% of patients, while 30–50% of patients experience refractory or relapsing (r/r) disease [5]. Treatment options in second line (2L) include salvage chemotherapy followed by stem cell transplantation (SCT), or chimeric antigen receptor T-cell therapy (CAR-T), the eligibility for which depends on patients’ individual fitness and health status. Moreover, not all patients eligible for SCT or CAR-T may receive those interventions given potential access barriers. In addition to the above treatments, several newer treatment combinations such as polatuzumab plus BR (bendamustine and rituximab) or tafasitamab plus lenalidomide have been approved in recent years [8]. While previous research reported epidemiology, treatment patterns and survival for patients with DLBCL using German claims data [7], real-world data on the burden of r/r DLBCL symptoms and healthcare use are limited, particularly for Europe. This study aims at providing real-world evidence (RWE) on patient characteristics, treatments, clinical complications, healthcare resource utilization (HCRU) and costs in DLBCL based on German claims data.
Materials & methods
This retrospective non-interventional cohort study used German claims data from the sickness fund AOK PLUS, covering approximately 3.5 million patients across the central eastern German states of Saxony and Thuringia. Collected for reimbursement purposes, the data include information on patient demographics, in- and outpatient diagnoses and procedures, outpatient and partly inpatient medications as well as HCRU and costs from 2010 to 2022. We identified incident DLBCL patients via diagnosis codes (ICD-10 GM: C83.3) from the inpatient (one discharge diagnosis) or outpatient sector (two confirmed diagnosis codes within two consecutive quarters from a hematologist, oncologist or radiologist) between 2012 and 2022. To ensure that only newly diagnosed patients were counted as incident cases, we applied a 2-year ‘wash-out’ period prior to the index date (the date of the first recorded DLBCL diagnosis), during which no DLBCL diagnosis codes were allowed. For example, a patient with a DLBCL diagnosis in 2012 was counted as incident if no prior DLBCL diagnosis in 2010 and 2011 was observed. Patients were followed up from index date until the end of data collection or death. Since treatment line information is not directly recorded in German claims data, we used the previously published algorithm by Pacis et al. to identify the first three treatment lines based on prescription patterns and hospital procedure codes [7]. DLBCL treatments starting within 45 days of index date were classified as 1L (see Supplementary Table 1 for a full list of treatments and codes considered for this study). Treatments that were initiated after discontinuation of the previous line or the introduction of new agents more than 30 days after treatment line start were classified as second (2L) or third line (3L) treatment. Discontinuation or end of treatment line was defined as any gap of 60 days of all drugs of the respective treatment line. To identify the gap, a runout date was determined. For oral drugs, the runout date was defined as the administration date plus the days of supply based on defined daily doses. In the outpatient sector, the defined daily doses are derived from information of package size and dosage of the administered pharmaceutical product and hence complete. Periods of hospitalization, during which drug supply from the hospital was assumed, and stock piling were considered. For medications administered otherwise, the runout date was defined as date of administration plus 60 days. When entering the next treatment line group, patients were censored in the previous group and outcomes were reported for the duration of each line. The treatment line algorithm also considered prescription and procedure codes for identifying SCT or CAR-T therapy (Supplementary Table 1). While we used ATC codes to identify outpatient treatments, we used OPS codes to identify inpatient treatments (Supplementary Table 1). For some treatment options, no specific OPS codes are available. To identify inpatient treatment in these cases, generic OPS codes for chemotherapy were considered. Patients without any of the predefined treatment codes were excluded from further analysis.
We determined baseline characteristics such as age, gender, and the Charlson Comorbidity Index (CCI) at index date and calculated the incidence rate (IR) of DLBCL. We assessed HCRU with regards to outpatient general practitioner (GP) and specialist (hematologist, oncologist or radiologist) visits as well as all-cause and DLBCL related hospitalizations including length of stay (LOS). We also assessed treatments, clinical complications and the number of patients with blood or platelet transfusions. For the cost analyses, we report costs for outpatient visits, prescriptions, hospitalizations (all-cause and DLBCL related) and others (medical aids, remedies, inpatient rehabilitation costs).
All variables were analyzed descriptively, and the absolute number of patients or days, proportions, means and standard deviation or medians were reported. Epidemiological estimates were reported per 100,000 persons per year, while HCRU and costs were reported per patient-year (PY) to account for variable follow-up duration across patients.
Results
From 2012 to 2022, we identified 3360 patients with a diagnosis record of incident DLBCL, leading to an IR of 8.7/100,000. Of these, 2432 initiated 1L treatment within 45 days of diagnosis (IR 6.3/100,000). A total of 188 patients received treatment after more than 45 days after index diagnosis and were not included in the treatment line subgroups. A total of 740 DLBCL patients without any study-relevant treatment (mean age: 75.9 years) were excluded from analyses of treatments, clinical complications, HCRU and costs (Figure 1).
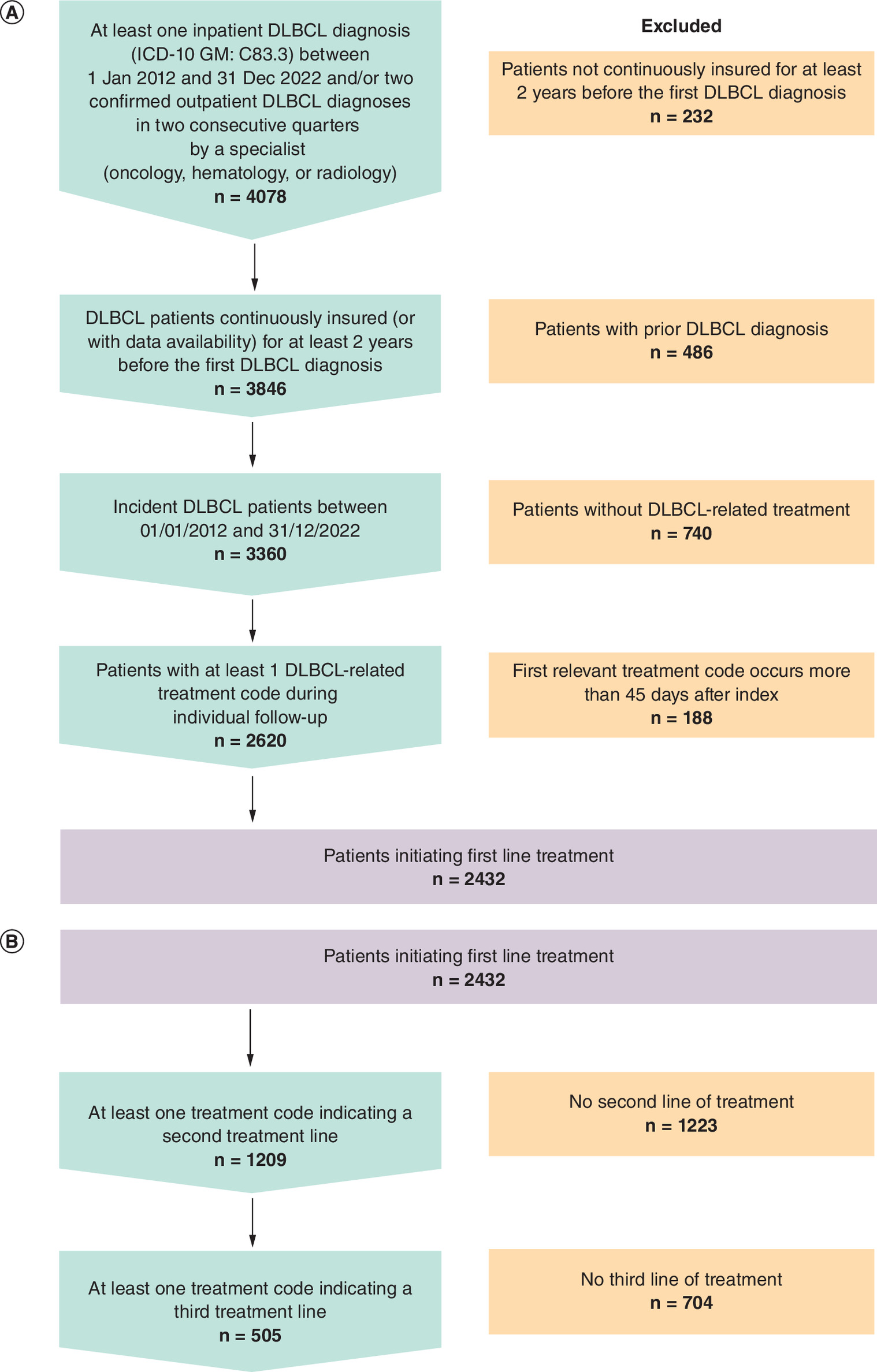
Figure 1. Attrition charts for incident diffuse large B-cell lymphoma patients: Overall and by treatment line group.
(A) Attrition chart for incident DLBCL patients. (B) Attrition chart for stratification of incident DLBCL patients into treatment line groups.
DLBCL: Diffuse large B-cell lymphoma.
A total of 1209 (49.7%) of 1L patients initiated a 2L treatment, and 505 (20.8%) received 3L treatment. Patients were followed up for a median of 29.3 months. Table 1 shows baseline characteristics of patients. Patients initiating later treatment lines had a slightly lower mean age at treatment line start compared with patients initiating earlier lines (1L: 69.7 years; 2L: 68.3 years; 3L: 67.5 years). The comorbidity burden of patients was high, with mean CCIs of 7.0 (1L), 6.8 (2L) and 7.9 (3L). Among the total 37 patients receiving CAR-T therapy, the mean age was 60.8 years and the mean CCI was 10.1.
| 1L patients | 2L patients | 3L patients | CAR-T patients† | |
|---|---|---|---|---|
| Total, n | 2432 | 1209 | 505 | 37 |
| Gender, n (%) | ||||
| Female | 1194 (49.1%) | 589 (48.7%) | 233 (46.1%) | 14 (38%) |
| Male | 1238 (50.9%) | 620 (51.3%) | 272 (53.9%) | 23 (62%) |
| Age (in years) | ||||
| Mean (SD) | 69.7 (13.9) | 68.3 (13.8) | 67.5 (13.3) | 60.8 (13.7) |
| Charlson comorbidity index, points | ||||
| Mean (SD) | 7.0 (4.0) | 6.8 (3.9) | 7.9 (4.0) | 10.1 (4.1) |
†
All CAR-T patients irrespective of inclusion into treatment line algorithm.
1L: First line; 2L: Second line; 3L: Third line; CAR-T: Chimeric antigen receptor T-cell therapy; SD: Standard deviation.
Table 2 shows treatments, clinical complications and blood and platelet transfusions during the follow-up per treatment line. Across all treatment lines, most patients were treated with rituximab-containing chemotherapies (1L: 84.7%; 2L: 81.2%; 3L: 65.9%). Chemotherapy without any additional monoclonal antibody or targeted therapy was administered to 9.1% (1L), 6.5% (2L), and 10.9% (3L) of patients. Of all patients with DLBCL treatment (n = 2620), regardless of treatment line, 209 patients (8.0%) received an SCT (mean age: 56.1 years) and 37 patients (1.4%) received a CAR-T therapy (mean age: 60.8 years) at any time during follow-up. Of the clinical complications investigated, neutropenia was most commonly reported, affecting 31.9% (1L), 27.0% (2L) and 46.9% (3L) of patients, followed by pneumonia and anemia (Table 2). Blood transfusions and platelet transfusions were common, with 39.1% (1L), 36.4% (2L) and 58.4% (3L) of patients receiving the former, while 13.2% (1L), 17.0% (2L) and 40.2% (3L) of patients received the latter.
| 1L patients | 2L patients | 3L patients | |
|---|---|---|---|
| Treatment patterns† | |||
| Chemotherapy with rituximab, n (%) | 2059 (84.7%) | 982 (81.2%) | 333 (65.9%) |
| Chemotherapy without additional monoclonal antibody or targeted therapy, n (%) | 221 (9.1%) | 78 (6.5%) | 55 (10.9%) |
| Clinical complications | |||
| Neutropenia, n (%) | 776 (31.9) | 327 (27.0) | 237 (46.9) |
| Pneumonia, n (%) | 477 (19.6) | 203 (16.8) | 153 (30.3) |
| Anemia, n (%) | 434 (17.8) | 226 (18.7) | 178 (35.2) |
| Thrombocytopenia, n (%) | 421 (17.3) | 264 (21.8) | 228 (45.1) |
| Sepsis, n (%) | 354 (14.6) | 157 (13.0) | 117 (23.2) |
| Nausea, n (%) | 153 (6.3) | 71 (5.9) | 35 (6.9) |
| Fatigue, n (%) | 74 (3.0) | 35 (2.9) | 34 (6.7) |
| Skin lesions, n (%) | 67 (2.8) | 28 (2.3) | 21 (4.2) |
| Pyrexia, n (%) | 23 (0.9) | 6 (0.5) | 14 (2.8) |
| CNS infections, n (%) | 24 (1.0) | 7 (0.6) | 3 (0.6) |
| Cytokine release syndrome, n (%) | 5 (0.2) | 3 (0.2) | 17 (3.4) |
| EBV infections, n (%) | 11 (0.5) | 3 (0.2) | 4 (0.8) |
| Osteomyelitis, n (%) | 8 (0.3) | 5 (0.4) | 2 (0.4) |
| Infections after transfusions, n (%) | 5 (0.2) | 3 (0.2) | 1 (0.2) |
| Meningitis, n (%) | 0 (0) | 2 (0.2) | 1 (0.2) |
| Diarrhoea, n (%) | 3 (0.1) | 2 (0.2) | 0 (0) |
| Hepatitis C infections, n (%) | 2 (0.1) | 0 (0) | 0 (0) |
| HTLV-1 infections, n (%) | 0 (0) | 0 (0) | 0 (0) |
| Blood and platelet transfusions | |||
| Blood transfusions, n (%) | 952 (39.1) | 440 (36.4) | 295 (58.4) |
| Platelet transfusions, n (%) | 322 (13.2) | 206 (17.0) | 203 (40.2) |
†
Information on individual inpatient medications is not fully available in German claims data as some medications are recorded via generic chemotherapy procedure codes. Exact regimens are therefore not reported.
1L: First line; 2L: Second line; 3L: Third line; EBV: Epstein–Barr virus; HTLV-1: Human T-lymphotropic virus 1.
Table 3 shows HCRU and costs of patients by treatment line. The number of outpatient visits per PY was highest in 1L (GP: 11.9; specialist: 4.2) and decreased in 2L (GP: 10.3; specialist: 3.8) and 3L (GP: 8.9; specialist: 4.1). Most patients were hospitalized for DLBCL at least once during follow-up (1L: 79.2%; 2L: 60.0%; 3L: 71.9%) with the highest mean LOS ranging from 6.4 days/PY to 15.2 days/PY (Table 3). Hospitalization costs (all-cause) per PY ranged from €10,909.26 to €27,379.63 and DLBCL related hospitalization ranged from €5993.49 to €17,407.56 per PY. Compared with hospitalization costs, costs for outpatient treatment (GP and specialist visits) were low and decreased across treatment lines (Table 3). Conversely, prescription costs increased across treatment lines and were particularly high in 3L (1L: €6374.07; 2L: €6574.87; 3L: 10,356.79€)
| 1L patients | 2L patients | 3L patients | |
|---|---|---|---|
| Total, n | 2432 | 1209 | 505 |
| Mean time on treatment line in days (SD) | 99.9 (113.6) | 112.1 (119.4) | 77.8 (110.5) |
| HCRU | |||
| All-cause GP visits (per PY) | 11.9 | 10.3 | 8.9 |
| All-cause outpatient specialist visits (per PY) | 4.2 | 3.8 | 4.1 |
| All-cause inpatient hospitalizations | |||
| n patients (%) | 2292 (94.2) | 1070 (88.5) | 490 (97.0) |
| Mean length of stay (days/PY) | 24.6 | 13.6 | 25.6 |
| DLBCL-related inpatient hospitalizations | |||
| Patients, n (%) | 1925 (79.2) | 726 (60.0) | 363 (71.9) |
| Mean length of stay (days/PY) | 15.2 | 6.4 | 14.2 |
| Costs (in EUR per PY) | |||
| All-cause inpatient hospitalizations | 18,823.35 | 10,909.26 | 27,379.63 |
| DLBCL-related inpatient hospitalizations | 12,777.44 | 5993.49 | 17,407.56 |
| GP visits | 277.28 | 248.08 | 204.45 |
| Outpatient specialist visits | 248.77 | 239.35 | 227.50 |
| Outpatient prescriptions | 6374.07 | 6574.87 | 10,356.79 |
| Other costs (includes medical aids, remedies, and inpatient rehabilitation) | 1672.44 | 1461.86 | 1743.12 |
| Total direct costs | 27,395.91 | 19,433.42 | 39,911.49 |
DLBCL: Diffuse large B-cell lymphoma; GP: General practitioner; HCRU: Health care resource utilization; PY: Per year; SD: Standard deviation.
Discussion
Evaluating real-world data from Germany, we generally found that patients with DLBCL had a high burden of disease across treatment lines. About half of the patients initiated a second line treatment, consistent with the literature that up to 50% of patients relapse following 1L or have refractory disease [2]. Notably, 22.0% of patients initially identified via DLBCL diagnosis codes had no claims record for DLBCL treatment, potentially indicating that these patients received no DLBCL related medical treatment during follow-up. A similar observation was reported by Borchmann et al. finding that 20.2% of patients did not receive any medical treatment. Likewise, a Belgian registry study reports that 15.5% of DLBCL patients received no treatment [4,9], and three US claims data and electronic health records studies found that only 54.0–60.1% of DLBCL patients received predefined treatments [5,10,11]. Possible explanations include the revision of initial diagnoses, an older age which might disqualify patients for certain treatment options, the presence of comorbidities, a short individual follow-up ending before treatment start, or radiation being chosen over systemic medical treatment [4,10,12]. Further, patients might be included into clinical trials as recommended by the German medical guideline and thus, their treatments would not be captured within claims data [8,12]. Given these diverse rationales for patients not receiving treatment, we decided to exclude these patients from analysis as they might potentially dilute the outcome results.
Across all treatment lines, the majority of patients received a chemotherapy in combination with rituximab, a finding consistent with treatment guidances [13,14] and real-world studies from England, Belgium and the USA [3–5,10,15,16]. Considering the high proportion of patients who relapse or are refractory to 1L treatment and the high number of patients treated with rituximab, our study indicates a need for new and more effective therapies.
The relatively low number of patients treated with an SCT is consistent with numbers published in the annual report of the German SCT centers (in 2022, a total of 546 DLBCL patients in Germany received autologous or allogeneic SCTs) [17]. Similarly, two US claims data studies found that, depending on treatment line, 3.1–9.6% of DLBCL patients received an SCT during follow-up [5,11]. The low number of SCTs is likely related to the relatively high age and comorbidity burden of our patient population, resulting in most patients not being eligible for the intensive treatment component of SCT. Additionally, some of the 2L patients might have received salvage R-chemo in preparation to proceed to SCT but did not respond adequately and thus switched to 3L treatment instead. The development of new pharmacological therapies could help to provide adequate treatment options to these older patients. The very low usage of CAR-T in our study could possibly be explained by the rather high age of our study population as well, as the mean age of CAR-T patients was 6.7–8.9 years below the mean age of 1–3L patients. Additionally, during most of the study period CAR-T therapy was only recommended for r/r disease following to two previous therapy lines [18]. Also, patients eligible for CAR-T therapy might have been selected for clinical trials and thus, their treatment would not have been collected in claims data [8]. Due to the high costs associated with CAR-T treatment, incomplete coding from medical staff seems unlikely. Bispecific monoclonal antibodies such as glofitamab or epcoritamab were approved for DLBCL treatment in Germany in 2023, thus missing the study period [19]. We observed a significant number of clinical complications during follow-up, further underlining the high disease burden of patients and the toxicity profile of existing DLBCL therapies. As these clinical complications were assessed based on recorded diagnosis codes, these events might be underestimated, and actual complication numbers may be even higher. Hospitalization and total costs were lowest for 2L patients and highest for 3L patients. While Borchmann et al. and Moertl et al. reported decreasing costs from 1L to 3L, observed in data from a different German sickness fund and from one tertiary teaching hospital, respectively, Gatwood et al. found that in the US, costs increased with increasing treatment lines. Tsutsué et al. reported almost equal costs for 2L and 3L based on Japanese claims data [9,20–22]. Note that costs in the US and Japan were generally much higher compared with Germany, and comparison is difficult due to different health systems [5,9,11,22]. Congruent with the low hospitalization costs in 2L in our study, 2L patients also had the shortest mean LOS and the lowest proportions of patients admitted to a hospital during follow-up. At the same time, 2L patients had slightly higher outpatient prescriptions costs than 1L patients. Considering additionally that most of the clinical complications we looked at were least frequent in 2L patients, 2L treatments might partly have been shifted from the inpatient to the outpatient sector toward less toxic options. However, this interpretation is speculative and would need to be explored more closely in future research.
Our study has several limitations. First, claims data are not primarily collected for research purposes leading to possibly missing information or coding imperfections. However, coding quality is generally considered to be high in German claims databases, and they are frequently used for epidemiological research. Yet, clinical variables of potential interest, such as Eastern Cooperative Oncology Group status, DLBCL subtype or Ann Arbor stage, are not available in claims data, thus limiting the detailed characterization of patients. Second, our study used data from one sickness fund, AOK PLUS, covering patients in central eastern parts of Germany, which could have resulted in some regional bias. However, given the uniform healthcare regulations in Germany, treatment of patients in AOK PLUS is not expected to differ from patients in other parts of Germany. Third, since neither treatment line nor information on r/r disease are directly available in German claims data, we used a previously developed algorithm based on treatment recommendations in Germany [8] to determine treatment lines and assumed patients proceeding to the next treatment line suffered from r/r DLBCL [7]. This could have resulted in some degree of misclassification. However, the number of r/r patients we found is consistent with another German claims data study and findings from clinical studies [12,23]. Fourth, while our data captured treatment classes, data on individual treatment is not accurately captured and therefore not reported in our study. At last, the study period ends in 2022 and thus does not capture more recent changes in the treatment landscape (for example, the label expansion for the CAR-T treatment axicabtagene-ciloleucel from 3L to 2L in Germany was only introduced a few weeks prior to the end of the study period). Future RWE studies utilizing more recent data can help to provide further insights about the impact of novel treatment options on current clinical practice. In addition, an analysis of treatment switching, disease progression and treatment discontinuation could further enhance understanding of real-world treatment patterns and inform strategies for improving patient care and outcomes.
In conclusion, the high proportion of patients progressing to second and later treatment lines, and the high number of hospitalizations, healthcare costs, clinical complications and related procedures indicate a high disease and treatment burden among patients with DLBCL. This underscores the unmet need for novel effective and well-tolerated treatment options for DLBCL patients.
Summary points
•
Diffuse large B-cell lymphoma (DLBCL) is the most frequent acute non-Hodgkin Lymphoma mostly affecting older patients who are often comorbid.
•
Being an aggressive cancer, DLBCL requires urgent treatment; while this is effective in 50–70% of patients, 30–50% of the patients need second or later line treatments.
•
In this retrospective observational cohort study, we used German claims data covering the years 2010–2022.
•
Of 3360 incident DLBCL patients identified, we found 2432 to initiate treatment. About half of these patients proceeded to second and 20% to third line treatment.
•
Rituximab containing chemotherapies were the most common treatment options across all treatment lines.
•
The most common clinical complications affected up to 47% of patients and included neutropenia, pneumonia, anemia, thrombocytopenia and sepsis.
•
Our findings indicate a high burden of disease and treatment, underscoring the need for novel effective and also well-tolerated treatments.
Author contributions
K Greth, M Lehne, M Ghiani, M Gokhale and A Russell were responsible for study design; M Gokhale, A Russell and W Jiang were responsible for study conception; A Mevius was responsible for acquisition of data; K Greth and M Lehne were responsible for data analysis, and drafting and revision of the manuscript; M Gokhale, A Mevius, A Russell, W Jiang and M Ghiani critically reviewed the manuscript; all authors provided final approval of the version submitted and agreed to be accountable for all aspects of the work.
Financial disclosure
The development of this publication including the underlying study was supported financially by Pfizer Inc. including the work of Cytel Inc.
Competing interests disclosure
K Greth, M Lehne and M Ghiani are employees of Cytel Inc. a research consultancy receiving funding from various pharmaceutical companies. A Mevius is employee of IPAM e.V., a scientific institute receiving financial compensation for its studies. W Jiang, M Gokhale and A Russell are employees of Pfizer Inc. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing disclosure
No funded writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
Due to the noninterventional, retrospective study design using anonymized data not focusing on any particular pharmacologic intervention, and in accordance with local laws and policies, patients’ informed consent was not required for this study. The study was approved by the responsible authority, the data owner AOK PLUS.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary materials.docx)
- Download
- 23.54 KB
References
Papers of special note have been highlighted as: • of interest
1.
Liu Y, Barta SK. Diffuse large B-cell lymphoma: 2019 update on diagnosis, risk stratification, and treatment. Am. J. Hematol. 94(5), 604–616 (2019).
2.
Kesireddy M, Lunning M. Relapsed or refractory diffuse large B-cell lymphoma: “dazed and confused”. Oncology (Williston Park) 36(6), 366–375 (2022).
3.
Hounsome L, Eyre TA, Ireland R et al. Diffuse large B cell lymphoma (DLBCL) in patients older than 65 years: analysis of 3 year real world data of practice patterns and outcomes in England. Br. J. Cancer 126(1), 134–143 (2022).
• This real world data study shows the influence of expedite treatment on superior survival outcomes for diffuse large B-cell lymphoma (DLBCL) patients in England.
4.
Daneels W, Rosskamp M, Macq G et al. Real-world estimation of first- and second-line treatments for diffuse large B-cell lymphoma using health insurance data: a Belgian population-based study. Front. Oncol. 12, 824704 (2022).
5.
Yang X, Laliberté F, Germain G et al. Real-world characteristics, treatment patterns, health care resource use, and costs of patients with diffuse large B-cell lymphoma in the U.S. Oncologist 26(5), e817–e826 (2021).
6.
SEER cancer stat facts: NHL – diffuse large B-cell lymphoma (DLBCL). National Cancer Institute, MD, USA. Available from: https://seer.cancer.gov/statfacts/html/dlbcl.html
7.
Pacis S, Bolzani A, Heuck A et al. Epidemiology and real-world treatment of incident diffuse large B-cell lymphoma (DLBCL): a German claims data analysis. Oncol. Ther. 12(2), 293–309 (2024).
• By describing the real world treatment landscape in DLBCL based on German claims data, this study highlights the challenging treatment of transplant-ineligble patients.
8.
Leitlinienprogramm Onkologie (Deutsche Krebsgesellschaft DK, AWMF). Diagnostik, Therapie und Nachsorge für erwachsene Patient*innen mit einem diffusen großzelligen B-Zell-Lymphom und verwandten Entitäten, Langversion 1.0. (2022).
9.
Borchmann P, Heger JM, Mahlich J et al. Healthcare resource utilization and associated costs of German patients with diffuse large B-cell lymphoma: a retrospective health claims data analysis. Oncol. Ther. 11(1), 65–81 (2023).
10.
Morrison VA, Shou Y, Bell JA et al. Evaluation of treatment patterns and survival among patients with diffuse large B-cell lymphoma in the USA. Future Oncol. 15(9), 1021–1034 (2019).
11.
Ren J, Asche CV, Shou Y, Galaznik A. Economic burden and treatment patterns for patients with diffuse large B-cell lymphoma and follicular lymphoma in the USA. J. Comp. Eff. Res. 8(6), 393–402 (2019).
12.
Borchmann P, Heger JM, Mahlich J et al. Survival outcomes of patients newly diagnosed with diffuse large B-cell lymphoma: real-world evidence from a German claims database. J. Cancer Res. Clin. Oncol. 149(10), 7091–7101 (2023).
13.
Dührsen U, Fridrik MA, Klapper W, Schmitz N. Diffuses großzelliges B-Zell-Lymphom. Berlin, Germany (2018).
14.
Dührsen U, Fridrik MA, Schmitz N. Diffuses großzelliges B-Zell-Lymphom. Berlin, Germany (2014).
15.
Shaw J, Harvey C, Richards C, Kim C. Temporal trends in treatment and survival of older adult diffuse large B-Cell lymphoma patients in the SEER-Medicare linked database. Leuk. Lymphoma 60(13), 3235–3243 (2019).
16.
Sineshaw HM, Zettler CM, Prescott J et al. Real-world patient characteristics, treatment patterns, and treatment outcomes of patients with diffuse large B-cell lymphoma by line of therapy. Cancer Med. 13(7), e7173 (2024).
• Finding an poorer overall survival for r/r DLBCL patients, this study based on US claims data underlines the need for effective treatment options in second and later line.
17.
DRST Deutsches Register für Stammzelltransplantationen e.V. Jahresbericht 2022. Ulm, Germany (2022).
18.
Georg Lenz BC, Bertram Glaß, Felix Keil et al. Diffuses großzelliges B-Zell-Lymphom. Onkopedia Leitlinie: DGHO, OeGHO, SGHSSH, SSMO (2021).
19.
Pharmazeutische Zeitung. Arzneistoffe: Avoxa - Mediengruppe Deutscher Apotheker GmbH (2024). Available from: https://www.pharmazeutische-zeitung.de/arzneistoff-wirkstoff/
20.
Moertl B, Dreyling M, Schmidt C et al. Inpatient treatment of relapsed/refractory diffuse large B-cell lymphoma (r/r DLBCL): a health economic perspective. Clin. Lymphoma Myeloma Leuk. 22(7), 474–482 (2022).
21.
Gatwood J, Masaquel A, Fox D et al. Real-world total cost of care by line of therapy in relapsed/refractory diffuse large B-cell lymphoma. J. Med. Econ. 27(1), 738–745 (2024).
• This claims data study on DLBCL patients from the US showed increasing total healthcare costs for patients in second or later line, urging for further improvements in first-line treatment.
22.
Tsutsué S, Makita S, Yi J, Crawford B. Cost drivers associated with diffuse large B-cell lymphoma (DLBCL) in Japan: a structural equation model (SEM) analysis. PLoS ONE 17(5), e0269169 (2022).
23.
Coiffier B, Thieblemont C, Van Den Neste E et al. Long-term outcome of patients in the LNH-98.5 trial, the first randomized study comparing rituximab-CHOP to standard CHOP chemotherapy in DLBCL patients: a study by the Groupe d'Etudes des Lymphomes de l'Adulte. Blood 116(12), 2040–2045 (2010).
Information & Authors
Information
Published In
Copyright
© 2025 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 14 November 2024
Accepted: 3 July 2025
Published online: 13 August 2025
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Patient characteristics, healthcare resource utilization and costs across treatment lines in diffuse large B-cell lymphoma – a German claims data study. (2025) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2024-0218
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Mugdha Gokhale, Philip K. Chan, Wei Jiang, Rebecca Levin, Joseph C. Cappelleri, Virginia Noxon-Wood, Anthony Yu, Ilya Okunev, Healthcare resource utilization, costs, and survival among Medicare beneficiaries with relapsed or refractory DLBCL receiving second-line therapy: a real-world evidence study, Leukemia & Lymphoma, 10.1080/10428194.2025.2602045, (1-10), (2026).